Embed Size (px)
DESCRIPTION
Distal intraarticular humerus fractures. Cimerman Matej Dpt. for Traumatology Univ. Clinical Centre Ljubljana, Slovenia. facts. distal humerus fractures remain one of the most demanding challenges in orthopedic and trauma surgery (Korner, J Orthop Trauma 2004, Soon, Injury 2004) - PowerPoint PPT Presentation
Citation preview
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
Distal intraarticular Distal intraarticular humerus fractureshumerus fractures
Cimerman MatejDpt. for Traumatology
Univ. Clinical Centre Ljubljana, Slovenia
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
factsfacts
• distal humerus fractures remain one of the most demanding challenges in orthopedic and trauma surgery (Korner, J Orthop Trauma 2004, Soon, Injury 2004)
• distal humerus fractures in adults are rare (2-6% of all fractures)
• unsatisfactory results in 20% (Jupiter and Morrey, 1993)
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
solution...solution...
• every senior trauma and orthopedic surgeon should know to treat basics of these fractures
• and should know and respect his limits
• every big trauma center needs some monomaniacs
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
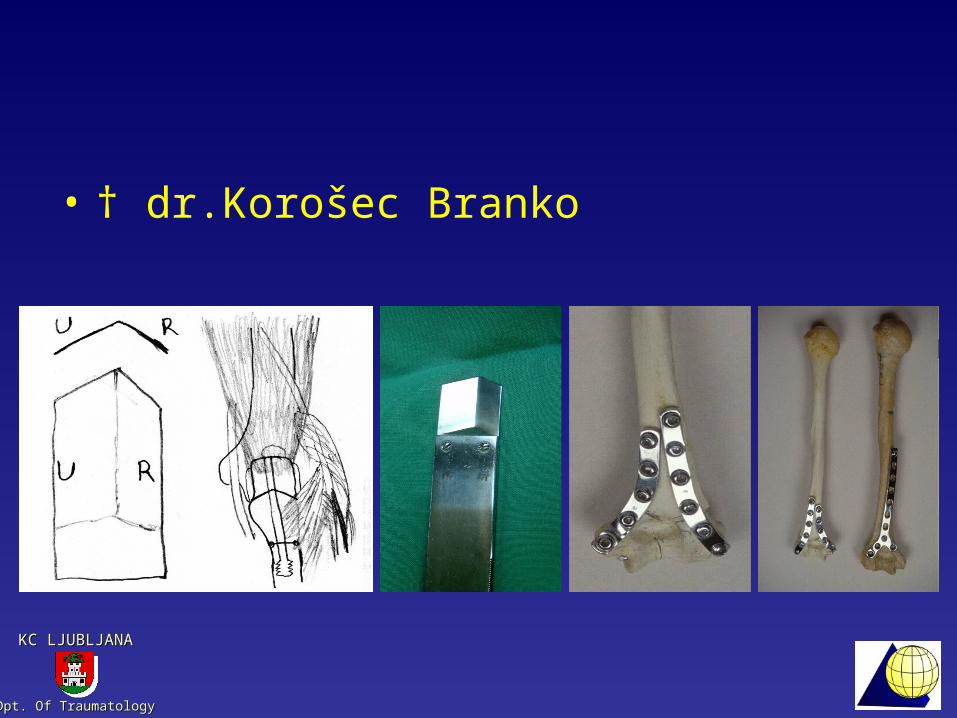
• † dr.Korošec Branko
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
