Embed Size (px)
Citation preview

837
Defibrillation Efficacy and Pain Perception of Two BiphasicWaveforms for Internal Cardioversion of Atrial Fibrillation
JENS JUNG, M.D., STEPHANOS SIAPLAOURAS, M.D., AXEL BUOB, M.D.,BERND D. SCHUBERT, M.D.,* STEPHEN J. HAHN, PH.D.,† and ARMIN HEISEL, M.D.‡
From Medizinische Klinik und Poliklinik, Innere Medizin III, Universitatskliniken des Saarlandes Homburg/Saar, Homburg/Saar,Germany; *Guidant CPI Research, Brussels, Belgium; †Guidant Tachyarrhythmia Research, St. Paul, Minnesota, USA;
and ‡Medizinische Klinik I, Reinhard-Nieter-Krankenhaus, Wilhelmshaven, Germany
Efficacy and Pain Perception of Two Biphasic Waveforms. Introduction: We evaluated the influ-ence of the peak voltage of waveforms used for internal cardioversion of atrial fibrillation on defibrillationefficacy and pain perception. A low peak voltage biphasic waveform generated by a 500-µF capacitor with40% tilt was compared to a standard biphasic waveform generated by a 60-µF capacitor with 80% tilt.
Methods and Results: In 19 patients with paroxysmal atrial fibrillation (79% male, age 55 ± 11 years, 21%with heart disease), the atrial defibrillation threshold (ADFT) was determined during deep sedation withmidazolam for both waveforms in a randomized fashion using a step-up protocol. Internal cardioversionwith a single lead (shock vector: coronary sinus to right atrium) was successful in 18 (95%) of 19 patients.ADFT energy and peak voltage were significantly lower for the low-voltage waveform (2.1 ± 2.4 J vs 3.5 ±3.9 J, P < 0.01; 100 ± 53 V vs 290 ± 149 V, P < 0.01). Sedation then was reversed with flumazenil afterADFT testing. Two shocks at the ADFT (or a 3-J shock if ADFT>3 J) were administered to the patient usingeach waveform in random order. Pain perception was assessed using both a visual scale and a numericalscore. ADFTs were above the pain threshold in 17 (94%) of 18 patients, even though the ADFT with the500-µF waveform was <100 V in 63% of the patients. Pain perception was comparable for both waveforms(numerical score: 6.5 ± 2.4 vs 6.3 ± 2.6; visual scale: 5.4 ± 2.6 vs 5.2 ± 3.1; P = NS, 500-µF vs 60-µF).The second shock was perceived as more painful in 88% of the patients, independent of the waveform used.
Conclusion: Despite a 66% lower peak voltage and a 40% lower energy, the 40% tilt, 500-µF capacitorbiphasic waveform did not change the pain perceived by the patient during delivery of internal cardioversionshocks. Pain perception for internal cardioversion probably is not influenced by peak voltage alone andincreases with the number of applied shocks. (J Cardiovasc Electrophysiol, Vol. 14, pp. 837-840, August 2003)
internal cardioversion, shock waveform, atrial defibrillation threshold, peak voltage, pain perception
Introduction
Electrical cardioversion is an established and widely usedtechnique for restoration of sinus rhythm in patients withsymptomatic atrial fibrillation.1 Numerous clinical studieshave shown that internal cardioversion is a safe and effec-tive method to convert atrial fibrillation, using much lowerenergies and with greater efficacy than transthoracic car-dioversion.2-8 Internal cardioversion usually is associatedwith significant discomfort for the patient, even at small en-ergies that are well below the atrial defibrillation threshold(ADFT).2,9-12 Several studies have suggested that the discom-fort associated with internal cardioversion shocks appears tobe determined by the voltage rather than by the energy of theshock.9-11
Other studies of internal defibrillation in the ventricleshave shown that voltage can be dramatically reduced by usinglow tilt waveforms generated from large capacitances.13,14
Therefore, the aim of this study was to evaluate the influence
Supported by Guidant Corporation.
