Embed Size (px)
Citation preview

IOTH ANNIVERSARY ARTICLE
Cytogenetics of Colorectal Adenocarcinomas
Martine Muleris, R6my-Jacques Salmon, and Bernard Dutrillaux
ABSTRACT: The occurrence of nonrandom chromosmnal anomalies in colorectal adenocarcinomas could be demonstrated from the cytogenetic study of 100 cases. The most frequent changes are a rearrangement of chromosome 17, leading to the loss of its short arm and a loss of one chromosome 18. Three types af tumors with abnormal karyotypes can be defined. First are the monosomic-type near-diploid tumors (MD), characterized by a monasomy of both 17p and chromosome 18 mostly associated with other recurrent monosomies. In two of three cases, one or several minor derived polyploid subclones are also observed. Second are the monasomic- type polyploid tumors (MP), which have a pattern of chromosome imbalance very similar to that of MD tumors. They derive from MD tumors by endoreduplication followed by complete disappearance of the original MD clone. Third are the trisomic-type tumors (TT), which lose either 17p or chromosome 18 or none, most of the anomalies being gains of entire chromosomes. These TT tumors never undergo endoreduplication. In addition, seven tumors with normal karyotypes were found and may constitute another category (NT). A nonrandom distribution of these tumor types in relation to tumor site was observed, since in the distal colon, TT and NT tumors are underrepresented and endoreduplications are significantly more frequent. The level of chromosomal mutagenesis is two- to threefold higher in MD and MP than in TT tumors. More than 95% of the rearrangements are unbalanced, and most of them result from breakpoints located in juxtacentromeric heterochromatin. A good correlation is found between our results and the available molecular data on ollelic losses. The involvement of recessive tumor suppres- sor genes in colorectal tumorigenesis and the possible relationship between chromosomal imbalances and deviations in metabolic pathways is described.
I N T R O D U C T I O N
A m o n g h u m a n so l id t u m o r s , a d e n o c a r c i n o m a s of the c o l o n a n d r e c t u m h a v e b e e n t h o s e m o s t e x t e n s i v e l y s t u d i e d cy togene t i ca l ly . T h i s i n t e r e s t c an be e x p l a i n e d by t he s e r ious c o n t r i b u t i o n of t h e s e cance r s to h u m a n m o r b i d i t y a n d also p r o b a b l y by the r e l a t ive ease of o b t a i n i n g a n a l y z a b l e m i t o s e s u s i n g va r i ous m e t h o d s of t u m o r p rocess - ing, c u l t u r i n g , a n d c h r o m o s o m e ha r ve s t i ng . Neve r the l e s s , as for o the r c a r c i n o m a s , t he q u a l i t y of c h r o m o s o m e b a n d i n g a n d the f r e q u e n t c o m p l e x i t y of the k a r y o t y p e s led to v a r i o u s i n t e r p r e t a t i o n s [1 -6 ] , a n d no s ing le cy togene t i c a n o m a l y ha s b e e n c o n s i s t e n t l y a s s o c i a t e d w i t h th i s t u m o r type. A n o n r a n d o m i n v o l v e m e n t of c h r o m o - s o m e s 17 a n d 18 w as first d e s c r i b e d in 1985 in s a m p l e s of 11 t u m o r s [7] a n d was f u r t h e r c o n f i r m e d in a larger ser ies [8]. It is s u r p r i s i n g t ha t the i n v o l v e m e n t of t h e s e
From the Departments of Biology (M. M., B. D.) and Surgery (R.-J. S.), Institut Curie, Paris, France.
Address reprint requests to: Martine Muleris, M.D., Structure et Mutagenese Chromosom- iques, C.N.R.S. URA 620, Institut Curie, Section de Biologie, 26 rue d'Ulm, 75231 Paris C~dex 05, France.
Received November 20, 1989; revision accepted December 8, 1989.
143
~ 1990 Elsevier Science Publishing Co., Inc. Cancer Genet Cytogenet 46:143 156 (1990} 655 Avenue of the Americas, New York, NY 10010 0165-4608/90/$03.50

144 M. M u l e r i s et al.
c h r o m o s o m e s , f o u n d w i t h s u c h r egu la r i t y s i nc e then , h a d b e e n r e po r t e d o n l y occa-
s i o n a l l y by o t h e r i nves t i ga to r s . In seve ra l p u b l i s h e d cases , h o w e v e r , one of the chro-
m o s o m e s 17 a p p e a r e d to h a v e b e e n lost, a n d s t r u c t u r a l l y r e a r r a n g e d c h r o m o s o m e s
17 m a y h a v e b e e n h i d d e n a m o n g u n i d e n t i f i e d ma rke r s . Loss of c h r o m o s o m e 18 h a d
a lso b e e n n o t i c e d [3]. We n o w h a v e s t u d i e d a se r ies of 100 cases , w h i c h e n a b l e s u s
to p r o p o s e s o m e of the m a i n c y t o g e n e t i c cha r a c t e r i s t i c s of t h e s e t u m o r s .
T h e M o s t R e c u r r e n t C h r o m o s o m a l A n o m a l i e s
W h e n w e b e g a n th i s r e s ea r ch , we e x p e c t e d to f ind one (or more) t u m o r - a s s o c i a t e d
c h r o m o s o m a l t r a n s l o c a t i o n ( s ) w h i c h w o u l d h a v e f o c u s e d s t u d i e s on the u n d e r l y i n g
m o l e c u l a r m e c h a n i s m of t h e s e defec ts , as d e s c r i b e d in v a r i o u s h e m a t o l o g i c m a l i g n a n -
cies. It b e c a m e r a p i d l y o b v i o u s , h o w e v e r , t ha t no " s p e c i f i c " s t r u c t u r a l c h a n g e occu r -
red in co lo rec t a l c a r c i n o m a s , as is p r o b a b l y the case in m o s t t y p e s of so l id t u m o r s .
