Embed Size (px)
Citation preview

Diabetic Ketoacidosis in ChildrenAn Intensivist’s Perspective for the Emergency Medicine Provider
September 12, 2020
Ashwin Krishna MD, MPH, FAAPAssistant Professor of PediatricsPICU/PCU Medical DirectorUniversity of Kentucky College of MedicineKentucky Children’s Hospital

I have no financial disclosures or conflicts of interest to report
Disclosure

• Epidemiology, Pathophysiology and Definition
• Risk Factors for Life Threatening Disease
• KCH DKA guideline
• Role of the Community Hospital Provider
Overview

• Leading cause of morbidity and mortality in patients with Type 1 Diabetes Mellitus (T1DM)
• Occurs at the time of diagnosis in 30% of Children in US and Canada
• Risk factors for DKA as initial presentation of T1DM:• Age <5 yo (heightened risk in age <2yo)• Low SES• Ethnic minorities (black, latinx, Native American)
• Occurs in 6-8% of Children with known T1DM per year
• Risk factors for DKA with known T1DM:• Poor glycemic/metabolic control• Immediate Hx gastroenteritis or other intercurrent illness• Peripubertal adolescents (F>M)• Hx psychiatric disorders• Low SES• Non-compliance to insulin regimen pump or SQ injection • Corticosteroid or atypical antipsychotic use
• Can occur in children with T2DM• Lower incidence than in patients with T1DM• Can present with mixed picture—DKA + hyperglycemic hyperosmolar state (HHS)
DKA
Kao KT, Islam N, Fox DA, Amed S. Incidence Trends of Diabetic Ketoacidosis in Children and Adolescents with Type 1 Diabetes in British Columbia, Canada. J Pediatr 2020; 221:165.Usher-Smith JA, Thompson MJ, Sharp SJ, Walter FM. Factors associated with the presence of diabetic ketoacidosis at diagnosis of diabetes in children and young adults: a systematic review. BMJ 2011; 343:d4092.
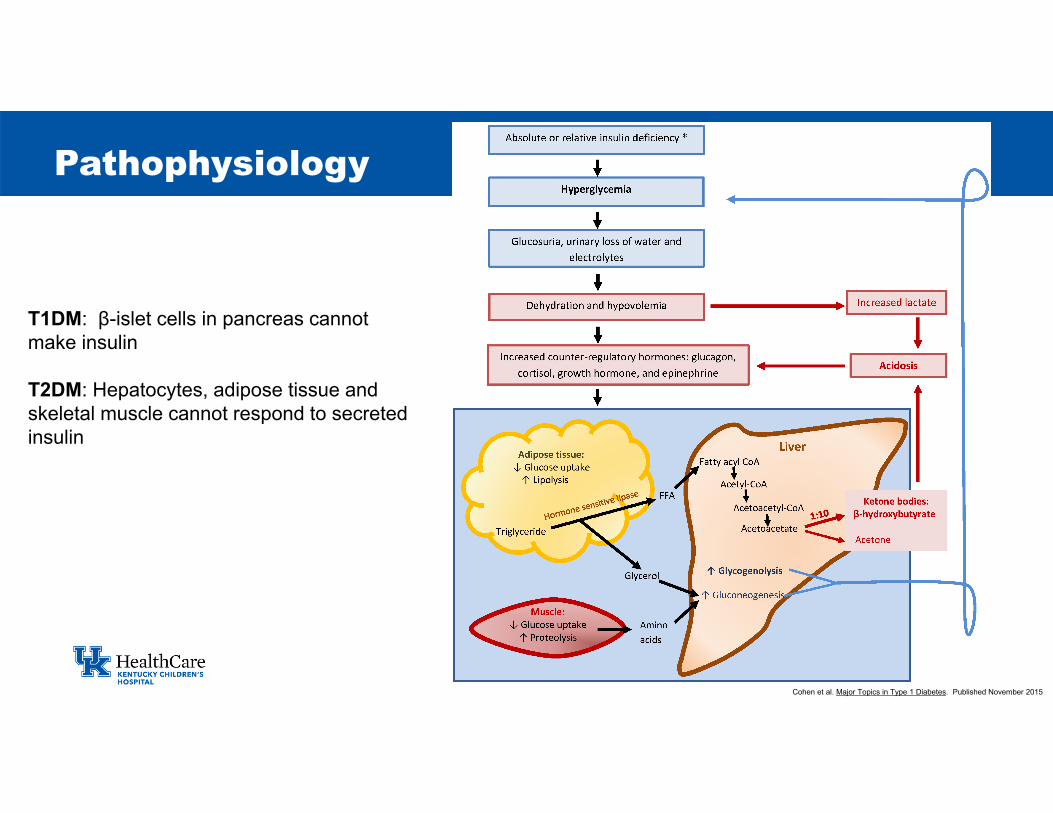
Pathophysiology
T1DM: β-islet cells in pancreas cannotmake insulin
T2DM: Hepatocytes, adipose tissue andskeletal muscle cannot respond to secretedinsulin
Cohen et al. Major Topics in Type 1 Diabetes. Published November 2015

