Embed Size (px)
Citation preview

Original Research
Dietary Magnesium Deficiency Induces Heart RhythmChanges, Impairs Glucose Tolerance, and DecreasesSerum Cholesterol in Post Menopausal Women
Forrest H. Nielsen, PhD, David B. Milne**, PhD, Leslie M. Klevay*, MD, Sandra Gallagher, BS, and LuAnn Johnson, MS
US Department of Agriculturea,b, Agricultural Research Service, Grand Forks Human Nutrition Research Center, Grand Forks,North Dakota
Key words: magnesium deficiency, magnesium balance, heart arrhythmia, glucose tolerance, cholesterol
Objective: To determine whether or not dietary magnesium restriction to about 33% of the RecommendedDietary Allowance (RDA) causes changes in glucose, cholesterol and electrolyte metabolism that could lead topathologic consequences.
Design: The length of the experiment was 136 days. Subjects were fed a basal Western-type diet thatprovided 4.16 mmol (101 mg) magnesium per 8.4 MJ (2000 kcal) for 78 days then replenished with magnesiumby supplementing the diet with 200 mg magnesium as the gluconate per day for 58 days. If a subject exhibitedadverse heart rhythm changes before 78 days of depletion were completed, she entered the repletion period early.
Setting: The metabolic research unit of the Grand Forks Human Nutrition Research Center.Subjects: A total of 14 post menopausal women were recruited by advertisement throughout the United
States. Thirteen women (ages 47 to 75 years) completed the study.Results: During magnesium depletion, heart rhythm changes appeared in 5 women and resulted in 4 prematurely
entering the magnesium repletion period (42 to 64 days of depletion instead of 78). Three women exhibited atrialfibrillation and flutter that responded quickly to magnesium supplementation. Magnesium deprivation resulted in anon-positive magnesium balance that became highly positive with magnesium repletion. Magnesium deprivationdecreased red blood cell membrane magnesium, serum total cholesterol and erythrocyte superoxide dismutaseconcentrations, increased the urinary excretion of sodium and potassium, and increased serum glucose concentration.
Conclusions: Magnesium balance may be a suitable indicator of magnesium depletion under experimentalconditions. Magnesium deficiency resulting from feeding a diet that would not be considered having an atypicalmenu induces heart arrhythmias, impairs glucose homeostasis, and alters cholesterol and oxidative metabolismin post menopausal women. A dietary intake of about 4.12 mmol (100 mg) Mg/8.4 MJ is inadequate for healthyadults and may result in compromised cardiovascular health and glycemic control in post menopausal women.
INTRODUCTION
Epidemiological surveys, supplementation trials, and animalstudies have suggested that magnesium deficiency in humans mayresult in impaired glucose, lipid and electrolyte metabolism. Be-cause of these impairments, magnesium deficiency has been sug-gested to be a factor in some cardiac arrhythmias, changing lipid
metabolism conducive to increased risk of cardiovascular disease,and contributing to complications of diabetes. However, directevidence that primary dietary magnesium deficiency of a severitysimilar to that which may occur in the general population (e.g.,10% of women over the age of 70 yr consume less than 42% of theRDA) provokes changes in glucose, lipid and electrolyte metab-olism that result in pathologic consequences is limited.
Address reprint requests to: Forrest H. Nielsen, PhD, USDA, ARS, Grand Forks Human Nutrition Research Center, PO Box 9034, Grand Forks, ND, 58202-9034. E-mail:[email protected]
*Current Address: School of Medicine, University of North Dakota, Grand Forks, ND.
**Current address: PO Box 366, Gallatin Gateway, MT 59730.aThe US Department of Agriculture, Agricultural Research Service, Northern Plains Area, is an equal opportunity/affirmative action employer, and all agency services areavailable without discrimination.bMention of a trademark or proprietary product does not constitute a guarantee or warranty by the US Department of Agriculture and does not imply its approval to theexclusion of other products that also might be suitable.
Journal of the American College of Nutrition, Vol. 26, No. 2, 121–132 (2007)Published by the American College of Nutrition
121

There are numerous reports indicating that hypomagnesmiamay be associated with complications in diabetic patients [1].However, whether the hypomagnesmia is a cause or an effect ofdiabetes is uncertain [2]. Some studies have shown that mag-nesium deficiency in otherwise healthy adults impairs someaspects of blood glucose homeostasis. Nadler et al [3] fed 12normal subjects a liquid diet providing only 0.5 mmol (12 mg)Mg/d for four weeks. The diet reduced both serum and redblood cell magnesium and decreased insulin sensitivity duringan intravenous glucose tolerance test (IVGTT). Paolisso et al[4] in a double blind, randomized, crossover study gave aplacebo or a supplement providing 16.2 mmol (394 mg) Mg/dto 12 elderly subjects with low erythrocyte magnesium con-centration. The magnesium supplement increased erythrocytemagnesium concentration and improved insulin response andaction during an IVGTT. They also stated that the increase inerythrocyte magnesium significantly and positively correlatedwith a decrease in erythrocyte membrane microviscosity andwith total-body and oxidative glucose metabolism. In healthyadults, an acute oral load of magnesium (30 mmol or 730 mg)after an overnight fast induced a decrease in blood glucoseconcentrations four hours after the magnesium ingestion, ap-parently by increasing insulin sensitivity [5].
Although magnesium deficiency has been suggested to be afactor in the development of cardiovascular disease partlythrough increasing circulating concentrations of cholesterol andcholesterol fractions in humans [6,7], support for this sugges-tion is not strong. In order to show that magnesium deficiencyaffects serum cholesterol in rats, experiments had to be long-term, use pair-feeding techniques with severe deficiency, orrequired high dietary cholesterol [8]. Instead of an increase, adecrease in serum cholesterol concentration was found withmagnesium deprivation in one human study [9]. Animal studiesalso suggested that hypertriglyceridemia may be a sign ofmagnesium deficiency [8]. However, like with cholesterol,changes in triglycerides induced by magnesium deficiencywere dependent upon the presence of certain experimental anddietary conditions. Thus, the effect of dietary magnesium de-privation on lipid metabolism in humans has not been clearlydefined.
There are numerous reports indicating that magnesium hasa role in maintaining normal heart rhythm. One study foundthat low dietary magnesium increased supraventricular ectopyin postmenopausal women [10]. Also, acute high doses ofmagnesium have been used to successfully convert atrial fibril-lation to sinus rhythm and to overcome multifocal atrial tachy-cardia [11]. Hypomagnesemia can increase the risk of su-praventricular and ventricular arrhythmias, includingventricular tachycardia and ventricular fibrillation [12,13].Some of these dysrhythmias may be the result of an imbalancein electrolytes such as potassium, sodium and calcium causedby low dietary magnesium [14].
Although magnesium deficiency caused by drugs and dis-ease is not rare [15], deficiency caused by dietary restriction
has been questioned. One expert group stated that a “dietarydeficiency of magnesium of a severity sufficient to provokepathologic change is rare” [16]. Other magnesium experts haveconcluded that chronic primary magnesium deficiency occursfrequently and has various pathological consequences resultingfrom altered carbohydrate, lipid and electrolyte metabolism[7,17,18]. The objective of the experiment described in thisreport was to determine if an inadequate magnesium intake(about 30% of the RDA) achieved through a diet that would not beconsidered having an atypical menu can cause changes in glucose,cholesterol and electrolyte metabolism. As a result, dietary mag-nesium deficiency causing pathologic consequences may be ofmore significance than currently acknowledged.
SUBJECTS AND METHODS
Subjects
Fourteen post-menopausal women were recruited for thestudy after they had been informed in detail both verbally andin writing about the nature of the research and associated risks,and after medical, psychological, and nutritional evaluation hadestablished that they were healthy and emotionally suited forthe project. One subject decided not to enter the study. The 13women (12 Caucasian and 1 African-American) who com-pleted the study were not on hormone replacement therapy, didnot smoke, and had a mean age 61.8 � 8.2 (range of 47 to 75years with five aged 65 years or older). The women ranged inheight from 149.7 to 167.7 cm, in weight from 49.9 to 96.8 kgand in body mass index of 19.9 to 34.4 (mean of 25.5 with onlyone woman greater than 30). Before entry into the study, aphysical examination in a local clinic that included a pap smear,lung x-ray, tuberculosis test and electrocardiogram (EKG), andlaboratory tests to assess liver, kidney and thyroid functionestablished that the women had no underlying disease. Thesubjects resided for the entire study in the metabolic researchunit of the Grand Forks Human Nutrition Research Center thatprovided a common environment for strict control of foodconsumption, weight, exercise, and data collection. Subjectsconsumed only food and beverages provided by the dietarystaff and were chaperoned on all outings from the metabolicunit to ensure compliance with the study protocol.
