Embed Size (px)
Citation preview
Distal pancreatectomy with splenicpreservation revisitedJ. Rubén Rodríguez, MD,a Michael G. Madanat, BA, MSc,a Brian C. Healy, PhD,b
Sarah P. Thayer, MD, PhD,a Andrew L. Warshaw, MD,a and Carlos Fernández-del Castillo, MD,a
Boston, Mass
Background. Splenic preservation (SP) during distal pancreatectomy can be accomplished by ligatingthe main splenic artery and vein relying on blood supply from the short gastric vessels. The purpose ofthis study was to examine the short-term implications of this operation, comparing it to the outcomesfollowing distal pancreatectomy with splenectomy.Methods. The records of 259 patients who underwent distal pancreatectomy with and without SP atMassachusetts General Hospital from 1994 to 2004 were reviewed.Results. A total of 29% of patients underwent SP with this technique. These patients were more likelyto be women (74% vs 56%, P � .008) and to have benign disease (93% vs 54%, P � .0001).Their operative times were shorter (2.5 vs 3.1 h, P � .0001), they had less blood loss (300 vs 500 ml,P � .0001) and a shorter duration of stay (6 days [interquartile range, 5 to 7] vs 7 days[interquartile range, 5 to 8], P � .001). SP was not a significant predictor of complications in eitherunivariate (P � .445) or adjusted analysis (P � .543). One patient (1.4%) in the SP group wasreoperated for splenic infarction and two patients (1.1%) in the splenectomy group for abscess andhemorrhage. There were 2 (0.8%) postoperative deaths, both in the splenectomy group.Conclusions. Splenic preservation relying on blood supply from the short gastric vessels is reliable andsafe and does not have a higher incidence of postoperative complications when compared to traditionaldistal pancreatectomy with splenectomy. The current series validates this approach and provides furtherevidence of its feasibility and safety. (Surgery 2007;141:619-25.)
From the Department of Surgery, Massachusetts General Hospital a and Harvard School of Public Health,b Boston,
MassIn 1988, Andrew L. Warshaw1 described an alter-native approach to splenic preservation during dis-tal pancreatectomy, which involved ligating themain splenic artery and vein, relying on blood sup-ply from the short gastric vessels for perfusion.Since then, this has been the technique of choice atMassachusetts General Hospital (MGH) for pa-tients with benign tumors in the body or tail of thepancreas with favorable anatomic relationships tothe spleen, vessels, and surrounding structures.
Presented at the 66th Annual Meeting of the Society of Univer-sity Surgeons, San Diego, California, February 7-11, 2006.
Supported in part by the Claude E. Welch, MD, Resident Re-search Fellowship, Massachusetts General Hospital, Boston,Mass (J.R.R.).
Accepted for publication September 9, 2006.
Reprint requests: Carlos Fernández-del Castillo, MD, Depart-ment of Surgery, Massachusetts General Hospital, 15 ParkmanSt, WACC 336, Boston, MA 02114.
0039-6060/$ - see front matter
© 2007 Mosby, Inc. All rights reserved.
doi:10.1016/j.surg.2006.09.020
The short-term implications of this operationhave not been examined in depth. The purpose ofthis study is to describe a large single institutionalexperience with this surgical technique and, specifi-cally, to determine whether distal pancreatectomywith splenic preservation (SP) relying on perfusionfrom the short gastric vessels results in a higher rate ofpostoperative morbidity compared with traditionaldistal pancreatectomy with splenectomy (DPS).