DKA• Hyperglycemia—Serum Glucose
>200 mg/dL (11mmol/L)• Metabolic Acidosis with elevated
anion gap• Venous pH <7.30 OR • Serum bicarbonate <15mEq/L
• Ketosis—presence of ketones in the blood
• BOHB>3mmol/L• Urine ketones of moderate/large is
sufficient in the presence of the other 2 criteria
HHS• Severe hyperglycemia—Serum
glucose>600mg/dL (>33.3mmol/L)• Mild acidosis
• Venous pH >7.25• NO elevated anion gap
• Absent or very mild ketosis• Marked elevation in serum
osmolality (>320mOsm/L)
Definition of DKA
Zeitler P, Haqq A, Rosenbloom A, et al. Hyperglycemic hyperosmolar syndrome in children: pathophysiological considerations and suggested guidelines for treatment. J Pediatr 2011; 158:9.Wolfsdorf JI, Glaser N, Agus M, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Pediatr Diabetes 2018; 19 Suppl 27:155.

Anion Gap= (Serum Na+) – (Cl- + HCO3-)
Serum Osmolality= 2(Serum Na+) + (BUN/2.7) + (Glucose/18)
MUDPILESMethanol Tox.UremiaDKAParaldehyde/phenforminINH/Iron ToxLactic AcidosisEthylene GlycolSalicylates
Some quick calculations

• Fluid status—generally have 5-10% fluid deficit• Reasonable to assume 7% fluid deficit in moderate/severe DKA• Measure weight loss from pre-illness status
• Acidosis • Mild DKA pH 7.2-7.3• Moderate DKA pH 7.1-7.19• Severe DKA pH <7.1
DKA—Fluid Status and Acidosis

DKA—Ketones and Electrolytes
KetonesSerum BOHB—most accurate clinical test for ketosis Urine Ketones—can confirm presence but not severityAnion Gap—useful surrogate if BOHB not available. Abnormal ≥15
ElectrolytesSodium deficit almost always present, but serum sodium concentrations can vary
Hyperglycemia increases serum osmolalitywater moves to extracellular space via osmotic gradientNa+ diluted Glucosuria induces osmotic diuresisincreased water lossraises serum sodium
Potassium deficit though levels are usually normal or highK moves into extracellular space Insulin (when you start it) moves K intracellularly so anticipate replacement
Phosphate balance negative due to poor diet and decreased intake—however often normal levels in serum
Osmotic diuresis causes phosphaturiaInsulin (when you start it) moves Phos intracellularly so anticipate replacement

