Embed Size (px)
Citation preview

REVIEW
Diagnostic Pacing Maneuvers for SupraventricularTachycardias: Part 2GEORGE D. VEENHUYZEN, M.D., F. RUSSELL QUINN, M.R.C.P., PH.D.,STEPHEN B. WILTON, M.D., ROBIN CLEGG, M.D., and L. BRENT MITCHELL, M.D.From the Libin Cardiovascular Institute of Alberta, University of Calgary and Calgary Health Region, Alberta, Canada
The approach to supraventricular tachycardia (SVT) diagnosis can be complex because it involvessynthesizing baseline electrophysiologic features, features of the SVT, and the response(s) to pacingmaneuvers. In this two-part review, we will mainly explore the latter while recognizing that neither ofthe former can be ignored, for they provide the context in which diagnostic pacing maneuvers mustbe correctly chosen and interpreted. Part 1 involved a detailed consideration of ventricular overdrivepacing, since this pacing maneuver provides the diagnosis in the majority of cases. In Part 2, otherdiagnostic pacing maneuvers that might be helpful when ventricular overdrive pacing is not diagnostic orappropriate, including attempts to reset SVT with single atrial or ventricular beats, para-Hisian pacing,apex versus base pacing, and atrial overdrive pacing, are discussed, as are some specific diagnostic SVTchallenges encountered in the electrophysiology lab. There is considerable literature on this topic, andthis review is by no means meant to be all-encompassing. Rather, we hope to clearly explain and illustratethe physiology, strengths, and weaknesses of what we consider to be the most important and commonlyemployed diagnostic pacing maneuvers, that is, those that trainees in cardiac electrophysiology shouldbe well familiar with at a minimum. (PACE 2012; 35:757–769)
ablation, electrophysiology - clinical, SVT, pacing
In part 1 of this review on diagnostic pac-ing maneuvers for supraventricular tachycardia(SVT), we explored ventricular overdrive pacing(VOP) in detail, since it provides a firm SVTdiagnosis in the majority of cases.1 We will nowconsider pacing maneuvers that can be performedwhen VOP is not diagnostic, including ones thatcan be performed when sustained, regular SVTcannot be induced. These will include single-paced ventricular beats during ongoing SVT, para-Hisian pacing, and apex versus base pacing.We will also explore some challenging specificsituations in SVT diagnosis including differen-tiating atrioventricular node reentry tachycardia(AVNRT) from atrial tachycardia (AT) and junc-tional tachycardia (JT), SVT with atrioventricular(AV) dissociation, and differentiating AVNRTwith a leftward atrionodal exit from orthodromicatrioventricular reciprocating tachycardia (AVRT)employing a left-sided accessory pathway (AP).
Address for reprints: George D. Veenhuyzen, M.D., F.R.C.P.C.,Libin Cardiovascular Institute of Alberta, University of Calgaryand Calgary Health Region, Foothills Medical Centre, Rm C836,1403-29 St. N.W., Calgary, Alberta, T2N 2T9, Canada. Fax: 403-944-1592; e-mail: [email protected]
Received September 19, 2011; revised December 22, 2011;accepted January 5, 2012.
doi: 10.1111/j.1540-8159.2012.03352.x
Scanning diastole with ventricular prematurebeats (VPBs)
Single VPB introduced decrementally duringdiastole in SVT offer an opportunity to determinethe relationship between altered timing of ven-tricular depolarization and the timing of atrialdepolarization. For example, if a VPB is able toterminate tachycardia without atrial depolariza-tion, then AT can be excluded, provided thisis not a coincidence. Furthermore, VPBs thatoccur during SVT at a time when the stimulatedwavefront would be expected to collide with theSVT wavefront in the His-Purkinje network orin ventricular myocardium cannot possibly affectatrial timing during either AVNRT or AT (unless abystander AP is present). Accordingly, such His-refractory VPBs (HRVPBs) should only be capableof affecting AVRT circuits (again, in the absenceof a bystander AP). VPBs that occur before Hisbundle refractoriness are potentially capable ofaffecting atrial timing (including terminating SVT)in any of AT, AVNRT, or AVRT.
How does one determine if a paced VPB isHis-refractory? If the QRS complex morphologyof the VPB shows evidence of fusion (i.e., theQRS complex morphology of the VPB shows somefeatures of the QRS complex morphology of apaced VPB and some features of the QRS complexmorphology of the SVT), then the paced VPB mustbe His-refractory, since the SVT wavefront that the
C©2012, The Authors. Journal compilation C©2012 Wiley Periodicals, Inc.
PACE, Vol. 35 June 2012 757
VEENHUYZEN, ET AL.
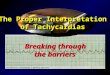
Figure 1. Advancement of atrial activation by a fusedHis-refractory ventricular premature beat (HRVPB).Panel A: During supraventricular tachycardia with astable cycle length of 444 ms, one-to-one atrioven-tricular relationship, and an earlier atrial electrogramrecorded in the right atrium (where the ablationcatheter, ABLp/d, is located) than in the septum(d/pHIS) or coronary sinus (proximal CS 9,10 throughdistal CS 1,2), a paced premature beat is deliveredby electrodes at the right ventricular apex (RVd). Thesubsequent atrial activation is advanced by 19 ms.The paced premature ventricular beat is His-refractory(HRVPB) because (1) it is fused: note QRS complexmorphology features and duration (122 ms) that areintermediate between those of the conducted SVT(narrow complex) and of a purely paced QRS complex(Panel B, QRS complex duration = 144 ms) and (2) thepacing stimulus is delivered at precisely the time ofthe expected His bundle potential (arrow). A ventricularpaced beat can be considered His-refractory if it occursup to 35–55 ms earlier than the anticipated His bundlepotential. Advancement of atrial activation without achange in the atrial activation sequence by an HRVPBindicates that an accessory pathway (AP) is present andalmost certainly participating in orthodromic AVRT, inthis case, employing a right-sided AP.
stimulated wavefront is fusing with in ventricularmyocardium must have exited the His-Purkinjenetwork (Fig. 1). If the pacing stimulus occursjust after a discernible antegrade His potential,then the paced VPB is obviously His-refractory.Finally, if the paced VPB occurs no more than35–55 ms earlier than the anticipated timing ofthe antegrade His potential, in the time that wouldbe required for that stimulated wavefront to enterthe distal arborization of the His-Purkinje networkand travel retrogradely to the His bundle, thetachycardia wavefront would have reached the Hisbundle where these wavefronts would collide.2When the paced VPB occurs more than 35–55 ms
earlier than the anticipated timing of the antegradeHis potential, it would not be considered to beHis-refractory, but rather, prior to His bundlerefractoriness.
There are three responses to an HRVPB thatare diagnostically useful:
(1) SVT terminates without conduction tothe atrium. This response indicates a diagnosisof AVRT, provided that this event is not acoincidence, as could be the case if the SVTfrequently spontaneously terminates. The fact thatan HRVPB can affect the SVT indicates that an APis present, and the fact that the SVT terminateswith ventriculoatrial (VA) block indicates thatventricular and atrial activation must be linkedso that if conduction to the atrium does notoccur via the AP, the circuit is interrupted.This cannot be the case with AT or AVNRT,even if a bystander AV AP is present. That is,the AP must also be participating in the SVTmechanism. Theoretically, this response could beobserved given the coexistence of AVNRT and abystander nodoventricular AP, but this occurrencehas not been convincingly demonstrated to ourknowledge, and would have to be extremely rare.
As we discussed in Part 1, sometimes VOPresults in an apparently noninterpretable responsewhen VOP repeatedly terminates the SVT. VOPmay be considered as a series of consecutiveVPBs. When the SVT repeatedly stops duringVOP because of VA block, if the paced beat thatprecedes VA block is His-refractory, and the atrialtiming has not changed prior to that VPB, thisconstitutes an equivalent of an HRVPB terminatingSVT without conduction to the atrium, therebyestablishing a diagnosis of AVRT (see “What if theresponse to VOP is not interpretable?” in Part I).
(2) Atrial activation is delayed without achange in the atrial activation sequence. Thisresponse indicates a diagnosis of AVRT employinga decremental AP (Fig. 2). As above, the factthat an HRVPB can affect the SVT indicatesthat an AP is present and delay of atrial timingindicates that atrial activation is decrementallylinked to ventricular activation. This cannot bethe case with either AT or AVNRT even if abystander AV AP is present; the decremental APmust also be participating in the SVT mechanism.Note that for this response to be appreciated,the degree of decremental conduction slowingmust exceed the prematurity of the HRVPB; ifthey are matched, AVRT employing a decrementalAP could be present but because no change inatrial timing would occur, one would concludethat the VPB had no effect on the SVT and thediagnosis could be missed. Accordingly, it isworth studying the effects of multiple HRVPBs
758 June 2012 PACE, Vol. 35
DIAGNOSTIC SVT PACING MANEUVERS 2
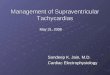
Figure 2. Delay of atrial activation by a His-refractoryventricular premature beat (HRVPB). During a long R-Pinterval supraventricular tachycardia with a stable cyclelength of 473 ms, a paced premature beat is delivered byelectrodes at the right ventricle. The subsequent atrialactivation is delayed by 20 ms without a change inthe atrial activation sequence. The paced prematureventricular beat is His-refractory because it occursvirtually simultaneously with and certainly not morethan 35–55 ms earlier than the expected inscriptionof the anterograde His bundle potential (arrow). Thisresponse indicates that an accessory pathway (AP) ispresent and participating in orthodromic AVRT, in thiscase, employing a slowly conducting concealed septalAP. (Tracing courtesy of Dr. G. Neal Kay.)
introduced throughout the His-refractory diastolicwindow to minimize this potential pitfall ofstudying only one HRVPB that had no apparenteffect. Theoretically, delayed atrial timing after anHRVPB could be observed in the setting of AVNRTwith a bystander nodoventricular AP.3 This isso rare that delay of atrial timing by an HRVPBwithout a change in the atrial activation sequenceshould be considered extremely strong evidencethat the SVT mechanism is AVRT employing adecremental AP.
