Embed Size (px)
Citation preview
Degenerative brain diseases

* Include:
1. Multiple sclerosis.2. Alzheimer disease.3. Parkinsonism.

1. Multiple sclerosis
• Demyelinating diseases of the CNS are acquired conditions characterized by preferential damage to myelin, with relative preservation of axons.
• The clinical deficits are due to the effect of myelin loss on the transmission of electrical impulses along axons.

• Multiple sclerosis (MS) is an autoimmune demyelinating disorder characterized by distinct episodes of neurologic deficits.
• It is the most common of the demyelinating disorders.
• The disease becomes clinically apparent at any age, although onset in childhood or after age 50 years is relatively rare.
• Women are affected twice as often as are men.
• In most patients with MS, the clinical course of the illness evolves as relapsing and remitting episodes of neurologic deficit followed by gradual, partial recovery of neurologic function.
• The frequency of relapses tends to decrease during the course of time, but there is a steady neurologic deterioration in most patients.

* Pathogenesis:• The lesions of MS are caused by a cellular
immune response that is directed against the components of the myelin sheath. The likelihood of developing this autoimmune process is influenced by genetic and environmental factors (microbial triggers).

• The disease is initiated by CD4+ TH1 T cells that react against self myelin antigens and secrete cytokines, such as IFN-γ, that activate macrophages.
• The demyelination is caused by these activated macrophages and their injurious products.
• Oligodendroglia are not primarily affected and may even multiply to remyelinate the periphery of the lesion the first time.
• Although with time oligodendroglia and remyelination decreases and astrocytes proliferate to form glial "scar" tissue.
* Morphology: • The lesions appear as multiple, well-
circumscribed, somewhat depressed, glassy, gray-tan, irregularly shaped plaques, both on external examination and on section.
• In the fresh state, these have firmer consistency than the surrounding white matter (sclerosis).
• The size of lesions varies considerably, from small foci that are recognizable only at microscopic examination to confluent plaques.

Seen here in white matter is a large "plaque" of demyelination. The plaque has a grey-tan appearance.
Such plaques are typical for multiple sclerosis (MS) .


MRI
• Plaques commonly occur beside the lateral ventricles and may be demonstrated to follow the course of paraventricular veins.
• They are also frequent in the optic nerves and chiasm, brain stem ascending and descending fiber tracts, cerebellum, and spinal cord.

Luxol fast stain (blue) for myleinated fibers. Note demylinated patches (green arrows).
• In an active plaques, there is evidence of ongoing myelin breakdown with abundant macrophages containing lipid-rich, PAS-positive debris. Inflammatory cells, including both lymphocytes and monocytes, are present, mostly as perivascular cuffs.
• In quiescent plaques, there is a diminution of the inflammatory cell infiltrate and of macrophages. Little to no myelin is found and there is a reduction in the number of oligodendrocyte nuclei; instead, astrocytic proliferation and gliosis are prominent.
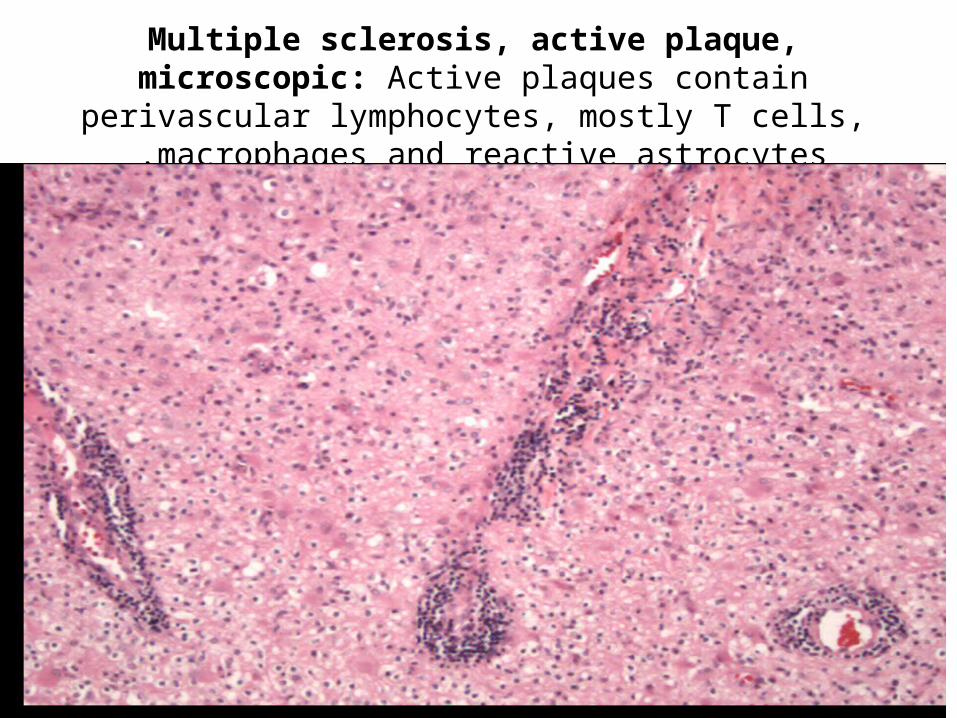
Multiple sclerosis, active plaque, microscopic: Active plaques contain perivascular lymphocytes, mostly T cells, macrophages
and reactive astrocytes .


