Embed Size (px)
Citation preview

In, J Kodmrmn Oncology Bml. Phw Vol. 9. pp 1961-1965 Prmted ,n the Ii S.A All rnghts reserved
0360 3016,‘83/$3.00 i 00 Copyrtghl ii 19X3 Pergamon Press L.td
??Magna- Field Symposium
CYCLIC, LOW-DOSE TOTAL BODY IRRADIATION FOR METASTATIC NEUROBLASTOMA
GIULIO J. D’ANGIO, M.D.' AND AUDREY E. EVANS, M.D.' ‘Professor of Radiation Therapy and Professor of Pediatric Oncology, ‘Professor of Pediatrics, Departments of Radiation Therapy and Pediatrics, University of Pennsylvania and the Children’s Cancer Research Center.
Children’s Hospital of Philadelphia, Philadelphia. PA
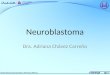
Total body irradiation (TBI) can be thought of as a systemic anticancer agent. It therefore might best be given like an adjuvant drug, i.e. in tolerable doses, cyclically. The therapeutic ratio between normal bone marrow stem cells and suitably sensitive cancer cells should be widened by these means. Fourteen children with advanced (Stage IV) neuroblastomas were given loo-150 rad TBI in 50 rad daily fractions along with each three-week cycle of standard triple-agent chemotherapy (vincristine, DTIC, cyclophosphamide). Two patients died of toxicity and one is still undergoing therapy. Four of the remaining 12 survive free of disease for 12+ to 31+ months. The regimen is well tolerated, but prolonged, pronounced hone marrow depression, especially thrombocytopenia, commonly occurs after doses of 300-450 rad.
Advanced neuroblastoma, Fractionated TBI, Cyclic TBl.
INTRODUCTION
The outlook for children with metastatic neuroblastoma has been poor, and remains so despite the advent of modern, multiagent chemotherapy. Two-year survival rates in the 1950’s and 60’s were less than 20%, and they remain at 25% or less according to recent studies con- ducted by the Children’s Cancer Study Group (CCSG),3,4 despite response rates in the 80% range. These results were obtained with the three drugs cyclophosphamide, DTIC, and vincristine with or without adriamycin.
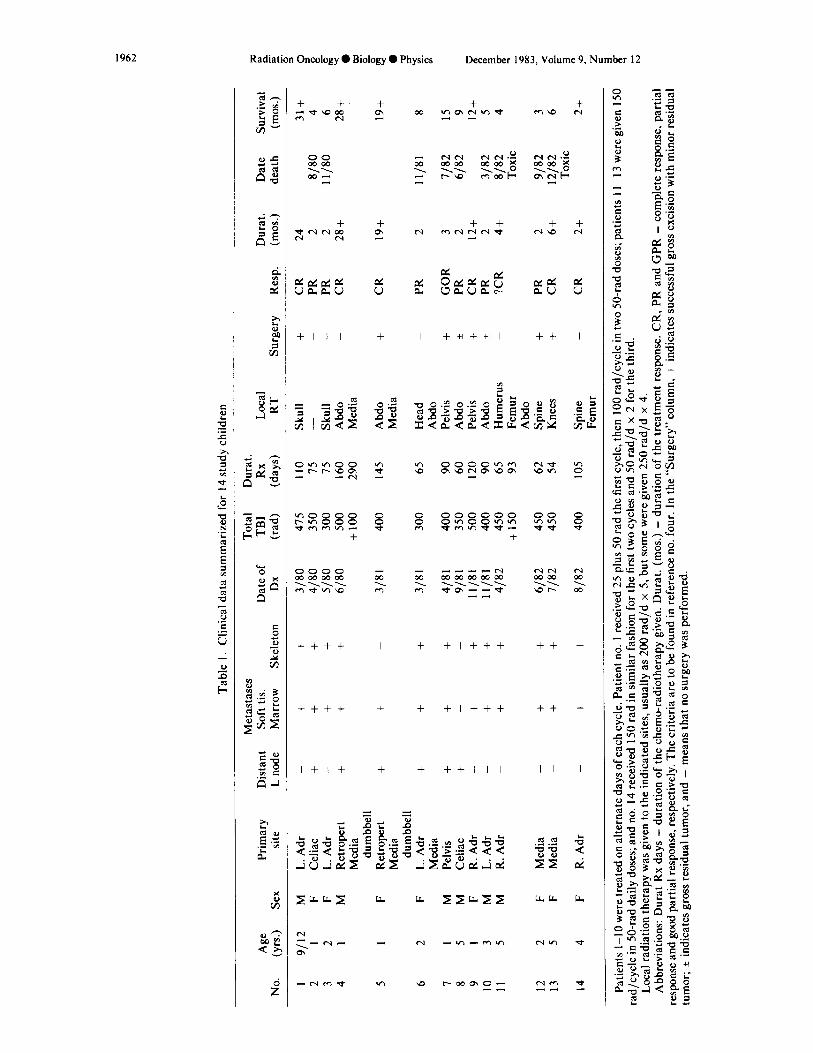
Neuroblastoma is sensitive to irradiation. Prompt responses are often achieved with modest doses; for example, 300 rad given in a single dose will initiate regression of masses and relieve pain. There is laboratory evidence to corroborate this clinical impression. Studies by Ohnuma et al.,” using human neuroblastoma in tissue culture, indicate that the neuroblastoma cell has little if any capacity for recovery, and that a dose of 260 rad will reduce the surviving fraction to 10%. Laboratory studies of bone marrow stem cells demonstrate them to be radiosensitive, but to have some capacity for recovery after low doses of irradiation.” It therefore was reasoned that low doses of total body irradiation (TBI) could exploit this potential, albeit small, therapeutic ratio.