It is often the case that AVRT employing adecremental AP manifests as a long RP intervalSVT. If the AP used for retrograde conductionhas decremental conduction properties, entrain-ment by VOP could be associated with longcorrected postpacing interval-tachycardia cyclelength (cPPI-TCL) and stimulus-atrial (SA)-VAinterval values that would normally be consideredevidence of atypical AVNRT. Fusion duringentrainment would still provide proof that themechanism is AVRT but, if fusion is not present,it is important to scan diastole with VPBs during
long RP interval SVTs, even if entrainment byVOP is associated with long cPPI-TCL and SA-VA interval values. In such a situation, the findingthat an HRVPB delays atrial timing (indicatinga diagnosis of AVRT, Fig. 2) has a greaterdiagnostic value than the finding of long cPPI-TCLor SA-VA interval values (suggesting a diagnosisof AVNRT).
Application of this maneuver requires thatany apparent delay in atrial timing exceeds thespontaneous variability in the SVT cycle length(CL). Accordingly, this maneuver may not bereliable in irregular SVTs.
(3) Atrial activation is advanced without achange in the atrial activation sequence. The factthat an HRVPB can affect atrial timing indicatesthat an AP is present. If the atrial activationsequence is unaltered, one can conclude withconfidence, but not with certainty, that the AP isparticipating in the SVT mechanism, establishinga diagnosis of AVRT (Fig. 1). Theoretically, ATor AVNRT could be advanced by conductionover a bystander AP, and if the bystander APwere close to the AT origin or atrionodal exit,respectively, the atrial activation sequence maynot change appreciably. This situation is so rarethat this finding is considered very strong evidence(but not proof) that the SVT mechanism isAVRT.
As before, application of this maneuverrequires that any apparent change in atrial timingexceeds the degree of spontaneous variability inthe SVT CL. Accordingly, this maneuver may notbe reliable in irregular SVTs.
Unfortunately, while these responses toHRVPBs are specific (or, in the third case, nearlyspecific) for AVRT, they are not particularlysensitive. If the pacing site is far from theparticipating AP, the orthodromic wavefront of theVPB may not have had enough time to reach the APand affect the AVRT circuit when delivered lateenough to be His-refractory. The classic situationin which an HRVPB delivered from the rightventricular (RV) apex does not affect an AVRTcircuit because of the distance of the RV apex tothe AP occurs when a left free wall AP is operative;nevertheless, this problem may arise when arelatively nearby septal AP is involved.4 As is thecase with fusion during VOP, the sensitivity of thethree responses to HRVPBs described earlier canbe increased by moving the pacing site close tothe AP, that is, to a basal ventricular site closeto the site of earliest atrial activation. This is notsurprising, since fusion during VOP constitutesthe continuous resetting of an AVRT circuit bya series of consecutive HRVPBs; the fact that theyare fused proves that they are His-refractory, asdiscussed earlier.
PACE, Vol. 35 June 2012 759
VEENHUYZEN, ET AL.
It is commonly taught that if none of thethree responses to HRVPBs described earlieris observed, no conclusion regarding the SVTmechanism can be drawn. However, it has beensuggested that, in the case of a short RP intervalSVT, advancing the local ventricular activationadjacent to the earliest atrial activation by morethan 30 ms without affecting atrial timing shouldexclude the participation of a conventional APfrom the SVT mechanism.5 Similarly, in the caseof a long RP interval SVT, advancing the localventricular activation adjacent to the earliest atrialactivation by more than 60 ms without affectingatrial timing should exclude the participation of adecremental AP from the SVT mechanism.5
Regarding the HRVPB maneuver, one pointseems to be underappreciated: if an SVT thatresembles typical AVNRT is induced (centralatrial activation and septal VA < 70 ms),this maneuver will not add further diagnosticinformation as it cannot distinguish AVNRT fromAT (see one exception for this in the section onAV-dissociated SVT). If the diagnosis is not clearfrom findings during spontaneous perturbations inthe SVT, the pacing maneuver of choice in thissituation is VOP.
Para-Hisian & Pure-Hisian Pacing
The pacing maneuvers described earlierrely on studying the response to an inducedperturbation (VOP or single premature beats) ofa stable tachycardia. However, it is commonto encounter SVTs that are difficult to induce,nonsustained, irregular, or repeatedly terminateduring pacing protocols. Such circumstances mayprevent diagnostic pacing maneuvers from beingperformed, or can limit interpretation of theirresults.
In a patient with documented SVT, butno preexcitation on their baseline ECG, one ofthe goals at an electrophysiologic study is todetermine the presence or absence of a concealedAP. Sometimes programmed stimulation from theRV apex (or even catheter-induced PVCs) canquickly give a clue: if the atrial activation sequenceis clearly “eccentric” (either right or left free wall),then an AP is very likely to be present. Furthercharacterization of the conduction propertieswill be required to be more certain, but withlittle effort, something of interest will have beendiscovered and further investigations can bedirected accordingly. A CS catheter is commonlyplaced at the start of an electrophysiology study, sothis works well for detecting nonseptal left-sidedAPs, which account for around 50% of all APs.6
The remainder of APs can be harder todetect by this method. With “standard” catheterpositions there is not usually a catheter recording
from sites all around the tricuspid annulus, soboth septal and right free wall APs, as well asretrograde AV nodal conduction, can show earliestatrial activation on the His catheter or at theproximal CS. Another pacing maneuver—para-Hisian pacing—can be useful in these circum-stances.7 The basic concept is simple—pacingis performed next to the His bundle/proximalright bundle (HB-RB) and the response is studiedwhen the HB-RB and adjacent myocardium arecaptured, versus when local myocardium aloneis captured. This is usually achieved by varyingthe pacing output and examining the surfaceQRS duration and, where possible, the stimulus-His (SH) interval. HB-RB capture will producea narrow QRS complex and short SH interval,whereas loss of HB-RB capture will produce awider QRS complex and lengthening of the SHinterval. In the latter circumstance, the His bundlewill only be activated after excitation has traveledthrough ventricular myocardium, penetrated thedistal Purkinje network, and traveled retrogradelythrough the conduction system. Often, with HB-RB capture, the His potential is difficult to discern(particularly when a single catheter is used forpacing and recording), either due to saturation ofthe His channel by the pacing stimulus, or maskingby the local ventricular potential. Appearance of aclear retrograde His potential, however, is usuallyan indication that HB-RB capture has been lost.