The participants gave their written informed consents toparticipate in the experimental protocol that was approved bythe Institutional Review Board of the University of NorthDakota and the Human Studies Review Committee of theUnited States Department of Agriculture, and followed theguidelines of the Department of Health and Human Servicesand the Helsinki Doctrine regarding the use of human subjects.
Experimental Protocol
Because potentially harmful electrocardiographic changeshave been found in people deficient in magnesium [10–14], a
Magnesium Deficiency in Postmenopausal Women
122 VOL. 26, NO. 2

20-hr EKG using a Holter Recorder was performed on eachvolunteer every two weeks during the study. Tapes obtainedwere machine (Model 363, Accuplus, Del Mar Avionics, Ir-vine, CA) scanned for signs of abnormal rhythm by trainednurses under the direction of a physician who confirmed thefindings of the nurses. If the EKG showed a significant increase(four times baseline obtained from the initial two Holter EKGs)in ventricular premature discharges, the appearance of AVheart blocks, or the appearance of atrial flutter and fibrillation,the change was confirmed by immediately performing anotherHolter EKG. Confirmation of one these changes while consum-ing the low magnesium diet prompted a premature entry intothe magnesium repletion dietary period.
Because magnesium deficiency has been correlated withhypertension [19], blood pressures were measured daily duringthe study. Upon wakening in the morning, each volunteerwould notify by intercom the on-duty nurse trained in bloodpressure measurement. The nurse then went to the room of eachwoman and determined their blood pressure by using a mercurysphygmomanometer while she was lying in bed. If the volun-teer had to use the toilet upon wakening, she was required toreturn to her bed and recline for 20 minutes before her bloodpressure was determined.
Upon arrival in the metabolic unit, all women immediatelybegan consuming the basal magnesium-deficient diet. The orig-inal design of the experiment was to have the magnesiumdeprivation period to last 93 days, but because of heart arrhyth-mias, this was shortened to 78 days. The subjects were replen-ished with magnesium for 58 days by supplementing the dietwith 8.23 mmol (200 mg) of magnesium as magnesium glu-conate per day. The supplementation resulted in a magnesium
intake near the 1989 U.S. Recommended Dietary Allowance(RDA) of 11.52 mmol (280 mg) per day [20] that was in placeat the time of the study. Two of the women were fed anadditional 4.12 mmol (100 mg) of magnesium per day for fourweeks because increased ventricular premature discharges(VPD) did not quickly return to baseline.
The diet used in the study was based on ordinary Westernfoods and is shown in Table 1. A three-day menu rotation wasused to give some variety but assured that variation in nutrientintake was not consequential. As shown in Table 2 the dietsupplied approximately 101 mg (4.16 mmol) magnesium per8.4 KJ (2,000 kcal). This intake was near the first percentileintake of women aged over 51 years according to the 1994Continuing Survey of Food Intake of Individuals (CSFII) [21].The diet energy distribution was 9.7% protein, 36.1% fat and54.2% carbohydrate. The diet was based on the 1989 Recom-mended Dietary Allowances (RDA) [20] because it was for-mulated before the issuance of the current Dietary ReferenceIntakes. To assure adequacy, supplements were used for nutri-ents present in low or unknown quantities in the diet. Thesesupplements were (per day) 625 mg (16 mmol) potassium aspotassium chloride, 270 mg (6.74 mmol) calcium as calciumgluconate, 20 mg (0.36 mmol) iron as ferrous gluconate, 6 mgzinc (92 �mol) as zinc sulfate, 1.1 mg (17 �mol) copper ascopper sulfate, 0.33 mg boron (31 �mol) as boric acid, 133 �g(301 mmol) of folic acid, 100 �g biotin, and 400 IU of vitaminD3. Although formulating a diet low in magnesium resulted ina relatively low protein intake of 48 g/8.4 KJ, the protein intakeof all women was near the RDA of 46 mg/d. Dietary iron wasprovided in excess of the RDA to mitigate the decline in ironstatus as a result of phlebotomy during the experiment. All food
Table 1. Food Composition of the 3-Day Rotation Diet
Breakfast Cranapple juice Tang Milk, 2%Cornflakes Pork sausage Coffee cakeNon-dairy creamer White bread ButterWhite bread ButterButter Grape jellyBlueberries
Lunch Carbonated citrus drinka Apple juice Cranapple juiceBeef stew Chicken rice casserole Crispy chickenLettuce Cauliflower Buttered ditaliniFrench Dressing Rusks Green beansRusks Carrot cake Vanilla wafersIce Cream Cream cheese frosting
Supper Tropical punch Lemonade Carbonated citrus drinkChicken cheese casserole Minestrone soup BBQ Pork with vegetablesCrackersb Rusks Steamed riceCherry jelloc Lettuce Shortbread cookies
Russian dressing Lemon fruit drinkApplesauce
Snack Orange fruit drink Milk, 2% Lime jelloc with pearsShortbread cookies Pound cake Whipped topping
a 7-Up; Dr Pepper/Seven Up, Inc., Plano, TX.b Ritz, Nabisco, East Hanover, NJ.c Kraft Foods, Inc., Rye Brook, NY.
Magnesium Deficiency in Postmenopausal Women
JOURNAL OF THE AMERICAN COLLEGE OF NUTRITION 123

was weighed with an accuracy of 0.1 g during preparation inthe metabolic kitchen and was completely consumed by thesubjects with the aid of spatulas and rinse bottles. Deionizedwater was consumed ad libitum. The initial energy requirementfor each subject was determined by using the Harris and Bene-dict equation [22] and adding 50% to compensate for normaldaily activities. Individually prescribed exercise was performedthree times weekly to maintain body composition and physicalwork capacity. Energy intake was adjusted in 0.84 KJ (200kcal) increments during the course of the study to maintainbody weight (measured daily) within � 2% of admissionweight.
For magnesium balance determinations, duplicate diets of8.4 MJ (2,000 kcal) were prepared daily for analysis andblended in a plastic blender with stainless steel blades. Urineand feces were collected in plastic containers and bags, respec-tively, to avoid mineral contamination. Venous blood, collectedin plastic syringes from antecubital veins that had been dis-tended by the temporary use of a tourniquet after the subjectshad fasted for 12 hr, was obtained weekly for routine healthassessment and mineral and cholesterol determinations; addi-tional blood was obtained during weeks 3, 6, 9, 11 and 13 forthe determination of other experimental variables, and duringweek 12 of depletion and week 6 of repletion for an intravenousglucose tolerance test (IVGTT). Total blood collected waslimited to �250 mL/mo.
At the time the Holter EKGs were performed, standardneuromuscular magnesium deficiency tests, checking forTrousseau’s and Chvostek’s signs (reflexes) were done. Thetest for Trousseau’s sign involves inflating a sphygmomanom-eter cuff to 10 mm above systolic blood pressure and holdingthis pressure for two minutes. Carpal spasm with relaxation 5to 10 s after deflation is considered positive. The test forChvostek’s sign involves tapping the facial nerve just anterior
to the ear lobe and just below the zygomatic arch (or betweenthe arch and the corner of the mouth). A positive responseranges from a simple twitching of the corner of the mouth to atwitching of all facial muscles on the stimulated side.
Laboratory Methods
The magnesium content of 6-d composites of diets and feceswere determined throughout the experiment by inductivelycoupled argon plasma emission spectroscopy (ICAP) (Jarrell-Ash Atom Comp 1140, Thermo Elemental, Franklin, MA) [23]after wet digestion of lyophilized blended samples with nitricand perchloric acids [24]. Urinary minerals (magnesium, cal-cium, sodium, and potassium) were determined by ICAP of adiluted aliquot. For diets and feces, concurrent replicate anal-ysis of a standard reference material, NIST 1577a bovine liver(National Institute of Standards and Technology, Gaithersburg,MD) yielded a mean � standard deviation of 568 � 12 �g/gcompared with certified values (means � confidence values) of600 � 15 �g/g for magnesium. For urine, concurrent replicateanalysis of UriChem 1 & 2 (Fisher Scientific, Orangeburg, NY)yielded a mean � standard deviation of 167 � 10 mg/Lcompared with a certified value of 160 � 58 mg/L. Magnesiumbalance was calculated as the difference between intake andexcretion (feces plus urine) for all days and for the last 36 daysof each dietary period. The 36-d data are presented becausethey correspond to the time that the biochemical variables thatwere statistically compared were determined. The balance orretention calculations did not include surface or phlebotomylosses.
