Embed Size (px)
Citation preview

Developing National Guidance on Genetic Testingfor Breast Cancer Predisposition:The Role of Economic Evidence?
William Sullivan,1 D. Gareth Evans,2 William G. Newman,2 Simon C. Ramsden,3
Hans Scheffer,4 and Katherine Payne5
Advancements in genetic testing to identify predisposition for hereditary breast cancer (HBC) mean that it isimportant to understand the incremental costs and benefits of the new technologies compared with current testingstrategies. This study aimed to (1) identify and critically appraise existing economic evidence for BRCA1/2mutation testing for HBC and (2) establish whether economic evidence was used to inform national guidance inEngland and Wales. A telephone interview with diagnostic laboratories (n = 14) offering BRCA1/2 mutation testingidentified that 9 (64%) used Sanger DNA sequencing with multiplex ligation-dependent probe amplification andtwo offered next generation sequencing. A systematic review identified 15 economic studies that evaluated:genetic testing for HBC (5 studies); preventive management options for women at risk of HBC (8 studies); anddifferent laboratory approaches for BRCA1 testing (2 studies). These evaluations were not relevant to U.K.practice, and therefore the development of national guidance using a risk threshold to trigger BRCA1/2 testing hasnot been informed by existing economic evidence. The lack of economic evidence supporting the current riskthreshold for national guidance has implications for the efficient use of healthcare resources and the design ofeconomic evaluations of new technologies for BRCA1/2 testing.
Introduction
Historically, neither diagnostic nor genetic testshave been a focus for health technology assessment
(HTA), perhaps because of their perceived low impact onhealthcare resources. More recently, it has been acknowl-edged that diagnostics have substantial cost implications interms of subsequent use of resources and selection of treat-ment pathways, which may translate into improved patientoutcomes (LewinGroup, 2009). Decision-making bodies pro-ducing guidance to inform the allocation of healthcare re-sources have been advised to turn their attention to the HTAof diagnostics including genetic testing (House of Lords Sci-ence and Technology Committee, 2009).
Finite resources in the available funding and the necessaryassessment skills mean that conducting HTAs of all diagnosticand genetic tests is not possible. The initial focus should, there-fore, perhaps be tests that have a potentially large impact on theuse of healthcare resources. Genetic testing for breast cancer
predisposition is a good example of an intervention that willhave a sizeable impact because of the large volume of tests un-dertaken and also significant implications for subsequent patientpreventive treatment and care pathways. Breast cancer consti-tutes the most common form of cancer among women world-wide and research suggests that over 500,000 women in theUnited Kingdom are living with breast cancer today (CancerResearch UK, 2011). In 3% to 5% of cases, breast cancer is causedby high-penetrance inherited genetic mutations (Newman et al.,1988; Claus et al., 1991; Evans and Howell, 2007). Since 1996,testing for mutations in two high-penetrance predisposing genes,BRCA1 and BRCA2, has been clinically available in a number ofcountries, including the United Kingdom (Peters et al., 2005). Arecent audit suggests that over 4000 full gene BRCA screens havebeen performed annually in U.K. clinical laboratories in recentyears (Clinical Molecular Genetics Society, 2011). Mutations inthe hereditary breast cancer (HBC) genes BRCA1 and BRCA2account for the majority (65%–90%) of high-penetrance inheritedbreast cancers (Stratton and Rahman, 2008).
1School of Health and Related Medicine, University of Sheffield, Sheffield, United Kingdom.2Academic Unit of Medical Genetics, St. Mary’s Hospital, Manchester, United Kingdom.3Department of Genetic Medicine, St. Mary’s Hospital, Manchester, United Kingdom.4Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands.5Health Sciences—Economics, School of Community Based Medicine, University of Manchester, Manchester, United Kingdom.
GENETIC TESTING AND MOLECULAR BIOMARKERSVolume 16, Number 6, 2012ª Mary Ann Liebert, Inc.Pp. 580–591DOI: 10.1089/gtmb.2011.0236
580

Sanger sequencing for BRCA1/2 (Sanger et al., 1977) used inconjunction with a technique to identify micro-deletions/duplications, for example, multiplex ligation-dependentprobe amplification (MLPA), is currently used in most mo-lecular diagnostic laboratories. Current U.K. cost estimates fora genetic test for BRCA1/2 using this method are around £600for the proband and £120 for a family member of a personalready identified as carrying a BRCA1/2 mutation. Recenttechnological developments have introduced next-generation(or highly parallel) sequencing (NGS), which has the potentialto increase the speed and volume of testing and also thenumber of genes tested simultaneously (Hutchison, 2007;MRC, 2009). This will potentially mean that laboratories couldincrease their capacity and offer more tests with faster turn-around times. In theory, laboratories could offer BRCA1/2testing to a higher proportion of women. Clinical scientists arealready developing methods that will move NGS from theresearch to the clinical laboratory environment (e.g., EU Fra-mework Seven Projects: ‘‘TECHGENE,’’ Project Reference223143; ‘‘EURO-GENE-SCAN,’’ Project Reference 223293;‘‘NMD-CHIP,’’ Project Reference 223026). To evaluate theincremental costs and benefits, and inform efficient resourceallocation, it is first necessary to understand the economicevidence currently available to support a genetic testing ser-vice using DNA Sanger sequencing technology for BRCA1/2mutations in the study populations and countries of interestfor a decision-maker. This is for two reasons: (i) it is necessaryto be clear whether current practice was informed by robustevidence that considered the cost and outcomes for a definedpatient population; (ii) identifying existing economic evidencewill potentially provide a useful starting point to design andpopulate an economic model evaluating a new technology forBRCA1/2 testing. Modeling methods enable researchers tocombine and analyze data from a number of sources and alsoprovide a summary of the extent of uncertainty in the currentevidence base (Drummond et al., 2005). Modeling methods area necessity if information is required for resource allocationdecisions about the incremental costs and benefits of a newhealthcare technology, such as innovations in diagnostics. Theaim of this current study was to identify, summarize, andcritically appraise current published economic evaluations ofgenetic testing for HBC predisposition to understand thecurrent level of economic evidence supporting U.K. guide-lines. A secondary aim was to assess the extent to whichSanger DNA sequencing is currently used in U.K. clinicallaboratories to test for BRCA1/2 mutations, in order to un-derstand whether this technique truly encapsulates currentstandard practice.
Materials and Methods
Two methods were used: telephone interviews and asystematic review of published literature and national guid-ance relevant to England and Wales (Scotland has a separatesystem for HTA and reimbursement).
Telephone interviews to establish currentBRCA1/2 testing practice
In September 2010, telephone interviews with the 14 U.K.diagnostic laboratories listed on the Clinical MolecularGenetics Society (CMGS) Web site (www.cmgs.org) as offer-ing a BRCA1/2 mutation testing service were undertaken to
understand current practice. The named contact person fromeach laboratory on the CMGS Web site was asked one ques-tion: What laboratory methods do you currently use to test forBRCA1/2 mutations?
Scope of the review
A systematic review, using Centre for Reviews and Dis-semination systematic review methods (Craig et al., 2007),aimed to identify all economic evaluations relevant to genetictesting for HBC. An economic evaluation was defined as ‘‘thecomparative analysis of alternative courses of action in termsof both their costs and consequences’’ (Drummond et al.,2005). A second pragmatic review, conducted using handsearching of key Web sites, was used to identify nationalguidance relevant to HBC in England and Wales.
