Embed Size (px)
Citation preview
De-escalation in CAP: fact or myth?
Carlos Glória
17° Infection and Sepsis Symposium Porto 1st March 2012
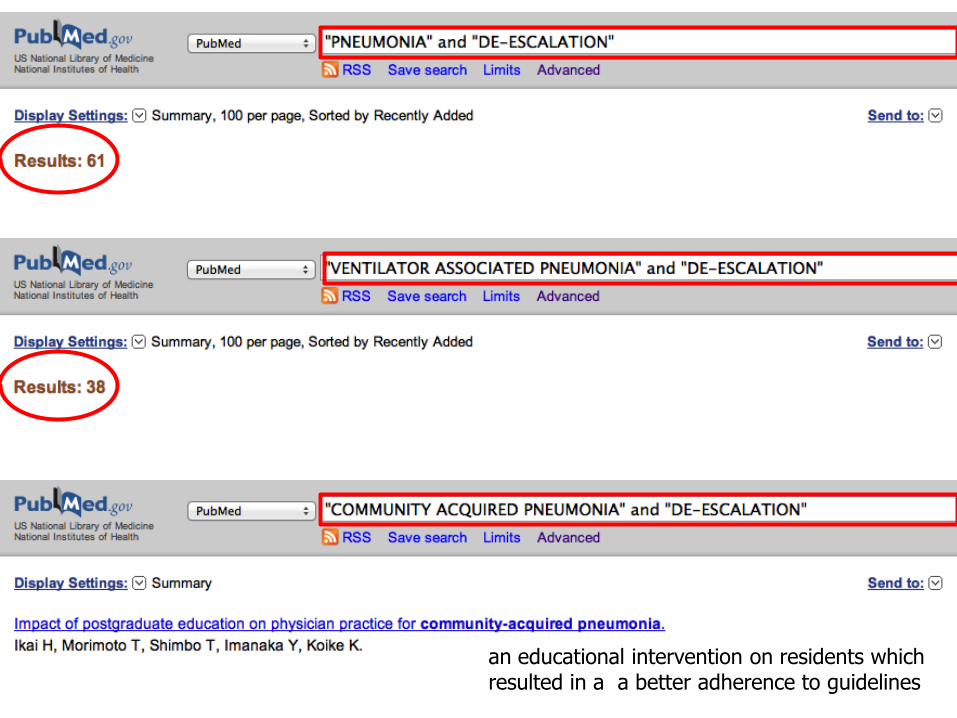
an educational intervention on residents which resulted in a a better adherence to guidelines
VAP
HAP
HCAP
CAP
It is a myth!
De-escalation in CAP: fact or myth?
2007 IDSA/ATS Consensus Guidelines on the Management of Community-Acquired Pneumonia
“ In clinical practice, narrowing of antibiotic therapy is, unfortunately, unusual, but the committee strongly recommends this as best medical practice…”
It is a myth!
It should it be a fact
De-escalation in CAP: fact or myth?
Purposal of de-escalation
appropriate initial
antimicrobial treatment
limit unnecessary antimicrobial
exposure
Two steps strategy of de-escalation
• Step 1- Give the broadest-spectrum antibiotic therapy to improve outcomes (decrease mortality, prevent organ dysfunction, and decrease length of stay)
• Step 2- Focus on de-escalating as a means to minimize resistance, decrease toxicity and improve cost-effectiveness
Pneumonias adquiridas na comunidade
Hit it hard Hit it early
Re-eavaluate (48-72h)
Get it right, the first time!
Hit it
The new treatment paradigm in severe infections
De-escalate Keep Escalate
Cover all probable agents Adequate dosage Maximize effect Combined treatment
• Narrow the spectrum – Change to antimicrobials with are not large spectrum
– Change from combined therapy to monotherapy
• Suspend antimicrobials
• Decrease the duration of treatment
Enlarged concept of de-escalation
Do we hit CAP really hard?

New kids on the block in CAP treatment
• Improved outcome with:
– Using macrolides instead of quinolones in combined therapy
– Combined therapy in bacteremic pneumococcal pneumonia
– Coverage of pseudomonas in COPD, malignancy and in patients on previous antimicrobials
• Concerns with DRSP and CA-MRSA
Inpatients, non-ICU treatment Antipneumococcal beta-lactam PLUS a macrolide Inpatients, ICU treatment Antipneumococcal beta-lactam PLUS azithromycin If Pseudomonas is a consideration Antipneumococcal, antipseudomonal beta-lactam (piperacillin-tazobactam, cefepime or meropenem) PLUS aminoglycoside PLUS azithromycin If CA-MRSA is a consideration Add vancomycin or linezolid
2007 IDSA/ATS most effective hit
Do we really need to hit hard in CAP?
