Embed Size (px)
Citation preview

Differential Diagnosis of Differential Diagnosis of EdemaEdemaJillian Caster PT DPT WCC CLTChatham University Grand Rounds11/10/16

ObjectivesObjectivesAt the conclusion of this course
you will be able to ◦Effectively evaluate and diagnose
causes of edema◦Rule out/in red flag causes of edema
and appropriately refer◦Effectively treat edema

EdemaEdemaWhat is edema?
◦Definition: Edema is a palpable swelling produced by expansion of the interstitial fluid volume

PathophysiologyPathophysiologyOver filtrationIncreased
capillary hydraulic pressure
Reduced capillary oncotic pressure
Increased capillary permeability
Reduced drainageVenous
insufficiencyLymphatic
insufficiencyIncreased
interstitial oncotic pressure

CausesCauses• Systemic– Allergic reaction– Cardiac disease– Hepatic disease– Malnutrition – Sleep Apnea– Pregnancy/
premenstrual– Renal disease– Pulmonary
hypertension– Idiopathic edema– Medication
• Localized– Acute injury– Cellulitis– Chronic Venous
Insufficiency– Compartment
Syndrome– Complex Regional
Pain Syndrome– DVT & Post
Thrombotic Syndrome
– Lipedema– Lymphedema– May Thurner

EvaluationEvaluation• History • Medication• Onset• Unilateral or
bilateral• Positional changes
in edema• Coloring and skin
texture• Pitting or non-pitting• History of wounds• Stemmer sign• Weight
PainTemperatureStrength and mobilityJugular vein
distentionSOBIrregular heart
rhythmLung cracklesWells RuleBlood Work

Red FlagsRed Flags• Red Flags– SOB and coughing– Tachypnea, tachycardia– Irregular heat beat– Ascites– Periorbital edema– Abnormal Labs– Acute onset– Redness– Warmth– Pain– Fever– + Wells

Red FlagsRed FlagsNumbness and tinglingPulslessnessAcute injuryProximal swelling distribution

Wells RuleWells Rule

StemmerStemmer’’ssPositive Negative

Pitting Edema ScalePitting Edema Scale
Grade Definition1+ 2mm or less
disappears immediately
2+ 2-4 mmfew second rebound
3+ 4-6 mm10-12 second rebound
4+ 6-8 mm> 20 second rebound

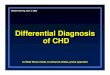
Case 1Case 165 year old male
with bilateral LE edema present for 10 years; former smoker; retired bus driver
PMH: obesity, retinopathy, CHF, CAD, HTN, hyperlipidemia, aortic valve disease and replacement, CABG, sleep apnea, CKD, CVA, DM type 2, skin CA

Case 1Case 1

Case 1 HistoryCase 1 History• Bilateral• Chronic• 3+ Pitting edema• Obesity • Cardiac disease• Sleep apnea • CKD• CVA• Medication

Evaluation & Special TestsEvaluation & Special TestsReduction with elevationBrawny, hemosiderin stainingHistory of wounds
◦ Large amount of exudate-Stemmer’sDull achinessVitals WNLAmbulates community distances with
minimal difficulty use of RWWell nourished4/5 strength in L LE DF/PF, Quads, Hams,
hip flexors otherwise LE MMT= WFL

What can we rule out?What can we rule out?LymphedemaLipedemaDependent edema

DiagnosisDiagnosisCVI
◦ Low viscosity/ protein poor
◦ Pitting edema◦ Chronic◦ Bilateral ◦ Achy/ heaviness◦ Volume reduction
overnight ◦ Possible
varicosities
◦ Hemosiderin staining
◦ Inverted champagne bottle
◦ Ulcerations◦ - Stemmer’s
CKDCardiac

TreatmentTreatmentWound care: absorbent dressingsABIVascular TestingShort stretch multilayer
compression bandagesCompression garments: 30-
40mmHgLE elevationTherapeutic exercise

ABIABIHighest systolic ankle / Highest
systolic Brachial1.0 < Normal0.8-0.99 Abnormal0.5-0.8 Compromised< 0.5 Severe PAD- Do not compress!

