Embed Size (px)
Citation preview

Desmopressin Resistant Nocturnal PolyuriaSecondary to Increased Nocturnal Osmotic ExcretionJo L. Dehoorne,* Ann M. Raes, Erik van Laecke, Piet Hoebeke and Johan G. Vande WalleFrom the Pediatric Nephrology and Pediatric Urology Department, University Hospital Ghent, Ghent, Belgium
Purpose: We investigated the role of increased solute excretion in children with desmopressin resistant nocturnal enuresisand nocturnal polyuria.Materials and Methods: A total of 42 children with monosymptomatic nocturnal enuresis and significant nocturnalpolyuria with high nocturnal urinary osmolality (more than 850 mmol/l) were not responding to desmopressin. A 24-hoururinary concentration profile was obtained with measurement of urine volume, osmolality, osmotic excretion and creatinine.The control group consisted of 100 children without enuresis.Results: Based on osmotic excretion patients were classified into 3 groups. Group 1 had 24-hour increased osmotic excretion,most likely secondary to a high renal osmotic load. This was probably diet related since 11 of these 12 patients were obese.Group 2 had increased osmotic excretion in the evening and night, probably due to a high renal osmotic load caused by thediet characteristics of the evening meal. Group 3 had deficient osmotic excretion during the day, secondary to extremely lowfluid intake to compensate for small bladder capacity.Conclusions: Nocturnal polyuria with high urinary osmolality in our patients with desmopressin resistant monosymptom-atic nocturnal enuresis is related to abnormal increased osmotic excretion. This may be explained by their fluid and diethabits, eg daytime fluid restriction, and high protein and salt intake.
Key Words: bladder, urination disorders, osmosis, deamino arginine vasopressin
Primary nocturnal enuresis is a heterogeneous disorderwith various underlying pathophysiological mecha-nisms, causing a mismatch between nocturnal BC and
the amount of urine produced during sleep at night in asso-ciation with simultaneous failure of the patient to respond tothe full bladder by awakening.1,2
Many groups have documented NP as one of the essentialcausal factors of this mismatch. Norgaard3 and Rittig4 et alnoted a deficient increase in nocturnal AVP in a large pro-portion of children with enuresis which was responsible atleast in part for this NP. A nocturnal defect in AVP secretionwith a resultant increase in free water excretion could ex-plain why most patients are found to produce large quanti-ties of hypo-osmolar urine at night compared to during theday.3–5 Based on these findings DDAVP has been used ex-tensively for PNE in the last 2 decades and a response of upto 70% has been reported in various studies.3,6 Althoughseveral studies have shown that decreased BC, possiblyrelated to overactive bladder, is an important factor inDDAVP resistance or nonresponse,1 DDAVP resistance inpatients with documented NP in the absence of any bladderdysfunction and/or a small BC remains obscure. A DDAVPresistance or nonresponse is classically defined as a decreasein the number of wet nights of less than 50% (anti-enureticeffect) without mentioning the antidiuretic effect. An insuf-ficient antidiuretic effect may be explained by 3 mecha-nisms, that is insufficient renal concentrating capacity, thepoor pharmacokinetic properties of intranasal DDAVP and
* Correspondence: Pediatric Nephrology and Pediatric UrologyDepartment, University Hospital Ghent, Ghent, Belgium.
0022-5347/06/1762-0749/0THE JOURNAL OF UROLOGY®
Copyright © 2006 by AMERICAN UROLOGICAL ASSOCIATION
749
high Eosm. In the absence of evidence of abnormal renalconcentrating capacity the well-known poor pharmacoki-netic and dynamic characteristics of DDAVP may explaininsufficient anti-enuretic effect related to an insufficient an-tidiuretic effect. However, this results rather in a partialresponse than in a nonresponse because the bioavailabilityof DDAVP may differ among individuals and among days in1 patient. Although it is evident that high nocturnal Eosmleads to NP after maximal concentrating capacity is at-tained, to our knowledge this has never been identified as apathogenetic factor in enuresis. We describe 42 childrenwith PNE and significant NP who were not responding toDDAVP. All had increased solute excretion, as reflected byhigh nocturnal urinary osmolality (more than 850 mmol/l).