PATIENTS AND METHODSA total of 259 patients who underwent distal
pancreatectomy from January 1, 1994 through Au-gust 31, 2004 at MGH were identified from a pro-spectively entered pancreatic surgery database.During that time period, 74 of the 259 patientsunderwent SP (29%). Comparisons were made be-tween these patients and those who underwentDPS. The patients’ postoperative clinical courseswere reviewed and detailed retrospectively throughcomputer, hospital, and clinic records to include30 postoperative days. This study was approved by
the MGH Institutional Review Board.SURGERY 619

620 Rodríguez et al SurgeryMay 2007
Definitions. Baseline data were collected, includ-ing age, sex, body mass index (BMI, kg/m2), his-tory of cardiac disease (defined as previousmyocardial infarction, stent placement, or coro-nary artery bypass grafting), history of chronic ob-structive pulmonary disease (COPD), history ofchronic renal insufficiency (defined as creatinine�2.0 mg/dL), history of preoperative diabetes mel-litus (defined as current use of oral hypoglycemicagents or insulin), documented history of priorpancreatitis, and history of previous pancreatic sur-gery. Operative data including operative time, esti-mated blood loss (as recorded in the anesthesiarecord), performance of splenectomy (our primarypredictor of interest), performance of additionalprocedures, final diagnosis, and presence of locallyinvasive disease on pathologic analysis of thespecimen.
The primary outcome of interest was the pres-ence or absence of any perioperative complication.Perioperative complications were defined as anymedical adverse event occurring within 30 days ofthe surgical procedure. Because complications af-ter distal pancreatectomy are largely due to thoseresulting from pancreatic leakage (PL) from thestump,2-5 complications were further subdividedinto those that were identified as PL-related andthose that were not. Complications identified asbeing related to PL were categorized using previ-ously published criteria.5 In brief, these complica-tions included: (1) pancreatic fistula, defined as dailyoutput of at least 30 ml of amylase-rich fluid (3times the serum concentration) from the surgicallyplaced drain after postoperative day 5; (2) sterilecollection, defined as a 3 � 3-cm or greater accumu-lation of fluid identified radiologically and prompt-ing interventional radiology drainage yieldingamylase-rich fluid; (3) abscess, defined as a collec-tion of fluid that upon aspiration and culture grewbacteria (although amylase concentration was notmeasured in all of these, they were considered tobe a result of PL); (4) wound disruption, consideredan indirect complication of a PL when ongoingdrainage of thick fluid through the incision waspresent, and the patient had a documented pan-creatic fistula, collection, or abscess. Other compli-cations not related to PL that met universallyaccepted definitions also were recorded. Thesecomplications included ileus, delirium, urinarytract infection, pneumonia, atelectasis, pulmonaryembolus, and myocardial infarction.
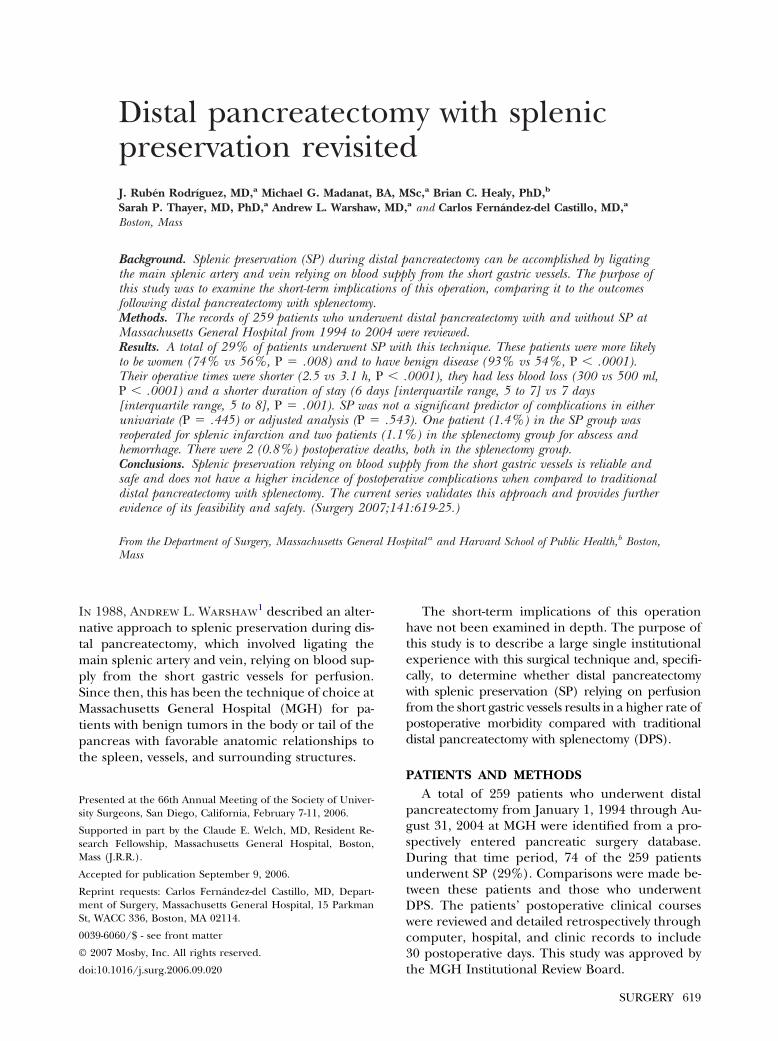
Operative technique. Splenic preservation usingthe technique of ligation of the splenic artery andvein relying on collateral circulation from the short
gastric vessels was performed for benign tumorsand when technically feasible in the absence oflocally advanced disease or splenomegaly. Thistechnique has been described in detail elsewhere.1
