Embed Size (px)
Citation preview

For debate
Br. J. Surg. 1988, Vol. 75, September, 901 -903 Definitive radiation therapy for
selected cancers of the rectum
B. Sischy, E. J. Hinson and D. R. Wilkinson
The Daisy Marquis Jones Radiation Oncology Center, Highland Hospital, 7 000 South Avenue, Rochester. New York 7 4620, USA Correspondence to: Dr B. Sischy
During the last 15 years, over 400 patients with adenocarcinoma of the rectum have undergone a course of endocavitary irradiation for cure or palliation of Dukes' A and B disease. This treatment method makes use of an unconventional fractionation scheme, by which the tumour receives 10 000-12 000 cGy in approximately four fractions over a period of about 60 days. The treatments are separated by an interval of 2 or 3 weeks. This method of definitive irradiation allows suitable patients to avoid abdominoperineal resection and its drawbacks. Hospitalization is avoided and the patients maintain a normal daily life. Approximately 15-20 per cent of all rectal cancer patients may be expected to fuljil the criteria for selection, which are sufficiently strict that the local control (95 per cent) and 5-year survival rates (94 per cent) can exceed those of surgery for comparable disease. Keywords: Endocavitary irradiation, rectum, neoplasm, radiation therapy, contact therapy
Sphincter-saving procedures have recently evoked great interest in the treatment of rectal cancer. A number of protocols is evolving in an attempt to identify optimal methods of local treatment. Following the pioneering work of Papillon' it has become apparent that endocavitary irradiation has a variety of advantages over other treatment methods for appropriate patients. An abdominoperineal resection with its associated colostomy and incidence of male impotence is avoided. The treatment is without any risk of mortality and has only minimal local morbidity. Patients are treated on an outpatient basis, they do not require general anaesthesia and can continue normal daily activities without loss of work time. Due to the nature and the quality of the X-ray beam used in this technique, perforation of the rectal wall does not occur and a high dose may be delivered to the tumour bed with minimal irradiation of the surrounding tissues. Patients may be followed without special facilities as sigmoidoscopy gives clear visualization of the rectal wall. Should a patient develop a second lesion in the rectum or a recurrence of the original lesion, radical surgery is not precluded. As the volume of tissue treated is minimal, surgical techniques and postoperative healing are not compromised.
This review examines our own results using this approach in patients with rectal cancer.
Patients and methods Selection of patients When offering patients local treatment as an alternative to radical excision, it is important to achieve results equal to those of traditional therapy. For this reason strict criteria must be applied to ensure patient suitability. At present it is estimated that approximately 15-20 per cent ofpatients with carcinoma of the rectum may be suitable for this method of treatmentz.
The lesion should be Dukes' A. According to Morson's review of surgical specimens3, lesions of this stage exhibit a probability of perirectal lymph node involvement of less than 10 per cent. The rectal mucosa must be examined by very careful digital palpation to exclude the presence of perirectal nodes.
~
From a paper delivered at the 50th Anniversary Conference of Megavoltage Radiotherapy at S t . Bartholomew's Hospital, London, September I987
Although digital examination by an experienced clinician may have an accuracy of over 80 per cent4 it is now possible to obtain more objective information regarding the extent of the lesion and the status of the perirectal lymph nodes pre-operatively by computed tomographic scanning, nuclear magnetic resonance imaging and transrectal ultra- sound5-*. Transrectal ultrasound appears able to provide optimal information in our own unpublished comparison of the three methods.
The lesion should be mobile as fixation indicates penetration through the muscularis into the serosa or perirectal fat. The diameter of the lesion should be no greater than 50cm. The treatment proctoscope allows a 2.9 cm target volume to be treated and lesions up to 5 cm may be treated by overlapping fields. The tumour must lie distal to the peritoneal reflection and must not encroach across the dentate line into the anal canal. The modified squamous epithelium of the anal canal is extremely senstive to high doses of irradiation and excessive morbidity would occur if this area were allowed to receive treatment by this technique and fractionation scheme.