N e v e r t h e l e s s , n o n r a n d o m c h r o m o s o m a l c h a n g e s c o u l d be d e m o n s t r a t e d , the m o s t
f r e q u e n t o n e s a f fec t ing c h r o m o s o m e s 17 a n d 18 [8].
T a b l e I F r e q u e n c y of the m o s t r e c u r r e n t c h r o m o s o m a l
a n o m a l i e s o b s e r v e d in ou r se r ies of 100 co lorec ta l
Chromosome Mean MD General imbalances MD MP and MP TT lnean
Tumor types
del(1)(p3) 61 74 69 18 53 4q 43 74 61 4 44
del(5)(q2] 32 78 60 18 47 6q 18 52 38 0 27
+ 7 21 17 19 86 33 - 8 p 61 70 66 18 51 + 8q 50 30 38 54 40 - 9 q 7 70 45 9 33 del(10)(q2) 32 87 65 14 49
11 18 52 38 4 28 +12 4 4 4 64 17 + 13 46 48 47 77 51 - 1 4 39 83 65 0 47
15 36 74 59 0 42 - 1 7 p 100 100 100 27 76 - 1 8 100 100 100 32 78 + 20 46 35 39 68 43 - 2 1 14 91 60 9 44 - 2 2 29 61 48 4 35 + Xe, F 42 56 50 62 43 + X ,M 60 85 74 62 59 - X I , F 17 87 57 25 41
- Y 40 85 65 37 49 No. of cases 28 42 70 22 100
Any anomaly whose frequency was >50% in one tumor type is shown. Anomalies of X chromosomes in female patients were estimated in the subset of tumors studied with BrdU incorporation to differentiate the early from the late replicating X (Xe and XI, respectively}.
Abbreviations: MD = monosomic diploid; MP - monosomic polyploid; TT - trisomic- type tumors (see text for definitions}.
t u m o r s

Cytogenetics of Colorectal Adenocarc inomas 145
In the present series, chromosome 17 was involved in a structural rearrangement in about 76% of cases. A detai led analysis showed that the breakpoints are located between the proximal part of the long arm and probably the middle of the short arm. Because most of these breakpoints lie in const i tut ive heterochromatin, the deregula- t ion of a s tructural gene of chromosome 17 because of the rearrangement cannot be suspected. The observed rearrangements are various: i sochromosomes i(17q), unbal- anced t ranslocat ions wi th various other chromosomes t(17q;other), or part ial delet ions wi th in the short arm del(17p). Some recurrences in the rearrangements were ob- served, with the fol lowing derivative chromosome 17 found in several cases: i(17q) (20 cases), der(8q17q) (seven cases), and der(4q17q), der(13q17q), der(14q17q), and der(17q22q) (two cases each). Whatever the rearrangement, it always leads to a total or, more rarely, part ial loss of the short arm. Loss of one chromosome 18 affected the entire chromosome in 71% of cases and only part of it in 7%.
The other most recurrent anomalies are shown in Table 1. When data of all tumors are pooled, most of the recurrent changes are whole chromosome losses or deletions. The relative frequencies of these anomalies are of little significance, however, because it appears that only the way in which they are associated is of significance. Indeed, the combinat ions of the chromosomal changes related to the mean number of chromo- somes in the tumors led us to define three types of tumors with abnormal karyotypes.
Cytogenetic Classification of Colorectal Carcinomas
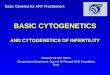
Monosomic near-diploid tumors. In 28 of 100 tumors, the chromosome numbers ranged between 41 and 49, wi th a mean value of 44.18 -+ 1.97 and a mode at 44 (Fig. 1). Indeed, we character ized these hypod ip lo id tumors more accurately by the s imul taneous loss of one chromosome 18 and of the short arm of one chromosome 17. When both these anomalies were present, other imbalances were recurrent ly associated in decreasing order of frequency: del(1)(p3) and - 8p; + X (in males); + 8q; + 13 and + 20; - 4q; + early repl icat ing X (Xe, in females); - Y; - 14; - 15; del(5)(q2) and del(lO)(q2) (Table 1). Because most of the observed al terat ions were losses or delet ions of chromosomes, these tumors were called "monosomic , " al though some chromosomes or chromosome segments may also have been dupl icated. In the major- ity of these tumors (68%), one or several minor der ived po lyp lo id subclones were observed beside the near -d ip lo id stemline.
Monosomic polyploid tumors. Monosomic po lyp lo id tumors (42 tumors) are more heterogeneous than MD tumors, as reflected by the great variat ion in their chromosome numbers from 58 to 129, with a mean value around t r ip lo idy (mean, 73.06 --- 3.61) (Fig. 1). A high intra tumoral heterogeneity of the karyotypes was also observed. Both a rearrangement of chromosome 17 leading to loss of its short arm and a deficiency for chromosome 18 were always found. The latter could be less obvious than in near- d ip lo id tumors because it was expressed only by a relative deficiency of chromosome 18, which was under represen ted as compared with the mean number of other chromo- somes. The associated recurrent anomalies were, in decreasing order of frequency: -21; del(10)(q2) and - late repl icat ing X (XI, in females); - Y and + Xe (in males); - 1 4 ; del(5)(q2); del(1)(p3), - 4 q and - 1 5 (Table 1). This pat tern of chromosome losses and gains is very s imilar to that of MD tumors. A correlated molecular and cytogenetic s tudy indica ted that MP tumors first developed as MD tumors before undergoing an endoredupl ica t ion , fol lowed by further losses of chromosomes and dele t ions wi th a comple te d isappearance of the original MD clone [9].

