-
8/11/2019 Diabetes Dan Usia Lanjut
1/39
Diabetes dan usialanjut
-
8/11/2019 Diabetes Dan Usia Lanjut
2/39
Sasaran Belajar
Describe an approach to the clinical care of diabetes and
comorbid conditions in older adults
Assess the special needs of diabetes management in
the elderly
Indicate the drug selection criteria for older adults with
diabetes
-
8/11/2019 Diabetes Dan Usia Lanjut
3/39
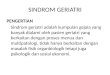
1972 2010 2020
5.3 million
(4.48% of the total
population)
23.99 million
(9.9% of the total
population)
28.82 million
(11.34% of the total
population)
1. Indonesian Ministry of Social Affairs. 2002.
2. ADA. Complete Nurses Guide to Diabetes Care. Second Edition.
2009.
Age is a risk factor for developing diabetes2
Undiagnosed and untreated diabetes is more commonin the elderly
than in any other age group2
Trend in Older Population in Indonesia
(Age 60+)1
-
8/11/2019 Diabetes Dan Usia Lanjut
4/39
0
2
4
6
8
10
12
14
15 - 24 th 25 - 34 th 35 - 44 th 45 - 54 th 55 - 64 th 65 - 74
th 75 keatas
0,6%1.8
5
10.5
13.514
12.5
PREVALENSI DM PERKOTAAN BERDASARKAN KELOMPOK UMUR
(RISKESDAS 2007)
4,9%
6,4%
PREVALENSI DM PERKOTAAN BERDASARKAN JENIS
KELAMIN (RISKESDAS 2007)
Laki-laki
Perempua
n
DM PREVALENCE BY AGE GROUP
DM PREVALENCE BY GENDER
Men
Women
-
8/11/2019 Diabetes Dan Usia Lanjut
5/39
Older Adults with Diabetes: Risks
Higher rates of premature death, functional disability,
coexisting illness (e.g. hypertension, CHD, stroke)
Greater risk for polypharmacy, depression, cognitiveimpairment,
urinary incontinence, injurious fall, and
persistent pain
Standards of Medical Care in Diabetes. Diabetes
Care2012;35(suppl 1) Jan 2012.
-
8/11/2019 Diabetes Dan Usia Lanjut
6/39
Diagnosis: Long-term vs. recent, substantial vs. no
complications, with range of physical and cognitive
functioning
Can have significant functional impairment or be very
active with no complications
Life expectancies variable but often longer than
clinicians realize
Older Adults with Diabetes:
Not All the Same
Standards of Medical Care in Diabetes. Diabetes
Care2012;35(suppl 1) Jan 2012.
-
8/11/2019 Diabetes Dan Usia Lanjut
7/39CDC. Available at:
http://www.cdc.gov/diabetes/statistics/dmany/fig4.htm.
0-44 years
45-64 years
65-74 years
75+ years
500
600
700
800
900
1000
0
100
200
300
400
80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00
01 02 03
Year
Rate(per
1000Diabetic
Population)
Risk of Hospitalization Among People
with Diabetes Increases with Age
-
8/11/2019 Diabetes Dan Usia Lanjut
8/39
Most elderly patients with diabetes have T2DM
Pathogenesis of T2DM in older patients is similar to
other age groups
Pathophysiology and Rationale for
Treatment
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
9/39
Coexisting
illness
Age-related
decreased
insulin secretion
Age-related
insulin
resistance
Adiposity
Decreased physical
activity
Genetics
Drugs
Factors
predisposing
the elderly to
diabetes
Factors Predisposing Older Adults to the Development of
Diabetes
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
10/39
Approach to Therapy
Goal: Prevent metabolic decompensation + control risk
factors for CVD
Control hypertension, lipid disorders, smoking
Treat severe hyperglycemia To control fatty acid mobilization
and oxidation, protein
catabolism/muscle wasting, excessive glucose production,
urinary loss of calories in the form of glucose
Standards of Medical Care in Diabetes. Diabetes
Care2012;35(suppl 1) Jan 2012.
-
8/11/2019 Diabetes Dan Usia Lanjut
11/39
Considerations
Patients life expectancy
Patient commitment
Availability of support services
Economic issues Coexisting health problems
Complexity of medical regimen
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition.