Systematic review inclusion criteria
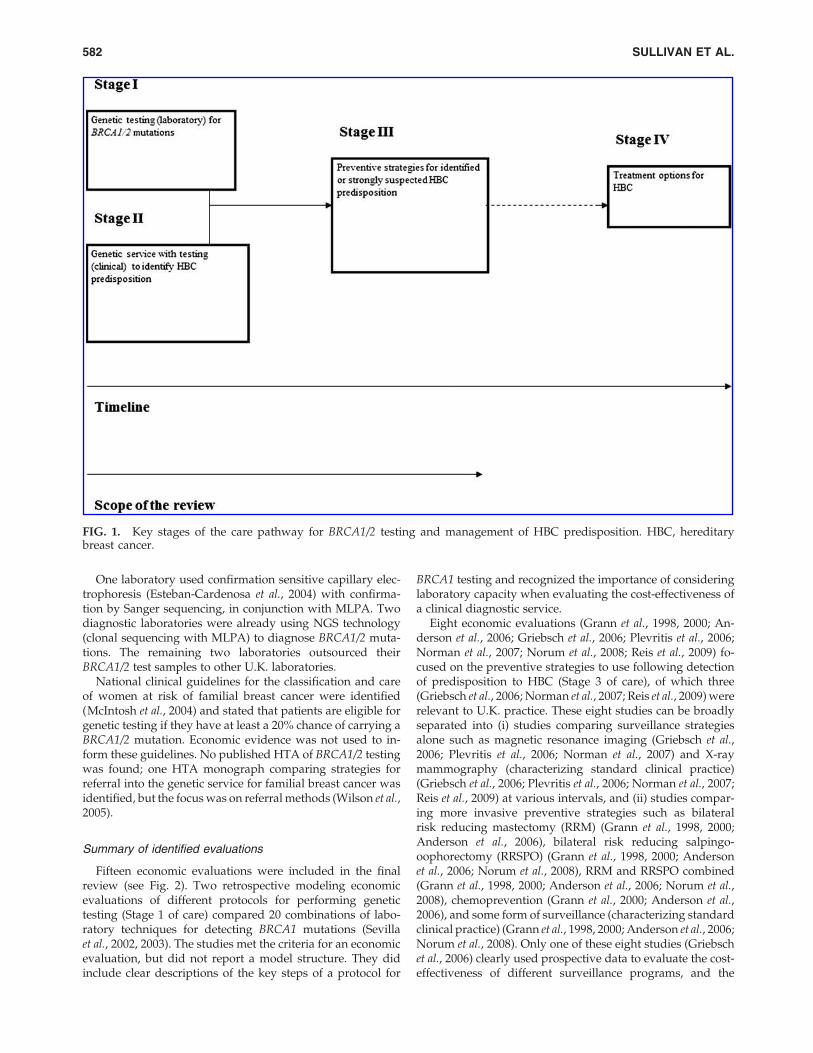
Figure 1 identifies four separate stages of the care pathwayfor which it is possible to undertake cost-effectiveness ana-lyses relevant to genetic testing in HBC and defines the scopeof the review (Stages 1, 2 and 3). Economic evaluations oftreatment options for HBC patients (Stage 4 of care) weredeemed beyond the scope of the review because as long asgenetic testing using a new technology for HBC does notidentify new genetic variants, a change in technology wouldnot affect treatment options. Electronic searches of MEDLINE(via Ovid), EMBASE (via Ovid), PsychINFO (via Ovid), andthe NHS Economic Evaluation Database (NHS EED; viawww.york.ac.uk) were run in February 2010. This search wassupplemented by hand searching key Web sites (NationalInstitute for Health Research Health Technology Assessmentmonographs [www.hta.ac.uk], NICE guidelines and tech-nology appraisals). The start date of 1996 was used becausethis was when BRCA1/2 testing became clinically available.The electronic search strategies combined terms to identifyeconomic evaluations, using the NHS EED search strategy(CRD, 2011), with terms relevant to HBC and genetic testing.The search strategies were modified for each database, andare available from the authors upon request. Commentary-type discussion articles and non-English-language publica-tions were excluded from the review. Two reviewers (W.S.and K.P.) screened titles, and potentially relevant articles wereretrieved in full and screened for inclusion. Included articleswere hand searched for potentially relevant references.
Data extraction and analysis
The primary focus was to critically appraise publishedeconomic evaluations of genetic testing for HBC predisposi-tion (see Stage 2 of Fig. 1). Data were extracted and summa-rized in tables and described in a narrative review, and allidentified studies were critically appraised for quality usingguidelines produced by the NHS Economic Evaluation Da-tabase (Craig et al., 2007) and good practice guidelines fordecision analytic modeling (Philips et al., 2006).
Results
The telephone survey identified that 9 (64%) of the U.K.diagnostic laboratories were offering BRCA1/2 mutationscreening using Sanger DNA testing in conjunction withMLPA.
ECONOMIC EVIDENCE ON GENETIC TESTING FOR BREAST CANCER PREDISPOSITION 581
One laboratory used confirmation sensitive capillary elec-trophoresis (Esteban-Cardenosa et al., 2004) with confirma-tion by Sanger sequencing, in conjunction with MLPA. Twodiagnostic laboratories were already using NGS technology(clonal sequencing with MLPA) to diagnose BRCA1/2 muta-tions. The remaining two laboratories outsourced theirBRCA1/2 test samples to other U.K. laboratories.
National clinical guidelines for the classification and careof women at risk of familial breast cancer were identified(McIntosh et al., 2004) and stated that patients are eligible forgenetic testing if they have at least a 20% chance of carrying aBRCA1/2 mutation. Economic evidence was not used to in-form these guidelines. No published HTA of BRCA1/2 testingwas found; one HTA monograph comparing strategies forreferral into the genetic service for familial breast cancer wasidentified, but the focus was on referral methods (Wilson et al.,2005).
Summary of identified evaluations
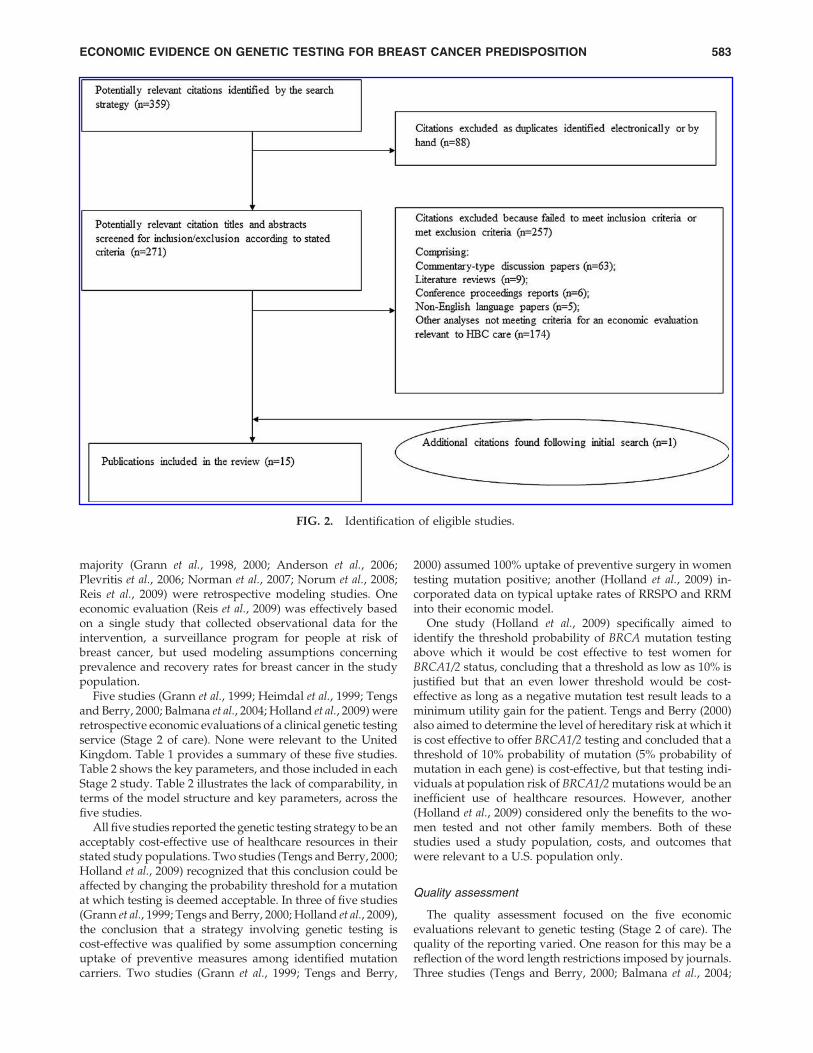
Fifteen economic evaluations were included in the finalreview (see Fig. 2). Two retrospective modeling economicevaluations of different protocols for performing genetictesting (Stage 1 of care) compared 20 combinations of labo-ratory techniques for detecting BRCA1 mutations (Sevillaet al., 2002, 2003). The studies met the criteria for an economicevaluation, but did not report a model structure. They didinclude clear descriptions of the key steps of a protocol for
BRCA1 testing and recognized the importance of consideringlaboratory capacity when evaluating the cost-effectiveness ofa clinical diagnostic service.
Eight economic evaluations (Grann et al., 1998, 2000; An-derson et al., 2006; Griebsch et al., 2006; Plevritis et al., 2006;Norman et al., 2007; Norum et al., 2008; Reis et al., 2009) fo-cused on the preventive strategies to use following detectionof predisposition to HBC (Stage 3 of care), of which three(Griebsch et al., 2006; Norman et al., 2007; Reis et al., 2009) wererelevant to U.K. practice. These eight studies can be broadlyseparated into (i) studies comparing surveillance strategiesalone such as magnetic resonance imaging (Griebsch et al.,2006; Plevritis et al., 2006; Norman et al., 2007) and X-raymammography (characterizing standard clinical practice)(Griebsch et al., 2006; Plevritis et al., 2006; Norman et al., 2007;Reis et al., 2009) at various intervals, and (ii) studies compar-ing more invasive preventive strategies such as bilateralrisk reducing mastectomy (RRM) (Grann et al., 1998, 2000;Anderson et al., 2006), bilateral risk reducing salpingo-oophorectomy (RRSPO) (Grann et al., 1998, 2000; Andersonet al., 2006; Norum et al., 2008), RRM and RRSPO combined(Grann et al., 1998, 2000; Anderson et al., 2006; Norum et al.,2008), chemoprevention (Grann et al., 2000; Anderson et al.,2006), and some form of surveillance (characterizing standardclinical practice) (Grann et al., 1998, 2000; Anderson et al., 2006;Norum et al., 2008). Only one of these eight studies (Griebschet al., 2006) clearly used prospective data to evaluate the cost-effectiveness of different surveillance programs, and the
FIG. 1. Key stages of the care pathway for BRCA1/2 testing and management of HBC predisposition. HBC, hereditarybreast cancer.