0 0 .8
Z
s 4 3 2 1 0 15
14
13
12
11
10 9 8
41
46
50
55
60
65
70
75
80
85 C
hro
mo
som
e n
um
ber
Fig
ure
1
Dis
trib
uti
on
of
the
100
colo
rect
al t
um
ors
acc
ord
ing
to
thei
r ch
rom
oso
me
nu
mb
ers.
Hat
ched
bar
s =
m
on
oso
mic
dip
loid
(M
D)
tum
ors
, li
ght
gray
ba
rs =
mo
no
som
ic p
oly
plo
id (
MP)
tu
mo
rs,
dark
gra
y ba
rs =
tri
som
icot
ype
(TT
) tu
mo
rs,
blac
k ba
rs =
no
rmal
kar
yo
typ
e (N
T)
tum
ors
, o
pen
bar
= t
um
or
that
co
uld
no
t be
cla
ssif
ied
in a
ny
of
the
cate
gori
es.

Cytogenetics of Colorectal Adenocarc inomas 147
Trisomic tumors, The chromosome numbers of the 22 TT tumors ranged from 47 to 58, wi th a mean value of 51.01 -+ 3.61 and a mode at 50 (Fig. 1). In contrast to the previous types, these tumors did not lose both chromosomes 17p and 18, but had a rearrangement of chromosome 17 or a loss of one chromosome 18 or none of these changes. Because most of the anomalies were gains of entire chromosomes, these tumors were cal led " t r isomic," al though some chromosome losses may also occur. The most recurrent changes were, in decreasing order of frequency: + 7, + 13, + 20, +12, +Xe, and + 8 q (Table 1). Figure 2 shows the main differences between the chromosomal pat tern of TT and MD tumors: the gains affecting chromosomes 7 and 12, never found in MD tumors, are very recurrent in TT tumors, whereas losses of chromosomes lp , 4, 8p, 10q, 14, 15, 17p, and 18, very frequent in MD tumors, are observed more rarely in TT tumors. Gains of chromosomes 8q, 13, 20, and Xe are found in both types. Polyplo id s idel ines are never observed in these tumors, indicat ing that they do not undergo endoredupl ica t ion .
Tumors with normal karyotypes. The finding of normal karyotypes in colorectal tumors is not except ional since seven such tumors in 100 cases were found in our series and three in 31 cases were reported by Reichmann et al. [10]. The finding of normal karyotypes raised the question of whether they represent cancerous cells or contaminat ing stromal or inf lammatory cells. In our study, flow cytometry was performed on tumor biopsies from all seven patients and always showed a DNA index of 1, which indicates that the karyotyped cells were malignant. These tumors were observed in pat ients whose mean age (57 +- 16 years) was lower than the average age of the other pat ients (64 +- 12 years) and occurred more frequently than the other tumors in the right colon (four of seven versus 10 of 92). Thus, they consti tute a separate category.
Atypical tumors. The 100 tumors s tudied were dis t r ibuted among the different cate- gories defined above. This classification could be easily appl ied to most cases, al- though seven remained atypical . Among the 28 MD tumors, three differed by a two- step chromosomal evolut ion, first losing chromosomes or chromosomal segments as MD tumors and secondar i ly dupl ica t ing some chromosomes as TT tumors. A fourth tumor was character ized by a loss of 17p in a minor clone only, and a fifth one was character ized by the presence of two normal chromosomes 17, al though molecular data demonst ra ted a loss of heterozygosi ty for 17p (unpubl ished observations). Among the 42 MP tumors, one previously reported [9] fol lowed a monosomic- type evolut ion before endoredup l ica t ion and a t r isomic-type evolut ion afterward. Last, one tumor could not be classified in any of the categories.
Correlations With Anatomoclinical Data
The 100 tumor samples were obtained by biopsy or as surgical specimens from 95 pat ients (mean age 64 -+ 13 years; range 29-89 years, 67% females) and inc luded 91 sporadic carcinomas from 87 patients (four of them had two synchronous tumors wi th different locat ions and karyotypes), five tumors from five pat ients with familial adenomatous polypos is (FAP), and four tumors from three patients with the Lynch syndrome (one of them had two metachronous tumors, both with normal karyotypes). In three patients, one of which was previously reported [11], a local recurrence or metastasis could be s tudied and a karyotype ident ical or s imilar to that of the pr imary tumor was found. Among these 100 tumors, 14 are located in the proximal colon, 42 are located in the distal colon, and 44 are located in the rectum.
Subgroups of tumors classified according to the chromosomal types MD, MP, TT, and NT as defined above do not differ significantly with respect to Dukes' stage. The

1 4 8
0
_ w
A w
0
0
Ii)
0
0
I
A I w
I
i 0 I
C ¢ I
0 I
O ¢ I
0 J I I
.k "r"
I
!
.k
I
© T
C ¢
o--, © ,.
I
A w
A w
i O w
: _' : _' : _. _. : : : : : : :
~ . W. el. ~ . ~ ,~. W. ~ ~ . ~ '~. W. el. ~ .
