Embed Size (px)
Citation preview
1
Diagnosing Carpal Tunnel Syndrome
Sensitivity of ultrasonography versus nerve conduction study and their necessity
A.W.F. Grift
s1973428 10 March 2016 Plastic Surgery, Isala Zwolle Supervisor: Dr. P. Houpt, Plastic Surgeon

2
3
Contents List of abbreviations ......................................................................................................................... 5
Abstract ............................................................................................................................................ 6
Samenvatting .................................................................................................................................... 7
1. Introduction .................................................................................................................................. 8
1.1 Carpal Tunnel Syndrome ........................................................................................................ 8
1.2 Pathophysiology ...................................................................................................................... 8
1.3 Etiology ................................................................................................................................... 8
1.4 Prevalence ............................................................................................................................... 9
1.5 Anatomy .................................................................................................................................. 9
1.6 Clinical Symptoms & Signs .................................................................................................. 10
1.7 Treatment .............................................................................................................................. 11
1.7.1 Conservative treatment ................................................................................................... 11
1.7.2 Surgery ........................................................................................................................... 11
1.8 Diagnosing CTS .................................................................................................................... 11
1.9 Electrodiagnostic studies ...................................................................................................... 12
1.9.1 Nerve conduction studies ............................................................................................... 12
1.9.2 Electromyography .......................................................................................................... 16
1.9.3 Electrodiagnostic studies – values and limitations ......................................................... 16
1.9.4 Costs of electrodiagnostic studies .................................................................................. 16
1.10 Ultrasonography .................................................................................................................. 16
1.10.1 Ultrasonography – values and limitations .................................................................... 17
1.10.2 Costs of ultrasonography .............................................................................................. 17
1.11 Aim of this study ................................................................................................................. 17
1.12 Hypothesis ........................................................................................................................... 17
2. Materials & Method ................................................................................................................... 18
2.1 Study design .......................................................................................................................... 18
2.2 Inclusion criteria ................................................................................................................... 18
2.3 Exclusion criteria .................................................................................................................. 18
2.4 Further analysis ..................................................................................................................... 18
2.5 Interventions ......................................................................................................................... 20
2.5.1 Ultrasonography ............................................................................................................. 20
2.5.2 Nerve Conduction Study ................................................................................................ 20
2.5.3 Surgery: Carpal Tunnel Release ..................................................................................... 21
4
2.6 Cut-off points measurements ................................................................................................ 21
2.7 Analysis of data ..................................................................................................................... 22
2.8 Typical or atypical CTS ........................................................................................................ 22
2.9 Surgery outcome ................................................................................................................... 22
2.10 Study outcomes ................................................................................................................... 22
3. Results ........................................................................................................................................ 23
3.1 Patient characteristics in the overall CTS group ................................................................... 23
3.2 Patient characteristics in the typical and atypical CTS group ............................................... 23
3.3 Incidence of symptoms and signs in the overall CTS group................................................. 24
3.4 Incidence of symptoms and signs in the typical and atypical CTS group ............................ 24
3.5 Primary study outcome ......................................................................................................... 24
3.5.1 Ultrasonography ............................................................................................................. 24
3.5.2 Nerve conduction study ……………………………………………………………….24
3.5.3 Ultrasonography and nerve conduction study outcomes combined ............................... 25
3.5.4 Ultrasonography and nerve conduction study, differences in outcomes ........................ 25
3.6 Secondary study outcome ..................................................................................................... 26
3.7 Surgery outcome ................................................................................................................... 26
4. Discussion .................................................................................................................................. 27
4.1 Mean results .......................................................................................................................... 27
4.1.1 Hypothesis ...................................................................................................................... 27
4.2 Other results .......................................................................................................................... 27
4.2.1 Differences between groups ........................................................................................... 27
4.2.2 Combined outcome US and NCS ................................................................................... 27
4.2.3 Surgery outcome ............................................................................................................ 27
4.2.4 Costs ............................................................................................................................... 28
4.4 Strengths of this study ........................................................................................................... 29
4.5 Limitations of this study ....................................................................................................... 29
4.6 Recommended future study design ....................................................................................... 30
4.7 Further recommendations ..................................................................................................... 31
5. Conclusion .................................................................................................................................. 32
6. Bibliography ............................................................................................................................... 33
7. Appendix .................................................................................................................................... 38
7.1 CTS-6 (Six-item CTS symptom scale) form......................................................................... 38
5
List of abbreviations
AAEM = American Association of Electrodiagnostic Medicine
AAN = American Academy of Neurology
AAOS = American Academy of Orthopedic Surgeons
AAPM&R = American Academy of Physical Medicine and Rehabilitation
CSA = cross-sectional area
CTR = carpal tunnel release
CTS = carpal tunnel syndrome
CTS-6 = Six-item Carpal Tunnel Syndrome Symptom Scale
ECTR = endoscopic carpal tunnel release
EMG = electromyography
MNCV = motor nerve conduction velocity
NCS = nerve conduction study
NIH = National Institute of Health
OCTR = open carpal tunnel release
SNCV = sensory nerve conduction velocity
SSCT = subsynovial connective tissue
US = ultrasonography

6
Abstract
Introduction. Carpal Tunnel Syndrome (CTS) is the most common nerve entrapment of the
upper extremity and results from an entrapment of the median nerve beneath the flexor
retinaculum at the wrist. The prevalence of CTS is high (5% to 15%) among the general
population, with women five times more affected than men. Symptoms of CTS are pain, tingling
in the median nerve distribution area of the hand, numbness, weakness, nocturnal paresthesia,
hypotrophy and/or paresis of the thenar musculature, dropping items due to loss of sensory and/or
motor function, and/or decreased sweat function. There is no golden standard for diagnosing
CTS. Nerve conduction study (NCS) and ultrasonography (US) are the most used examinations
for confirming clinical CTS. Although NCS is frequently used to diagnose CTS, the rate of false-
negatives can be as high as 10% to 34%. Also, NCS is time consuming and uncomfortable for
patients. In order to determine whether the diagnosis CTS could be made by US only so NCS
would be unnecessary, the aim of this study is to examine the sensitivity of US and NCS of the
median nerve related to the clinical symptoms in diagnosing CTS.
Methods. In this retrospective study, a database with patients with clinical CTS was used.
Clinical symptoms, US outcomes and NCS outcomes were retrieved from medical records. The
outcomes of US and NCS were analyzed in three groups: an overall CTS group, a typical CTS
group and an atypical CTS group. The primary study outcomes were the outcomes of US and
NCS in these groups. The secondary study outcome was the sensitivity of US and NCS in
patients with clinical CTS.
Results. A total of 92 wrists from 57 patients were analyzed (67 (72,8%) wrists of women): 54
(57,7%) wrists in the typical CTS group and 38 (42,3%) wrists in the atypical CTS group. US
was positive in 73,9%, 72,2% and 76,3% of the overall group, the typical CTS group and the
atypical CTS group, respectively. NCS was positive in 81,5%, 79,6% and 84,2% in the overall
group, the typical CTS group and the atypical CTS group, respectively. The sensitivity of US and
NCS in the overall group was 73,9% and 81,5%, respectively (p 0,204). In the typical CTS group,
the sensitivity for US and NCS was 72,2% and 79,6%, respectively (p 0,289). In the atypical CTS
group, the sensitivity for US and NCS was 76,3% and 84,2%, respectively (p 0,238).
Conclusion. This study showed that the sensitivity of US is comparable with the sensitivity of
NCS in the overall CTS group, the typical CTS group and atypical CTS group. Although there
was no significant difference between US and NCS, US could be preferred as first examination to
confirm the diagnosis CTS, because this examination is less uncomfortable for patients in
comparison with NCS. Further prospective and blinded studies are needed to confirm these
outcomes.
7
Samenvatting
Introductie. Het Carpale Tunnel Syndroom (CTS) is de meest voorkomende zenuwbeklemming
van de bovenste extremiteit en ontstaat door een beklemming van de nervus medianus onder het
flexor retinaculum in de pols. De prevalentie van CTS is hoog onder de algemene bevolking (5-
15%), waarbij vrouwen vijf keer vaker zijn aangedaan dan mannen. Symptomen van CTS zijn
pijn, tintelingen in het gebied van de nervus medianus, doofheid, zwakte, nachtelijke pijn,
hypotrofie en/of parese van de thenar musculatuur, het laten vallen van objecten door verlies van
sensorische en/of motore functie, en/of verminderde zweet productie. Er is geen Gouden
Standaard voor het diagnosticeren van CTS. Zenuwgeleidingsonderzoek en echografie zijn de
meest gebruikte onderzoeken om klinisch CTS te bevestigen. Hoewel zenuwgeleidingsonderzoek
vaak gebruikt wordt om CTS te diagnosticeren, is het percentage vals-negatieven 10-34%.
Daarnaast kost het zenuwgeleidingsonderzoek veel tijd en is het oncomfortabel voor patiënten.
Om vast te stellen of de diagnose CTS gesteld kan worden met alleen echografie en om vast te
stellen of zenuwgeleidingsonderzoek overbodig zou zijn, is het doel van deze studie om de
sensitiviteit van echografie en zenuwgeleidingsonderzoek van de nervus medianus te bepalen ten
opzichte van de klinische diagnose CTS.
Methode. In deze retrospectieve studie werd gebruik gemaakt van een database met patiënten
met klinisch gediagnosticeerd CTS. De klinische symptomen, echografie uitslagen en
zenuwgeleidingsonderzoek uitslagen werden verzameld uit de medische dossiers. De uitkomsten
van de onderzoeken werden geanalyseerd in drie groepen: een totale groep, de groep met typisch
CTS en de groep met atypisch CTS. De primaire studie uitkomsten waren de uitkomsten van
echografie en zenuwgeleidingsonderzoek in deze drie groepen. De secundaire studie uitkomst
was de sensitiviteit van echografie en zenuwgeleidingsonderzoek.
Resultaten. In totaal werden 92 polsen van 57 patiënten geanalyseerd (67 (72,8%) polsen van
vrouwen): 54 (57,7%) polsen behoorden in de typisch CTS groep en 38 (42,3%) polsen in de
atypische groep. Echografie was positief in respectievelijk 73,9%, 72,2% and 76,3% van de totale
groep, de typisch CTS groep en de atypisch CTS groep. Het zenuwgeleidingsonderzoek was
positief in respectievelijk 81,5%, 79,6% en 84,2% van de totale groep, de typisch CTS groep en
de atypisch CTS groep. De sensitiviteit van echografie en zenuwgeleidingsonderzoek in de totale
groep was respectievelijk 73,9% en 81,5% (p 0,204). In de typisch CTS groep was dit
respectievelijk 72,2% en 79,6% (p 0,289) en in de atypisch CTS groep was dit 76,3% en 84,2%
(p 0,238).
Conclusie. Deze studie toont aan dat de sensitiviteit van echografie vergelijkbaar is met die van
het zenuwgeleidingsonderzoek in zowel de totale, de typische, als de atypische CTS groep.
Hoewel er geen significant verschil is in de sensitiviteit van echografie en het
zenuwgeleidingsonderzoek, zou echografie het onderzoek van eerste keus kunnen zijn om de
diagnose te bevestigen bij patienten met klinische CTS, omdat echografie minder oncomfortabel
en belastend is voor patienten ten opzichte van het zenwgeleidingsonderzoek. Verder prospectief
en geblindeerd onderzoek is nodig om deze uitkomsten te bevestigen.
8
1. Introduction
1.1 Carpal Tunnel Syndrome
Carpal Tunnel Syndrome (CTS) is the most common nerve entrapment of the upper extremity
and results from an entrapment of the median nerve beneath the flexor retinaculum at the
wrist(1). The American Academy of Orthopedic Surgeons (AAOS) defines CTS as ‘‘a
symptomatic compression neuropathy of the median nerve at the level of the wrist’’(2).
A similar description of CTS was first given by Paget (1814-1899). Paget described the
compression of the median nerve after a fracture of the distal radius(3). Marie and Foix reported a
lesion of the median nerve with a neuroma, next to the flexor retinaculum, in 1913(4). Finally,
Phalen was the first to describe the current principles of CTS in 1950: numbness and tingling in
the first, second, third, and fourth finger, which is worse at night and after using the hand(s)(5).
Phalen also found that most of the time a positive Tinel sign (see section 1.6) over the median
nerve at the wrist and flexion of the wrists worsens the symptoms(5). The latter is now called
Phalen’s sign.
1.2 Pathophysiology The exact pathophysiology of CTS is unknown, but the cause of idiopathic CTS is suggested to
be due to compression of the median nerve(6). This compression may lead to alterations of the
morphological structure of the nerve and demyelination, which is due to mechanical stress
deforming the myelin sheath(7). Paresthesia experienced by patients during the night could be the
cause of a decreased blood flow in the microcirculation and, due to the decreased circulation, the
ischemia that occurs(4,7). Additionally, it is suggested that fibrosis, thickening of the synovium,
new axonal growth, endoneurial edema and remyelination contributes to compression(8). The
edema could result from the increase of pressure in the carpal tunnel(4). When the pressure
increases more than 40-50 mmHg, the intraneural microcirculation is diminished, which causes
venous stasis with edema. Furthermore the axonal transport decreases, which could contribute to
the development of CTS, since the lack of nutrients could degrade the median nerve(4).
Microtear hypothesis
The microtear hypothesis, described by Werthel et al.(9) in 2014, suggests that CTS starts with a
tear in the surrounding Subsynovial Connective Tissue (SSCT). Repetitive movements of the
wrist, the hand or the fingers can lead to idiopathic CTS, probably due to the alterations of the
SSCT. With flexion, the pressure in de carpal tunnel increases and the forces on the SSCT
increase. A tiny tear could originate in the SSCT. With this tear the cascade of the woundhealing
process starts, causing inflammation and fibrosis, which provides thickening of the structures in
the carpal tunnel and in that way an increase in pressure in the carpal tunnel. This causes the
entrapment of the median nerve, which can lead to problems like ischemia, edema and
remyelination. Werthels’ hypothesis is that these problems cause CTS.
1.3 Etiology
Many factors may contribute to the development of CTS, including rheumatological diseases,
acromegaly, myxedema, bursal fibrotic alterations or pregnancy. Other contributing factors
mentioned in literature are abnormalities of the carpal tunnel, such as dislocation or subluxation
of the carpal bones, fractures of the distal radius and arthritis. Also inflammatory alterations,
tenosynovitis, lipoma’s, neuroma’s, cysts and hematoma’s may contribute(4,7,8). Furthermore,
9
manual activities may contribute to the development of CTS(7), but the major part (65-80%) of
CTS is idiopathic(4).
1.4 Prevalence
The prevalence of CTS is high, ranging from 5% to 15% among the general population with
women five times more affected than man. In The Netherlands the prevalence is 9% among
women and only 0,6% among men(10). The majority of patients (80%) is older than 40
years(7,11). The National Institute of Health (NIH) suggests that the carpal tunnel in women may
be smaller than in men, which could be the cause of the higher amount of woman that is
affected(12).