treatment of articular treatment of articular fractures (we know fractures (we know
everything)everything)• ...anatomical reduction and stable
fixation• metaphyseal defects should be
grafted to prevent articular displacement
• metaphyseal and diaphyseal displacement should be reduced to prevent joint overloading
• immediate motion (AO, Shatzker 1987)

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
easy to say, difficult to easy to say, difficult to realizerealize
• small bone fragments• a lot of elderly people with
osteopenic bone• difficult approach• elbow joint hates even short
immobilization• long lever arms
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
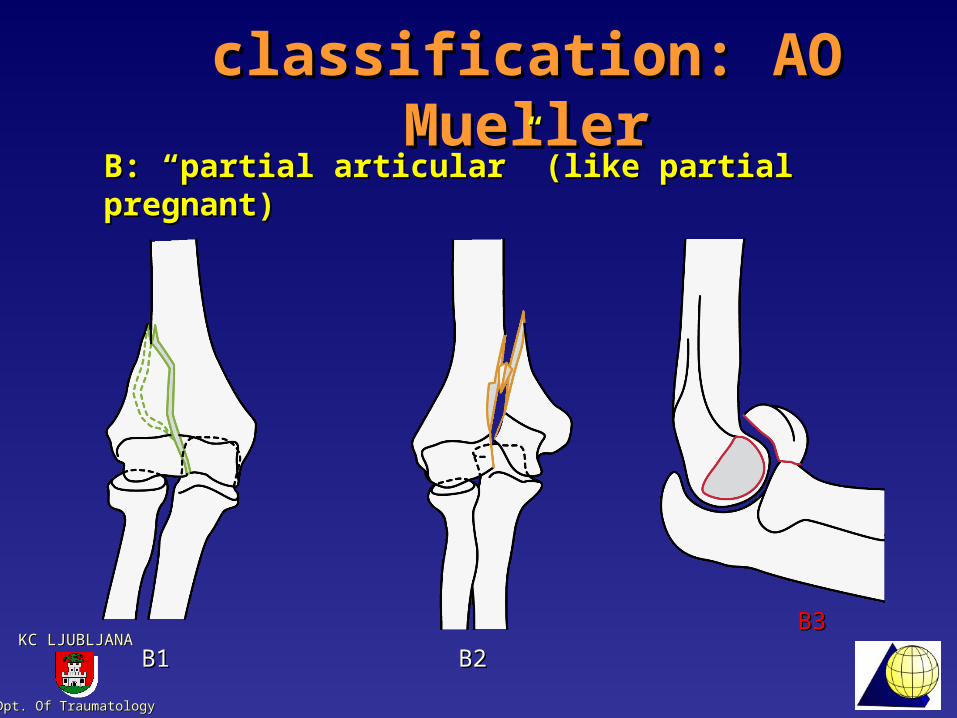
classification: AO Muellerclassification: AO Mueller
B1B1 B2B2
B3B3
B: “partial articular” (like partial pregnant)B: “partial articular” (like partial pregnant)
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
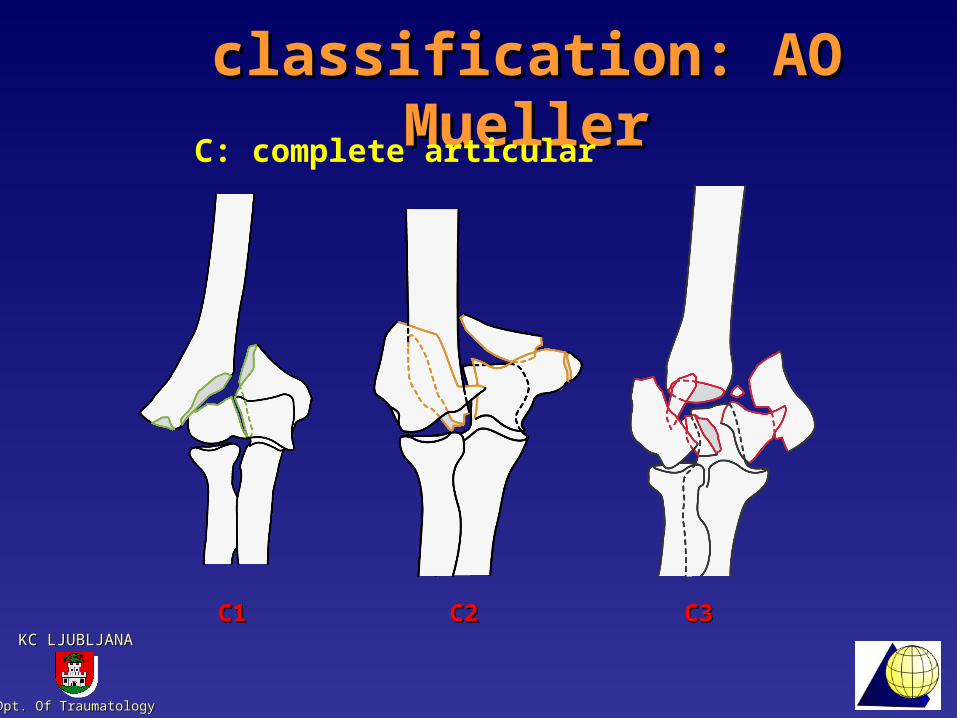
classification: AO Muellerclassification: AO Mueller
C1C1 C2C2 C3C3
C: complete articular
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
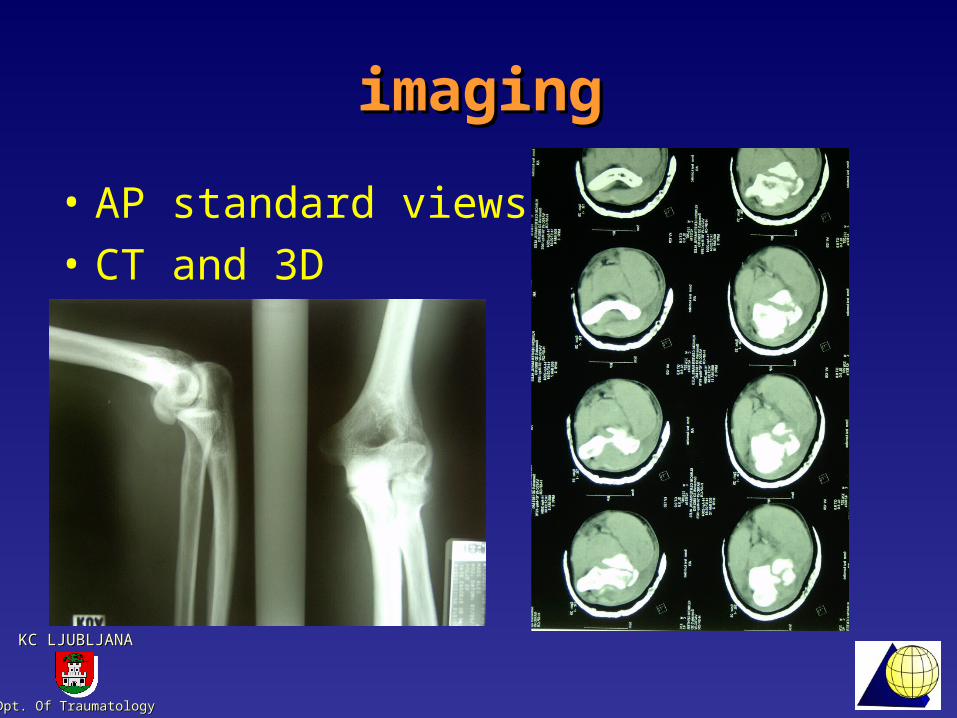
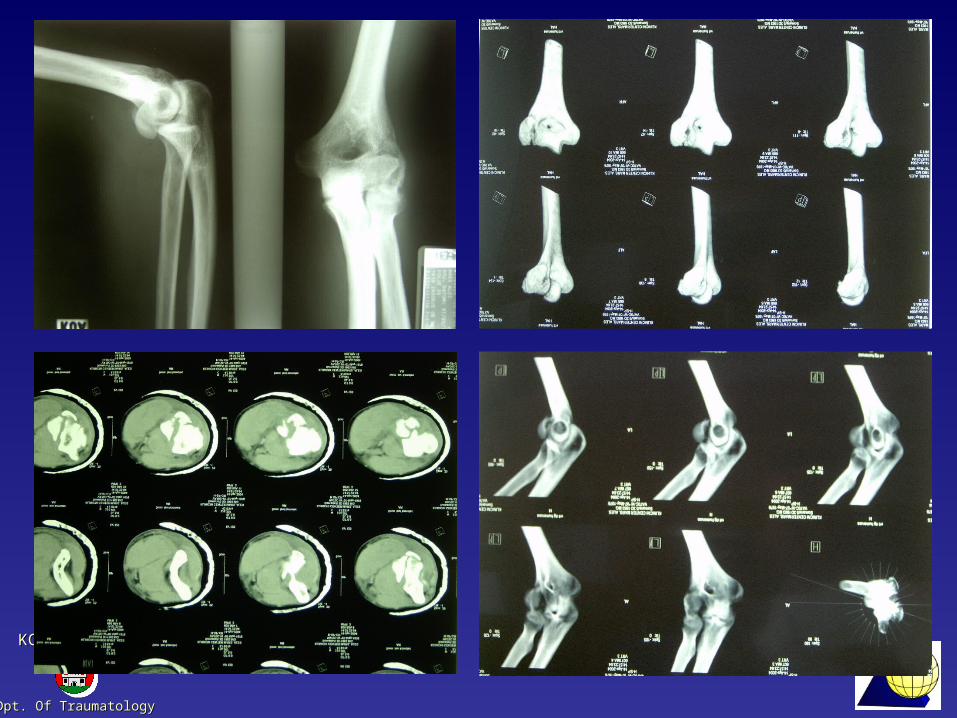
imagingimaging
• AP standard views• CT and 3D

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