582 SULLIVAN ET AL.
majority (Grann et al., 1998, 2000; Anderson et al., 2006;Plevritis et al., 2006; Norman et al., 2007; Norum et al., 2008;Reis et al., 2009) were retrospective modeling studies. Oneeconomic evaluation (Reis et al., 2009) was effectively basedon a single study that collected observational data for theintervention, a surveillance program for people at risk ofbreast cancer, but used modeling assumptions concerningprevalence and recovery rates for breast cancer in the studypopulation.
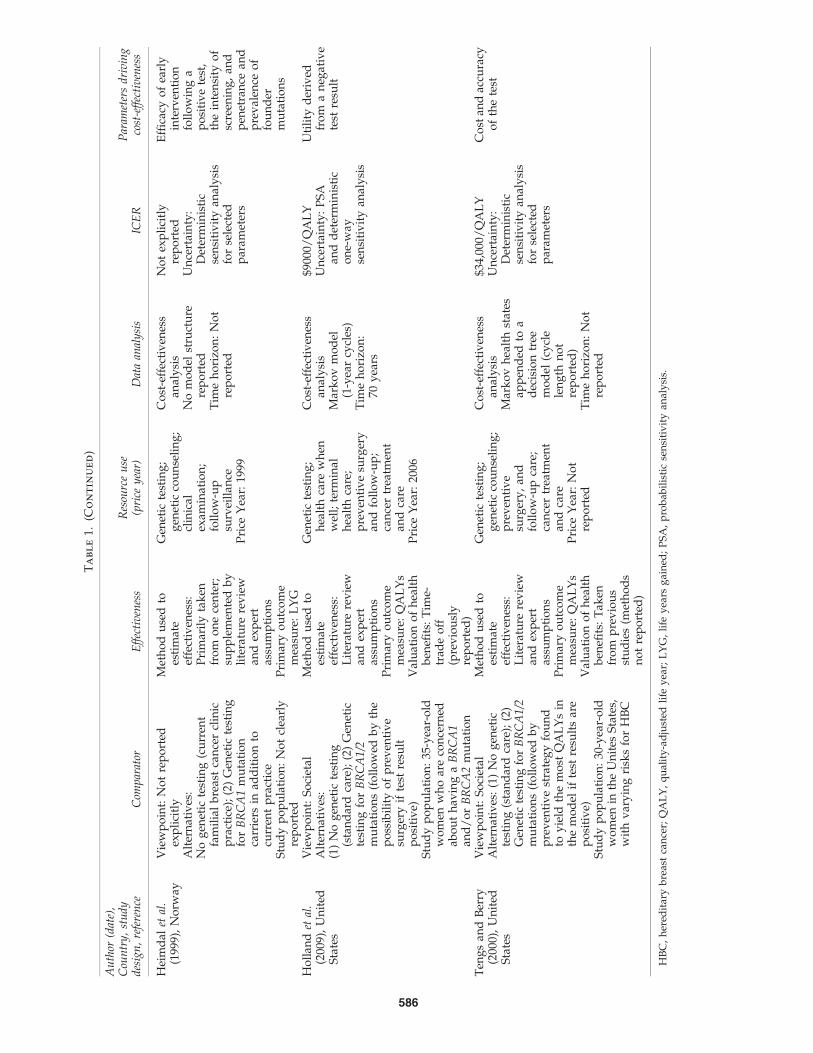
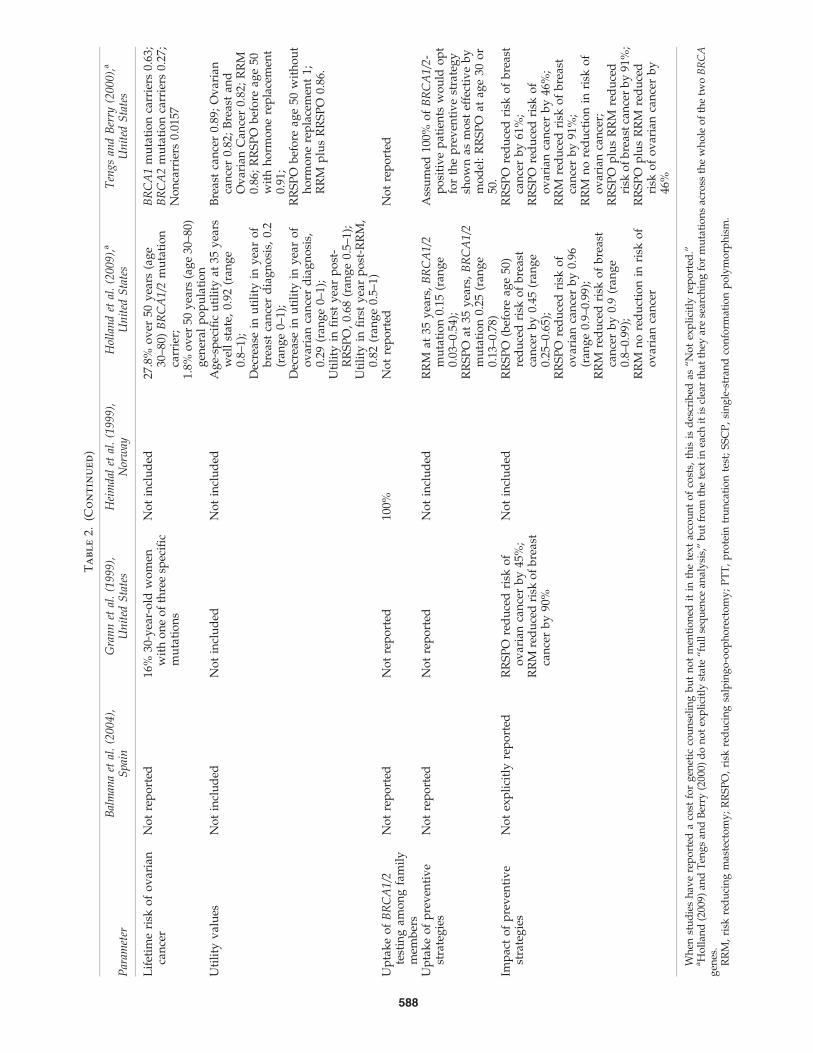
Five studies (Grann et al., 1999; Heimdal et al., 1999; Tengsand Berry, 2000; Balmana et al., 2004; Holland et al., 2009) wereretrospective economic evaluations of a clinical genetic testingservice (Stage 2 of care). None were relevant to the UnitedKingdom. Table 1 provides a summary of these five studies.Table 2 shows the key parameters, and those included in eachStage 2 study. Table 2 illustrates the lack of comparability, interms of the model structure and key parameters, across thefive studies.
All five studies reported the genetic testing strategy to be anacceptably cost-effective use of healthcare resources in theirstated study populations. Two studies (Tengs and Berry, 2000;Holland et al., 2009) recognized that this conclusion could beaffected by changing the probability threshold for a mutationat which testing is deemed acceptable. In three of five studies(Grann et al., 1999; Tengs and Berry, 2000; Holland et al., 2009),the conclusion that a strategy involving genetic testing iscost-effective was qualified by some assumption concerninguptake of preventive measures among identified mutationcarriers. Two studies (Grann et al., 1999; Tengs and Berry,
2000) assumed 100% uptake of preventive surgery in womentesting mutation positive; another (Holland et al., 2009) in-corporated data on typical uptake rates of RRSPO and RRMinto their economic model.
One study (Holland et al., 2009) specifically aimed toidentify the threshold probability of BRCA mutation testingabove which it would be cost effective to test women forBRCA1/2 status, concluding that a threshold as low as 10% isjustified but that an even lower threshold would be cost-effective as long as a negative mutation test result leads to aminimum utility gain for the patient. Tengs and Berry (2000)also aimed to determine the level of hereditary risk at which itis cost effective to offer BRCA1/2 testing and concluded that athreshold of 10% probability of mutation (5% probability ofmutation in each gene) is cost-effective, but that testing indi-viduals at population risk of BRCA1/2 mutations would be aninefficient use of healthcare resources. However, another(Holland et al., 2009) considered only the benefits to the wo-men tested and not other family members. Both of thesestudies used a study population, costs, and outcomes thatwere relevant to a U.S. population only.
Quality assessment
The quality assessment focused on the five economicevaluations relevant to genetic testing (Stage 2 of care). Thequality of the reporting varied. One reason for this may be areflection of the word length restrictions imposed by journals.Three studies (Tengs and Berry, 2000; Balmana et al., 2004;
FIG. 2. Identification of eligible studies.
ECONOMIC EVIDENCE ON GENETIC TESTING FOR BREAST CANCER PREDISPOSITION 583

Holland et al., 2009) explicitly reported the model structureused. All of the studies reported the use of literature reviewsto identify data to populate the economic models, but nonereported sufficient details on the methods used to identify andassess the quality of identified studies. Therefore, it was dif-ficult to assess whether the most appropriate and unbiasedinput values, and ranges around these values, were used asmodel parameters. Four of five studies (Grann et al., 1999;Tengs and Berry, 2000; Balmana et al., 2004; Holland et al.,2009) report using expert opinion data where other datasources were not available but again none report the methodsused to elicit expert opinion and assessment of whether theseestimates of the input parameters are fair and unbiased wasnot possible.
