Embed Size (px)
Citation preview

Percutaneous mitral interventions:
where are we, where do we go?
Alec Vahanian, FESC, FRCP (Edin.)
Bichat Hospital, Paris, France

Percutaneous Mitral Commissurotomy:
The gold standard?
Percutaneous Mitral Commissurotomy
Surgical Commissurotomy
(K. Inoue, 1984) (D.Harken, 1948)

Bouleti C, Iung B, Himbert D, Brochet E,
Messika-Zeitoun D, Garbarz E, Cormier B,
Michel PL, Luxereau P, Vahanian A.
Bichat Hospital, Tenon Hospital, AP-HP, Paris, France
Twenty-Year Results of Percutaneous
Mitral Commissurotomy in a Series of
1024 Patients.
(ESC Annual congress 2010)

Immediate Results
Adverse events
- In-hospital death: 4 patients (0.4%)
- Embolism with sequelae: 3 patients (0.3%)
- Mitral regurgitation ≥ 3/4: 35 patients (3.4%)
Valve function
Valve area Mean gradient
0
0,5
1
1,5
2
Planimetry Doppler0
2
4
6
8
10
12
Mean Gradient
Before PMC
After PMC
cm² mmHg

20-Year Results
Survival without Surgery or Re-PMC, and in NYHA class I or II
n= 912 836 752 651 553 483 424 353 222 105 43
n= 1024 867 768 665 563 492 433 361 227 108 45
n= 112 31 16 14
32.3±2.5%
29.4±2.0%
12.1±3.1%
YEARS
(%)
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16 18 20
Good immediate results (n=912) All patients (n=1024) Poor immediate results (n=112)

The Role of Percutaneous
Valve Interventions
0%
20%
40%
60%
80%
100%
AS AR MS MR
Percut. Int.
Valve Repair
Bioprosthesis
Mech Prosthesis
Homograft
Autograft
N = 512 119 112 155
(Iung. Eur Heart J 2003;24:1231)

Current percutaneous techniques
Future directions
Conclusion
Percutaneous Treatment of
Mitral Regurgitation

Transcatheter Mitral Valve Therapies
Above water
MitraClip
Coronary Sinus
Annuloplasty devices
Still under the waterline
Direct Annuloplasty
Mitral Valve Replacement
…..

Edge to Edge Percutaneous Repair

Edge-to-Edge Technique

Clinical Experience
Data as of 9/10/2010.
.
Study Population n
EVEREST I (Feasibility)* Non-randomized 55
EVEREST II* Pre-randomization 60
EVEREST II High Risk Registry 78
EVEREST II (Pivotal) Randomized patients 279
REALISM (Continued Access) Patients 408
EUROPE Commercial Patients 1109
Total1,894 MitraClip
+ 95 surgery

EVEREST II Randomised Clinical Trial
Study Design
279 Patients enrolled at 37 sites
Randomised 2:1
Echocardiography Core Lab and Clinical Follow-Up:
Baseline, 30 days, 6 months, 1 year, 18 months, and
annually through 5 years
Control GroupSurgical Repair or Replacement
n=95
Significant MR (3+-4+)Specific Anatomical Criteria
Device GroupMitraClip System
n=184
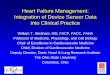
EVEREST II Randomised Clinical Trial
Key Inclusion/Exclusion Criteria
Inclusion
Candidate for MV Surgery
Moderate to severe (3+) or
severe (4+) MR
• Symptomatic
– >25% EF & LVESD
≤55mm
• Asymptomatic with one or
more of the following
– LVEF 25-60%
– LVESD ≥40mm
– New onset atrial
fibrillation
– Pulmonary hypertension
Exclusion
AMI within 12 weeks
Need for other cardiac surgery
Renal insufficiency
• Creatinine >2.5mg/dl
Endocarditis
Rheumatic heart disease
MV anatomical exclusions
• Mitral valve area <4.0cm2
• Leaflet flail width (≥15mm) and
gap (≥10mm)
• Leaflet tethering/coaptation
depth (>11mm) and length
(<2mm)