There is a decrease in oligodendroglial nuclei and an increase of astrocyte nuclei characteristic of an older MS plaque .

* Clinical Features:• Unilateral visual impairment during the course
of a few days, due to involvement of the optic nerve (optic neuritis) is a frequent initial manifestation of MS.
• Involvement of the brainstem produces cranial nerve signs, ataxia, nystagmus, and ophthalmoplegia.

• Spinal cord lesions give rise to motor and sensory impairment of trunk and limbs, spasticity, and difficulties with the voluntary control of bladder function.
2. Alzheimer disease
• Alzheimer disease (AD) is the most common cause of dementia in the elderly.
• The disease usually becomes clinically apparent as insidious impairment of intellectual function, with alterations in mood and behavior. Later, progressive disorientation, memory loss, and aphasia indicate severe cortical dysfunction, and eventually, in 5 to 10 years, the patient becomes profoundly disabled, mute, and immobile.
• Patients are symptomatic after the age of 50 years. • Most cases are sporadic, although at least 5% to 10%
of cases are familial.

* Pathogenesis of AD:
• Current understanding of the principal events in the pathogenesis of AD is centered on the properties of Aβ (amyloid beta protein). This peptide aggregates, is relatively resistant to degradation and can be directly neurotoxic.

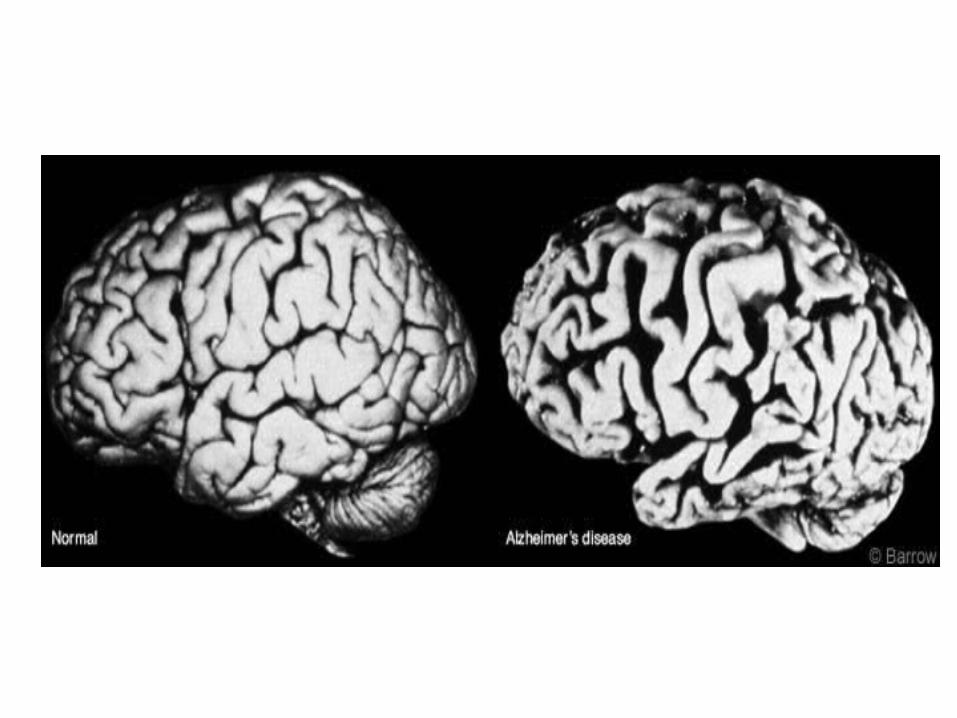
* Gross features: • Variable degree of cortical atrophy with
widening of the cerebral sulci that is most pronounced in the frontal, temporal, and parietal lobes.
• With significant atrophy, there is compensatory ventricular dilatation (hydrocephalus ex vacuo) secondary to loss of parenchyma.
* Microscopic features:• The major microscopic abnormalities of
Alzheimer disease are; 1. Neuritic (senile) plaques:2. Neurofibrillary tangles.3. Amyloid angiopathy.
• Neuritic plaques are focal, spherical collections of dilated, tortuous, silver-staining neuritic processes (dystrophic neurites) often around a central amyloid core. Microglial cells and reactive astrocytes are present at their periphery.
• Plaques can be found in the hippocampus and amygdala as well as in the neocortex.