IIOa / so!doa j o aoqumu tre9tu
v~
• ~ o E
e,,i
E
~ cv
© (j
0 ( J c O
¢",1

Cytogenetics of Colorectal Adenocarc inomas 149
22.
19. 18- 17. 16. 15. 14. 13. 12. 11,
O, proximal
colon
a
34 32 30 28
~ 26 O 24 .~ 22
20
Z 16 14 12 10
8
h ' 4 2 0
distal rectum colon
~roximal colon
i!i!~!! distal colon
b
i rectum
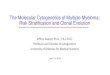
Figure 3 (a) Distribution of the colorectal tumors according to tumor site. Hatched bars = monosomic diploid (MD) tumors, light gray bars - monosomic polyploid (MP) tumors, dark gray bars = trisomic-type (TT) tumors, black bars = normal karyotype (NT) tumors. (b) Occurrence of endoreduplication in relation to tumor site. Tumors with endoreduplication (+) include MD tumors with a polyploid subcloue and MP tumors. Tumors without endoreduplication ( - ) include MD tumors with no detected polyploid clone, TT, and NT tumors. The tumors were classified as proximal (from cecum to splenic flexure), distal (from splenic flexure to the end of the sigmoid), and rectal.
results of the comparison of the frequencies of MD, MP, TT, and NT tumors with respect to the site of the tumor within the colon are as follows (Figure 3a). First, the distributions of MD and MP tumors by tumor site do not differ. Second, about 90% of MD and MP tumors are found in the distal or rectal locations. Third, the distribution of monosomic- type (MD + MP) and TT tumors was significantly different, with a lack of TT tumors in the distal colon (chi square = 9.91, v = 2, p < 0.01). Fourth, when tumors with normal (NT) and abnormal karyotypes were compared, a significant excess of NT was found in the proximal colon (chi square = 11.69, v = 2, p < 0.005). This finding must be combined with the finding of Reichmann et al., who reported the presence of three tumors with normal karyotypes in the proximal colon [10]. Molecular data on allelic losses for chromosomes 17p, 18, and 5 in relation to tumor site are in agreement with our results [12]. When the occurrence of endoredupl icat ion was correlated with tumor location (Fig. 3b), there was a nonrandom distribution resulting from an excess of endoredupl icat ion in the distal colon (chi square -- 13.55, v -- 2, p < 0.005). This is largely but not exclusively related to the abovement ioned lack of TT and NT tumors in the distal colon, since these tumors do not undergo endoreduplicat ion. The various tumor types (MD, MP, TT, and NT) were observed in patients with FAP or Lynch syndrome.
Structura l R e a r r a n g e m e n t s
Quantitative analysis. Statistical analysis of the chromosomal anomalies was compli- cated by the presence of several subclones with different but related karyotypes wi thin the same tumor. To overcome this difficulty, for each tumor we took into considerat ion

1 5 0 M. M u l e r i s et al,
Table 2 M e a n n u m b e r of r e a r r a n g e m e n t s pe r t u m o r
MD tumors TT tumors MP tumors
Types of Before rearrange- endore- ments Mini Maxi Mini Maxi duplication Mini Maxi
del 1.15 1.45 .68 .68 .7 .95 1.4 i .7 .85 .41 .77 1.05 1.4 1.45 rcp .2 .2 .09 .14 0 0 0 rob .25 .25 .05 .05 .05 .15 .2 inv .05 .05 .05 .05 .05 .05 .05 der, rea 2.85 3.3 1.23 1.68 2.15 3.55 4.45 + mar, + rain .95 1.05 .27 .36 .1 .4 .5 Total(SD) 6.15 (3.92) 7.15 (3.83) 2.78 (3.42) 3.73 (3.71) 4.1 (1.54} 6.5 (2.48) 8.05 (2.78) No. of cases 20 22 20
For each type of tumor, the values found in the simplest (mini) and most comple× clone (maxi) are shown. In addition. in MP tumors we differentiated the rearrangements that occurred before endnreduplication.
Abbreviations: MD - monosolnic diploid: MP - mollosomic polyploid: TT trisomic-type tumors; del deletion; i = isochromosome; rcp = reciprocal translocation: rob = Robertsonian translocation; inv inversion; der = derivative chromosonle; rea = rearranged chromosome: mar marker; rain minute: SD standard deviation.
the n u m b e r of r e a r r a n g e m e n t s o b s e r v e d in the s i m p l e s t c l o n e a n d the n u m b e r o b s e r v e d in t he m o s t c o m p l e x c lone . In a d d i t i o n , for M P t u m o r s we t r i ed to r e c o n s t r u c t t he c h r o m o s o m a l e v o l u t i o n of e a c h t u m o r a n d to date the o c c u r r e n c e of the a n o m a l i e s in r e l a t i o n to t he e n d o r e d u p l i c a t i o n p roces s a c c o r d i n g to a m e t h o d p r e v i o u s l y d e s c r i b e d [9]. T h i s a l l o w e d us to d i f f e ren t i a t e the c h a n g e s t ha t o c c u r r e d before a n d af ter the e n d o r e d u p l i c a t i o n a n d a m o n g the la t ter to d i s t i n g u i s h those c o m m o n to all ce l ls f r om the la te o c c u r r i n g c h a n g e s t ha t d i f fe red f rom s ide l ine to s ide l ine. Data o b t a i n e d f rom 20 to 22 t u m o r s of e a c h type, s e l ec t ed for the qua l i t y of the c h r o m o s o m e b a n d i n g , are s h o w n in Tab le 2. O n the average, the n u m b e r of s t ruc tu ra l r e a r r a n g e m e n t s pe r t u m o r is s ign i f i can t ly l o w e r in TT t u m o r s (2.78 in the s i m p l e s t c l o n e to 3.73 in the m o s t r e a r r a n g e d c lone) t h a n in MD (6 .15-7 .15) ( S t u d e n t ' s t tes t p < 0.05) or M P t u m o r s (6 .5 -8 .05 ) ( S t u d e n t ' s t tes t p < 0.01). In MP tumor s , the re is a n ave rage of s ix r e a r r a n g e m e n t s pe r t u m o r c o m m o n to all c lones , a m o n g w h i c h o n l y 4.1 o c c u r r e d before e n d o r e d u p l i c a t i o n .