(Does inadequate antimicrobial treatment affects outcome in CAP?)
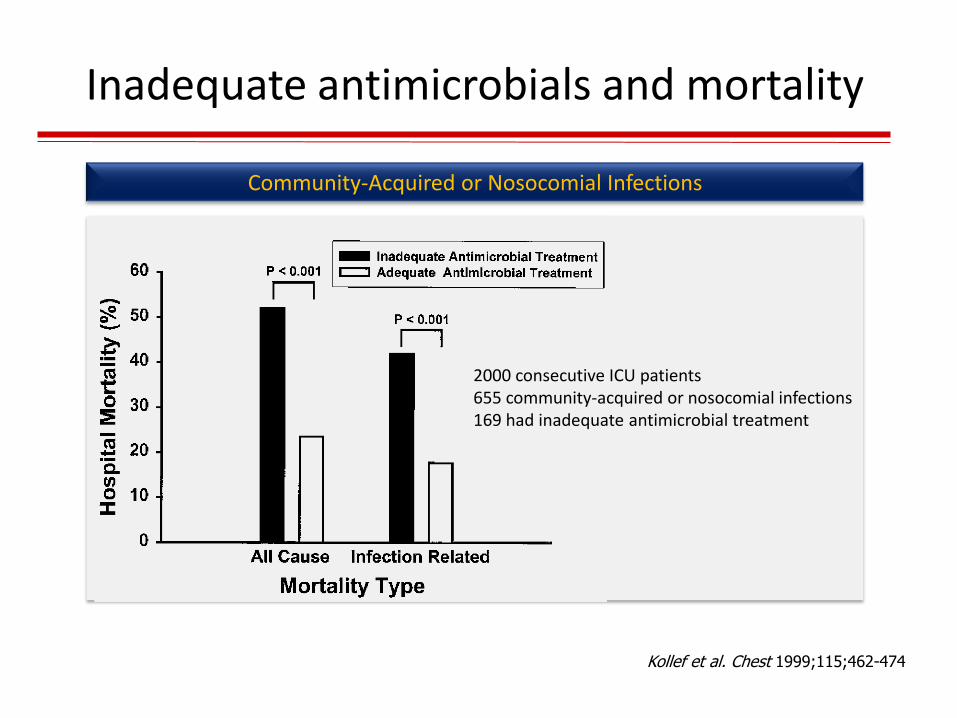
Inadequate antimicrobials and mortality
Kollef et al. Chest 1999;115;462-474
2000 consecutive ICU patients 655 community-acquired or nosocomial infections 169 had inadequate antimicrobial treatment
Community-Acquired or Nosocomial Infections

Inadequate antimicrobials and mortality
Ventilator Associated Pneumonia
Luna et al. Eur Respir J. 2006 Jan;27(1):158-64
Alvarez-Lerma et all. Intensive Care Med. 1996 May;22(5):387-94
Rello et al. Am J Respir Crit Care Med. 1997 Jul;156(1):196-200