The types of resources and costs included in the studiesvaried. The chosen study perspectives were not always re-ported explicitly (Heimdal et al., 1999; Balmana et al., 2004)and on two occasions (Tengs and Berry, 2000; Holland et al.,2009) the resources included were not consistent with thestated study perspective. The costs reported were not con-sistent across the five studies and included: genetic testing;genetic counseling; follow-up examinations and care; pre-ventive care; cancer care and terminal care. Sources of costdata were generally well reported across studies but in four ofthe five studies (Grann et al., 1999; Heimdal et al., 1999; Tengsand Berry, 2000; Holland et al., 2009) charges rather than unitcosts were used. Charges, set for reimbursement purposes, donot generally reflect the true cost of a procedure. There isevidence to suggest that charges for a medical procedure orcare is not by necessity equivalent to and is in fact likely to behigher than the sum of the unit costs of its constituent parts(Drummond et al., 2005). Cost data in these four studies wereeither informed solely by insurance reimbursement paymentsand drug cost records (Grann et al., 1999; Heimdal et al., 1999)or also relied on data from the literature (Tengs and Berry,2000; Holland et al., 2009), and one study (Holland et al., 2009)also used unit cost data in part to estimate the cost of care. Theremaining study (Balmana et al., 2004) used hospital data toestimate costs.
Current guidelines for economic evaluation of pharma-ceuticals in the United Kingdom (National Institute for Healthand Clinical Excellence, 2008) advocate the use of a generichealth-related quality of life measure to quantify patientbenefits. Three of the five identified economic evaluations of aclinical genetic testing service for HBC predisposition mea-sure outcomes in life years gained, which were estimatedfrom epidemiological survival data (Grann et al., 1999;Heimdal et al., 1999) and patient-specific hospital data (Bal-mana et al., 2004). Two of the studies attempted to estimatequality-adjusted life years (QALYs) to measure health out-comes. Holland et al. (2009) used utility estimates from a timetrade-off study designed to elicit preferences for cancer healthstates and prevention strategies by women: who had breastcancer (n = 21); who were at high risk of breast cancer (n = 28);or who had neither condition (n = 135). Tengs and Berry (2000)used utility estimates from a previously reported decisionanalytic model to weight the additional years of life with avalue (utility) to reflect the quality of the years gained, but didnot provide details on how the utility values were elicited.
Incremental analysis examines the additional costs ofone technology over another, usually current practice, andcompares these with the additional benefits delivered
(Drummond et al., 2005). It was not always clearly reportedhow the incremental analysis of costs and benefits was per-formed across the five studies. In Heimdal et al. (1999), it wasnot clear whether an incremental analysis has been under-taken. In two studies (Grann et al., 1999; Tengs and Berry,2000) it was unclear how the incremental analyses were per-formed from the total cost and outcomes data reported. Onlyone study (Grann et al., 1999) reported a measure of variationaround the base case incremental analysis.
Economic models use inputs (parameter values) assimi-lated from a variety of data sources. Sampling uncertainty is,therefore, inherent in economic evaluations and this impre-cision should be reflected around the input parameters ineconomic models (Drummond et al., 2005; Philips et al., 2006).All five evaluations performed some type of sensitivity anal-ysis focusing on parameter uncertainty and two evaluations(Grann et al., 1999; Holland et al., 2009) conducted probabi-listic sensitivity analysis as recommended by publishedguidance (National Institute for Health and Clinical Ex-cellence, 2008). There was no investigation into the impact ofother types of uncertainty that could be explored in an eco-nomic decision model (methodological, heterogeneity, andstructural). From the sensitivity analyses reported, the fol-lowing model-driving parameters were identified in all butone of the studies (Grann et al., 1999; Heimdal et al., 1999;Balmana et al., 2004; Tengs and Berry, 2000): penetrance ofBRCA1 and BRCA2 mutations in study populations andpenetrance of breast and ovarian cancer among mutationcarriers. One study reported that the efficacy of preventivestrategies taken up by patients testing positive for predis-posing mutations as an important driver of cost-effectiveness(Grann et al., 1999). Both studies measuring QALYs (Tengsand Berry, 2000; Holland et al., 2009) reported that their cost-effectiveness estimates were sensitive to the utility valuesused to derive QALYs. Participation in preventive strategieswas also a key driver of cost-effectiveness.
Discussion
This review identified 15 published economic evaluationsrelevant to interventions for predisposition for HBC, but 8 ofthese were evaluations of preventive strategies for womenpredisposed to HBC and did not directly consider the eco-nomic impact of genetic testing as an intervention. Twofurther studies were potentially promising because theywere purportedly evaluations of different genetic testingstrategies for BRCA1 testing but neither used sufficientlyrobust reporting of modeling methods to provide a usefulstarting point for evaluating a new genetic testing technol-ogy. Five economic evaluations of genetic testing for HBCpredisposition as a clinical service were identified, but nonewere relevant to the focus of economic evidence informing orsupporting national guidance for BRCA1/2 testing in Eng-land and Wales. The quality of reporting for all identifiedpublished economic evaluations was varied, and in mostinstances it was not possible to clearly identify both themodel structure and reliability of the model inputs used togenerate estimates of cost-effectiveness. This limits the extentto which a decision maker, representing a jurisdiction dif-ferent to the viewpoint of the published study, can use andinterpret whether the findings are relevant to local clinicalpractice.
584 SULLIVAN ET AL.

Ta
bl
e1.
Su
mm
ar
yo
fP
ub
lish
ed
Ec
on
om
ic
Ev
al
ua
tio
ns
of
Ge
ne
tic
Te
st
in
gfo
rH
er
ed
it
ar
yB
re
ast
Ca
nc
er
Pr
ed
isp
osit
io
n
Au
thor
(dat
e),
Cou
ntr
y,
stu
dy
des
ign
,re
fere
nce
Com
par
ator
Eff
ecti
ven
ess
Res
ourc
eu
se(p
rice
yea
r)D
ata
anal
ysi
sIC
ER
Par
amet
ers
dri
vin
gco
st-e
ffec
tiv
enes
s
Bal
man
aet
al.
(200
4),
Sp
ain
Vie
wp
oin
t:N
ot
rep
ort
edA
lter
nat
ives
:(1
)N
og
enet
icte
stin
g(s
tan
dar
dca
re);
(2)
BR
CA
1/
2te
stin
gan
dco
un
seli
ng
wit
hap
pro
pri
ate
foll
ow
-up
care
,d
epen
din
go
nG
rou
pS
tatu
s.G
rou
p1:
fem
ales
fro
mh
igh
-ris
kfa
mil
ies
wit
ho
ut
anid
enti
fied
mu
tati
on
;G
rou
p2:
BR
CA
1o
rB
RC
A2
fem
ale
mu
tati
on
carr
iers
;G
rou
p3:
fem
ale
no
nm
uta
tio
nca
rrie
rsfr
om
fam
ilie
sw
ith
ap
ath
olo
gic
alB
RC
A1
or
BR
CA
2g
ene
mu
tati
on
Stu
dy
po
pu
lati
on
:N
ot
exp
lici
tly
rep
ort
ed
Met
ho
du
sed
toes
tim
ate
effe
ctiv
enes
s:D
ata
fro
mF
amil
ial
Cen
tre
dat
abas
e,su
pp
lem
ente
db
yli
tera
ture
rev
iew
and
exp
ert
assu
mp
tio
ns
Pri
mar
yo
utc
om
em
easu
re:
LY
G
Gen
etic
cou
nse
lin
gan
dg
enet
icte
stin
go
fin
dex
case
;cl
inic
alb
reas
tex
amin
atio
ns;
bre
ast
bio
psy
;d
eter
min
atio
no
fg
enet
icst
atu
sP
rice
yea
r:N
ot
rep
ort
ed
Co
st-e
ffec
tiv
enes
san
aly
sis
Dec
isio
ntr
eem
od
elT
ime
ho
rizo
n:
Lif
etim
e
e42
94/
LY
GU
nce
rtai
nty
:D
eter
min
isti
cse
nsi
tiv
ity
anal
ysi
sfo
rse
lect
edp
aram
eter
s
Pro
bab
ilit
yo
fb
ein
ga
mu
tati
on
carr
ier
Per
cen
tag
eo
fn
od
e-n
egat
ive
neo
pla
sms
dia
gn
ose
dL
ifet
ime
risk
of
bre
ast
can
cer
Gra
nn
etal
.(1
999)
,U
nit
edS
tate
s
Vie
wp
oin
t:P
ub
lic
hea
lth
Alt
ern
ativ
es:
(1)
No
gen
etic
test
ing
,st
and
ard
care
—su
rvei
llan
ce;
(2)
BR
CA
1/2
gen
etic
test
ing
(neg
ativ
e)fo
llo
wed
by
stan
dar
dca
re—
surv
eill
ance
;(3
)B
RC
A1
/2g
enet
icte
stin
g(p
osi
tiv
e),
foll
ow
edb
yo
ne
of
fou
rp
oss
ible
pre
ven
tiv
est
rate
gie
sS
tud
yp
op
ula
tio
n:
30-y
ear-
old
Ash
ken
azi
Jew
ish
wo
men
Met
ho
du
sed
toes
tim
ate
effe
ctiv
enes
s:L
iter
atu
rere
vie
wP
rim
ary
ou
tco
me
mea
sure
:L
YG
Gen
etic
test
for
spec
ific
mu
tati
on
s;fu
llse
qu
ence
anal
ysi
so
fB
RC
A1
and
BR
CA
2;
gen
etic
cou
nse
lin
g;
exam
inat
ion
san
dte
sts;
surg
ery
;d
rug
sP
rice
yea
r:19
95
Co
st-e
ffec
tiv
enes
san
aly
sis
Mar
ko
vm
od
el(c
ycl
ele
ng
thn
ot
rep
ort
ed)
Tim
eh
ori
zon
:50
yea
rs
$20,
717/
LY
G($
9507
–$46
,998
)fo
llo
wed
by
mas
tect
om
yan
do
op
ho
rect
om
yco
mb
ined
;$2
9,97
0/L
YG
($15
,333
–$65
,281
)m
aste
cto
my
alo
ne;
$72,
780/
LY
G($
23,0
14–$
240,
275)
oo
ph
ore
cto
my
alo
ne;
$134
,273
/L
YG
($82
,838
–$2
67,6
05)
surv
eill
ance
Un
cert
ain
ty:
PS
Aan
dd
eter
min
isti
co
ne-
way
sen
siti
vit
yan
aly
sis
Co
sto
fg
enet
icco
un
seli
ng
and
test
ing (c
onti
nu
ed)
585
Ta
bl
e1.
