Embed Size (px)
DESCRIPTION
DIABETES Arshia Panahloo Consultant Diabetologist St. George's Hospital , London. www.addison.ac.uk. Topics to be covered:. Diagnosis Classification Epidemiology and Pathogenesis Complications. Diagnosis. Diagnosis. Hyperglycaemia central to the diagnosis Diagnostic confusion - PowerPoint PPT Presentation
Citation preview

DIABETES
Arshia Panahloo
Consultant Diabetologist
St. George's Hospital , London

www.addison.ac.uk

Topics to be covered:
• Diagnosis
• Classification
• Epidemiology and Pathogenesis
• Complications

Diagnosis

Diagnosis
• Hyperglycaemia central to the diagnosis
• Diagnostic confusion
• 1985 WHO criteria,based on an oral glucose tolerance test
• American Diabetes Association set their own criteria in 1997
• WHO revised in 1998
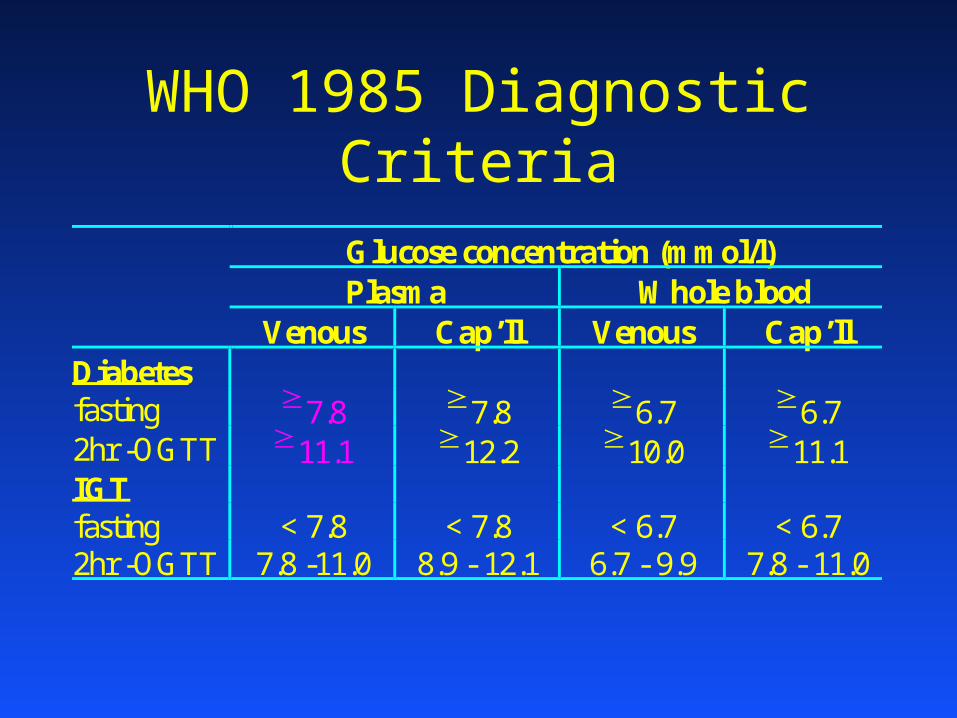
WHO 1985 Diagnostic Criteria
Glucose concentration (mmol/l)Plasma Whole blood
Venous Cap’ll Venous Cap’llDiabetesfasting 7.8 7.8 6.7 6.72hr -OGTT 11.1 12.2 10.0 11.1IGTfasting < 7.8 < 7.8 < 6.7 < 6.72hr -OGTT 7.8 -11.0 8.9 - 12.1 6.7 - 9.9 7.8 - 11.0

ADA 1997 Diagnostic CriteriaGlucose concentration (mmol/l)plasma whole bloodvenous venous cap’ll
Diabetesfasting or 7.0 6.1 6.12hr OGTT 11.1 10.0 11.1IGTfasting & < 7.0 < 6.1 < 6.12hr OGTT 7.8, <11.1 6.7, <10.0 7.8, < 11.1IFGfasting 6.1, < 7.0 5.6, < 6.1 5.6, < 6.12hr OGTT < 7.8 < 6.7 < 7.8

Diagnosis In the presence of symptoms:
(polyuria, polydipsia,weight loss)– Random plasma glucose 11.1 mmol/l
OR– Fasting plasma glucose 7.0 mmol/l
OR– 2 hour plasma glucose 11.1 mmol/l, 2hrs
after a 75g oral glucose tolerance test

Diagnosis In the absence of symptoms
• Diagnosis should not be based on a single sample
• Two samples on separate days, either:– fasting– random– 2 hour post load