W e c o n c l u d e t h a t t he leve l of c h r o m o s o m a l m u t a g e n e s i s is two- to t h r e e f o l d h i g h e r in MD a n d M P t u m o r s t h a n in TT t um or s . C o m p a r i s o n b e t w e e n MD a n d TT t u m o r s s h o w s t ha t the leve l of m u t a g e n e s i s is no t p r o p o r t i o n a l to the n u m b e r of c h r o m o s o m e s . B e c a u s e we c o n s i d e r e d the r e a r r a n g e m e n t s as such , a n d no t the c h r o m o s o m e s gener - a ted by t he r e a r r a n g e m e n t s , t he da ta of Tab le 2 do no t ref lect the n u m b e r of r e a r r a n g e d c h r o m o s o m e s p rec i se ly .
Qualitative analysis. Data s h o w n in Tab le 2 a l l ow the f o l l o w i n g obse rva t i ons .
1. T h e d i s t r i b u t i o n s of the d i f f e ren t types of r e a r r a n g e m e n t s are s i m i l a r in the t h r e e t ypes of t u m o r s .
2. B a l a n c e d r e a r r a n g e m e n t s (rcp, inv) are ve ry rare, c o n s t i t u t i n g less t h a n 5% of all r e a r r a n g e m e n t s . De l e t i ons r e p r e s e n t a b o u t 20% of the r e a r r a n g e m e n t s , w h i c h m a y be o v e r e s t i m a t e d b e c a u s e a p r o p o r t i o n of t h e m m a y r e su l t f rom u n b a l a n c e d t r ans lo - ca t ions . I s o c h r o m o s o m e s c o n s t i t u t e 1 0 % - 2 0 % of the s t ruc tu ra l changes , a n d un - b a l a n c e d r e a r r a n g e m e n t s r e v e a l e d by the p r e s e n c e of d e r i v a t i v e c h r o m o s o m e s , s o m e t i m e s u n c o m p l e t e l y i den t i f i ed (der, rea, mar , ra in) are ve ry f r e q u e n t (60%).

Cytogenetics of Colorectal Adenocarcinomas 151
3. The high frequency and the type of the unbalanced rearrangements observed provide information on the possible mechanism of their formation. They may originate either from a balanced rearrangement with further loss of one derivative chromosome, indicating involvement of a prereplicative (G1) mechanism, or from a rearrangement that leads to an imbalance such as a chromatid exchange during the postreplicative phase (S-G2) of the cell cycle. The high frequency of isochromo- somes and the very low frequency of reciprocal translocations suggest that these rearrangements preferentially occur in the S-G2 phase, which could also be in accordance with the occasional observation of radials.
4. Although the different types of rearrangements are equally distributed in MD and TT tumors, the consequences of the structural changes in terms of chromosomal imbalances are quite different. Formation of the derivative chromosomes generally leads to a loss of material in MD tumors and to a gain in TT tumors, which suggests that the tumors have selected the derivative chromosome differently. This selection could have occurred immediately after the rearrangement in case of a chromatid exchange or more or less at a distance in case of a balanced rearrangement. Because the various combinations of segregation of a rearrangement never coexist in a tumor, a rapid mechanism of selection and therefore a postreplicative rearrange- ment is more likely.
Breakpoints analysis. Breakpoints are not randomly distributed and only the main conclusions are presented as previously reported [7, 13]. Most of the breakpoints are located in the juxtacentromeric heterochromatin, especially of chromosomes 1, 8, 13, and 17. Even for chromosome 17, however, which is very frequently rearranged, C- banding showed that breakpoints vary from the proximal part of the short arm to the proximal part of the long arm. Recurrent breakpoints in euchromatin are rare. Only chromosomes lp, 5q, 'and 10q were recurrently affected by interstitial deletions, and although these deletions can involve the same common region in all tumors (lp3, 5q2, and 10q22- q24), the breakpoints were variable.
Comparison of Molecular and Cytogenetic Data
Losses of individual chromosomal regions can be investigated by two independent approaches: cytogenetic and molecular. In the latter, the patient's constitutional and tumor DNA are compared by restriction fragment length polymorphism (RFLP) analy- sis to seek eventual allelic losses in tumor cells. Because methodologies and possible artifacts differ according to the approach, we wished to compare the two sets of data (Table 3). For this purpose, we selected the chromosome arms most frequently involved in deletions or losses in our series of 100 tumors for which allelic losses were reported in the literature. For cytogenetic data, two values are given. The highest one is that indicated in Table 1, which includes all 100 tumors; the other takes into account the possible misinterpretations in polyploid tumors in which a single loss before endoreduplication which should lead to allelic loss cannot always be distin- guished from two consecutive losses after endoreduplication, which may preserve heterozygosity. Thus, in the second estimate, because MP are derived from MD, we have considered for the whole group of monosomic tumors (MP and MD) only the frequencies of losses observed in MD tumors, which gives the lowest value. Molecular data were separated into two categories depending on whether studies were performed after physical or biological purification of the tumor samples [14-17] or not [18-20]. The comparison of these two sets of data leads to the following conclusions:
1. Within the molecular data, the frequency of allelic loss for an individual chromo- somal region was generally the highest in studies that involved DNA purification.