2009ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
12/39
Healthy adult with reasonable life expectancy:
FG 100-130 mg/dl
PG
-
8/11/2019 Diabetes Dan Usia Lanjut
13/39
Nutrition Therapy
Weight reduction = better control of hyperglycemia
Barriers: Lifelong dietary habits; changes in taste, smell,
vision; neurological or muscular disorders; chewing and
swallowing difficulties; cost
Poor eating habits due to cost and difficulty shopping are
common
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
14/39
Nutrition Therapy
Goal of MNT: Meet nutritional needs; keep blood
glucose, blood pressure, blood lipids as close to normal
as possible
Dietician can be helpful to set up and maintain
appropriate diet
MNT= medical nutrition therapy
ADA. Complete Nurses Guide to Diabetes Care. 2ndEdition.
2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
15/39
Exercise in Older Diabetic Patients
Exercise is beneficial in all ages
Recommend: Exercise tolerance test, supervision,
proper footwear
Important to minimize risk of hypoglycemia
ADA. Therapy for Diabetes Mellitus and Related
Disorders. 5thEdition. 2009
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
16/39
Exercise in Older Diabetic Patients
Intensity must match patients physical fitness level
Stationary bike
Walking
Water aerobics
Exercise videos Armchair fitness
ADA. Complete Nurses Guide to Diabetes Care.
Second Edition.2009
ADA. Complete Nurses Guide to Diabetes Care. 2ndEdition.
2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
17/39
Physiologic Changes in the Elderly
Neurological
Ophthalmologic
Body composition
Gastrointestinal
Hepatic
Renal
Endocrine
ADA. Complete Nurses Guide to Diabetes Care.
Second Edition.2009
ADA. Complete NursesGuide to Diabetes Care. 2ndEdition.
2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
18/39
Hypoglycemic Drugs Other than Insulin
Start with small dose and increase slowly
Combination therapy: Limited evidence in older patients;
weigh benefits versus risks and adherence problems
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
19/39
Hypoglycemic Drugs Other than Insulin
Oral drugs can cause hypoglycemia
Renal and hepatic insufficiency risk factors for severe
hypoglycemia
If hypoglycemia occurs, observation required, especially
with long-acting agents
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
20/39
Hypoglycemic Drugs Other than Insulin
Sulfonylureas: Risk for hypoglycemia low if nutrition isgood and
no major renal and hepatic insufficiency
Avoid chlorpropamide and glyburide because of
hypoglycemia risk
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
21/39
Approach to Therapy
Metformin contraindicated with renal insufficiency orsignificant
heart failure
TZDs can cause fluid retention (contraindicated in CHF)
Sulfonylureas, other insulin secretagogues, and insulincan cause
hypoglycemia
Standards of Medical Care in Diabetes. Diabetes
Care2012;35(suppl 1) Jan 2012.
CHF= congestive heart failure
-
8/11/2019 Diabetes Dan Usia Lanjut
22/39
-
8/11/2019 Diabetes Dan Usia Lanjut
23/39
Insulin
Consider insulin when goals not met by weight
reduction,exercise, or other glucose-lowering drugs
Simple insulin regimen preferred
No contraindications to use
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
24/39
Insulin
Insulin use requires good visual, motor, and cognitiveskills
Can the patient administer insulin?
If not, can caregiver administer?
Insulin pen?
Patient and/or caregiver must be trained in self-
monitoring of BG
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
-
8/11/2019 Diabetes Dan Usia Lanjut
25/39
Impaired autonomic nervous system function
Impaired counter-regulatory responses
Poor nutrition
Cognitive disorder
Use of alcohol or sedating agent
Polypharmacy
Kidney or liver failure
ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition.
2009ADA. Therapy for Diabetes Mellitus and Related Disorders.
5thEdition. 2009.
Potential Risk Factors for Hypoglycemia
in Older Patients
-
8/11/2019 Diabetes Dan Usia Lanjut
26/39
After age 60, patient visits often decrease because thereis no
one to take the patient to the doctor
More homecare services by primary care doctors are
needed to address this gap in care:
Determine goals of therapy
Monitor glucose control
Special Issues: Access to Care
-
8/11/2019 Diabetes Dan Usia Lanjut
27/39
Older adults who are functional, cognitively intact and/or
with significant life expectancies should receive diabetes
care using goals developed for younger adults
Glycemic goals for those not meeting the above criteria
may be relaxed, but avoid hyperglycemia leading to
symptoms or risk of acute hyperglycemic complications
Recommendations: Older Adults
Standards of Medical Care in Diabetes. Diabetes
Care2012;35(suppl 1) Jan 2012.