1.5 Anatomy
The carpal tunnel has a complicated anatomy with many different structures. On the dorsal,
medial and lateral sides it is limited by the carpal bones. On the palmar side the flexor
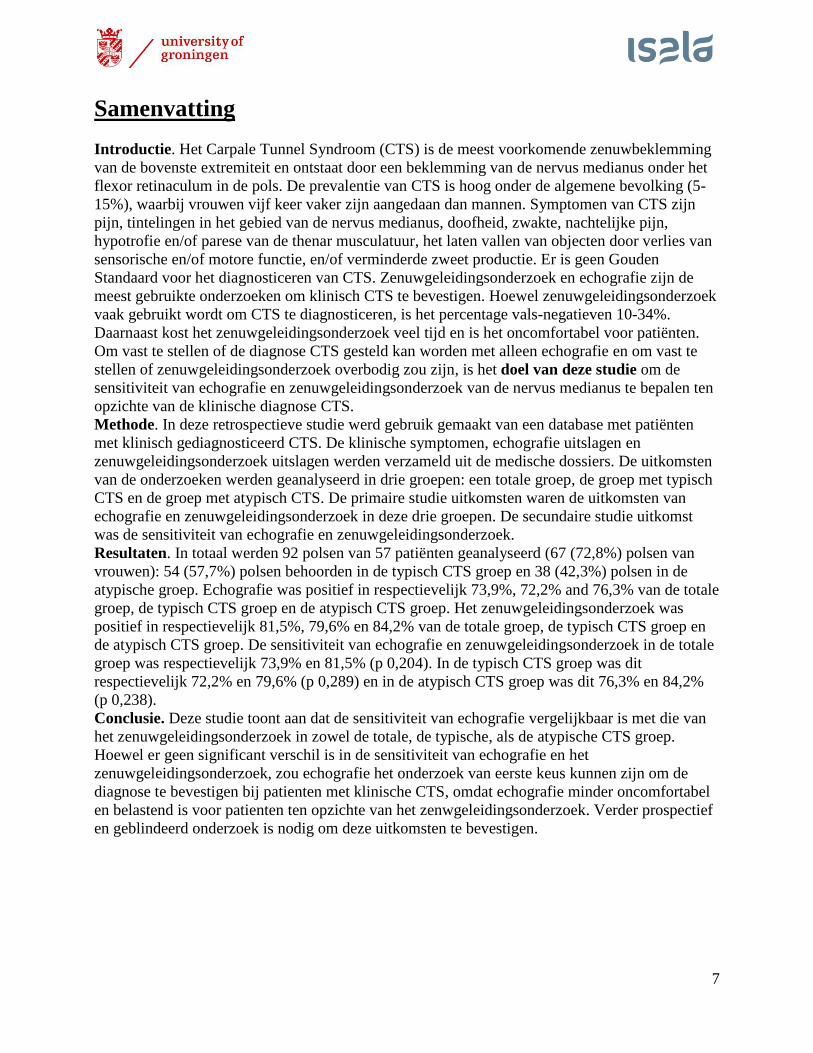
retinaculum (transverse carpal ligament) limits the carpal tunnel. The carpal tunnel contains nine
flexor tendons (four flexor digitorum profundus tendons, four flexor digitorum superficialis
tendons and the flexor pollicis longus tendon) and the median nerve, all of which are surrounded
by subsynovial connective tissue(9)(fig. 1).
Fig. 1. Anatomy of the carpal tunnel with the nine tendons, the median nerve and the flexor
retinaculum.
The median nerve passes the carpal tunnel beneath the flexor retinaculum and then continues into
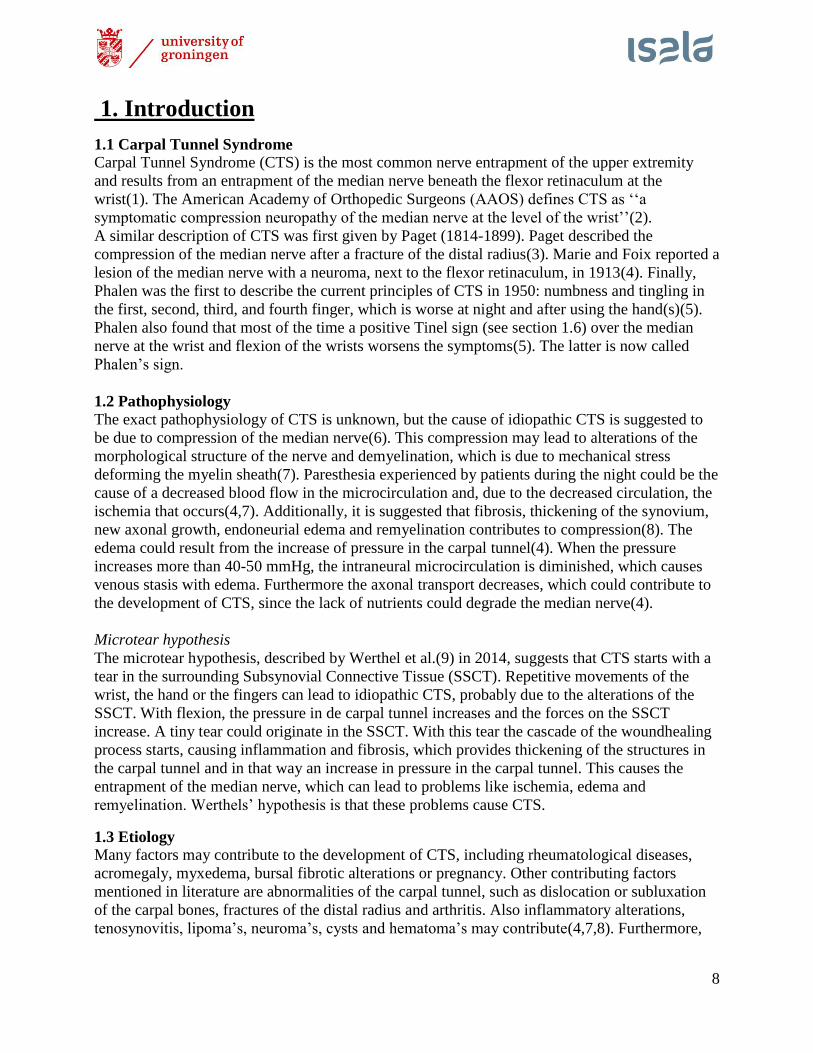
two branches. The first branch, the palmar digital nerve, is responsible for the sensory innervation
of the palmar skin of the first, second, third and the lateral side of the fourth digit. The palmar
digital nerve is also responsible for the sensory innervation of the dorsal nail beds of these digits
(fig. 2). Besides the sensory innervation, this branch also provides the motor innervation to the
lateral two lumbrical muscles. These muscles are responsible for the flexion of the
metacarpophalangeal joints of the second and third digit. The second branch of the median nerve
is the so-called recurrent branch. This branch innervates two of the four the thenar muscles: the
abductor pollicis brevis muscle and the opponens pollicis muscle, which are associated with
10
abduction and opposition of the thumb. The third thenar muscle, the flexor pollicis brevis muscle,
is partly innervated by the median nerve, but also by the ulnar nerve. The fourth thenar muscle,
the adductor pollicis muscle, is innervated by a branch of the ulnar nerve only.
Fig. 2. Median nerve distribution area of the hand. Left: palmar side of the hand. Right: dorsal
side of the hand. In blue, the area in which the median nerve supplies the sensory innervations
(13).
1.6 Clinical Symptoms & Signs
Patients with CTS can experience pain, tingling in the median nerve distribution of the hand,
numbness and weakness. Also nocturnal paresthesia, hypotrophy of the thenar musculature,
dropping items due to loss of sensory and/or motor function, and/or decreased sweat function
have been described(8,14,15). When patients with suspicion of CTS are examined, several signs
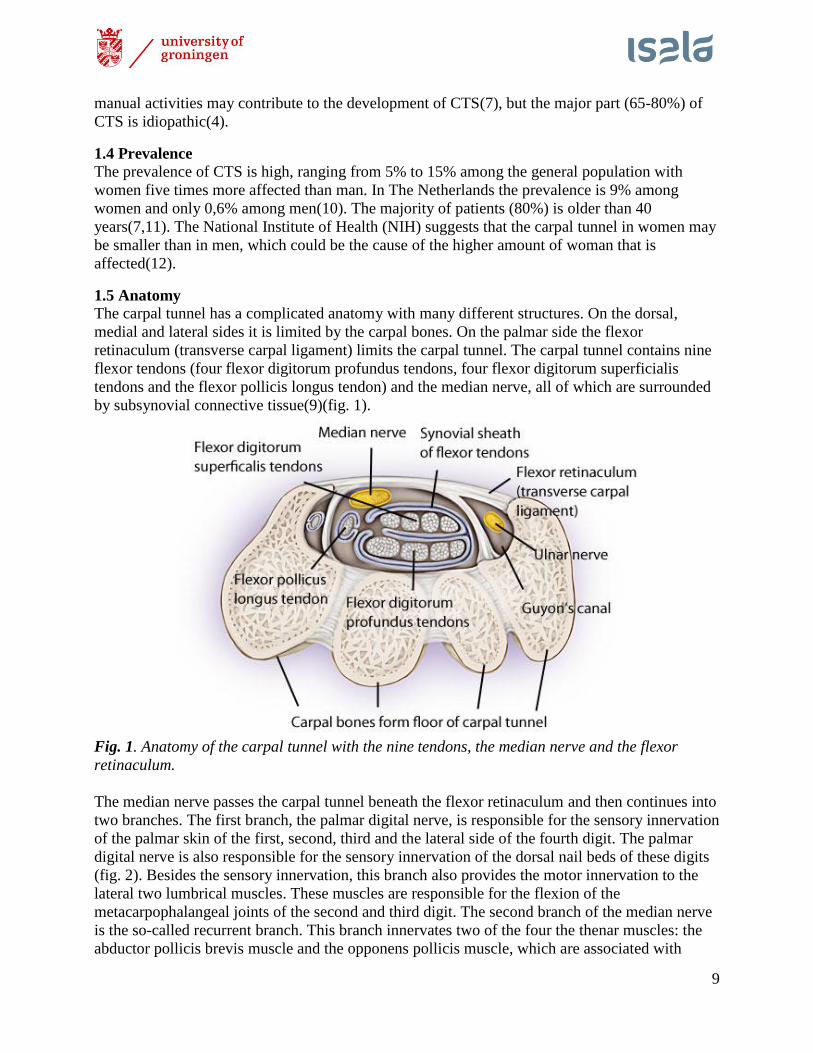
suggest the diagnosis CTS. One of these is a positive Tinel’s test. This test is positive when
tapping on the palmar side of the wrist gives paresthesia in the median nerve distribution of the
hand (fig. 3). The sensitivity of Tinel’s test is 26% to 79% and its specificity is 40% to 100%(4).
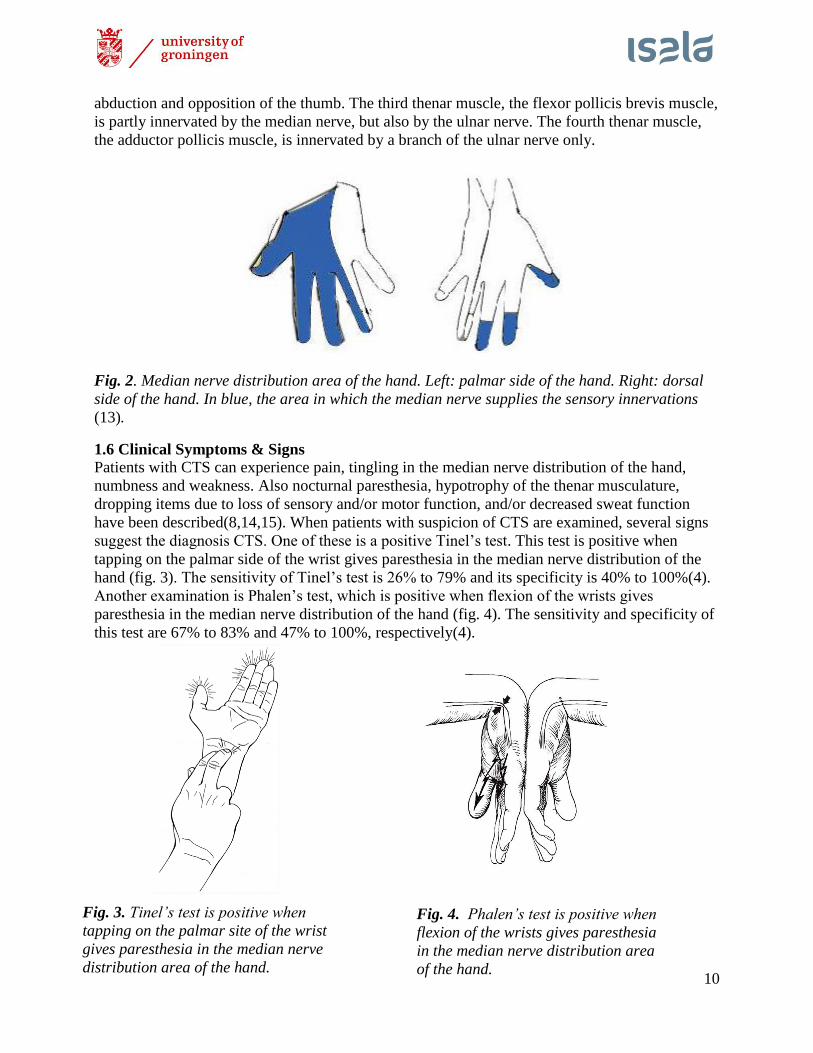
Another examination is Phalen’s test, which is positive when flexion of the wrists gives
paresthesia in the median nerve distribution of the hand (fig. 4). The sensitivity and specificity of
this test are 67% to 83% and 47% to 100%, respectively(4).
Fig. 3. Tinel’s test is positive when
tapping on the palmar site of the wrist
gives paresthesia in the median nerve
distribution area of the hand.
Fig. 4. Phalen’s test is positive when
flexion of the wrists gives paresthesia
in the median nerve distribution area
of the hand.
11
1.7 Treatment The treatments of CTS can be divided in two groups: conservative treatment and surgical
treatment.
1.7.1 Conservative treatment
The conservative treatment of CTS consists for example of rest, exercise, splinting of the wrist in
neutral position, injection with corticosteroids, medication (e.g. NSAID’s or vitamin B6), or
education about e.g. positioning the wrists(16-18). In general, conservative treatments have a
worse outcome(17,19): more than 50% of the patients who received a conservative treatment,
eventually received surgery(17).
1.7.2 Surgery
Carpal Tunnel Release (CTR) is a surgery in which the flexor retinaculum (transverse carpal
ligament) is released(19). Recent studies have found no difference in outcome when performing
an Open Carpal Tunnel Release (OCTR) or an Endoscopic Carpal Tunnel Release (ECTR)(20-
22). The symptom improvement within three months (short term) and after three months (long
term) is not significantly different between both surgeries(20,21). One of the advantages of
OCTR is that the anatomical structures can be seen properly(20). Furthermore, ECTR seems to
give more nerve problems, but only temporary (e.g. numbness, neurapraxia, parasthesia)(20). On
the other hand, OCTR seems to give more wound problems (e.g. infection, scar tenderness or
hypertrophic scarring)(21). Overall, Gerritsen et al.(20) recommend to perform an OCTR.
Although the outcome of OCTR is equal to ECTR, OCTR is technically less hard to perform,
which lowers the risks of complications(20). After CTR, 88% had a significant improvement of
the symptoms and 79% of the patients had improvement of function(23).
1.8 Diagnosing CTS
Finding the best way to diagnose CTS has been subject of many studies, but there is no consensus
in these studies. Some studies suggest to diagnose CTS based on the clinical symptoms with an
electrodiagnostic study alone(7,11,24,25). Some studies suggest to diagnose CTS based on the
clinical symptoms in combination with ultrasonography(1,26-29). Other studies suggest to
diagnose CTS based on clinical symptoms with a combination of an electrodiagnostic study and
ultrasonography(14,30-32). Beside this, some studies suggest to diagnose CTS based on clinical
symptoms alone(33). Furthermore, it is described that the diagnosis CTS could be made only
post-operative, when the patient experience no more symptoms.