Diagnosis IGT and IFG • IGT (Impaired Glucose Tolerance)
– Fasting plasma glucose < 7.0 mmol and 2 hour OGT value 7.8 -11.1
• IFG (Impaired Fasting Glycaemia)– fasting plasma glucose 6.1 - 7.0 mmol/l
• IGT and IFG are not clinical entities in their own right but risk categories for cardiovascular disease (IGT) and/or future diabetes (IFG)

Diagnosis• The diagnosis of diabetes has important
legal and medical implications
• Diagnosis should NOT be made on:– Glycosuria– Finger prick blood glucose– HbA1c
• A venous plasma sample is needed in an accredited laboratory

Classification
Aetiological Classification WHO 1998
• Type 1 cell destruction
• Type 2– insulin resistance +/- insulin deficiency– due to cell dysfunction
• Gestational diabetes

Classification• Other specific types
– genetic defects (cell)– genetic defects (insulin)– exocrine pancreas– endocrinopathies– drug / chemical induced– infections– immune-mediated– other genetic syndromes

Classification• Diabetes due to other endocrine
disease:– Cushing’s syndrome– Acromegaly– Thyrotoxicosis– Phaeochromocytoma– Hyperaldosteronism– Glucagonoma

Classification• Diabetes due drugs and chemicals:
– Glucocorticoids– Diuretics– B-Blockers
– B2-agonists
– Phenytoin– Cyclosporin– Nicotinic acid

Classification• Diabetes associated with genetic
syndromes– DIDMOAD (Wolfram) syndrome– Myotonic dystrophy and other muscular
disorders– Lipoatrophic diabetes– Type-1 glycogen storage disease– Cystic fibrosis
Epidemiology and Pathogenesis of
Type-1 Diabetes
Type-1 Diabetes
• Develops predominantly in children and young adults
• Can occur in all age groups• Occurs in all continents• Marked geographical variation
– Finland and Sardinia highest, 30-35 cases per 100,000 children aged up to 14 years
– oriental populations lowest, <1 per 100,000
Geographical variation• Variability is unexplained:
– genetic factors– environmental factors– Incidence in childhood in increasing– ‘outbreaks’ suggest infectious agents– seasonal variation, highest in autumn and
winter when viral infections more prevalent
Presentation
• Peak age of onset 11-13 years
• 10% of diabetic patients over 60 years are insulin dependent
• In UK the prevalence of type-1 DM is 1% (20% of total DM patients)
• 20% of typical type-2 DM display evidence of autoimmunity

Natural History of Type-1 DM
• Commonest cause is autoimmune destruction of B-cells
• Interaction between genetic factors and environment
• Onset is abrupt, but B-cell antigens may be present for many years
• Pre-diabetic state mild abnormalities of insulin secretion and glucose tolerance can be detected

‘Honeymoon period’
• After starting insulin, some patients need very small amounts
• Last 2-12 months
• Improvement in B-cell function once ‘glucose toxicity’ removed
• True remission rare
• Research into preserving B-cell function
Genetic Factors (1)
• Account for a third of the susceptibility to type-1 DM
• 36% concordance for monozygotic twins• Over 20 regions of the human genome
show some linkage with type-1 DM• Strongest linkage is with HLA genes
within the MCH region on chrom. 6

Genetic Factors (2)
• HLA haplotypes DR3 and DR4 predispose to type-1 DM
• linkage disequilibrium with true susceptibility loci
• HLA class II antigens on the cell surface present foreign and self antigens to T-lymphocytes and initiate the auto- immune response
Genetic Factors (3)• Strong linkage between HLA-DR and DQ
regions
• Polymorphisms of the DQB1 gene resulting in amino acid substitution in class II antigens may determine B-cell damage
• Region of the insulin gene on chrom. 11 is linked to type-1 DM, insulin or pre-cursors can act as B-cell autoantigens

Environmental Factors
• Viruses
• Dietary components
• Stress
• Drugs and toxins
Viruses
• Viruses can directly destroy B-cells or indirectly by an autoimmune response
• Mumps– Occasionally precedes IDDM– autoimmune B-cell destruction– islet cell antibodies develop– can induce interleukin production and HLA
hyperexpression in B-cells

Viruses• Coxsackie B
– IgM anti-coxsackie B antibodies in newly diagnosed type-1 DM
– Antigen identified in islets post-mortem– Direct cytotoxic action on B-cells
• Retroviruses• Rubella• CMV• Epstein-Barr