152
T a b l e 3 C o m p a r i s o n b e t w e e n m o l e c u l a r a n d c y t o g e n e t i c d a t a
No. of Allelic losses (%) C h r o m o s o m e informat ive a rm Reference t umor s a b
C h r o m o s o m e dele t ions or losses (%)
l p [18] 15 0 47 .5 -53 [14] 36 15 [19] 23 9 [15] 23 9
4q [18] 5 0 3 1 - 4 4 [14] 20 10 [19] 9 0
5q [14] 55 38 27 .5 -47 [16] 31 19 [2O] 44 27
6q [14] 31 32 12 .5 -27 8p [14] 22 50 47 .5 -51 9q [18] 6 0 7 -33
[14] 39 27 [19] 16 0
10q [18] 3 0 25 .5 -49 [14] 37 15
11p [18] 10 0 13 .5 -28 [14] 33 17 [19] 19 O [15] 25 12 [20] 19 0
11q [14] 28 16 13 .5 -28 [19] 6 0
14 [18] 10 30 28 .5 -47 [14] 5O 20 [19] 24 8
15 [18] 8 0 2 6 - 4 2 [14] 24 12 [19] 20 5
17p [14] 56 80 76 [19] 19 37 [15] 33 76 [16] 34 56 [20] 15 O [17] 15 73
18p [14] 27 45 71 [19] 5 0 [16] 7 43 [17] 16 87
18q [14] 53 77 78 [16] 33 52 [17] 5 80
21q [18] 6 0 1 2 - 4 4 [14] 27 22 [19] 11 0
22q [18] 21 19 21 -35 [14] 41 30 [16] 33 0
For cytogenetic data, two values are given: the highest is the general mean indicated in Table 1, and the lowest takes into consideration the possible misinterpretations in monosomic polyploid tumors (see text for explanations). Molecular data are separated into two categories depending on whether studies were performed after purification of tumor samples (b) or not (a).

Cytogenetics of Colorectal Adenocarc inomas 15 3
This was expected since colorectal tumors contain variable percentages of nonneo- plast ic cells that can mask allelic delet ions occurring wi thin tumor cell popula- tions.
2. Even after DNA purification, the frequencies of allelic losses are lower than the lowest frequencies of delet ions detected by cytogenetics, on the average.
3. For the chromosomes well known to be involved in colon cancer (5q, 17q, and 18), molecular and cytogenetic data are remarkably comparable.
That the frequencies of allelic losses are generally lower than the frequencies of cytogenetic dele t ions is surpris ing because small delet ions would be expected to be more readi ly detected by a molecular approach. This may indicate that for most chromosomes delet ions are fairly large and that the molecular probes used are distant from the involved chromosomal segment. Another interpretat ion is that for a number of chromosomes losses may occur late and affect either maternal or paternal homo- logues in the same tumor. This could be related to the fact that MP tumors, presumed to have a longer evolut ion than MD tumors from which they derive, have higher percentages of chromosome losses than MD tumors (Table 1) and thus would accumu- late delet ions wi thout al lel ic losses. If this interpretat ion is correct, we could conclude that delet ions play a part not only in allelic losses, but also in gene dosage modifica- tions.
Possible Biological Meaning of Chromosomal Anomalies
Loss of chromosome 17p. The frequent loss of 17p is the best documented chromo- somal anomaly. An enhanced expression of gene p53 localized on human chromo- some 17p13 [21] was descr ibed in about 44-55% of colorectal cancers [22-24] which appears to be in contradic t ion to loss of the p arm of chromosome 17. Al though the gene encoding p53 was usual ly considered an oncogene, the normal p53 gene was recent ly suggested to have a tumor suppressor activity [25]. This tumor suppressor act ivi ty would be rel ieved by mutat ions of p53 gene, and the effect should be enhanced by the loss of the normal allele. Recently, mutat ions of p53 gene were observed in two colorectal cancers [26]. Al though these data need confirmation, they suggest that p53 gene may be involved in colorectal neoplasia, perhaps through mutat ions result ing in inact ivat ion of a tumor suppressor function of the normal p53 gene and loss of the normal al lele due to a rearrangement of chromosome 17.
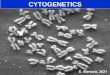
Other chromosomal anomalies. The biological meaning of chromosomal anomalies can be mult iple , and their in terpreta t ion is ambiguous. We first discuss the mechanis- tic aspects, using chromosome 8 as an example. The chromosomal combinat ions resul t ing from the various anomalies of chromosome 8 observed in MD and TT tumors are shown in Figure 4. The observed chromosomal changes comprised numerica l anomalies which consis ted of the gain of one or two copies of chromosome 8 and structural rearrangements. In TT tumors, gains and rearrangements were equal ly represented, whereas in MD tumors rearrangements were the most frequent (85%). Rearrangements were always unbalanced, involving a breakpoint in the centromeric heterochromatin , and resul t ing in a decrease of the 8p/8q ratio. When MD and TT tumors were compared, the mechanism leading to this imbalance appeared to be different, because it resul ted pr inc ipa l ly from gain of the long arm in TT and loss of the short arm in MD tumors. When structural and numerica l anomalies were pooled, the difference remained: the gain of 8q was more frequent in TT than in MD (100% versus 75%), whereas the loss of 8p is more frequent in MD tumors (85% versus 33%). As shown in Figure 4, many of these different chromosomal combinat ions result in