We can now consider the response (timingand pattern of retrograde atrial activation) in theabsence and presence of an AP (Fig. 3). If AV nodalconduction alone is present then loss of HB-RBcapture will cause a lengthening of the stimulus-atrial (SA) interval (because excitation has a longerpath to travel back to the atrium), without achange in the atrial activation sequence. Thechange in SA interval should match the changein the SH interval, when this can be measured,and the His-atrial (HA) interval should be thesame. If AP conduction alone is responsible forretrograde atrial activation (i.e. no VA conductionis present through the AV node), then loss ofHB-RB capture should have little or no effect onthe SA interval and no change in the patternof atrial activation. The SH interval will stilllengthen when HB-RB capture is lost, thus the HAinterval will shorten, since atrial timing dependsonly on conduction over the AP. When both AVnodal and AP conduction is present then a morecomplex response may be obtained, depending onthe proximity of the AP to the pacing site andthe conduction properties of the AP and the AVnode/conduction system. Generally, a change inthe retrograde atrial activation sequence shouldbe seen, although this will depend on how muchof the atrium is activated via the AP versus the
760 June 2012 PACE, Vol. 35
DIAGNOSTIC SVT PACING MANEUVERS 2
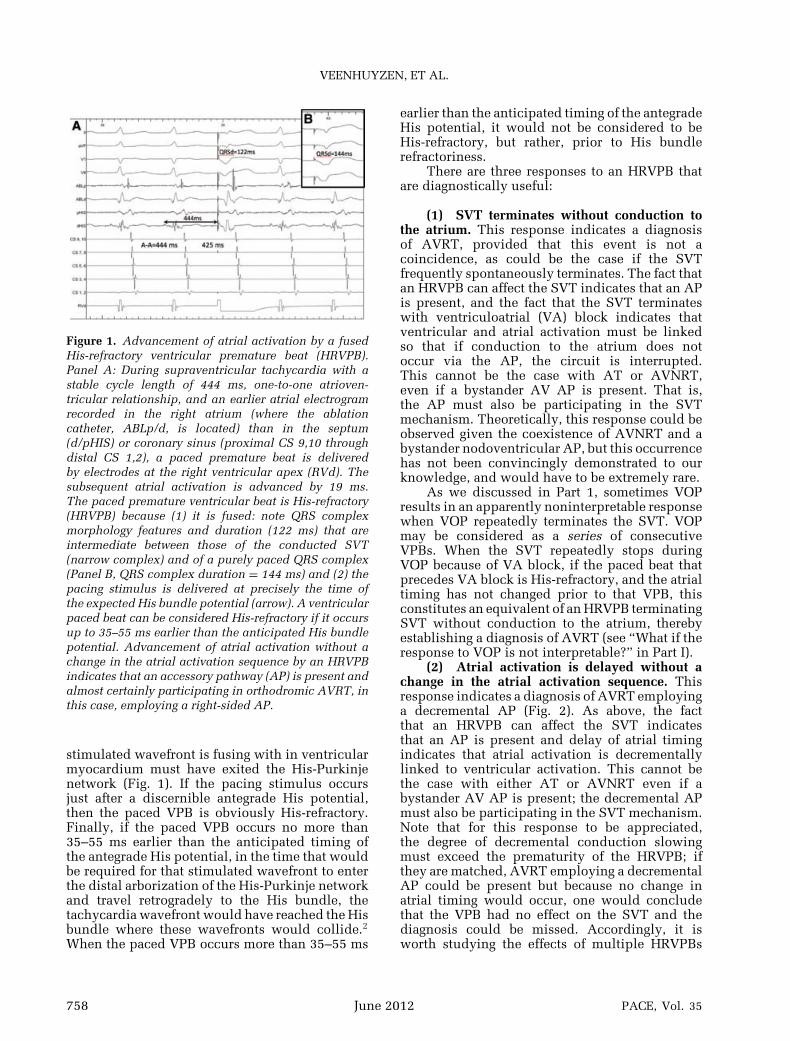
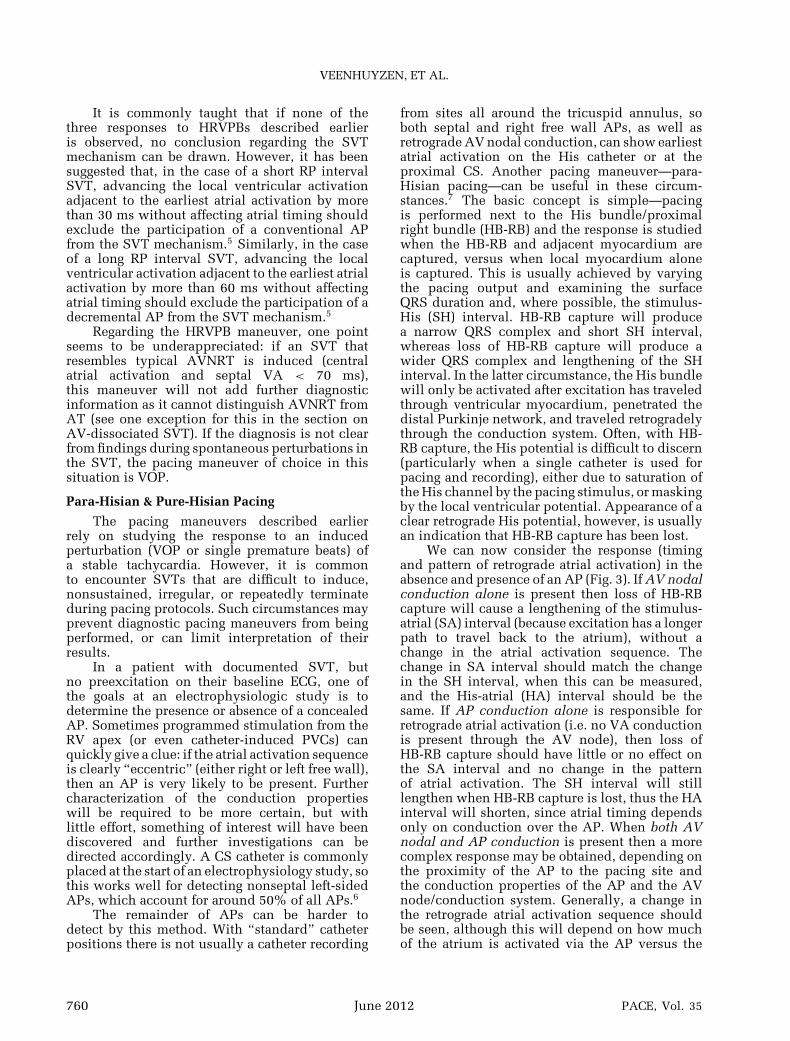
Figure 3. Responses to para-Hisian pacing. In bothpanels, pacing is being performed from the distal polesof the His catheter (dHis). The first beat in eachpanel captures the His bundle and local ventricularmyocardium (narrow QRS complex), whereas thesecond beat loses His capture and only stimulates ven-tricular myocardium. Panel A shows the response whenretrograde conduction is occurring over a concealedaccessory pathway; with loss of His capture there isno change in the SA interval (the time from stimulus[dotted line] to earliest atrial activation [dashed line]),nor is there a change in the atrial activation sequence.In this case, a right para-Hisian pathway was present,with earliest atrial activation on the HRA catheter. PanelB shows the response after successful ablation of theaccessory pathway, demonstrating the response whenpurely AV nodal retrograde conduction is present. Withloss of His capture the SA interval extends by 61 mssince the stimulated wavefront must now travel throughventricular myocardium, penetrate the distal branchesof the His-Purkinje system, then travel retrogradelythrough the AV node. Earliest atrial activation is tiedbetween the proximal bipole of the His catheter (pHis)and the CS os (CS 9–10). HRA = high right atrium; CS =coronary sinus; RVA = right ventricular apex; QRSd =QRS complex duration (ms); SA = time from stimulusto atrial electrogram (ms).
AV node, relative to the position of the recordingsites in the atrium (i.e. where fusion is occurringin the atrium in each case). Demonstrating thischange is facilitated by having a catheter closeto the site of earliest retrograde atrial activation(i.e. some additional mapping in the atrium maybe required). If the AP is close enough to thepacing site and has sufficiently rapid conductionthen the SA interval should remain the same withloss of HB-RB capture, but there will be a changein the atrial activation sequence. For example, ifa posteroseptal AP is present then loss of HB-RB capture may lead to a similar SA interval on
proximal poles of the CS catheter but some delayin atrial timing on the His catheter.
Pitfalls
(1) APs distant from the pacing site: Inter-pretation of the response to para-Hisian pacing hasbeen shown to be reliable for septal and right freewall APs, but can be misleading for left lateral APs.In the latter case, the pathway may be so far fromthe pacing site that the atria are entirely activatedvia the AV node whether the HB-RB is captured ornot (assuming AV nodal conduction is sufficientlyrapid). However, as previously mentioned, aneccentric atrial activation sequence may be clearlyapparent for left-sided APs simply with RV apicalpacing or programmed stimulation.
(2) Slowly-conducting APs: Similarly, ifconduction over an AP is slow relative to AVnodal conduction then the response to para-Hisianpacing may falsely suggest AV nodal conductionalone.7,8
(3) Lack of ventricular capture during HB-RB pacing: Occasionally, pure-Hisian pacing canoccur, without capture of the local ventricularmyocardium (sometimes called “reverse para-Hisian pacing”). This phenomenon is usuallytransient, but can be associated with changes inthe QRS duration and if not recognized can leadto a misinterpretation of the response. If it isrecognized, then the response can be analyzed andcan also give diagnostic information.9
(4) Presence of a fasciculoventricular con-nection: These rare pathways connect the prox-imal conduction system to basal septal my-ocardium and, if present, can prevent low outputpacing from capturing myocardium alone; evenwith loss of direct His bundle capture, excitationcan still reach the conduction system so littlechange in QRS duration may be seen.10
(5) Loss of capture of the proximal leftbundle branch alone: This can cause QRSwidening without loss of retrograde conductionto the AV node and if not recognized could lead tomisinterpretation of the response.11
(6) Inadvertent atrial capture: This can givethe impression that retrograde conduction is viathe AV node when a septal AP is present, andit can also give the impression that retrogradeconduction is via a septal AP when no such APis present. Atrial capture is best identified bynoting a change in atrial timing when adjustingthe catheter basally (to deliberately capture theatrium and reduce the interval from the pacingstimulus to a septal atrial electrogram) or apically(to deliberately lose capture of the atrium andprolong the interval from the pacing stimulusto a septal atrial electrogram by more than
PACE, Vol. 35 June 2012 761
VEENHUYZEN, ET AL.