However the evidence that the adequacy of antimicrobials affects outcome in patients with CAP is not so strong

Vallés et al. Chest 2003;123;1615-1624.
Inadequate antimicrobials and mortality
Community-Acquired Bloodstream Infections
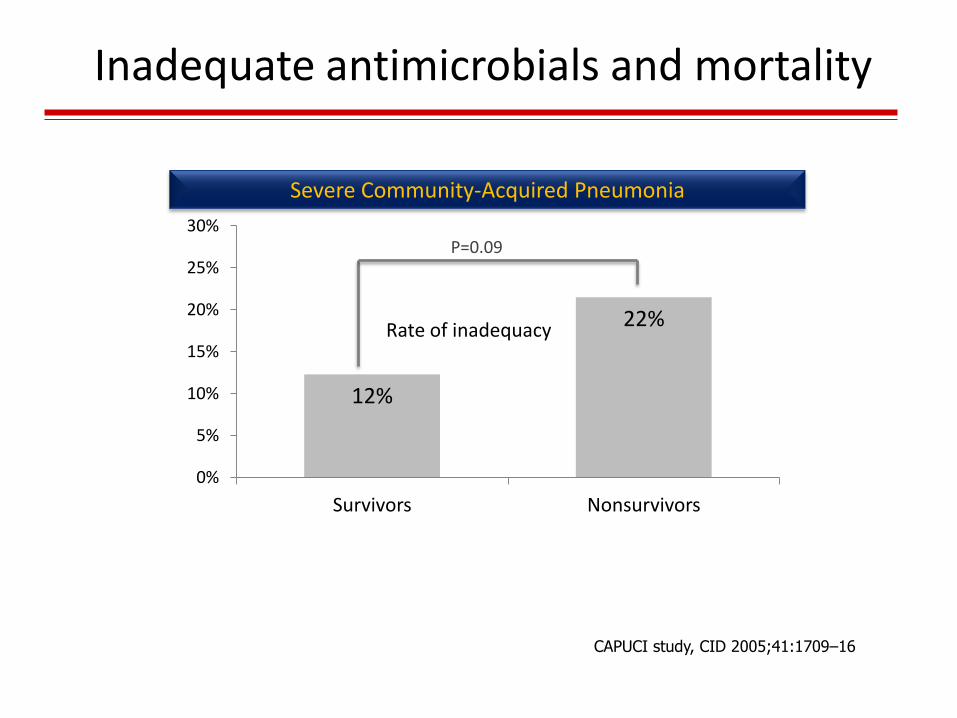
Inadequate antimicrobials and mortality
12%
22%
0%
5%
10%
15%
20%
25%
30%
Survivors Nonsurvivors
Rate of inadequacy
P=0.09
Severe Community-Acquired Pneumonia
CAPUCI study, CID 2005;41:1709–16
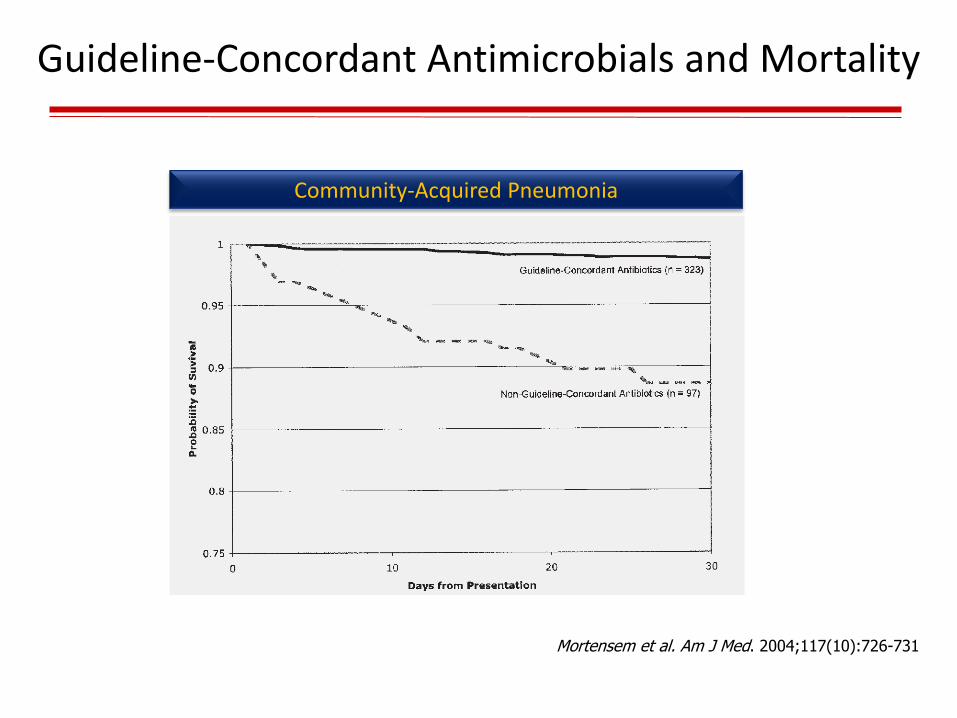
Mortensem et al. Am J Med. 2004;117(10):726-731