Polypoid, exophytic and ulcerative lesions are all suitable for endocavitary irradiation provided the above criteria are fulfilled. It is important to review the histological differentiation of these tumours, and only well or moderately differentiated lesions should be accepted for this treatment. Poorly differentiated lesions are more likely to metastasize, both to perirectal nodes3 and to distant sites. It may be argued however that these higher grade lesions have such a poor prognosis, even when radical surgery is performed, that in special situations palliative endocavitary irradiation may be an excellent method of gaining local control.
Certain patients may be referred because they are medically inoperable or have refused an abdominoperineal resection. Some of these patients, who do not fit within the selection criteria for this treatment method, can be offered a course of therapy and are then placed into a separate palliative group. Many patients are d e h e d unsuitable and are not offered endocavitary irradiation because of advanced disease and some are rejected if technical difficulties prevent the adequate delivery of treatment.
Method Endocavitary irradiation is delivered on an outpatient basis. Patients have an enema before examination and treatment; dietary restrictions are unnecessary. Some patients require local anaesthesia which is administered by perianal block using 1 per cent lignocaine. The patient is positioned on a proctological tilt table. After digital and proctoscopic examinations, using specially designed applicators equipped with fibreoptics, treatment is delivered from a Philips (Philips, Eindhoven, The Netherlands) RT-50contact machine. The patient is able to resume normal activity immediately after therapy.
ooO7-1323/88/090901-03$3.00 1 ' 1988 Butterworth & Co (Publishers) Ltd 901
Endocavitary irradiation for rectal cancer: B. Sischy et al.
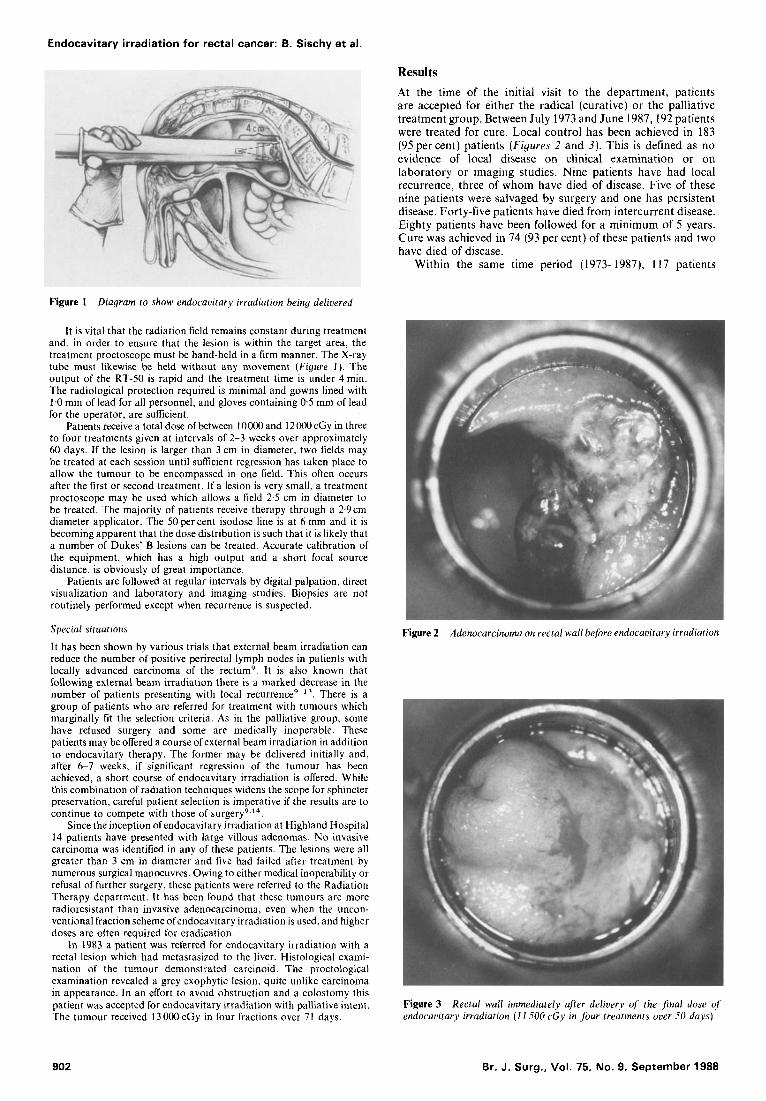
Results At the t ime of t h e initial visit t o t h e depar tment , pat ients are accepted for either t h e radical (curative) or t h e palliative t reatment group. Between July 1973 and June 1987,192 pat ients were t reated for cure. Local control has been achieved in 183 (95 per cent) pat ients (Figures 2 and 3). This is defined as no evidence of local disease on clinical examinat ion or on laboratory or imaging studies. Nine pat ients have had local recurrence, three of whom have died of disease. Five of these nine pat ients were salvaged by surgery and one has persistent disease. Forty-five pat ients have died from intercurrent disease. Eighty pat ients have been followed for a minimum of 5 years. C u r e was achieved in 74 (93 per cent) of these pat ients and t w o have died of disease.