20 ms).12 Aditionally, it seems that when theinterval from the pacing stimulus to the atrial elec-trogram recorded by the proximal CS electrodesis < 60 ms (or < 70 ms to the atrial electrogramrecorded by the high right atrial electrodes), atrialcapture is almost certainly present, and whenthese intervals exceed 90 and 100 ms, respectively,atrial capture is almost certainly not present.12
Another fundamental issue with para-Hisianpacing is that demonstrating the presence of anAP does not prove that it participates in SVT—the maneuver alone cannot distinguish betweenan AP that participates in AVRT from one whichis a bystander. However, in the presence of a stablesustained tachycardia, entrainment pacing canalso be performed from the para-Hisian region andthe response can demonstrate whether an AP ispart of the SVT circuit (para-Hisian entrainment),though the details remain beyond the scope of thisreview.13
Apex versus Base Pacing
Another pacing maneuver that can help todisclose the presence of a retrogradely conductingseptal AP even in the absence of inducible sus-tained SVT is apex versus posterobasal pacing.14
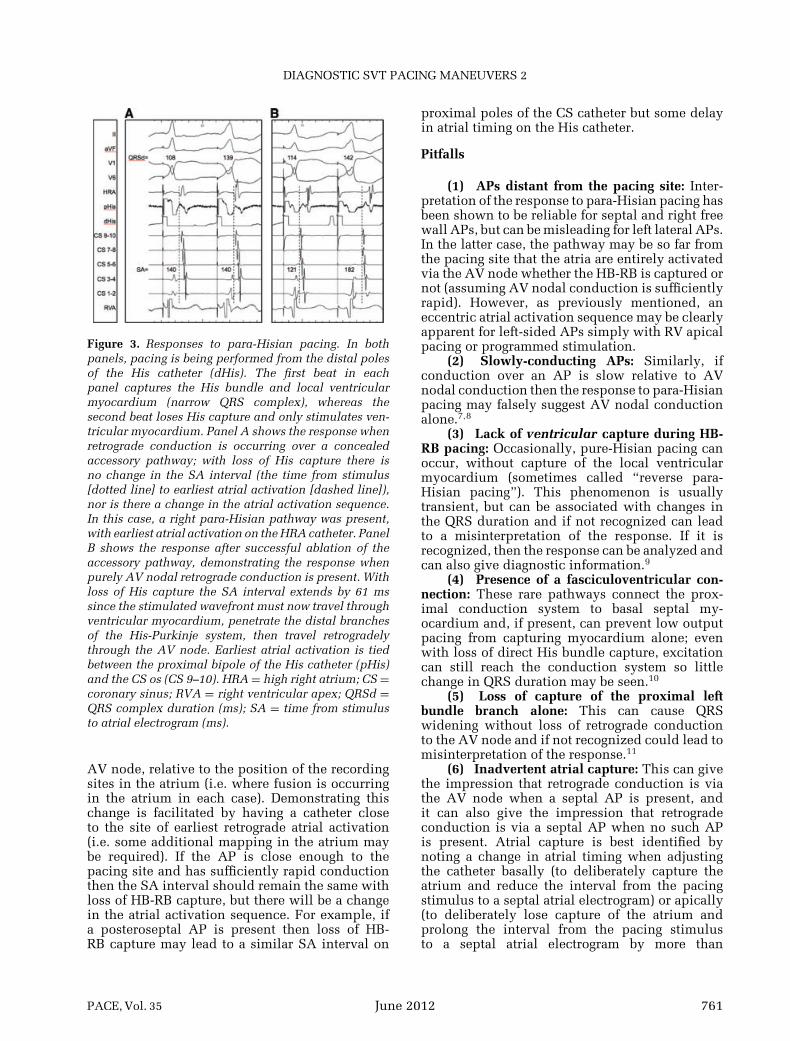
This maneuver is, in our opinion, easier toperform and easier to interpret than para-Hisianpacing. Just like para-Hisian pacing, apex versusposterobasal pacing takes advantage of the shorterVA conduction time expected with VA conductionvia a septal AP during basal pacing than apicalpacing. This maneuver was first described byMartinez-Alday in an elegant study where apicaland right posterobasal pacing were performedeither in sinus rhythm or as VOP during SVTin patients with posteroseptal APs (resulting inentrainment with fusion in the majority of cases)and patients without posteroseptal APs. Care wastaken to avoid atrial capture during pacing at theright posterobasal site.14 The VA index (VAI) wasdefined as the VA interval (measured from thepacing stimulus artifact to a stable reference at thehigh right atrium) after pacing from the RV apexminus the VA interval after pacing from the RVbase (Fig. 4). All patients with a septal AP had apositive VAI. While most patients without septalAPs had negative VAIs, surprisingly, a couple ofpatients without septal APs had VAIs of 0 or +5ms, most likely indicating some anatomic and/orphysiologic heterogeneity in the retrograde inputof the His-Purkine network. Nevertheless, a VAI >10 ms had 100% sensitivity and specificity for aseptal AP in that small study. This discriminatoryvalue is close to the VAI of 0–5 ms observed intwo patients without septal APs, so care should
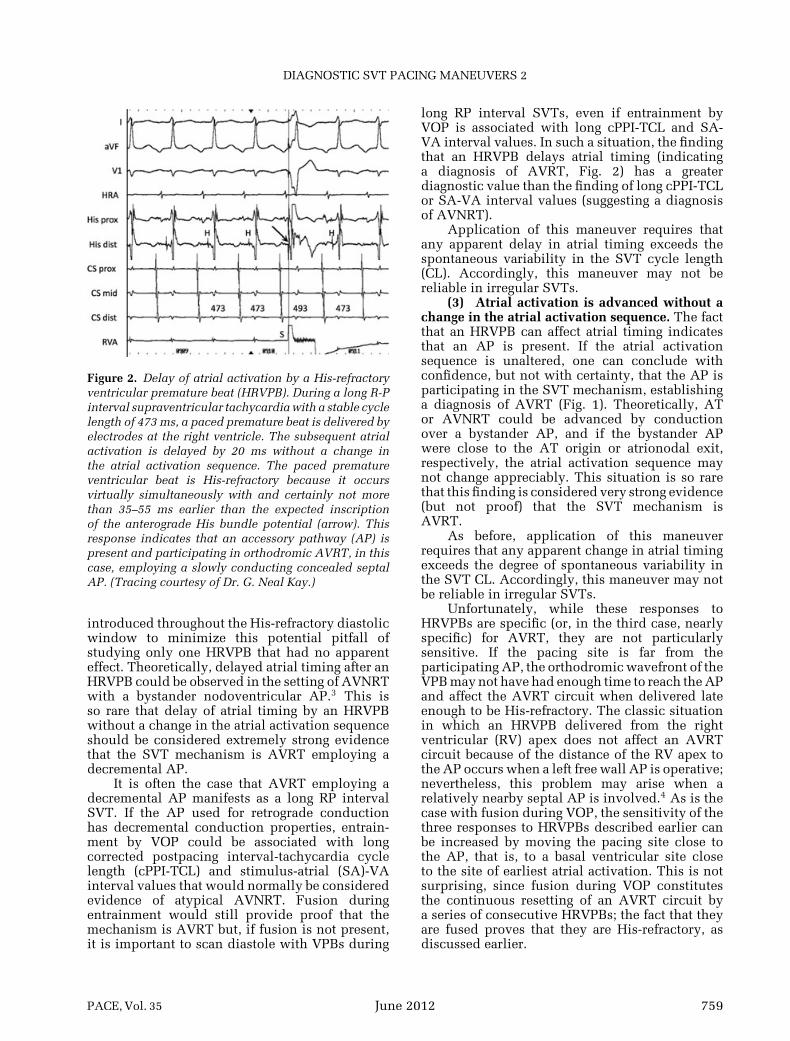
Figure 4. Apex versus base pacing consistent with thepresence of an accessory pathway. Panel A shows rightventricular (RV) apical pacing (note the superior QRScomplex frontal plane axis) with a ventriculoatrial (VA)interval of 142 ms measured from the pacing stimulusto the earliest atrial electrogram recorded by electrodesalong the middle of the coronary sinus catheter (CS1,2 =distal; CS 9,10 = proximal). Panel B shows pacing fromthe basal RV (note the inferior QRS complex frontalplane axis) with a resulting VA interval of 120 ms. Thedifference between these values is the VA Index (+22ms), which is consistent with VA conduction over anaccessory pathway.
probably be taken in reaching firm conclusionsbased on borderline VAI values.
Like para-Hisian pacing, this maneuver canbe limited in the detection of a slowly conductingAP. Also, because retrograde conduction can fuseover an AP and the normal AV conduction system,this maneuver should probably be limited tothe identification of posteroseptal APs. Becausedifferential entrainment (discussed in Part 1 of thisReview) employs the same retrograde pathway asthe tachycardia, this limitation may not apply, anddifferential entrainment certainly did appear to bediagnostically useful in patients with nonseptalAPs.15
AVNRT versus AT
Distinguishing AVNRT from AT is usuallyproblematic when VOP does not acceleratethe atria to the pacing CL (the ventricles aredissociated from the atria) and the SVT has a 1:1AV relationship with central atrial activation. Theability to dissociate the ventricles from the SVTmechanism excludes the participation of an APin the SVT mechanism, but AVNRT must still be
762 June 2012 PACE, Vol. 35

DIAGNOSTIC SVT PACING MANEUVERS 2
distinguished from a septal AT. It is noteworthythat in approximately 80% of such cases, thediagnosis is AT,16 but the AT mechanism is by nomeans proven. Strictly speaking, the VA intervalcannot differentiate septal AT from AVNRT as anyVA interval is possible with either mechanism.Nevertheless, virtually simultaneous atrial andventricular activation, as is observed in typicalAVNRT, has a very high positive predictivevalue for that diagnosis, largely because AVNRTis so much more common than AT (predictiveaccuracy of a test is influenced by prevalence).16
Nevertheless, it is possible for the AV relationshipin a septal AT to coincidentally mimic that oftypical AVNRT.17 Other SVT features that may beuseful to distinguish AVNRT from AT include:
(1) The termination (either spontaneously, orafter a vagal maneuver or adenosine administra-tion) of SVT on a nonpremature atrial electrogramimplies that termination is associated with AVblock. This observation favors AVNRT but couldoccur by coincidence in AT.