Nutrients• ? Nitrosamines in diet
• Breast feeding– short duration associated with increased
risk of adult Type-1 diabetes in some studies
– Antibodies to cow’s milk protein found in higher titres in children with recent onset type-1 diabetes
Epidemiology and Pathogenesis of
Type-2 Diabetes

Dia
bete
s p
reva
len
ce (
thou
san
ds)
0
500
1000
1500
2000
2500
3000
1995 2000 2010
Type 1Type 2
Amos AF et al. Diabet Med 1997;14(Suppl 5);S1–S85
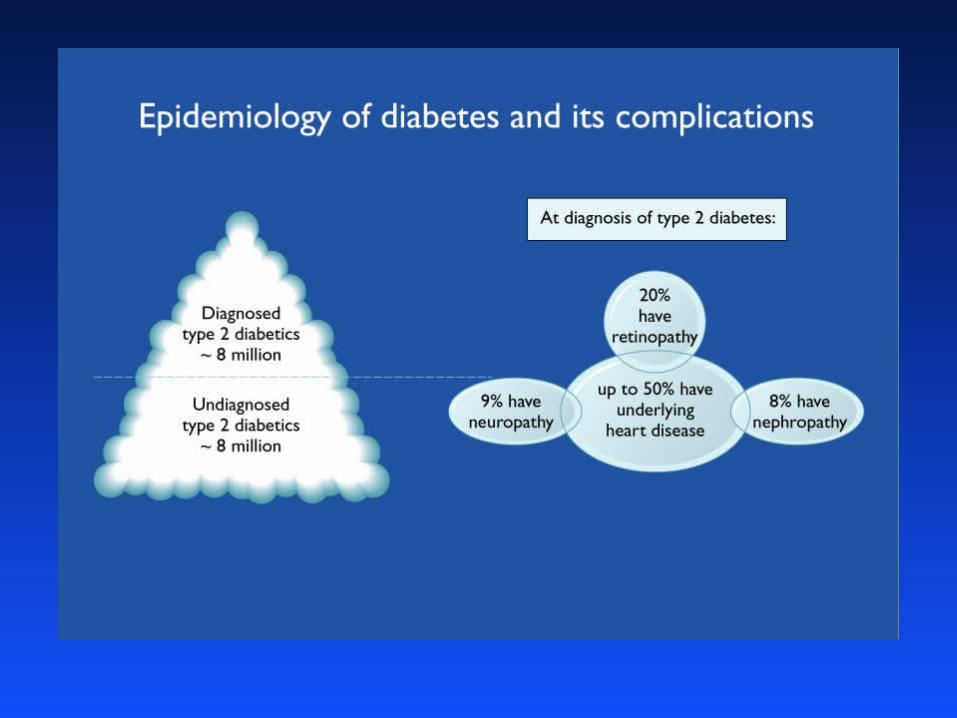
3 million in the UK by 2010
Incidence of type 2 diabetes rapidly increasing

Geographical variation
• Large variation• Highest in some native American tribes
(Pima Indians) in Arizona (50%) and South Pacific Islands
• Low prevalence in least developed rural communities
• Prevalence is closely associated with BMI
Type-2 Diabetes in the UK
• Prevalence:– 1-2% for the white population– 11% for Indian– 9% for African-Caribbeans
• Compared to white patients Indian patients have younger age of onset of type-2 diabetes and earlier protinuria and renal disease, and excess CHD.
Type-2 Diabetes
• Accounts for 85% of the diabetic population
• Patients do not require insulin to remain alive, although 20% are treated with insulin to control blood glucose
• Peak age of onset is 60 years, younger age of onset seen with MODY
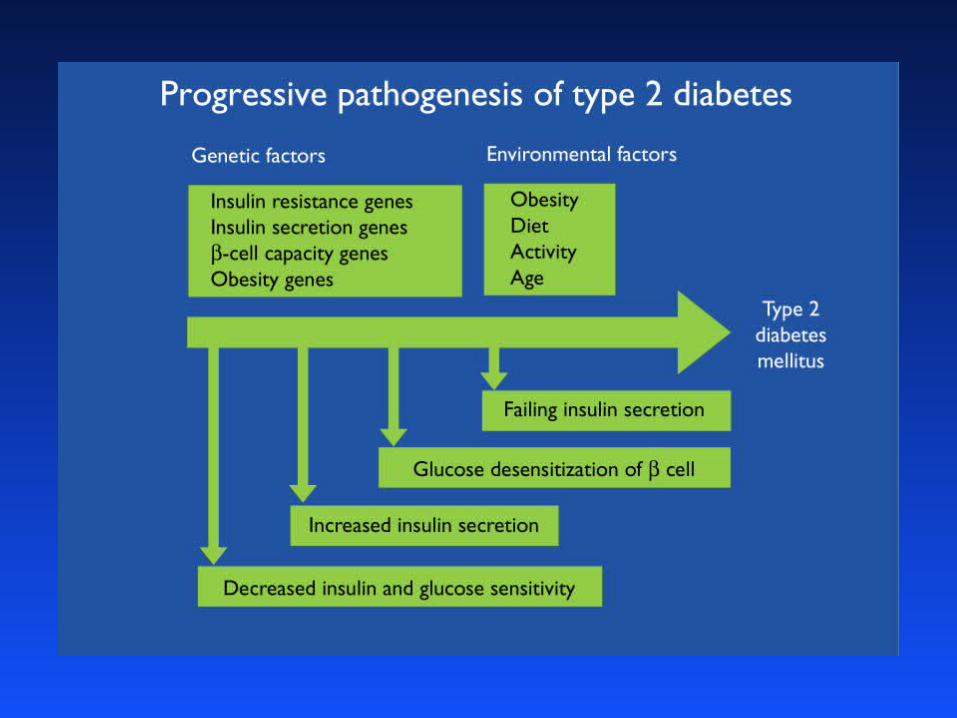