MATERIALS AND METHODS
We retrospectively reviewed the records of a patient group of30 boys and 12 girls 8 to 15 years old with clinical charac-teristics of DDAVP resistant NP. These patients were re-cruited from 2,112 consecutive patients treated for bedwet-ting at a tertiary enuresis center during 2000 to 2002. Atstudy intake all patients answered a standard questionnaireand while at home they recorded a 2-week diary document-ing voiding frequency, wetting episodes and bowel habits.Health was confirmed by physical examination and ultra-sound of the bladder and kidney. Children with organicurological and renal disease, diabetes insipidus, insulin de-pendent diabetes mellitus, cardiopathy and the ongoing useof drugs interfering with renal function were excluded. Noc-
turnal urine output was calculated as the sum of the changeVol. 176, 749-753, August 2006Printed in U.S.A.
DOI:10.1016/S0022-5347(06)00297-7
DESMOPRESSIN RESISTANT NOCTURNAL POLYURIA750
in diaper weight and volume of the first morning void. Blad-der volume was estimated as MBC during water load andforced diuresis. The patient was asked to drink as much aspossible, postpone voiding as long as possible and then mea-sure the volume after micturition. The largest volume of atleast 6 measurements was considered MBC. MBC was pre-ferred instead of functional BC (largest daytime void on afrequency-volume chart) during school time because func-tional BC is mainly influenced by the number of voidingmoments (playtimes) and fluid intake and, thus, it does notidentify maximal functional bladder volume.
Inclusion criteria were 1) PNE according to ICCS criteriawith at least 10 enuresis episodes in 2 weeks and absentdaytime incontinence, 2) DDAVP nonresponse to a mini-mum dose of 20 �g DDAVP intranasally daily for at least 4weeks and 3) NP for more than 10 of 14 nights, defined asnocturnal diuresis volume higher than EBC for age usingthe formula of Koff,7 (age in years � 2) � 30 ml, and higherthan MBC.
To evaluate the circadian rhythm of diuresis in thishighly select study population a simple domestic test wasdesigned in which the 24-hour urinary concentration profilewas obtained during a normal day and night (normal sleep-ing hours). Day and night were divided into 4 equal periods,including D1 to D4 and N1 to N4, respectively, starting inthe morning with D1 and ending with the last nighttimecollection N4. In each timed urine collection urine volumeUosm and Eosm were measured. Because sleep durationdiffers with age, we preferred to use normal sleeping hoursto differentiate the day and night instead of using fixedperiods of 4 � 3 hours. Parents woke their children withenuresis at the scheduled times at night. The diuresis rate isexpressed in ml/kg per hour and Eosm is expressed inmOsm/kg per hour. This allowed us to compare childrenwith different sizes and ages while avoiding a large SD.
Normalization for body weight was done because bodyweight differed significantly among patients due to the largesize and age distribution. All patients had already beentreated more than 6 months and, therefore, they received astandardized fluid intake advice (� 1,500 ml/kg/m2 dailydivided throughout the day). All drugs were stopped at least48 hours before urine collection. Patients were classifiedaccording to Eosm results. The control group consisted of ahistorical cohort of 100 children 7 to 16 years old with anequal male-to-female ratio that was randomly selected froma population not presenting for NE, on whom part of thesedata have already been published.5
Values are reported as the mean � 1 SD. Differences inall parameters between patients and controls were evalu-ated statistically using the Kruskal-Wallis and Mann-Whit-ney U tests.
RESULTS
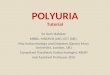
All patients had significant NP and increased overnightEosm compared to the control group (greater than 0, 81mOsm/kg per hour). Patients were further subtyped into 3groups according to Eosm during the day, that is D1 to D3greater or less than 1, 7 mOsm/kg per hour and D4 greateror less than 1, and 79 mOsm/kg per hour. We used as a cutoffpoint the mean � 1 SD in the control population (table 1).Results were plotted as the mean � 1 SD against the refer-
ence frame of controls for urinary Eosm, diuresis rate andurinary osmolality in each of the 3 patient groups during24-hour collections (see figure).