Guideline-Concordant Antimicrobials and Mortality
Community-Acquired Pneumonia
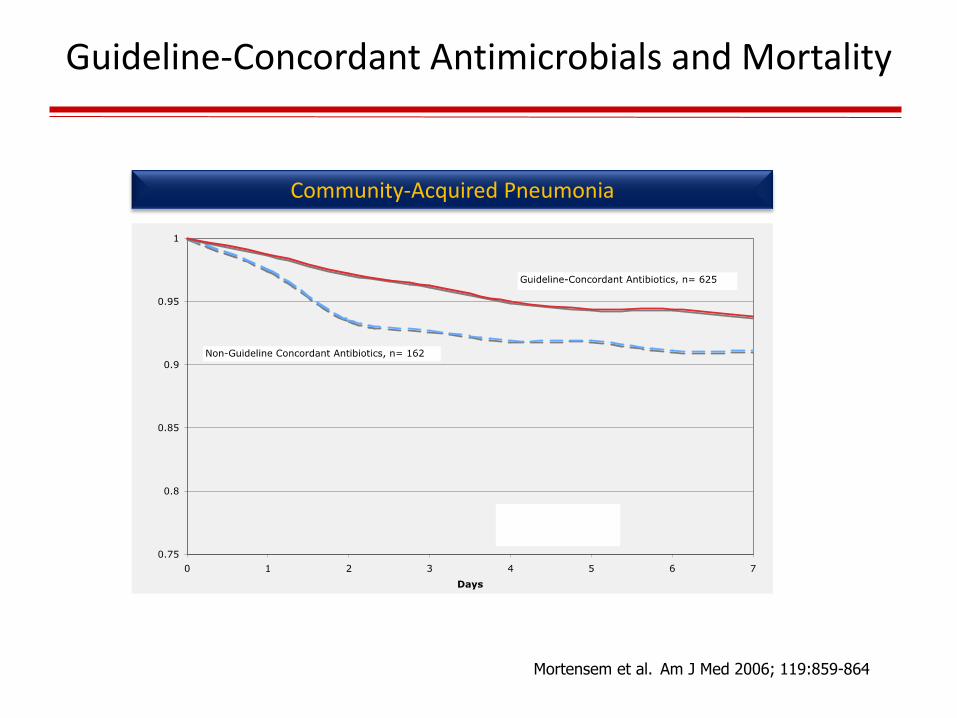
Mortensem et al. Am J Med 2006; 119:859-864
Community-Acquired Pneumonia
Guideline-Concordant Antimicrobials and Mortality
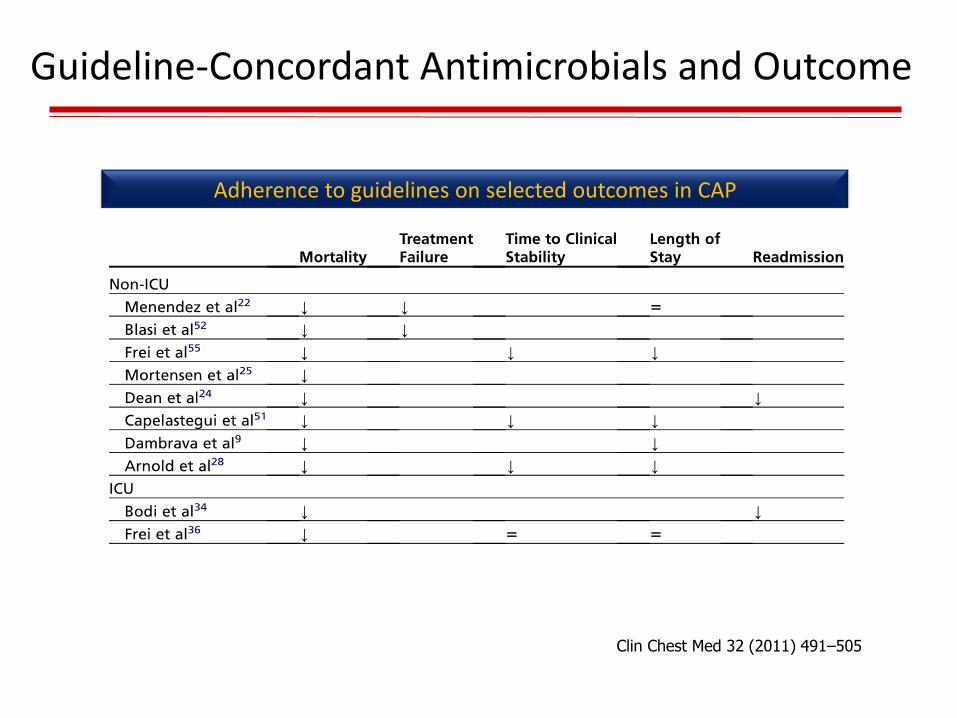
Clin Chest Med 32 (2011) 491–505
Guideline-Concordant Antimicrobials and Outcome
Adherence to guidelines on selected outcomes in CAP

• So available data suggest that inappropriate antimicrobial treatment negatively affects outcomes in CAP.
• But… it is inappropriate treatment frequent in CAP?