Type-2 Diabetes
• Is characterized by variable combinations of insulin resistance and insulin deficiency
• Insulin deficiency is less severe than type-1 diabetes and insulin levels remain high enough to prevent excess lipolysis and ketoacidosis
• Patients are C-peptide positive
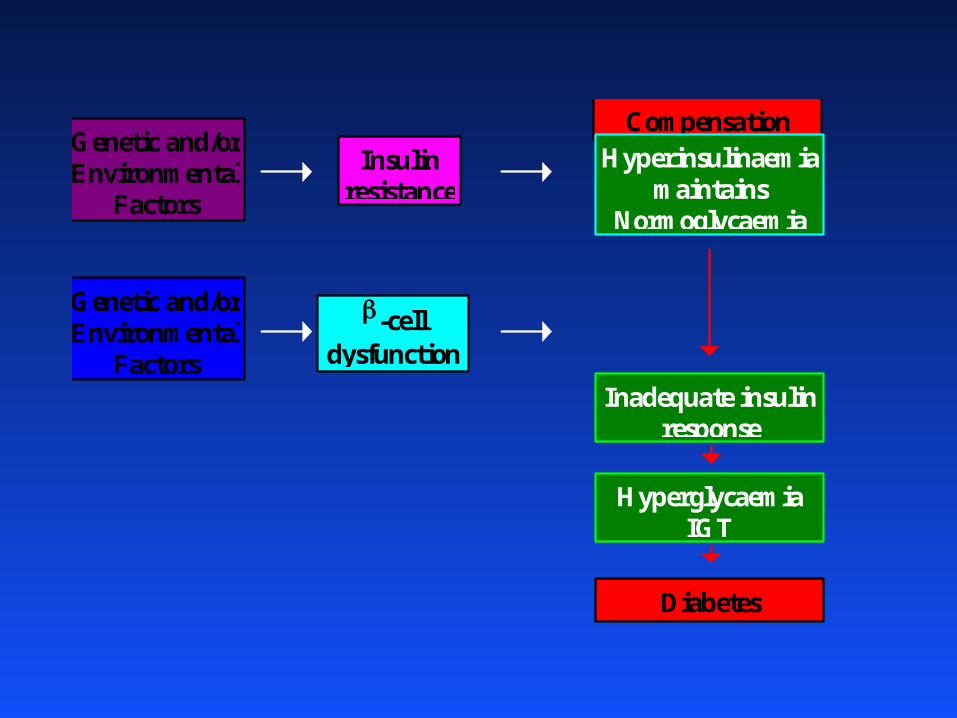
Genetic and/orEnvironmental
Factors
Genetic and/orEnvironmental
Factors
Insulinresistance
CompensationHyperinsulinaemia
maintainsNormoglycaemia
-celldysfunction
Inadequate insulinresponse
HyperglycaemiaIGT
Diabetes

Insulin Resistance
Inability of insulin to produce its usual biological effects at circulating concentrations that are effective in normal subjects.