Address for correspondence: Jens Jung, M.D., Medizinische Klinik undPoliklinik, Innere Medizin III, Universitatskliniken des Saarlandes, 66421Homburg/Saar, Germany. Fax: 49-6841-1623394; E-mail: [email protected]
Manuscript received 16 December 2002; Accepted for publication 28 May2003.
of two biphasic waveforms, one with a low peak voltage gen-erated form a large 500-µF capacitance and a second standardbiphasic waveform generated from a 60-µF capacitance, onatrial defibrillation efficacy and on the perception of painduring internal cardioversion of atrial fibrillation.
Methods
Patients
Patients with a history of paroxysmal atrial fibrillation whodeveloped atrial fibrillation lasting>15 minutes during a clin-ically indicated electrophysiologic study were included. Theelectrophysiologic study was performed to investigate themechanism of the arrhythmia or to perform ablation proce-dures. All patients gave written informed consent to the studyprotocol, which was approved by the Ethics Committee onHuman Research.
Internal Atrial Defibrillation
For internal cardioversion, a 7-French dual-coil lead(ATAK, Vascomed, Lorrach, Germany) was introduced. Thecharacteristics of the lead have been described elsewhere.7
The distal coil served as cathode and was positioned in thecoronary sinus. The proximal coil served as the anode andwas located at the anterolateral aspect of the right atrium.Patients received 5,000 IU of heparin after catheter inser-tion. Determination of ADFT was performed with the patient

838 Journal of Cardiovascular Electrophysiology Vol. 14, No. 8, August 2003
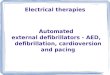
Figure 1. Voltage of the two biphasic waveforms (solid line: 60-µF capaci-tance; dashed line: 500-µF capacitance) when applying a 2-J shock againsta resistance of 50 �.
under deep sedation with midazolam. Shocks were deliveredby using two modified versions of an external cardioverterdefibrillator (ECD models R3 and R4, CPI-Guidant, St. Paul,MN, USA). These devices allowed delivery of a 60-µF, 80%tilt (model R3) or a 500-µF, 40% tilt (model R4) biphasicwaveform with a phase I/phase II ratio of 60/40. For equaldelivered energies, the 500-µF capacitor device had a 58%lower peak voltage than the 60-µF capacitor (Fig. 1). The 60-µF waveform was very similar to that available in the originalMetrix 3000 Implantable Atrial Defibrillator (80-µF wave-form) and to that used in previously reported studies.15,16
Atrial defibrillation efficacy of both waveforms was testedusing a step-up protocol (0.1, 0.3, 0.5, 0.8, 1, 1.5, 2, 2.5, 3, 4, 6,8, 10 J). Shocks were delivered 1 minute apart until an energywas reached that successfully terminated atrial fibrillation(defined as ADFT). All shocks were synchronized to the Rwave using a lead inserted in the apex of the right ventricle forappropriate sensing. ADFT was determined for both biphasicwaveforms in a random fashion. After termination with thefirst randomized waveform, atrial fibrillation was reinducedby atrial burst pacing, and the ADFT of the second waveformwas determined.
Pain Perception
After completion of the ADFT protocol, sedation was re-versed by flumazenil. Approximately 10 minutes after ad-ministration of flumazenil, the unsedated patients receivedtwo shocks, one of each waveform in randomized order andnot more than 3 minutes apart. Both shocks were deliveredduring normal sinus rhythm, with energy levels at the previ-ously determined ADFT for that waveform. If the ADFT was>3 J, the shock delivered for assessment of pain perceptionwas set at 3 J. All patients were asked to report their painperception after each shock, independently. For this assess-ment, a numerical score from 0 to 10 (0 = not felt, 10 =intolerable) and a visual scale from 0 to 10 (0 = not felt,10 = intolerable) were used. Each patient was allowed to ter-minate the protocol if the first shock was perceived as intoler-able. After both shocks had been delivered, each patient wasasked to indicate which shock was more uncomfortable. Thenext day, the potential for acceptance of therapeutic shocksby an implantable atrial defibrillator was analyzed using a
questionnaire. The patients received the questionnaire fromtheir attending physician, who was blinded to the order of theshock waveforms tested. Each patient was asked how oftenthey would accept the first and the second shock. The frequen-cies of shock delivery addressed in the questionnaire were asfollows: one shock per day, one shock per week, one shockper 2 weeks, one shock per month, one shock per 6 months,one shock per year, or shock delivery was not accepted at all.