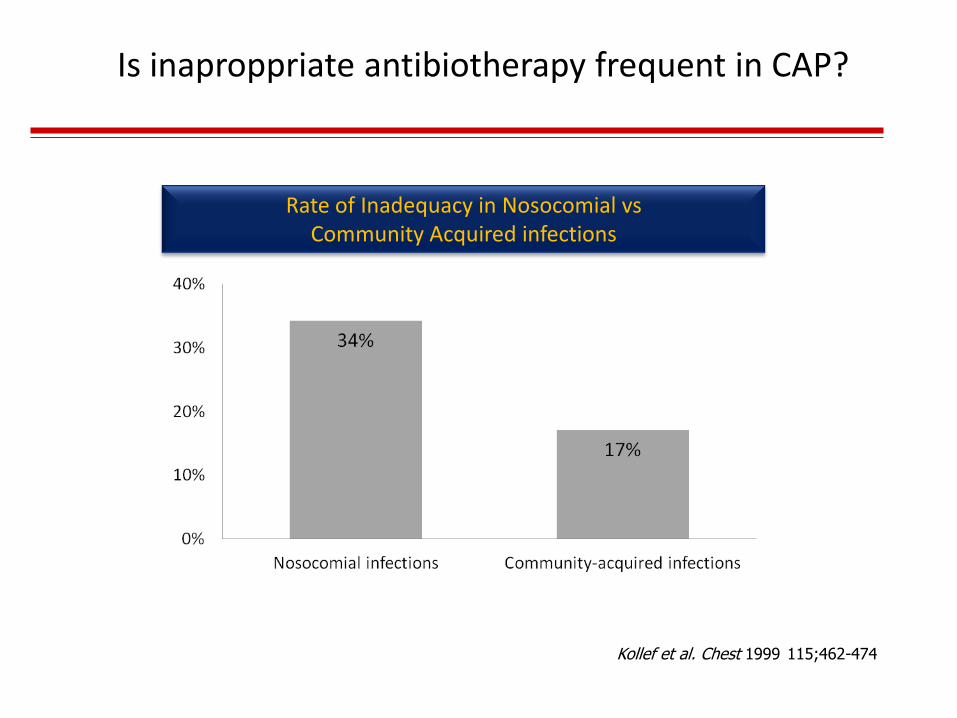
Rate of Inadequacy in Nosocomial vs Community Acquired infections
Kollef et al. Chest 1999 115;462-474
Is inaproppriate antibiotherapy frequent in CAP?
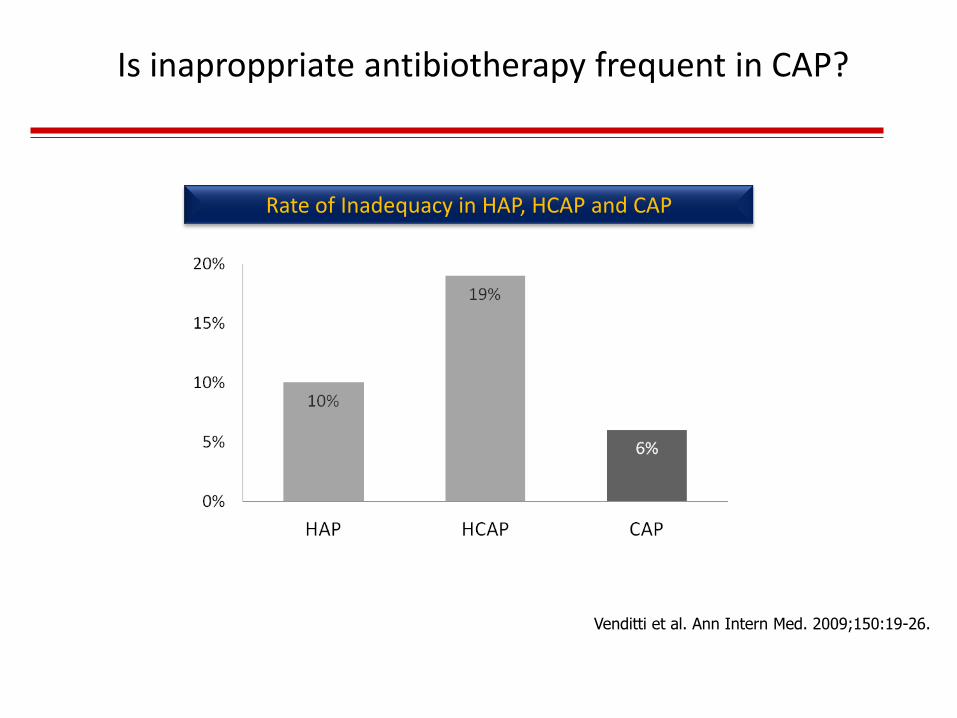
Rate of Inadequacy in HAP, HCAP and CAP
Venditti et al. Ann Intern Med. 2009;150:19-26.
Is inaproppriate antibiotherapy frequent in CAP?
Is inaproppriate antibiotherapy frequent in CAP?