Device (%)
n=184
Control (%)
n=95 P
Age (mean) 67.3 years 65.7 years 0.32
Male 62.5 66.3 0.60
Congestive heart failure 90.8 77.9 <0.01
Coronary artery disease 47.0 46.3 >0.99
Myocardial infarction 21.9 21.3 >0.99
Angina 31.9 22.2 0.12
Atrial fibrillation 33.7 39.3 0.42
Cerebrovascular disease 7.6 5.3 0.62
Peripheral vascular disease 6.5 11.6 0.17
Cardiomyopathy 17.9 14.7 0.61
Hypercholesterolemia 61.0 62.8 0.80
Hypertension 72.3 78.9 0.25
Moderate to severe renal disease 3.3 2.1 0.72
Diabetes 7.6 10.5 0.50
Previous cardiovascular surgery 22.3 18.9 0.54
MR Severity: 3+ to 4+ 95.7 92.6 0.48
MR Etiology: Degenerative / Functional 73 / 27 73 / 27 0.81
EVEREST II RCT
Baseline Demographics & Co-morbidities

EVEREST II RCT: Patient Flow
Acute Procedural Success (APS) = MR ≤2+ at discharge
12 months
n=13498.5% Clinical Follow-up
98% Echo Follow-up
12 months
n=7494% Clinical Follow-up92% Echo Follow-up
30 days
n=13699% Clinical Follow-up
30 days
n=7999% Clinical Follow-up
Acute Procedural SuccessAchieved
n=137 (77%)
Randomized, not treatedDevice, n=6
Control, n=15
Treatedn=178
Treatedn=80
(86% MV repair)
Device Groupn=184
Acute Procedural SuccessNot Achieved
n=41**20 of 41 no implant
Control Groupn=95
Randomised Cohort n=279
Intent to Treat Cohort

1616
EII RCT: Safety & Effectiveness Endpoints
Intention to Treat Cohort
Met superiority hypothesis• Pre-specified margin =2%• Observed difference = 34.2%
Met non-inferiority hypothesis• Pre-specified margin = 25% • Observed difference = 7.3%

30 Day Modified MAE II*
Intent to Treat, Hierarchical EventsSafety endpoint met with a wide margin
0
10
20
30
40
50
Device Control
30 D
ay
Modifie
d M
AE I
I (%
)
Major Bleeding Complication*
GI Complication
New Onset Atrial Fibrillation
Ventilation >48hrs
Urgent CV Surgery
Stroke
Death5.0%
30.9%
*Major bleeding requiring transfusion ≥ 4U or surgical intervention Based on STS reporting of RBC transfusions
p<0.0001
Device Control

Primary Effectiveness Endpoint
Components
12 Month Endpoint
Components
% Patients experiencing event
Device Group
(n=134)
Control Group
(n=74)p-value
Death 4.5% 6.8% 0.5260
MV Surgery or
Re-operation for MV
dysfunction
6.7% 2.7% 0.3344
MR>2+ 16.4% 2.7% 0.0026
Total 27.6% 12.2%
Difference Device-Control 15.4%
(90% two-sided Conf Int: 5.4%, 25.4%)

0
20
40
60
80
100
Baseline 12 Months
Perc
ent Patients
0
20
40
60
80
100
Baseline 12 Months
MR Reduction
Baseline vs 12 Months, Per ProtocolSurgery more often achieves lower degree of residual MR
p<0.0001
1+
1+-2+
2+
4+
(n=119) (n=119)
Device Control
3+
2+
4+
3+
1+
1+-2+
2+
4+
(n=67) (n=67)
3+
2+
3+
0+1+-2+ 7.7% (1/13)
Replacement
13.4%
36.1%
11.8%
33.6%
16.0%
17.4%
58.2%
8.7%
3.0%
18.4% (7/38) Replacement
2.5%
p-value compares the distribution of MR grade in device with the distribution of MR grade in control at 12 months (Fishers’ Exact test)

