Embed Size (px)
Citation preview

DCHAP Stakeholders Conference Call
February 19, 2014
Polly E. Ross, MD Division Director
Department of Health and Human Services Health Resources and Services Administration
HIV/AIDS Bureau Division of Community HIV/AIDS Programs
Part C


Agenda for Today’s Call
• Brief Program Updates
• Outline of Enrollment Activities and Affordable Care Act
• Increasing Access to HIV Care and Treatment –Year One Results
• Part C Capacity Development Funding Opportunity Announcement

FY14 Part C Grant Awards
• No additional sequester for fiscal year (FY) 2014. FY13 sequester remains.
• January and April FY14 awards – will be partial funding with the balance available in May or June
• Review your Notice of Award (NoA) carefully, especially the terms, conditions, and reporting requirements and discuss any inaccuracies or questions with your Project Officer

Salary Limitations – Cap Raised
• As you recall, as a result of the 2012 Appropriations Act, HRSA grantees are required to limit salaries charged to grants
• The cap has been raised from $179,700 annually to $181,500 by Executive Order
• This amount reflects an individual’s base salary, exclusive of fringe benefits and income earned outside of the applicant organization
• The limitation also applies to subcontractor personnel

Change in the Email Regarding NoA’s
All Notices of Awards will now come from: Grantsolutions.gov

Affordable Care Act- Update
Expansion of Insurance Coverage
Many previously uninsured patients are now eligible for affordable health care coverage beginning this year.
The Affordable Care Act: • Strengthens private insurance for consumers • Creates a Marketplace in each state where individuals
and small businesses can shop for insurance • Provides financial help for many people to better afford
insurance through the Marketplace • Gives states the opportunity to expand Medicaid coverage
to low-income adults

Health Insurance Marketplace
• Every state has a Marketplace where individuals and small businesses can shop for and purchase private health insurance
• All options will be in one place, with clear language and apples-to-apples comparisons about prices and benefits
• Plans offered through the Marketplace are called Qualified Health Plans (QHPs) Enrollment starts October 1, 2013 Coverage starts January 1, 2014
Enrollment open until March 31, 2014 Coverage began January 1, 2014

Marketplace Establishment
Source: Kaiser Family Foundation. Status of State Health Insurance Exchange Decision, as of July 1, 2013, available at http://kff.org/health-reform/state-indicator/state-decisions-for-creating-health-insurance-exchanges-and-expanding-medicaid/#
State-Based (SBM):16 states and DC are setting up and managing their own Marketplaces State Partnership (SPM): 7 states are working in partnership with the federal government Federally-Facilitated (FFM): In 27 states the federal government is setting up the Marketplace

Help Paying for Qualified Health Plans
• 90% of the uninsured qualify for some form of financial assistance based on family income and size
• Eligible persons can get premium tax credits and/or purchase plans with lower cost-sharing (e.g., co-pays and deductibles)
% of Federal Poverty Level (FPL) Individuals household income* Family of 4 household income*
• Discounted Premiums • 100-400% • $11,490 - $45,960 • $23,550 - $94,200 • Reduced Cost-sharing • 100-250% • $11,490 - $28,725 • $23,550-$58,875
% of Federal Poverty Level (FPL)
Individuals household income*
Family of 4 household income*
Premium Tax Credits 100-400% $11,490 -
$45,960 $23,550 - $94,200
Reduced Cost-sharing 100-250% $11,490 -
$28,725 $23,550-$58,875
*Based on 2013 Federal Poverty Guidelines

Expanding Medicaid
SOURCES: State decisions on the Medicaid expansion as of December 11, 2013. Based on data from CMS, available at: http://medicaid.gov/AffordableCareAct/Medicaid-Moving-Forward-2014/Medicaid-and-CHIP-Eligibility-Levels/medicaid-chip-eligibility-levels.html. Data have been updated to reflect more recent activity.
WY
WI*
WV
WA
VA
VT
UT
TX
TN
SD
SC
RI PA*
OR
OK
OH
ND
NC
NY
NM
NJ
NH
NV NE
MT
MO
MS
MN
MI* MA
MD
ME
LA
KY KS
IA* IN* IL
ID
HI
GA
FL
DC
DE
CT
CO
CA
AR* AZ
AK
AL
Implementing Expansion in 2014 (26 States including DC) Seeking to Move Forward with Expansion post-2014 (2 States) Not Moving Forward at this Time (23 States)