In the hospital this research is conducted, Isala in Zwolle, The Netherlands, the diagnosis for CTS
is made by clinical symptoms in combination with an electrodiagnostic study: Nerve Conduction
Study (NCS). When the NCS is negative for CTS, additionally ultrasonography (US) is carried
out.
1.8.1 Gold standard There is no gold standard for diagnosing CTS. However, the electrodiagnostic studies have a
sensitivity of 49% to 84% and a specificity of at least 94%(7,8). Because of this high sensitivity
and specificity percentages, these examinations in combination with clinical symptoms and signs
(section 1.6) are considered to be the best for CTS diagnosis in most hospitals(6,8,14,34). The
CBO-guideline, a guideline from the Dutch institute of healthcare quality, advises to confirm the
clinical diagnosis of CTS with NCS(35). This guideline states that US should be carried out only
if desired, in order to determine structural abnormalities.

12
1.9 Electrodiagnostic studies
Electrodiagnostic studies are techniques that can trace abnormalities of the median nerve fibers
within the carpal tunnel(36). By comparing the median nerve responses with other healthy
nerves, abnormalities of the median nerve are documented. Several studies proved that
comparison of sensory nerve responses are more useful than the absolute median nerve latency
time(36,37). The reason for this is the larger proportion of large myelinated fibers in the sensory
fibers. These large fibers require more energy and thus are more prone to ischemic damage(38).
Damage of the myelin and ischemia could result from the compression of the median nerve
which is present in CTS. This results in a reduced conduction velocity, because damaged myelin
causes a decrease in axonal conduction.
The greatest accuracy to confirm the clinical diagnosis of CTS with electrodiagnostic studies is
by comparing the median nerve sensory latency to the radial and/or ulnar nerve sensory latency.
The comparison with a segment of the median nerve outside the carpal tunnel can also contribute
to diagnosing CTS(36).
The electrodiagnostic study used most for diagnosing CTS is the nerve conduction study, but
when this examination does not confirm CTS, an electromyography may be carried out as
well(2,37,39).
1.9.1 Nerve conduction studies Nerve Conduction Studies (NCS) are performed with electrodes, which are placed on the skin.
With electrical signals the nerves are stimulated and the electrical activity is measured. The
electrodes measure the nerve conduction latency time. The value of the nerve conduction latency
time is compared with the cut-off point, which is defined differently at each hospital. If the nerve
conduction latency time is lower than the cut-off point, the diagnosis CTS is set.
There are several options to measure the nerve conduction latency time. The American
Association of Electrodiagnostic Medicine (AAEM), the American Academy of Neurology
(AAN) and the American Academy of Physical Medicine and Rehabilitation (AAPM&R) have
formulated recommendations to confirm a clinical diagnosis of CTS with the assistance of
electrodiagnostic studies(39) (table 1).
With NCS the sensory latency time, the Sensory Nerve Conduction Velocity (SNCV) and the
motor latency time are measured. These variables can say something about the rate of conduction
of the sensory or motor nerve. The diagnosis CTS is suggested when the latency time of the
median nerve is decreased compared with other, healthy, nerves. The decreased latency time
suggests that the conduction is decreased and this could be caused by CTS.
The recommendations from the American institutions in table 1, are comparable with the Dutch
guideline for diagnosing CTS(35). The Dutch guideline recommends measuring the latency time
of the sensory action potential of the median nerve, the latency time of the sensory action
potential of the median nerve compared with the ulnar nerve and the SNCV of the median nerve
across the wrist/palm segment. These three measurements are comparable with the measurements
mentioned in table 1; number 1, 2a, 2b and 2c.
13
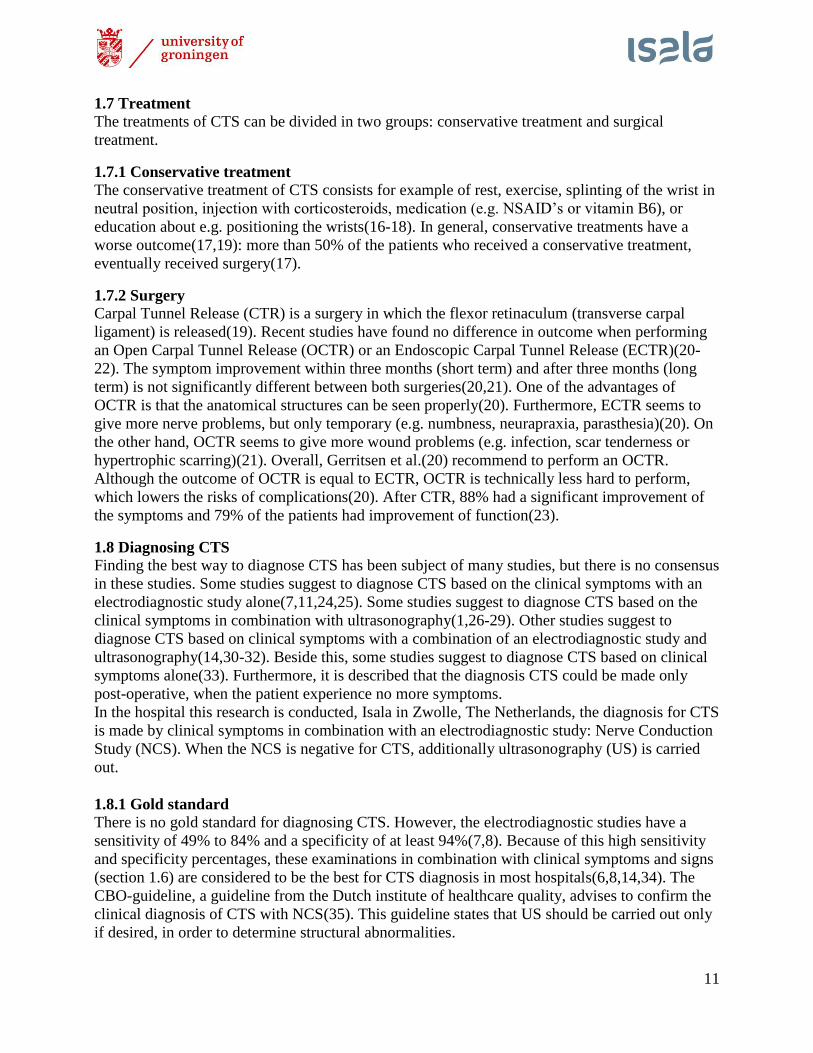
Fig. 5. The sensory latency time of the median
nerve can be measured across the wrist and a
digit, with a conduction distance of 13-14 cm.
The electrode is usually placed on the second or
third finger. If the sensory latency time is
abnormal, it should be compared with another
nerve at the same limb, for example the ulnar
nerve(37).
SNCV: sensory nerve conduction velocity; MNCV: motor nerve conduction velocity; EMG:
electromyography. Further explanation: see next pages.
Firstly, the sensory latency time of the median nerve can be measured across the wrist and a digit,
with a conduction distance of 13-14 cm (fig. 5). If the sensory latency time is abnormal, it should
be compared with the ulnar or radial nerve in the same limb (fig. 5). This comparison is needed
because a difference has to be proved.
If the initial median nerve sensory latency time is normal, three options are left to examine to
determine if the median nerve is abnormal compared to other nerves.
Table 1. Recommendations of the AAEM, AAN and AAPM&R to diagnose CTS
with assistance of electrodiagnostic studies
1. Median nerve sensory latency time across the wrist and a digit with a long distance
of 13-14cm;
2. If the measurement mentioned at number 1) is normal:
a. Median nerve sensory latency time across the wrist and the palm with a short
distance of 7-8 cm, compared with the ulnar sensory latency time;
b. Median nerve sensory latency time across the wrist, compared with the ulnar
sensory latency time (at fourth digit) and/or the radial sensory latency time (at the
first digit);
c. Median nerve SNCV across the wrist/palm segment compared with the
segment of the forearm/digit;
3. Motor latency time of the median nerve, innervating the thenar muscle;
4. Motor latency time of the median nerve, innervating the lumbrical muscles, and the
ulnar nerve, innervating the interossei muscles;
5. EMG, including thenar muscle innervated by the median nerve.
14
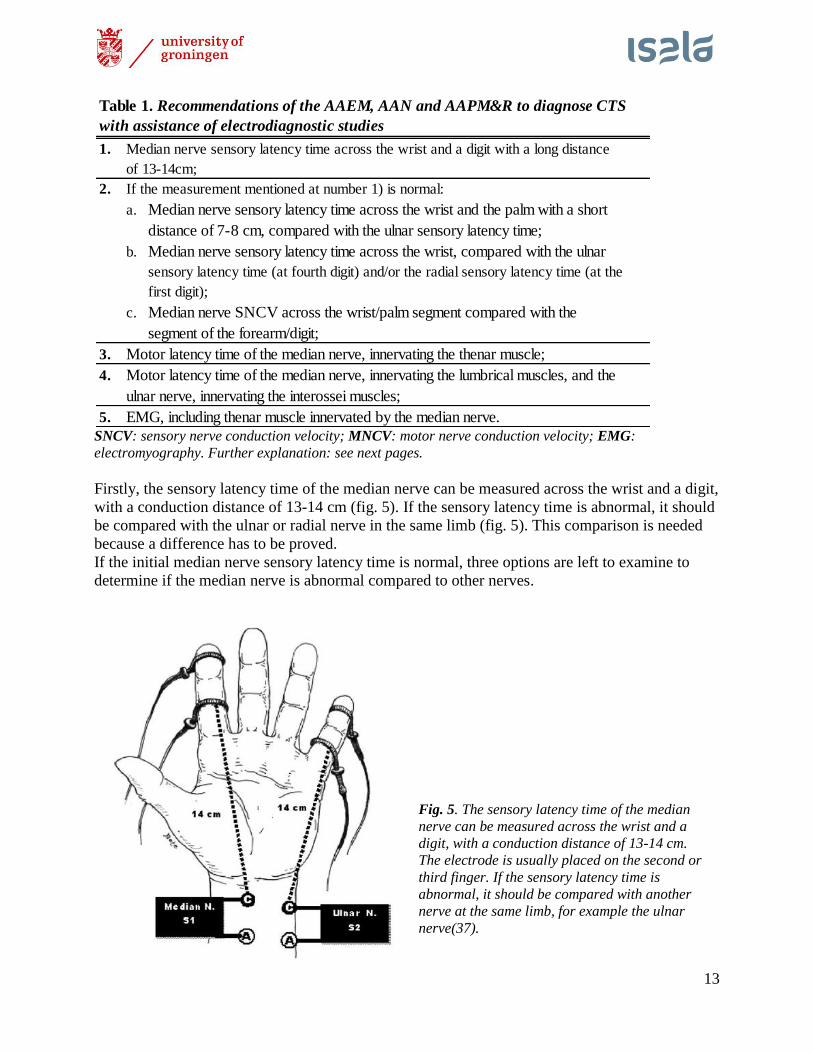
Firstly, the median nerve sensory latency time
across the wrist over a short conduction distance
(7-8 cm) can be compared with the ulnar
sensory latency time(fig. 6). If the median nerve
latency time is decreased compared to the ulnar
nerve, this measurement is abnormal.
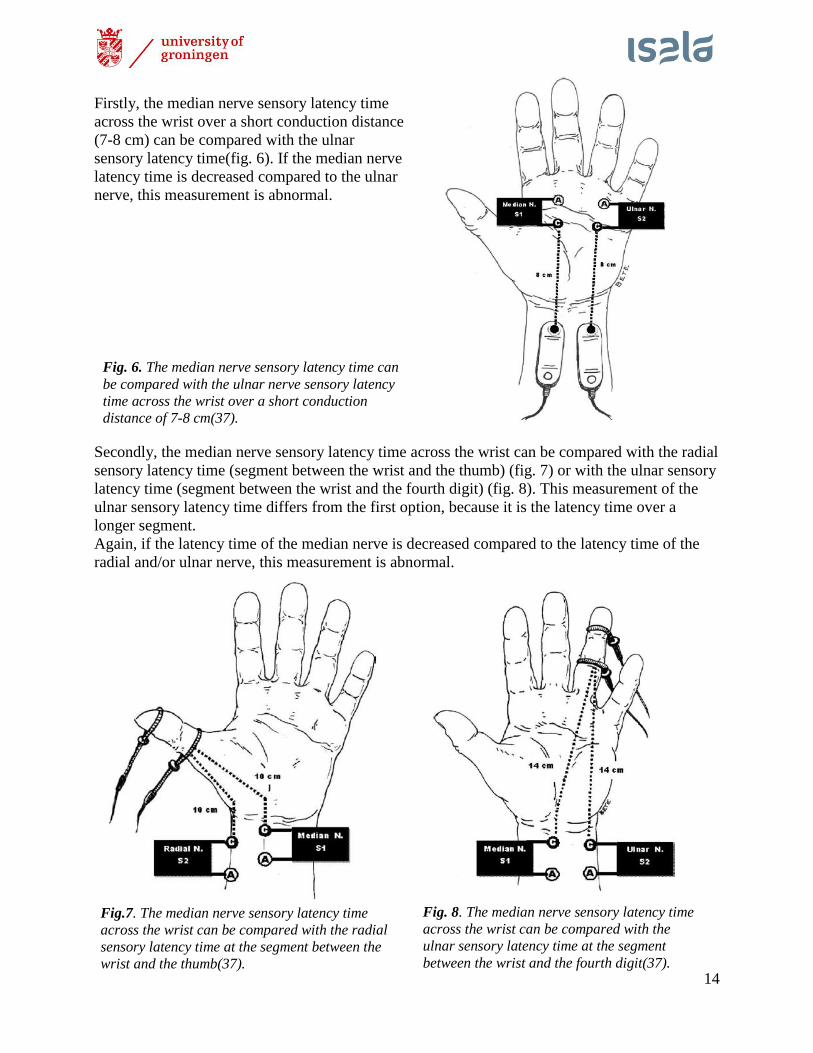
Secondly, the median nerve sensory latency time across the wrist can be compared with the radial
sensory latency time (segment between the wrist and the thumb) (fig. 7) or with the ulnar sensory
latency time (segment between the wrist and the fourth digit) (fig. 8). This measurement of the
ulnar sensory latency time differs from the first option, because it is the latency time over a
longer segment.
Again, if the latency time of the median nerve is decreased compared to the latency time of the
radial and/or ulnar nerve, this measurement is abnormal.
Fig.7. The median nerve sensory latency time
across the wrist can be compared with the radial
sensory latency time at the segment between the
wrist and the thumb(37).
Fig. 8. The median nerve sensory latency time
across the wrist can be compared with the
ulnar sensory latency time at the segment
between the wrist and the fourth digit(37).
Fig. 6. The median nerve sensory latency time can
be compared with the ulnar nerve sensory latency
time across the wrist over a short conduction
distance of 7-8 cm(37).