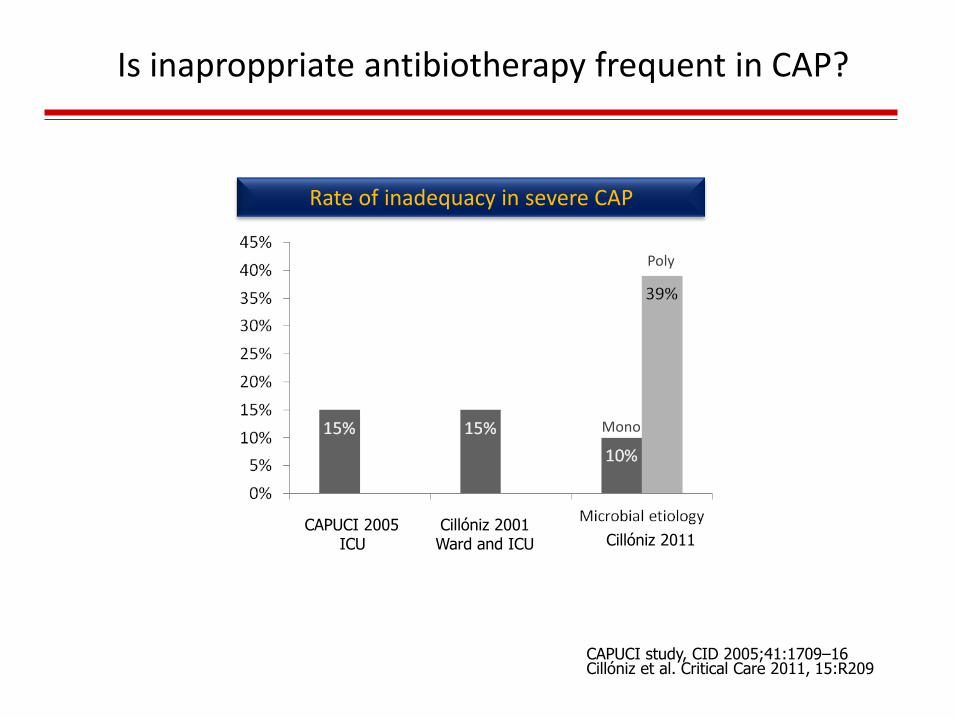
Rate of inadequacy in severe CAP
Mono
Poly
Cillóniz 2001 Ward and ICU
Cillóniz et al. Critical Care 2011, 15:R209 CAPUCI study, CID 2005;41:1709–16
CAPUCI 2005 ICU Cillóniz 2011
Are we de-escalating in CAP?
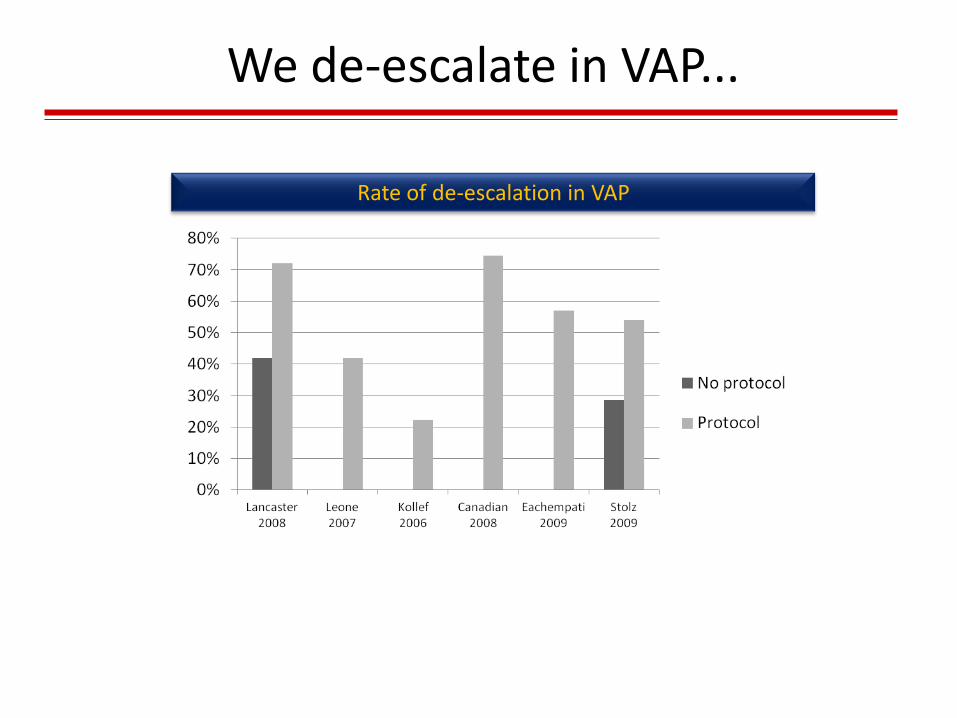
We de-escalate in VAP...
Rate of de-escalation in VAP

Rate of de-escalation in CAP
Kothe et al (Capnetz). Eur Respir J 2008; 32: 139–146
Change of antibiotic treatment
Overall change 28,6%
Ineffectiveness 11,2%
Sequential therapy 10,7%
De-escalation 4,3%
Intolerance 1,2%
Resistance 1,2%
Change of antibiotic treatment

Why don’t we de-escalate more often in CAP?