In brief, the lesser sac is entered through the gas-trocolic omentum outside the gastroepiploic ar-cade while carefully sparing the short gastricarteries and veins and, when possible, the commu-nicating vessel between the splenic hilum and theleft gastroepiploic artery. It is important to assesswhether splenic size is greater than normal and torecognize vascular anatomic variations, such as apaucity of short gastric vessels. These assessmentsare done by computed tomography (CT)and intra-operative assessment. Surgical judgment also mustbe applied as to whether the spleen will survive. Ifeither of these conditions is present, splenic pres-ervation using splenic artery and vein ligationshould not be attempted. The pancreas is thenmobilized by incising the retroperitoneum alongthe left inferior margin and opening the avascularplane behind it. Dissection is carried to the left,past the tip of the pancreas. The splenic artery andvein are ligated as close as possible to the pancreasto leave collaterals in the hilum untouched and atthe point of pancreatic transection. The spleen isleft undisturbed in its bed (Fig 1, A and B). Thepancreas routinely is transected with electrocau-tery, the pancreatic duct is ligated if identified, andthe stump closed with silk sutures. In fewer than5% of cases, a TA-55 reticulating stapler (UnitedStates Surgical Corp, Norwalk, Conn) is used to di-vide the pancreas. A closed suction drain (Jackson-Pratt, Dublin, Ohio) is left in the vicinity of thepancreatic stump, and removed on postoperativeday 4 or 5 (once the patient has resumed oralintake) if the output is �30 ml/day and/or theamylase is �3 times the normal serum concentra-tion. There were no laparoscopic resections in thiscohort.
Statistical methods. For comparisons betweenthe SP and DPS groups with respect to baseline andsurgical characteristics, the Fisher exact test andthe Wilcoxon rank sum test were used. Medianvalues of the continuous variables and interquartileranges are presented. A P value �.05 was consid-ered statistically significant. Univariate logistic re-gression was used to determine if there was anassociation between SP and postoperative compli-cations and to examine other variables to assesstheir effects as potential confounders. Odds ratioswith the appropriate confidence intervals for eachof these factors were calculated. A multiple logisticregression was modeled, which included variablesidentified in the univariate analysis as potential
confounders and variables identified a priori as
Surgery Rodríguez et al 621Volume 141, Number 5
related to the exposure and outcome. Other factorswere added to the model if there was a 10% changein the odds ratio of the exposure.
RESULTSCharacteristics of patients who had SP and pa-
Figure. a, Technique of mobilization of the left pancreasby incising the retroperitoneum along the pancreaticmargins. b, The splenic vessels are then ligated as close aspossible to the pancreas and also at the point of pancre-atic transection. The collateral circulation to the spleenvia short gastric vessels is preserved.
tients who underwent DPS are shown in Table 1. As
expected, patients selected to undergo SP weremore likely to have benign disease as an indication(93% vs 54%, P � .0001) and to be women (74% vs56%, P � .008). The SP and DPS groups wereotherwise similar in regard to their clinical charac-teristics. Table II depicts the indications for surgeryin the entire cohort.