Group 1 consisted of 12 patients with significantly in-creased 24-hour Eosm (1.60 � 0.14 vs 1.10 � 0.17 mOsm/kgper hour, p �0.01). This increase in Eosm persisted duringthe day and night (table 1 and part A of figure). Uosm washigher during the day and night, although only significantlydifferent from D1 to D3 (p �0.01, table 2 and part C offigure). These patients excreted significantly larger volumesof urine during the night (p �0.01, table 3 and part B offigure). Of these 12 patients 11 had a body mass indexgreater than the 90th percentile, indicating obesity.
Group 2 consisted of 9 patients with a moderate increasein 24-hour Eosm (1.34 � 0.17 vs 1.10 � 0.17 mOsm/kg perhour, p �0.05, table 1). This was due to an important in-crease in Eosm before bedtime (D4) and in nighttime Eosm(part A of figure). The diuresis rate was lower during the day(D1 to D3), although not statistically significantly, and itincreased before bedtime (D4). During the night except forthe early morning period (N4) there was a significant in-crease in the diuresis rate (p �0.05, table 3 and part B offigure). Uosm was higher throughout the whole day andnight but only statistically significant in the pre-bedtimeperiod (D4) (p �0.05, table 2 and part C of figure).
Group 3 consisted of 21 patients with normal 24-hourEosm (table 1). Eosm was low during the day (D1 to D4) andonly statistically significant for D1 (table 1). However, Eosmincreased during the night (N1 to N4). N1 and N2 valueswere statistically significant (p �0.05, part A of figure).
Uosm was significantly higher throughout the day (ex-cept for D4 p �0.05). It was also significantly higherthroughout the night and only statistically significant for N4(p �0.05, table 2 and part C of figure). There was no increasein 24-hour Eosm.
The diuresis rate was significantly lower during the day(D1 to D4) (p �0.05). Except for N4 the nighttime diuresisrate was significantly increased (p �0.05, table 3 and part Bof figure). Of these 21 patients 20 had a small BC and MBCwas less than 65% of EBC, as calculated with the Koffformula.
DISCUSSION
Healthy children and adults have pronounced circadianvariations in the amount and composition of urine outputwith a decrease in nocturnal diuresis as well as in theamount of water, electrolytes and other osmotically activesolutes excreted.8,9 In children this nycthemeral rhythm iscontrolled by increased nocturnal release of hormones thatregulate free water excretion (AVP)4 or solute excretion (an-
TABLE 1. Eosm during day and night
Mean Eosm � SD (mOsm/kg/hr)
Controls Group 1* Group 2 Group 3
No. pts 100 12 9 21D1–3 1.43 � 0.14 2.06 � 0.16 1.40 � 0.17 1.08 � 0.07*D4 1.41 � 0.19 2.01 � 0.16 2.12 � 0.25* 1.40 � 0.06N1–4 0.65 � 0.08 0.99 � 0.09 1.00 � 0.12 0.89 � 0.07*24-Hr 1.10 � 0.17 1.60 � 0.14 1.34 � 0.17* 1.05 � 0.08
* p �0.05.
