Embed Size (px)
Citation preview
8/8/2019 Diogenes Lancet 1975
http://slidepdf.com/reader/full/diogenes-lancet-1975 1/5
366
19. Estrada-Parra, S., Olguin-Palacios, E. in Nucleic Acids in Immuno-
logy (edited by O. J. Plescia and W. Braun); p. 96, New York,1968.
20. Schur, P. H., Monroe, M. Proc. natn. Acad. Sci. U.S.A. 1969, 63,1108.
21. Talal, N., Steinberg, A. D., Daley, G. G. J. clin. Invest. 1971, 50,1248.
22. Epstein, W. V., Tan, M., Easterbrook, M. New Engl. J. Med.
1971, 285, 1502.23. Koffler, D., Carr, R., Agnello, V., Thoburn, R., Kunkel, H. G.
J. exp. Med. 1971, 134, 294.
24. Stollar, D., Levine, L. Archs Biochem. Biophys. 1963, 101, 417.
25. Stollar, D., Levine, L., Lehrer, H. I., Van Vunakis, H. Proc. natn.
Acad. Sci. U.S.A. 1962, 48, 874.26. Arana, R., Seligmann, M. J. clin. Invest. 1967, 46, 1867.
27. Erickson, E., Braun, W., Plescia, O. J., Kwiatokowski, Z. in Nucleic
Acids in Immunology (edited by O. J. Plescia and W. Braun);p. 201. New York, 1968.
28. Tanenbaum, S. W., Karol, M. H. ibid. p. 222.29. Leroy, E. C. J. clin. Invest. 1974, 54, 880.
DIOGENES SYNDROME*
A CLINICAL STUDY OF GROSS NEGLECT
IN OLD AGE
A. N. G. CLARK G. D. MANKIKAR
IAN GRAY
Department of Geriatric Medicine, Brighton General
Hospital, Brighton BN2 3EW
A study of elderly patients (fourteenSummary
men, sixteen women) who were ad-
mitted to hospital with acute illness and extreme self-
neglect revealed common features which might be
called Diogenes syndrome. All had dirty, untidyhomes and a filthy personal appearance about which
they showed no shame. Hoarding of rubbish (syllo-gomania) was sometimes seen. All except two lived
alone, but poverty and poor housing standards were
not a serious problem. All were known to the social-
services departments and a third had persistentlyrefused offers of help. An acute presentation with
falls or collapse was common, and several physicaldiagnoses could be made. Multiple deficiency states
were found—including iron, folate, vitamin B12, vita-
min C, calcium and vitamin D, serum proteins and
albumin, water, and potassium. The mortality,especially for women, was high (46%); most of the
survivors responded well and were discharged. Half
showed no evidence of psychiatric disorder and
possessed higher than average intelligence. Manyhad led successful professional and business lives,with good family backgrounds and upbringing. Per-
sonality characteristics showed them to tend to be
aloof, suspicious, emotionally labile, aggressive,group-dependent, and reality-distorting individuals.
It is suggested that this syndrome may be a reaction
late in life to stress in a certain type of personality.
Introduction
THE acutely ill old person with a dirty and neg-
lected appearance, in a setting of gross domestic dis-
* DIOGENES (4th century B.C.). Greek philosopher, the first of
the cynics. Supplied his needs in food and clothing, which
he kept to the minimum, by begging.... His ideals were
" life according to nature ","
self-sufficiency "," freedom
from emotion ", " lack of shame ","
outspokenness ", and
" contempt for social organisation ".1
order and squalor, is not uncommon, yet has attracted
little study.2,3 Such people pose serious problems in
terms of community care and sometimes need urgent
hospital admission. We describe here the back-
ground, presentation, psychiatric factors, and out-
come in thirty such cases and investigate the sugges-
tionthat this social and clinical picture might repre-
sent a syndrome.
Patients and Methods
Thirty patients (foutteen male, sixteen female) aged66-92 (average 79) were seen. All lived in a desperatestate of domestic disorder, squalor, and self-neglect, and
they were referred for urgent admission to the geriatricunit between October, 1972, and July, 1973. The social
and environmental background was examined in every
case, together with conventional medical examination and
investigations on admission. Comprehensive intelligenceand psychometric testing were assessed by the intellectual
rating scale (I.R.S.), intelligence quotient by Wechsler
adult intelligence scale,4 and by Cattell’s methodfor
personality.