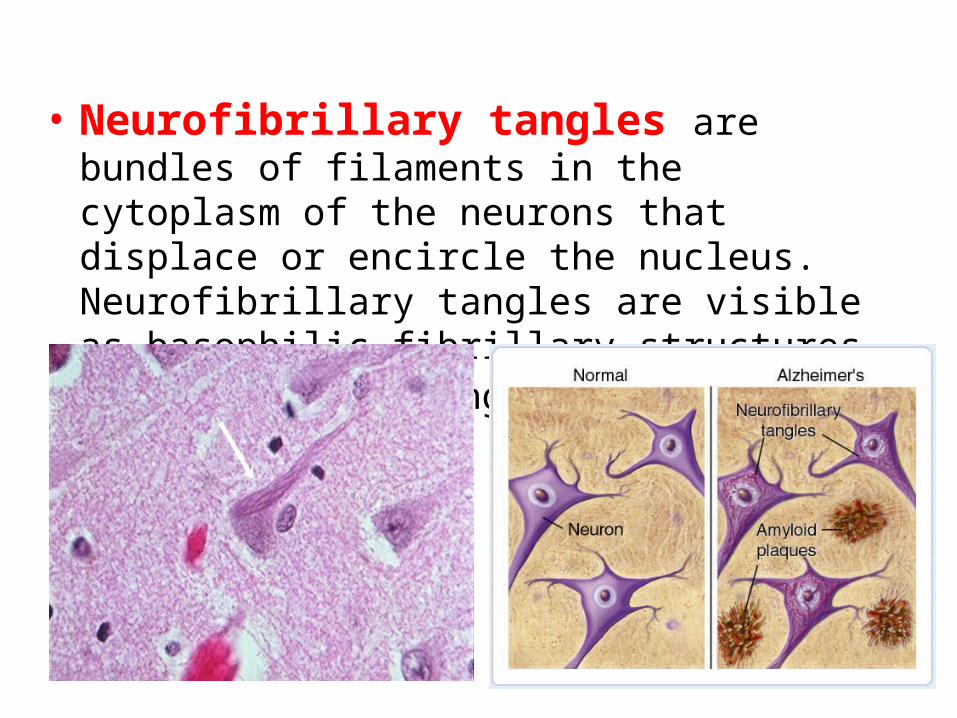
• Neurofibrillary tangles are bundles of filaments in the cytoplasm of the neurons that displace or encircle the nucleus. Neurofibrillary tangles are visible as basophilic fibrillary structures with H & E staining.
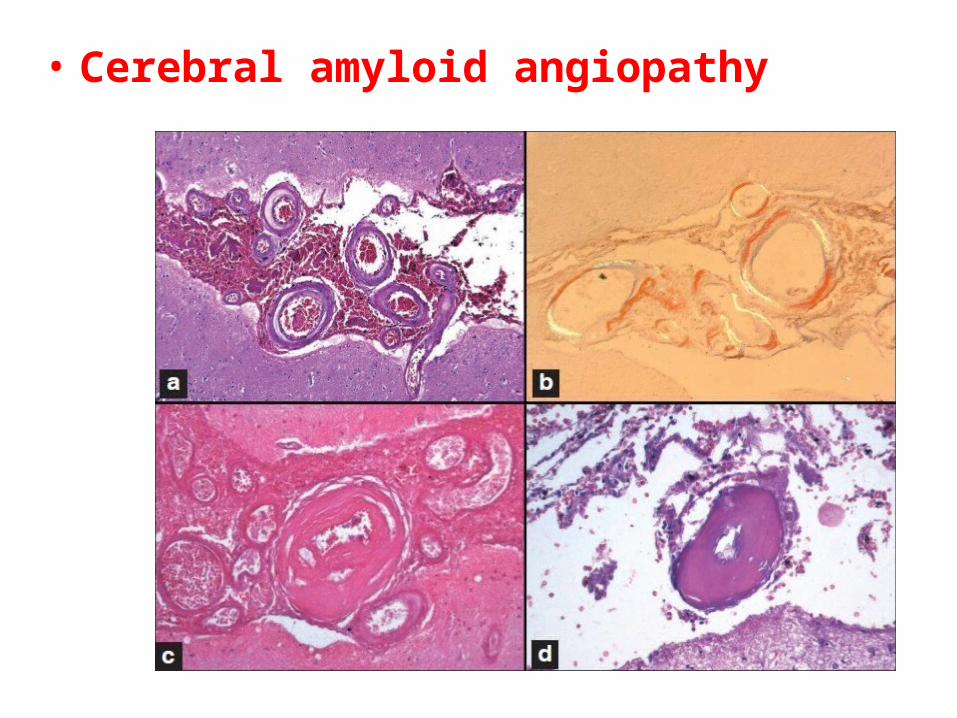
• Cerebral amyloid angiopathy
3. Parkinsonism