(Co
nt
in
ue
d)
Au
thor
(dat
e),
Cou
ntr
y,
stu
dy
des
ign
,re
fere
nce
Com
par
ator
Eff
ecti
ven
ess
Res
ourc
eu
se(p
rice
yea
r)D
ata
anal
ysi
sIC
ER
Par
amet
ers
dri
vin
gco
st-e
ffec
tiv
enes
s
Hei
md
alet
al.
(199
9),
No
rway
Vie
wp
oin
t:N
ot
rep
ort
edex
pli
citl
yA
lter
nat
ives
:N
og
enet
icte
stin
g(c
urr
ent
fam
ilia
lb
reas
tca
nce
rcl
inic
pra
ctic
e);
(2)
Gen
etic
test
ing
for
BR
CA
1m
uta
tio
nca
rrie
rsin
add
itio
nto
curr
ent
pra
ctic
eS
tud
yp
op
ula
tio
n:
No
tcl
earl
yre
po
rted
Met
ho
du
sed
toes
tim
ate
effe
ctiv
enes
s:P
rim
aril
yta
ken
fro
mo
ne
cen
ter;
sup
ple
men
ted
by
lite
ratu
rere
vie
wan
dex
per
tas
sum
pti
on
sP
rim
ary
ou
tco
me
mea
sure
:L
YG
Gen
etic
test
ing
;g
enet
icco
un
seli
ng
;cl
inic
alex
amin
atio
n;
foll
ow
-up
surv
eill
ance
Pri
ceY
ear:
1999
Co
st-e
ffec
tiv
enes
san
aly
sis
No
mo
del
stru
ctu
rere
po
rted
Tim
eh
ori
zon
:N
ot
rep
ort
ed
No
tex
pli
citl
yre
po
rted
Un
cert
ain
ty:
Det
erm
inis
tic
sen
siti
vit
yan
aly
sis
for
sele
cted
par
amet
ers
Effi
cacy
of
earl
yin
terv
enti
on
foll
ow
ing
ap
osi
tiv
ete
st,
the
inte
nsi
tyo
fsc
reen
ing
,an
dp
enet
ran
cean
dp
rev
alen
ceo
ffo
un
der
mu
tati
on
s
Ho
llan
det
al.
(200
9),
Un
ited
Sta
tes
Vie
wp
oin
t:S
oci
etal
Alt
ern
ativ
es:
(1)
No
gen
etic
test
ing
(sta
nd
ard
care
);(2
)G
enet
icte
stin
gfo
rB
RC
A1
/2m
uta
tio
ns
(fo
llo
wed
by
the
po
ssib
ilit
yo
fp
rev
enti
ve
surg
ery
ifte
stre
sult
po
siti
ve)
Stu
dy
po
pu
lati
on
:35
-yea
r-o
ldw
om
enw
ho
are
con
cern
edab
ou
th
avin
ga
BR
CA
1an
d/
or
BR
CA
2m
uta
tio
n
Met
ho
du
sed
toes
tim
ate
effe
ctiv
enes
s:L
iter
atu
rere
vie
wan
dex
per
tas
sum
pti
on
sP
rim
ary
ou
tco
me
mea
sure
:Q
AL
Ys
Val
uat
ion
of
hea
lth
ben
efits
:T
ime-
trad
eo
ff(p
rev
iou
sly
rep
ort
ed)
Gen
etic
test
ing
;h
ealt
hca
rew
hen
wel
l;te
rmin
alh
ealt
hca
re;
pre
ven
tiv
esu
rger
yan
dfo
llo
w-u
p;
can
cer
trea
tmen
tan
dca
reP
rice
Yea
r:20
06
Co
st-e
ffec
tiv
enes
san
aly
sis
Mar
ko
vm
od
el(1
-yea
rcy
cles
)T
ime
ho
rizo
n:
70y
ears
$900
0/Q
AL
YU
nce
rtai
nty
:P
SA
and
det
erm
inis
tic
on
e-w
ayse
nsi
tiv
ity
anal
ysi
s
Uti
lity
der
ived
fro
ma
neg
ativ
ete
stre
sult
Ten
gs
and
Ber
ry(2
000)
,U
nit
edS
tate
s
Vie
wp
oin
t:S
oci
etal
Alt
ern
ativ
es:
(1)
No
gen
etic
test
ing
(sta
nd
ard
care
);(2
)G
enet
icte
stin
gfo
rB
RC
A1
/2m
uta
tio
ns
(fo
llo
wed
by
pre
ven
tiv
est
rate
gy
fou
nd
toy
ield
the
mo
stQ
AL
Ys
inth
em
od
elif
test
resu
lts
are
po
siti
ve)
Stu
dy
po
pu
lati
on
:30
-yea
r-o
ldw
om
enin
the
Un
ites
Sta
tes,
wit
hv
ary
ing
risk
sfo
rH
BC
Met
ho
du
sed
toes
tim
ate
effe
ctiv
enes
s:L
iter
atu
rere
vie
wan
dex
per
tas
sum
pti
on
sP
rim
ary
ou
tco
me
mea
sure
:Q
AL
Ys
Val
uat
ion
of
hea
lth
ben
efits
:T
aken
fro
mp
rev
iou
sst
ud
ies
(met
ho
ds
no
tre
po
rted
)
Gen
etic
test
ing
;g
enet
icco
un
seli
ng
;p
rev
enti
ve
surg
ery
,an
dfo
llo
w-u
pca
re;
can
cer
trea
tmen
tan
dca
reP
rice
Yea
r:N
ot
rep
ort
ed
Co
st-e
ffec
tiv
enes
san
aly
sis
Mar
ko
vh
ealt
hst
ates
app
end
edto
ad
ecis
ion
tree
mo
del
(cy
cle
len
gth
no
tre
po
rted
)T
ime
ho
rizo
n:
No
tre
po
rted
$34,
000/
QA
LY
Un
cert
ain
ty:
Det
erm
inis
tic
sen
siti
vit
yan
aly
sis
for
sele
cted
par
amet
ers
Co
stan
dac
cura
cyo
fth
ete
st
HB
C,
her
edit
ary
bre
ast
can
cer;
QA
LY
,q
ual
ity
-ad
just
edli
fey
ear;
LY
G,
life
yea
rsg
ain
ed;
PS
A,
pro
bab
ilis
tic
sen
siti
vit
yan
aly
sis.
586

Ta
bl
e2.
Su
mm
ar
yo
fK
ey
Mo
de
lIn
pu
ts
an
dA
ssu
mp
tio
ns
Par
amet
erB
alm
ana
etal
.(2
00
4),
Sp
ain
Gra
nn
etal
.(1
99
9),
Un
ited
Sta
tes
Hei
md
alet
al.