Results
Social and Environmental Factors
All patients lived in a state of domestic squalor, dis-
order, and extreme self-neglect. Their homes were
filthy on the outside-peeling paintwork and dirty,often broken, windows with dingy net curtains serv-
ing as external markers to conditions within. Inside
there was a characteristic strong, stale, and slightlysuffocating smell. The patients were usually dressed
in’layers of dirty clothing sometimes covered by an
old raincoat or overcoat, and, when confined to bed,
they lay beneath a pile of ragged blankets, clothing,or newspapers. They never appeared to undress or
wash, the hair being long and unkempt, with exposedsurfaces of skin deeply engrained with dirt. Onlytwo patients apologised about their personal or domes-
tic state. Several hoarded useless rubbish (syllogo-mania)-newspapers, tins, bottles, and rags, often in
bundles and stacks-and in six instances the size of
the collection seriously reduced living space.
Family and Home Support
Twenty-eight lived alone-one man lived with a
son and grandson, and one lived with his unmarried
daughter; seventeen had relatives (eight in the Brigh-
ton area) while thirteen had none. Every patient hadbeen known to the community authorities for several
weeks to years, and the domestic predicament was
well recognised. Twelve had home services (home
help, nursing, and meals) while ten repeatedly de-
clined offers of help, sometimes refusing to open the
door to callers.
Nutrition
Little food was to be found in the house, and old
dishes and mouldy scraps were often seen. Tea,bread, biscuits, cakes, and tinned food seemed to be
the staple diet.
FinanceAll the patients received the old-age pension and
six had supplementary pension; two had savings of
E2600 and E5000, and seven owned their homes. No-
one complained of shortage of money, and poverty
8/8/2019 Diogenes Lancet 1975
http://slidepdf.com/reader/full/diogenes-lancet-1975 2/5
367
did not seem to be a feature. Food and clothing were
sometimes accepted from sympathetic neighbours.
ProfessionsThree men had held Service commissions; two had
been journalists; one had been a dentist, and one a
professional violinist. Three women had been school-
teachers, one a West-End fashion designer, one a
music teacher, one an opera singer (Covent Garden),and one a teacher of needlework. Their careers
seemed to have been successful and they had enjoyedsound family backgrounds, education, and social
standing in earlier life.
Admission and Presentation
Two were compulsorily admitted (under Section 47
of the Mental Health Act), the rest voluntarily; eighthad previously refused until the point where illness
became critical. A fall or collapse (seventeen) was the
most common presentation.
DiagnosisAll were acutely ill, and the principal diagnoses
were congestive heart-failure (eight), cerebrovascular
disease (seven), bronchopneumonia (four), malignantdisease (two), Parkinson’s disease (two), osteoarthritis
(two), and leukaemia, gangrene, cervical spondylosis,pulmonary embolism, and renal failure were present
in single cases.