• is a degenerative disorder of the central nervous system. The motor symptoms of Parkinson's disease result from the death of dopamine-generating cells in the substantia nigra, a region of the midbrain; the cause of this cell death is unknown.
• Early in the course of the disease, the most obvious symptoms are movement-related; these include shaking, rigidity, slowness of movement and difficulty with walking and gait.

• Later, cognitive and behavioural problems may arise, with dementia commonly occurring in the advanced stages of the disease. Other symptoms include sensory, sleep and emotional problems.
• PD is more common in the elderly, with most cases occurring after the age of 50.

* Pathogenesis: • An abnormal accumulation of the protein
alpha-synuclein in the damaged cells. This insoluble protein accumulates inside neurones forming inclusions called Lewy bodies.

* Morphology:• On pathologic examination, the typical
macroscopic findings are pallor of the substantia nigra.
• On microscopic examination, there is loss of the pigmented neurons in the affected regions associated with gliosis.
• Lewy bodies may be found in some of the remaining neurons. These are single or multiple, cytoplasmic, eosinophilic, round to elongated inclusions.
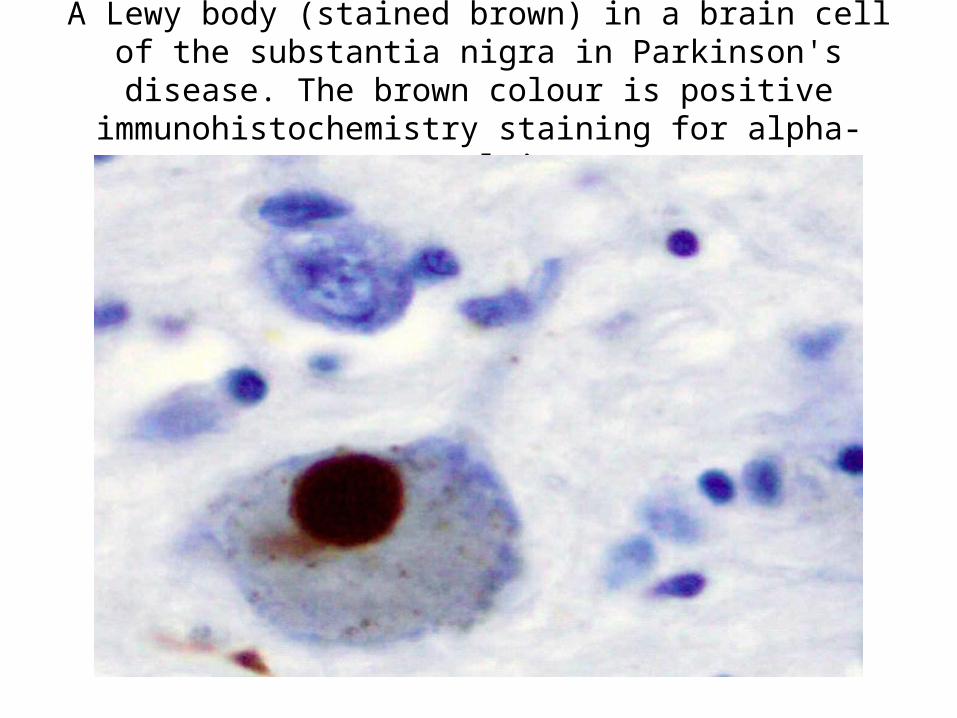
A Lewy body (stained brown) in a brain cell of the substantia nigra in Parkinson's disease. The brown colour is positive
immunohistochemistry staining for alpha-synuclein.

* Treatment:• There is no cure for Parkinson's disease, but
medications, surgery and multidisciplinary management can provide relief from the symptoms. The main families of drugs useful for treating motor symptoms are levodopa and dopamine agonists.

Thanks








![Evaluation of Brain Atrophy Estimation Algorithms using ...1. Introduction Brain atrophy is a common feature of many neuro-degenerative diseases such as Multiple Sclerosis (MS)[1]](https://img.dokumen.tips/doc/110x75/60366758719d65527f1d649e/evaluation-of-brain-atrophy-estimation-algorithms-using-1-introduction-brain.jpg)




