-
8/11/2019 Diabetes Dan Usia Lanjut
28/39
Greater reductions in morbidity and mortality may result
from the control of CVD risk factors rather than tight
glycemic controls alone
Evidence supports treatment of hypertension; less
evidence for lipid-lowering and aspirin therapy
Individualize screening for diabetes complications with
attention to those leading to functional impairment (e.g.
visual, lower extremity complications)
Recommendations: Older Adults
Standards of Medical Care in Diabetes. Diabetes
Care2012;35(suppl 1) Jan 2012.
-
8/11/2019 Diabetes Dan Usia Lanjut
29/39
A schedule of blood glucose self-monitoring should beconsidered,
depending on:
Functional and cognitive abilities
Goals of care
Target A1C levels Potential for modifying therapy
Risk of hypoglycemia
California Healthcare Foundation/American Geriatrics Society
Panel on ImprovingCare for Elders with Diabetes. J Am Geriatr
Soc2003;51:S265-S280.
Blood Glucose Monitoring in the Older
Adult with Diabetes
Bl d Gl M i i i h Old
-
8/11/2019 Diabetes Dan Usia Lanjut
30/39
The measurement of A1C may not be accurate in
older adults due to:
anemia and other conditions that impact red blood cell
lifespan
chronic kidney disease
recent transfusions and erythropoietin infusions
recent acute illness or hospitalizations chronic liver
diseases
Blood Glucose Monitoring in the Older
Adult with Diabetes
http://www.uptodate.com/contents/treatment-of-type-2-diabetes-mellitus-in-the-elderly-patient
-
8/11/2019 Diabetes Dan Usia Lanjut
31/39
Integrated geriatric services in hospitals and communityhealth
services (PUSKESMAS)
Home-based care centres & Centre for Family
Assistance (PUSAKA)
National Plan of Action for Elderly Welfare
Health of the Elderly in South-East Asia. WHO2004
Programs for the Elderly in Indonesia
Health of the Elderly in South-East Asia. WHO 2004.
St t i f I i Adh i
-
8/11/2019 Diabetes Dan Usia Lanjut
32/39
Verify comprehension:
E.g.: Tell me your understanding of how and when to take
your
medications.
Clarify treatment benefits:
E.g.: When people take their insulin, they notice that their
blood glucose control improves, and they have more energy.Do you
notice that?
Strategies for Improving Adherence in
the Older Patient
Rubin RR.Am J Med2005;118 Suppl 5A:27S-34S.
-
8/11/2019 Diabetes Dan Usia Lanjut
33/39
Goals of diabetes care in the elderly:
Control of hyperglycemia
Prevention and treatment of macro- and microvascular
complications
Self-management through education
Maintenance or improvement of general health status
.
Summary
-
8/11/2019 Diabetes Dan Usia Lanjut
34/39
Case Study 1
Patient profile:
82-year-old woman with mild dementia
To be cared at home after brief stay in hospital for
pneumonia
Medical history:
CAD (MI 5 years ago), CHF, COPD, HTN, T2DM
-
8/11/2019 Diabetes Dan Usia Lanjut
35/39
Case Study 1 (contd)
Physical exam BP: 130/84; Weight 105 lbs
Medications
Lisinopril 10 mg/day
Simvastatin 40 mg/day
Fluticasone/salmeterol inhaler bid
Insulin:
Glargine 15 units/day
Lispro 3 units before each meal
-
8/11/2019 Diabetes Dan Usia Lanjut
36/39
Case Study 1: Discussion
What is your A1C goal for this patient?
What are your recommendations for her insulin regimen?
-
8/11/2019 Diabetes Dan Usia Lanjut
37/39
Case Study 1: Follow-up
A month later, the nurses tell you the patient is
belligerent and tries to avoid receiving her insulin or
checking her BG
BG monitoring results are 140-190 fasting and 160-220
postprandial
What are you recommendations for the continued
management of this patient?
-
8/11/2019 Diabetes Dan Usia Lanjut
38/39
Case Study 2
70-year-old male with history of T2DM
HTN, hyperlipidemia
Routine physical exam:
Alert and interactive
BP 136/84; pulse 72;
Height 155 cm (5 1); Weight 66 kg (145 lbs); BMI 27.5
Labs: A1C=7.8%; Cr: 1.1
Medications:
Metformin 500 mg bid; Glipizide 10 mg qd
-
8/11/2019 Diabetes Dan Usia Lanjut
39/39
Case Study 2: Discussion
What is your A1C target for this patient?
What is your glycemic management plan for this patient?
Would you make any changes to his current
medications?