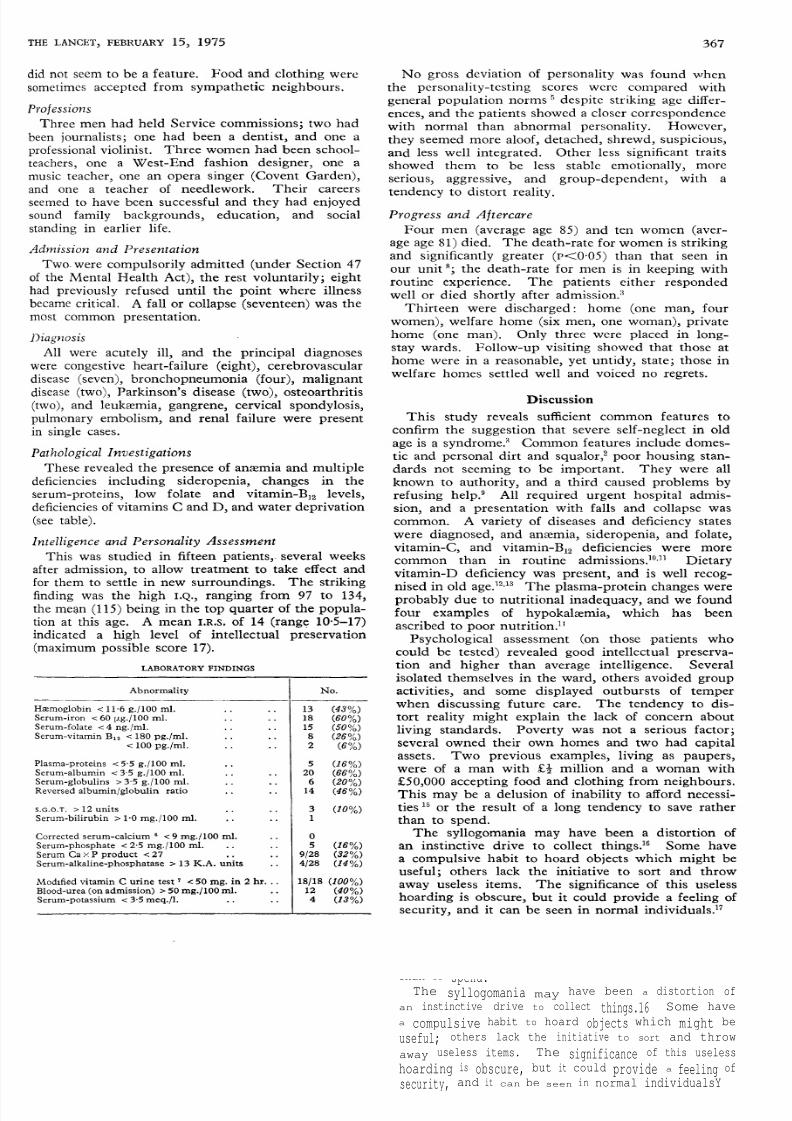
Pathological InvestigationsThese revealed the presence of anaemia and multiple
deficiencies including sideropenia, changes in the
serum-proteins, low folate and vitamin-B]2 levels,deficiencies of vitamins C and D, and water deprivation(see table).
Intelligence and Personality Assessment
This was studied in fifteen patients,- several weeks
after admission, to allow treatment to take effect and
for them to settle in new surroundings. The strikingfinding was the high l.Q., ranging from 97 to 134,the mean (115) being in the top quarter of the popula-tion at this age. A mean I.R.S. of 14 (range 10-5-17)indicated a high level of intellectual preservation(maximum possible score 17).
LABORATORY FINDINGS
No gross deviation of personality was found when
the personality-testing scores were compared with
general population norms ’despite striking age differ-
ences, and the patients showed a closer correspondencewith normal than abnormal personality. However,
they seemed more aloof, detached, shrewd, suspicious,and less well integrated. Other less significant traits
showed them to be less stable emotionally, more
serious, aggressive, and group-dependent, with a
tendency to distort reality.
Progress and AftercareFour men (average age 85) and ten women (aver-
age age 81) died. The death-rate for women is strikingand significantly greater (P<0-05) than that seen in
our unit 8; the death-rate for men is in keeping with
routine experience. The patients either respondedwell or died shortly after admission.’
Thirteen were discharged: home (one man, four
women), welfare home (six men, one woman), privatehome (one man). Only three were placed in long-stay wards. Follow-up visiting showed that those at
home were in a reasonable, yet untidy, state; those in
welfare homes settled well and voiced no regrets.
Discussion
This study reveals sufficient common features to
confirm the suggestion that severe self-neglect in old
age is a syndrome.’ Common features include domes-
tic and personal dirt and squalor,2 poor housing stan-
dards not seeming to be important. They were all
known to authority, and a third caused problems by
refusing help.9 All required urgent hospital admis-
sion, and a presentation with falls and collapse was
common. A variety of diseases and deficiency states
were diagnosed, and anxmia, sideropenia, and folate,vitamin-C, and vitamin-Bl2 deficiencies were more
common than in routine admissions.’°°" Dietaryvitamin-D deficiency was present, and is well recog-
nised in old age.12,13 The plasma-protein changes were
probably due to nutritional inadequacy, and we found
four examples of hypokalxmia, which has been
ascribed to poor nutrition."