15
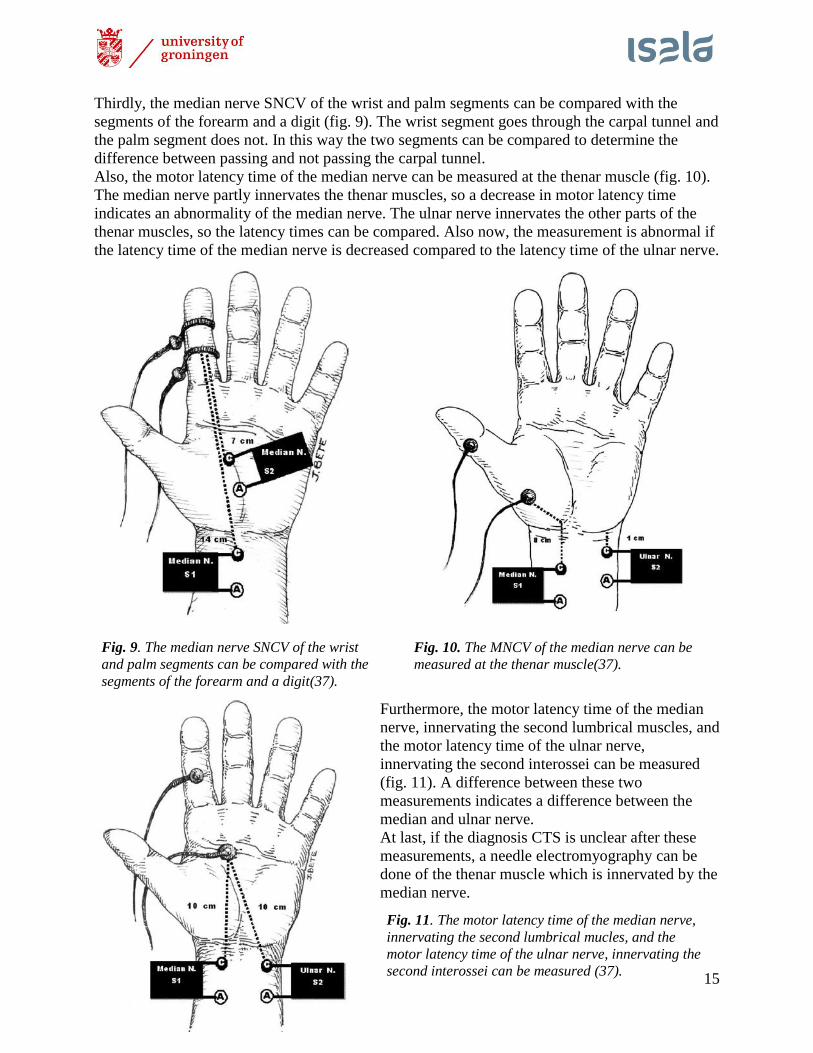
Fig. 11. The motor latency time of the median nerve,
innervating the second lumbrical mucles, and the
motor latency time of the ulnar nerve, innervating the
second interossei can be measured (37).
Thirdly, the median nerve SNCV of the wrist and palm segments can be compared with the
segments of the forearm and a digit (fig. 9). The wrist segment goes through the carpal tunnel and
the palm segment does not. In this way the two segments can be compared to determine the
difference between passing and not passing the carpal tunnel.
Also, the motor latency time of the median nerve can be measured at the thenar muscle (fig. 10).
The median nerve partly innervates the thenar muscles, so a decrease in motor latency time
indicates an abnormality of the median nerve. The ulnar nerve innervates the other parts of the
thenar muscles, so the latency times can be compared. Also now, the measurement is abnormal if
the latency time of the median nerve is decreased compared to the latency time of the ulnar nerve.
Furthermore, the motor latency time of the median
nerve, innervating the second lumbrical muscles, and
the motor latency time of the ulnar nerve,
innervating the second interossei can be measured
(fig. 11). A difference between these two
measurements indicates a difference between the
median and ulnar nerve.
At last, if the diagnosis CTS is unclear after these
measurements, a needle electromyography can be
done of the thenar muscle which is innervated by the
median nerve.
Fig. 9. The median nerve SNCV of the wrist
and palm segments can be compared with the
segments of the forearm and a digit(37).
Fig. 10. The MNCV of the median nerve can be
measured at the thenar muscle(37).
16
1.9.2 Electromyography
Electromyography (EMG) can be used in combination with NCS, when NCS does not confirm
the diagnosis CTS(39). With EMG, the electrical activity in the muscles is measured. Needles are
placed into the muscles and register the electrical activity of the muscles in relaxed or tensed
position(40). A healthy muscle in relaxed position does not show electrical activity. When the
patient tenses the muscles, electrical activity will occur. In severe CTS, the innervation of the
muscles can be decreased, causing a decrease of electrical activity during attempts to activate the
muscle. In the resting state there will be abnormal electrical activity.
This examination is carried out rarely in the hospital this study is conducted, because it is an
invasive examination.
1.9.3 Electrodiagnostic studies – values and limitations
Electrodiagnostic studies have a sensitivity of 56-85% and a specificity of 94% or higher(31).
Becker et al.(41) suggest that electrodiagnostic studies could contribute to the decision to operate,
because they could determine the severity of CTS. In case of patients with more severe CTS, the
decision to operate could be made earlier.
Although electrodiagnostic studies are frequently used to diagnose CTS, the rate of false-
negatives can be as high as 10% to 34%(6,8,14,42). Also, electrodiagnostic studies are time
consuming, uncomfortable for patients and it is sometimes an invasive procedure, when using
EMG(14,26,42). Furthermore, electrodiagnostic studies cannot assess the anatomy of the carpal
tunnel with the median nerve in it, so abnormal anatomy cannot be seen(26). One of the factors
that can affect the outcome of electrodiagnostic studies is skin temperature(4). When the skin
temperature is below 30 degrees Celsius, the nerve conduction velocity can decrease, which can
be interpreted as a false positive outcome(15).
1.9.4 Costs of electrodiagnostic studies The costs of all electrodiagnostic studies differ at each centre. In Isala in Zwolle, the Netherlands,
where this study is conducted, the costs of NCS are €340,- in the year 2015(43). The price
depends on the extent of the examination.
1.10 Ultrasonography
Several recent studies have described ultrasonography (US) as a useful tool in diagnosing
CTS(7,14,26). It has a sensitivity of 44% to 95% and a specificity of 57% to 100%(8). US is used
to measure the Cross-Sectional Area (CSA) of the median nerve in the wrist. Several studies
suggest that an increase of the CSA of the median nerve can diagnose CTS(1,15,26-29,44-46).
The hypothesis is that in CTS, the CSA of the median nerve increases because of e.g. the edema,
as mentioned in section 1.2.
There is no consensus about the cut-off point above which the diagnosis CTS could be made. The
values differ between 6,0 mm2 to 16,0mm
2(11). The most used cut-off point is around 10,0
mm2(11).
Also the location where to measure in the wrist to determine the CSA is unclear. Some studies
suggest that the carpal-inlet (at the level of the pisiform) is the best location
(6,8,14,28,29,32,42,46). Another study suggests that the carpal-outlet is the best location to
measure(1).
17
1.10.1 Ultrasonography – values and limitations US at the wrist provides more insight into the cause of the symptoms as it can assess structural
abnormalities(7,26), such as space-occupying lesions, malalignment of the carpal bones,
tenosynovitis, ganglia, tumors or changes in the vascularization(8,32). Furthermore, it is simple,
pain-free, quickly and non-invasive(7,8,15). Beside this, recent studies suggest that also US could
determine the severity of CTS(31,47).
The biggest limitation of US is that this examination is observer-dependent(7,8).
1.10.2 Costs of ultrasonography The costs of all US examinations differ at each centre. In Isala in Zwolle, the Netherlands, where
this study is conducted, the costs of US are €412,- in the year 2015(43). The price depends on the
extent and duration of the examination.
1.11 Aim of this study
Because no consensus exists about the best way to diagnose CTS, probably a lot of unnecessary
examinations are conducted. This could be unpleasant and aggravating for patients and is not
cost-effective. In order to ascertain that the diagnosis CTS could be made by one test, the aim of
this study is to examine the sensitivity of US and NCS of the median nerve related to the clinical
symptoms in diagnosing CTS. Secondly, this study attempts to determine whether US alone can
be enough to diagnose CTS in patients with typical CTS symptoms.
1.12 Hypothesis
The first hypothesis is that US and NCS have a comparable sensitivity. The second hypothesis is
that in patients with clinical CTS, US could be enough to diagnose CTS and NCS would be
unnecessary.
18
2. Materials & Method
To determine whether US has a higher sensitivity than NCS and to determine whether US alone
can be enough to confirm the diagnosis in patients with clinical CTS, we studied 92 wrists in a
retrospective study.
2.1 Study design
For this study we used a database that was recorded in the period of December 2012 until
November 2015 in Isala in Zwolle, the Netherlands. The database consisted of 607 patients with
clinical CTS who are planned for CTR. Patients could be added twice to the database, if they
were planned for CTR on both hands. They were identified by patient number and ‘’left’’ of
‘’right’’. The patient characteristics were added to the database. All patients were seen before
surgery by a nurse who inquired about all the clinical symptoms.
2.2 Inclusion criteria
The inclusion criteria were: 1) ≥18 years of age; 2) underwent both US and NCS of the median
nerve; 3) both US and NCS outcome of the median nerve were known; 4) symptoms were noted.
2.3 Exclusion criteria
The exclusion criteria were: 1) previous CTS surgery on the same side; 2) wrist fracture/trauma
in history; 3) polyneuropathy; 4) diabetes mellitus; 5) cervical neuropathy; 6) pregnancy.
These exclusion criteria were used because of the probable influence of these disorders on the
development of CTS, as mentioned in section 1.3, or because the disorder could cause the same
symptoms, as in cervical neuropathy.
2.4 Further analysis
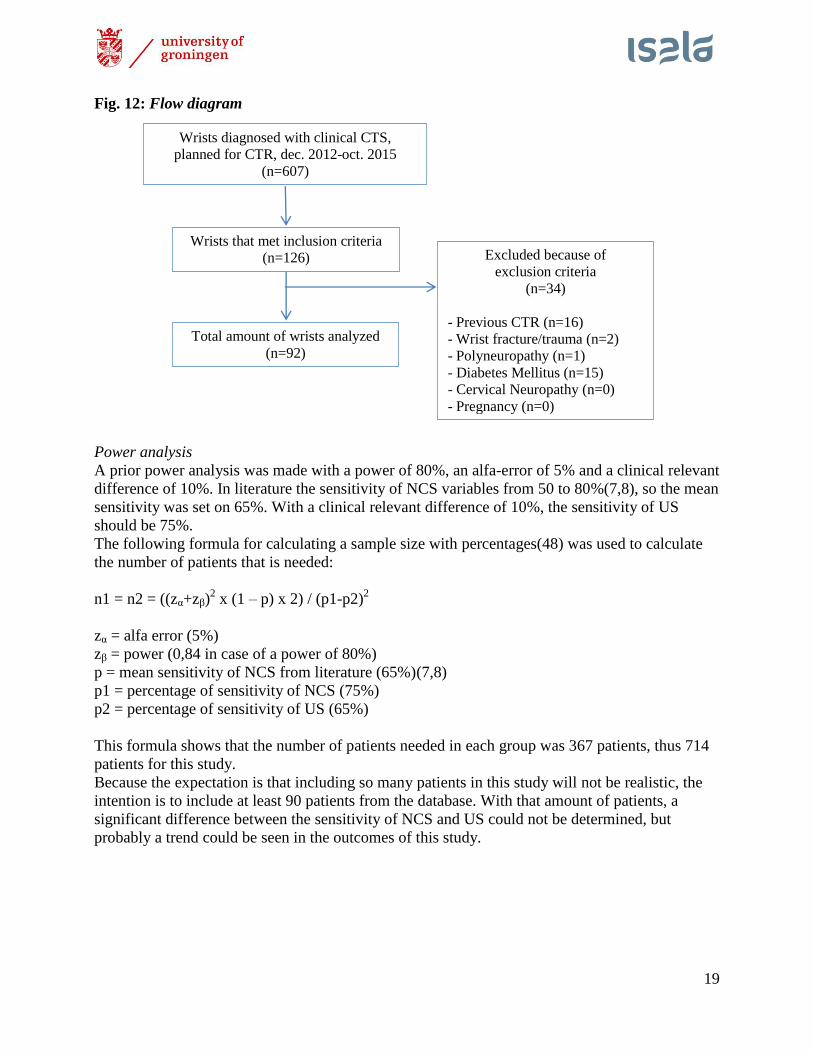
A total of 126 wrists met the inclusion criteria, however, 34 wrists were excluded; 16 because of
previous CTS surgery, 2 because of wrist fracture or trauma in history, 1 because of
polyneuropathy and 15 because of diabetes mellitus. A total of 92 wrists from 57 patients
remained (fig. 12). For these wrists, the outcomes of the US and NCS were retrieved from the
medical record and added to the database. Also the surgery outcome was added to the database.
The following variables were added:
Ultrasonography:
Cross-sectional area (CSA) of the median nerve in the carpal tunnel (in mm2).
Nerve conduction study:
Sensory latency time: latency difference between the median nerve and the ulnar nerve
and between the median nerve and the radial nerve (in milliseconds);
The speed difference between the sensory conduction of the median nerve in the palm of
the hand and the conduction of the median nerve in the wrist (SNCV) (in meter/second);
Motor latency time: latency difference between the median nerve and the ulnar nerve (in
milliseconds).
Surgery outcome:
Positive (patient was satisfied and experienced no more symptoms post-operative) or
negative (patient was dissatisfied and experienced still symptoms post-operative).
After completing the database, the database was exported to SPSS for analysis.
19
Fig. 12: Flow diagram
Power analysis
A prior power analysis was made with a power of 80%, an alfa-error of 5% and a clinical relevant
difference of 10%. In literature the sensitivity of NCS variables from 50 to 80%(7,8), so the mean
sensitivity was set on 65%. With a clinical relevant difference of 10%, the sensitivity of US
should be 75%.
The following formula for calculating a sample size with percentages(48) was used to calculate
the number of patients that is needed:
n1 = n2 = ((zα+zβ)2 x (1 – p) x 2) / (p1-p2)
2
zα = alfa error (5%)
zβ = power (0,84 in case of a power of 80%)
p = mean sensitivity of NCS from literature (65%)(7,8)
p1 = percentage of sensitivity of NCS (75%)
p2 = percentage of sensitivity of US (65%)
This formula shows that the number of patients needed in each group was 367 patients, thus 714
patients for this study.
Because the expectation is that including so many patients in this study will not be realistic, the
intention is to include at least 90 patients from the database. With that amount of patients, a
significant difference between the sensitivity of NCS and US could not be determined, but
probably a trend could be seen in the outcomes of this study.
Wrists diagnosed with clinical CTS,
planned for CTR, dec. 2012-oct. 2015
(n=607)
Wrists that met inclusion criteria
(n=126)
Total amount of wrists analyzed
(n=92)
Excluded because of
exclusion criteria
(n=34)
- Previous CTR (n=16)
- Wrist fracture/trauma (n=2)
- Polyneuropathy (n=1)
- Diabetes Mellitus (n=15)
- Cervical Neuropathy (n=0)
- Pregnancy (n=0)
20
2.5 Interventions
All patients included in this study have had ultrasonography, nerve conduction study and a carpal
tunnel release.
2.5.1 Ultrasonography
Ultrasonography was executed at the neurology department of the hospital by technicians of the
clinical neurophysiology department. The equipment used was the Philips iU22, NZE 934 with
the L16-4 nerve transducer for superficial measurement, at a frequency of 4,8MHz. The patient
was seated in front of the researcher with the forearm supinated. The wrist was positioned in
neutral position, with the fingers in normal resting position, which means in mild flexion at the
metacarpophalangeal joints and the proximal interphalangeal joints. The transducer was held
perpendicular to the median nerve and the median nerve was followed from proximal to distal,
from the forearm to the palm of the hand. At the level of the carpal tunnel, the biggest cross-
sectional area (CSA) of the median nerve was measured by using a continuous tracing method.
To measure the CSA of the median nerve properly, the area within the hyperechoic epineurium
was measured. The cut-off point for diagnosing CTS was ≥11,0 mm2. In order to not deform the
nerve, the researcher gave just enough pressure to bring the median nerve into vision.