imagingimaging
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
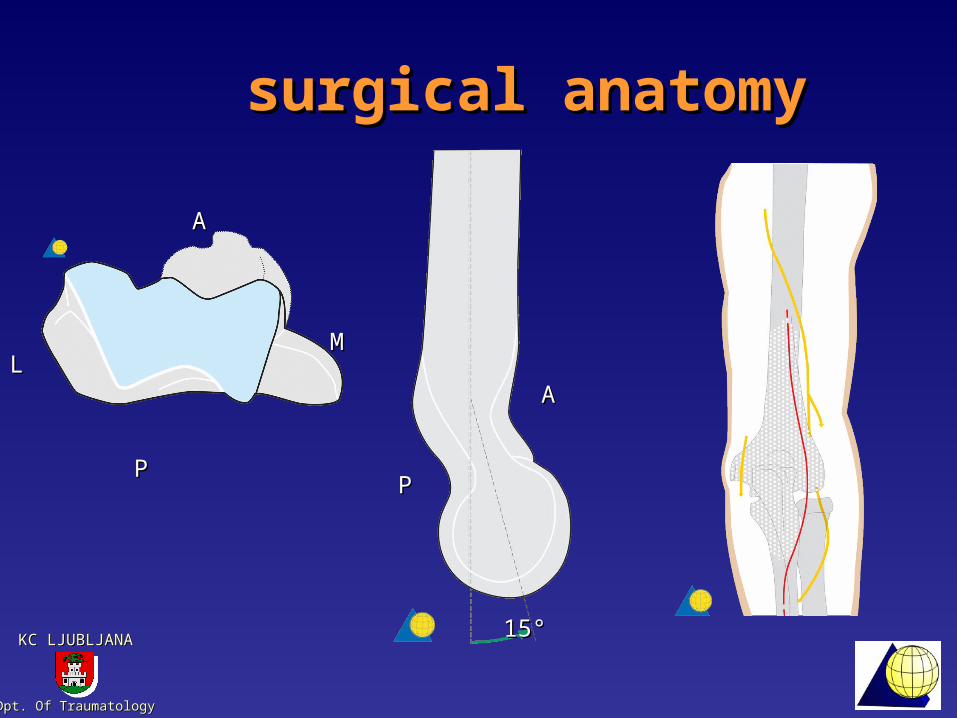
surgical anatomysurgical anatomy
1515°°
PP
AA
AA
PP
MMLL
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
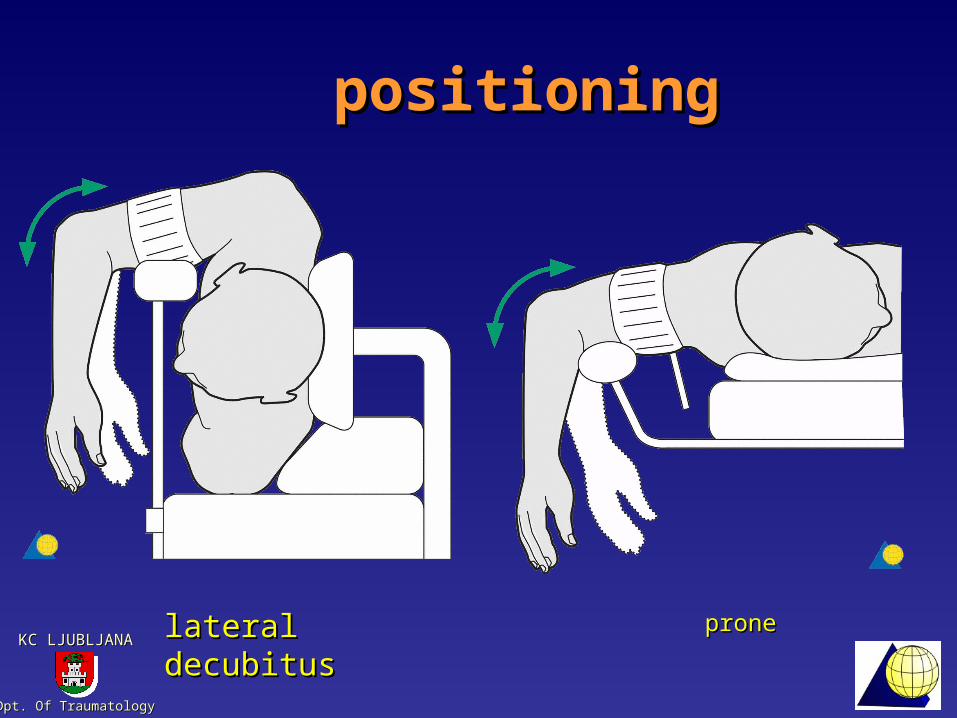
positioningpositioning
lateral decubituslateral decubitus proneprone
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
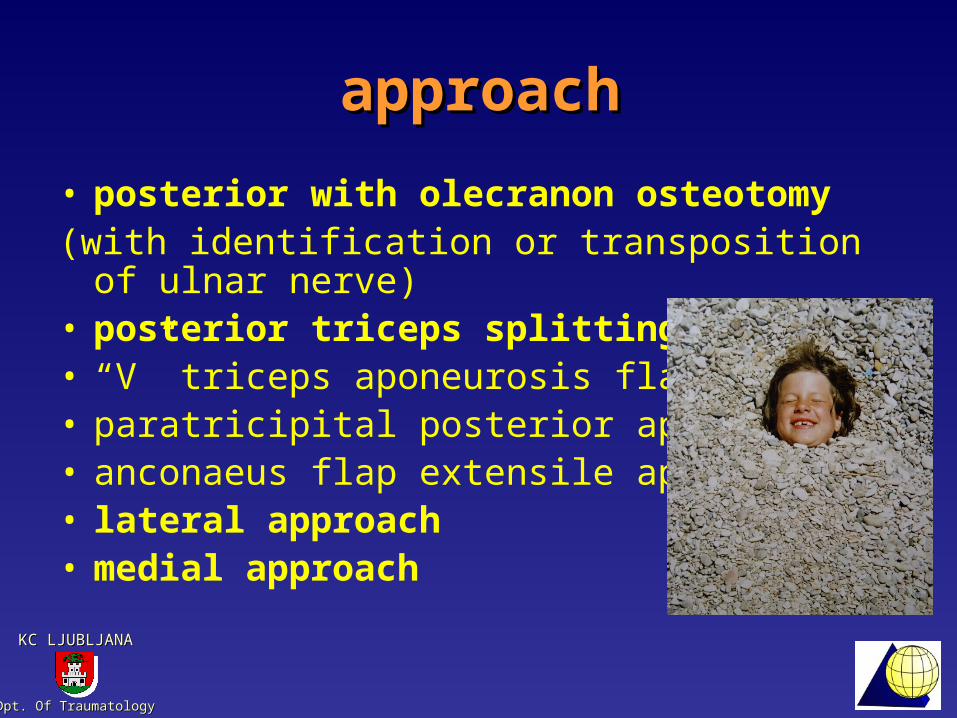
approachapproach
• posterior with olecranon osteotomy(with identification or transposition of ulnar
nerve) • posterior triceps splitting• “V” triceps aponeurosis flap• paratricipital posterior approach• anconaeus flap extensile approach• lateral approach• medial approach