• Polyuria—presents differently at different ages• Polydipsia• Weight loss
• Anorexia (initially)• Nausea/Vomiting• Abdominal Pain
• Candida infections • Hyperventilation—compensation for metabolic acidosis
• Tachypnea • Deep, heaving breaths (Kussmaul Respirations)• Ketone breath
• Dehydration• Tachycardia• Poor perfusion• Decreased skin turgor
• Mental Status Change (late)• Drowsiness• Lethargy• Coma
DKA—Presentation
Considerations/Red Flags• New onset enuresis in apreviously toilet trained child
• Younger children may not have apparent polyuria/polydipsia if they are not toilet trained
• Dehydrated patients don’t have polyuria!!!
Wolfsdorf JI, Glaser N, Agus M, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Pediatr Diabetes 2018; 19 Suppl 27:155.
Assessment of the DKA Patient• ABCs• Vital Signs• Mental Status • Evaluate for Evidence of Infection• Obtain weight—compare with pre-
illness weight if possible• Labs:
• Fingerstick Glucose• VBG—assess severity of acidosis• BOHB—best direct test• Urine Ketones• Full chemistry panel, including phos
Treatment of the DKA Patient• Gentle isotonic volume
expansion (limit fluid bolus to 10-20mg/kg) based on fluid status
• Initiation of an insulin infusion (.05-0.1u/kg/hr)
• Initiation of hourly fluids at supramaintenance but not excessive rate
Initial Assessment and Treatment

• 1% of children with DKA• 40-70% mortality• Most common cause of death from Diabetes
This Study:• Retrospective Case Control • 61 patients identified with Cerebral Edema and DKA• 174 Matched controls by age, sex, new onset vs known• 181 randomly selected controls
Other Risk Factors• Overadministration of fluid (>50ml/kg in first 4hrs)• Age <5yo • New onset T1DM
DKA—Cerebral Edema
RISK FACTORS FOR CEREBRAL EDEMA IN CHILDREN WITH DIABETIC KETOACIDOSISN Engl J Med, Vol. 344, No. 4
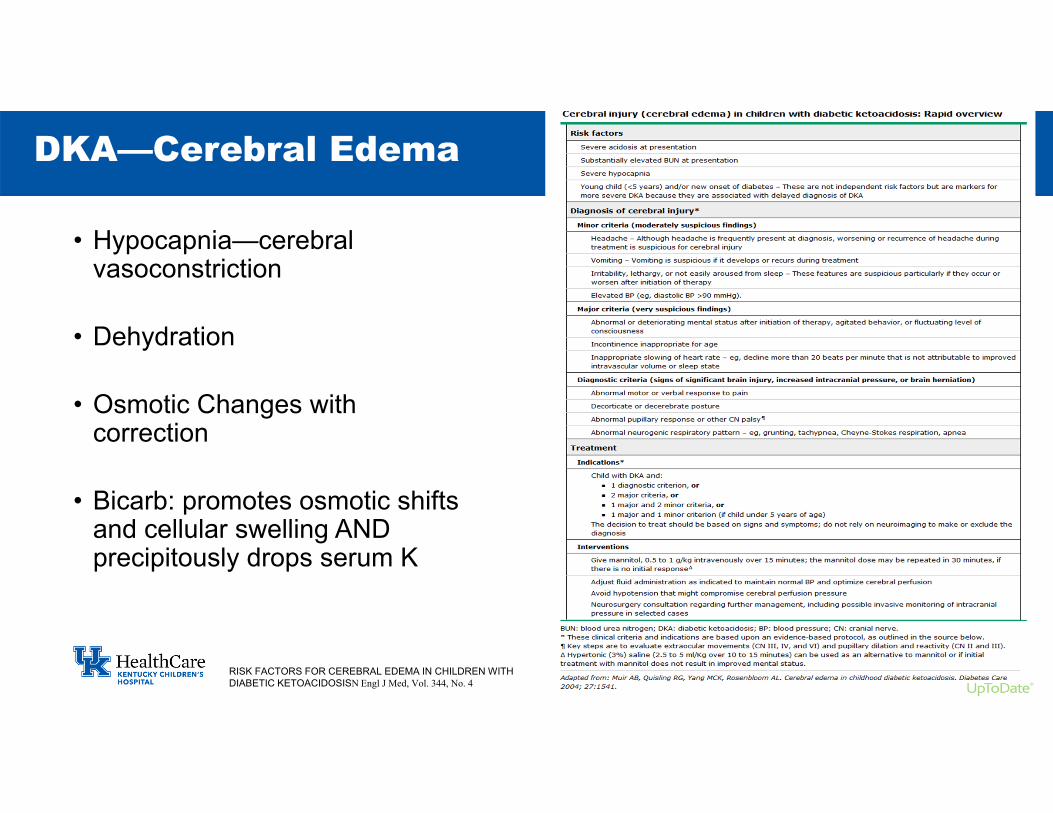
• Hypocapnia—cerebral vasoconstriction
• Dehydration
• Osmotic Changes with correction
• Bicarb: promotes osmotic shifts and cellular swelling AND precipitously drops serum K
DKA—Cerebral Edema
RISK FACTORS FOR CEREBRAL EDEMA IN CHILDREN WITH DIABETIC KETOACIDOSISN Engl J Med, Vol. 344, No. 4