• There is nothing to de-escalate (patient on narrow spectrum antimicrobials)- “ecologic” view • Adherence to guidelines
• Low propensity for de-escalation

Protocols increase rate of de-escalation...
Rate of de-escalation in VAP
Lancaster et al. Pharmacotherapy 2008;28:852-62
Stolz et al. Eur Respir J 2009;34:1364:1375
Why don’t we de-escalate more often?
• There is nothing to de-escalate (patient on narrow spectrum antimicrobials)- “ecologic” view • Adhesion to guidelines
• Low propensity for de-escalation • Protocoled de-escalation • Stewardship approach
• Concern that de-escalation may induce a worst outcome (if it is working, why change?...)
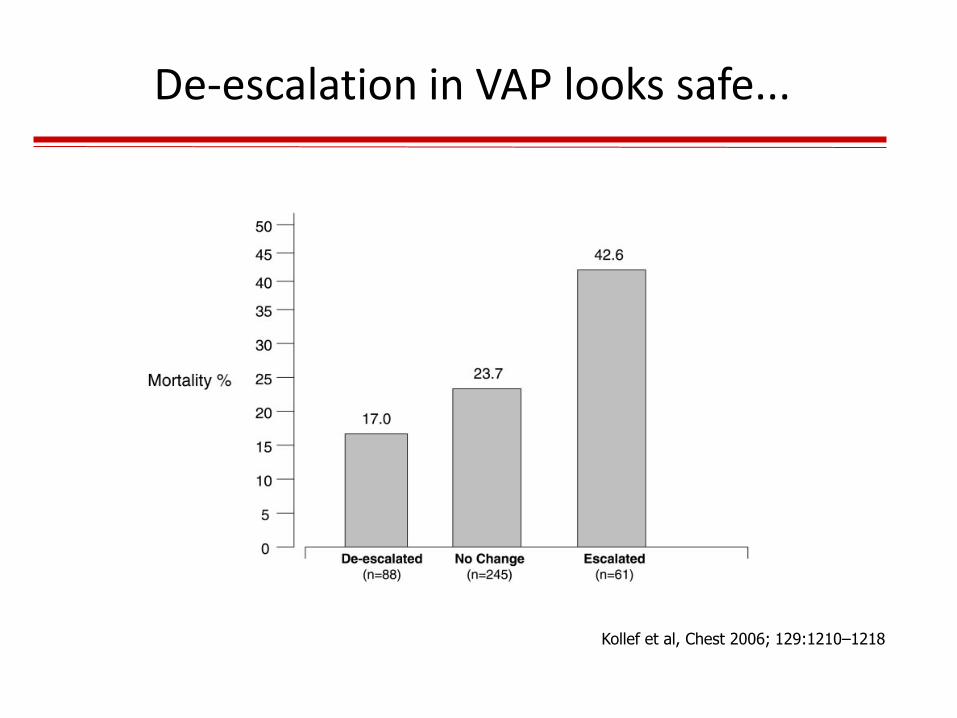
Kollef et al, Chest 2006; 129:1210–1218
De-escalation in VAP looks safe...
Why don’t we de-escalate more often?
• There is nothing to de-escalate (patient on narrow spectrum antimicrobials)- “ecologic” view • Adhesion to guidelines
• Low propensity for de-escalation • Protocoled de-escalation • Stewardship approach
• Concern that de-escalation may induce a worst outcome (if it is working, why change?...) • No evidence in CAP • Evidence in VAP suggests de-escalation is safe
• Microbiology is negative • Although 50% of CAPs are unknown etiology de-escalation still