Starting in 2014, all Americans must:

Who will Remain Uninsured?
After these new options are implemented, there may still be up to 31 million uninsured persons in the U.S in 2023, including: • Citizens under 100% FPL in states that don’t expand
Medicaid
• Individuals who are not “lawfully present”
• Persons who are exempt from the Individual Responsibility Payment (e.g., members of Indian Tribes, those with religious objections)
• Persons who choose to pay the Individual Responsibility Payment
http://www.hrsa.gov/gethealthcare/

Timelines for Enrolling
• Initial Open Enrollment started on October 1, 2013, and ends March 31, 2014, with QHP coverage effective as early as January 1, 2014
• Annual Open Enrollment: October 15, 20xx-December 7, 20xx • Special Enrollment Periods available • Medicaid enrollment will continue to occur throughout the year
Enrollment Date Effective Date of Coverage Oct. 1, 2013 - Dec. 23, 2013 January 1, 2014 Dec. 24, 2013 - Jan. 15, 2014 February 1, 2014 Jan. 16, 2014 - Feb. 15, 2014 March 1, 2014 Feb. 16, 2014 - Mar. 15, 2014 April 1, 2014 Mar. 16, 2014 - Mar. 31, 2014 May 1, 2014

4 Ways to Get Marketplace Coverage

What Providers Can Do
1. Educate patients: • What the options are: Many individuals who stand to benefit
under the expansion are not aware of their options • How insurance works: Many newly-eligible individuals would
benefit from education on how insurance works (e.g., how cost-sharing works, what a provider network is)
2. Sign up to be a Champion for Coverage
3. Partner with local organizations that provide application
assistance to: • Offer on-site application assistance • Develop a plan for referring patients to assistors

What Providers Can Do
4. Assist patients with applying for and enrolling in health coverage:
• Apply to be a Certified Application Counselor • Accessing the eligibility and enrollment system
(ideally through computer kiosks; also accessible via the phone or mail.)
• Working their way through the application • Understanding and evaluating factors they should
consider when selecting a plan. For example: o Does it cover the Rx I need? o Does it include the provider(s) I want to see?

Healthcare.gov
• Healthcare.gov is where consumers can go to: o Learn about their health insurance options o Get accurate information on different plans o Apply for and enroll in coverage o Get directed to the Marketplace in their state
• Assisters are listed at Localhelp.HealthCare.gov
• Twitter@HealthCareGov • Facebook.com/Healthcare.gov

• HRSA Affordable Care Act Website • www.hrsa.gov/affordablecareact
• Provider Marketplace Toolkit • www.hrsa.gov/affordablecareact/toolkit.html
• HIV/AIDS Bureau Affordable Care Act Website • http://hab.hrsa.gov/affordablecareact
HRSA Resources

Increasing Access to HIV Care and Treatment (IAHCT)
Emily Chew, DCHAP Project Officer Anna Huang, MD, DCHAP Clinical Advisor
22
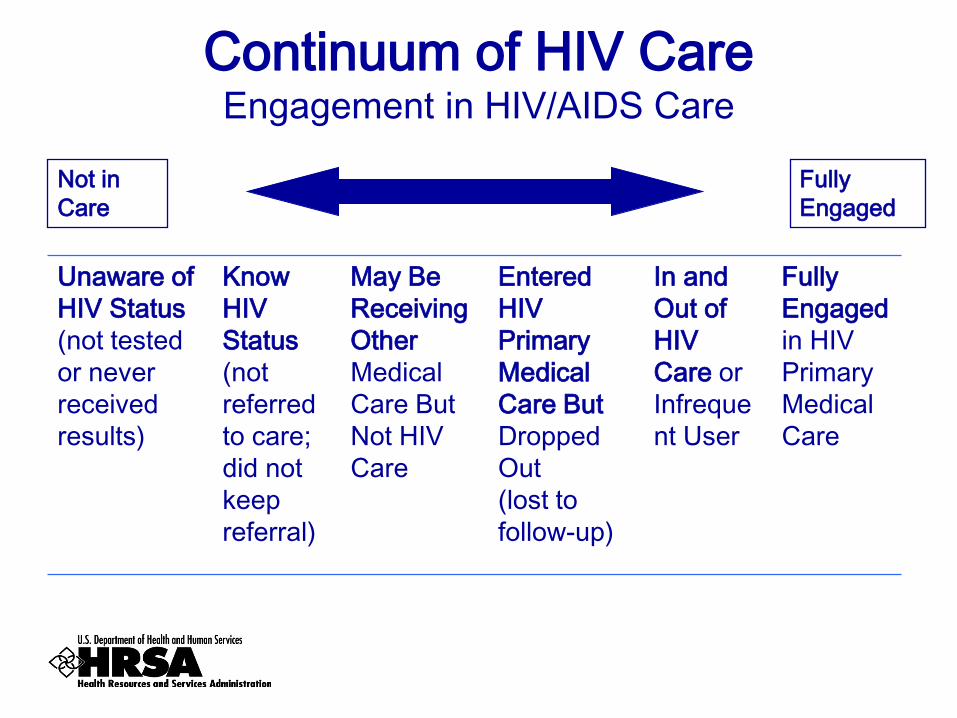
Continuum of HIV Care Engagement in HIV/AIDS Care
Unaware of HIV Status (not tested or never received results)
Know HIV Status (not referred to care; did not keep referral)
May Be Receiving Other Medical Care But Not HIV Care
Entered HIV Primary Medical Care But Dropped Out (lost to follow-up)
In and Out of HIV Care or Infrequent User
Fully Engaged in HIV Primary Medical Care
Not in Care
Fully Engaged