2.5.2 Nerve Conduction Study
Nerve Conduction Study (NCS) was also performed at the neurology department of the hospital
by technicians of the clinical neurophysiology department. The equipment used was the Medelec
Synergy. The patient was seated in front of the researcher with the forearm supinated. The wrist
was positioned in neutral position. Patients were asked to try to keep their hands warm, for
example to wear gloves when they came to the hospital. The temperature of the hands was not
monitored, but when the hands felt cold they were warmed and all the tests were done at room
temperature. This was because it is suggested that when the skin temperature is below 30 degrees
Celsius, the conduction velocity decreases (see also section 1.9.3). The hands were degreased
before starting the procedure.
First the sensory latency time was measured. Two electrodes were placed on the fourth digit with
some gel between the skin and the electrodes for better conduction. The median nerve was
stimulated just proximal of the wrist and the sensory action potential is monitored on the
computer with special Medelec Synergy software. Then the ulnar nerve was stimulated just
proximal of the wrist and the latency time of this nerve was also monitored on the computer. The
software calculated the difference between the two nerve sensory latencies. A difference in
latencies larger than 0,4 milliseconds was abnormal.
The second measurement was the sensory latency difference between the median nerve and the
radial nerve. The two electrodes with some gel were placed on the first digit. The median nerve
and radial nerve were stimulated just proximal of the wrist. Again the latency times were
monitored on the computer and the software calculated the difference. A difference in latencies
larger than 0,4 milliseconds was abnormal.
The third measurement was the motor latency time. Two electrodes were placed; one on the distal
phalanx of the second digit and one in the palm of the hand. The median nerve was stimulated
proximal of the wrist. The amperage was increased until the monitored amplitude was at the
maximum. At that point, the motor latency time was monitored. Then the radial nerve was
stimulated proximal of the wrist till the monitored amplitude was at the maximum and the motor
latency time of the radial nerve was monitored. The difference between the two latencies was
calculated by the software. A difference in latencies larger than 0,4 milliseconds was abnormal.
21
The fourth measurement was not a standard measurement, but could be an additional
confirmation of the diagnosis. This measurement was the SNCV. It measured differences
between the proximal SNCV and the distal SNCV (proximal-distal ratio). Two electrodes were
placed on the third digit. Seven centimeter proximal of the most proximal electrode, the median
nerve was stimulated and the SNCV is monitored. Then fourteen centimeter proximal to the most
proximal electrode, the median nerve was stimulated and the SNCV was monitored. The
difference was again calculated by the software. The difference in SNCV’s was abnormal when
the velocity difference was more than 10,0 meter/second in the distal segment compared to the
proximal segment.
When two of the first three measurements were abnormal, the diagnosis CTS was set. So, if two
of the following three measurements were abnormal, the diagnosis CTS was set: the sensory
latency time difference between the median and ulnar nerve, the sensory latency time difference
between the median and radial nerve and/or the motor latency time difference between the
median and radial nerve. The SNCV of the proximal and distal ratio was an additional
measurement to confirm the diagnosis.
2.5.3 Surgery: Carpal Tunnel Release
The carpal tunnel releases (CTR) in the hospital where this study was conducted, was an open
CTR. The surgery took place as an outpatient surgery procedure and under local anaesthesia, with
lidocaine 1% with adrenaline. A pneumatic tourniquet was placed on the upper arm to control
bleeding. The hand and forearm were disinfected and were covered with sterile surgical drapes.
The incision was marked at the palmar side of the wrist, just distal to the wrist flexion crease,
with a length of three centimeters. The incision was located slightly ulnar to the midline of the
wrist, in line with the third web space. With a 15-scalpel the incision was made and the cutis and
subcutis were opened with use of a blunt scissor or mayo scissor and a tissue forceps. After that,
the wound was held open with a spreader and with a blunt hook. The flexor retinaculum was cut
to the distal and proximal side. The cutis was closed with 3.0 ethilon. In order to compress the
wound, it was bandaged with cotton wool and a swaddle for two days. Patients were advised to
start active movement of the fingers as soon as possible and to keep their hand high. The stitches
were removed after fourteen days.
At all the surgeries, an experienced plastic surgeon performed the surgery or was present at the
surgery, to make sure the procedure was well done, with a complete release of the flexor
retinaculum.
2.6 Cut-off points measurements
The cut-off points for the examinations are tabulated in table 2.
Table 2: Cut-off points examinations
Examination Cut-off point
Ultrasonography – CSA at carpal tunnel 11,0 mm2
NCS – Sensory latency time median-ulnar nerve Difference -0,4 ms
NCS – Sensory latency time median-radial nerve Difference -0,4 ms
NCS – Motor latency time 2nd
digit-palm Difference -0,4 ms
NCS – SNCV prox-dist ratio Difference 10,0 m/s
CSA: cross-sectional area; NCS: nerve conduction study; prox: proximal; dist: distal; SNCV: sensory
nerve conduction velocity; ms: milliseconds; m/s: meter/second.
22
2.7 Analysis of data
For the statistical analysis, IBM SPSS Statistics for Windows, version 23.0.0.0 (IBM Corp,
Armonk, NY) was used. To compare groups and to calculate the significance, the Student T-test,
Spearman test, Pearson test and Chi-square test were used.
In case of results with a normal distribution, the mean and standard deviation were mentioned.
When results were non-normally distributed, the median and interquartile range were mentioned.
Differences between normally distributed scale variables were analyzed with the independent
Student T-test. The Mann-Whitney U-test was used to analyze differences between non-normally
distributed scale variables or categorical variables. Correlation between scale and categorical
variables were analyzed with the Spearman test and correlations between categorical variables
were analyzed with the Pearson test. The Chi-square test was used to analyze correlations
between nominal variables or between nominal and categorical variables.
A p-value <0,05 was considered to be significant, with a confidence-interval of 95%.
2.8 Typical or atypical CTS Because recent literature suggests that nerve conduction studies could be unnecessary in typical
CTS(49), in this study difference was made between typical and atypical CTS in order to
determine whether or not the outcome found in this study corresponds with recent literature.
There are no specific symptoms mentioned in literature to call the diagnosis of CTS ‘’typical’’.
Mentioned in literature are symptoms like tingling, pain and diminished sensibility in the median
nerve area, a positive Tinel test and/or a positive Phalen test, as described in section 1.6, but no
criteria are set to call the diagnosis ‘’typical’’ CTS. After asking the plastic surgeons in the
hospital this study is conducted what they call typical clinical CTS, the diagnosis typical CTS
was set to be tingling in the median nerve distribution area. All other cases were diagnosed as
atypical CTS. Beside this, when other diagnosis were likely (e.g. ulnaropathy of the elbow or De
Quervain tenosynovitis), these patients were labeled as atypical CTS.
2.9 Surgery outcome
Because some literature suggests the diagnosis CTS could be made only post-operative, when
patient experience no more symptoms, the surgery outcome was analyzed in this study. The
outcome was retrieved from the medical record. There were three options: positive, negative or
unknown surgery outcome. In case of the positive surgery outcome, the patient was satisfied with
the result of the surgery and experienced no more symptoms post-operative. In case of the
negative surgery outcome, the patient was dissatisfied with the result of the surgery and
experienced still symptoms post-operative. When the surgery outcome could not be retrieved
from the medical record, this outcome was labeled as ‘’unknown’’.
2.10 Study outcomes The primary study outcomes are the outcomes of ultrasonography and nerve conduction study in
patients in the overall group, in the typical CTS group and in the atypical CTS group.
The secondary study outcome is the sensitivity of ultrasonography and nerve conduction study in
patients with clinical CTS. This is determined by analyzing the outcome of the ultrasonography
and the nerve conduction study in each patient.
23
3. Results
3.1 Patient characteristics in the overall CTS group (table 3)
A total of 92 wrists from 57 patients were analyzed (67 (72,8%) wrists of women), with an
average age of 51,4 years (±14,13 years, range 19 to 87 years). The age of men and women had
an average of 57,92 and 51,39 years, respectively (significant difference, p 0,041). Of all the
wrists, in 91,3% the right hand was dominant and in 51,1% the right hand was operated. The
duration of symptoms had a median of 16 months (interquartile range (IQR): 6-24 months).
Sixteen percent of the wrists had a conservative treatment before surgery, against 84% of the
wrists that underwent surgery. Fifteen patients in this study had co-morbidities: two patients had
rheumatoid arthritis, two patients osteoporosis, one patient thyroid gland disease, three patients
fibromyalgia, one patient gout, two patients breast cancer, two patients colon cancer and two
patients had osteoarthritis. The other 42 patients did not have co-morbidities. Of the 92 wrists, 56
(60,9%) wrists were from patients with a paid job. Of these wrists from patients with a paid job,
19 (33,9%) did light physical work like a office job, 35 (62,5%) did an intermediate physical job
like working in a store and 2 (3,6%) did heavy physical work like construction work. Except for
the age, there were no differences in patients characteristics between men and women (p > 0,05).
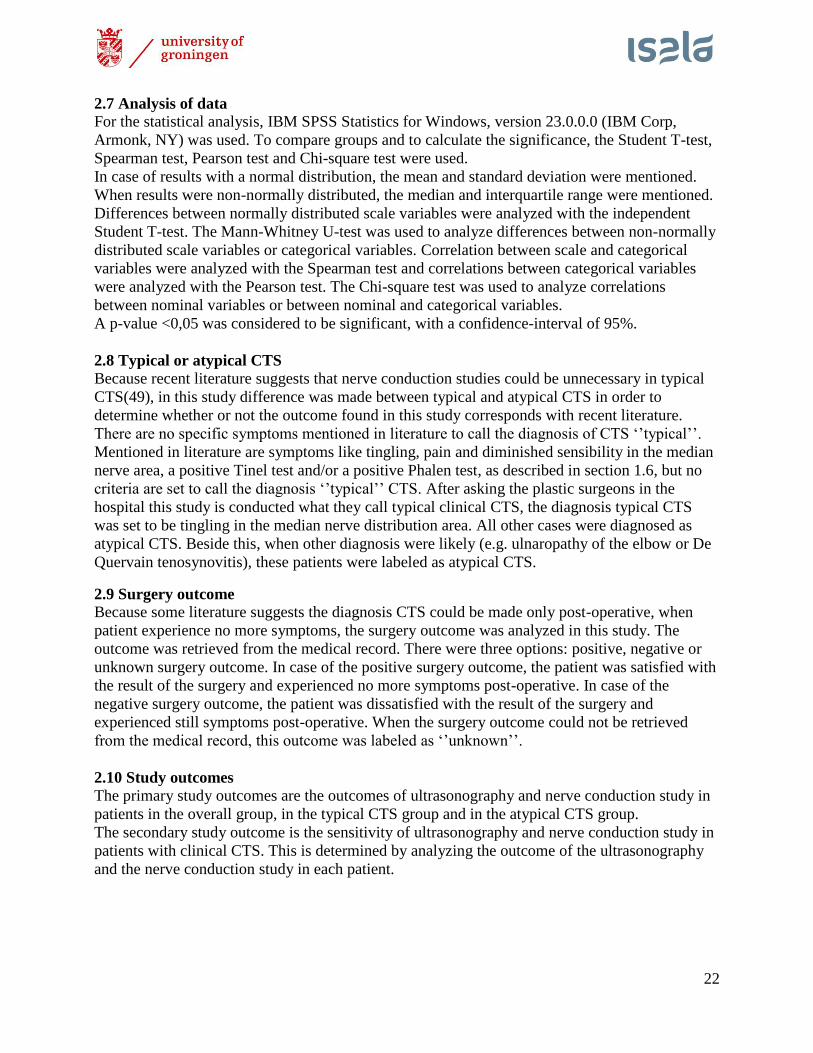
3.2 Patient characteristics in the typical and atypical CTS group (table 3)
Sixty wrists did met the criteria of typical CTS. In 6 wrists another diagnosis was likely, so 54
(57,7%) wrists remained in the typical CTS group and 38 (42,3%) wrists were added to the
atypical CTS group. There were no significant differences found in patient characteristics
between the typical and atypical CTS group.
Table 3: Patient characteristics
Variable All CTS
(n=92) Typical CTS
(n=54) Atypical CTS
(n=38) Sign (p)
Women, No. (%) 67 (72,8) 42 (77,8) 25 (65,8) 0,203
Age, mean (SD), y 53,16 (14,05) 53,37 (14,42) 52,87 (13,68) 0,867
Dominant right hand, No. (%) 84 (91,3) 47 (87,0) 37 (97,4) 0,083
Operated hand right, No. (%) 47 (51,1) 26 (48,1) 21 (55,3) 0,501
Duration of symptoms, median (IQR),
months 12 (6-24) 12 (6-24) 12 (5,75-24) 0,506
Conservative treatment, No. (%) 13 (14,1) 6 (11,1) 7 (18,4) 0,322
Paid job, No. (%) 56 (60,9) 34 (63,0) 22 (57,9) 0,624
Work, No. (%)
Light 19 (33,9) 12 (22,2) 6 (15,8) 0,444
Intermediate 35 (62,5) 21 (38,9) 14 (36,8) 0,842
Heavy 2 (3,6) 1 (1,9) 2 (5,3) 0,364
Sign : significance (significant difference when p <0,05)
24
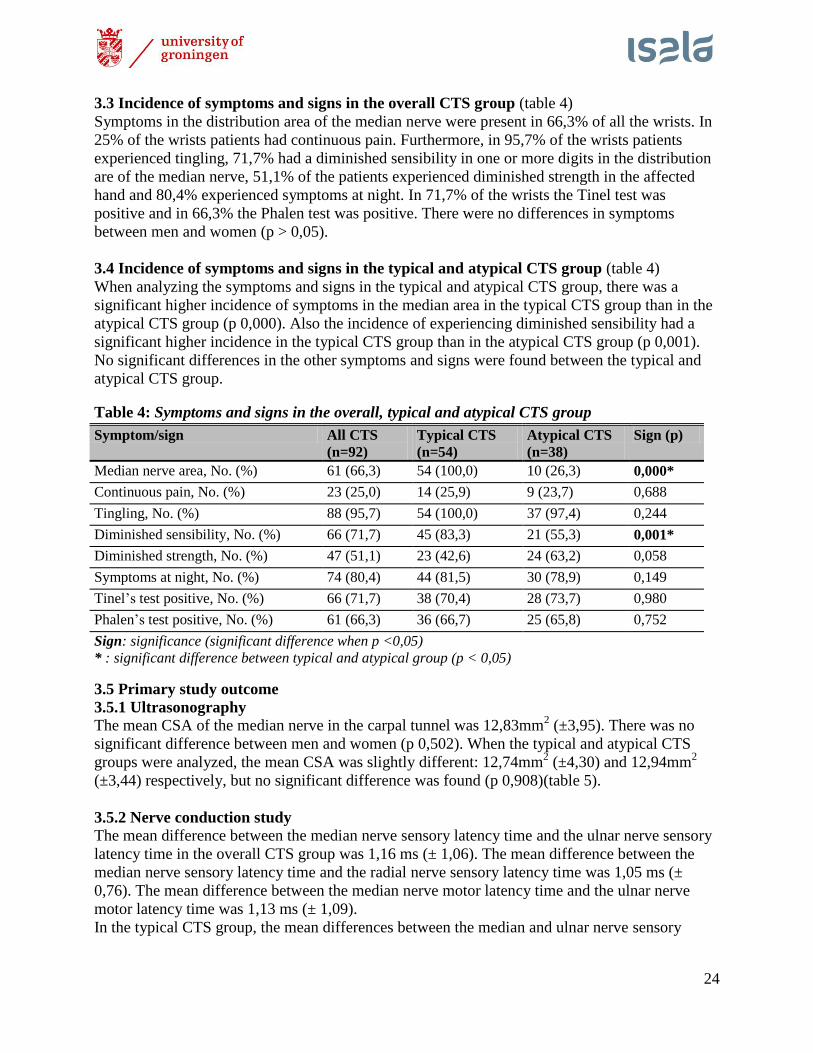
3.3 Incidence of symptoms and signs in the overall CTS group (table 4)
Symptoms in the distribution area of the median nerve were present in 66,3% of all the wrists. In
25% of the wrists patients had continuous pain. Furthermore, in 95,7% of the wrists patients
experienced tingling, 71,7% had a diminished sensibility in one or more digits in the distribution
are of the median nerve, 51,1% of the patients experienced diminished strength in the affected
hand and 80,4% experienced symptoms at night. In 71,7% of the wrists the Tinel test was
positive and in 66,3% the Phalen test was positive. There were no differences in symptoms
between men and women (p > 0,05).