can be considered if the patient is improving • Clinical parameters as a tool for de-escalation (CPIS) • Biomarkers as a tool for de-escalation (PCT)
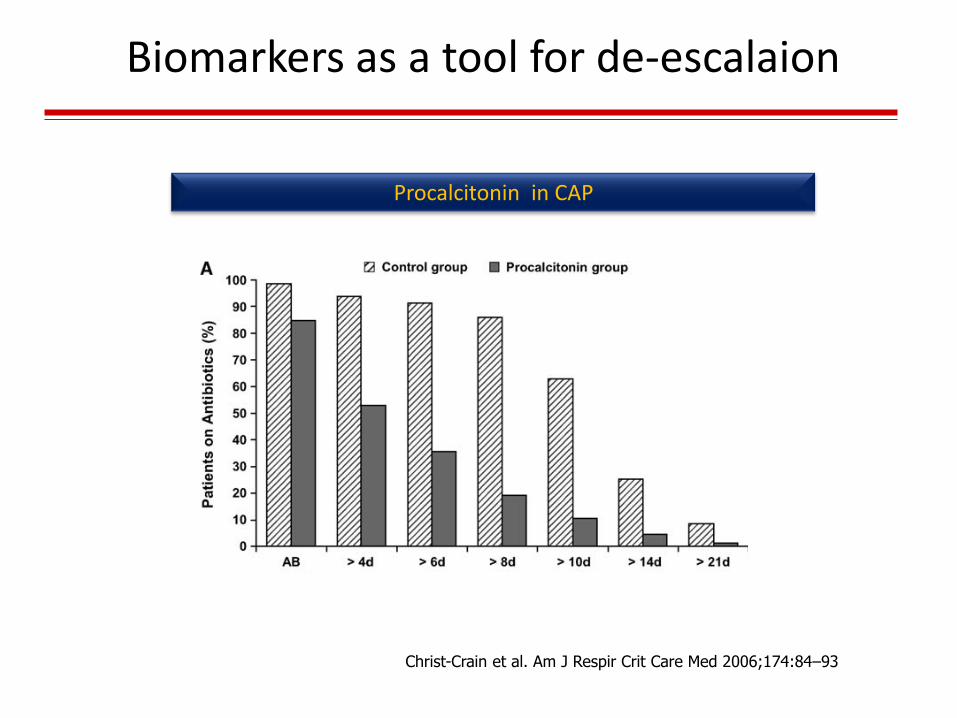
Christ-Crain et al. Am J Respir Crit Care Med 2006;174:84–93
Biomarkers as a tool for de-escalaion
Procalcitonin in CAP
Acceptable justifications for not de-escalating
• CAP etiology is polymicrobial • Bacteremic streptococcal pneumonia • CA-MRSA • DRSP • GNRB • Complications (empyema, etc.)
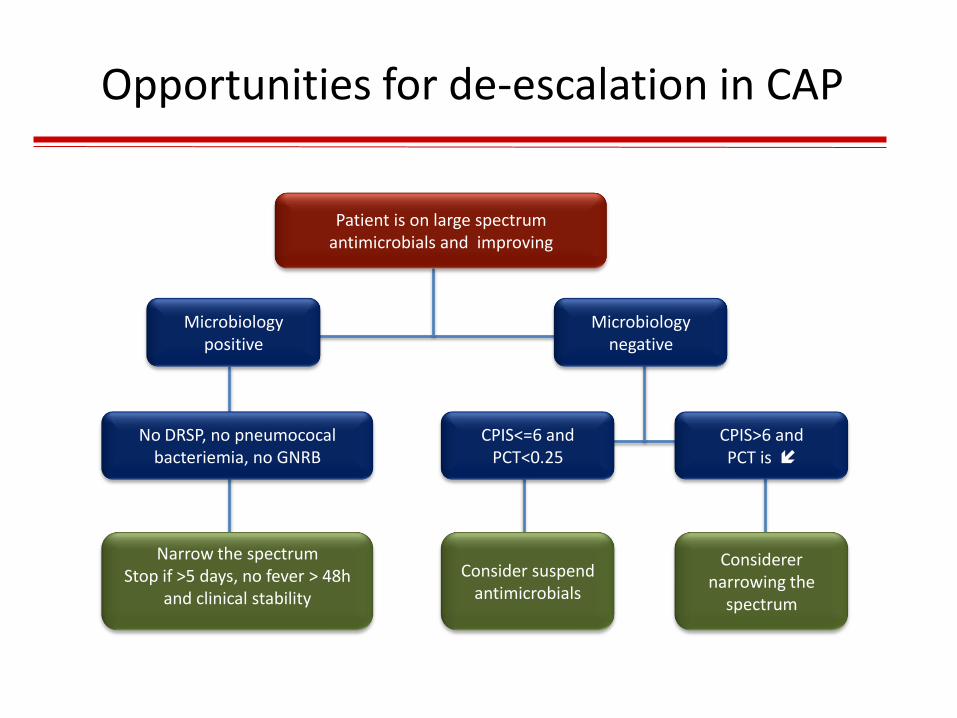
Opportunities for de-escalation in CAP
Narrow the spectrum Stop if >5 days, no fever > 48h
and clinical stability
Consider suspend antimicrobials
Patient is on large spectrum antimicrobials and improving
Microbiology positive
Microbiology negative
CPIS<=6 and PCT<0.25
CPIS>6 and PCT is
No DRSP, no pneumococal bacteriemia, no GNRB
Considerer narrowing the
spectrum
• Opportunities for de-escalation can be found in hospital practice
• Adherence to guidelines, de-escalation protocols and a stewardship approach may improve rates of de-escalation
• Available evidence on the safety of de-escalation in CAP is poor and may induce reluctance on generalized acceptance
Conclusions
Maybe de-escalation in CAP is a myth, but...
It should be a fact!
De-escalation in CAP: fact or myth?
Filipe Froes dixit
“Further studies are needed”