Table III compares operative factors and postop-erative morbidity between the groups. Patients whounderwent SP had shorter operative times (2.5 h vs3.1 h, P � .0001), less blood loss (300 vs 500 ml,P � .0001) and a shorter duration of stay (6 days[interquartile range, 5 to 7] vs 7 days [interquartilerange, 5 to 8], P � .001). They also were less likelyto undergo additional procedures and to have lo-cally advanced disease.
No significant differences between the SP andDPS groups were found for pancreatic leak–relatedcomplications (36% vs 33%, P � .668) or for othercomplications not related to PL (18% vs 25%, P �.191). Table IV describes the breakdown of thePL-specific complications between groups. As ex-pected, significant overlap existed between patientsthat experienced PL-related complications, withmany of the pancreatic leaks manifesting as com-binations of fistula, collection, abscess, and/orwound disruption.
SP was not identified as a significant predictor ofpostoperative complications on univariate analysis(Table V). The odds ratio of having a complicationcomparing splenectomy to splenic preservation was1.23 (P � .445). The odds of having a complicationwere slightly higher in the splenectomy group, butthis result was not significant. To gain further in-sight into other factors that might be related topostoperative complications, other variables wereassessed as potential predictors or confounders.Male sex was identified as being significantly asso-ciated with the occurrence of a postoperative com-plication (P � .011). Additional procedures (P �.006), operative time (P � .001), locally advanceddisease (P � .031), and blood loss (P � .001) alsowere significant predictors of a postoperative com-plication on univariate analysis. A history of pan-creatitis did not reach statistical significance(P � .08).
Multiple logistic regression models were usedto control for potential confounders. BMI and ahistory of pancreatitis were included in all modelsbecause previous reports have identified them asbeing factors related to PL.6,7 Sex also was includedin all models based on results from Tables 1 and III.Operative time, blood loss, locally advanced dis-ease, and additional procedures also were included
in different combinations in the models because
622 Rodríguez et al SurgeryMay 2007
these factors were considered indirect measures ofa more difficult operation, a principal confounderthat cannot be directly measured. Operative timeand blood loss were found to be significantly cor-related (P � .0001), and so only 1 of these wasincluded in the final model because of colinearity.The model that best fit the data with the aboveconstraints is shown in Table VI. No additionalvariables significantly improved the fit of themodel. These results indicate that, on adjustedanalysis, SP was again not identified as a predictorof morbidity (P � .5). The only significant predic-tors of morbidity in the multivariate model wereincreased blood loss (odds ratio, 1.62) and addi-tional procedures (odds ratio, 1.9).
One patient (1.4%) in the SP group had to bereoperated for splenic infarction. Another patientwas reexplored out of concern for infarction. On
Table I. Characteristics of patients who underwentraditional splenectomy
SPn � 74
DemographicsFemale 74%Median age (y) 54.5 (IQR,Median BMI (kg/m2) 25 (IQR,
Clinical HxCardiac history 10.3COPD 1.3Chronic renal insufficiency 2.6Preoperative diabetes 9%History of pancreatitis 19.2History of pancreatic surgery 10.3Benign disease 93.2
SP, Splenic preservation; DPS, distal pancreatectomy with splenectomypulmonary disease.*Fisher exact test.†Wilcoxon rank sum test.
Table II. Indications for distal pancreatectomy in259 patients
Indication %
Mucinous cystic neoplasm 20Adenocarcinoma 17Neuroendocrine tumor 17Chronic pancreatitis 10Serous cystadenoma 7Pseudocyst 5†Other 16
†Intraductal papillary mucinous neoplasm, sarcoma, metastatic cancer,acinar carcinoma, lymphoma, solid pseudopapillary tumor, dermoid tu-mor, simple cyst.
the fourth postoperative day, this patient devel-
oped left upper quadrant pain and a CT scan wasinterpreted as showing absence of perfusion. Uponexploration, the spleen was found to be normal.Two patients (1.1%) in the DPS group were reop-erated for abscess and hemorrhage. Overall mor-tality was 0.8% (2 patients); both deaths occurred
l pancreatectomy with splenic conservation vs.