Blood was processed within 90 min to obtain serum orplasma. The blood was allowed to clot for 20 min beforecentrifuging at 2000 RPM for 10 min to obtain serum. Todetermine the amount of magnesium in serum loosely bound to
Table 2. Calculated and Analyzed Nutrient Composition of the Diet per 8.4 MJ (2000 kcal)
Calculated component Amount Analyzed componenta Amount
Energy, MJ 8.4 (2000 kcal) Potassium, mg 1803Protein, g 48 Phosphorus, mg 845Protein, % 9.6 Calcium, mg 694Carbohydrate, g 276 Iron, mg 28Carbohydrate, % 54.3 Magnesium, mg 101Fat, g 82 Zinc, mg 9.37Fat, % 36.1 Copper, mg 1.35Cholesterol, mg 201 Manganese, mg 1.0Vitamin A, IU 9749 Boron, mg 1.09Thiamin, mg 0.98 Sodium, mg 2237Riboflavin, mg 1.19Niacin, mg 14.0Ascorbic acid, mg 188Vitamin B6 0.99Vitamin B12, �g 2.65Folacin, �g 361Vitamin D, IU 400�-Tocopherol, mg 3.53
a Minerals determined by inductively coupled argon plasma emission spectroscopy. Some minerals were in the form of supplements; see text.
Magnesium Deficiency in Postmenopausal Women
124 VOL. 26, NO. 2

albumin and more tightly bound to �-macroglobulin, the�-macroglobulin was precipitated from serum with polyethyl-ene glycol 6000 (PEG). The PEG solution was prepared byadding 100 g PEG, 3.03 g (50 mmol) Tris and 0.1 g sodiumazide to 400 mL of deionized water. The pH was adjusted to 7.1with glacial acetic acid before filtering through a 0.45 �mMillipore filter (Millipore, Bedford, MA). The PEG solutionwas stored at 0° to 4°C. A 0.5 mL aliquot of clear serum wastransferred to each of four tubes; 1.5 mL of 6.7% trichloroace-tic acid (TCA) was added to two of the tubes for duplicateanalysis of serum total magnesium. For obtaining the albuminfraction in duplicate, 0.5 mL of the PEG reagent was added toeach of two tubes. All tubes were centrifuged at 2550 RPM for30 min. An aliquot of 0.5 mL was taken from each of the tubescontaining PEG and placed in a separate set of tubes to which0.5 mL of 10% TCA solution was added before centrifugingagain at 2550 RPM for 30 min; the supernatant contained thealbumin-bound magnesium. The ultrafiltrable fraction of serumwas obtained from serum that was collected under anaerobicconditions. The Millipore Ultrafree-PF system (Cat. No. UFP1TGC 24, Millipore, Bedford, MA) was used to obtain theultrafiltrate. One mL of serum was placed in the filter cupbefore being capped tightly with and pressured applied throughthe top cap by a 30 mL syringe with a luer lock hub. Pressurewas maintained by using a wide rubber band extending over thetop of the syringe and surrounding the lower sample collectioncup. The assembly was placed in a refrigerator at 4°C for 3 daysto obtain the ultrafiltrable serum fraction. The total serum,albumin-bound, and ultrafiltrable magnesium concentrationswere determined by ICAP. Concurrent analysis of Sera Chemcontrols (Fisher Scientific, Orangeburg, NY) yielded the valueof 21.1 � 1.6 mg/L compared with the certified value of 22.4 �
6.2 mg/L for magnesium. The �-macroglobulin-bound magne-sium was calculated as the difference between total serum andalbumin-bound magnesium. The method of Dodge et al [25]was used to obtain red blood cell membranes from 10 mL ofblood collected using EDTA as the anticoagulant. The proteincontent of the membranes was determined by using a commer-cially available kit (Biorad Protein Kit #500-0006, Standard#500-0007, Biorad, Hercules, CA). Each membrane samplewas diluted by a factor of 5 with deionized water beforeanalyzing for magnesium by ICAP.
Red blood cell number, mean corpuscular volume (MCV),mean corpuscular hemoglobin concentration (MCHC), meancorpuscular hemoglobin (MCH), hemoglobin concentrationand hematocrit of blood were determined by using a CoulterCounter (Model S�4, Coulter Electronics, Hialeah FL). Serumtotal cholesterol, high-density lipoprotein (HDL)-cholesterol,triglycerides, iron, sodium and potassium were determined bystandard methods using the Cobas Fara Centrifugal Analyzer(Roche Diagnostics Systems, Sommerville, NJ). Dividing tri-glyceride values by five indicates the serum concentration ofvery low-density lipoprotein (VLDL) [26] and low-density
lipoprotein (LDL)-cholesterol was calculated by difference be-tween total cholesterol and other cholesterol fractions. Com-mercially available kits were used to determine ferritin (CA590Gamma DAB, Baxter Travenol Diagnostic, Inc., Cambridge,MA) and aldosterone (TKAL 1, Diagnostic Products, Los An-geles, CA). Erythrocyte superoxide dismutase (ESOD) wasdetermined by using the method of Winterbourne et al [27].
The IVGTT determination was made after an overnight fast.A glucose load of 0.5 g/kg body weight in 110 mL of water wasinfused into an antecubital vein of one arm. Blood was obtainedfrom the contralateral arm by using a butterfly needle tubingsystem. Blood for serum insulin and glucose and plasma glu-cagon was taken at 0, 2.5, 5, 10, 20, 30, 45 and 60 minutes afterglucose infusion. Serum glucose was determined by using thestandard method of Cobas Fara Centrifugal Analyzer (RocheDiagnostic Systems, Sommerville, NJ). Commercially avail-able radioimmunoassay kits were used to determine insulin(TKIN 1, Diagnostic Products Corp., Los Angeles, CA) andglucagon (Kit #133, ICN Biomedical, Inc., Carson, CA).
Data Analysis
All balance and biochemical determinations made duringthe last 36 days in each dietary period were used in thestatistical analyses. These determinations were used becauselongitudinal graphing of primary variables of interest (Figs.1–4) showed that the response to the low and supplementaldietary magnesium had occurred during the last five weeks ofeach dietary period. Figs. 1–4 also indicate the baseline orinitial values for the primary variables of interest. The datawere analyzed by repeated measures analysis of variance witha SAS general linear model program (SAS 8.02, SAS Institute,Cary, NC). A p � 0.05 was considered significant. Variances inthe data are expressed as a pooled standard deviation, calcu-lated as the square root of the mean square error from theanalysis of variance.
Fig. 1. Erythrocyte membrane magnesium concentrations. �Valuedoes not contain four subjects that began magnesium repletion after 42,52 and 64 days of magnesium depletion.
Magnesium Deficiency in Postmenopausal Women
JOURNAL OF THE AMERICAN COLLEGE OF NUTRITION 125
RESULTS
During the low dietary magnesium period, heart rhythmchanges appeared in 4 of the 13 subjects that resulted inpremature entry into the magnesium repletion dietary period(Table 3). When the fifth subject showed a heart rhythm at 75days, all remaining subjects started the magnesium repletionperiod after 78 days of deprivation. All the heart rhythmchanges were confirmed by a repeat 20-hour Holter EKG. Thefirst woman (age 59.5 years) began the magnesium repletionperiod after 42 days of deprivation because of the appearanceof atrial flutter and fibrillation. These heart rhythm changesdisappeared two weeks after the magnesium repletion wasstarted and did not reappear for the remainder of the study.After 52 days of magnesium deprivation, two more subjectsshowed heart rhythm changes. One subject (age 67.3 years)
exhibited increased ventricular premature discharges (VPDs)and second degree AV heart blocks of Mobitz types I and II.Her last Holter EKG in the magnesium repletion period showedneither of these arrhythmias. The second subject (age 75.3years) exhibited increased VPDs; the number of VPDs de-creased by the end of magnesium repletion but did not reachbaseline levels. After 64 days of magnesium depletion, a sub-ject (age 65.2 years) exhibited atrial flutter and fibrillation thatdisappeared shortly after magnesium repletion and did notreappear. At 75 days, another subject (age 47.2 years) exhibitedan increase in VPDs and atrial flutter. The atrial flutter disap-peared two weeks after magnesium repletion began and theVPDs declined to below baseline at the end of the magnesiumrepletion period. Although it did not prompt a premature entryinto the magnesium repletion period, one subject (age 67.0years) exhibited occasional supraventricular tachycardia duringmagnesium deprivation period; she did not exhibit this duringthe magnesium repletion period.
Blood pressure was not significantly affected by magnesiumdepletion. During the last five weeks of depletion and repletionthe mean systolic/diastolic pressures of the 13 volunteers were114/70 mm and 113/70 mm, respectively. However, the vol-unteer that showed heart rhythm changes after 42 days ofdepletion had an elevated mean blood pressure of 146/89 mmduring depletion that decreased to an average 126/81 mmduring the last five weeks of magnesium repletion. This de-crease was countered by small unremarkable increases in bloodpressure during magnesium repletion in some women (includ-ing two women that exhibited heart rhythm changes) whosemean systolic pressure during depletion did not exceed 122 mmand mean diastolic pressure did not exceed 75 mm.