Wi th in t h e same t ime period (1973-1987), 117 pat ients
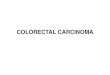
Figure 1 Diagram to show endocavitary irradiation being delivered
It is vital that the radiation field remains constant during treatment and, in order to ensure that the lesion is within the target area, the treatment proctoscope must be hand-held in a firm manner. The X-ray tube must likewise be held without any movement (Figure I ) . The output of the RT-50 is rapid and the treatment time is under 4 min. The radiological protection required is minimal and gowns lined with 1.0 mm of lead for all personnel, and gloves containing 0.5 mm of lead for the operator, are suflicient.
Patients receive a total dose of between 1OooO and 12000cGy in three to four treatments given at intervals of 2-3 weeks over approximately 60 days. If the lesion is larger than 3 cm in diameter, two fields may be treated at each session until sufficient regression has taken place to allow the tumour to be encompassed in one field. This often occurs after the first or second treatment. If a lesion is very small, a treatment proctoscope may be used which allows a field 2.5 cm in diameter to be treated. The majority of patients receive therapy through a 2.9cm diameter applicator. The 50 per cent isodose line is a t 6 mm and it is becoming apparent that the dose distribution is such that it is likely that a number of Dukes' B lesions can be treated. Accurate calibration of the equipment, which has a high output and a short focal source distance, is obviously of great importance.
Patients are followed at regular intervals by digital palpation, direct visualization and laboratory and imaging studies. Biopsies are not routinely performed except when recurrence is suspected.
Special situations
It has been shown by various trials that external beam irradiation can reduce the number of positive perirectal lymph nodes in patients with locally advanced carcinoma of the rectumg. It is also known that following external beam irradiation there is a marked decrease in the number of patients presenting with local r e c ~ r r e n c e ~ ~ ' ~ . There is a group of patients who are referred for treatment with tumours which marginally fit the selection criteria. As in the palliative group, some have refused surgery and some are medically inoperable. These patients may be offered a course of external beam irradiation in addition to endocavitary therapy. The former may be delivered initially and, after 6 7 weeks, if significant regression of the tumour has been achieved, a short course of endocavitary irradiation is offered. While this combination of radiation techniques widens the scope for sphincter preservation, careful patient selection is imperative if the results are to continue to compete with those of ~ u r g e r y ~ , ' ~ .
Since the inception of endocavitary irradiation at Highland Hospital 14 patients have presented with large villous adenomas. No invasive carcinoma was identified in any of these patients. The lesions were all greater than 3 cm in diameter and five had failed after treatment by numerous surgical manoeuvres. Owing to either medical inoperability or refusal of further surgery, these patients were referred to the Radiation Therapy department. It has been found that these tumours are more radioresistant than invasive adenocarcinoma, even when the uncon- ventional fraction scheme ofendocavitary irradiation is used, and higher doses are often required for eradication.