Psychological assessment (on those patients who
could be tested) revealed good intellectual preserva-
tion and higher than average intelligence. Several
isolated themselves in the ward, others avoided group
activities, and some displayed outbursts of temperwhen discussing future care. The tendency to dis-
tort reality might explain the lack of concern about
living standards. Poverty was not a serious factor;several owned their own homes and two had capitalassets. Two previous examples, living as paupers,
were of a man with E’2 million and a woman with
30,000 accepting food and clothing from neighbours.This may be a delusion of inability to afford necessi-
ties 15 or the result of a long tendency to save rather
than to
spend.The syllogomania may have been a distortion of
an instinctive drive to collect things.16 Some have
a compulsive habit to hoard objects which might be
useful; others lack the initiative to sort and throw
away useless items. The significance of this useless
hoarding is obscure, but it could provide a feeling of
security, and it can be seen in normal individualsY

8/8/2019 Diogenes Lancet 1975
http://slidepdf.com/reader/full/diogenes-lancet-1975 3/5
368
There are two possible explanations why intelligenteducated individuals descend to such .debased stan-
dards of living. One might be a lifelong proclivityto give personal and domestic care a low priority-a disorganised style of life becoming exaggerated byageing and physical infirmity-or it might be a
reaction to stress in an elderly person with certain
personality characteristics. Sometimes previouslystable old people develop neurotic breakdown with-
out previous history,17 due to social, economic, and
declining health factors with predisposing features
in the personality (e.g., being aloof, moody, and
anxious). A vicious circle of increasing anxiety, help-lessness, and anger is accentuated by inadequacy to
master everyday problems, producing a further ineffici-
ency.18 Social, psychological, and economic stress
produce mental illness in old age 19 and invoke defence
mechanisms of withdrawal and denial of need." Our
patients seem to need social contact which earlier may
have been found within their profession and family.
Enforced isolation by bereavement,3 with loss of sup-port, or retirement could result in reactive rejectionof contemporary standards and social contacts.
What can be done to help these people? If accep-
ted, a home help is often unable to make any impres-sion on the dirt and untidiness and finds the work
distasteful. On the other hand, compulsory removal
to a welfare home or to hospital should never be
applied merely to ensure cleanliness and conformity.Community-service agencies have no right to enter
a home without consent, and if, after offers of care
have been refused, a sane person suffers or dies alone,then no criminal negligence is involved.21 Society
may protestat
the standards of these people and neigh-bours may complain, but compulsory powers are rarelyused and care by consent should be the principle in
management. If they recover, their freedom to decide
their future should be respected.
We thank Dr N. I. Condon, Dr W. S. Parker, and Dr J. A.
Whitehead, and the health visitors and social workers for their
interest and help in this study. Prof. J. F. Scott gave statisti-
cal advice.
Requests for reprints should be addressed to A. N. G. C.
REFERENCES
1. Chambers Encyclopædia; vol. IV, p. 533. Oxford, 1966.
2. Stevens, R. S. Br. J. geriat. Pract. 1963, 2, 88.
3. MacMillan, D., Shaw, P. Br. med. J. 1966, ii, 1032.
4. Britton, P. G., Savage, R. D. Br. J. Psychiat. 1966, 112, 417.
5. Cattell, R. B., Stice, G. F. Handbook of the Sixteen PersonalityFactor Questionnaire; and handbook supplement for form C.
Institute for Personality and Ability Testing, Illinois, 1957.
6. Payne, R. B., Little, A. J., Williams, R. B., Milner, J. T. Br. med. J.1973, iv, 643.
7. Harris, L. J., Abbasy, M. A. Lancet, 1937, ii, 1429.
8. Clark, A. N. G. Publ. Hlth, Lond. 1973, 88, 11.
9. Rudd, T. N. Br. J. clin. Pract. 1960, 14, 345.
10. Powell, D. E. R., Thomas, J. H., Mills, P. Geront. clin. 1968, 10,21.
11. Hurdle, A. D. F., Picton Williams, T. C. Br. med. J. 1966, ii, 202.
12. Anderson, I., Campbell, A. E., Dunn, A. Scott. med. J. 1966, 11, 429.13. Chalmers, J. Jl R. Coll. Surg. Edinb. 1968, 13, 225.