Table 4 shows that magnesium balance was positive whenthe diet provided an average of 12.67 to 13.13 mmol (308 to319 mg) Mg/d. Urinary magnesium excretion was significantlydecreased when the diet provided a mean of only 4.28 to 4.44mmol (104 to 108 mg) Mg/d. This homeostatic response wasnot enough to prevent a non-positive (negative value but not
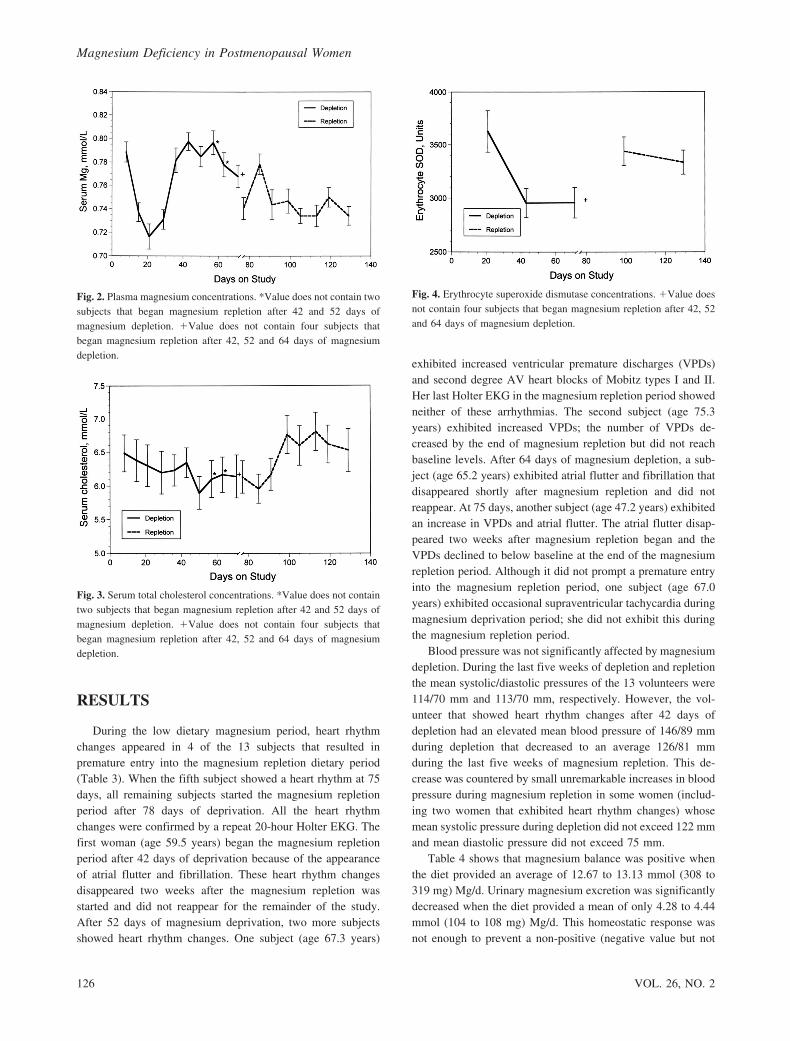
Fig. 2. Plasma magnesium concentrations. *Value does not contain twosubjects that began magnesium repletion after 42 and 52 days ofmagnesium depletion. �Value does not contain four subjects thatbegan magnesium repletion after 42, 52 and 64 days of magnesiumdepletion.
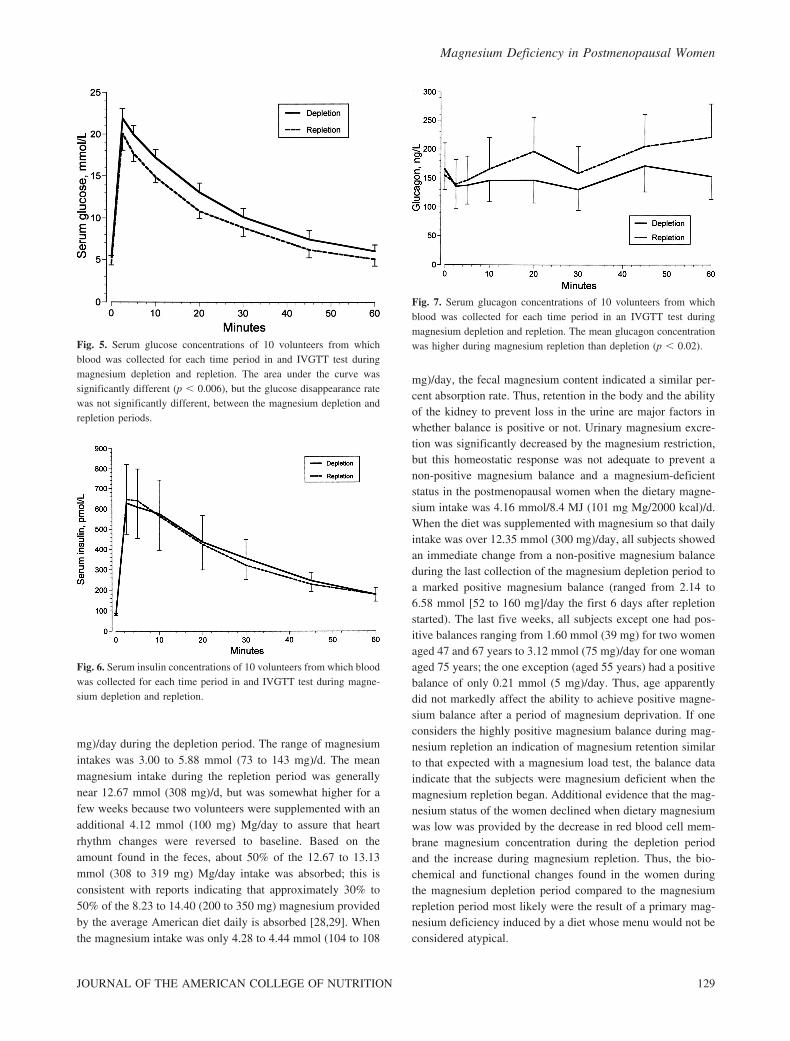
Fig. 3. Serum total cholesterol concentrations. *Value does not containtwo subjects that began magnesium repletion after 42 and 52 days ofmagnesium depletion. �Value does not contain four subjects thatbegan magnesium repletion after 42, 52 and 64 days of magnesiumdepletion.
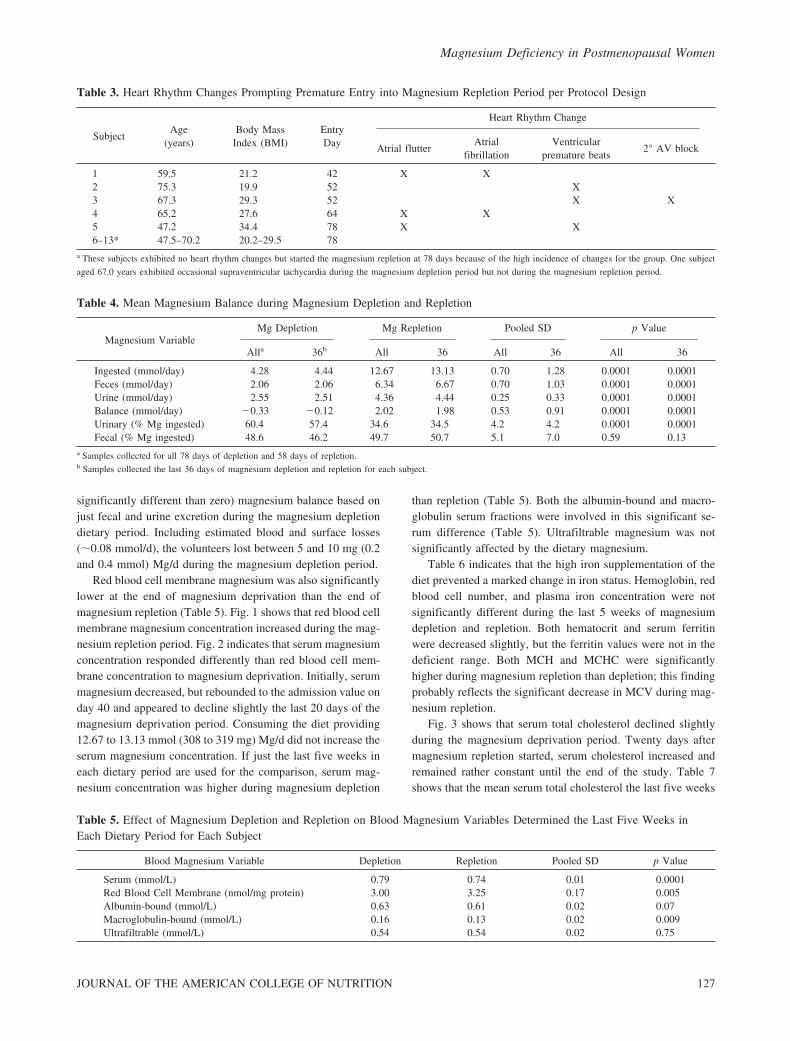
Fig. 4. Erythrocyte superoxide dismutase concentrations. �Value doesnot contain four subjects that began magnesium repletion after 42, 52and 64 days of magnesium depletion.
