Embed Size (px)
Citation preview

Clinical Vignette
60 Hong Kong J Nephrol • April 2004 • Vol 6 • No 1
Dissection of the Thoracic Aorta in a Patient with AutosomalDominant Polycystic Kidney Disease
Ozcan Keskin, Enes Murat Atasoyu,1 Murat Kalemoglu, Suat Unver,1 Yasar Kucukardali,2
Selim Nalbant,2 T. Rifki Evrenkaya1
Departments of Emergency Medicine, 1Nephrology, and 2Internal Medicine,Gulhane Military Medical Academy, Haydarpasa Training Hospital, Istanbul, Turkey.
Autosomal dominant polycystic kidney disease(ADPKD) is a systemic illness with a number of extra-renal manifestations. A 61-year-old male patient withknown ADPKD was admitted to the emergency roomof our hospital in May 2003 with severe chest painradiating to his neck and back, and a sense ofbreathlessness. There was no history of trauma.
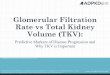
On admission, he was hypotensive (90/50 mmHg)and his heart rate was 110 beats/min. He had a mid-systolic murmur, which was most marked at the leftsternal edge. His peripheral pulses were weak. Bilater-al basal crepitations were found on pulmonaryexamination. Abdominal examination was normalexcept for large palpable polycystic kidneys. He hadno focal neurologic signs. Laboratory examinationshowed no significant abnormalities except for raisedserum urea (121 mg/dL) and creatinine (4.1 mg/dL).An electrocardiogram showed depression of ST seg-ments in the anterior leads. Emergency computerizedtomography scanning of the thorax and abdomen de-monstrated dissection and intramural thrombus withinthe descending thoracic aorta and bilateral polycystickidneys (Panels A and B).
He was transferred immediately for aortic surgery.During the operation, a type II thoracic aortic dissection
was observed. His recovery was complicated by theexpansion of the dissection and he died on the thirdpostoperative day.
Numerous cardiovascular abnormalities have beenreported in ADPKD patients, including heart valvelesion, cerebral aneurysm, splenic artery aneurysm,aortic root dilatation, abdominal aortic aneurysm,thoracic aortic dissection, and cervical artery dissection[1–3]. The prevalence of intracranial aneurysm andrupture are five-fold higher in ADPKD patients than inthe general population [4]. However, the prevalence ofextracerebral aneurysms is not clear. One autopsy seriesdescribed aortic dissection as being seven times morecommon in patients with ADPKD than in the generalpopulation [2]. Spontaneous artery dissection wasreported as a major complication in five unrelatedADPKD patients. All underwent spontaneous dissect-ion and none had phenotype of elastic tissue disorderor thoracic aortic dissection. Torra et al, in their case-control study, found a similar distribution of aorticdiameters in 139 ADPKD patients and their 149unaffected relatives [5]. The case reported by Paynteret al appears to be very similar to our case [3]. Arterialdissection may belong to the spectrum of extrarenalmanifestations of ADPKD. The association of ADPKD
Panel A. Thoracic computerized tomography scan showing aorticdissection and intramural thrombus (arrow).
Panel B. Abdominal computerized tomography scan showingbilateral multiple renal cysts: polycystic kidney disease (arrows).

Hong Kong J Nephrol • April 2004 • Vol 6 • No 1 61
Dissection of thoracic aorta in ADPKD
with aneurysms and arterial dissections suggests anabnormality of the structure of the arterial wall [6].Extracellular matrix components have been demon-strated to be abnormal in the pattern of deposition andin their proportions [7].
Aortic dissection is a fatal complication of ADPKD;clinicians need to maintain a high index of suspicionwhen dealing with ADPKD patients who present withchest pain.
REFERENCES
1. Leier CV, Baker PB, Kilman JW, Wooley CF. Cardiovascular ab-normalities associated with adult polycystic kidney disease. AnnIntern Med 1984;100:683–8.
2. Torres VE. Systemic manifestation of renal cystic disease. In:Gardner KD, Bernstein J, eds. Cystic Kidney (Developments in
Nephrology, No 27). Dordrecht: Kluwer Academic Publishers1990;295–326.
3. Paynter HE, Parnham A, Feest TG, Dudley CR. Thoracic aorticdissection complicating autosomal dominant polycystic kidneydisease. Nephrol Dial Transplant 1997;12:1711–3.
4. Pyrson Y, Chauveau D. Intracranial aneurysms. In: Watson M,Torres VE, eds. Autosomal Dominant Polycystic Kidney Disease.Oxford: Oxford University Press 1996;530–47.
5. Torra R, Nicolau C, Badenas C, Bru C, Perez L, Estivill X, et al.Abdominal aortic aneurysms and autosomal dominant polycystickidney disease. J Am Soc Nephrol 1996;7:2483–6.
6. Somlo S, Rutecki G, Giuffra LA, Reeders ST, Cugino A, WhittierFC. A kindred exhibiting cosegregation of an overlap connective tis-sue disorder and the chromosome 16 linked form of autosomal domi-nant polycystic kidney disease. J Am Soc Nephrol 1993;4:1371–8.
7. Calvet JP. Polycystic kidney disease: primary extracellular matrixabnormality or defective cellular differentiation? Kidney Int 1993;43:101–8.