(19
99
),N
orw
ayH
olla
nd
etal
.(2
00
9),
a
Un
ited
Sta
tes
Ten
gs
and
Ber
ry(2
00
0),
a
Un
ited
Sta
tes
Ty
pe
of
gen
etic
test
Fu
llse
qu
ence
anal
ysi
so
fB
RC
A1
/2:
PT
Tan
dS
SC
PT
est
for
thre
esp
ecifi
cm
uta
tio
ns
com
mo
nin
the
po
pu
lati
on
:18
5del
AG
and
5382
insC
inB
RC
A1
and
6174
del
Tin
VR
CA
2
Tes
tfo
rtw
osp
ecifi
c(t
ho
ug
hu
nsp
ecifi
ed)
mu
tati
on
sin
BR
CA
1
Fu
llse
qu
ence
anal
ysi
so
fB
RC
A1
/2F
ull
seq
uen
cean
aly
sis
of
BR
CA
1/2
Gen
etic
cou
nse
lin
gan
d/
or
oth
erg
enet
ics
serv
ice
incl
ud
ed
Yes
No
tex
pli
citl
yre
po
rted
Yes
No
tex
pli
citl
yre
po
rted
No
tex
pli
citl
yre
po
rted
Pre
ven
tiv
est
rate
gie
sin
clu
ded
An
nu
alC
lin
ical
bre
ast
exam
inat
ion
and
mam
mo
gra
ph
y
Bil
ater
alR
RS
PO
;B
ilat
eral
RR
M;
RR
Mp
lus
RR
SP
O;
Su
rvei
llan
ce(a
nn
ual
mam
mo
gra
m)
No
tin
clu
ded
RR
SP
O;
RR
M;
scre
enin
gac
cord
ing
tore
com
men
dat
ion
s(n
ot
exp
lici
tly
defi
ned
)
RR
SP
O;
RR
M;
RR
SP
Op
lus
RR
M;
‘‘no
pre
ven
tiv
em
easu
re’’
(no
tex
pli
citl
yd
efin
ed)
Pro
bab
ilit
yo
fb
ein
ga
mu
tati
on
carr
ier
No
tex
pli
citl
yre
po
rted
2.5%
inan
Ash
ken
azi
Jew
ish
po
pu
lati
on
0.6%
of
all
bre
ast
can
cers
(est
imat
edfr
om
ov
aria
nca
nce
rd
ata)
Var
ied
and
use
dfo
ran
aly
sis
(ran
ge
0%–2
0%)
Var
ied
and
use
dfo
ran
aly
sis;
BR
CA
1ra
ng
e0–
0.5;
BR
CA
2ra
ng
e0–
0.5;
Av
erag
ep
op
ula
tio
nri
skB
RC
A1
0.00
06;
Av
erag
ep
op
ula
tio
nri
skB
RC
A2
0.00
02T
est
Sen
siti
vit
yN
ot
rep
ort
ed98
%N
ot
rep
ort
ed99
%(9
5%–1
00%
ran
ge
exp
lore
din
sen
siti
vit
yan
aly
sis)
98%
Tes
tS
pec
ifici
tyN
ot
rep
ort
ed99
%N
ot
rep
ort
ed99
%(9
5%–1
00%
ran
ge
exp
lore
din
sen
siti
vit
yan
aly
sis)
99%
Tes
tco
st(p
rice
yea
r)e
1202
.02
for
gen
etic
stu
dy
of
ind
exca
sep
erfa
mil
y;
e11
26.8
8fo
rg
enet
icco
un
seli
ng
per
fam
ily
;(t
hen
calc
ula
tein
div
idu
alp
rice
sb
yes
tim
atin
gsi
xw
om
enp
erfa
mil
yre
ceiv
edth
esc
reen
ing
reco
mm
end
atio
ns
(pri
cey
ear
no
tre
po
rted
)
$450
gen
ete
stin
gfo
rth
ree
spec
ific
mu
tati
on
s;$3
00g
enet
icco
un
seli
ng
;F
ull
seq
uen
ceB
RC
A1
/2an
aly
sis
$240
0(p
rice
yea
r19
95)
e23
4,87
9fo
rte
stin
go
fp
rob
and
plu
s15
fam
ily
mem
ber
s;e
131,
221
gen
etic
cou
nse
lin
go
fp
rob
and
plu
s15
fam
ily
mem
ber
s;e
2250
full
gen
esc
reen
ing
BR
CA
1/2
(pri
cey
ear
1999
)
$254
2,ra
ng
e$1
301–
5421
(pri
cey
ear
2006
)$3
10p
rete
stco
un
seli
ng
;$2
580
firs
tfa
mil
ym
emb
erte
sted
(pri
cey
ear
no
tre
po
rted
)
Lif
etim
eri
sko
fb
reas
tca
nce
r58
.5%
30-y
ear-
old
BR
CA
1/2
mu
tati
on
carr
ier;
8.6%
30-y
ear-
old
no
nm
uta
tio
nca
rrie
r
56%
30-y
ear-
old
wo
men
wit
ho
ne
of
thre
esp
ecifi
cm
uta
tio
ns
50%
ov
er25
yea
rs(a
ge
35–6
0)fo
rsp
ecifi
cB
RC
A1
mu
tati
on
carr
iers
;18
.25%
ov
er25
yea
rs(a
ge
35–6
0)fo
rn
on
mu
tati
on
carr
iers
inth
ep
rog
ram
73.5
%o
ver
50y
ears
(ag
e30
–80
)B
RC
A1
/2m
uta
tio
nca
rrie
r;6.
8%o
ver
50y
ears
(ag
e30
–80)
gen
eral
po
pu
lati
on
BR
CA
1m
uta
tio
nca
rrie
rs0.
71;
BR
CA
2m
uta
tio
nca
rrie
rs0.
84;
no
nca
rrie
rs0.
126
(con
tin
ued
)
587
Ta
bl
e2.
(Co
nt
in
ue
d)
Par
amet
erB
alm
ana
etal
.(2
00
4),
Sp
ain
Gra
nn
etal
.(1
99
9),
Un
ited
Sta
tes
Hei
md
alet
al.
(19
99
),N
orw
ayH
olla
nd
etal
.(2
00
9),
a
Un
ited
Sta
tes
Ten
gs
and
Ber
ry(2
00
0),
a
Un
ited
Sta
tes
Lif
etim
eri
sko
fo
var
ian
can
cer
No
tre
po
rted
16%
30-y
ear-
old
wo
men
wit
ho
ne
of
thre
esp
ecifi
cm
uta
tio
ns
No
tin
clu
ded
27.8
%o
ver
50y
ears
(ag
e30
–80)
BR
CA
1/2
mu
tati
on
carr
ier;
1.8%
ov
er50
yea
rs(a
ge
30–8
0)g
ener
alp
op
ula
tio
n
BR
CA
1m
uta
tio
nca
rrie
rs0.
63;
BR
CA
2m
uta
tio
nca
rrie
rs0.
27;
No
nca
rrie
rs0.
0157
Uti
lity
val
ues
No
tin
clu
ded
No
tin
clu
ded
No
tin
clu
ded
Ag
e-sp
ecifi
cu
tili
tyat
35y
ears
wel
lst
ate,
0.92
(ran
ge
0.8–
1);
Dec
reas
ein
uti
lity
iny
ear
of
bre
ast
can
cer
dia
gn
osi
s,0.
2(r
ang
e0–
1);
Dec
reas
ein
uti
lity
iny
ear
of
ov
aria
nca
nce
rd
iag
no
sis,
0.29
(ran
ge
0–1)
;U
tili
tyin
firs
ty
ear
po
st-
RR
SP
O,
0.68
(ran
ge
0.5–
1);
Uti
lity
infi
rst
yea
rp
ost
-RR
M,
0.82
(ran
ge
0.5–
1)
Bre
ast
can
cer
0.89
;O
var
ian
can
cer
0.82
;B
reas
tan
dO
var
ian
Can
cer
0.82
;R
RM
0.86
;R
RS
PO
bef
ore
age
50w
ith
ho
rmo
ne
rep
lace
men
t0.
91;
RR
SP
Ob
efo
reag
e50
wit
ho
ut
ho
rmo
ne
rep
lace
men
t1;
RR
Mp
lus
RR
SP
O0.
86.
Up
tak
eo
fB
RC
A1
/2te
stin
gam
on
gfa
mil
ym
emb
ers
No
tre
po
rted
No
tre
po
rted
100%
No
tre
po
rted
No
tre
po
rted
Up
tak
eo
fp
rev
enti
ve
stra
teg
ies
No
tre
po
rted
No
tre
po
rted
No
tin
clu
ded
RR
Mat
35y
ears
,B
RC
A1
/2m
uta
tio
n0.
15(r
ang
e0.
03–0
.54)
;R
RS
PO
at35
yea
rs,
BR
CA
1/2
mu
tati
on
0.25
(ran
ge
0.13
–0.7
8)
Ass
um
ed10
0%o
fB
RC
A1
/2-
po
siti
ve
pat
ien
tsw
ou
ldo
pt
for
the
pre
ven
tiv
est
rate
gy
sho
wn
asm
ost
effe
ctiv
eb
ym
od
el:
RR
SP
Oat
age
30o
r50
.Im
pac
to
fp
rev
enti
ve
stra
teg
ies
No
tex
pli
citl
yre
po
rted
RR
SP
Ore
du
ced
risk
of
ov
aria
nca
nce
rb
y45
%;
RR
Mre
du
ced
risk
of
bre
ast
can
cer
by
90%
No
tin
clu
ded
RR
SP
O(b
efo
reag
e50
)re
du
ced
risk
of
bre
ast
can
cer
by
0.45
(ran
ge
0.25
–0.6
5);
RR
SP
Ore
du
ced
risk
of
ov
aria
nca
nce
rb
y0.
96(r
ang
e0.
9–0.
99);
RR
Mre
du
ced
risk
of
bre
ast
can
cer
by
0.9
(ran
ge
0.8–
0.99
);R
RM
no
red
uct
ion
inri
sko
fo
var
ian
can
cer
RR
SP
Ore
du
ced
risk
of
bre
ast
can
cer
by
61%
;R
RS
PO
red
uce
dri
sko
fo
var
ian
can
cer
by
46%
;R
RM
red
uce
dri
sko
fb
reas
tca
nce
rb
y91
%;
RR
Mn
ore
du
ctio
nin
risk
of
ov
aria
nca
nce
r;R
RS
PO
plu
sR
RM
red
uce
dri
sko
fb
reas
tca
nce
rb
y91
%;
RR
SP
Op
lus
RR
Mre
du
ced
risk
of
ov
aria
nca
nce
rb
y46
%
Wh
enst
ud
ies
hav
ere
po
rted
aco
stfo
rg
enet
icco
un
seli
ng
bu
tn
ot
men
tio
ned
itin
the
tex
tac
cou
nt
of
cost
s,th
isis
des
crib
edas
‘‘No
tex
pli
citl
yre
po
rted
.’’aH
oll
and
(200
9)an
dT
eng
san
dB
erry
(200
0)d
on
ot
exp
lici
tly
stat
e‘‘f
ull
seq
uen
cean
aly
sis,
’’b
ut
fro
mth
ete
xtin
each
itis
clea
rth
atth
eyar
ese
arch
ing
for
mu
tati
on
sac
ross
the
wh
ole
of
the
two
BR
CA
gen
es.