DKA—Cerebral Edema
• Multi-center RCT
• 1389 DKA admissions
• Children were randomly assigned to one of four treatment groups in a 2-by-2 factorial design
• 0.9% NaCl vs 0.45% NaCl solution• Rapid versus Slow administration
• No Differences in complications or cerebral edema for either the fluids or rate of replacement
RISK FACTORS FOR CEREBRAL EDEMA IN CHILDREN WITH DIABETIC KETOACIDOSISN Engl J Med, Vol. 344, No. 4

• First KCH guideline created 2014• Revised in 2019• Reviewed by Critical Care and Endocrinology teams at KCH
Goal: Prevent complications with either aggressive correction or administration of therapeutics with a high risk of CE
DKA at KCH
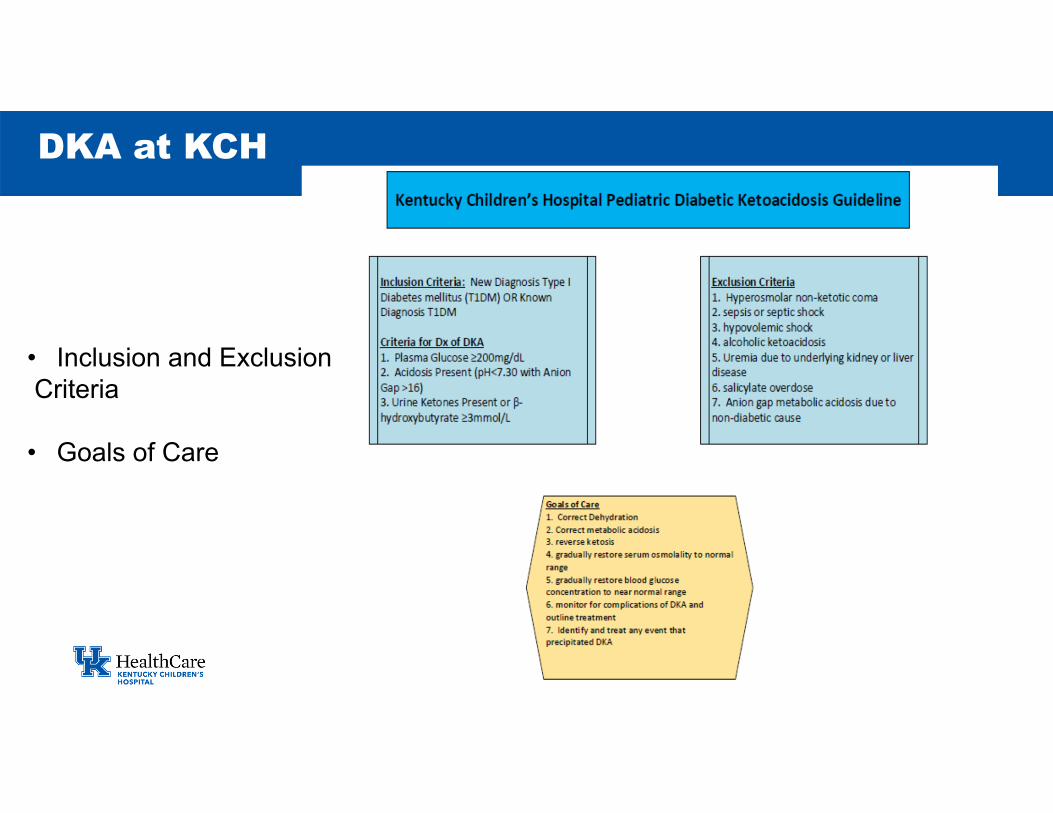
DKA at KCH
• Inclusion and ExclusionCriteria
• Goals of Care