3,6 3,53,3 3,3
0
1
2
3
4
5
65,55,1
5,4
4,8
0
1
2
3
4
5
6
Dim
ensi
on (
mm
)
Baseline
12 Months
Device(n=122)
Control(n=66)
LV Dimensions
Baseline vs 12 Months, Per Protocol, Matched Cases
p<0.0001 p<0.0001
Device(n=120)
Control(n=66)
p=0.0564 p=0.4785
End Diastolic Dimension (LVIDd) End Systolic Dimension (LVIDs)
*p=0.0030
p-value compares baseline to 12 month measurements within device and control* p-value compares change from baseline to 12 months between device and control
*p=0.4070

NYHA Functional Class
Baseline vs 12 Months, Per Protocol, Matched Cases
0
20
40
60
80
100
Perc
ent
Patients
97.6%NYHA
Class I/II
87.9%NYHA
Class I/II
n=124 n=66
I
II
III
I
II
III
IVIV
III
II
I
II
I
Device Control
Baseline Baseline12 months 12 months
p<0.0001 p<0.0001
*p=0.0162
p-value compares the distribution of NYHA class at baseline to the distribution at 12 months within device and control*p-value compares the distribution of NYHA class in device to the distribution in control at 12 months (Fishers’ Exact test)

European Experience
*Data as of 8/31/2010. Source: EU Case Observation Reports
N = 1060 Total Patients
4
10 912
7
1614
19
26 25
3028
35 35
47
53 54
70
7880
87
112
97
112
0
20
40
60
80
100
120
Sep
08
Oct Nov Dec Jan
09
Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan
10
Feb Mar Apr May Jun Jul Aug
Co
un
t
# of Patients Treated
# of Sites
# of Sites Treating Patients
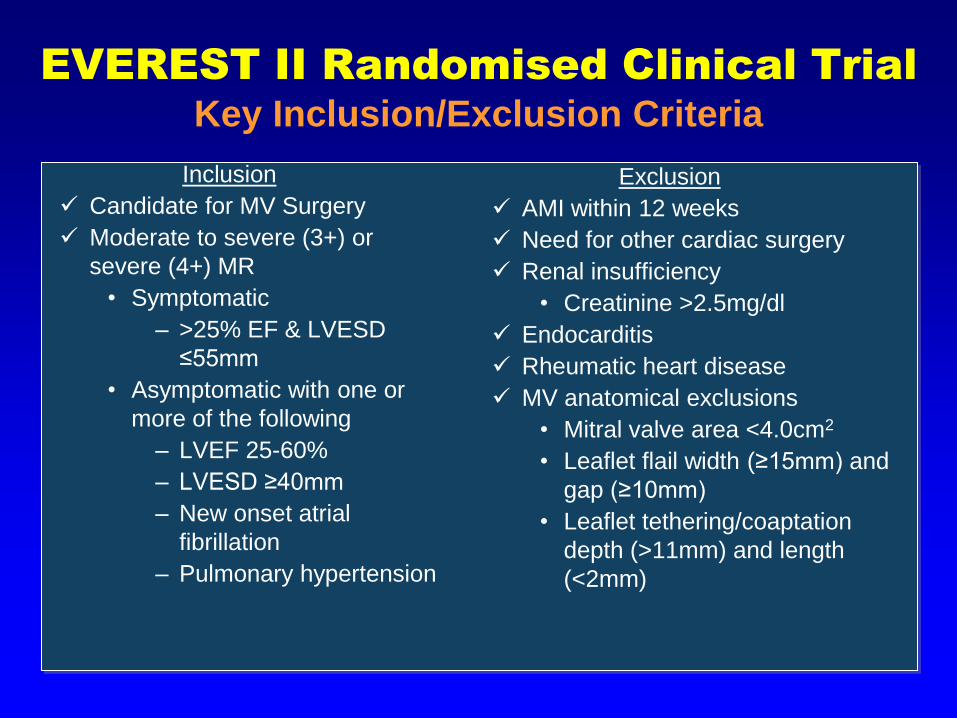
European Experience
Overall Results
Patients Treated 1060
Hospitals/Sites 56
Etiology: FMR/DMR/Mixed (%) 64%/29%/8%
Average Device Time (hr:min) 1:51
Clip Implant Rate (%) 96%
1 Clip/2 Clip/3 Clip/4 Clip(%) 67%/30%/2%/<1%
Site Reported MR Reduction (%) 98%
Clip Embolization (%) 0.01%
(Maisano,TCT 2010)