)DPS
n � 185 (71%) P value
56% .008†68) 58 (IQR, 47-70) .30*) 25 (IQR, 22-30) .48*
11.6% .83†2.8% .67†3.9% .73†
13.3% .41†22.1% .74†8.3% .64†
53.5% �.001†
body mass index; IQR, interquartile range; COPD, chronic obstructive
Table III. Operative factors and postoperativecomplications of patients who underwent distalpancreatectomy with splenic conservation vstraditional splenectomy
SPn � 74(29%)
DPSn � 185(71%) P value
Median OR time (h) 2.5 3.1 �.001*Additional
procedures24.4% 39.7% .02†
Blood loss (ml) 300 500 �.001*Locally advanced 6.4% 32.6% �.001†Median LOS (d) 6 (IQR, 5-7) 7 (IQR, 5-8) .001*Pancreatic leak 36% 33% .67†Fistula 27% 17% .09†Collection 8% 9% 1.00†Abscess 8% 14% .21†Wound disruption 8% 10% .65†Other (complication
not related toleak)
18% 25% .20†
Reoperation 2.7% 1.1% .70†Mortality 0 1.1% .90†
SP, Splenic preservation; DPS, distal pancreatectomy with splenectomy;OR, operating room; LOS, length of stay; IQR, interquartile range.*Fisher exact test.†Wilcoxon rank sum test.
t dista
(29%
pve 44-22-30
%%%
%%%
; BMI,
in the DPS group.

Surgery Rodríguez et al 623Volume 141, Number 5
DISCUSSIONFriedrich Trendelenburg8 is credited as the first
surgeon to resect a solid tumor of the tail of thepancreas in 1882 at the University of Bonn, Ger-many. For decades, concomitant splenectomy wasconsidered a necessity in distal pancreatectomy un-til splenic preservation was formally described byMallet-Guy and Vachon in 1943.9 These authorsdescribed a technique whereby the multiple small
Table IV. Comparison of PL-relatedcomplications and other complications notrelated to PL between patients who underwent SPand patients who underwent traditional DPS
Complication SP (%) DPS (%)
Fistula 27 17Collection 8 9Abscess 8 14Wound disruption 8 10Other 18 25
PL, Pancreatic leakage; SP, splenic preservation; DPS, distal pancreatec-tomy with splenectomy.All differences failed to reach statistical significance.
Table V. Univariate analysis between predictorand occurrence of any postoperativecomplication following distal pancreatectomy,These results are the odds of having acomplication
Factor* Odds ratio (95% CI)†
Operation performedSplenectomy 1.23 (0.721, 2.11)Splenic preservation 1
SexMale 1.98 (1.17, 3.36)Female 1
History of pancreatitisYes 1.76 (0.935, 3.33)No 1
Additional proceduresYes 2.15 (1.25, 3.71)No 1
Operative time (h) 1.46 (1.18, 1.82)Locally advanced disease
Yes 1.95 (1.06, 3.57)No 1
Blood loss (/1000) 3.14 (1.72, 5.73)
CI, Confidence interval.Results shown are the odds of a patient experiencing a complication.*Other variables including age, body mass index, cardiac history, chronicobstructive pulmonary disease, renal failure, preoperative diabetes, andhistory of pancreatic surgery did not reach statistical significance.†Continuous predictors were not categorized, and so the odds ratios forthese predictors correspond to a 1-unit increase in each predictor.