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
olecranon osteotomyolecranon osteotomy
Chevron osteotomy, Korošec chissel, oscilating saw and chissel
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
triceps splittingtriceps splitting
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
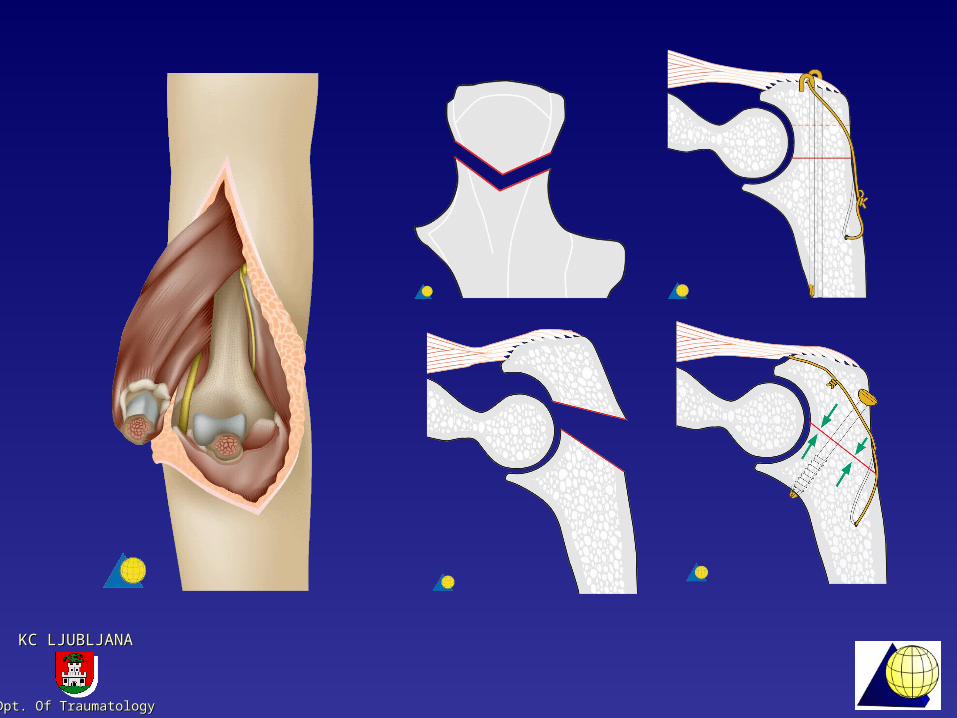
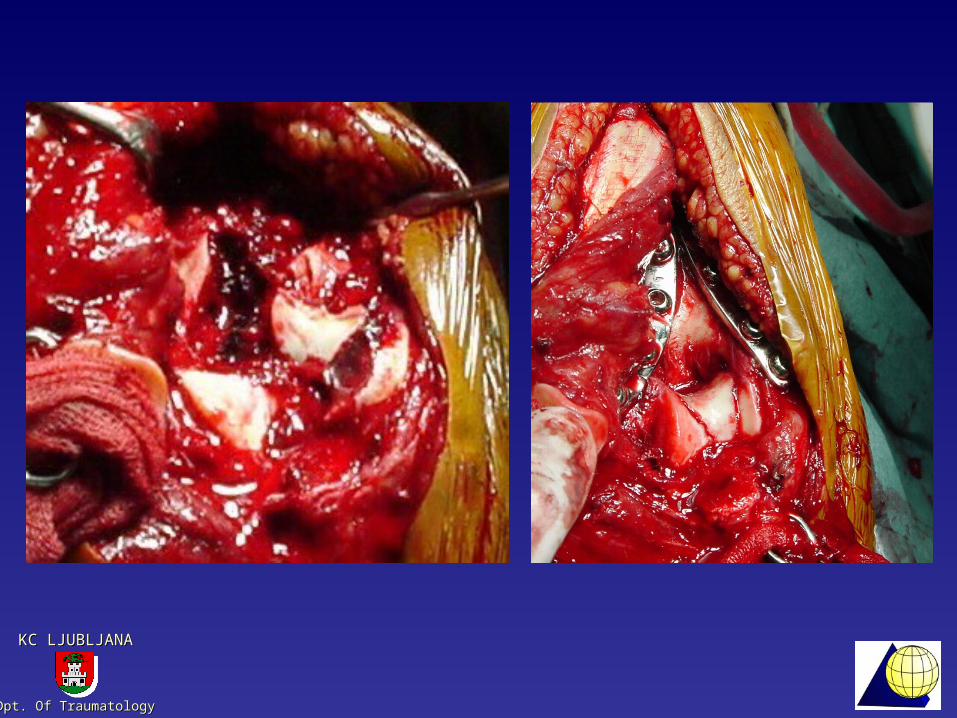
reduction and fixation reduction and fixation strategystrategy
• reducing and fixation of joint components
• coupling to methaphisys
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
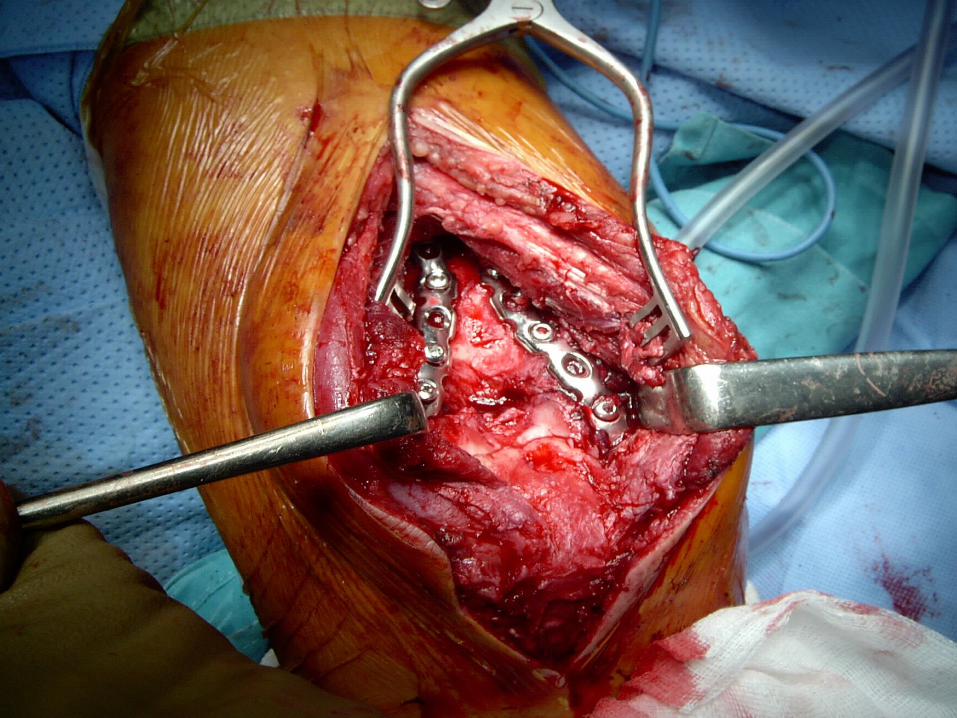
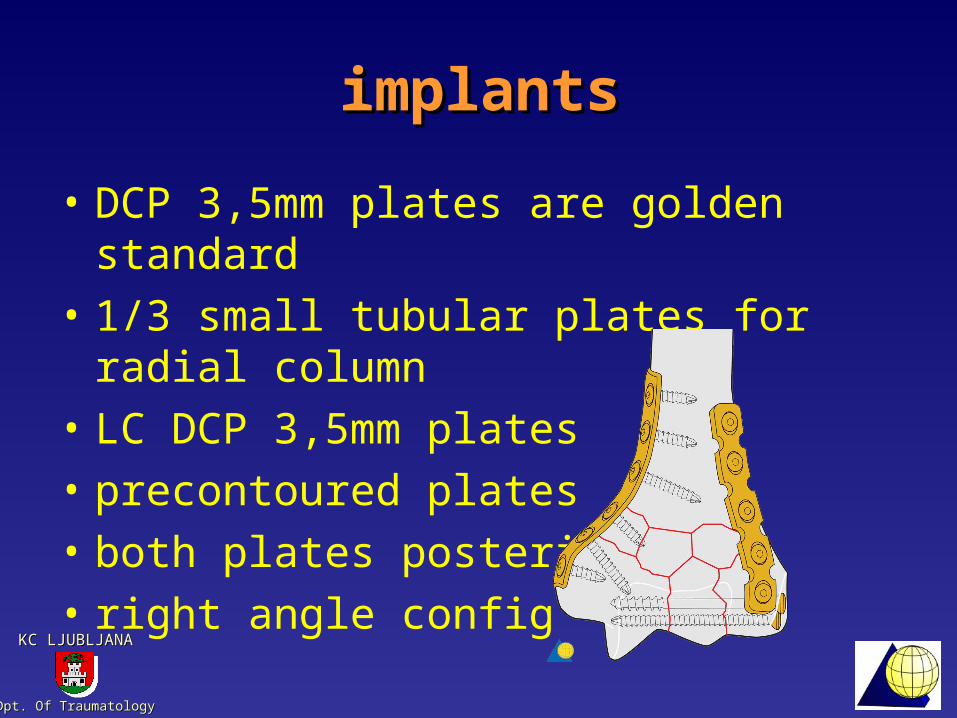