Magnesium Deficiency in Postmenopausal Women
126 VOL. 26, NO. 2
significantly different than zero) magnesium balance based onjust fecal and urine excretion during the magnesium depletiondietary period. Including estimated blood and surface losses(�0.08 mmol/d), the volunteers lost between 5 and 10 mg (0.2and 0.4 mmol) Mg/d during the magnesium depletion period.
Red blood cell membrane magnesium was also significantlylower at the end of magnesium deprivation than the end ofmagnesium repletion (Table 5). Fig. 1 shows that red blood cellmembrane magnesium concentration increased during the mag-nesium repletion period. Fig. 2 indicates that serum magnesiumconcentration responded differently than red blood cell mem-brane concentration to magnesium deprivation. Initially, serummagnesium decreased, but rebounded to the admission value onday 40 and appeared to decline slightly the last 20 days of themagnesium deprivation period. Consuming the diet providing12.67 to 13.13 mmol (308 to 319 mg) Mg/d did not increase theserum magnesium concentration. If just the last five weeks ineach dietary period are used for the comparison, serum mag-nesium concentration was higher during magnesium depletion
than repletion (Table 5). Both the albumin-bound and macro-globulin serum fractions were involved in this significant se-rum difference (Table 5). Ultrafiltrable magnesium was notsignificantly affected by the dietary magnesium.
Table 6 indicates that the high iron supplementation of thediet prevented a marked change in iron status. Hemoglobin, redblood cell number, and plasma iron concentration were notsignificantly different during the last 5 weeks of magnesiumdepletion and repletion. Both hematocrit and serum ferritinwere decreased slightly, but the ferritin values were not in thedeficient range. Both MCH and MCHC were significantlyhigher during magnesium repletion than depletion; this findingprobably reflects the significant decrease in MCV during mag-nesium repletion.
Fig. 3 shows that serum total cholesterol declined slightlyduring the magnesium deprivation period. Twenty days aftermagnesium repletion started, serum cholesterol increased andremained rather constant until the end of the study. Table 7shows that the mean serum total cholesterol the last five weeks
Table 3. Heart Rhythm Changes Prompting Premature Entry into Magnesium Repletion Period per Protocol Design
SubjectAge
(years)Body Mass
Index (BMI)EntryDay
Heart Rhythm Change
Atrial flutterAtrial
fibrillationVentricular
premature beats2° AV block
1 59.5 21.2 42 X X2 75.3 19.9 52 X3 67.3 29.3 52 X X4 65.2 27.6 64 X X5 47.2 34.4 78 X X6–13* 47.5–70.2 20.2–29.5 78
a These subjects exhibited no heart rhythm changes but started the magnesium repletion at 78 days because of the high incidence of changes for the group. One subject
aged 67.0 years exhibited occasional supraventricular tachycardia during the magnesium depletion period but not during the magnesium repletion period.
Table 4. Mean Magnesium Balance during Magnesium Depletion and Repletion
Magnesium VariableMg Depletion Mg Repletion Pooled SD p Value
Alla 36b All 36 All 36 All 36
Ingested (mmol/day) 4.28 4.44 12.67 13.13 0.70 1.28 0.0001 0.0001Feces (mmol/day) 2.06 2.06 6.34 6.67 0.70 1.03 0.0001 0.0001Urine (mmol/day) 2.55 2.51 4.36 4.44 0.25 0.33 0.0001 0.0001Balance (mmol/day) �0.33 �0.12 2.02 1.98 0.53 0.91 0.0001 0.0001Urinary (% Mg ingested) 60.4 57.4 34.6 34.5 4.2 4.2 0.0001 0.0001Fecal (% Mg ingested) 48.6 46.2 49.7 50.7 5.1 7.0 0.59 0.13
a Samples collected for all 78 days of depletion and 58 days of repletion.b Samples collected the last 36 days of magnesium depletion and repletion for each subject.
Table 5. Effect of Magnesium Depletion and Repletion on Blood Magnesium Variables Determined the Last Five Weeks inEach Dietary Period for Each Subject
Blood Magnesium Variable Depletion Repletion Pooled SD p Value
Serum (mmol/L) 0.79 0.74 0.01 0.0001Red Blood Cell Membrane (nmol/mg protein) 3.00 3.25 0.17 0.005Albumin-bound (mmol/L) 0.63 0.61 0.02 0.07Macroglobulin-bound (mmol/L) 0.16 0.13 0.02 0.009Ultrafiltrable (mmol/L) 0.54 0.54 0.02 0.75
Magnesium Deficiency in Postmenopausal Women
JOURNAL OF THE AMERICAN COLLEGE OF NUTRITION 127

of depletion was significantly lower than in the similar periodof magnesium repletion. Most of the change was in the LDL-cholesterol fraction. Magnesium depletion slightly decreasedthe serum triglyceride concentration also. Table 7 also showsthat erythrocyte superoxide dismutase (ESOD) was higher dur-ing the last weeks of magnesium repletion than depletion. Thetime course of the change in ESOD is shown in Fig. 4.
Dietary magnesium did not significantly affect serum aldo-sterone, sodium and potassium concentrations, and urine cal-cium concentration (Table 8). However, based on 24-h urinedeterminations, both urinary sodium and potassium were sig-nificantly lower during magnesium depletion than repletion.
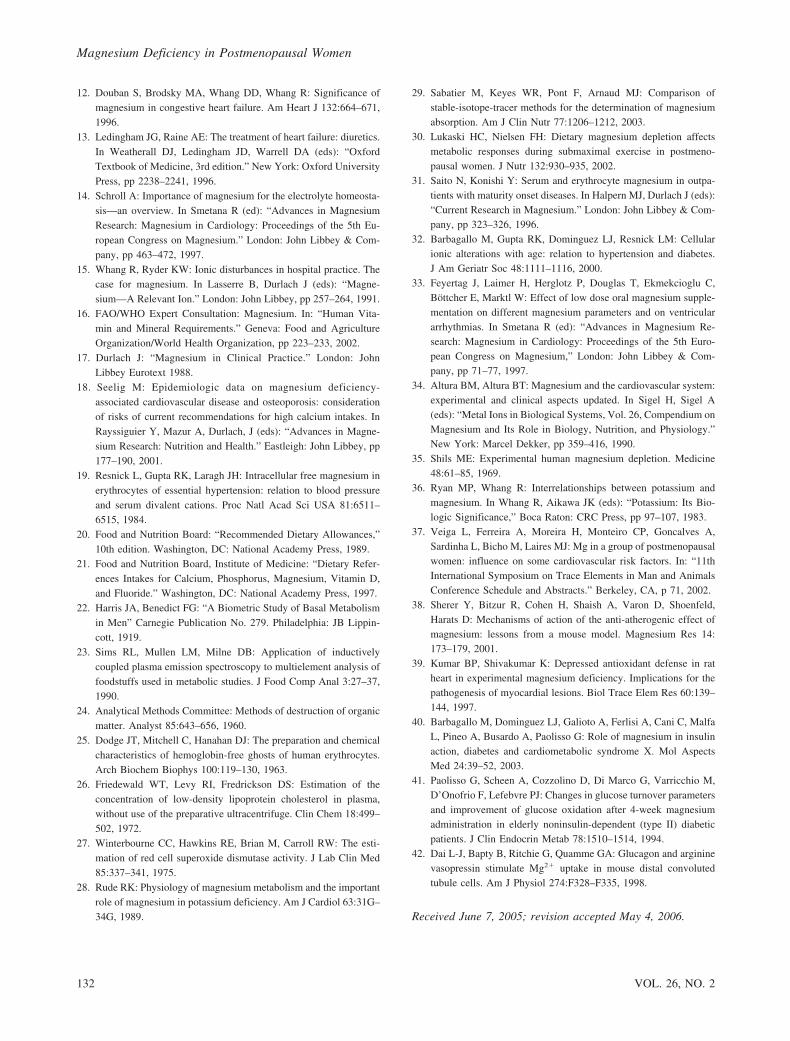
The glucose, insulin and glucagon responses to the glucosetolerance test are shown in Figs. 5–7. These figures show thatfasting serum glucose was higher during magnesium depletionthan repletion. In the IVGTT test during magnesium depletion,serum glucose rose to a higher concentration and remainedhigher until the end of the test than during the magnesiumrepletion (Fig. 5). Thus, the area under the curve for glucose
was significantly greater (p � 0.006) during magnesium de-pletion than repletion. However, the rate of glucose decrease inthe IVGTT test was not significantly affected by magnesiumdeprivation, nor was the insulin response (Fig. 6). At the startof the IVGTT test, basal serum glucagon concentration was notdifferent during the two dietary periods. A few minutes afterglucose infusion, plasma glucagon decreased in the magnesiumdepletion dietary period, and increased in the magnesium re-pletion period such that average glucagon concentration wassignificantly lower (p � 0.02) during magnesium deprivation.