Increasing Access to HIV Care and Treatment (IAHCT)
• On World AIDS Day 2011, President Barack Obama announced the Increasing Access to HIV Care and Treatment (IAHCT) initiative to increase the number of people living with HIV (PLWH) who are linked to and retained in HIV care and treatment.
• In FY12, HRSA’S Bureau of Primary Health Care (BPHC) and HIV/AIDS Bureau (HAB) worked in collaboration to award over $10 million to Ryan White HIV/AIDS Program (RWHAP) Part C grantees. Supplemental awards of up to $38,000 each were awarded to 275 (77%) existing Part C grantees
• Additionally 14 new Part C grants were established throughout the U.S.

Increasing Access to HIV Care & Treatment Initiative (IAHCT)
• In FY 2012, HRSA awarded 275 grantees the Increasing Access to HIV Care and Treatment (IAHCT) supplemental funds.
• Funding for FY 2012: o Up to $38,000 o 141 awards for Part C only grantees o 134 awards for Bureau of Primary Health
Care (BPHC)/Part C dually-funded grantees

IAHCT: Five Activity Areas Funded
• Expand outreach and HIV testing for high risk populations
• Expand service hours for medical care • Enhance systems to identify, connect with
and keep people living with HIV in care • Expand support services • Hire additional providers experienced in HIV
primary medical care
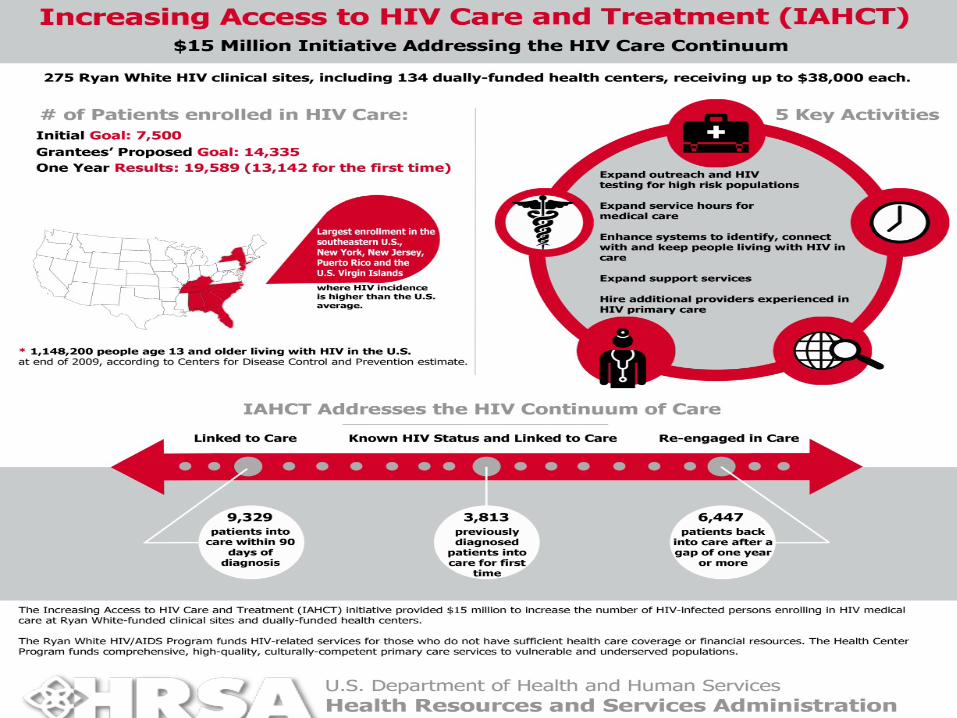