DKA at KCH

DKA at KCH

DKA at KCH—Management
• Insulin Drip (.05-0.1unit/kg/hr)
• 2 bag system• Without dextrose• With dextrose
• 1.5x Maintenance• 40/20/10 rule • For adult sized patients canrun at 150ml/hr
• Q1h fingerstick glucose• Repeat BMP in 4 hours if noK in fluids• Q8h labs otherwise or thereafter
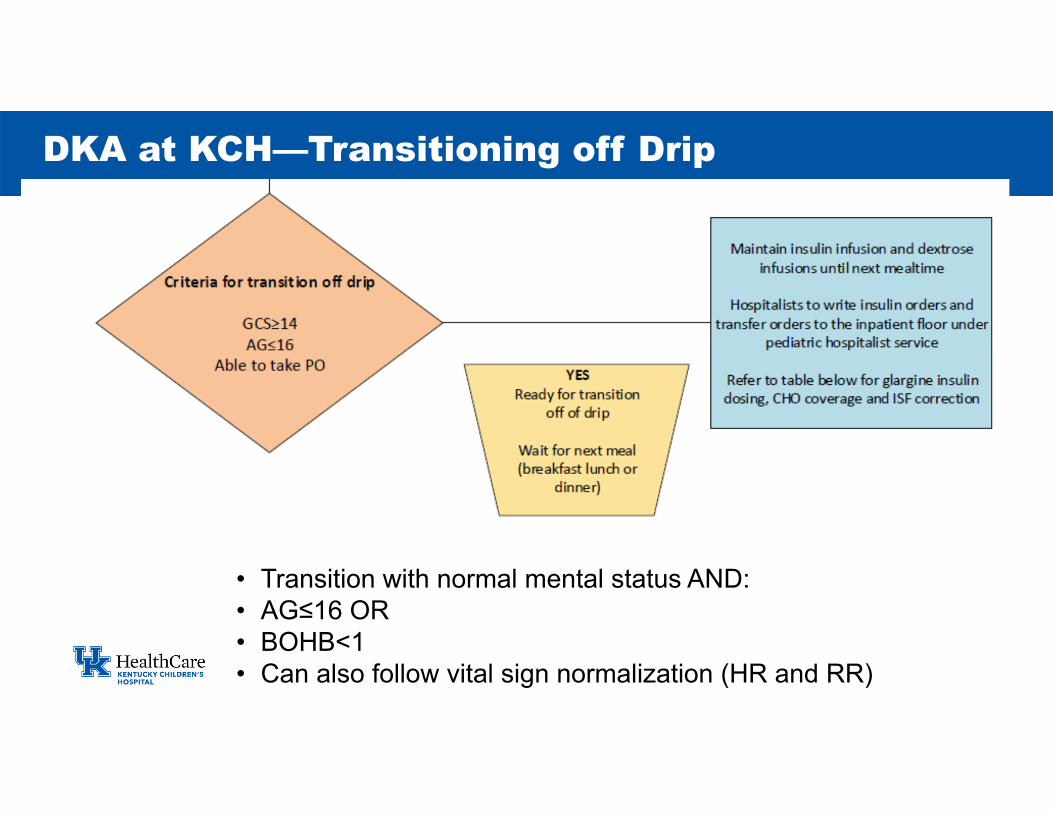
DKA at KCH—Transitioning off Drip
• Transition with normal mental status AND:• AG≤16 OR• BOHB<1• Can also follow vital sign normalization (HR and RR)