14. Judge, T. G. Geront. clin. 1968, 10, 102.
15. Beatson, A. W. Br. med. J. 1960, ii, 468.
16. James, W. Principles of Psychology. London, 1901.
17.Slater, E., Rother,
M.Clinical Psychiatry; p. 117. London, 1969.18. Freedman, A. M., Kaplan, M. D. Comprehensive Textbook of
Psychiatry. Baltimore, 1967.
19. Padmore, F. B. in Mental Illness in Later Life (edited by E. Pfeiffer
and E. W. Busse); p. 46. American Psychiatric Association, 1973.
20. Pfeiffer, E., Busse, E. W. (editors). Mental Illness in Later Life;p. 110. American Psychiatric Association, 1973.
21. Kinsey, E. W. Times, Jan. 9, 1973.
Preliminary Communication
ABNORMAL ORGANIC ACIDURIAS IN
MENTALLY RETARDED PATIENTS
R. W. E. WATTS R. A. CHALMERS
Division of Inherited Metabolic Diseases,Medical Research Council Clinical Research Centre,
Harrow, Middlesex HA1 3UJ
A. M. LAWSON
Division of Clinical Chemistry, M.R.C. Clinical
Research Centre
SummaryUrine specimens from 1778 mentallyretarded patients and 420 age and sex
matched non-retarded controls selected from a general
practice have been analysed for non-amino organicacids by a quantitative extraction and gas chromato-
graphic method. The compounds were identified by
combined gas chromatography and mass spectro-metry. Approximately 5% of the patients had an
abnormal organic aciduria. The frequency of abnor-
malities was slightly higher (about 7%) in a group
of 248 severely subnormal children, but not in cases
with a family history of mental retardation, retarded
sibs, or whose parents were consanguineous. The
most frequently observed abnormalities were phenyl-alanine metabolites in cases of phenylketonuria (about1%), increased excretion of benzoic acid (about 1%),and increased excretion of 2-oxoglutaric acid with or
without raised urinary citric-acid levels (about 1%).The biochemical and clinical significance of these
findings is being further investigated.INTRODUCTION
ABOUT 3 % of the general population are mentallyretarded, with i.Q. values below 70, and in about
0-4% of the population the i.Q. is less than 50 when
measured at the age of seven years.1,2 If the mental
retardation can be shown to be linked with a specificbiochemical abnormality, it may be possible to improvethe situation by specific treatment or by developingmethods of prenatal diagnosis upon which to base
appropriate genetic counselling, with the option of
aborting an affected fetus.
Many inherited metabolic diseases that manifest asan organic aciduria include mental retardation among
their symptoms. Previous work has concentrated on
aminoacidopathies and certain other disorders for
which relatively simple screening methods are avail-
able. Although isolated examples of organic acid-
urias associated with mental retardation are known,3there are no previous reports of comprehensive meta-
bolic screening for abnormal non-amino organicacidurias. New quantitative methods H have now
enabled this to be undertaken, and we describe here
a study of the incidence of metabolic disorders associ-
ated with an organic aciduria in mentally defective
adults and children.
The analytical methods used permit the quantitativeanalysis of one approximately 5 ml. urine sample(equivalent to 3 mg. creatinine) for any acidic com-
pound with a pKa value less than about 5-5. Prior
knowledge of the likely acidic metabolites is not
8/8/2019 Diogenes Lancet 1975
http://slidepdf.com/reader/full/diogenes-lancet-1975 4/5
515
Letters to the Editor
RECOGNITION OF DIPHTHERIA
SiR,—We read with interest the report of diphtheriain the Manchester area by Dr Butterworth and colleagues(Dec. 28, p. 1558). They clearly imply that there is a
need to investigate routinely every case of sore throat for
the presence of diphtheria bacilli. This is an assertionwith which we cannot agree. On the contrary, we believe
that routine examination for Corynebacterium diphtheria, at
present, is wasteful and may be counter-productive. In
support of this view we would quote from Sir JamesHowie’s summing-up of a symposium on diphtheria 1:
" Obviously the disease has now reached such clinical
levels that to look for diphtheria in all throat swabs routinelyas we did in the 1930s would not be practical politics-thecost would scarcely be justified. We really must beg our
clinical colleagues to raise their index of suspicion and
make a clear approach to us, either a personal approach or
a definite note on the request form ’diphtheria suspected’and that ought to put the staff of any reasonable laboratoryon its toes."