Statistical Analysis
All data are expressed as mean ± SD. Comparison ofcontinuous variables between groups was performed by Stu-dent’s t-test. For nonparametric analysis, the Wilcoxon signrank test was used. Discrete variables were compared us-ing Chi-square analysis or Fisher exact test. P < 0.05 wasconsidered statistically significant.
Results
Patients
Nineteen patients with drug-refractory paroxysmal atrialfibrillation entered the study. The characteristics of the studypopulation are given in Table 1. Antiarrhythmic drugs werediscontinued due to inefficacy in 14 patients. The remaining5 patients were taking antiarrhythmic drugs (amiodarone 3,sotalol 2) during the study.
Internal Atrial Defibrillation
Successful cardioversion was achieved in 18 (95%) of 19patients with both waveforms. In one patient, atrial fibrilla-tion was not terminated with a 20-J shock using the 500-µFcapacitor (ADFT was 8 J with the 60-µF capacitor). As ex-pected, peak voltage at the ADFT was much lower with the500-µF waveform versus the 60-µF waveform (100 ± 53 Vvs 290 ± 149 V, P < 0.01). The mean ADFT energy also wassignificantly lower for the 500-µF waveform (2.1 ± 2.4 J vs3.5 ± 3.9 J, P < 0.01, n = 18 patients). Pulse width of the500-µF waveform was significantly longer than that of the60-µF waveform (16.6 ± 1.2 msec vs 6.4 ± 0.4 msec, P <0.01). Low energy cardioversion (<3 J) was achievable in13 (72%) of 18 patients. The electrical parameters for these13 patients with ADFT <3 J are summarized in Table 2.
Pain Perception
In 17 (94%) of 18 patients, the threshold for pain per-ception was below the ADFT. One patient perceived no painwhen a 0.5-J shock (45 V) was applied using the 500-µFcapacitor or when a 1.0-J shock (175 V) was applied by the
TABLE 1
Clinical Parameters of the Study Population
n 19Men/women 15/4Age (years) 55 ± 11Structural heart disease 4Left atrial diameter (mm) 40 ± 2Left ventricular ejection fraction (%) 64 ± 3History of AF (years) 4.4 ± 3.1AF episodes per month 3.6 ± 4.2Ineffective antiarrhythmic drugs 2.2 ± 1.3
AF = atrial fibrillation.

Jung et al. Efficacy and Pain Perception of Two Biphasic Waveforms 839
TABLE 2
Electrical Parameters of Patients with Atrial Defibrillation Threshold LessThan 3 J
500 µF 60 µF P Value
Stored energy (J) 1.5 ± 0.8 1.5 ± 0.7 NSDelivered energy (J) 0.9 ± 0.5 1.5 ± 0.6 <0.01Voltage (V) 73 ± 20 211 ± 48 <0.0001Current (A) 1.2 ± 0.4 3.6 ± 0.9 <0.0001Impedance (�) 66 ± 7 61 ± 5 <0.001Duration (msec) 16.9 ± 1.3 6.6 ± 0.4 <0.0001
n = 13.
60-µF capacitor. Pain perception testing was not completedin one patient who felt intolerable pain after application of afirst shock with an energy of 0.5 J (55 V) generated by the500-µF capacitor. The amount of discomfort as assessed byeither the numerical score or the visual scale was not influ-enced by the type of waveform used (Table 3). A low-voltageshock (500-µF capacitor) was applied as first shock in 8 pa-tients. The standard voltage waveform (60-µF capacitor) wasthe first shock waveform used in 10 patients. In 15 (88%) of17 patients, the second shock was perceived as more painfulthan the first (P < 0.05). Only 2 patients perceived the firstshock, delivered by the 500-µF capacitor, as more painfulthan the second shock.