giotensin II and aldosterone).10 Although many groups have
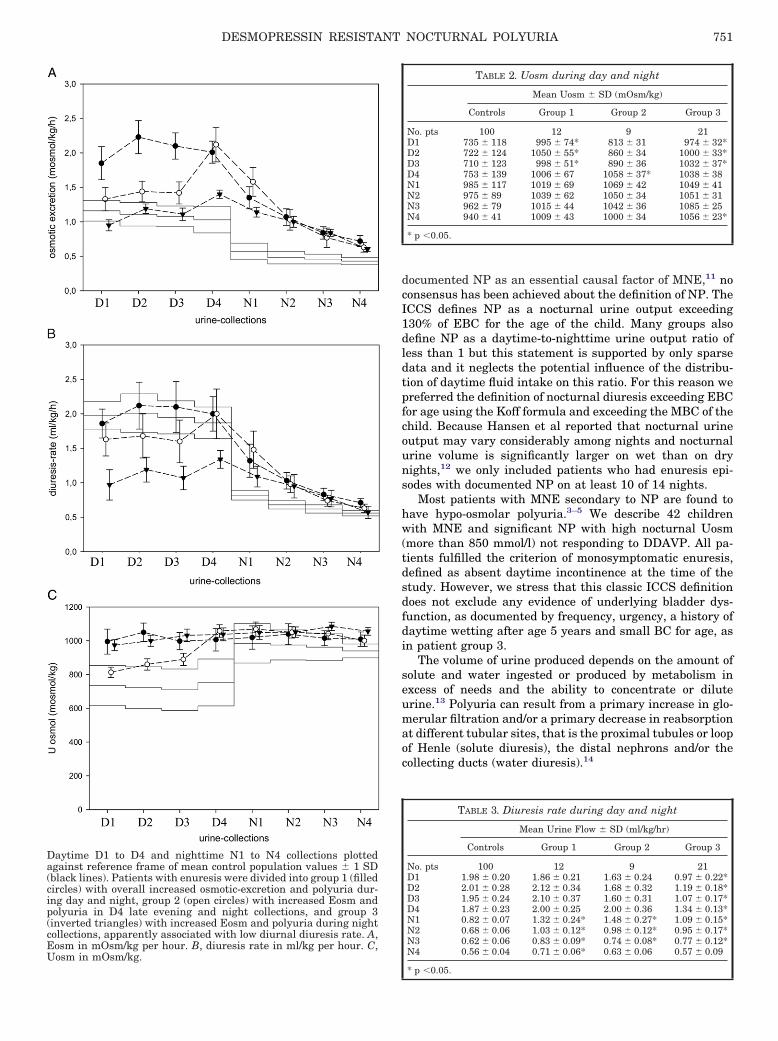
Eosm in mOsm/kg per hour. B, diuresis rate in ml/kg per hour. C,Uosm in mOsm/kg.
DESMOPRESSIN RESISTANT NOCTURNAL POLYURIA 751
documented NP as an essential causal factor of MNE,11 noconsensus has been achieved about the definition of NP. TheICCS defines NP as a nocturnal urine output exceeding130% of EBC for the age of the child. Many groups alsodefine NP as a daytime-to-nighttime urine output ratio ofless than 1 but this statement is supported by only sparsedata and it neglects the potential influence of the distribu-tion of daytime fluid intake on this ratio. For this reason wepreferred the definition of nocturnal diuresis exceeding EBCfor age using the Koff formula and exceeding the MBC of thechild. Because Hansen et al reported that nocturnal urineoutput may vary considerably among nights and nocturnalurine volume is significantly larger on wet than on drynights,12 we only included patients who had enuresis epi-sodes with documented NP on at least 10 of 14 nights.
Most patients with MNE secondary to NP are found tohave hypo-osmolar polyuria.3–5 We describe 42 childrenwith MNE and significant NP with high nocturnal Uosm(more than 850 mmol/l) not responding to DDAVP. All pa-tients fulfilled the criterion of monosymptomatic enuresis,defined as absent daytime incontinence at the time of thestudy. However, we stress that this classic ICCS definitiondoes not exclude any evidence of underlying bladder dys-function, as documented by frequency, urgency, a history ofdaytime wetting after age 5 years and small BC for age, asin patient group 3.