branches that connect the splenic vessels to the
pancreas are individually dissected and ligated.10
Since then, several authors have reported theirexperience with this operation with minimal mor-tality and acceptable morbidity.11-14
In a large series of distal pancreatectomy (n �235) from Johns Hopkins, this traditional splenicpreservation was possible in 16% of patients.15 Theauthors of this study found no difference in oper-ative time, blood loss, morbidity, or mortality be-tween the 2 groups, but they did report anunexplained longer duration of stay in the SPgroup (15 vs 10 days, P � .008).15
In another large series of distal pancreatectomy(n � 125) from Memorial Sloan Kettering (whichexcluded patients with adenocarcinoma), 37% ofpatients had SP using the traditional technique.14
The authors of this study demonstrated a lowerincidence of what they considered severe compli-cations in the SP group compared to the DPSgroup and concluded that, in their hands, SP usingthe traditional technique was the operation ofchoice for distal pancreatic disease other than ad-enocarcinoma.14
In this paper, we described the largest single-institution series of distal pancreatectomy. Further-more, we illustrated that SP relying on the shortgastric vessels applied to 29% of patients, althoughassociated with a small need for reexploration re-lated to splenic infarct (2.7%), did not have ahigher incidence of postoperative complicationswhen compared to DPS. We also found that pa-tients who underwent SP with this technique hadshorter operative times (2.5 h vs 3.1 h, P � .0001),
Table VI. Multiple logistic regression model ofpredictors of morbidity following distalpancreatectomy
Predictors Odds ratio (95% CI)
Type of operationSplenectomy 0.814 (0.451, 1.47)Splenic preservation
BMI (kg/m2) 1.01 (0.955, 1.06)History of pancreatitis
Yes 1.53 (0.767, 3.06)No
SexMale 1.43 (0.796, 2.56)Female
Blood loss (/1000) 2.62 (1.39, 4.95)Additional procedures
Yes 1.90 (1.05, 3.44)No
BMI, Body mass index.
less blood loss (300 vs 500 ml, P � .0001) and a

624 Rodríguez et al SurgeryMay 2007
shorter duration of stay (6 days [interquartilerange, 5 to 7] vs 7 days [interquartile range, 5 to 8],P � .001).
The original report describing this techniquefor SP1 included 1 patient who was reexplored forsplenic infarction in a series of 22 patients. Conse-quently, radionuclide spleen scans were performedroutinely in all patients undergoing SP at our insti-tution. This practice has since been abandonedsecondary to its low yield. We currently do notrecommend routine imaging for these patients andrely only on close clinical follow-up. To avoidsplenic infarction, it is important to select patientswithout a large spleen. Perfusion from the shortgastric vessels has proven to be inadequate to sup-port more than the usual volume of parenchyma.1
Consequently, the surgeon must also inspect thecolor of the spleen at the outset and again atthe conclusion of the operation. The spleen willusually appear a darker gray than it was, but it willretain at least a burgundy red hue showingthrough, indicating sufficient perfusion. Some-times a demarcated geographic area may clearly bedifferentially underperfused relative to the rest ofthe organ. If this is small (for example, only thelower pole), it has not proven to be a problem. Ifmore than a third of the spleen appears to beunderperfused, it is safer to resect it. Presence ofacute inflammation is also a contraindication forthis technique, because the patency of the shortgastric vessels cannot be ascertained.
Caution also must be used when interpreting theresults of postoperative imaging studies when thistechnique is performed. In the current series, 1patient who underwent reexploration on postoper-ative day 4 in the SP group was incorrectly identi-fied as having massive splenic infarction by CT. Shewas experiencing pain in the left upper quadrant,but intraoperative findings included a viable spleenthat was left in situ. In retrospect, the apparent lackof splenic perfusion by CT was in reality an overre-action to hypoperfusion and a “delayed” arrival ofthe bolus of contrast via the short gastric vesselsinstead of the splenic artery. The second patientthat was reexplored on postoperative day 3 for leftupper quadrant pain and fever did have splenicinfarction requiring splenectomy. It is important tonote that reoperation rates were no different in theDPS group compared with the SP group (2.7% vs1.1%, P � .70). The 2 reoperations in the DPSgroup were for abscess and hemorrhage.
The mortality in this series of distal pancreatec-tomy was 0.8%, but the overall complication rateremained high, particularly complications associ-
ated to PL. We sought to identify factors associatedwith development of postoperative complicationsand found that SP was not associated with a higherlikelihood of developing complications by univari-ate and multivariate analysis. The only factors thatwere found to be significantly and independentlyassociated with a higher complication rate wereincreased blood loss and additional procedures.