There were no statistically significant differences in thepatient’s responses to questions about the future acceptanceof either shock waveform if the patient were provided withan implanted atrial defibrillator (Table 4).
Discussion
Major Findings
To improve the clinical acceptance of internal atrial de-fibrillation by an implantable device, a significant reductionin the discomfort associated with shock delivery is needed.Whereas some clinical studies2,8,17 have suggested that thetolerability of atrial shocks is related to the applied energy,other investigators hypothesized that the leading-edge volt-age might be the primary factor responsible for the perceptionof delivered shocks.9,10,11,18
The present study demonstrated that a 40% tilt biphasicwaveform generated by a 500-µF capacitor provided a 66%decrease in peak voltage at the ADFT compared to an 80%tilt biphasic waveform generated by a 60-µF capacitor. Themean ADFT energy was significantly lower for the 500-µFwaveform but still was above the threshold for pain percep-
TABLE 3
Pain Perception at ADFT Less Than 3 J or at 3 J for Patients with ADFTGreater Than 3 J
500 µF 60 µF P Value
Delivered energy (J) 1.7 ± 1.1 2.0 ± 0.9 <0.05Voltage (V) 97 ± 35 252 ± 64 <0.0001Numerical score 6.5 ± 2.4 6.3 ± 2.6 NSVisual scale 5.4 ± 2.6 5.2 ± 3.1 NSMore discomfort (no. patients) 11 6 NS
n = 18.ADFT = atrial defibrillation threshold.
TABLE 4
Estimated Acceptance of Therapeutic Shocks If Patient Were Providedwith an Implantable Device
500 µF 60 µF
1 shock/day 4 71 shock/week 6 31 shock/2 weeks 2 11 shock/month 5 21 shock/6 months 0 21 shock/year 0 1No shock at all 1 2
n = 18.
tion in 94% of the patients studied. Low-energy internal car-dioversion using a biphasic waveform with a 66% lower peakvoltage was not associated with a reduction of pain percep-tion compared to the use of a biphasic waveform similar tostandard waveforms reported previously.9-11
Prior Studies
The effect of symmetric biphasic waveforms generated bydifferent capacitances on pain perception during atrial defib-rillation was studied by Tomassoni et al.10 in 10 patients withparoxysmal atrial fibrillation. They found that 1.5-J bipha-sic shocks with a 50-µF capacitance were perceived as morepainful than 1.5-J shocks with a 120-µF capacitance, de-spite a significant reduction of energy requirements for suc-cessful atrial cardioversion when using the 50-µF capaci-tor. Leading-edge voltage was 21% lower with the 120-µFcapacitor compared to the 50-µF capacitance.
In a series of 19 patients with persistent atrial fibrilla-tion, Boriani et al.9 reported a significant reduction in theleading-edge voltage and a significant reduction in painperception with an asymmetric biphasic waveform (phaseduration 6.5/2.5 msec) compared to a symmetric biphasicwaveform (phase duration 3.0/3.0 msec).9 Delivered energyfor successful atrial defibrillation was comparable for bothwaveforms.9
Ammer et al.11 compared two symmetric biphasic wave-forms in 31 patients with persistent atrial fibrillation. The au-thors reported that leading-edge voltage and pain perceptionwere lower with a biphasic shock of longer duration (phaseduration 6/6 msec) compared to a waveform with shorterduration (phase duration 3/3 msec) at comparable energyrequirements.
In contrast to the studies mentioned, we investigated twoasymmetric biphasic waveforms with dramatically differentcapacitances and found that a significant reduction in en-ergy requirements and a much lower leading-edge voltagewere not associated with an improvement in the perceptionor acceptance of internal shocks. This might be explained bythe different characteristics of the waveforms used, differ-ences in patient populations, or different protocols used forassessment of pain perception.