DISCUSSION
Although the analyzed magnesium content of the basal dietat the beginning of the study was 4.16 mmol/8.4 MJ (101mg/2000 kcal), different caloric intakes by the volunteers tomaintain weight at admission weight � 2% resulted in meanmagnesium intakes between 4.28 and 4.44 mmol (104 and 108
Table 7. Effect of Magnesium Depletion and Repletion on Serum Total Cholesterol, Cholesterol Fractions, Triglycerides, andErythrocyte Superoxide Dismutase (ESOD) Determined the Last Five Weeks of Each Dietary Period for Each Subject
Variable Mg Depletion Mg Repletion Pooled SD P Value
Total Cholesterol (mmol/L) 6.10 6.67 0.28 0.0003LDL-Cholesterol (mmol/L) 4.01 4.34 0.38 0.05HDL-Cholesterol (mmol/L) 1.53 1.53 0.05 0.68Triglycerides (mg/dL) 1.55 1.61 0.07 0.02ESOD (Ua/mg hemoglobin) 2973 3387 438 0.03
a Units are amount needed to inhibit pyrogallol oxidation by 50%.
Table 8. Effect of Magnesium Depletion and Repletion on Urinary and Serum Sodium, Potassium and Aldosterone Determinedthe Last Five Weeks of Each Dietary Period for Each Subject
Variable Mg Depletion Mg Repletion Pooled SD P Value
Serum Sodium (mmol/L) 149.1 148.3 1.1 0.08Serum Potassium (mmol/L) 4.57 4.60 0.14 0.54Urinary Sodium (mmol/d) 68 77 8 0.01Urinary Potassium (mmol/d) 29 32 2 0.002Urinary Calcium (mmol/d) 3.24 3.29 0.30 0.78Serum Aldosterone (pmol/L) 355 386 89 0.36
Table 6. Effect of Magnesium Depletion and Repletion on Red Blood Cell and Iron Variables Determined the Last Five Weeksof Each Dietary Period for Each Subject
Variable Mg Depletion Mg Repletion Pooled SD p Value
Red Blood Cell Number (106) 4.15 4.10 0.10 0.26MCVa (fL) 93.2 91.3 1.0 0.0005MCHC,b % 33.2 34.0 0.1 0.0001MCHc (pg) 30.6 30.9 0.2 0.02Hemoglobin (g/L) 128 127 4 0.52Hematocrit (%) 38.6 37.3 1.1 0.02Plasma Iron (�mol/L) 16.3 17.0 9 0.32Serum Ferritin (�g/L) 4.04 (56.6)d 3.60 (36.6)d 0.26 0.001
a Mean corpuscular volume.b Mean corpuscular hemoglobin concentration.c Mean corpuscular hemoglobin.d Mean of the ln-transformed values with the mean of the back-transformed values in parenthesis.
Magnesium Deficiency in Postmenopausal Women
128 VOL. 26, NO. 2
mg)/day during the depletion period. The range of magnesiumintakes was 3.00 to 5.88 mmol (73 to 143 mg)/d. The meanmagnesium intake during the repletion period was generallynear 12.67 mmol (308 mg)/d, but was somewhat higher for afew weeks because two volunteers were supplemented with anadditional 4.12 mmol (100 mg) Mg/day to assure that heartrhythm changes were reversed to baseline. Based on theamount found in the feces, about 50% of the 12.67 to 13.13mmol (308 to 319 mg) Mg/day intake was absorbed; this isconsistent with reports indicating that approximately 30% to50% of the 8.23 to 14.40 (200 to 350 mg) magnesium providedby the average American diet daily is absorbed [28,29]. Whenthe magnesium intake was only 4.28 to 4.44 mmol (104 to 108
mg)/day, the fecal magnesium content indicated a similar per-cent absorption rate. Thus, retention in the body and the abilityof the kidney to prevent loss in the urine are major factors inwhether balance is positive or not. Urinary magnesium excre-tion was significantly decreased by the magnesium restriction,but this homeostatic response was not adequate to prevent anon-positive magnesium balance and a magnesium-deficientstatus in the postmenopausal women when the dietary magne-sium intake was 4.16 mmol/8.4 MJ (101 mg Mg/2000 kcal)/d.When the diet was supplemented with magnesium so that dailyintake was over 12.35 mmol (300 mg)/day, all subjects showedan immediate change from a non-positive magnesium balanceduring the last collection of the magnesium depletion period toa marked positive magnesium balance (ranged from 2.14 to6.58 mmol [52 to 160 mg]/day the first 6 days after repletionstarted). The last five weeks, all subjects except one had pos-itive balances ranging from 1.60 mmol (39 mg) for two womenaged 47 and 67 years to 3.12 mmol (75 mg)/day for one womanaged 75 years; the one exception (aged 55 years) had a positivebalance of only 0.21 mmol (5 mg)/day. Thus, age apparentlydid not markedly affect the ability to achieve positive magne-sium balance after a period of magnesium deprivation. If oneconsiders the highly positive magnesium balance during mag-nesium repletion an indication of magnesium retention similarto that expected with a magnesium load test, the balance dataindicate that the subjects were magnesium deficient when themagnesium repletion began. Additional evidence that the mag-nesium status of the women declined when dietary magnesiumwas low was provided by the decrease in red blood cell mem-brane magnesium concentration during the depletion periodand the increase during magnesium repletion. Thus, the bio-chemical and functional changes found in the women duringthe magnesium depletion period compared to the magnesiumrepletion period most likely were the result of a primary mag-nesium deficiency induced by a diet whose menu would not beconsidered atypical.
Fig. 5. Serum glucose concentrations of 10 volunteers from whichblood was collected for each time period in and IVGTT test duringmagnesium depletion and repletion. The area under the curve wassignificantly different (p � 0.006), but the glucose disappearance ratewas not significantly different, between the magnesium depletion andrepletion periods.
Fig. 6. Serum insulin concentrations of 10 volunteers from which bloodwas collected for each time period in and IVGTT test during magne-sium depletion and repletion.
Fig. 7. Serum glucagon concentrations of 10 volunteers from whichblood was collected for each time period in an IVGTT test duringmagnesium depletion and repletion. The mean glucagon concentrationwas higher during magnesium repletion than depletion (p � 0.02).
Magnesium Deficiency in Postmenopausal Women
JOURNAL OF THE AMERICAN COLLEGE OF NUTRITION 129

Based on the results presented, the concentration of mag-nesium in serum or its albumin and macroglobulin fractions arenot suitable variables for ascertaining whether a person isbecoming magnesium deficient under experimental conditions.Fig. 2 suggests, depending upon the length of time of magne-sium deprivation, a decrease, increase, or no change in serummagnesium concentration may be seen during experimentalmagnesium deprivation. The initial response to magnesiumdeprivation may be a decrease in the concentration of serummagnesium. However, in this study the concentration increasedas magnesium depletion progressed. This increase may havebeen the result of increased mobilization from internal magne-sium stores in muscle [30] and bone. The reason magnesiumrepletion did not significantly increase the serum concentrationof magnesium may have been that magnesium was beingremoved from the blood to restore muscle and bone magnesiumconcentrations.
One sign of primary dietary magnesium deficiency mostlikely is heart arrhythmia. In this study, the arrhythmias thatresponded the best and quickest to magnesium repletion wereatrial flutter and fibrillation (exhibited by three subjects). In-creased VPDs during the magnesium depletion period did notrespond quickly to magnesium repletion, but the number ofVPDs decreased to baseline in one subject, near baseline inanother, and below baseline in a third by the end of repletion.The suggestion that atrial flutter and fibrillation can result fromdietary magnesium deficiency is supported by the finding thatsupplemental magnesium has been used to successfully convertatrial fibrillation to sinus rhythm [11]. Also, patients with atrialfibrillation have been found to have low erythrocyte magne-sium concentrations [31].