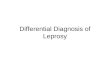
Case 2Case 266 y.o. Female
with 30 year history of bilateral LE edema; works as CNA
PMH: obesity, cataract repair, hyperlipidemia, HTN, CKD II, bilateral knee arthritis, DM type 2, hypothyroidism

Case 2Case 2

Case 2 HistoryCase 2 History• Bilateral • Chronic• 2+ Pitting edema• Obesity• Cardiac disease• CDK Stage II• Bilateral knee arthritis• Hypothyroidism

Evaluation & Special TestsEvaluation & Special TestsEdema is stable with positional
changesNo wounds+ Stemmer’s10# weight gainNo painNormal Temp and skin coloringAreas of fibrosis and papillomasBil LE strength WNLAmbulates unlimited distances no ADVitals WNL

What can we rule out?What can we rule out?Venous insufficiencyLipedemaDependent edemaMedicationMalnutrition

DiagnosisDiagnosisLymphedema
◦ Protein rich swelling◦ Chronic◦ Painless◦ Unilateral or
Bilateral◦ Stage I – Stage II
Pitting◦ Stage II – III non
pitting◦ Fibrosis
◦ Hyperkeratotic skin
◦ Squared of toes◦ + Stemmers
CKD

Squared off toes Fibrosis & Hyperkeratosis

LymphedemaLymphedemaPrimary
◦ Milroy’s Birth-2 years
◦ Meigs 2-35 years
◦ Lymphedema Tarda 35+
Secondary◦ Tumor◦ Surgery◦ Radiation◦ Infection◦ Filariasis◦ Venous
Insufficiency Bilateral Phlebolymphostatic
edema

TreatmentTreatmentABICDT
◦MLD◦Short stretch compression bandages
Therapeutic exerciseFlat knit custom compression
garments

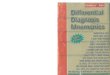
Case 3Case 382 y.o. female; 3
month history of bilateral LE swelling; retired secretary; former smoker; limited ambulation
PMH: HTN, CAD, CHF, A-fib, GERD, bowel obstruction, CKD, gout, bipolar disorder, hysterectomy, thyroidectomy

Case 3Case 3

Case 3 HistoryCase 3 HistoryBilateralChronic4+ Pitting edema
◦CHF, A-fib, HTN, CAD◦CKD◦Medication◦Malnutrition◦Dependent edema◦Gout◦Hysterectomy

Evaluation & Special TestsEvaluation & Special Tests Increased edema in dependent positionNormal skin color and tempNo Hx of non healing wounds- Stemmers 10# weight loss in 1 monthNo pain associated with edemaMin A for sit <> stand; ambulates with RW
household distances and uses W/C long distances
Bilateral LE weakness Jugular vein distention Irregular hear rhythmSOB

What can we rule out?What can we rule out?CVILymphedemaLipedemia

DiagnosisDiagnosisCHF
◦Chronic◦Bilateral ◦Pitting◦Jugular vein distention◦Gallop rhythm◦C/O dyspnea
CKDDependentMalnutrition

TreatmentTreatmentRefer to cardiologist/kidney
specialistNutrition consultLight compression garments
once medically managedEducation on elevating LEs

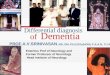
Case 4Case 443 y.o. female
with negative history of LE edema; woke up on 2 days ago with a red, swollen LE; typical, active life style, works as an elementary school teacher
PMH: HTN, LBP

Case 4Case 4

Case 4 HistoryCase 4 HistoryUnilateral edema Acute symptoms3+ Pitting

Evaluation & Special TestsEvaluation & Special TestsNo change in edema with elevationRedness with irregular borders, warmth7/10 pain in R LENo woundsOnchomychosis-Stemmer’s signTemp: 99.1, BP: 137/88, HR: 92, SpO2:
98%Strength and mobility WNL- Well’s

What can we rule out?What can we rule out?LymphedemaLipedemaCVICardiacKidneyLiverDVTBaker’s Cyst
CRPSCompartment
SyndromeMay ThurnerMalnutritionDependentIdiopathic

CellulitisCellulitisUnilateral Acute onsetPainfulRedWarmthSystemic
symptoms◦ Fever◦ malaise◦ achiness
PittingWoundsOnychomycosis

CellulitisCellulitisAntibioticsRefer Pt to ERMultilayer short stretch
compression

Everything else to keep in Everything else to keep in mindmindLipedema
◦Chronic, bilateral, pitting◦Abnormal fat distribution from ankles
to hips◦Treat with CDT and flat knit garments
DVT◦Acute, unilateral, pitting◦Painful with palpation, redness,
warmth, + Wells◦Refer to ER