154 M. Muleris et al.
structural rearrangements
tt tt °rlt llt°rttt a b c d
numerical anomalies
1tt tttt°rtttt e f
MD 60% 25% 0% 0% 15% 0%
TT 33% 0% 8% 8% 42% 8%
8p / 8q 1/3 I/2 2/3 2/4 3/3 4/4
8Pl /8P2 1/0 1/0 1/1 or 2/0 1/1 or 2/0 1/2 1/3 or 2/2
Figure 4 Schema of the chromosomal combinations (a-f) resulting from the various structural and numerical anomalies of chromosmne 8 observed in 20 monosomic diploid (MD) and 12 trisomic-type (TT) tumors. (a) one chromosome 8 is replaced by an i(Sq); (b) one chromosome 8 underwent an unbalanced rearrangement leading to the loss of the short arm; (c} same as (b) with an additional chromosome 8; (d) same as {a) with an additional chromosome 8; (e) gain of one chromosome 8; (f) gain of two copies of chromosome 8. Numbers 1 and 2 indicate the different parental homologues (light gray and dark gray), respectively. For each combination, the frequency of occurrence is given for MD and TT tumors, with the resulting 8p/8q ratio and 8pl/8p2 ratio for the expected imbalance between the parental alleles 1 and 2. The combinations that would result from the unlikely occurrence of repeated missegregations leading to the presence of three or four copies of the same parental homologue are not represented.
imbalances between maternal and paternal alleles to various extents: hemizygosity for the short arm of chromosome 8 is expected in 85% of MD tumors, whereas it would affect 33-49% of TT tumors only. In the other cases, except in the case of an unlikely occurrence of repeated missegregations which would lead to the presence of three or four copies of the same parental homologue, an allelic imbalance with a ratio 1 : 2 or 1 : 3 is more probable.
The hypothesis commonly proposed to explain the role of chromosome losses in tumorigenesis is that recessive tumor suppressor genes are involved: the observed chromosomal deletions would unmask recessive mutant allele(s) by the loss of the balancing wild-type homologue{s). In our example, we could hypothesize that such a gene is located on the short arm of chromosome 8, but this hypothesis, which accounts for the cases with hemizygosity, does not fit with those with an allelic imbalance because at least one copy of the wild-type homologue should be retained. Moreover, this model does not explain why all TT tumors gain 8q; an additional hypothesis is needed. Actually, the explanation of the observed anomalies of chromo- some 8 by the unmasking of a recessive tumor suppressor gene only appears to be a reducing hypothesis, and the same applies to the various chromosomal losses shown in Table 1.
Another interpretation is that these chromosomal anomalies are related to devia- tions of metabolic pathways. The simplest hypothesis is that chromosome anomalies

Cytogenetics of Colorectal Adenocarcinomas 1 5 5
are responsible for the metabolic perturbations by gene dosage effect: a gain or a loss of a chromosome segment would result in an increase or decrease in the transcription, respectively, and thus in activity of the enzymes coded by the genes located on these chromosome segments [27]. The activity of several enzymes involved in nucleotides synthesis were measured in a number of colorectal tumors and demonstrated that the relat ionships between the number of chromosomes and the activity of the correspond- ing enzymes in tumor cells was obviously not direct [28]. Although it could be masked by the numerous difficulties related to the study of fresh tumors, it is almost certain that a simple gene dosage effect can be excluded. If a relat ionship exists, it is more likely that the metabolic deviat ion occurs first and that chromosome segments are duplicated or deleted depending on whether they carry genes of the metabolic path- ways that are increased or decreased in the tumor. Thus, there could be a differential selection of the chromosome segments to obtain a better adjustment between the number of gene copies and the transcription and the enzyme activity. This was previously proposed for endometrial cancer [29]. In this hypothesis, a direct correla- tion with the number of gene copies is not expected, but chromosome gains and losses should follow increases or decreases of the enzyme activities. Even if we could not demonstrate this positively, such an interpretation does not contradict our data. This hypothesis and that of the unmasking of recessive tumor suppressor genes are not mutual ly exclusive, and the two processes could cooperate in chromosomal evolut ion of the tumor. The occurrence of chromosome gains or losses in relation to metabolic: constraints could even represent an active selective process leading to allelic imbal- ances or losses.
REFERENCES
1. Sonta S, Sandberg AA (1978): Chromosomes and causation of human cancer and leukemia. XXX. Banding studies of primary intestinal tumors. Cancer 41:164-173.
2. Reichmann A, Martin P, Levin B (1981): Chromosomal banding patterns in human large bowel cancer. Int J Cancer 28:431-440.
3. Couturier-Turpin MH, Couturier D, Nepveux P, Louvel A, Chapuis Y, Guerre J (1982): Human chromosome analysis in 24 cases of primary carcinoma of the large intestine: Contribution of the G-banding technique. Br J Cancer 46:856-868.
4. Ochi H, Takeuchi J, Holyoke D, Sandberg A (1983): Possible specific chromosome changes in large bowel cancer. Cancer Genet Cytogenet 10:121-122.
5. Levin B, Reichmann A (1986): Chromosomes and large bowel tumors. Cancer Genet Cyto- genet 19:159-162.
6. Pathak S, Goodacre A (1986): Specific chromosome anomalies and predisposition to human breast, renal cell, and colorectal carcinoma. Cancer Genet Cytogenet 19:29-36.