During 1973, the isolation of 5 toxigenic and 45 non-
toxigenic strains of C. diphtheriae was reported to the
Communicable Disease Report of the Public Health
Laboratory Service. The figures for 1974 (still provisional)were 3 and 73 respectively (Mrs E. Vernon, personalcommunication). A routine test for an organism with
such a low prevalence may breed carelessness and inatten-
tion in the use of that test.
When a strain of C. diphtherice is isolated from a patientwithout clinical features of diphtheria, its significancemust be carefully assessed. It is not unknown for wards
to be closed and the management of sick patients seriouslydisrupted before evidence of the toxigenic status of an
organism isolated from a"
routine"
specimen has been
determined, even though it is most likely that such a strainwill be non-toxigenic.We make these observations because we believe that the
detection of diphtheria at an early stage will best be
achieved by urging clinicians to voice their suspicions to the
laboratory, and also to alert practitioners to the fact that not
all laboratories routinely examine specimens forC. diphtheria.We are indebted to Prof. M. G. McEntegart for the proceed-
ings of the symposium on diphtheria.Public Health Laboratory and
Department of Microbiology,Central Middlesex Hospital,
Park Royal, LondonNW107NS.
D. A. MCSWIGGAN
C. E. D. TAYLOR.
DIOGENES SYNDROMESIR,—The article by Dr Clark and his colleagues (Feb.
15, p. 366) is important in so far as it draws attention to a
characteristic picture by no means rare in clinical prac-
tice, but which as far as I know has never been clearlydescribed before. I should, however, like to point out that
this syndrome is not restricted to the elderly. Frommy own
unpublished observations on a series of recluses a similar
picture is found in much younger persons and betokens a
variety of psychiatric anomalies, including certain person-
ality disorders, frank psychosis, or dementia, and these need
not necessarily be associated with physical handicap. It is a
pity that Dr Clark and his colleagues did not include a
psychiatric evaluation of their patients. We have not yetreached the stage when psychometric testing can replaceclinical examination by a psychiatrist.
Oldham and District Hospital,Rochdale Road, Oldham OL1 2JH. N. BERLYNE.
1. Unpublished Proceedings of Symposium on Diphtheria, Sheffield,1970.
SIR,-It is likely that the name Diogenes syndromewill become common currency, and it is refreshing to read
for the first time a study of this by no means rare condition.
The authors are undoubtedly right in urging that insistence
on conventional standards of cleanliness and behaviour
never justifies the compulsory removal of a person from
his or her home. There is, however, an important omission
in the article-namely, fire risk. The combination of a frail,
unsupported old person and masses of hoarded rubbish
often adds up to a danger of fire, not only to the person
concerned but to neighbours as well, if there are other
houses nearby. In my experience, it is this that causes the
most worry when trying to deal with these difficult old
people.Warwickshire Area Health Authority,Rugby District, 17 Warwick Street,
Rugby, Warwicks. J. TWOMEY.
SiR,—That some independently minded old peopleresist the pressure of society to conform (Feb. 15, p. 366)should be a source of satisfaction to those who care for the
freedom of the human spirit. One wonders whether self-
neglect in such cases is not a manifestation of the death-wish, as in some cases of hypothermia. If so are we neces-
sarily justified in interference as long as the person’s habits
and behaviour are not a nuisance to others ?
Perhaps the existence of such cases supports the con-
tention that theoption ofan arranged voluntary dying shouldbe available to the elderly in a civilised society. It should
not be left to the individual to have to take steps himself
either by forcible or more protracted means to terminate
his existence.
To rescue such persons from their self-imposed exile
from society presupposes that our ideas of conventional
behaviour are correct. Whether we are ever justified in
doing so is debatable. The application of pressure in such
cases is all too frequent and is excused by a devotion to the
theory of " the sanctity of life " which overrides respectfor individual self-determination.