(2) Termination of SVT on a nonprematureatrial electrogram by ice-mapping in the region ofthe slow AVN pathway implies that terminationis associated with AV block and also favorsAVNRT.18
(3) Continuation of the SVT despite AV blockfavors AT but AVNRT with AV block (usuallyinfranodal) can occur.
(4) Termination of SVT after a VPB that doesnot conduct to the atrium favors AVNRT but couldoccur by coincidence in AT.
(5) When there are small variations in TCL,if HH or VV interval changes precede and predictAA interval changes (i.e. the HA or VA interval isconstant despite HH or VV interval changes), thena diagnosis of AVNRT can be made.
(6) The apparent requirement of SVT induc-tion upon a “jump” to the AVN slow pathwayfavors AVNRT but does not prove this diagnosis.
(7) An AV Wenckebach CL that exceeds thetachycardia CL favors AVNRT.
In addition to the features described earlier,atrial overdrive pacing (AOP) may be useful inthis situation (Fig. 5). If, after AOP at a CL 10–40ms shorter than the SVT CL, the VA intervalon the first return beat of the entrained SVT iswithin 10 ms of the VA interval of the SVT(“VA linking”), a diagnosis of AVNRT is favored.Linking of atrial and ventricular activation wouldnot be expected in AT.16 Unfortunately, it is notuncommon for the VA interval on the first returnbeat of AVNRT to vary by more than 10 ms (justas it can in the first few beats after the inductionof AVNRT).16 Moreover, on rare occasions, the
appearance of VA linking could occur during anAT by coincidence.16 Accordingly, this findingshould be considered strong evidence, rather thanproof, that the SVT mechanism is AVNRT. Thestrength of that evidence can be increased ifAOP is performed repeatedly and from differentatrial sites, all yielding similar results. Variabilityin the postpacing VA interval after AOP frommultiple distant atrial sites would be expectedin the case of AT because the timing of the firstreturn atrial impulse will depend on the proximityof the pacing site to the AT origin, and not onthe timing of the first return ventricular beat.One small study suggested that first return VAintervals all within 14 ms of each other after“differential AOP” (AOP from two or three atrialsites: right atrial appendage, coronary sinus [CS]os, and distal CS) is consistent with a diagnosis ofAVNRT (or AVRT) while VA interval differencesobtained after differential AOP exceeding 14 ms isconsistent with a diagnosis of septal AT.19
Typical AVNRT versus JT
The only certain way to distinguish typicalAVNRT from JT would be to record from thelimbs of an AVNRT circuit within the AVN anddemonstrate fusion in those recordings duringresetting or entrainment of AVNRT, which wouldnot occur in JT since its mechanism is not reentry.At present, this is not possible. Fortunately,typical AVNRT is both much more common thanJT and is strongly favored when there is otherevidence of dual AVN pathway physiology. Inparticular, AVNRT is strongly favored when theinitiation of SVT appears to require a “jump”to the slow AVN pathway. Nevertheless, not allAVNRTs have demonstrable discontinuities intheir AV nodal refractory curves and JT couldappear to require a critical Atrio-His (AH) intervalfor its initiation by coincidence. An AH responsewould be expected after VOP in the case of eithertachycardia.
AOP is helpful in distinguishing AVNRT fromJT.20 The last atrial paced beat would be expectedto conduct with a long AH interval (slow AVnodal pathway conduction) to the last ventricularelectrogram that is accelerated to the pacing CLbefore SVT resumes (Fig. 5). A prospective studyhas recently confirmed that this is the case.21 Theobvious pitfall for this maneuver would be theexceptional circumstance where JT coexists withdual AVN physiology and where the last pacedbeat conducts to the ventricles via the slow AVNpathway and echoes back to the atria via the fastAVN pathway before JT resumes. As we will see,the coexistence of JT with dual AVN physiology isa common caveat for pacing maneuvers employedto distinguish AVNRT from JT.
PACE, Vol. 35 June 2012 763
VEENHUYZEN, ET AL.
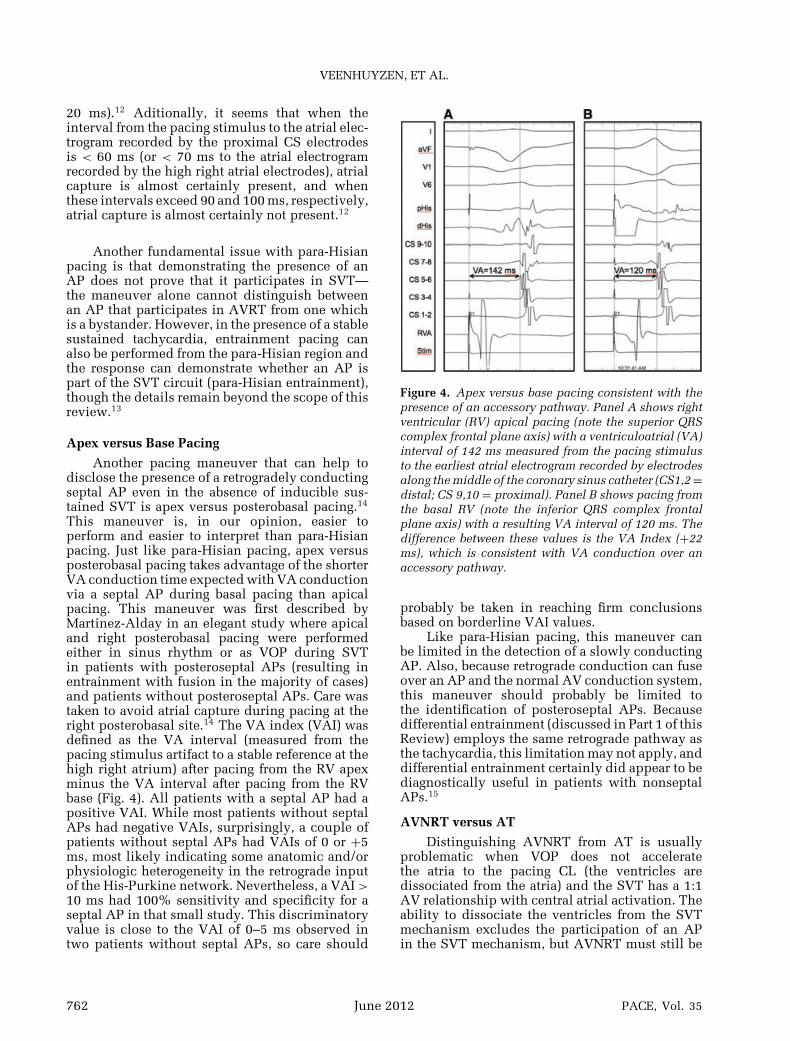
Figure 5. Atrial overdrive pacing to distinguish AVNRT from AT and JT. The termination of high right atrial pacing(from the electrode pair labeled ABLd) at a cycle length of 340 ms during SVT at a CL of 350 ms is shown, revealingthe continuation of SVT after pacing stops. Atrial and ventricular activation during SVT is virtually simultaneous.The star indicates the last entrained His and ventricular electrograms and QRS complex. This beat and subsequentbeats of the SVT demonstrate “VA linking”: the atrial activation sequence and VA interval on the last entrained beatis the same as during the tachycardia, suggesting that ventricular and atrial activation are mechanistically linked,which would not be expected if the diagnosis were atrial tachycardia (AT). During pacing, the PR interval exceeds theRR interval. This is consistent with antegrade conduction over a slow AV node pathway during pacing, which wouldnot be the expected if the diagnosis were junctional tachycardia (JT). The AH interval, including the last entrainedAH interval, is long, and the tachycardia resumes as the last entrained impulse echoes back up the fast AV nodepathway. Again, this would not be expected if the diagnosis were JT.