The volume of urine produced depends on the amount ofsolute and water ingested or produced by metabolism inexcess of needs and the ability to concentrate or diluteurine.13 Polyuria can result from a primary increase in glo-merular filtration and/or a primary decrease in reabsorptionat different tubular sites, that is the proximal tubules or loopof Henle (solute diuresis), the distal nephrons and/or thecollecting ducts (water diuresis).14
TABLE 2. Uosm during day and night
Mean Uosm � SD (mOsm/kg)
Controls Group 1 Group 2 Group 3
No. pts 100 12 9 21D1 735 � 118 995 � 74* 813 � 31 974 � 32*D2 722 � 124 1050 � 55* 860 � 34 1000 � 33*D3 710 � 123 998 � 51* 890 � 36 1032 � 37*D4 753 � 139 1006 � 67 1058 � 37* 1038 � 38N1 985 � 117 1019 � 69 1069 � 42 1049 � 41N2 975 � 89 1039 � 62 1050 � 34 1051 � 31N3 962 � 79 1015 � 44 1042 � 36 1085 � 25N4 940 � 41 1009 � 43 1000 � 34 1056 � 23*
* p �0.05.
TABLE 3. Diuresis rate during day and night
Mean Urine Flow � SD (ml/kg/hr)
Controls Group 1 Group 2 Group 3
No. pts 100 12 9 21D1 1.98 � 0.20 1.86 � 0.21 1.63 � 0.24 0.97 � 0.22*D2 2.01 � 0.28 2.12 � 0.34 1.68 � 0.32 1.19 � 0.18*D3 1.95 � 0.24 2.10 � 0.37 1.60 � 0.31 1.07 � 0.17*D4 1.87 � 0.23 2.00 � 0.25 2.00 � 0.36 1.34 � 0.13*N1 0.82 � 0.07 1.32 � 0.24* 1.48 � 0.27* 1.09 � 0.15*N2 0.68 � 0.06 1.03 � 0.12* 0.98 � 0.12* 0.95 � 0.17*N3 0.62 � 0.06 0.83 � 0.09* 0.74 � 0.08* 0.77 � 0.12*N4 0.56 � 0.04 0.71 � 0.06* 0.63 � 0.06 0.57 � 0.09
Daytime D1 to D4 and nighttime N1 to N4 collections plottedagainst reference frame of mean control population values � 1 SD(black lines). Patients with enuresis were divided into group 1 (filledcircles) with overall increased osmotic-excretion and polyuria dur-ing day and night, group 2 (open circles) with increased Eosm andpolyuria in D4 late evening and night collections, and group 3(inverted triangles) with increased Eosm and polyuria during nightcollections, apparently associated with low diurnal diuresis rate. A,
* p �0.05.

DESMOPRESSIN RESISTANT NOCTURNAL POLYURIA752
NP seems to correlate with increased salt excretion fromthe renal tubuli. Moreover, increased calcium excretion dur-ing the night has frequently been associated with NP.15 Paceet al suggested that NE can be caused by absorptive hyper-calciuria and it can be treated with a combination of diet(low sodium and low calcium) and DDAVP.16 They sug-gested that DDAVP may also favor urinary calcium resorp-tion, although the opposite was reported by Müller et al.17
This hypercalciuria may be a consequence of hypernatriuriasince urinary calcium excretion increases together with ex-cessive urinary sodium output in patients ingesting exces-sive sodium. Thus, to our knowledge it remains to be eluci-dated if the DDAVP response subsequent to dietarymodifications was purely related to correcting hypercalci-uria or rather by associated changes in the renal osmoticand sodium load.
First morning urine specific gravity greater than 1.010 orUosm greater than 400 mOsm/kg is found in children withsolute diuresis or in normal children, whereas urine specificgravity less than 1.005 or urine osmolality less than 200mOsm/kg indicates water diuresis.13,18 Although these val-ues might still be applicable in Eastern populations, in theWestern world overnight Uosm is apparently higher thanthe references of a few decades ago, probably because ofchanges in dietary habits. Solute diuresis causing polyuriais due to solute excretion greater than the usual excretoryrate19 and it may be caused by electrolytes or other osmoticagents. The most common nonelectrolyte solute diuresis iscaused by glucose in diabetes mellitus. Excessive urea ex-cretion is an important primary or contributing cause ofpolyuria, eg following high protein feeds. Protein and so-dium consumption is important for maximal Uosm in in-fants and possibly also in older children. A high proteinintake increases the urea content of the papillae and anenhanced amount of water is extracted from the collectingducts under the influence of antidiuretic hormone.20 There-fore, a difference in Uosm can be expected depending on thefeeding pattern of the child.