7. Muleris M, Salmon RJ, Zafrani B, Girodet J, Dutrillaux B (1985): Consistent deficiencies of chromosome 18 and of the short arm of chromosome 17 in eleven cases of human large bowel cancer: A possible recessive determinism. Ann Genet 28:206-213.
8. Muleris M, Salmon RJ, Dutrillaux AM, Viehl P, Zafrani B, Girodet J, Dutrillaux B (1987): Characteristic chromosomal imbalances in near-diploid colorectal tumors. Cancer Genet Cytogenet 29:289-301.
9. Muleris M, Delattre O, Olschwang S, Dutrillaux AM, Remvikos Y, Salmon RJ, Thomas G, Dutrillaux B (1990): Cytogenetic and molecular approaches of polyploidization in colorectal adenocarcinomas. Cancer Genet Cytogenet 44:107-118.
10. Reichmann A, Levin B, Martin P (1982): Human large bowel cancers: Correlation of clinical and histopathological features with banded chromosomes. Int J Cancer 29:625-629.
11. Muleris M, Salmon RJ, Dutrillaux B (1986): Chromosomal study demonstrating the clonal evolution and metastatic origin of a metachronous colorectal carcinoma. Int J Cancer 38:167-172.
12. Delattre O, Law DJ, Remvikos Y, Sastre X, Feinberg AP, Olschwang S, Melot T, Salmon RJ,

156 M. M u l e r i s et al.
Validire P, Thomas G (1989): Multiple genetic alterations in distal and proximal colorectal cancer. Lancet ii:353-356.
13. Muleris M, Salmon RJ, Dutrillaux B (1988): Existence of two distinct processes of chromo- somal evolution in near-diploid colorectal tumors. Cancer Genet Cytogenet 32:43-50.
14. Vogelstein B, Fearon ER, Kern SE, Hamilton SR, Preisinger AC, Nakamura Y, White R (1989): Allelotype of colorectal carcinomas. Science 244:207-211.
15. Fearon ER, Hamilton SR, Vogelstein B (1987): Clonal analysis of human colorectal tumors. Science 238:193-196.
16. Law DJ, Olschwang S, Monpezat JP, Lefranqois D, Jagelman D, Petrelli NI, Thomas G, Feinberg AP (1988): Concerted nonsynthenic allelic loss in human colorectal carcinoma. Science 241:961-965.
17. Monpezat JP, Delattre O, Bernard A, Grunwald D, Remvikos Y, Muleris M, Salmon RJ, Frelat G, Dutrillaux B, Thomas G (1988): Loss of alleles on chromosome 18 and on the short arm of chromosome 17 in polyploid colorectal carcinomas. Int J Cancer 41:404-408.
18. Sasaki M, Okamoto M, Sato C, Sugio K, Soejima JI, lwama T, Ikeuchi T, Tonomura A, Miyaki M, Sasazuki T (1989): Loss of constitutional heterozygosity in colorectal tumors from patients with familial polyposis coli and those with nonpolyposis colorectal carcinoma. Cancer Res 49:4402-4406.
19. Lothe RA, Nakamura Y, Woodward S, Gedde-Dahl T, White R (1988): VNTR (variable number of tandem repeats) markers show loss of chromosome 17p sequences in human colorectal carcinomas. Cytogenet Cell Genet 48:167-169.
20. Solomon E, Voss R, Hall V, Bodmer WF, Jass JR, Jeffreys AJ, Lucibello FC, Patel I, Rider SH (1987): Chromosome 5 allele loss in human colorectal carcinomas. Nature 328:616-619.
21. Isobe M, Emmanuel BS, Givol D, Oren M, Croce CM (1986): Localization of gene for human p53 tumor antigen to band 17p13. Nature 320:84-85.
22. Crawford LV, Pim DC, Lamb P (1984): The cellular protein p53 in human tumors. Mol Cell Med 2:261-272.
23. Van Den Berg FM, Tigges AJ, Schipper MEI, Den Hartog-Jager FCA, Kroes WGM, Walboomers JMM (1989): Expression of the nuclear oncogene p53 in colon tumours. J Patho1157:193-199.
24. Remvikos Y, Laurent-Puig P, Sahnon RJ, Frelat G, Dutrillaux B, Thomas G (1990): Simultane- ous monitoring of p53 protein and DNA content of colorectal adenocarcinomas by flow cytometry. Int J Cancer (in press).
25. Finlay CA, Hinds PW, Levine AJ (1989): The p53 protooncogene can act as a suppressor of transformation. Cell 57:1083-1093.
26. Baker SJ, Fearon ER, Nigro JM, Hamilton SR, Preisinger AC, Jessup JM, VanTuinen P, Ledbetter DH, Barker DF, Nakamura Y, White R, Vogelstein B (1989): Chromosome 17 deletions and p53 gene mutations in colorectal carcinomas. Science 244:217-221.
27. Dutrillaux B, Muleris M (1986): Induction of increased salvage pathways of nucleotide synthesis by dosage effect due to chromosome imbalances may be fundamental in carcino- genesis: The example of colorectal carcinoma. Ann Genet 29:11-15.
28. Luccioni C, Muleris M, Sabatier L, Dutrillaux B (1988): Chromosomal and enzymatic patterns provide evidence for two types of human colon cancers with abnormal nucleotide metabo- lism. Mutat Res 200:55-62.
29. Dutrillaux B, Couturier J (1986): Chromosome imbalances in endometrial adenocarcinomas: A possible adaptation to abnormal metabolic pathways. Ann Genet 29:76-81.