(Alfieri et al. J Thorac Cardiovasc Surg 2001;122:674-81)
Potential Limitations of Percutaneous
Edge to Edge technique
Lack of annuloplasty

(De Bonis et al. Circulation 2005;112:I-402) (Bhudia. Ann Thoracic Surgery
2004;77:1598-606)
Potential Limitations of Percutaneous
Edge to Edge technique
Controversial Surgical Results
(N=31) (N=230)

Management of Symptomatic Severe
Chronic Organic Mitral Regurgitation
LVEF > 30%
NoYes
Valve repair is likelyand low comorbidity
NoYes
* valve replacement can be considered in selected patients
Surgery (repair whenever
possible) Medical therapy*
Transplantation
Refractory to medical therapy
Yes No
Medical therapy
Severe symptomatic organic MR
(ESC Guidelines, Eur Heart J 2007;28:230-68)
A role for E to E?
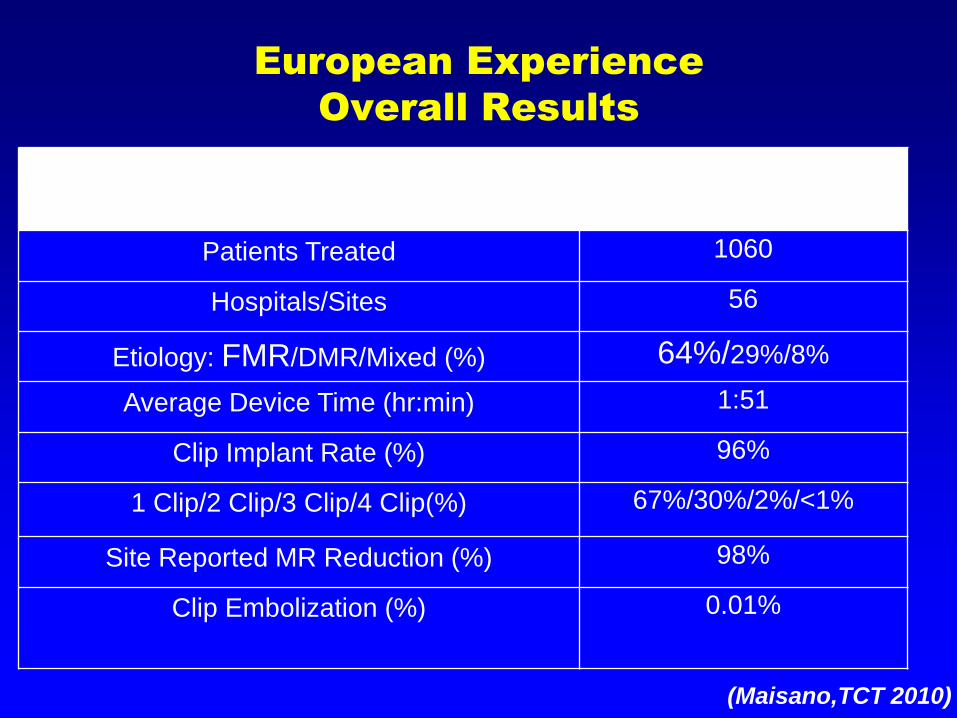
Potential Candidates for Percutaneous
E to E Technique in Organic MR
After assessment by the ‘Team’
Severe MR
Absence of anatomic contraindication according to EVEREST
criteria
Symptomatic
Life expectancy >1year
Contraindication for surgery, or high risk for surgery
AND/OR
History of thoracic irradiation
Patent coronary bypass
Severe calcification of mitral annulus
Previous aortic valve replacement

Indications for Surgery in
Ischaemic / Functional MR
Chronic Ischemic MR Class
Patients with severe MR, LV EF > 30% undergoing CABG I C
Patients with moderate MR undergoing CABG if repair is
feasible
IIa C
Symptomatic patients with severe MR, LV EF < 30% and
option for revascularization
IIa C
Patients with severe MR, LVEF > 30%, no option for
revascularization, refractory to medical therapy, and low
comorbidity
IIb C
Functional MR : surgery can be considered only in selected
patients with severe symptoms despite optimal medical therapy
(ESC Guidelines, Eur Heart J 2007;28:230-68)
A role for E to E?