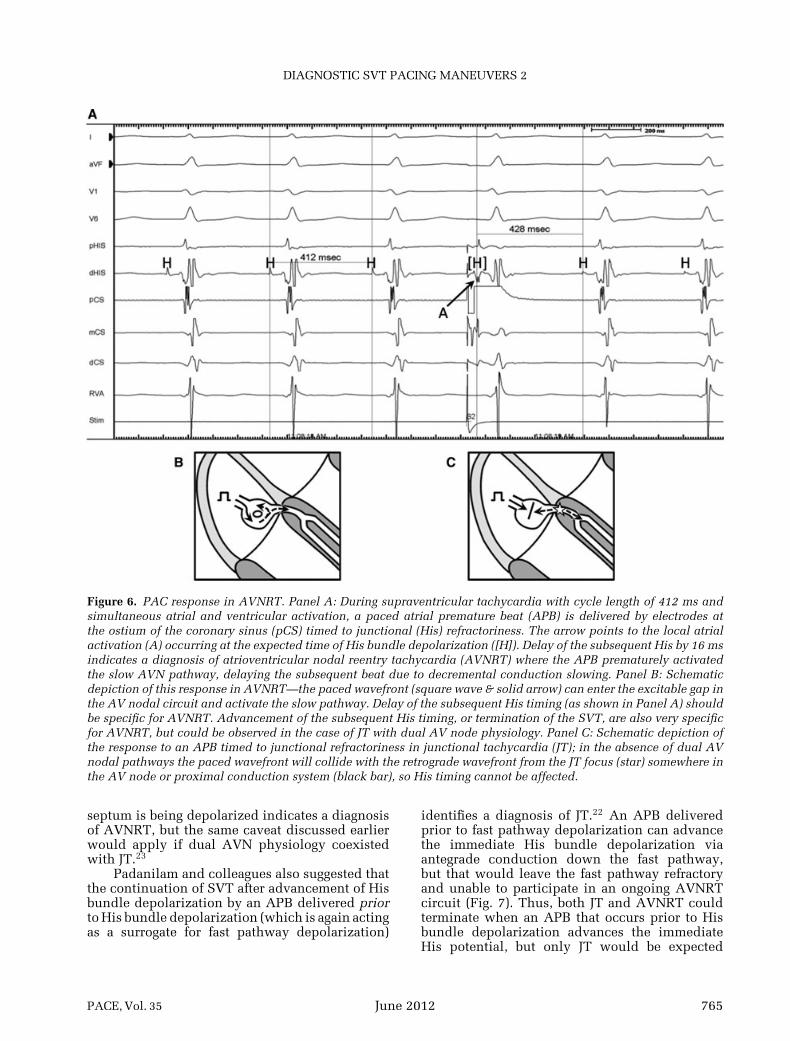
Padanilam and colleagues suggested thatscanning diastole with atrial premature beats(APBs) can often be helpful to distinguish AVNRTfrom JT.22 A His-refractory APB (HRAPB) thataffects the timing of the next His potential inany way (i.e. that advances or delays the nextHis potential, or that terminates the SVT) isconsistent with a diagnosis of AVNRT (Fig. 6).An HRAPB should not be able to reach the AVNfocus of a JT if retrograde conduction from thatfocus proceeds with roughly the same timingas antegrade conduction to the His bundle. Thetiming of His bundle depolarization is actually asurrogate for the timing of retrograde fast AVNpathway conduction. An APB that occurs whenthe fast pathway is refractory cannot affect a
JT focus since the stimulated wavefront wouldcollide with the JT wavefront in or proximal tothe fast AVN pathway. On the other hand, anAPB that occurs when the FP is refractory canaffect an AVNRT circuit by engaging the slow AVNpathway. Accordingly this response is specific forAVNRT. As with AOP, the coexistence of JT withdual AVN physiology represents a caveat since itcould permit an HRAPB to advance (but not delay)the timing of the next His bundle depolarizationif conducted via the slow pathway, leading to anecho beat via the fast pathway, only to have JTresume afterwards. Hamdan and colleagues havesuggested that resetting by an APB delivered closeto the AVN slow pathway region at a time when the
764 June 2012 PACE, Vol. 35
DIAGNOSTIC SVT PACING MANEUVERS 2
Figure 6. PAC response in AVNRT. Panel A: During supraventricular tachycardia with cycle length of 412 ms andsimultaneous atrial and ventricular activation, a paced atrial premature beat (APB) is delivered by electrodes atthe ostium of the coronary sinus (pCS) timed to junctional (His) refractoriness. The arrow points to the local atrialactivation (A) occurring at the expected time of His bundle depolarization ([H]). Delay of the subsequent His by 16 msindicates a diagnosis of atrioventricular nodal reentry tachycardia (AVNRT) where the APB prematurely activatedthe slow AVN pathway, delaying the subsequent beat due to decremental conduction slowing. Panel B: Schematicdepiction of this response in AVNRT—the paced wavefront (square wave & solid arrow) can enter the excitable gap inthe AV nodal circuit and activate the slow pathway. Delay of the subsequent His timing (as shown in Panel A) shouldbe specific for AVNRT. Advancement of the subsequent His timing, or termination of the SVT, are also very specificfor AVNRT, but could be observed in the case of JT with dual AV node physiology. Panel C: Schematic depiction ofthe response to an APB timed to junctional refractoriness in junctional tachycardia (JT); in the absence of dual AVnodal pathways the paced wavefront will collide with the retrograde wavefront from the JT focus (star) somewhere inthe AV node or proximal conduction system (black bar), so His timing cannot be affected.
septum is being depolarized indicates a diagnosisof AVNRT, but the same caveat discussed earlierwould apply if dual AVN physiology coexistedwith JT.23
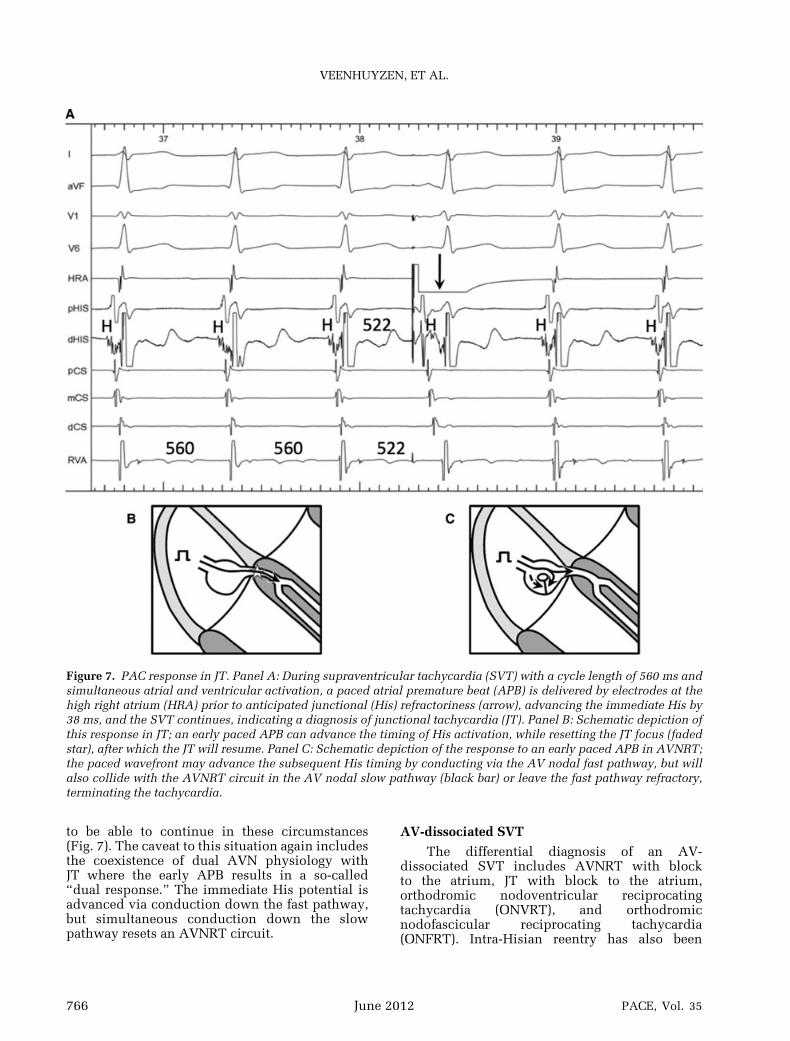
Padanilam and colleagues also suggested thatthe continuation of SVT after advancement of Hisbundle depolarization by an APB delivered priorto His bundle depolarization (which is again actingas a surrogate for fast pathway depolarization)
identifies a diagnosis of JT.22 An APB deliveredprior to fast pathway depolarization can advancethe immediate His bundle depolarization viaantegrade conduction down the fast pathway,but that would leave the fast pathway refractoryand unable to participate in an ongoing AVNRTcircuit (Fig. 7). Thus, both JT and AVNRT couldterminate when an APB that occurs prior to Hisbundle depolarization advances the immediateHis potential, but only JT would be expected
PACE, Vol. 35 June 2012 765
VEENHUYZEN, ET AL.
Figure 7. PAC response in JT. Panel A: During supraventricular tachycardia (SVT) with a cycle length of 560 ms andsimultaneous atrial and ventricular activation, a paced atrial premature beat (APB) is delivered by electrodes at thehigh right atrium (HRA) prior to anticipated junctional (His) refractoriness (arrow), advancing the immediate His by38 ms, and the SVT continues, indicating a diagnosis of junctional tachycardia (JT). Panel B: Schematic depiction ofthis response in JT; an early paced APB can advance the timing of His activation, while resetting the JT focus (fadedstar), after which the JT will resume. Panel C: Schematic depiction of the response to an early paced APB in AVNRT;the paced wavefront may advance the subsequent His timing by conducting via the AV nodal fast pathway, but willalso collide with the AVNRT circuit in the AV nodal slow pathway (black bar) or leave the fast pathway refractory,terminating the tachycardia.
to be able to continue in these circumstances(Fig. 7). The caveat to this situation again includesthe coexistence of dual AVN physiology withJT where the early APB results in a so-called“dual response.” The immediate His potential isadvanced via conduction down the fast pathway,but simultaneous conduction down the slowpathway resets an AVNRT circuit.
AV-dissociated SVT
The differential diagnosis of an AV-dissociated SVT includes AVNRT with blockto the atrium, JT with block to the atrium,orthodromic nodoventricular reciprocatingtachycardia (ONVRT), and orthodromicnodofascicular reciprocating tachycardia(ONFRT). Intra-Hisian reentry has also been
766 June 2012 PACE, Vol. 35
DIAGNOSTIC SVT PACING MANEUVERS 2
proposed, but we are not aware of any casesdemonstrating the existence of this mechanism,and it will not be discussed further. (Of course,ventricular tachycardia, including bundle branchreentry, would have to be excluded, but the meansto do so are beyond the scope of this review.)