3.4 Incidence of symptoms and signs in the typical and atypical CTS group (table 4)
When analyzing the symptoms and signs in the typical and atypical CTS group, there was a
significant higher incidence of symptoms in the median area in the typical CTS group than in the
atypical CTS group (p 0,000). Also the incidence of experiencing diminished sensibility had a
significant higher incidence in the typical CTS group than in the atypical CTS group (p 0,001).
No significant differences in the other symptoms and signs were found between the typical and
atypical CTS group.
3.5 Primary study outcome
3.5.1 Ultrasonography The mean CSA of the median nerve in the carpal tunnel was 12,83mm
2 (±3,95). There was no
significant difference between men and women (p 0,502). When the typical and atypical CTS
groups were analyzed, the mean CSA was slightly different: 12,74mm2 (±4,30) and 12,94mm
2
(±3,44) respectively, but no significant difference was found (p 0,908)(table 5).
3.5.2 Nerve conduction study
The mean difference between the median nerve sensory latency time and the ulnar nerve sensory
latency time in the overall CTS group was 1,16 ms (± 1,06). The mean difference between the
median nerve sensory latency time and the radial nerve sensory latency time was 1,05 ms (±
0,76). The mean difference between the median nerve motor latency time and the ulnar nerve
motor latency time was 1,13 ms (± 1,09).
In the typical CTS group, the mean differences between the median and ulnar nerve sensory
Table 4: Symptoms and signs in the overall, typical and atypical CTS group
Symptom/sign All CTS
(n=92) Typical CTS
(n=54) Atypical CTS
(n=38) Sign (p)
Median nerve area, No. (%) 61 (66,3) 54 (100,0) 10 (26,3) 0,000*
Continuous pain, No. (%) 23 (25,0) 14 (25,9) 9 (23,7) 0,688
Tingling, No. (%) 88 (95,7) 54 (100,0) 37 (97,4) 0,244
Diminished sensibility, No. (%) 66 (71,7) 45 (83,3) 21 (55,3) 0,001*
Diminished strength, No. (%) 47 (51,1) 23 (42,6) 24 (63,2) 0,058
Symptoms at night, No. (%) 74 (80,4) 44 (81,5) 30 (78,9) 0,149
Tinel’s test positive, No. (%) 66 (71,7) 38 (70,4) 28 (73,7) 0,980
Phalen’s test positive, No. (%) 61 (66,3) 36 (66,7) 25 (65,8) 0,752
Sign: significance (significant difference when p <0,05) * : significant difference between typical and atypical group (p < 0,05)
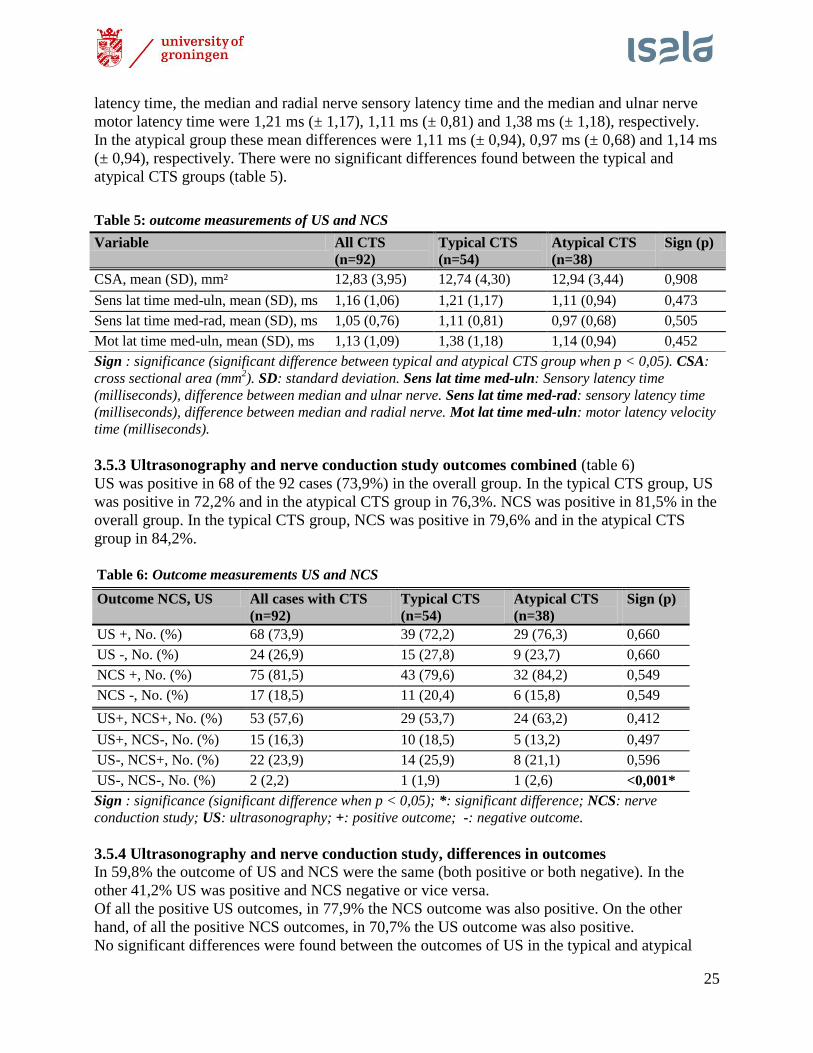
25
latency time, the median and radial nerve sensory latency time and the median and ulnar nerve
motor latency time were 1,21 ms (± 1,17), 1,11 ms (± 0,81) and 1,38 ms (± 1,18), respectively.
In the atypical group these mean differences were 1,11 ms (± 0,94), 0,97 ms (± 0,68) and 1,14 ms
(± 0,94), respectively. There were no significant differences found between the typical and
atypical CTS groups (table 5).
Sign : significance (significant difference between typical and atypical CTS group when p < 0,05). CSA:
cross sectional area (mm2). SD: standard deviation. Sens lat time med-uln: Sensory latency time
(milliseconds), difference between median and ulnar nerve. Sens lat time med-rad: sensory latency time
(milliseconds), difference between median and radial nerve. Mot lat time med-uln: motor latency velocity
time (milliseconds).
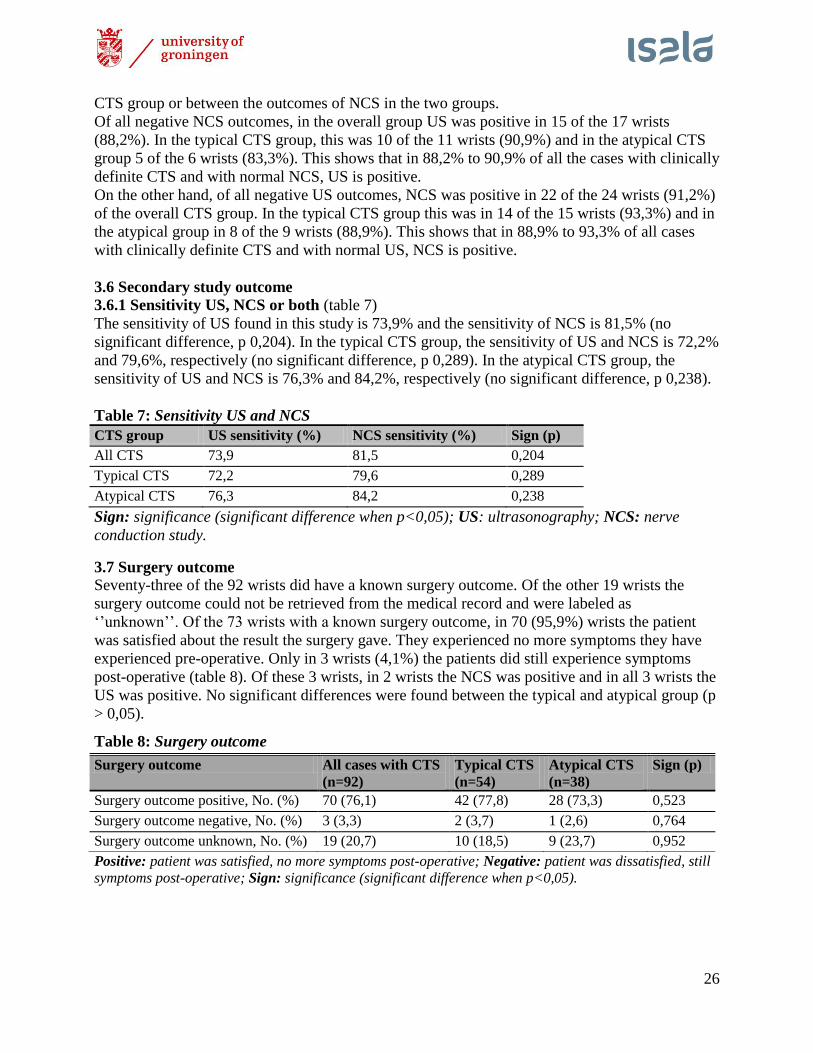
3.5.3 Ultrasonography and nerve conduction study outcomes combined (table 6)
US was positive in 68 of the 92 cases (73,9%) in the overall group. In the typical CTS group, US
was positive in 72,2% and in the atypical CTS group in 76,3%. NCS was positive in 81,5% in the
overall group. In the typical CTS group, NCS was positive in 79,6% and in the atypical CTS
group in 84,2%.
Table 6: Outcome measurements US and NCS
Outcome NCS, US All cases with CTS
(n=92) Typical CTS
(n=54) Atypical CTS
(n=38) Sign (p)
US +, No. (%) 68 (73,9) 39 (72,2) 29 (76,3) 0,660
US -, No. (%) 24 (26,9) 15 (27,8) 9 (23,7) 0,660
NCS +, No. (%) 75 (81,5) 43 (79,6) 32 (84,2) 0,549
NCS -, No. (%) 17 (18,5) 11 (20,4) 6 (15,8) 0,549
US+, NCS+, No. (%) 53 (57,6) 29 (53,7) 24 (63,2) 0,412
US+, NCS-, No. (%) 15 (16,3) 10 (18,5) 5 (13,2) 0,497
US-, NCS+, No. (%) 22 (23,9) 14 (25,9) 8 (21,1) 0,596
US-, NCS-, No. (%) 2 (2,2) 1 (1,9) 1 (2,6) <0,001*
Sign : significance (significant difference when p < 0,05); *: significant difference; NCS: nerve
conduction study; US: ultrasonography; +: positive outcome; -: negative outcome.
3.5.4 Ultrasonography and nerve conduction study, differences in outcomes In 59,8% the outcome of US and NCS were the same (both positive or both negative). In the
other 41,2% US was positive and NCS negative or vice versa.
Of all the positive US outcomes, in 77,9% the NCS outcome was also positive. On the other
hand, of all the positive NCS outcomes, in 70,7% the US outcome was also positive.
No significant differences were found between the outcomes of US in the typical and atypical
Table 5: outcome measurements of US and NCS
Variable All CTS
(n=92) Typical CTS
(n=54) Atypical CTS
(n=38) Sign (p)
CSA, mean (SD), mm² 12,83 (3,95) 12,74 (4,30) 12,94 (3,44) 0,908
Sens lat time med-uln, mean (SD), ms 1,16 (1,06) 1,21 (1,17) 1,11 (0,94) 0,473
Sens lat time med-rad, mean (SD), ms 1,05 (0,76) 1,11 (0,81) 0,97 (0,68) 0,505
Mot lat time med-uln, mean (SD), ms 1,13 (1,09) 1,38 (1,18) 1,14 (0,94) 0,452
26
CTS group or between the outcomes of NCS in the two groups.
Of all negative NCS outcomes, in the overall group US was positive in 15 of the 17 wrists
(88,2%). In the typical CTS group, this was 10 of the 11 wrists (90,9%) and in the atypical CTS
group 5 of the 6 wrists (83,3%). This shows that in 88,2% to 90,9% of all the cases with clinically
definite CTS and with normal NCS, US is positive.
On the other hand, of all negative US outcomes, NCS was positive in 22 of the 24 wrists (91,2%)
of the overall CTS group. In the typical CTS group this was in 14 of the 15 wrists (93,3%) and in
the atypical group in 8 of the 9 wrists (88,9%). This shows that in 88,9% to 93,3% of all cases
with clinically definite CTS and with normal US, NCS is positive.
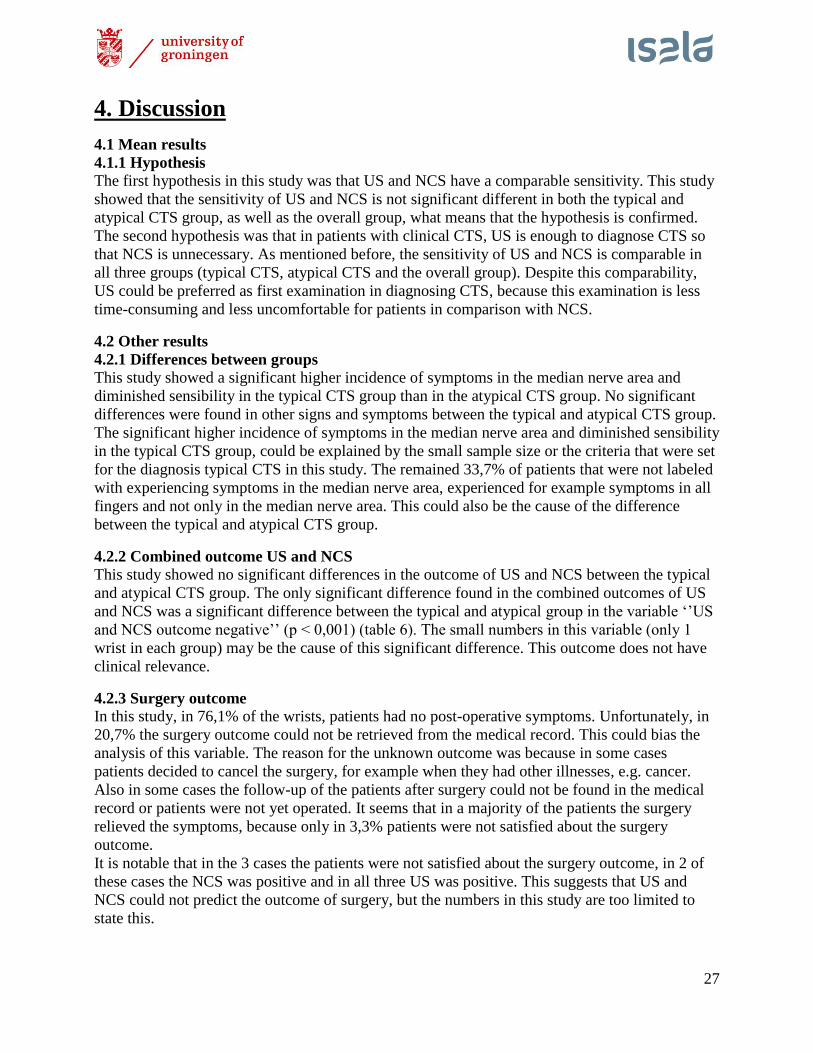
3.6 Secondary study outcome 3.6.1 Sensitivity US, NCS or both (table 7)
The sensitivity of US found in this study is 73,9% and the sensitivity of NCS is 81,5% (no
significant difference, p 0,204). In the typical CTS group, the sensitivity of US and NCS is 72,2%
and 79,6%, respectively (no significant difference, p 0,289). In the atypical CTS group, the
sensitivity of US and NCS is 76,3% and 84,2%, respectively (no significant difference, p 0,238).