Patients at Increased Risk for
Mitral Valve Repair in CHF
Presence of >4 of the following:
LV end diastolic Diam. >80mm
Peak Vo2<13ml/kg/mn
Resting BP<80mmHg
Atrial fibrillation
Heart failure duration >8years
Exercise-induced increase
in systolic BP<10%
Six-mn walk <350m
Previous cardiac surgery
BUN>100mg/dl
Cachexia
(Mehta. J Am Coll Cardiol 2005;45:388-90)
Need for a team discussion with HF specialists and transplant team to discuss indications of E to E or LV assist as a destination therapy or transplant

Coronary Sinus Annuloplasty

The Devices
The Edwards MONARC
system*
The CARILLON device
The PTMA Implant
System*
* abandoned
Distal AnchorProximal Anchor
Bridge
Elongated bridge at implant Foreshortened state at ~6 weeks

Prosthetic Ring Annuloplasty
Technique

EVOLUTION I Study Overview
INCLUSION
Functional mitral valve regurgitation: dilated or ischemic cardiomyopathy
MR grade 2+ to 4+ on a scale of 4+
Coronary Sinus Dimensions Target Area is ≥ 14 cm
and ≤ 18 cm in length, Distal section of Target
Area, the AIV is ≥ 3 mm in diameter
EXCLUSION
Organic mitral regurgitation
Ischemia requiring cardiac revascularisation within 3 months prior to or planned after the implant procedure
Implanted cardiac defibrillator (ICD) or pacing leads within the coronary sinus
Ejection Fraction < 25%
Moderate to severe mitral annulus calcification

Monarc* Carillon † Viacor ‡
n= 72 48 27
Success implantation (%) 82 63 48
In-hospital death (%) 0 2 0
Myocardial infarction (%) 4 6 0
Tamponade (%) 3 6 4
Dissection of coron. sinus (%) 0 6 NA
* JACC Intervention, in press
† Circulation 2009;120:326-33
‡ Circ Cardiovasc Intervention 2009;2:277-84
Percutaneous Mitral Annuloplasty
Feasibility / Safety at 30 Day

Percutaneous Mitral Annuloplasty
Six Minute Walk Test
307
387403
100
200
300
400
500
Me
ters
n=30 n=28 n=23
304
400
100
200
300
400
500
349 351
100
200
300
400
500
Implanted Patients (N=32))
Non-Implanted Patients (N=14)
P<0.001
NS
P<0.001
Implanted Patients
Baseline 1 Month 6 Months
AMADEUS™ TITAN™(Interim)
(Courtesy J Schofer)

Mitral valve
Tricuspid
valve
Coronary
sinus
Potential Limitations of Percutaneous
Coronary Sinus Annuloplasty

Monarc*
n=27
Carillon†
n=23
Viacor‡
n=9
Pre 3 yr Pre 6 Mo. Pre Post
Reduction MR
≥1/4 (%)
- 59 - NA - 22
ERO ( cm²) 0.22 0.15 0.25 0.17 NA NA
Rvol (ml) 32 23 35 24 NA NA
* JACC Intervention in press
† Circulation 2009;120:326-33
‡ Circ Cardiovasc Intervention 2009;2:277-84
Potential Limitations of Percutaneous
Coronary Sinus Annuloplasty
Limited Efficacy

50 PatientsBaseline & 90-Day Angio
35 PatientsNo Coronary
Vessel Changes
15 Patients (30%)Coronary
Vessel Changes
( 3MI’s (1death))
9 PatientsBridge
Compression
5 Patients Anchor
Compression
1 PatientAnchor & Bridge
Compression
5 Faulty devices4 Device separation
1 Device slippage
• Monarc
• Carillon6 cases (12%) of coronary compression (device recaptured)
(Schofer et al. Circulation 2009;120:326-33)
Potential Limitations of Percutaneous
Coronary Sinus Annuloplasty
Coronary Compression