IAHCT: Year One Results
• During the first 12 months of IAHCT, RWHAP Part C clinics and dually-funded health centers enrolled 19,589 patients into HIV care. • 13,142 PLWH had never been in HIV care;
and • 6,447 PLWH were re-engaged in care after
being out of care 12 months or more. • The 14 new Part C grantees enrolled 1,629
PLWH into HIV medical care

Increasing Access to HIV Care & Treatment Initiative (IAHCT)
• The IAHCT funding is being continued in 2013 to the same grantees who were awarded in 2012. The same goals and objectives and work plan activities will remain in place for 2013. Reporting requirements for IAHCT activities will be reduced from quarterly to semi-annually.
• IAHCT reports will be due on January 31, 2014,
and July 30, 2014 for Part C funded grantees; February 28, 2014 and August 31, 2014 for the BPHC/HAB dually funded grantees.

FY2013 IAHCT Reporting
• The FY13 semi-annual progress reports should be submitted in the respective EHB file associated with the IAHCT award (either H76 or H80).
• Please contact your HAB project
officer, Anna Huang, or Emily Chew with questions or problems.

FY2014 Part C Capacity Development FOA
Carrie Jeffries, CRNP, MS, MPH, AACRN Chief, Northeast Branch
Health Resources and Services Administration HIV/AIDS Bureau
Division of Community HIV/AID Programs

Funding Opportunity Announcement HRSA-14-061
• This FOA solicits applications from existing Part C grantees under the Ryan White HIV/AIDS Program (RWHAP) Part C Capacity Development Program.
• Awards will support activities that address and impact gaps in the HIV Care Continuum, which have been identified in the grantee’s service area.

FY2014 Capacity Development Awards
• Applicants may propose one or more activities that address gaps in their local HIV Care Continuum for a one-year project period
• Funding requests may not exceed $100,000 for the project period
• Only specific short term activities will be
funded under this grant
Please refer to page 4 of the FOA.

HHS Core HIV Indicators and the HIV Care Continuum
Viral Load Suppression ART
Mugavero M et al. Clin Infect Dis 2011; 52(Suppl 2): S238-S246.
• Retention in medical care
• Housing status
Linkage to Medical Care
HIV Positivity Late HIV Diagnosis

Activities Funded Under FY14 Capacity Development
• Trainings, skills building activities, innovative interventions, which can be rapidly implemented to allow follow up evaluation of impact on the grantee’s HIV Care Continuum during the performance period.
• 4 major areas: • Disease Case Finding • Motivational Interviewing • Patient-Based Treatment Adherence • Patient Self-Managed Chronic Disease Management

Capacity Development Activities
• These should be short term activities that increase the capacity of grantee or sub-awardee staff to implement activities that will reduce gaps in specific Care Continuum stages across your HIV service system or in the local service area
• Evaluation will involve required data collection for the Ryan White Services Report on the HHS core/HAB HIV indicators

Application: Where is it?
• Final Guidance located at www.grants.gov • Also can be found at:
• www.hrsa.gov/grants • Announcement HRSA-14-061, CFDA 93.918
Application Instructions (FOA & Application Guide) • Application Guide Package www.hrsa.gov/grants/guideforreview/applicationguideforreview.doc
• Adobe Reader 8.1.1 version or later
36

REMINDER
• The application should be electronically submitted in Grants.gov by March 17, 2014, 11:59 pm ET
• We recommend submission of the application
at least four business days before due date

Your Questions are Welcome
Applicants in need of technical assistance as they prepare their applications may call or email:
Program Contact Grants Contact Carrie Jeffries Beverly Smith [email protected] [email protected] 301-443-2399 301-443-7065
HAB TARGET Website
http://careacttarget.org/webcasts.asp

QUESTIONS?
Please use the Chat pod for any questions

Contact Information
Polly Ross, MD Division Director
Division of Community HIV/AIDS Programs
301-443-0493 [email protected]





