Table 7: Sensitivity US and NCS
CTS group US sensitivity (%) NCS sensitivity (%) Sign (p)
All CTS 73,9 81,5 0,204
Typical CTS 72,2 79,6 0,289
Atypical CTS 76,3 84,2 0,238
Sign: significance (significant difference when p<0,05); US: ultrasonography; NCS: nerve
conduction study.
3.7 Surgery outcome
Seventy-three of the 92 wrists did have a known surgery outcome. Of the other 19 wrists the
surgery outcome could not be retrieved from the medical record and were labeled as
‘’unknown’’. Of the 73 wrists with a known surgery outcome, in 70 (95,9%) wrists the patient
was satisfied about the result the surgery gave. They experienced no more symptoms they have
experienced pre-operative. Only in 3 wrists (4,1%) the patients did still experience symptoms
post-operative (table 8). Of these 3 wrists, in 2 wrists the NCS was positive and in all 3 wrists the
US was positive. No significant differences were found between the typical and atypical group (p
> 0,05).
Positive: patient was satisfied, no more symptoms post-operative; Negative: patient was dissatisfied, still
symptoms post-operative; Sign: significance (significant difference when p<0,05).
Table 8: Surgery outcome
Surgery outcome All cases with CTS
(n=92) Typical CTS
(n=54) Atypical CTS
(n=38) Sign (p)
Surgery outcome positive, No. (%) 70 (76,1) 42 (77,8) 28 (73,3) 0,523
Surgery outcome negative, No. (%) 3 (3,3) 2 (3,7) 1 (2,6) 0,764
Surgery outcome unknown, No. (%) 19 (20,7) 10 (18,5) 9 (23,7) 0,952
27
4. Discussion
4.1 Mean results
4.1.1 Hypothesis
The first hypothesis in this study was that US and NCS have a comparable sensitivity. This study
showed that the sensitivity of US and NCS is not significant different in both the typical and
atypical CTS group, as well as the overall group, what means that the hypothesis is confirmed.
The second hypothesis was that in patients with clinical CTS, US is enough to diagnose CTS so
that NCS is unnecessary. As mentioned before, the sensitivity of US and NCS is comparable in
all three groups (typical CTS, atypical CTS and the overall group). Despite this comparability,
US could be preferred as first examination in diagnosing CTS, because this examination is less
time-consuming and less uncomfortable for patients in comparison with NCS.
4.2 Other results
4.2.1 Differences between groups
This study showed a significant higher incidence of symptoms in the median nerve area and
diminished sensibility in the typical CTS group than in the atypical CTS group. No significant
differences were found in other signs and symptoms between the typical and atypical CTS group.
The significant higher incidence of symptoms in the median nerve area and diminished sensibility
in the typical CTS group, could be explained by the small sample size or the criteria that were set
for the diagnosis typical CTS in this study. The remained 33,7% of patients that were not labeled
with experiencing symptoms in the median nerve area, experienced for example symptoms in all
fingers and not only in the median nerve area. This could also be the cause of the difference
between the typical and atypical CTS group.
4.2.2 Combined outcome US and NCS
This study showed no significant differences in the outcome of US and NCS between the typical
and atypical CTS group. The only significant difference found in the combined outcomes of US
and NCS was a significant difference between the typical and atypical group in the variable ‘’US
and NCS outcome negative’’ (p < 0,001) (table 6). The small numbers in this variable (only 1
wrist in each group) may be the cause of this significant difference. This outcome does not have
clinical relevance.
4.2.3 Surgery outcome
In this study, in 76,1% of the wrists, patients had no post-operative symptoms. Unfortunately, in
20,7% the surgery outcome could not be retrieved from the medical record. This could bias the
analysis of this variable. The reason for the unknown outcome was because in some cases
patients decided to cancel the surgery, for example when they had other illnesses, e.g. cancer.
Also in some cases the follow-up of the patients after surgery could not be found in the medical
record or patients were not yet operated. It seems that in a majority of the patients the surgery
relieved the symptoms, because only in 3,3% patients were not satisfied about the surgery
outcome.
It is notable that in the 3 cases the patients were not satisfied about the surgery outcome, in 2 of
these cases the NCS was positive and in all three US was positive. This suggests that US and
NCS could not predict the outcome of surgery, but the numbers in this study are too limited to
state this.
28
As mentioned before, some literature uses a post-operative diagnosis of CTS. In this study, this
means that in 76,1% the diagnosis CTS could be made, but in 20,7% the diagnosis could not be
made due to unknown surgery outcome. Therefore, this study could not be used to diagnose CTS
post-operative.
It should also be noticed that when the post-operative diagnosis is used, it could occur that patient
would undergone surgery unnecessarily. Because of this, the present study does not recommend
to use these criteria to diagnose CTS.
4.2.4 Costs
The outcome of this study suggests that NCS could be unnecessary as first examination to
confirm the diagnosis of CTS when the clinical diagnosis is set. This means that initially only US
could be performed instead of both NCS and US. Performing US only could lead to a decrease in
costs of €340,- for each patient that could be examined with US only. In this study, in 68 cases
US was positive. This suggests that in these 68 cases NCS should not have been performed to
confirm the clinical diagnose of CTS, what means a total of €23.120,- could have been saved. In
literature, only one study was found that describes the costs of US and NCS(34). In that study the
costs of NCS was $400,30 what is about €365,-. Although this is a comparable amount of money,
it is difficult to compare these costs because of changes in valuta value, inflation and differences
in costs between institutions.
Beside this, an ethical dilemma raises from this outcome. NCS costs less than US, but US is less
uncomfortable for patients. The question is what is more important: the costs of examinations or
the patient’s well-being. Another question could be: What is the maximum of costs that is
accepted for examinations? This study prefers to perform US, because in our opinion the small
difference in costs counts for little compared to the patient’s well-being.
4.3 Outcome of other studies about ultrasonography and nerve conduction study in
diagnosing CTS.
The present study showed that the sensitivity of US and NCS was comparable in both the typical
and atypical CTS group, as well as the overall group. This suggests that in patients with clinical
symptoms of CTS, US could be preferred as first examination for confirming the diagnosis CTS,
because this is less time-consuming and less uncomfortable for patients in comparison with NCS.
A recent study in The Netherlands from Kasius et al.(49), suggests that in patients with typical
CTS symptoms, such as tingling in the median nerve area, US can be used as first diagnostic tool.
When US outcome is negative, NCS can be used as second diagnostic tool. Kasius suggests that
in patients with typical CTS, which is 60% of the patients in her study, NCS does not need to be
performed to confirm the diagnosis of CTS. These findings are partly comparable with the
findings in the present study. Also other literature describes US as the preferred first examination
in diagnosing CTS(50-53).
The sensitivity of NCS found in this study was 79,6-84,2%. This is higher than found in literature
(56-85%, see section 1.9.3). The cause of this difference could be that in this study no difference
was made in the severity of CTS. It could be possible that in other studies a lot of patients were
included with mild CTS and in this study patients were included with more severe CTS. In
patients with mild CTS, the symptoms they experience could be due to damage to the small fibers
only and not (yet) the large fibers. These small fibers cannot be measured with NCS, only the
large fibers can be measured. This could lead to a normal NCS, although patients do experience
symptoms(54). This lowers the percentage of abnormal NCS outcomes and thus the sensitivity.
Furthermore, in this study in 88,2% of the 17 wrists in the overall CTS group with a negative
29
NCS outcome, US is positive. This is higher than described in other literature(55). El-Hashel
found that in patients with clinical definite CTS and with normal NCS, US was positive in
49%(55). This difference possibly could be explained by small sample sizes, differences in the
origin of patients or differences in the equipment that was used. The meaning of this outcome is
that US is recommended when NCS is negative, because in 88,2% to 90,9% the diagnosis CTS
can still be made.
Although US and NCS has a comparable sensitivity, US cannot be the only diagnostic tool for
CTS. In this study, in 2 cases US was negative and NCS was positive. In order not to miss the
diagnosis CTS in these patients, NCS should be performed as second examination when US is
negative.
4.4 Strengths of this study
A strength of this study is the comparison of NCS and US and the aim to say something about the
necessity of both examinations. In recent literature, a lot of studies are conducted about the use of
NCS and/or US, but fewer studies were conducted about the necessity of NCS in diagnosing
CTS.
4.5 Limitations of this study One limitation of this study was the small sample size. This could lead to a statistical bias with
less precise outcomes. It could occur that the sensitivity of US and NCS changes, when the
sample size is big enough. Further studies are needed to determine this.
Also the retrospective design was a limitation. Because of this retrospective design, the
information was searched from medical records. In some cases information about symptoms
missed in the medical record and this information could not always be retrieved.
Beside this, there was no control group to compare with the study group. All patients in this
database were diagnosed with clinical definite CTS, no healthy people were added to the
database. Because there was no control group, no specificity could be calculated. The specificity
in combination with the sensitivity, could say more about the accuracy of examinations. That is
because the specificity is the proportion of negative results of a test in patients who does not have
the disease. So it would be the proportion of healthy people who have a negative US and/or NCS.
To determine the specificity of US and NCS could be helpful in diagnosing CTS.
Furthermore, in this study different technicians performed the US and NCS examinations.
Although all the technicians have had the same education, differences in measurements could
occur. Beside this, the inter-rater reliability is not tested, because of the retrospective design.
Also only patients with an email address were added to the database. The reason for this was that
they were asked by mail to fill in questionnaires about their symptoms. Unfortunately these
questionnaires could not be used in this study, because of the lack of enough completed
questionnaires. People without an email address were not added to the database, which could lead
to a bias in the study population.
Another limitation is that only patients seen by a nurse were added to the database. Patients who
were seen directly by the plastic surgeon were not added. The reason for this was because of the
limited time plastic surgeons had to see a patient. This time was not enough to conduct all the
needed proceedings to add the patient to the database.
In order to collect a sample size that was as big as possible, patients with bilateral symptoms
were added with both wrists to the database, which is a limitation too. This could lead to a
statistical bias.
30
Also the fact that in this study typical CTS was defined as tingling in the median nerve
distribution area is a limitation. Because no clear criteria for typical CTS were described in
literature, the definition this study used was chosen after asking plastic surgeon what they thought
was typical CTS. The outcomes of this study, for example the sensitivity of US and NCS in
patients with typical CTS, could be different when using other criteria for typical CTS.
Finally, only patients with primary CTS were included in this study, so the value of US and NCS
in patients with recurrent CTS is not sure.
4.6 Recommended future study design Because the limitations of this study, further research is recommended. This future study should
be a prospective study with a large sample size and with a control group. Patients with clinical
CTS and healthy patients should be examined with US and NCS. There should be a limited
amount of technicians to conduct these examinations. In order to make sure the technicians
measure the same outcomes, the interrater reliability should be analyzed. All technicians should
perform the examinations blinded for the outcome of earlier (clinical) examinations in order not
to influence their outcome.
Furthermore, not only patients with an email address or patients seen by a nurse should be
selected, but all patients who have clinical diagnosis of CTS seen in the clinic. In order to collect
a large sample size, the study could be conducted in different hospitals.
Beside this, there should be a guideline about how to perform US. This guideline should give
exact indications about, for example, the location of measuring the CSA and the cut-off point of
the CSA.
The exact location for measuring the CSA of the median nerve should be determined. In literature
there is a lot of controversy about this (50-53). The most used location for measuring the CSA is
the pissiform, also named the carpal tunnel inlet(6,8,14,28,29,32,42,46). The reason for this is
that when the CSA is measured at other locations in the wrist the values were too heterogeneous
to determine one cut-off point(32). Also, the low inter-reader reliability of measuring the CSA of
the carpal tunnel outlet (the hook of the hamatum(56)) is described in literature(57), what could
be a reason for not choosing the carpal tunnel outlet as location for measuring the CSA of the
median nerve. Furthermore, it is difficult to measure the exactly CSA of the median nerve at the
location of the carpal tunnel outlet, because of the distance between the skin and the median
nerve. At the level of the carpal tunnel inlet, the median nerve is located relative superficial, what
makes it easier to determine the CSA. In contrast with this, at the carpal tunnel outlet, the median
nerve is located deeper underneath other structures such as fat and muscles. Because of this, the
CSA is difficult to measure at the carpal tunnel outlet and the measurement is less reliable.
The cut-off point of the CSA of the median nerve in the carpal tunnel is also a point of
controversy in the literature. This varies from 6,0mm2 to 16,0mm
2(11,52). The most recent study
(2014) suggests that the best cut-off point for the CSA of the median nerve, located at the carpal
tunnel inlet, is 10,5mm2(52). Further studies are needed to determine the best cut-off point. In
these studies the differences in CSA between races should be taken into account, because it is
known there is a difference in normal CSA between races(58).
Furthermore, there should be an international guideline for performing NCS. Although there are
just little differences between, for example, the American and Dutch guideline(35), these small
differences could lead to other outcomes of the examination. This aggravates the comparison of
different international studies.
Also, there are no clear criteria for diagnosing CTS. These criteria should be international the
same. When all studies use the same criteria, this could contribute to the knowledge about, for

31
example, US and NCS, because all these studies could be compared. Nowadays, a lot of different
criteria are used and this hinders the comparison of different international studies. Clear criteria
for diagnosing CTS with clinical symptoms should be made, but also the difference between
typical and atypical CTS or the use of post-operative diagnosis should be studied.
Finally, because in this study only patients with primary CTS were included, no conclusions
could be made about the values of US and NCS in patients with recurrent CTS. The value of NCS
and US for diagnosing recurrent CTS should be determined in future studies.
4.7 Further recommendations
A point of interest is the use of a questionnaire to determine whether or not a patient has clinical
definite CTS or ‘’typical’’ CTS, before executing any examinations. By making an inventory of
the symptoms that patients experience, the diagnosis of clinical CTS could be made. This could
be helpful in deciding to execute first US alone, in order not to load patients unnecessary. An
example of this is the Six-item Carpal Tunnel Syndrome symptom scale (CTS-6)(59)(see also:
appendix). This validated questionnaire is developed by Brent Graham(59). It combines data
from the history and data from the physical examination in order to predict the outcome of
electrodiagnostic testing(45). Graham suggested that, in patients with a positive CTS-6, the pre-
test probability of having CTS is that high, that it makes electrodiagnostic testing
unnecessary(59). Fowler confirmed this with his study(45). Fowler found in his study also that
most physician consider patients with a positive CTS-6 as ‘’typical CTS’’, so this indicates that
this questionnaire could be helpful in differentiate between typical or atypical CTS. This
questionnaire could be used to set the clinical diagnose of CTS and this could help in making the
decision to perform only US. Although the outcome of Graham’s study was promising, there is a
lot of controversy about the value of provocative tests in literature(60-63). Two provocative tests
are used in the CTS-6: Phalen’s test and Tinel’s test. Further studies are thus needed to confirm
the functioning of this questionnaire and to examine the value of the provocative tests.