In an individual the dietary solute is influenced by cul-ture, ethnicity and habit. Therefore, daily urinary soluteexcretion varies considerably (500 to 1,000 mOsm) inhealthy adults18 and children. Every intervention, even doc-umenting nutrition, may influence fluid and nutritional in-take. We tried to avoid this bias to a maximum by notimplementing a standardized nutritional regimen.
Group 1 consisted of 12 children with significantly in-creased 24-hour Eosm. Uosm was constantly greater than1,000 mOsm/l and there was a high diuresis volume duringthe day (D1 to 3 and D4) and night (N1 to N4) (parts A andB of figure). This constantly increased Uosm reflected highrenal Eosm, most likely secondary to a high protein andsodium intake. Of these 12 patients 11 had a body massindex of greater than 90 centile, indicating obesity, correlat-ing with a high calorie and osmotic intake.
In comparison with the findings in group 1, the signifi-cantly higher evening and overnight Eosm, and diuresis ingroup 2 suggest a high osmotic load of protein, sodium, etcduring the evening meal shortly before bedtime (parts A andC of figure). In contrast to historical feeding habits, when themain meal with the highest solute load was served at lunch,most contemporary families have the main meal often quite
late in the evening.Increased daytime and nighttime Uosm (greater than 850mOsm/l) in association with decreased 24-hour diuresis andlow MBC in group 3 could probably be explained by deficientEosm during the day secondary to extremely low fluid intaketo compensate for the small BC because overall 24-hourEosm was within the normal range (part B of figure).
CONCLUSIONS
NP secondary to subnormal AVP excretion is a well recog-nized cause of PNE. The majority of these patients werefound to have hypo-osmolar polyuria as a result of increasedfree water excretion. We describe 42 patients with NP whohad high nighttime Uosm. Although a relation to abnormalfluid and diet habits is logical, eg daytime fluid restriction,and high protein and salt intake, further studies must doc-ument it. This polyuria secondary to osmotic diuresis wasfound to be DDAVP resistant. Because normalization of thisosmotic diuresis is necessary to achieve a DDAVP response,we advise correcting fluid and food intake in children beforestarting DDAVP treatment.
Abbreviations and Acronyms
AVP � arginine vasopressinBC � bladder capacity
D1 to D4 � daytime urine collections 1 to 4,respectively
DDAVP � desmopressinEBC � expected BC
Eosm � osmotic excretionICCS � International Children’s Continence
SocietyMBC � maximal BCMNE � monosymptomatic NE
N1 to N4 � nighttime urine collections 1 to 4,respectively
NE � nocturnal enuresisNP � nocturnal polyuria
PNE � primary NEUosm � urine osmolalityUvol � urine volume
REFERENCES
1. Hjalmas, K., Arnold, T., Bower, W., Caione, P., Chiozza, L.M.and von Gontard, A.: Nocturnal enuresis: an internationalevidence based management strategy. J Urol, 171: 2545,2004
2. Yeung, C. K.: Nocturnal enuresis (bedwetting). Curr OpinUrol, 13: 337, 2003
3. Nørgaard, J. P., Pedersen, E. B. and Djurhuus, J. C.: Diurnalanti-diuretic-hormone levels in enuretics. J Urol, 134: 129,1985