Surgery of Ischaemic MR CABG
With or Without Valve Repair
2 groups of patients with ischaemic MR 3/4 matched according to a propensity score
54 had isolated CABG54 had CABG + valve repair
No significant difference in survival and NYHA class III-IV during F.U.
(Mihajlevic. J Am Coll Cardiol 2007;49:2191-201)

Current percutaneous techniques
Future directions
Conclusion
Percutaneous Treatment of
Mitral Regurgitation

« Valve in a Valve »
(Courtesy D Himbert)

(De Weger et al. Eur J Cardio-thorac Surg. 2010)
« Valve in a Ring »
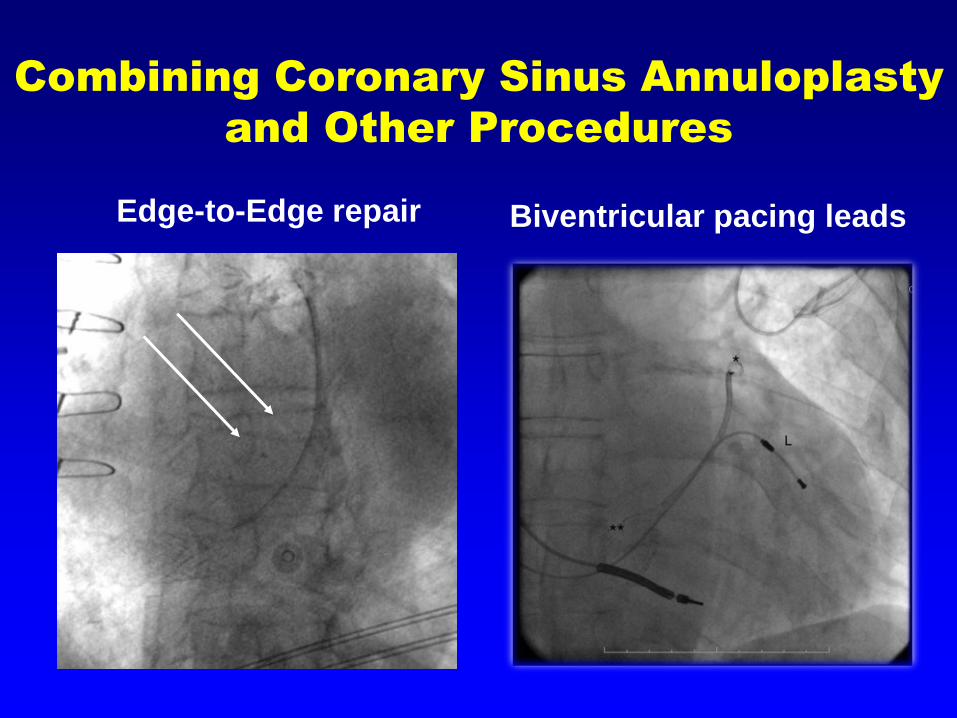
Biventricular pacing leadsEdge-to-Edge repair
Combining Coronary Sinus Annuloplasty
and Other Procedures
Transcatheter Mitral Valve Therapies
Above water
MitraClip
Coronary Sinus Annuloplasty
devices
Still under the waterline
Direct Annuloplasty
Mitral Valve Replacement
…..