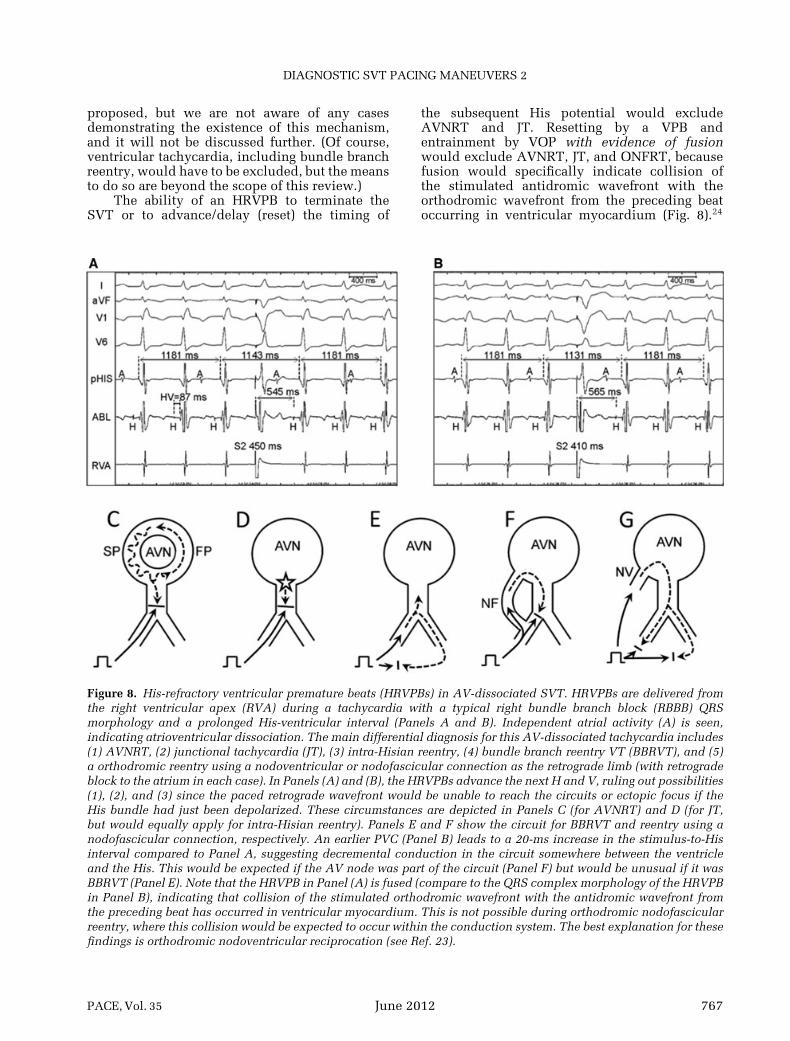
The ability of an HRVPB to terminate theSVT or to advance/delay (reset) the timing of
the subsequent His potential would excludeAVNRT and JT. Resetting by a VPB andentrainment by VOP with evidence of fusionwould exclude AVNRT, JT, and ONFRT, becausefusion would specifically indicate collision ofthe stimulated antidromic wavefront with theorthodromic wavefront from the preceding beatoccurring in ventricular myocardium (Fig. 8).24
Figure 8. His-refractory ventricular premature beats (HRVPBs) in AV-dissociated SVT. HRVPBs are delivered fromthe right ventricular apex (RVA) during a tachycardia with a typical right bundle branch block (RBBB) QRSmorphology and a prolonged His-ventricular interval (Panels A and B). Independent atrial activity (A) is seen,indicating atrioventricular dissociation. The main differential diagnosis for this AV-dissociated tachycardia includes(1) AVNRT, (2) junctional tachycardia (JT), (3) intra-Hisian reentry, (4) bundle branch reentry VT (BBRVT), and (5)a orthodromic reentry using a nodoventricular or nodofascicular connection as the retrograde limb (with retrogradeblock to the atrium in each case). In Panels (A) and (B), the HRVPBs advance the next H and V, ruling out possibilities(1), (2), and (3) since the paced retrograde wavefront would be unable to reach the circuits or ectopic focus if theHis bundle had just been depolarized. These circumstances are depicted in Panels C (for AVNRT) and D (for JT,but would equally apply for intra-Hisian reentry). Panels E and F show the circuit for BBRVT and reentry using anodofascicular connection, respectively. An earlier PVC (Panel B) leads to a 20-ms increase in the stimulus-to-Hisinterval compared to Panel A, suggesting decremental conduction in the circuit somewhere between the ventricleand the His. This would be expected if the AV node was part of the circuit (Panel F) but would be unusual if it wasBBRVT (Panel E). Note that the HRVPB in Panel (A) is fused (compare to the QRS complex morphology of the HRVPBin Panel B), indicating that collision of the stimulated orthodromic wavefront with the antidromic wavefront fromthe preceding beat has occurred in ventricular myocardium. This is not possible during orthodromic nodofascicularreentry, where this collision would be expected to occur within the conduction system. The best explanation for thesefindings is orthodromic nodoventricular reciprocation (see Ref. 23).
PACE, Vol. 35 June 2012 767
VEENHUYZEN, ET AL.
As with conventional orthodromic AVRT circuits,basal pacing sites close to the ventricular insertionof the nodoventricular AP would be expected toincrease the likelihood of detecting fusion, andalso decrease the postpacing interval (PPI)-TCLdifference and could, theoretically, be used as amethod of mapping the ventricular insertion ofthe AP; sites closest to the ventricular insertionwould be expected to have the shortest PPI-TCLdifference (provided that decremental conductionthrough the AVN does not influence the result,so the VOP CL should be as consistent aspossible) and a QRS complex morphology closestto that of the native SVT, possibly even revealingentrainment with concealed fusion. Haı̈ssaguerreand colleagues have described the use of singleventricular extrasystoles to accomplish the samediscriminatory goals.25
It is noteworthy that ONVRT and ONFRTneed not be AV dissociated. Indeed, if AVassociated, either could have any VA interval,including one short enough to mimic typicalAVNRT. Clues to their presence may includean SVT that otherwise appears consistent withAVNRT but where: (1) VOP yields cPPI-TCLand SA-VA interval values that are too short tobe consistent with AVNRT; (2) VOP results inmanifest entrainment (which should not be pos-sible in AVNRT or ONFRT, therefore indicatinga diagnosis of ONVRT); or (3) HRVPBs terminatethe SVT or affect the timing of the next Hispotential. The latter is the only reason we canthink of to bother scanning diastole with VPBsduring an SVT that appears consistent with typicalAVNRT.
AVNRT with Eccentric Left Atrial Activation
AVNRT with eccentric left atrial activation isan uncommon SVT whose existence is well doc-umented.26–32 Although it is widely recognizedthat the atrial exit of the AVN is not alwaysin the superior septum but may also be in theinferior septum where it can extend along the leftinferior aspect of the mitral annulus, it is not aswell recognized that AVNRT can rarely have itsearliest atrial activation along the lateral mitralannulus. Normally, this atrial activation sequencewould lead one to exclude AVNRT and to considerAVRT employing a left free wall AP or a left-sidedAT. If one entertains the possibility of AVNRTwith a left atrionodal extension in the differentialdiagnosis, then one faces a similar diagnosticchallenge to that posed by SVT with concentricatrial activation: all SVT mechanisms are possible.The usual ventricular pacing maneuvers may behelpful, but the yield is likely to be lower if theyare only performed from the RV apex, which isrelatively far from the lateral mitral annulus. As
discussed earlier, an HRVPB may not be capableof resetting AVRT employing a left free wall APbecause the stimulated wavefront may not haveenough time to reach the operative AP if deliveredlate enough to be His refractory. In the settingof AVRT employing a left free wall AP, VOP isunlikely to result in manifest entrainment, and thecPPI-TCL and SA-VA interval differences may belong by virtue of the distance of the RV apicalpacing site from the circuit (this would not bethe case if there was left bundle branch blockduring SVT, as the RV would be part of thecircuit in this circumstance). Thus, if the usualventricular pacing maneuvers are not helpful,one should consider scanning diastole with VPBsdelivered from basal sites in the left ventricle(LV) or performing VOP from basal sites in theLV (which can be stimulated via a branch of theCS, obviating the need to access the systemiccirculation prior to making a diagnosis in at leastone-third of cases). Alternatively, “differentialentrainment,” as described in Part 1 of thisreview, could be performed.1 It is noteworthy thatdifferential entrainment has only been studied ina few cases of AVRT employing left free wallAPs and we consider it at least theoreticallypossible that a patient could have a considerablyshorter conduction time from the RV apex to a leftposterior AP than from the basal infundibulumto such an AP, potentially making the results ofdifferential entrainment misleading.
ConclusionIn Part 1 of this review, we explored how
attempts to continuously reset (i.e. entrain) SVTby VOP can be used to provide a diagnosis inthe majority of sustained, regular SVTs. In thispart, we have explored other diagnostic pacingmaneuvers that might be helpful when VOP isnot diagnostic or appropriate including attemptsto reset SVT with single atrial or ventricularbeats, para-Hisian pacing, apex versus basepacing, and AOP. We have also discussed somespecific diagnostic SVT challenges encounteredin the electrophysiology lab. To be sure, thereare other pacing maneuvers that we have notaddressed, but this review should serve as athorough foundation for SVT diagnosis and forunderstanding the strengths and weaknesses ofthose other maneuvers. We hope that by gaining athorough understanding of how these maneuversexploit differences in the underlying anatomy andphysiology of the various SVT mechanisms, onewill gain an appreciation of which diagnostic pac-ing maneuvers constitute “proof” and which aremerely “evidence” in favor of one mechanism oranother.