Age may have influenced the appearance of heart arrhyth-mias with magnesium deprivation in the present experiment.Barbagallo et al [32] compared the concentrations of cytosolicfree magnesium (Mgi) in erythrocytes from subjects older andyounger than 65 years. They found that Mgi was lower in olderthan younger normal subjects. If the woman who exhibitedsupraventricular tachycardia during magnesium deprivation isincluded, four of the six women aged 65 or over showed heartrhythm changes. Only two of the seven women younger of than65 years showed heart rhythm changes and one of these had ahigh BMI (34.4). Perhaps more of the women aged 65 years orolder started the present study with a lower magnesium statusthan those younger than 65 years.
The heart arrhythmias also may have been related to thechange in the urinary excretion of sodium and potassium.Feyertag et al [33] found that a magnesium supplement of 15mmol magnesium citrate compared to a placebo for 3 weeksgiven to patients after myocardial infarction decreased ventric-ular extrasystoles. Urinary potassium and sodium excretionalso increased in the magnesium supplemented patients. Theincreased excretion may be an indication that an electrolyteimbalance was present during the magnesium depletion period.Much evidence exists that magnesium has a regulatory role in
Na� and K� transport, cellular distribution, and intracellularconcentration. Magnesium activates the Na�, K�-ATPasepump that has a major role in regulating Na� and K� transport[34]. The finding of decreased urinary excretion of potassiumduring magnesium deprivation in the present study contrasts tothat found with humans made severely magnesium deficient (6to 10 mg/day); they had increased urinary potassium [35]. Theincrease was suggested to occur through a stimulation of aldo-sterone secretion that increases urinary potassium excretion[36]. Perhaps the severity of the magnesium deficiency was thereason for the contrasting results. This possibility is supportedby the finding of no significant change in circulating aldoste-rone and blood pressure induced by the magnesium deficiencyin the present experiment.
The finding that the concentration of total cholesterol waslower during magnesium depletion than repletion was surpris-ing. Animal experiments suggested that magnesium deficiencyshould increase serum cholesterol. However, in order to showthat magnesium deficiency affects serum cholesterol in rats,experiments had to be long-term, use pair-feeding techniqueswith severe deficiency, or required high dietary cholesterol [8].No convincing reports have indicated that increased serum totalcholesterol is a primary sign of magnesium deficiency in hu-mans. Two other reports gave cholesterol findings that supportour data showing that magnesium deprivation may decreaseserum total cholesterol. Veiga et al [37] found that postmeno-pausal women with RBC magnesium concentrations lower than44 mg (1.81 mmol)/L had lower plasma total and LDL-choles-terol than postmenopausal women with RBC magnesium con-centrations higher than 44 mg. Nielsen [9] found that a dietsupplying about 4.86 mmol (118 mg) magnesium/day com-pared to a diet supplying about 13.09 mmol (318 mg) magne-sium/day resulted in decreased plasma total cholesterol in post-menopausal women. Perhaps the change in circulatingcholesterol reflected a change in erythrocyte cellular membranelipid composition. Lipid components of the erythrocyte mem-brane exchange rapidly with plasma lipoproteins, and erythro-cyte cellular membrane composition and fluidity is altered bymagnesium deficiency [8].
Recent studies suggest that magnesium deficiency can pro-mote atherogenesis through mechanisms (e.g., LDL-cholesteroloxidation, formation of pro-inflammatory substances) otherthan by increasing circulating cholesterol [7,38]. The onlyindicator of reactive oxygen metabolism measured in this studywas ESOD, which was significantly decreased by magnesiumdeprivation. This finding is similar to that found with rats.Kumar and Shivakumar [39] found that magnesium deficiencydepressed the activity of superoxide dismutase in both plasmaand heart in rats. Depressed ESOD may be an indicator thatdietary magnesium deficiency may enhance the susceptibilityof postmenopausal women to oxidative injury.
The response to the IVGTT indicates that dietary magne-sium deficiency in humans impairs glucose homeostasis. Thefindings that fasting glucose was higher and rose to a higher
Magnesium Deficiency in Postmenopausal Women
130 VOL. 26, NO. 2

concentration suggest impaired glucose disposal and possibledecreased insulin sensitivity during magnesium deprivation.This would be in agreement with findings that indicate intra-cellular magnesium concentration modulates insulin action andoxidative glucose metabolism, and epidemiological studiesshowing that higher daily intakes of magnesium are associatedwith a lower incidence of noninsulin-dependent diabetes mel-litus [40]. The reason for the apparent difference in the gluca-gon response during the IVGTT test is unclear. The differencemay be reflecting a response to an acute rise is the circulatingconcentration of glucose because the fasting concentration wasnot significantly different during magnesium deprivation andrepletion. The finding of no fasting difference is similar to thatof Paolisso et al [41] who found that the plasma glucagonconcentration did not increase with magnesium supplementa-tion that increased erythrocyte magnesium in elderly diabeticpatients. The major target organ for glucagon is the liver, whereit stimulates glycogen breakdown to glucose. In the liver,glucagon also binds to specific receptors and increases bothintracellular adenosine 3�, 5�-monophosphate and calcium.Glucagon also is involved in magnesium conservation at thekidney level [42]. Perhaps glucose infusion induces a change inmagnesium distribution, or the lack of magnesium results in achange in the cellular membrane response to glucagon thatresults in a different glucagon secretion with an acute rise incirculating glucose.
CONCLUSION
Findings were obtained that indicate magnesium balancemay be a suitable method for determining whether subjects arebeing depleted of magnesium when fed a magnesium restricteddiet under experimental conditions. If magnesium balance be-comes non-positive upon feeding a diet low in magnesium, andpersists for several weeks, it is likely that the subject willbecome magnesium deficient. A highly positive magnesiumbalance upon feeding a magnesium adequate diet after thismagnesium deprivation would be confirmation of a low ordeficient magnesium status. Thus, functional changes seen withsuch balance changes can be considered as signs of primarydietary magnesium deficiency. The present experiment sug-gests that signs of dietary magnesium deficiency may includeheart arrhythmias, impaired glucose homeostasis, and alteredlipid and oxidative metabolism. The study also establishes thatan intake of 4.12 mmol Mg/8.4 MJ (100 mg Mg/2000 kcal) isinadequate for postmenopausal women. Because 10% of theelderly women in the United States consume less than 5.6mmol (136 mg) Mg/d, magnesium deficiency may be a signif-icant factor compromising cardiovascular health and glycemiccontrol in this population.
ACKNOWLEDGMENT
The author expresses gratitude to the members of the GrandForks Human Nutrition Research Center clinical staff whosespecial talents and skills made this study possible: James Pen-land (psychology), Henry Lukaski (exercise physiology),Loanne Mullen and staff (dietary), Sandra Gallagher and staff(clinical chemistry), Betty Vetter and nursing staff (metabolicunit care), Donna Neese (protocol processing and scheduling),Nicholas Ralston, Rogers Sims and staff (mineral analysis),LuAnn Johnson (statistical analysis), and Christine Bogenreif(manuscript processing).
REFERENCES
1. Eibl N, Schernthaner G: Clinical relevance of hypomagnesaemia indiabetes mellitus: a review. In Smetana R (ed): “Advances inMagnesium Research: Magnesium in Cardiology: Proceedings ofthe 5th European Congress on Magnesium.” London: John Libbey& Company, pp 151–163, 1997.
2. Sanders GT, Huijgen HJ, Sanders R: Magnesium in disease: areview with special emphasis on the serum ionized magnesium.Clin Chem Lab Med 37:1011–1033, 1999.
3. Nadler JL, Buchanan T, Natarajan R, Antonipillai I, Bergman R,Rude R: Magnesium deficiency produces insulin resistance andincreased thromboxane synthesis. Hypertension 21:1024–1029,1993.
4. Paolisso G, Sgambato S, Gambardella A, Pizza G, Tesauro P,Varricchio M, D’Onofrio F: Daily magnesium supplements im-prove glucose handling in elderly subjects. Am J Clin Nutr 55:1161–1167, 1992.
5. Castillo MJ, Meludu SC, Scheen AJ, Lefebvre PJ: Effect of anacute oral load of magnesium on blood glucose and plasma insulinlevels in healthy subjects. In Smetana R (ed): “Advances in Mag-nesium Research: Magnesium in Cardiology: Proceedings of the5th European Congress on Magnesium.” London: John Libbey &Company, pp 197–203, 1997.