Lenox HillHeart and VascularInstituteOf New York

Lenox HillHeart and VascularInstituteOf New York
• Transcatheter apically-anchored balloon
• Phase 1 clinical
• Target: FMR
• Everest II completed
• Pending FDA approval
• Target: OMR and FMR
Lenox HillHeart and VascularInstituteOf New York
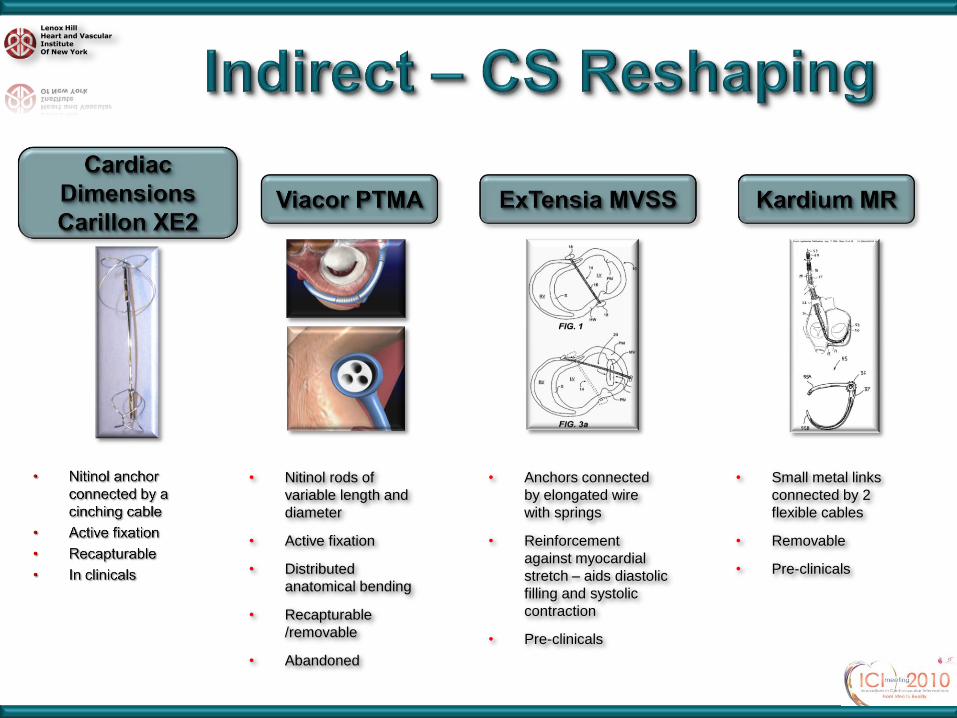
• Nitinol rods of
variable length and
diameter
• Active fixation
• Distributed
anatomical bending
• Recapturable
/removable
• Abandoned
• Anchors connected
by elongated wire
with springs
• Reinforcement
against myocardial
stretch – aids diastolic
filling and systolic
contraction
• Pre-clinicals
• Small metal links
connected by 2
flexible cables
• Removable
• Pre-clinicals

Lenox HillHeart and VascularInstituteOf New York
• HIFU on a non-occlusive balloon
• Change in collagen ⇒ shrinkage
• Successful FIM study

Lenox HillHeart and VascularInstituteOf New York
• Retro-aortic approach
• Sub-annular placement of self-expanding anchors
encasing a cinching cable along the posterior annulus
• In clinical trials
Cinching cable
P1
P3
P2

Lenox HillHeart and VascularInstituteOf New York
• Transseptal ring secured from trigone-to-
trigone with miniature anchors
• Adjustable

Lenox HillHeart and VascularInstituteOf New York

Lenox HillHeart and VascularInstituteOf New York
• Transpericardial (mini-thoracotomy)
• Adjustable over time
• Impacts annular and subannular
• Approximation of both papillary
muscles
• Preclinical

Lenox HillHeart and VascularInstituteOf New York
• Nitinol frame
• Bovine pericardium
• PTFE membrane
• Transapical
• Repositionable
• Nitinol frame
• Proprietary pericardium
• Annular anchoring without relying
on radial force
• Transseptal
• Nitinol frame
• Refocused on direct transatrial
delivery
Transcatheter valve interventions are
the natural evolution of mitral valve
surgery
Most surgical procedures can be delivered through a catheter
Image guidance will enable feasibility and safety
Physiologic fine tuning will enhance therapeutic benefit
New concepts could expand current indications
The Future of
Cardiac Surgery:
The Times, They
Are a Changin’
ATS
2005;79:1470-
1472

• The current results obtained with E to E technique suggest
that it may be useful in selected high risk patients.
• The results with coronary sinus annuloplasty are
disappointing
• In the future combination of techniques and evaluation of
new devices aimed at reproducing surgical techniques is
expected
• Results should be carefully evaluated in comparison to
surgery and contemporary medical treatment
Percutaneous Treatment of
Mitral Regurgitation

Remember…..