In 1983 a patient was referred for endocavitary irradiation with a rectal lesion which had metastasized to the liver. Histological exami- nation of the tumour demonstrated carcinoid. The proctological examination revealed a grey exophytic lesion, quite unlike carcinoma in appearance. In an effort to avoid obstruction and a colostomy this patient was accepted for endocavitary irradiation with palliative intent. The tumour received 13 000 cGy in four fractions over 71 days.
Figure 2 Adenocarcinoma on rectal wall before endocavitary irradiation
Figure 3 endocavitary irradiation ( 1 I 500 cGy in four treatments over 50 days)
Rectal wall immediately u fer delivery of the $rial dose of
902 Br. J. Surg., Vol. 75, No. 9, September 1988

Endocavitary irradiation for rectal cancer: B. Sischy et al.
to sigmoidoscopy. There is a tendency to view with suspicion the area of the rectal mucosa that has received treatment. In an effort to rule out local recurrence, post-treatment biopsies of mucosa with normal appearance are sometimes taken; subseqently a fibrotic nodule may be palpated, prompting further investigation which may include a second biopsy. At this time there appears to be a lack of understanding that tissue which has received high doses of irradiation heals by fibrosis and frequent biopsies may lead to unnecessary radical procedures, performed for suspected recurrence.
It has become apparent that the timedose relationship of endocavitary irradiation is very important. It is felt that the optimal schedule is approximately four treatments within 60 days, given at intervals of 2-3 weeks; if additional doses are required, they should be given over a proportionate time. Three of nine patients in the curative group who had local recurrence received therapy over what is now considered an excessive time period. All three patients came from outside the community and experienced travel difficulties for a variety of reasons.
For three-quarters of a century surgery has been the traditional accepted management for all stages of carcinoma of the rectum. Radiotherapy is now challenging the role of surgery in the treatment of early disease. It is interesting that this should be accomplished by the peculiar use of a low energy beam machine which has been available for many years, rather than by one of the more powerful machines that takes advantage of new technology. It is regrettable that this machine is no longer in production.
References
were assigned to the palliative group. In this group, 49 (42percent) patients appear to be cured in that they have not manifested recurrent disease to date; a further 51 patients (44 per cent) achieved significant palliation of symptoms; and 17 (14 per cent) patients received no discernible benefit from therapy.
Of the 14 patients who received treatment for villous adenomas, 4 have had local recurrence following endocavitary irradiation and were salvaged by a repeat course of therapy. Two of the four patients have died from other causes and two remain alive and well. Ten patients have required no further therapy.
The patient with a carcinoid tumour was observed carefully and after therapy moderate superficial necrosis was evident in the treatment area. Examination at 24 months revealed an increase in the size of liver metastases with the addition of mediastinal and bone involvement. He died of liver metastases 3.2 years after therapy; post-mortem examination revealed that the rectum was free of disease.
The mucosa of the rectum reacts remarkably well when subjected to the fractionation scheme used in endocavitary irradiation; following total doses as high as 17 500 cGy in six treatments over 100 days, sublethal damage is repaired. Over 400 patients have been thus treated at Highland Hospital and no serious local morbidity has been encountered although patients may experience minor bleeding or mucous discharge during the course of treatment. Of 403 patients 87 (22 per cent) have exhibited some superficial necrosis in the treatment area and healing has occurred after the use of steroid enemas. Long-term follow-up usually reveals an area of slight atrophy at the treatment site but otherwise the rectal wall is smooth and soft on palpation. Some patients demonstrate telangiectasia within the atrophic area and these patients may report minor bleeding following the ingestion of excessive roughage. A few patients have reported unusually persistent bleeding after treatment and it is interesting that on careful questioning a number of these patients admit to the use of routine aspirin for anticoagulation.