4. Rittig, C., Knutdsen, U. B., Nørgaard, J. P., Pedersen, E. B.and Djurhuus, J. C.: Abnormal diurnal rhythm of plasmavasopressin and urinary output in patients with enuresis.Am J Physiol, 256: 664, 1989
5. Vande Walle, J., Hoebeke, P., Van Laecke, E., Castillo, D.,Milicic, C. and Marraina, C.: Persistent enuresis caused bynocturnal polyuria is a maturation defect in the nycthem-eral rhythm of diuresis. BJU Int, 81S3: 40, 1998
6. Moffatt, M. E., Harlos, S., Kirshen, A. J. and Burd, L.: Desmo-pressin acetate and nocturnal enuresis: how much do we
know? Pediatrics, 92: 420, 1993
DESMOPRESSIN RESISTANT NOCTURNAL POLYURIA 753
7. Koff, S. A.: Estimating bladder capacity in children. Urology,21: 248, 1983
8. Kamperis, K., Hansen, M. N., Hagstroem, S., Hvistendahl, G.,Djurhuus, J. C. and Rittig, S.: The circadian rhythm ofurine production, and urinary vasopressin and prostaglan-din E2 excretion in healthy children. J Urol, 171: 2571,2004
9. Mattsson, S. and Lindstrom, S.: Diuresis and voiding patternin healthy schoolchildren. Br J Urol, 76: 783, 1995
10. Rittig, S., Matthiesen, T. B., Pedersen, E. B. and Djurhuus,J. C.: Sodium regulating hormones in enuresis. ScandJ Urol Nephrol Suppl, 202: 45, 1999
11. Hunsballe, J. M., Hansen, T. K., Rittig, S., Pedersen, E. B. andDjurhuus, J. C.: The efficacy of DDAVP is related to thecircadian rhythm of urine output in patients with persist-ing nocturnal enuresis. Clin Endocrinol (Oxf), 49: 703, 1998
12. Hansen, M., Rittig, S., Siggaard, C., Kamperis, K., Hvisten-dahl, G. and Schaumburg, H.: Intra-individual variabilityin nighttime urine production and functional bladder ca-pacity estimated by home recordings in patients with noc-
turnal enuresis. J Urol, 166: 2452, 200113. Leung, A. K., Robson, W. and Halperin, M. L.: Polyuria inchildhood. Clin Pediatr, 30: 634, 1991
14. Bichet, D. G.: Hereditary nephrogenic diabetes insipidus. AdvNephrol, 20: 175, 1991
15. Aceto, G., Penza, R., Coccioli, M. S., Palumbo, F., Cresta, L.and Chiozza, M. L.: Enuresis subtypes based on nocturnalhypercalciuria: a multicenter study. J Urol, 17: 1670, 2003
16. Pace, G., Aceto, G., Cormio, L., Traficante, A., Tempesta, A.and Lospalluti, M.: Nocturnal enuresis can be caused byabsorptive hypercalciuria. Scan J Urol Nephrol, 33: 111,1999
17. Müller, D., Kuehnle, K. and Eggert, P.: Increased urinarycalcium excretion in enuretic children treated with desmo-pressin. J Urol, 171: 2618, 2004
18. Oster, J. R., Singer, I. and Thatte, L.: The polyuria of solutediuresis. Arch Intern Med, 157: 721, 1997
19. Gennari, F. J. and Kassirer, J. P.: Osmotic diuresis. N EnglJ Med, 3: 714, 1974
20. Mårild, S., Jodal, U. and Jonasson, G.: Reference values forrenal concentrating capacity in children by the desmopres-
sin test. Pediatr Nephrol, 6: 254, 1992![Medical Treatment of Nocturia in Men with Lower …...balance [2], leading to excessive production of urine at all times (global polyuria) or primarily at night (nocturnal polyuria),](https://img.dokumen.tips/doc/110x75/5fa935277a549e105b2545fb/medical-treatment-of-nocturia-in-men-with-lower-balance-2-leading-to-excessive.jpg)
![0.1公絲 020826 MINIRIN Tablets 0.1 mg 迷你寧錠0.2公絲 ......[成分] 0.1 mg每錠含desmopressin acetate 0.1 mg ,相當於desmopressin (free base) 0.089 mg。 0.2 mg每錠含desmopressin](https://img.dokumen.tips/doc/110x75/5f4a71a5f323cb0eaf20a5c8/01c-020826-minirin-tablets-01-mg-eeoe02c-01.jpg)