Portland House,Lindley,
Huddersfield. S. L. HENDERSON SMITH.
GASTRIC ACID AND DUODENOGASTRIC
REFLUX
SiR,-Dr Kallner (Feb. 8, p. 338) rightly emphasises the
importance of duodenogastric reflux, which, as he states,
is often overlooked. This error, although of greatest
importance during the basal period, will also distort
results during stimulated secretlon.1
The effect of reflux on hydrogen-ion concentration is
even more striking than the effect on basal acid output,since not only neutralisation but also dilution is involved.
This undoubtedly accounts for the large spontaneousvariations in basal hydrogen-ion concentration2 and is a
major factor in the difficulties of interpretation of the
insulin test. It is for this reason that we have ignoredbasal collections in our investigations of postvagotomyinsulin status,3 and our criteria have allowed us to give the
insulin test predictive accuracy in the individual cast for
the first time.4,6
1. Faber, R. G., Russell, R. C. G., Royston, C. M. S., Whitfield, P.,
Hobsley, M. Gut, 1974, 15, 880.
2. Gillespie, G., Elder, J. B., Smith, J. S., Kennedy, F., Gillespie,
I. R., Kay, A. W., Campbell, E. H. G. Gastroenterology, 1972, 62,903.
3. Faber, R. G., Parkin, J. V., Russell, R. C. G., Whitfield, P.,
Hobsley, M. Br. J. Surg. 1974, 61, 911.
4. Weinstein, V. A., Hollander, F. Gastroenterology, 1950, 14, 586.
5. Faber, R. G., Russell, R. C. G., Parkin, J. V., Whitfield, P.,
Hobsley, M. Gut (in the press).
8/8/2019 Diogenes Lancet 1975
http://slidepdf.com/reader/full/diogenes-lancet-1975 5/5
750
However, the cells display a growth pattern characteristic
of cultured human B lymphoid cells: they grow in largeclumps. The cultured lymphoid cells have extremely longsurface projections and produce mature virions of a herpes-type virus, probably those of the Epstein-Barr virus (seeaccompanying figure). It is known that this virus selectivelytransforms only B but not T human llmphocytes.10 Thus,the cells obtained in permanent culture from the spleenof a patient with L.R.E. appear and behave like B lympho-cytes but display unusually long surface villi.
University of Texas SystemCancer Center,
M. D. Anderson Hospital,Houston, Texas 77025, U.S.A.
Veterans Administration Hospitaland Baylor College of Medicine,Houston, Texas 77025, U.S.A.
JOSEPH G. SINKOVICS
CHIU-HWA WANG.
FERENC GYÖRKEY.
THE CONSULTANTS’ CONTRACT
SiR,—The proposals put forward by the Secretary of
State on Dec. 2011 seem on the surface to be good for the
N.H. S. However, even if consultants were able to give moretime to the N.H.S. as a result of this reshaped contract,
there is not money available to provide the operatingsuites and outpatient consulting-rooms necessary.
The situation is, however, more serious than this because
by the Secretary of State’s proposals the scene would be set
for changes of pattern of consultant activity that would
worsen both the short and long term manpower situation
so far as service and postgraduate education is concerned.
How could the profession’s negotiators have accepted this
at a time when there is insufficient money to maintain even
the agreed 4% annual increase in consultant establishment
and when, because of the continued effect of the Willink
recommendation, the hospital service is more dependenton overseas doctors than at any time in its history ? Theprinciples behind the Secretary of State’s proposalsremain and it is for this reason that impasse has been
reached.
Editorial pens move people. Perhaps yours can be
instrumental in urging the Government and professionto jointly seek a judicial definition of what the consultant
contract really means.
Hellingly Hospital,Hailsham,
Sussex BN27 4ER.
RONALD MAGGS,Whole-time consultant.
SiR,-In view of the escalating and irresponsible sanctions
by some N.H.S. consultants, I call upon my fellow retired
consultants to report for unpaid part-time duty, either at
their former place of work or at the nearest hospital that
needs them. In this way we may hope to salvage what is
left of our reputation at home and abroad and to break the
stranglehold that threatens our patients.llA Acol Road,
London NW6 3AA. L. S. MICHAELIS.