6. Seelig MS, Heggtveit HA: Magnesium interrelationships in isch-emic heart disease: a review. Am J Clin Nutr 27:59–79, 1974.
7. Altura BM, Altura BT: Magnesium metabolism, atherogenesis andcardiovascular pathology. In Smetana R (ed): “Advances in Mag-nesium Research: Magnesium in Cardiology: Proceedings of the5th European Congress on Magnesium.” London: John Libbey &Company, pp 28–37, 1997.
8. Rayssiguier Y: Magnesium and lipid metabolism. In Sigel H, SigelA (eds): “Metal Ions in Biological Systems, Vol 26, Compendiumon Magnesium and Its Role in Biology, Nutrition and Physiology.”New York: Marcel Dekker, pp 341–358, 1990.
9. Nielsen FH: The alteration of magnesium, calcium and phosphorusmetabolism by dietary magnesium deprivation in postmenopausalwomen is not affected by dietary boron deprivation. MagnesiumRes 17:197–210, 2004.
10. Klevay L, Milne DB: Low dietary magnesium increases supraven-tricular ectopy. Am J Clin Nutr 75:550–554, 2002.
11. Dacey MJ: Hypomagnesemic disorders. Crit Care Clinics 17:155–173, 2001.
Magnesium Deficiency in Postmenopausal Women
JOURNAL OF THE AMERICAN COLLEGE OF NUTRITION 131
12. Douban S, Brodsky MA, Whang DD, Whang R: Significance ofmagnesium in congestive heart failure. Am Heart J 132:664–671,1996.
13. Ledingham JG, Raine AE: The treatment of heart failure: diuretics.In Weatherall DJ, Ledingham JD, Warrell DA (eds): “OxfordTextbook of Medicine, 3rd edition.” New York: Oxford UniversityPress, pp 2238–2241, 1996.
14. Schroll A: Importance of magnesium for the electrolyte homeosta-sis—an overview. In Smetana R (ed): “Advances in MagnesiumResearch: Magnesium in Cardiology: Proceedings of the 5th Eu-ropean Congress on Magnesium.” London: John Libbey & Com-pany, pp 463–472, 1997.
15. Whang R, Ryder KW: Ionic disturbances in hospital practice. Thecase for magnesium. In Lasserre B, Durlach J (eds): “Magne-sium—A Relevant Ion.” London: John Libbey, pp 257–264, 1991.
16. FAO/WHO Expert Consultation: Magnesium. In: “Human Vita-min and Mineral Requirements.” Geneva: Food and AgricultureOrganization/World Health Organization, pp 223–233, 2002.
17. Durlach J: “Magnesium in Clinical Practice.” London: JohnLibbey Eurotext 1988.
18. Seelig M: Epidemiologic data on magnesium deficiency-associated cardiovascular disease and osteoporosis: considerationof risks of current recommendations for high calcium intakes. InRayssiguier Y, Mazur A, Durlach, J (eds): “Advances in Magne-sium Research: Nutrition and Health.” Eastleigh: John Libbey, pp177–190, 2001.
19. Resnick L, Gupta RK, Laragh JH: Intracellular free magnesium inerythrocytes of essential hypertension: relation to blood pressureand serum divalent cations. Proc Natl Acad Sci USA 81:6511–6515, 1984.
20. Food and Nutrition Board: “Recommended Dietary Allowances,”10th edition. Washington, DC: National Academy Press, 1989.
21. Food and Nutrition Board, Institute of Medicine: “Dietary Refer-ences Intakes for Calcium, Phosphorus, Magnesium, Vitamin D,and Fluoride.” Washington, DC: National Academy Press, 1997.
22. Harris JA, Benedict FG: “A Biometric Study of Basal Metabolismin Men” Carnegie Publication No. 279. Philadelphia: JB Lippin-cott, 1919.
23. Sims RL, Mullen LM, Milne DB: Application of inductivelycoupled plasma emission spectroscopy to multielement analysis offoodstuffs used in metabolic studies. J Food Comp Anal 3:27–37,1990.
24. Analytical Methods Committee: Methods of destruction of organicmatter. Analyst 85:643–656, 1960.
25. Dodge JT, Mitchell C, Hanahan DJ: The preparation and chemicalcharacteristics of hemoglobin-free ghosts of human erythrocytes.Arch Biochem Biophys 100:119–130, 1963.
26. Friedewald WT, Levy RI, Fredrickson DS: Estimation of theconcentration of low-density lipoprotein cholesterol in plasma,without use of the preparative ultracentrifuge. Clin Chem 18:499–502, 1972.
27. Winterbourne CC, Hawkins RE, Brian M, Carroll RW: The esti-mation of red cell superoxide dismutase activity. J Lab Clin Med85:337–341, 1975.
28. Rude RK: Physiology of magnesium metabolism and the importantrole of magnesium in potassium deficiency. Am J Cardiol 63:31G–34G, 1989.
29. Sabatier M, Keyes WR, Pont F, Arnaud MJ: Comparison ofstable-isotope-tracer methods for the determination of magnesiumabsorption. Am J Clin Nutr 77:1206–1212, 2003.
30. Lukaski HC, Nielsen FH: Dietary magnesium depletion affectsmetabolic responses during submaximal exercise in postmeno-pausal women. J Nutr 132:930–935, 2002.
31. Saito N, Konishi Y: Serum and erythrocyte magnesium in outpa-tients with maturity onset diseases. In Halpern MJ, Durlach J (eds):“Current Research in Magnesium.” London: John Libbey & Com-pany, pp 323–326, 1996.
32. Barbagallo M, Gupta RK, Dominguez LJ, Resnick LM: Cellularionic alterations with age: relation to hypertension and diabetes.J Am Geriatr Soc 48:1111–1116, 2000.
33. Feyertag J, Laimer H, Herglotz P, Douglas T, Ekmekcioglu C,Bottcher E, Marktl W: Effect of low dose oral magnesium supple-mentation on different magnesium parameters and on ventriculararrhythmias. In Smetana R (ed): “Advances in Magnesium Re-search: Magnesium in Cardiology: Proceedings of the 5th Euro-pean Congress on Magnesium,” London: John Libbey & Com-pany, pp 71–77, 1997.
34. Altura BM, Altura BT: Magnesium and the cardiovascular system:experimental and clinical aspects updated. In Sigel H, Sigel A(eds): “Metal Ions in Biological Systems, Vol. 26, Compendium onMagnesium and Its Role in Biology, Nutrition, and Physiology.”New York: Marcel Dekker, pp 359–416, 1990.
35. Shils ME: Experimental human magnesium depletion. Medicine48:61–85, 1969.
36. Ryan MP, Whang R: Interrelationships between potassium andmagnesium. In Whang R, Aikawa JK (eds): “Potassium: Its Bio-logic Significance,” Boca Raton: CRC Press, pp 97–107, 1983.
37. Veiga L, Ferreira A, Moreira H, Monteiro CP, Goncalves A,Sardinha L, Bicho M, Laires MJ: Mg in a group of postmenopausalwomen: influence on some cardiovascular risk factors. In: “11thInternational Symposium on Trace Elements in Man and AnimalsConference Schedule and Abstracts.” Berkeley, CA, p 71, 2002.
38. Sherer Y, Bitzur R, Cohen H, Shaish A, Varon D, Shoenfeld,Harats D: Mechanisms of action of the anti-atherogenic effect ofmagnesium: lessons from a mouse model. Magnesium Res 14:173–179, 2001.
39. Kumar BP, Shivakumar K: Depressed antioxidant defense in ratheart in experimental magnesium deficiency. Implications for thepathogenesis of myocardial lesions. Biol Trace Elem Res 60:139–144, 1997.
40. Barbagallo M, Dominguez LJ, Galioto A, Ferlisi A, Cani C, MalfaL, Pineo A, Busardo A, Paolisso G: Role of magnesium in insulinaction, diabetes and cardiometabolic syndrome X. Mol AspectsMed 24:39–52, 2003.
41. Paolisso G, Scheen A, Cozzolino D, Di Marco G, Varricchio M,D’Onofrio F, Lefebvre PJ: Changes in glucose turnover parametersand improvement of glucose oxidation after 4-week magnesiumadministration in elderly noninsulin-dependent (type II) diabeticpatients. J Clin Endocrin Metab 78:1510–1514, 1994.
42. Dai L-J, Bapty B, Ritchie G, Quamme GA: Glucagon and argininevasopressin stimulate Mg2� uptake in mouse distal convolutedtubule cells. Am J Physiol 274:F328–F335, 1998.
Received June 7, 2005; revision accepted May 4, 2006.
Magnesium Deficiency in Postmenopausal Women
132 VOL. 26, NO. 2





