DKA—Transitioning off drip

• Data reporting metrics
• Revision every 3-4 years based on new evidence
• Bedside BOHB testing—fingerstick + rapid turnaround time
• Outreach—We want to sync our practice with community providers
Future Plans with DKA
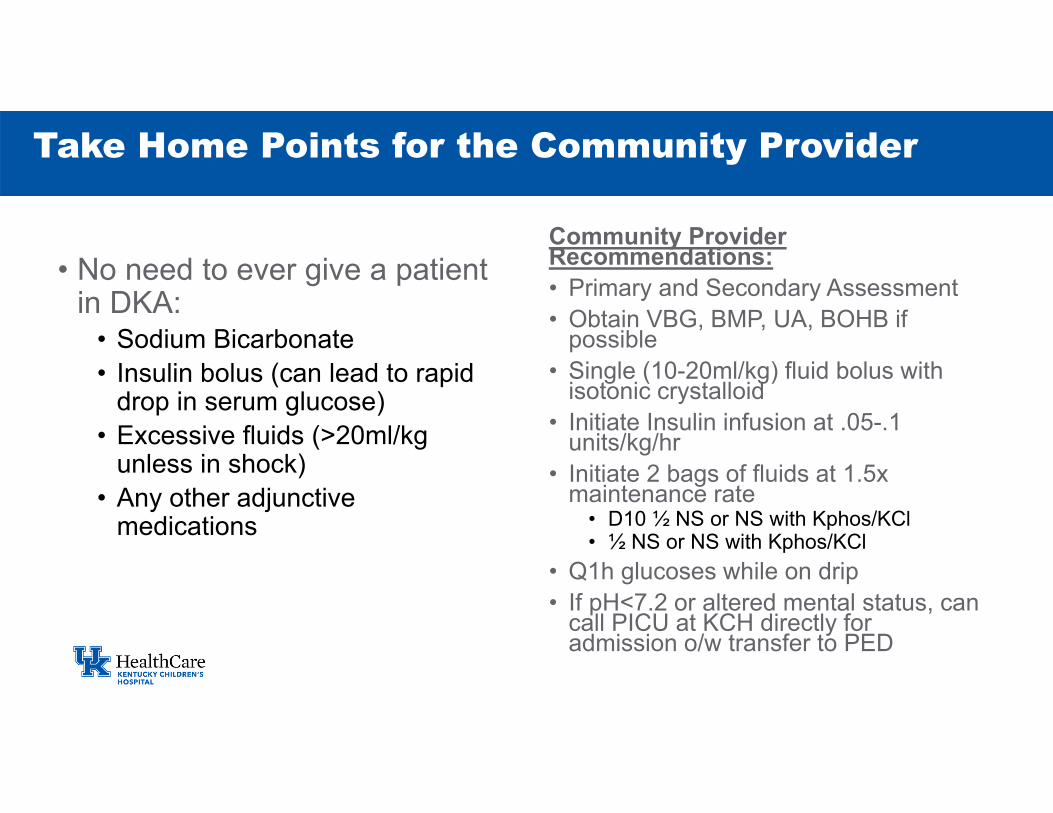
• No need to ever give a patient in DKA:
• Sodium Bicarbonate• Insulin bolus (can lead to rapid
drop in serum glucose) • Excessive fluids (>20ml/kg
unless in shock)• Any other adjunctive
medications
Community Provider Recommendations:• Primary and Secondary Assessment• Obtain VBG, BMP, UA, BOHB if
possible• Single (10-20ml/kg) fluid bolus with
isotonic crystalloid• Initiate Insulin infusion at .05-.1
units/kg/hr• Initiate 2 bags of fluids at 1.5x
maintenance rate• D10 ½ NS or NS with Kphos/KCl• ½ NS or NS with Kphos/KCl
• Q1h glucoses while on drip• If pH<7.2 or altered mental status, can
call PICU at KCH directly for admission o/w transfer to PED
Take Home Points for the Community Provider

Thanks





