Pain perception appeared to increase with the number ofapplied shocks; the second shock applied was more uncom-fortable to the majority of our patients (88%). This findingis in agreement with a previous study in which we assessedthe tolerability of low-energy shocks in 10 patients providedwith an implantable cardioverter defibrillator for malignantventricular arrhythmias.12 Randomized delivery of 1-J and

840 Journal of Cardiovascular Electrophysiology Vol. 14, No. 8, August 2003
2-J shocks resulted in comparable scores for pain percep-tion, but the second shock was perceived as more painfulthan the first in all patients, independent of the energy leveldelivered first.12 Similar results have been reported by otherinvestigators.19
Study Limitations
The assessment of pain perception was performed afterreversal of sedation with flumazenil, which might have in-fluenced the patient’s perception of delivered shocks. Shockswere delivered during sinus rhythm and not during a symp-tomatic episode of atrial fibrillation. Whether the relief ofsymptoms associated with restoration of sinus rhythm in-fluences an individual’s perception of the shock, or theiracceptance of future shock therapy, could not be determinedby our study. Therefore, the shock acceptance data may beof limited value.
Clinical Implications
Although some studies have suggested that voltage playsa more critical role than energy in determining a patient’sperception of an internal cardioversion shock, the presentstudy was not able to demonstrate any difference in percep-tion, despite testing a waveform with a 66% lower voltage.Furthermore, the 500-µF waveform yielded an ADFT withvoltages <100 V in 63% of patients but did not appear toreduce pain. Thus, the pain perception threshold probablyis well below 100 V (probably <50 V) and, therefore, notachievable with the types of waveforms and leads systemsknown in the field today. A much more significant scientificbreakthrough is needed if pain perception is to be reduced oreliminated.
On a positive note, the estimated acceptance of therapeuticshocks if the patients were to be provided with an atrial de-fibrillator was relatively high. The majority of patients (94%if delivered by a 500-µF capacitor and 72% if delivered bythe 60-µF capacitor) would accept at least one therapeuticshock per month. Therefore, in clinical use, one should con-sider setting the first shock at an energy expected to give ahigh probability of success. This should help to prevent mul-tiple shock delivery, which appears to be perceived as morepainful than single shock delivery.
Conclusion
A 40% tilt biphasic waveform generated by a 500-µF ca-pacitor provided a decrease in energy and peak voltage at theADFT compared to a 60-µF, 80% tilt biphasic waveform.Pain perception for low-energy internal cardioversion cannotbe reduced by using a 500-µF, 40% tilt biphasic shock with66% lower peak voltage compared to a 60-µF, 80% tilt bipha-sic waveform. Pain perception probably is not influenced bypeak voltage alone and increases with the number of appliedshocks.
Acknowledgments: The authors thank Karsten Wittke and Ulrich Michel fortechnical support during the study.
References
1. Lown B, Amarasingham R, Neuman J: New method for terminatingcardiac arrhythmias: Use of synchronized capacitor discharge. JAMA1962;182:548-555.
2. Murgatroyd FD, Slade AKB, Sopher SM, Rowland E, Ward DE, CammAJ: Efficacy and tolerability of transvenous low energy cardiover-sion of paroxysmal atrial fibrillation in humans. J Am Coll Cardiol1995;25:1347-1353.
3. Schmitt C, Alt W, Plewan A, Ammer R, Leibig M, Karch M, Schomig A:Low energy intracardiac cardioversion after failed conventional exter-nal cardioversion of atrial fibrillation. J Am Coll Cardiol 1996;28:994-999.
4. Sopher SM, Murgatroyd FD, Slade AKD, Blankoff I, Rowland E, WardDE, Camm AJ: Low energy internal cardioversion of atrial fibrillationresistant to transthoracic shocks. Heart 1996;75:635-638.
5. Cooper RAS, Johnson EE, Kanter RJ, Merrill JJ, Sorentino RA,Wharton JM: Internal cardioversion in two patients with atrial fibril-lation refractory to external cardioversion. PACE 1996;19:872-875.