Acquired causes of insulin resistance1) Obesity
– truncal obesity (visceral fat) is related to insulin resistance
– BMI >35 have 40 x risk of developing DM compared with those with BMI < 23
– visceral fat is especially susceptible to lipolysis and hence raised NEFA
– truncal obesity is associated with increased proportion of white muscle fibres which are more insulin resistant than red fibres
2) Reduced physical activity– exercise increases :
• insulin sensitive red fibres
• fat oxidative enzymes
• tissue (white adipose) sensitivity to catecholamines and enhancing lipolysis
– hence exercise increases insulin sensitivity & increased utilisation of fat as fuel
3) Malnutrition in foetal/early infant life– low birth wt. assoc with metabolic syndorme X
in later life (obesity,insulin resistance & DM, hypertension, dyslipidaemia, atherosclerosis)
Management of Type II Diabetes
Aims :-
• Abolish symptoms and acute complications of hyperglycaemia
• Reduce threat of chronic complications
• Increase life expectancy
• Restore quality of life

Genetics of Type II Diabetes
• High rate of concordance (60-100%) for the disease in identical twins
• Familial aggregation
• Different prevalence in ethnic groups
• Polygenic trait with environmental factors
• MODY (0.3% type-2) mutations in glucokinase gene
• Mutations in mitochondrial DNA (rare)

Complications
Complications of Diabetes
• Microvascular:
• Nephropathy
• Retinopathy
• Neuropathy
• Macrovascular
• Coronary heart disease / Stroke /lipids
• Peripheral vascular disease
• Blood pressure
Retinopathy• Type-1:
• Rare less than 5 years of diabetes• With increasing prevalence the incidence rises
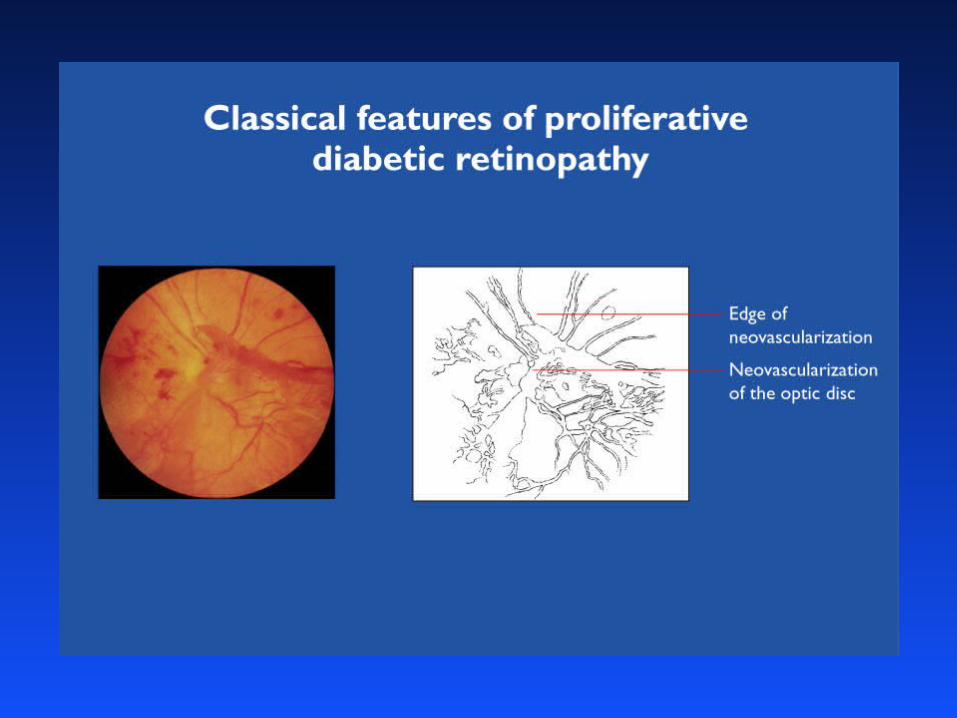
to a peak at 15-20 years• Severe proliferative retinopathy also increases
with diabetes duration, >20yrs
• Type-2:• Can be present at diagnosis• Increased incidence of macular oedema

Retinopathy
• Risk Factors:
• Poor glycaemic control
• Genetic factors
• Blood pressure
• Smoking


Nephropathy
Type-1
• Associated with the duration of DM
• Peak incidence after 15-20 years, followed by a steady decline after 30-40 years
• Higher incidence in men
• Higher incidence in patients who develop DM prior to age of 15 years

Nephropathy
• Risk Factors:
• Age at onset
• Poor glycaemic control
• Genetic factors
• Blood pressure
• Smoking


Neuropathy
• Symmetrical sensory neuropathy
• Affects 20-30% diabetics, prevalence rises with duration and severity of diabetes
• Autonomic neuropathy
• Acute mononeuropathy (femoral or oculomotor)
• Pressure palsies (median and ulnar nerve)





