The benefits of SP are well documented. Asple-nia confers a modest lifetime risk for developingoverwhelming postsplenectomy infection (OPSI)of 1% to 5% in general populations, and OPSI isassociated with a mortality of up to 50%.16-21
In addition, concern for an increased risk of ma-lignancy in later years also has been raised in pa-tients undergoing elective splenectomy.22 It is forthis reason that we concur with others that splenicpreservation should be carried out, when anatom-ically feasible, for benign lesions of the body andtail of the pancreas.10,14
It is important to reiterate that the present studyfocuses on the short-term outcomes of this opera-tion, and there is only scant information on thelong-term consequences of splenic vessel ligation.Although splenic function and circulation aftersplenic vessel ligation have been well documented,the appearance of gastric and perigastric varices onsubsequent imaging as the short gastric and gastro-epiploic vessels accommodate to the increasedblood flow is to be expected.23-25 Miura et al,25 infact, reported the presence of perigastric varicesseen on CT in 7 of 10 patients who underwent SPand a 20% frequency of submucosal varices. In ourexperience, upper gastrointestinal bleeding as aresult of SP has not occurred. However, there hasbeen a single case report of gastrointestinal bleed-ing from gastric varices occurring 6.5 years aftermiddle segment pancreatectomy after SP with ex-cision of the splenic artery and vein.25
The current series confirms that distal pancrea-tectomy with splenic preservation can be accom-plished by ligating the splenic artery and vein,relying on the short gastric vessels for splenicperfusion in selected patients. When feasible, thetechnique is reliable and, as attested to by theshorter operative time and less blood loss, simpler.We propose that this technique provides an attrac-tive alternative to the more tedious, traditionalapproach of ligating the branches between thesplenic vessels and the pancreas. As laparoscopicdistal pancreatic resections are becoming morecommonplace, this simplified method of SP is be-ing increasingly utilized.26-31 The current series val-idates this approach and provides further evidence
of its feasibility and safety.
Surgery Rodríguez et al 625Volume 141, Number 5
REFERENCES1. Warshaw AL. Conservation of the spleen with distal pancre-
atectomy. Arch Surg 1988;123:550-3.2. Fahy BN, Frey CF, Ho HS, Beckett L, Bold RJ. Morbidity,
mortality, and technical factors of distal pancreatectomy.Am J Surg 2002;183:237-41.
3. Bassi C, Butturini G, Molinari E, et al. Pancreatic fistula rateafter pancreatic resection. The importance of definitions.Dig Surg 2004;21:54-9.
4. Balzano G, Zerbi A, Cristallo M, Di Carlo V. The unsolvedproblem of fistula after left pancreatectomy: the benefit ofcautious drain management. J Gastrointest Surg 2005;9:837-42.
5. Rodriguez JR, Soto SG, Pandharipande PV, Gazelle GS,Thayer SP, Warshaw AL, et al. Implications and cost ofpancreatic leak following distal pancreatic resection. ArchSurg 2006;141:361-5; discussion 366.
6. Sledzianowski JF, Duffas JP, Muscari F, Suc B, Fourtanier F.Risk factors for mortality and intra-abdominal morbidityafter distal pancreatectomy. Surgery 2005;137:180-5.
7. Montorsi M, Zago M, Mosca F, et al. Efficacy of octreotide inthe prevention of pancreatic fistula after elective pancreaticresections: a prospective, controlled, randomized clinicaltrial. Surgery 1995;117:26-31.
8. Howard JM, Hess W. History of the pancreas: mysteries of ahidden organ. New York: Kluwer Academic/Plenum Pub-lishers; 2002.
9. Mallet-Guy P, Vachon A. Pancreatites chroniques gauches.Paris: Masson & Cie; 1943.
10. Von Hoff D, Evans DB, Hruban RH. Pancreatic cancer.Sudbury: Jones and Bartlett Publishers; 2005.
11. Kimura W, Inoue T, Futakawa N, Shinkai H, Han I, Muto T.Spleen-preserving distal pancreatectomy with conservationof the splenic artery and vein. Surgery 1996;120:885-90.
12. Aldridge MC, Williamson RC. Distal pancreatectomy withand without splenectomy. Br J Surg 1991;78:976-9.
13. Richardson DQ, Scott-Conner CE. Distal pancreatectomywith and without splenectomy. A comparative study. AmSurg 1989;55:21-5.