RR
M,
risk
red
uci
ng
mas
tect
om
y;
RR
SP
O,
risk
red
uci
ng
salp
ing
o-o
op
ho
rect
om
y;
PT
T,
pro
tein
tru
nca
tio
nte
st;
SS
CP
,si
ng
le-s
tran
dco
nfo
rmat
ion
po
lym
orp
his
m.
588

The telephone survey confirmed that Sanger DNA se-quencing followed by MLPA is used in the majority of U.K.diagnostic laboratories offering a BRCA1/2 mutation testingservice. These findings suggest that Sanger sequencing fol-lowed by MLPA is the legitimate choice for a standard prac-tice comparator in England and Wales. However, 2 of 14laboratories were using NGS technology at time of the survey.There is, therefore, some evidence that new genetic testingtechnologies are already being used for BRCA1/2 testing. Thissuggests that it is timely to think about generating economicevidence to support the use of NGS methods before they arewidely used in clinical practice.
BRCA1/2 testing is offered as part of a clinical geneticsservice and involves a defined care pathway for womensuspected to be predisposed to HBC and their family mem-bers. Not all women who have family members with breastcancer can be or should be referred and offered genetic testing.National guidelines specify who should be offered mutationtesting on the basis of a patients’ risk for carrying a mutationdetermined by the presence and age at diagnosis of cancer inother family members, using a risk assessment tool such as theManchester scoring system (Evans et al., 2004). Results fromgenetic testing may then impact the coordination of preven-tive care for patients. None of the economic evaluationsidentified considered the challenge of identifying variants ofuncertain significance (VUS), which are found in around 5%–6% of samples. These VUS results potentially have a negativeoutcome on individuals concerned as they create greater un-certainty. As such, thresholds may need to take into account abalance that reflects a greater chance of identifying a mean-ingful pathogenic mutation than a VUS. The findings fromthis review of published economic evaluations indicates thatdevelopment of national guidelines, as well as the current riskthreshold of carrying a BRCA1/2 mutation, was not informedby economic evidence. This lack of economic evidence sup-porting current clinical practice has implications for futureHTA of genetic testing strategies using new technologies. Thefirst key step of any evaluation is to identify current practiceand understand how a new intervention will change currentpractice. In the absence of published data, it is not clearwhether current practice, using Sanger DNA sequencing withMLPA combined with a risk threshold for testing set at 20%, isthe most effective or cost-effective use of healthcare resources.Existing national guidelines have been largely informedby pragmatic decision making by experts advising in guide-line development. The setting of the 20% threshold in 2004likely reflected the large backlog of untested samples andthe need to fully test samples that were previously only par-tially screened by techniques employed at the time of theguidelines.
Providing BRCA1/2 testing will also be constrained by theavailability of genetic counseling services in addition to lab-oratory capacity and test result turnaround time. Only two ofthe economic evaluations (Heimdal et al., 1999; Balmana et al.,2004) identified clearly considered genetic testing as an inte-gral part of a clinical genetics service with associated geneticcounseling. Furthermore, the nature of the genetic testing in-tervention differed in the key studies. One study (Heimdalet al., 1999) only considered testing for BRCA1 mutations,while two (Grann et al., 1999; Heimdal et al., 1999) used anintervention testing for specific mutations instead of full se-quence analysis. However, current U.K. clinical practice is to
fully sequence both BRCA1 and BRCA2 even though availableevidence would suggest that the probability of an individualcarrying a mutation in both genes is negligible.
Significant costs and benefits of genetic testing for HBCpredisposition are associated with events that occur after thetest, as a result of the test outcome. The same is true for a rangeof medical diagnostic interventions. It is therefore necessary tobe clear what current care pathways involve and how a ge-netic test will change such pathways. There is no publishedevidence that adequately describes current care pathways forgenetic testing for predisposition to HBC. Furthermore, whilethe QALY is now routinely used to measure benefits in theeconomic evaluation of pharmaceuticals, there is concern inthat such a measure cannot capture the full potential benefits,such as familial and nonhealth effects, which are relevant togenetic testing and diagnostics (Basu and Meltzer, 2005;Grosse et al., 2008).
More generally, challenges for HTA of genetic testing werealso identified when conducting this review. One key chal-lenge is how best to generate data on the resource use for carepathways affected by genetic testing and also how to quantifythe relative benefits to patients from different approaches togenetic testing in terms of life-years gained and QALYs. Thisis particularly problematic because of the lack of robust pro-spective data on the relative effectiveness of genetic tests thatis driven, in part, by the current regulatory processes for di-agnostics. This lack of data places reliance on the elicitation ofexpert opinion to generate effectiveness, utility, and cost data,but the elicitation process should also use robust and appro-priate methods (Sullivan and Payne, 2011). Diagnostic accu-racy is a surrogate outcome (Caro et al., 2010), but still anecessary component of an economic evaluation of NGS ge-netic testing; however, the sensitivity and specificity of cur-rent testing methods were not always explicitly reported.Current regulatory mechanisms do not encourage the pro-duction of robust evidence sufficient for populating economicmodels to inform decision making (Payne, 2009).
Policy implications
As decision-making bodies such as NICE move to evaluatediagnostic services alongside pharmaceuticals as part of thereimbursement package and technology in medical diagnos-tics continues to evolve rapidly, it is necessary that sufficienteconomic evidence is generated. This study has highlightedspecific challenges for the robust economic evaluation of newtechnological developments for diagnostic testing. The keychallenges are as follows: clearly describing current practiceand how the existing technology is used and understandinghow the new technology can change current practice, in thelaboratory and in terms of clinical services and subsequentcare pathways. The lack of robust economic data to supportnational guidance on genetic testing for HBC in England andWales is likely to be a reflection of a broader paucity of data topopulate economic models.
Conclusions
There is a lack of economic evidence to support the choiceof the current risk threshold for BRCA1/2 testing in Englandand Wales. The lack of economic evidence supporting thecurrent risk threshold for in national guidance has implica-tions for the efficient use of healthcare resources and the
ECONOMIC EVIDENCE ON GENETIC TESTING FOR BREAST CANCER PREDISPOSITION 589

design of economic evaluations of new technologies forBRCA1/2 testing. It is not clear, from currently available eco-nomic evidence, whether the most efficient use of healthcareresources is to improve the use and selection of women usingthe current DNA sequencing technology or to introduce a newNGS technology to improve laboratory capacity to expand thenumber of women tested for predisposition to HBC.
Acknowledgments
The authors would like to acknowledge the expertise andkind help of the following people, who helped us to under-stand cross-border differences in laboratory procedures andcare pathways relevant to genetic testing for breast cancerpredisposition:
Marion McAllister, Developmental Biomedicine, Uni-versity of Manchester; Gert Matthijs, Centre for Human Ge-netics, University Hospitals Leuven; Harry Cuppens, Centrefor Human Genetics, University Hospitals Leuven; GenevieveMichils, Centre for Human Genetics, University HospitalsLeuven; Frans Hogervorst, Diagnostic Oncology, Nether-lands Cancer Institute.
Disclosure Statement
The research leading to these results has received fundingfrom the European Community’s Seventh Framework Pro-gram FP7/2007-2013 under grant agreement no. 223143(Project acronym TECHGENE). The work of D.G.E., S.C.R.,and W.G.N. is supported by the NIHR Manchester Biomedi-cal Research Centre.
References
Anderson K, Jacobson JS, Heitjan DF, Zivin JG, Hershman D,Neugut AI, Grann VR (2006) Cost-effectiveness of preventivestrategies for women with a BRCA1 or a BRCA2 mutation.[Summary for patients in Ann Intern Med 2006, 144:I40;PMID: 16549849]. Ann Intern Med 144:397–406.
Balmana J, Sanz J, Bonfill X, Casado A, Rue M, Gich I, Diez O,Sabate JM, Baiget M, Alonso MC (2004) Genetic counsel-ing program in familial breast cancer: analysis of its effec-tiveness, cost and cost-effectiveness ratio. Int J Cancer 112:647–652.
Basu A, Meltzer D (2005) Implications of spillover effects withinthe family for medical cost-effectiveness analysis. J HealthEcon 24:751–773.
Cancer Research Uk (2011) Breast Cancer: UK Incidence Statis-tics. London. Available at http://info.cancerresearchuk.org/cancerstats/types/breast/incidence/#prev, (accessed October15, 2011). (Online).
Caro JJ, Nord E, Siebert U, Mcguire A, Mcgregor M, Henry D,De Pouvourville G, Atella V, Kolominsky-Rabas P (2010) Theefficiency frontier approach to economic evaluation of health-care interventions. Health Econ 19:1117–1127.