implantsimplants
• DCP 3,5mm plates are golden standard
• 1/3 small tubular plates for radial column
• LC DCP 3,5mm plates• precontoured plates• both plates posterior• right angle config

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA

Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
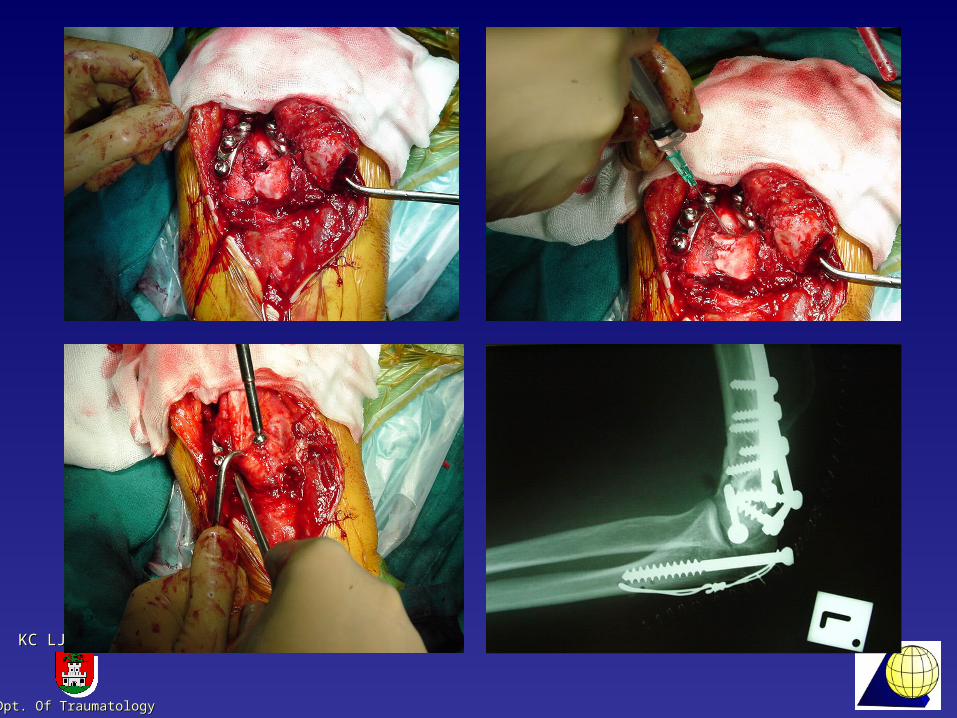
do not be afraid of ulnar do not be afraid of ulnar nervenerve
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
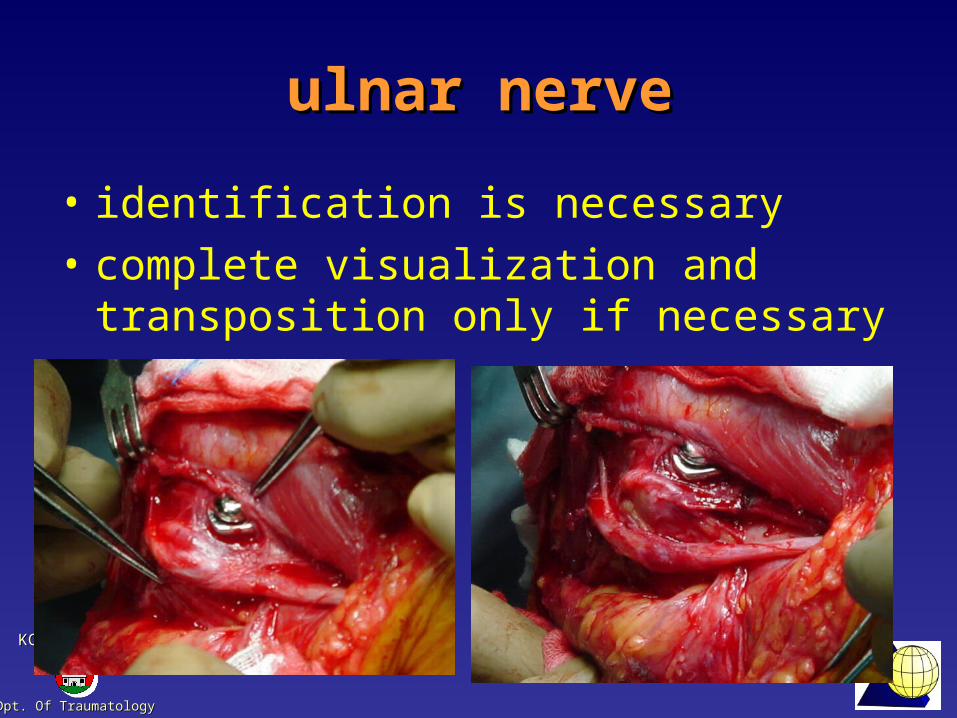
ulnar nerveulnar nerve
• identification is necessary• complete visualization and
transposition only if necessary
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
postoppostop
• active exercise under the control a soon as possible
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
complicationscomplications
• stiffness: arthrolysis, salvage procedures
• non union: refixation, TEP• infection• ulnar nerve paresis: revisions
Dpt. Of TraumatologyDpt. Of Traumatology
KC LJUBLJANAKC LJUBLJANA
conclusionsconclusions
• respect the fracture and your limits• olecranon osteotomy for C type
fractures• 3.5 mm reco plates golden standard• LC 3.5mm reco plates, 1/3 tubular
plates and precontoured plates• identify ulnar nerve• stable fixation mandatory• endoprosthesis as an option





