14. Shoup M, Brennan MF, McWhite K, Leung DH, Klimstra D,Conlon KC. The value of splenic preservation with distalpancreatectomy. Arch Surg 2002;137:164-8.
15. Lillemoe KD, Kaushal S, Cameron JL, Sohn TA, Pitt HA, YeoCJ. Distal pancreatectomy: indications and outcomes in 235patients. Ann Surg 1999;229:693-8; discussion 698-700.
16. Cullingford GL, Watkins DN, Watts AD, Mallon DF. Severe
late postsplenectomy infection. Br J Surg 1991;78:716-21.17. Holdsworth RJ, Irving AD, Cuschieri A. Postsplenectomysepsis and its mortality rate: actual versus perceived risks.Br J Surg 1991;78:1031-8.
18. Lynch AM, Kapila R. Overwhelming postsplenectomy infec-tion. Infect Dis Clin North Am 1996;10:693-707.
19. Davidson RN, Wall RA. Prevention and management ofinfections in patients without a spleen. Clin Microbiol Infect2001;7:657-60.
20. Lutwick LI. Life threatening infections in the asplenic orhyposplenic individual. Curr Clin Top Infect Dis 2002;22:78-96.
21. Bowman SM, Zimmerman FJ, Christakis DA, Sharar SR,Martin DP. Hospital characteristics associated with the man-agement of pediatric splenic injuries. JAMA 2005;294:2611-7.
22. Mellemkjoer L, Olsen JH, Linet MS, Gridley G, McLaughlinJK. Cancer risk after splenectomy. Cancer 1995;75:577-83.
23. Sato Y, Shimoda S, Takeda N, Tanaka N, Hatakeyama K.Evaluation of splenic circulation after spleen-preserving dis-tal pancreatectomy by dividing the splenic artery and vein.Dig Surg 2000;17:519-22.
24. Miura F, Takada T, Asano T, Ochiai T. Gastric varicesoccurring after middle-segment pancreatectomy preservingspleen with division of splenic artery and vein. Surgery2004;135:696-7.
25. Miura F, Takada T, Asano T, et al. Hemodynamic changesof splenogastric circulation after spleen-preserving pancre-atectomy with excision of splenic artery and vein. Surgery2005;138:518-22.
26. Shimizu S, Tanaka M, Konomi H, Tamura T, Mizumoto K,Yamaguchi K. Spleen-preserving laparoscopic distal pancre-atectomy after division of the splenic vessels. J Laparoen-dosc Adv Surg Tech A 2004;14:173-7.
27. Shimizu S, Tanaka M, Konomi H, Mizumoto K, YamaguchiK. Laparoscopic pancreatic surgery: current indications andsurgical results. Surg Endosc 2004;18:402-6.
28. Fernandez-Cruz L, Martinez I, Gilabert R, Cesar-Borges G,Astudillo E, Navarro S. Laparoscopic distal pancreatectomycombined with preservation of the spleen for cystic neo-plasms of the pancreas. J Gastrointest Surg 2004;8:493-501.
29. Mabrut JY, Fernandez-Cruz L, Azagra JS, et al. Laparoscopicpancreatic resection: results of a multicenter Europeanstudy of 127 patients. Surgery 2005;137:597-605.
30. Root J, Nguyen N, Jones B, et al. Laparoscopic distal pan-creatic resection. Am Surg 2005;71:744-9.
31. Velanovich V. Case-control comparison of laparoscopic ver-sus open distal pancreatectomy. J Gastrointest Surg 2006;
10:95-8.
![Disclaimer - s-space.snu.ac.krs-space.snu.ac.kr/bitstream/10371/142374/1/000000150887.pdf · 1994, when Cuschieri [5] reported the first laparoscopic distal pancreatectomy and Gagner](https://img.dokumen.tips/doc/110x75/6050877ca02ba774652bd998/disclaimer-s-spacesnuackrs-spacesnuackrbitstream103711423741-1994.jpg)



