6. Alt E, Ammer R, Schmitt C, Evans F, Lehmann G, Pasquantonio J,Schomig A: A comparison of treatment of atrial fibrillation with low-energy intracardiac cardioversion and conventional external cardiover-sion. Eur Heart J 1997;18:1796-1804.
7. Heisel A, Jung J, Neuzner J, Michel U, Pitschner HF: Low-energytransvenous cardioversion of atrial fibrillation using a single atrial leadsystem. J Cardiovasc Electrophysiol 1997;8:607-614.
8. Levy S, Ricard P, Gueunoun M, Yapo F, Trigano J, Mansouri C,Paganelli F: Low-energy cardioversion of spontaneous atrial fibrilla-tion. Immediate and long-term results. Circulation 1997;96:253-259.
9. Boriani G, Biffi M, Zannoli R, Branzi A, Magnani B: Transvenousinternal cardioversion for atrial fibrillation: A randomized study on de-fibrillation threshold and tolerability of asymmetrical compared withsymmetrical shocks. Int J Cardiol 1999;71:63-69.
10. Tomassoni G, Newby KH, Kearney MM, Brandon MJ, Barold H, NataleA: Testing different biphasic waveforms and capacitances: Effect onatrial defibrillation threshold and pain perception. J Am Coll Cardiol1996;28:695-699.
11. Ammer R, Alt E, Ayers G, Schmitt C, Pasquantonio J, Schmidt M, PutterK, Schomig A: Pain threshold for low energy intracardiac cardioversionof atrial fibrillation with low or no sedation. Pacing Clin Electrophysiol1997;20:230-236.
12. Jung J, Heisel A, Fries R, Kollner V: Tolerability of internal low-energyshock strengths currently needed for endocardial atrial cardioversion.Am J Cardiol 1997;80:1489-1490.
13. Block M, Hammel D, Bocker D, Borggrefe M, Budde T, Isbruch F,Scheld HH, Breithardt G: Biphasic defibrillation using a single capacitorwith large capacitance: Reduction of peak voltages and ICD device size.Pacing Clin Electrophysiol 1996;19:207-214.
14. Brugada J, Herse B, Sandsted B, Michel U, Schubert BD, Hahn SJ:Clinical evaluation of defibrillation efficacy with a new single-capacitorbiphasic waveform in patients undergoing implantation of an im-plantable cardioverter defibrillator. Europace 2001;3:278-284.
15. Wellens HJJ, Lau CP, Luderitz B, Akhtar M, Waldo AL, Camm AJ,Timmermans C, Tse HF, Jung W, Jordaens L, Ayers G, for the MetrixInvestigators: Atrioverter, an implantable device for the treatment ofatrial fibrillation. Circulation 1998;98:1651-1656.
16. Daoud EG, Timmermans C, Fellows C, Hoyt R, Lemery R, Dawson K,Ayers GM, for the Metrix Investigators: Initial clinical experience withthe ambulatory use of an implantable atrial defibrillator for conversionof atrial fibrillation. Circulation 2000;102:1407-1413.
17. Keane D: Impact of pulse characteristics on atrial defibrillation energyrequirements. Pacing Clin Electrophysiol 1994;17:1048-1057.
18. Levy S, Ricard PH, Lau CP, Lok NS, Camm AJ, Murgatroyd FD,Jordaens LJ, Kappenberger LJ, Brugada P, Ripley KL: Multicenterlow energy transvenous atrial defibrillation (XAD) trial results in dif-ferent subsets of atrial defibrillation. J Am Coll Cardiol 1997;29:750-755.
19. Steinhaus DM, Cardinal DS, Mongeon L, Musley SK, Foley L,Corrrigan S: Internal defibrillation: Pain perception of low energyshocks. Pacing Clin Electrophysiol 2002;25:1090-1093.





![High-energy external defibrillation and transcutaneous ...quire external defibrillation or cardioversion [1]. The feasibility of in-bore defibrillation has been demon-strated in a](https://img.dokumen.tips/doc/110x75/60a040fa5ed69b1bff53b63d/high-energy-external-defibrillation-and-transcutaneous-quire-external-defibrillation.jpg)