SIR,-It is with interest that we read Mr Robinson’s
letter (March 15, p. 626). Do you, Sir, regard The Lancet
as"
essentially a consultants’ journal "?
Medical Students’ Residence,Alder Hey Hospital,
West Derby,Liverpool 12.
M. G. BAMBER
H. R. L. BISHOP-CORNET
A. F. MANLEY
SUSAN M. MURRAY
M. WARMINGER.
** *No: we do not look upon this journal as being"
essentially " for (or against, for that matter !) any parti-cular group of readers.-ED. L.
10. Pattengale, P. K., Smith, R. W., Gerber, P. Lancet, 1973, ii, 93.
11. See Lancet, Jan. 11, 1975, p. 92.
DIOGENES SYNDROME
SIR,-I should like to agree with some of the pointsmade in this correspondence (March 1, p. 515, March 15,
p. 627). Fire hazards to the patient and to neighbourscan be very real, and can often ultimately tip the scales
towards compulsory removal. One must also add the
danger of gassing and explosions if the house has gas
appliances.I cannot, however, agree that one must always respectthe wish of the individual to neglect himself even unto
death. I have seen some patients who did not do well in a
geriatric unit or eventide home, but I have also seen manytake on a new and happy life after admission to such units,particularly if the units are stimulating and well run.
In Scotland, such cases are rarely handled by compulsoryadmission powers under the Mental Health (Scotland)Act 1960. More appropriate (and .effective) is Section 47
of the National Assistance Act 1948 (" unable to devote to
themselves proper care and attention, and not receiving it
from others... " &c.) or the National Assistance (Amend-ment) Act 1951.
Non-conformity in itself is never a sure sign of psychiatricdisorder and whether or not one invokes compulsory powers
may well depend on as accurate a psychiatric assessment
as possible. Personality inventories and psychometricassessments, I fear, have no place in helping the clinician
to make up his mind in the patient’s home. Repeatedvisits are nearly always necessary before an accurate
assessment can be made.
The decision on the correct course of action will alwaysbe difficult, but I feel that if the physician approaches each
case with an open mind and weighs all the clinical, social,and domestic factors carefully, he will usually take the
action which is in the patient’s best interests.
Department of Community
Medicine,Ruchill Hospital,
Glasgow G20 9NB. H. MACANESPIE.
LEVAMISOLE
SIR,—Your editorial (Jan. 18, p. 151) calls for controlled
clinical trials of levamisole, and at least two centres are
already using it in the treatment of human malignancies.I,2We wish to support the caution sounded by Dr Hopper and
others,3 regarding the experimental evidence for tumour
inhibition by levamisole.
In our experience with levamisole (L-tetramisole), and
with the racemic mixture (D-L-tetramisole) to which greater
activityhas been
attributed,4the
drug didnot stimulate
humoral or cellular immune responsiveness. We found no
evidence of altered humoral antibody response to sheeperythrocytes injected in groups of mice receiving 1-25 mg.
per kg. body-weight intraperitoneally of levamisole over
various time schedules.- We did not observe either immuno-
suppression associated with drug therapy before antigenchallenge, or immunostimulation associated with drugadministration with or soon after antigen challenge, as
reported by others.4 Similarly, we found no evidence of
accelerated rejection of tail skin grafts in mice treated bysimilar schedules, which also failed to inhibit growth of a
transplanted fat tumour. In this last experiment, rats
immunised with irradiated Walker 256 tumour cells or
inoculatedwith
viable tumour received thedrug (2-5 mg.
per kg. body-weight) intraperitoneally. In-vitro assays
showed no increase in serum-antibody potency or spleen-cell cytotoxicity at different times following tumour
1. Webster, D. J. T., Hughes, L. E. Lancet, Feb. 15, 1975, p. 389.2. Amery, W. ibid.
3. Hopper, D. G., Pimm, M. V., Baldwin, R. W. ibid. March 8, 1975,
p. 574.4. Renoux, G., Renoux, M. J. Immun. 1974, 113, 779.




