Claus EB, Risch N, Thompson WD (1991) Genetic analysis ofbreast cancer in the cancer and steroid hormone study. Am JHum Genet 48:232–242.
Clinical Molecular Genetics Society (2011) Clinical MolecularGenetics Society Audit 2009–2010. Clinical Molecular GeneticsSociety, London.
Craig D, Rice S, Aguiar-Ibanez R, Glanville J, Kleijnen J,Drummond M (2007) Chapter III: guidance for writing NHSEED abstracts. In: Craig D, Rice S (eds) NHS Economic Eva-
luation Database Handbook, 3rd edition. Centre for Reviewsand Dissemination, University of York, York, United King-dom.
CRD (2011) Centre for Reviews and Dissemination: IdentifyingStudies for Inclusion in NHS EED: Search Filter Resource.London. Available at www.york.ac.uk/inst/crd/intertasc/nhs_eed_strategies.html, (accessed July 25, 2011). (Online).
Drummond MF, Sculpher M, Torrance GW, O’brien B, StoddartGL (2005) Methods for the Economic Evaluation of HealthCare Programmes. Oxford University Press, Oxford.
Esteban-Cardenosa E, Duran M, Infante M, Velasco E, Miner C(2004) High-throughput mutation detection method to scanBRCA1 and BRCA2 based on heteroduplex analysis by cap-illary array electrophoresis. Clin Chem 50:313–320.
Evans DG, Eccles D, Rahman N, Young KC, Bulman M, Amir E,Shenton A, Howell A, Lalloo F (2004) A new scoring systemfor the chances of identifying a BRCA1/2 mutation outper-forms existing models including BRCAPRO. J Med Genet41:474–480.
Evans DG, Howell A (2007) Breast cancer risk-assessmentmodels. Breast Cancer Res 9:213.
Grann VR, Jacobson JS, Whang W, Hershman D, Heitjan DF,Antman KH, Neugut AI (2000) Prevention with tamoxifenor other hormones versus prophylactic surgery in BRCA1/2-positive women: a decision analysis. Cancer J Sci Am 6:13–20.
Grann VR, Panageas KS, Whang W, Antman KH, Neugut AI(1998) Decision analysis of prophylactic mastectomy and oo-phorectomy in BRCA1-positive or BRCA2-positive patients. JClin Oncol 16:979–985.
Grann VR, Whang W, Jacobson JS, Heitjan DF, Antman KH,Neugut AI (1999) Benefits and costs of screening AshkenaziJewish women for BRCA1 and BRCA2. J Clin Oncol 17:494–500.
Griebsch I, Brown J, Boggis C, Dixon A, Dixon M, Easton D,Eeles R, Evans DG, Gilbert FJ, Hawnaur J, Kessar P, LakhaniSR, Moss SM, Nerurkar A, Padhani AR, Pointon LJ, PottertonJ, Thompson D, Turnbull LW, Walker LG, Warren R, LeachMO; UK Magnetic Resonance Imaging in Breast Screening(MARIBS) Study Group (2006) Cost-effectiveness of screeningwith contrast enhanced magnetic resonance imaging vs X-raymammography of women at a high familial risk of breastcancer. Br J Cancer 95:801–810.
Grosse SD, Wordsworth S, Payne K (2008) Economic methodsfor valuing the outcomes of genetic testing: beyond cost-effectiveness analysis. Genet Med 10:648–654.
Heimdal K, Maehle L, Moller P (1999) Costs and benefits ofdiagnosing familial breast cancer. Dis Markers 15:167–173.
Holland ML, Huston A, Noyes K (2009) Cost-effectiveness oftesting for breast cancer susceptibility genes. Value Health12:207–216.
House of Lords Science and Technology Committee (2009)House of Lords Science and Technology Committee, 2nd Re-port of Session 2008–2009: ‘‘Genomic Medicine’’. London:House of Lords.
Hutchison CA (2007) DNA sequencing: bench to bedside andbeyond. Nucleic Acids Res 35:6227–6237.
Lewingroup (2009) The Value of Diagnostic Screening and La-boratory Tests for Prevention and Health Care Improvement.The Lewin Group, Falls Church, Virginia.
Mcintosh A, Shaw C, Evans DG, Turnbull N, Bahar N, BarclayM, Easton D, Emery J, Gray J, Halpin J, Hopwood P, Mckay J,Sheppard C, Sibbering M, Watson W, Wailoo A (2004) Clinicalguidelines and evidence review for the classification and care
590 SULLIVAN ET AL.

of women at risk of familial breast cancer. National Collabor-ating Centre for Primary Care/University of Sheffield, London.
MRC (2009) Medical Research Council. News & Publications.Further MRC Investment in High-Throughput Sequencing.Available at www.mrc.ac.uk/Newspublications/News/MRC006188, (accessed May 3, 2010). (Online).
National Institute for Health and Clinical Excellence (2008)Guide to the Methods of Technology Appraisal. NationalHealth Service National Institute for Health and Clinical Ex-cellence, London.
Newman B, Austin MA, Lee M, King MC (1988) Inheritance ofhuman breast cancer: evidence for autosomal dominanttransmission in high-risk families. Proc Natl Acad Sci U S A85:3044–3048.
Norman RPA, Evans DG, Easton DF, Young KC (2007) The cost-utility of magnetic resonance imaging for breast cancer in BRCA1mutation carriers aged 30–49. Eur J Health Econ 8:137–144.
Norum J, Hagen AI, Maehle L, Apold J, Burn J, Moller P (2008)Prophylactic bilateral salpingo-oophorectomy (PBSO) with orwithout prophylactic bilateral mastectomy (PBM) or no in-tervention in BRCA1 mutation carriers: a cost-effectivenessanalysis. Eur J Cancer 44:963–971.
Payne K (2009) Fish and chips all round? Regulation of DNA-based genetic diagnostics. Health Econ 18:1233–1236.
Peters N, Domchek SM, Rose A, Polis R, Stopfer J, Armstrong K(2005) Knowledge, attitudes, and utilization of BRCA1/2testing among women with early-onset breast cancer. GenetTest 9:48–53.
Philips Z, Bojke L, Sculpher M, Claxton K, Golder S (2006) Goodpractice guidelines for decision-analytic modelling in healthtechnology assessment: a review and consolidation of qualityassessment. Pharmacoeconomics 24:355–371.
Plevritis SK, Kurian AW, Sigal BM, Daniel BL, Ikeda DM,Stockdale FE, Garber AM (2006) Cost-effectiveness of screen-ing BRCA1/2 mutation carriers with breast magnetic reso-nance imaging. JAMA 295:2374–2384.
Reis MM, Tavakoli M, Dewar J, Goudie D, Cook A, Mcleish L,Young D, Kenyon J, Steel M (2009) Evaluation of a surveil-lance programme for women with a family history of breastcancer. J Med Genet 46:319–323.
Sanger F, Nicklen S, Coulson AR (1977) DNA sequencing withchain-terminating inhibitors. Proc Natl Acad Sci U S A74:5463–5467.
Sevilla C, Julian-Reynier C, Eisinger F, Stoppa-Lyonnet D,Bressac-De Paillerets B, Sobol H, Moatti J-P (2003) Impact ofgene patents on the cost-effective delivery of care: the case ofBRCA1 genetic testing. Int J Technol Assess Health Care19:287–300.
Sevilla C, Moatti, J-P, Julian-Reynier C, Eisinger F, Stoppa-Lyonnet D, Bressac-De Paillerets B, Sobol H (2002) Testing forBRCA1 mutations: a cost-effectiveness analysis. Eur J HumGenet 10:599–606.
Stratton MR, Rahman N (2008) The emerging landscape ofbreast cancer susceptibility. Nat Genet 40:17–22.
Sullivan W, Payne K (2011) The appropriate elicitation of expertopinion in economic models: making expert data fit for pur-pose. Pharmacoeconomics 29:455–459.
Tengs TO, Berry DA (2000) The cost effectiveness of testing forthe BRCA1 and BRCA2 breast-ovarian cancer susceptibilitygenes. Dis Manage Clin Outcomes 1:15–24.
Wilson BJ, Torrance N, Mollison J, Wordsworth S, Gray JR,Haites NE, Grant A, Campbell MK, Miedyzbrodzka Z, ClarkeA, Watson MS, Douglas A (2005) Improving the referral pro-cess for familial breast cancer genetic counselling: findings ofthree randomised controlled trials of two interventions. HealthTechnol Assess 9:iii–iv, 1–126.
Address correspondence to:Katherine Payne, Ph.D.
Department of Health Sciences—EconomicsSchool of Community Based Medicine
The University of Manchester4th Floor, University Place
Jean McFarlane Building, Oxford RoadManchester M13 9PL
United Kingdom
E-mail: [email protected]
ECONOMIC EVIDENCE ON GENETIC TESTING FOR BREAST CANCER PREDISPOSITION 591






![Genetic predisposition to ductal carcinoma in situ of the breast · 2017. 5. 4. · (OR=2.2, 95 % CI 1.0, 4.2) than invasive disease (OR=1.5, 95 % CI 1.0, 2.2) [14]. However, this](https://img.dokumen.tips/doc/110x75/60a43a3fc43332279826c041/genetic-predisposition-to-ductal-carcinoma-in-situ-of-the-breast-2017-5-4-or22.jpg)