A number of patients are referred for endocavitary irradiation following unsuccessful attempts at local excision with or without fulguration. In some instances these procedures have been carried out on several occasions and the patient presents for endocavitary irradiation after more than one recurrence. The outcome of these patients after therapy is comparable to that of patients who have undergone a pretreatment biopsy, but the local reaction is considerably more pronounced. In the group of 192 patients treated for cure by endocavitary irradiation, 32 patients had undergone prior surgical procedures in addition to a biopsy. After treatment, excessive local reaction was demonstrated in 14 (44 per cent) of these patients. Superficial necrosis in the target area, although asymptomatic, may require protracted courses of steroid retention enemas before healing takes place. After surgical procedures the vasculature of the rectal mucosa is disturbed and tumour cells may be lodged in anoxic scar tissue, causing increased radioresistance.
Discussion The modified squamous epithelium of the anal canal responds to irradiation in a manner similar to that of normal skin. It is crucial therefore that patients in whom the rectal lesion encroaches into the anal canal are not treated in this way. Some patients have been treated where the inferior border of the lesion was 0.25 cm above the dentate line. A few months after therapy, proctitis developed which eventually responded to steroid retention enemas. If the anal canal is treated the possibility exists that a very severe proctitis would develop, necessitating an abdominoperineal resection for pain control. After endocavitary irradiation many patients are followed not only in the radiation therapy department but also by their surgeon and/or endoscopist. This allows optimal follow-up as patients are able to undergo regular colonoscopy in addition
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
Papillon J. Rectal and Anal Cancers-Conservative Treatment by Irradiatiori- An Alternative to Radical Surgery. New York: Springer-Verlag, 1982. Axtell LM, Cutler SJ, Myers MH. End results in cancer. 1972; Report No. 4 HEW Publication (NIH): 173-272. Morson BC. Factors influencing the progress of early cancer of the rectum. Proc R SOC Med 1966; 59: 607-8. Nicholls RJ. The clinical staging of rectal cancer. Br J Surg 1982; 69: 404-9. Beynon J, Roe AM. Foy DMA, Channer JL, Virjee J, Mortensen NJ McC. Preoperative staging of local invasion in rectal cancer using endoluminal ultrasound. J R SOC Med 1987; 80: 23-4. Thoeni RF, Moss AA, Schnyder P, Margulis AR. Detection and staging of primary rectal and rectosigmoid cancer by computed technology. Radiology 1981; 141: 135-8. Hodgeman CG, MacCarty RL, Wolff BG et al. Preoperative staging of rectal carcinoma by computed tomography and 0.1 ST magnetic resonance imaging. Preliminary report. Dis Colon Rectum 1986; 29: 446-SO. Butch RJ, Stark DD, Wittenburg J. Staging rectal cancer by MR and CT. AJR 1986; 146: 1155-60. Papillon J. The future of external beam irradiation as initial treatment of rectal cancer. Br J Surg 1987; 74: 449-54. Higgins Jr GA, Conn JH, Jordan Jr PHJ, Humphrey EW, Roswit B, Keehn RJ. Pre-operative radiotherapy for colorectal cancer. Ann Surg 1975; 181: 624-31. Withers HR, Romsdahl M, Barkley HT et 01. Post-op radiation therapy for rectal cancer. In: Salmon SE, Jones SE, eds. Adjuvant Therapy of Cancer 11. New York: Grune & Stratton Inc, 1979:
Pahlman L, Glimelius B, Graffman S . Pre- uersus postoperative radiotherapy in rectal carcinoma: an interim report from a randomized multicentre trial. Br J Surg 1985; 7 2 : 961-6. Boulis-Wassif S, Gerard A, Loygue J, Camelot D, Buyse M, Duez N. Final results of a randomized trial on the treatment of rectal cancer with pre-operative radiotherapy alone or in combination with 5-Fluorouracil, followed by radical surgery. Trial of the European Organization on Research and Treatment of Cancer. Gastrointestinal Tract Cancer Cooperative Group. Cancer 1984; 53: 1811-18. Myerson RJ, Walz BJ, Kodner IJ et al. Endocavitary radiation for early rectal carcinomas: the experience at Washington University. (Abstract) Int J Radiat Oncol B i d Phys 1987; 13 (Suppl. 1) : 194.
621-8.
Paper accepted I1 April 1988
Br. J. Surg., Vol. 75, No. 9, September 1988 903