32
5. Conclusion In conclusion, this present study showed that the sensitivity of US and NCS is not significant
different in both the typical and atypical CTS group, as well as the overall group. Although there
was not a significant difference between US and NCS, US could be preferred as first examination
to confirm the diagnosis CTS, because this examination is less uncomfortable for patients and
less time-consuming in comparison with NCS. Further prospective and blinded studies are
needed to confirm these outcomes.

33
6. Bibliography
(1) Paliwal PR, Therimadasamy AK, Chan YC, Wilder-Smith EP. Does measuring the median
nerve at the carpal tunnel outlet improve ultrasound CTS diagnosis? J Neurol Sci 2014 Apr
15;339(1-2):47-51.
(2) American Academy of Orthopedic Surgeons. Clinical practice guidelines on diagnosis of
carpal tunnel syndrome. 1st ed. Rosemont: American Academy of Orthopedic Surgeons. 2007.
(3) Paget J. The first description of carpal tunnel syndrome. J Hand Surg Eur Vol 2007
Apr;32(2):195-197.
(4) Chammas M, Boretto J, Burmann LM, Ramos RM, Dos Santos Neto FC, Silva JB. Carpal
tunnel syndrome - Part I (anatomy, physiology, etiology and diagnosis). Rev Bras Ortop 2014
Aug 20;49(5):429-436.
(5) Phalen GS. The carpal-tunnel syndrome. Seventeen years' experience in diagnosis and
treatment of six hundred fifty-four hands. J Bone Joint Surg Am 1966 Mar;48(2):211-228.
(6) Roll SC, Case-Smith J, Evans KD. Diagnostic accuracy of ultrasonography vs.
electromyography in carpal tunnel syndrome: a systematic review of literature. Ultrasound Med
Biol 2011 Oct;37(10):1539-1553.
(7) de Jesus Filho AG, do Nascimento BF, Amorim Mde C, Naus RA, Loures Ede A, Moratelli
L. Comparative study between physical examination, electroneuromyography and
ultrasonography in diagnosing carpal tunnel syndrome. Rev Bras Ortop 2014 Sep 16;49(5):446-
451.
(8) Ghasemi-Rad M, Nosair E, Vegh A, Mohammadi A, Akkad A, Lesha E, et al. A handy
review of carpal tunnel syndrome: From anatomy to diagnosis and treatment. World J Radiol
2014 Jun 28;6(6):284-300.
(9) Werthel JD, Zhao C, An KN, Amadio PC. Carpal tunnel syndrome pathophysiology: role of
subsynovial connective tissue. J Wrist Surg 2014 Nov;3(4):220-226.
(10) de Krom MC, Knipschild PG, Kester AD, Thijs CT, Boekkooi PF, Spaans F. Carpal tunnel
syndrome: prevalence in the general population. J Clin Epidemiol 1992 Apr;45(4):373-376.
(11) Descatha A, Huard L, Aubert F, Barbato B, Gorand O, Chastang JF. Meta-analysis on the
performance of sonography for the diagnosis of carpal tunnel syndrome. Semin Arthritis Rheum
2012 Jun;41(6):914-922.
(12) National Institute of Neurological Disorders and Stroke. Carpal Tunnel Syndrome Fact
Sheet. NIH Publication No. 12-4898. 2015.
(13) Jones O. The Carpal Tunnel. 2015; Available at: www.teachmeanatomy.info.
34
(14) Tajika T, Kobayashi T, Yamamoto A, Kaneko T, Takagishi K. Diagnostic utility of
sonography and correlation between sonographic and clinical findings in patients with carpal
tunnel syndrome. J Ultrasound Med 2013 Nov;32(11):1987-1993.
(15) Roll SC, Evans KD, Li X, Freimer M, Sommerich CM. Screening for carpal tunnel
syndrome using sonography. J Ultrasound Med 2011 Dec;30(12):1657-1667.
(16) Jordan R, Carter T, Cummins C. A systematic review of the utility of electrodiagnostic
testing in carpal tunnel syndrome. Br J Gen Pract 2002 Aug;52(481):670-673.
(17) Baker NA, Livengood HM. Symptom severity and conservative treatment for carpal tunnel
syndrome in association with eventual carpal tunnel release. J Hand Surg Am 2014
Sep;39(9):1792-1798.
(18) Viera AJ. Management of carpal tunnel syndrome. Am Fam Physician 2003 Jul
15;68(2):265-272.
(19) Gerritsen AA, de Vet HC, Scholten RJ, Bertelsmann FW, de Krom MC, Bouter LM.
Splinting vs surgery in the treatment of carpal tunnel syndrome: a randomized controlled trial.
JAMA 2002 Sep 11;288(10):1245-1251.
(20) Gerritsen AA, Uitdehaag BM, van Geldere D, Scholten RJ, de Vet HC, Bouter LM.
Systematic review of randomized clinical trials of surgical treatment for carpal tunnel syndrome.
Br J Surg 2001 Oct;88(10):1285-1295.
(21) Vasiliadis HS, Georgoulas P, Shrier I, Salanti G, Scholten RJ. Endoscopic release for carpal
tunnel syndrome. Cochrane Database Syst Rev 2014 Jan 31;1:CD008265.
(22) Atroshi I, Hofer M, Larsson GU, Ranstam J. Extended Follow-up of a Randomized Clinical
Trial of Open vs Endoscopic Release Surgery for Carpal Tunnel Syndrome. JAMA 2015 Oct
6;314(13):1399-1401.
(23) Badger SA, O'Donnell ME, Sherigar JM, Connolly P, Spence RA. Open carpal tunnel
release--still a safe and effective operation. Ulster Med J 2008 Jan;77(1):22-24.
(24) Dudley Porras AF, Rojo Alaminos P, Vinuales JI, Ruiz Villamanan MA. Value of
electrodiagnostic tests in carpal tunnel syndrome. J Hand Surg Br 2000 Aug;25(4):361-365.
(25) Kaymak B, Ozcakar L, Cetin A, Candan Cetin M, Akinci A, Hascelik Z. A comparison of
the benefits of sonography and electrophysiologic measurements as predictors of symptom
severity and functional status in patients with carpal tunnel syndrome. Arch Phys Med Rehabil
2008 Apr;89(4):743-748.
(26) Cartwright MS, Hobson-Webb LD, Boon AJ, Alter KE, Hunt CH, Flores VH, et al.
Evidence-based guideline: neuromuscular ultrasound for the diagnosis of carpal tunnel syndrome.
Muscle Nerve 2012 Aug;46(2):287-293.
35
(27) El Miedany YM, Aty SA, Ashour S. Ultrasonography versus nerve conduction study in
patients with carpal tunnel syndrome: substantive or complementary tests? Rheumatology
(Oxford) 2004 Jul;43(7):887-895.
(28) Pastare D, Therimadasamy AK, Lee E, Wilder-Smith EP. Sonography versus nerve
conduction studies in patients referred with a clinical diagnosis of carpal tunnel syndrome. J Clin
Ultrasound 2009 Sep;37(7):389-393.
(29) Rahmani M, Ghasemi Esfe AR, Vaziri-Bozorg SM, Mazloumi M, Khalilzadeh O, Kahnouji
H. The ultrasonographic correlates of carpal tunnel syndrome in patients with normal
electrodiagnostic tests. Radiol Med 2011 Apr;116(3):489-496.
(30) Dineen JM, Greenberg SA. What role for ultrasound in diagnosing carpal tunnel syndrome?
Pract Neurol 2014 Oct;14(5):286-287.
(31) Ghasemi M, Abrishamchi F, Basiri K, Meamar R, Rezvani M. Can we define severity of
carpal tunnel syndrome by ultrasound? Adv Biomed Res 2015 Jul 27;4:138-9175.161537.
eCollection 2015.
(32) Tai TW, Wu CY, Su FC, Chern TC, Jou IM. Ultrasonography for diagnosing carpal tunnel
syndrome: a meta-analysis of diagnostic test accuracy. Ultrasound Med Biol 2012
Jul;38(7):1121-1128.
(33) Fowler JR, Cipolli W, Hanson T. A Comparison of Three Diagnostic Tests for Carpal
Tunnel Syndrome Using Latent Class Analysis. J Bone Joint Surg Am 2015 Dec 2;97(23):1958-
1961.
(34) Fowler JR, Maltenfort MG, Ilyas AM. Ultrasound as a first-line test in the diagnosis of
carpal tunnel syndrome: a cost-effectiveness analysis. Clin Orthop Relat Res 2013
Mar;471(3):932-937.
(35) Nederlandse Vereniging voor Neurologie. CBO-richtlijng - Diagnostiek en behandeling van
het carpale-tunnel syndroom. 2005.
(36) Werner RA, Andary M. Electrodiagnostic evaluation of carpal tunnel syndrome. Muscle
Nerve 2011;44(4):597-607.
(37) Jablecki CK, Andary MT, So YT, Wilkins DE, Williams FH. Literature review of the
usefulness of nerve conduction studies and electromyography for the evaluation of patients with
carpal tunnel syndrome. AAEM Quality Assurance Committee. Muscle Nerve 1993
Dec;16(12):1392-1414.
(38) Sunderland S. The anatomy and physiology of nerve injury. Muscle Nerve 1990
Sep;13(9):771-784.
36
(39) Jablecki CK, Andary MT, Floeter MK, Miller RG, Quartly CA, Vennix MJ, et al. Practice
parameter: Electrodiagnostic studies in carpal tunnel syndrome. Report of the American
Association of Electrodiagnostic Medicine, American Academy of Neurology, and the American
Academy of Physical Medicine and Rehabilitation. Neurology 2002 Jun 11;58(11):1589-1592.
(40) Daube JR, Rubin DI. Needle electromyography. Muscle Nerve 2009 Feb;39(2):244-270.
(41) Becker SJ, Makanji HS, Ring D. Changes in treatment plan for carpal tunnel syndrome
based on electrodiagnostic test results. J Hand Surg Eur Vol 2014 Feb;39(2):187-193.
(42) Fowler JR, Gaughan JP, Ilyas AM. The sensitivity and specificity of ultrasound for the
diagnosis of carpal tunnel syndrome: a meta-analysis. Clin Orthop Relat Res 2011
Apr;469(4):1089-1094.
(43) Isala Klinieken Zwolle. Passantenprijslijst Isala 2015. 2015.
(44) Finsen V, Russwurm H. Neurophysiology not required before surgery for typical carpal
tunnel syndrome. J Hand Surg Br 2001 Feb;26(1):61-64.
(45) Fowler JR, Munsch M, Tosti R, Hagberg WC, Imbriglia JE. Comparison of ultrasound and
electrodiagnostic testing for diagnosis of carpal tunnel syndrome: study using a validated clinical
tool as the reference standard. J Bone Joint Surg Am 2014 Sep 3;96(17):e148.
(46) Visser LH, Smidt MH, Lee ML. High-resolution sonography versus EMG in the diagnosis of
carpal tunnel syndrome. J Neurol Neurosurg Psychiatry 2008 Jan;79(1):63-67.
(47) Klauser AS, Abd Ellah MM, Halpern EJ, Siedentopf C, Auer T, Eberle G, et al. Sonographic
cross-sectional area measurement in carpal tunnel syndrome patients: can delta and ratio
calculations predict severity compared to nerve conduction studies? Eur Radiol 2015
Aug;25(8):2419-2427.
(48) Twisk JWR. Inleiding in de toegepaste biostatistiek, section 8.3 Een dichotome
uitkomstvariabele. . 2nd ed. Amsterdam: Elsevier gezondheidszorg; 2010. p. 279-282.
(49) Kasius KM. Part II: Ultrasonography. An Alternative or Additional Test to Nerve
Conduction Studies? Diagnostic considerations in carpal tunnel syndrome. Amsterdam: VUmc;
2015. p. 97.
(50) Azami A, Maleki N, Anari H, Iranparvar Alamdari M, Kalantarhormozi M, Tavosi Z. The
diagnostic value of ultrasound compared with nerve conduction velocity in carpal tunnel
syndrome. Int J Rheum Dis 2014 Jul;17(6):612-620.
(51) McDonagh C, Alexander M, Kane D. The role of ultrasound in the diagnosis and
management of carpal tunnel syndrome: a new paradigm. Rheumatology (Oxford) 2015
Jan;54(1):9-19.
37
(52) Sarraf P, Malek M, Ghajarzadeh M, Miri S, Parhizgar E, Emami-Razavi SZ. The best cutoff
point for median nerve cross sectional area at the level of carpal tunnel inlet. Acta Med Iran
2014;52(8):613-618.
(53) Kanikannan MA, Boddu DB, Umamahesh, Sarva S, Durga P, Borgohain R. Comparison of
high-resolution sonography and electrophysiology in the diagnosis of carpal tunnel syndrome.
Ann Indian Acad Neurol 2015 Apr-Jun;18(2):219-225.
(54) Tamburin S, Cacciatori C, Praitano ML, Cazzarolli C, Foscato C, Fiaschi A, et al. Median
nerve small- and large-fiber damage in carpal tunnel syndrome: a quantitative sensory testing
study. J Pain 2011 Feb;12(2):205-212.
(55) Al-Hashel JY, Rashad HM, Nouh MR, Amro HA, Khuraibet AJ, Shamov T, et al.
Sonography in carpal tunnel syndrome with normal nerve conduction studies. Muscle Nerve 2015
Apr;51(4):592-597.
(56) Fu T, Cao M, Liu F, Zhu J, Ye D, Feng X, et al. Carpal tunnel syndrome assessment with
ultrasonography: value of inlet-to-outlet median nerve area ratio in patients versus healthy
volunteers. PLoS One 2015 Jan 24;10(1):e0116777.
(57) Moran L, Perez M, Esteban A, Bellon J, Arranz B, del Cerro M. Sonographic measurement
of cross-sectional area of the median nerve in the diagnosis of carpal tunnel syndrome:
correlation with nerve conduction studies. J Clin Ultrasound 2009 Mar-Apr;37(3):125-131.
(58) Burg EW, Bathala L, Visser LH. Difference in normal values of median nerve cross-
sectional area between Dutch and Indian subjects. Muscle Nerve 2014 Jul;50(1):129-132.
(59) Graham B. The value added by electrodiagnostic testing in the diagnosis of carpal tunnel
syndrome. J Bone Joint Surg Am 2008 Dec;90(12):2587-2593.
(60) Ansari NN, Adelmanesh F, Naghdi S, Mousavi S. The relationship between symptoms,
clinical tests and nerve conduction study findings in carpal tunnel syndrome. Electromyogr Clin
Neurophysiol 2009 Jan-Feb;49(1):53-57.
(61) D'Arcy CA, McGee S. The rational clinical examination. Does this patient have carpal
tunnel syndrome? JAMA 2000 Jun 21;283(23):3110-3117.
(62) Bozek M, Gazdzik TS. The value of clinical examination in the diagnosis of carpal tunnel
syndrome. Ortop Traumatol Rehabil 2001 Jul-Sep;3(3):357-360.
(63) Bruske J, Bednarski M, Grzelec H, Zyluk A. The usefulness of the Phalen test and the
Hoffmann-Tinel sign in the diagnosis of carpal tunnel syndrome. Acta Orthop Belg 2002
Apr;68(2):141-145.
38
7. Appendix
7.1 CTS-6 (Six-item CTS symptom scale) form
The CTS-6 form(57) can be used when clinical diagnosing CTS. The clinician determines which
symptoms the patient experience.
A ‘’positive’’ CTS-6, which is at a total score of 12 points or more, corresponds to a pre-test
probability of CTS of approximately 0.80. When the score was below 5, the pretest probability
was about 0.25. In patients with a positive CTS-6, the pre-test probability of having CTS is that
high, that it makes electrodiagnostic testing unnecessary.

39





