768 June 2012 PACE, Vol. 35
DIAGNOSTIC SVT PACING MANEUVERS 2
References1. Veenhuyzen GD, Quinn FR, Wilton SB, Clegg R, Mitchell LB.
Diagnostic pacing maneuvers for supraventricular tachycardia: Part1. Pacing Clin Electrophysiol 2011; 34:767–782.
2. Josephson ME. Supraventricular tachycardias. In: Josephson ME(ed): Clinical Cardiac Electrophysiology. Philadelphia, PA, Lea andFebiger; 1993, p. 242.
3. Boonyapisit W, Kuhne M, Morady F, Jongnarangsin K, Supraven-tricular tachycardia with delayed atrial depolarization followingHissynchronous ventricular stimulation: What is the mechanism?Heart Rhythm 2010; 7:280–281.
4. Matsushita T, Badhwar N, Collins KK, Van Hare GF, Barbato G,Lee BK, Lee RJ, et al. Usefulness of a ventricular extrastimulusfrom the summit of the ventricular septum in diagnosis of septalaccessory pathway in patients with supraventricular tachycardia.Am J Cardiol 2004; 93:643–646.
5. Anselme F. Minimal/essential electrophysiologic assessment beforeablation. In: Zipes DP, Haissaguerre M. (eds.): Catheter Ablationof Arrhythmias, 2nd Ed. Armonk, New York, Futura PublishingCompany, Inc; 2002, p. 38.
6. Hsu JC, Tanel RE, Lee BK, Scheinman MM, Badhwar N, Lee RJ,Tseng ZH, et al. Differences in accessory pathway location by sexand race. Heart Rhythm 2010; 7:52–56.
7. Hirao H, Otomo K, Wang X, Beckman KJ, McClelland JH, WidmanL, Gonzalez MD, et al. Para-Hisian pacing. A new methodfor differentiating retrograde conduction over an accessory AVpathway from conduction over the AV node. Circulation 1996;94:1027–1035.
8. Matsushita T, Hongo RH, Badhwar N, Scheinman MM. Define themechanism of the tachycardia and explain the results of para-Hisianpacing. J Cardiovasc Electrophysiol 2004; 15:504–505.
9. Takatsuki S, Mitamura H, Tanimoto K, Fukuda Y, Ieda M, MiyoshiS, Soekima K, et al. Clinical implications of “pure” Hisian pacing inaddition to para-Hisian pacing for the diagnosis of supraventriculartachycardia. Heart Rhythm 2006; 3:1412–1418.
10. Heidbuchel H, Ector H, Adams J, Van de Werf F. Use of only a regulardiagnostic His-Bundle catheter for both fast and reproducible “para-Hisian pacing” and stable right ventricular pacing. J CardiovascElectrophysiol 1997; 8:1121–1132.
11. Adachi M, Igawa O, Miyake J, Yano A, Inoue Y, Ogura K, KatoM, et al. QRS complex widening due to loss of left bundle branchcapture: Pitfall of para-Hisian pacing. J Interv Card Electrophysiol2009; 25:213–216.
12. Obeyesekere M, Leong-Sit P, Skanes A, Krahn A, Yee R, Gula LJ,Bennett M, et al. Determination of inadvertent atrial capture duringpara-Hisian pacing. Circ Arrhythm Electrophysiol 2011; 4:510–514.
13. Reddy VY, Jongnarangsin K, Albert CM, Sabbour H, Keane D, MelaT, McGovern B, et al. Para-Hisian entrainment: A novel pacingmaneuver to differentiate orthodromic atrioventricular reentranttachycardia from atrioventricular nodal reentrant tachycardia. JCardiovasc Electrophysiol 2003; 12:1321–1328.
14. Martinez-Alday JD, Almendral J, Arsenal A, Ormaetxe JM, PastorA, Villacastı́n JP, Medina O, et al. Identification of concealedposteroseptal Kent pathways by comparison of ventriculoatrialintervals from apical and posterobasal right ventricular sites.Circulation 1994; 89:1060–1067.
15. Segal OR, Gula LJ, Skanes AC, Krahn AD, Yee R, Klein GJ.Differential ventricular entrainment: A maneuver to differentiateatrioventricular node reentrant tachycardia from orthodromicreciprocating tachycardia. Heart Rhythm 2008; 6:493–500.
16. Knight BP, Ebinger M, Oral H, Kim MH, Sticherling C, Pelosi F,Michaud GF, et al. Diagnostic value of tachycardia features andpacing maneuvers during paroxysmal supraventricular tachycardia.J Am Coll Cardiol 2000; 36:574–782.
17. Yamada T, Huizar JF, McElderry HT, Kay GN. Atrial tachycardiawith slow pathway conduction mimicking typical atrioventricularnodal reentrant tachycardia. Europace 2007; 9:299–301.
18. Gula LJ, Skanes A, Krahn AD, Klein GJ. Novel approach to diagnosisof a wide-complex tachycardia. J Cardiovasc Electrophysiol 2004;15:466–469.
19. Maruyama M, Kobayashi Y, Miyauchi Y, Ino T, Atarashi H, KatohT, Mizuno K. The VA relationship after differential atrial overdrivepacing: A novel tool for the diagnosis of atrial tachycardia in theelectrophysiologic laboratory. J Cardiovasc Electrophysiol 2007;18:1127–1133.
20. McElderry, Kay GN. Ablation of atrioventricular nodal reentry bythe anatomic approach. In: Huang S, Wood MA (eds.): CatheterAblation of Cardiac Arrhythmias. Philadelphia, OA, SaundersElsevier, 2006, p. 334.
21. Fan R, Tardos JG, Almasry I, Barbera S, Rashba EJ, Iwai W. Noveluse of atrial overdrive pacing to rapidly differentiate junctionaltachycardia from atrioventricular nodal reentrant tachycardia.Heart Rhythm 2011; 8:840–844.
22. Padanilam BJ, Manfredi JA, Steinberg LA, Olson JA, FogelRI, Prystowsky EN. Differentiating junctional tachycardia andatrioventricular node re-entry tachycardia based on response toatrial extrastimulus pacing. J Am Coll Cardiol 2008; 52:1711–1717.
23. Hamdan MH, Page RL, Scheinman MM. Diagnostic approach tonarrow complex tachycardia with VA block. Pacing Elecrophysiol1997; 20:2984–2988.
24. Quinn FR, Mitchell LB, Mardell AP, Disler D, Veenhuyzen GD.Entrainment mapping of a concealed nodoventricular accessorypathway in a man with complete heart block and tachycardiainduced cardiomyopathy. J Cardiovasc Electrophysiol 2008;19:90–94.
25. Haı̈ssaguerre M, Campos J, Marcus FI, Papouin G, Clementy J.Involvement of a nodofascicular connection in supraventriculartachycardia with VA dissociation. J Cardiovasc Electrophysiol 1994;5:854–862.
26. Dizon J, Reiffel J, Kassotis J, Woollett, Garan H. Change inthe retrograde atrial activation sequence following radiofre-quency modification of the atrioventricular node: Implicationsfor the electrophysiologic circuit of a variant of atrioventricularnode reentrant tachycardia. J Cardiovasc Electrophysiol 2003;14:461–466.
27. Hwang C, Martin DJ, Goodman JS, Gang ES, Mandel WJ,Swerdlow CD, Peter CT, et al. Atypical atrioventricular nodereciprocating tachycardia masquerading as tachycardia using aleft sided accessory pathway. J Am Coll Cardiol 1997; 30:218–225.
28. Nam GB, Rhee KS, Kim J, Choi KJ, Kim YH. Left atrionodalconnections in typical and atypical atrioventricular nodal reentranttachycardias: Activation sequence in coronary sinus and results ofradiofrequency catheter ablation. J Cardiovasc Electrophysiol 2006;17:1–7.
29. Otomo K, Okamura H, Noda T, Satomi K, Shimizu W, KuritaT, Aihara N, et al. “Left variant” atypical atrioventricular nodalreentrant tachycardia: Electrophysiological characteristics andeffect of slow pathway ablation within coronary sinus. J CardiovascElectrophysiol 2006; 17:1184–1186.
30. Anselme F, Papageorgiou P, Monahan K, Zardini M, Boyle N,Epstein LM, Josephson ME. Presence and significance of theleft atrionodal connection during atrioventricular nodal reentranttachycardia. Am J Cardiol 1999; 83:1530–1536.
31. Chen J, Anselme F, Smith TW, Zimetbaum P, Epstein LM,Papageorgiou P, Josephson ME. Standard right atrial ablationis effective for atrioventricular nodal reentry with earliestactivation in the coronary sinus. J Cardiovasc Electrophysiol 2004;15:2–7.
32. Ong MG, Lee PC, Tai CT, Lin YJ, Hsieh MH, Chen YJ, Lee KT,et al. The electrophysiologic characteristics of atrioventricularnodal reentry tachycardia with eccentric retrograde activation. Int JCardiol 2007; 120:115–122.
PACE, Vol. 35 June 2012 769