Everything else to keep in Everything else to keep in mindmindCRPS
◦Chronic, unilateral, pitting◦Sweating, pallor, irregular hair growth◦Hx of traumatic injury◦Therapeutic exercise, refer for medical
managementRuptured Baker’s Cyst
◦Acute, unilateral, pitting◦Redness, warmth, trickling feeling◦Hx of knee complications◦Rest, elevation, compression

Everything else to keep in Everything else to keep in mindmindPulmonary Hypertension
◦Chronic, bilateral, pitting◦History of sleep apnea◦Refer to cardiologist
Idiopathic edema◦Chronic, bilateral, pitting◦Females <50, menstruating, weight gain
through day, c/o hand and face edema, obesity, depression
◦Refer- Spironolactone ◦Compression garments if tolerated

Everything else to keep in Everything else to keep in mindmindDependent edema
◦Chronic, unilateral or bilateral, pitting◦Paralysis, reduced strength, dependent
position◦Hx of CVA, MS etc◦Short stretch compression, compression
garmentsMedication
◦Chronic, bilateral, pitting◦Occurs with use of medication◦Refer for change in medication or compression

MedicationMedicationClass Specific MedicationAntidepressants MAOIs, trazodoneAntihypertensives Beta blockers, Ca++ blockers,
clonidine, hydralazine, methyldopa, minoxidil
Antivirals ZoviraxChemotherapeutics Cyclophosphamide,
cyclosporine, cytosine arabinoside, mithramycin
Cytokines G-CSF, GM-CSF, interferon alfa, interluken-2 and 4
Hormones Androgen, corticosteroids, estrogen, progesterone, testosterone
NSAIDs Celebrex, ibuprofen

Everything else to keep in Everything else to keep in mindmindCompartment Syndrome
◦Acute, unilateral, pitting◦Pain, redness, paresthesia, pulse◦ER referral
May Thurner◦Chronic, unilateral, pitting◦Left iliac vein is compressed by the
right iliac artery◦Refer to vascular surgeon◦Compression following surgery

Everything else to keep in Everything else to keep in mindmindMalnutrition
◦ Chronic, bilateral, pitting◦ Interstitial oncotic pressure is higher than
capillary oncotic pressure drawing fluid out◦ Typically older individuals, refer for blood work,
nutrition consult◦ Compression
Kidney disease◦ Chronic, bilateral, pitting◦ Reduced protein levels in blood causing
interstitial oncotic pressure is higher than capillary oncotic pressure drawing fluid out
◦ Refer to nephrologist, conservative compression, garments

Everything else to keep in Everything else to keep in mindmindLiver disease
◦Chronic, bilateral, pitting◦Ascites, jaundice, spider hemangiomas◦Reduced protein circulating, portal vein
hypertension, refer for blood work and liver specialist
Post thrombotic syndrome◦Chronic, unilateral or bilateral, pitting◦History of DVT causing deep venous
insufficiency◦Blood clotting disorder◦Wound care, compression, refer for
vascular testing and vascular surgeon

ReferencesReferences Al-Niami, F. (2009) Cellulitis and Lymphedema: A Vicious Cycle. Journal of
Lymphedema 4(2): 38-42. Ely, JW. (2006) Approach to Leg Edema of Unclear Etiology. JABFM 19(2):
148-160. Sterns, RH. (2016) Clinical manifestations and diagnosis of edema in
adults. Available from UpToDate.com. Accessed on 10 October 2016. World Union of wound healing societies initiative (2012). Compression in
venous leg ulcers: A consensus document. Principles of Best Practice. Trayes, KP. (2013) Edema: Diagnosis and Management. Am Fam
Physician 88(2): 102-110. Norton, S. Norton School of Lymphatic Therapy Course Manual. Diagnosis
& Therapy. Norton School of Lymphatic Therapy 2013. Banu, A. (2007) Lymphoedema- Up to Now- Review. Mædica A Journal of
Clinical Medicine 2(1) 25-32. Hogan, M (2007) Medical-Surgical Nursing (2nd ed.). Salt Lake City:
Prentice Hall Zuther, J., Norton, S. Lymphedema Management: The Comprehensive
Guide for Practitioners. 3rd Ed. 2013. Theime, Stuttgart, Germany. Goodman, Fuller, Boissonnault. Pathology: Implications for the Physical
Therapist. 2nd Ed. 2003. Elsevier, USA. Caster, M (2016) Differential diagnosis & treatment considerations for the
lower extremity.