Figure I provides an illustration of what might occur under such limited yet favorable circumstances. Accord- ing to this construct, low doses of TBI can be likened to a systemic chemotherapeutic agent and might improve therapeutic results if given like anti-cancer drugs, i.e. cyclically and for a protracted period. This approach is similar to that used by del Regato’ and by Osgood,” who used low-dose, cyclic TBI for the management of chronic leukemias in adults. It is different from that used by those who have employed TBI for the treatment of neuroblas- toma and other solid tumors. They have delivered TBI in single courses, a technique followed by others who have used TBI for non-Hodgkin’s lymphoma and leukemia.2.6.7 9.13.14
The preliminary results of a trial of low-dose, fraction- ated TBI given cyclically to children with advanced neuroblastoma are reported here. A literature search did not reveal any reports of the use of TBI in this fashion in patients with solid tumors.
METHODS AND MATERIALS
All patients with metastatic neuroblastoma (Stage IV) were eligible for entry into this pilot investigation. Four- teen such patients were seen consecutively at the Chil-
Presented at the 24th annual meeting of the American Society of Therapeutic Radiologists, October 1982, Orlando, FL.
This investigation was supported in part by U.S. Public Health Service grants nos. CA- 14489 and CA- I 1796, awarded by the National Cancer Institute, Department of Health and Human Resources.
Reprint requests to: G.J. D’Angio, M.D., Children’s Hospital
1961
of Philadelphia, 34th and Civic Center Blvd., Philadelphia, PA 19104. Acknowledgements-The authors thank Drs. R. Wimmer of St. Christopher’s Hospital for Children, Philadelphia, N. Hornback of Indiana University and S. Feig of the University of California at Los Angeles for their cooperation and assistance.
Accepted for publication 27 July 1983.
Tabl
e 1.
Clin
ical
da
ta
sum
mar
ized
fo
r 14
stu
dy
child
ren
No.
A
ge
(yrs
.) Se
x Pr
imar
y si
te
Met
asta
ses
Tota
l D
urat
. D
ista
nt
Soft
tis.
Dat
e of
TB
I R
x Lo
cal
Dur
at.
Dat
e Su
rviv
al
L no
de
Mar
row
Sk
elet
on
Dx
(rad
) (d
ays)
R
T Su
rger
y R
esp.
(m
os.)
deat
h (m
os.)
I 91
12
M
2 1
F 3
2 F
4 1
M
5 1
F
6 2
F
I 1
M
8 5
M
9 1
F IO
3
M
11
5 M
12
2 F
13
5 F
14
4 F
L. A
dr
Cel
iac
L. A
dr
Ret
rope
rt M
edia
du
mbb
ell
Ret
rope
rt M
edia
du
mbb
ell
L. A
dr
Med
ia
Pelv
is
Cel
iac
R.
Adr
L.
Adr
R
. A
dr
_ +
+ 31
80
+ +
+ 41
80
- +
+ 51
80
+ +
+ 61
80
+ +
_ 31
81
+ +
3/81
+ +
+ _
- +
_ + +
4181
9/
81
11/8
1 1 l
/81
4182
Med
ia
_ +
+ 61
82
Med
ia
_ +
t l/8
2
R.
Adr
_
+ +
8/82
415
350
300
500
+lO
O
400
300
400
350
500
400
450
+I50
450
450
400
110
Skul
l 15
-
15
Skul
l 16
0 A
bdo
290
Med
ia
145
Abd
o M
edia
65
90
60
120 90
65
93
62
54
105
Hea
d _
Abd
o Pe
lvis
+
Abd
o +
Pelv
is
+ A
bdo
f H
umer
us
Fem
ur
Abd
o Sp
ine
+ K
nees
+
Spin
e +
Fem
ur
+ _ - _ +
CR
24
PR
2
PR
2 C
R
28+
8180
1 l
/80
31+ 4 6 28+
CR
19
+ 19
+
PR
2 1 l
/81
8
GO
R
3 PR
2
CR
12
+ PR
2
?CR
4+
7182
61
82
3182
81
82
Toxi
c
15 9 12+ 5 4
PR
2 C
R
6+
9182
12
182
Toxi
c
3 6
CR
2+
2+
Patie
nts
I-10
w
ere
treat
ed
on a
ltern
ate
days
of
eac
h cy
cle.
Pa
tient
no
. 1
rece
ived
25
plu
s 50
rad
the
firs
t cy
cle,
th
en
100
rad/
cycl
e in
tw
o 50
-rad
do
ses;
pa
tient
s 1 t
-13
wer
e gi
ven
150
rad/
cycl
e in
50-
rad
daily
do
ses;
an
d no
. 14
rec
eive
d 15
0 ra
d in
sim
ilar
fash
ion
for
the
first
tw
o cy
cles
an
d 50
rad
/d
x 2
for
the
third
. Lo
cal
radi
atio
n th
erap
y w
as g
iven
to
the
in
dica
ted
site
s, us
ually
as
200
rad
/d
x 5,
but
som
e w
ere
give
n 25
0 ra
d/d
x 4.
A
bbre
viat
ions
: D
urat
R
x da
ys
= du
ratio
n of
the
ch
emo-
radi
othe
rapy
gi
ven.
D
urat
. (m
os.)
= du
ratio
n of
the
tre
atm
ent
resp
onse
. C
R,
PR
and
GPR
=
com
plet
e re
spon
se,
parti
al
resp
onse
an
d go
od p
artia
l re
spon
se,
resp
ectiv
ely.
Th
e cr
iteria
ar
e to
be
foun
d in
ref
eren
ce
no.
four
. In
the
“S
urge
ry”
colu
mn,
+
indi
cate
s su
cces
sful
gr
oss
exci
sion
w
ith
min
or
resi
dual
tu
mor
; +
indi
cate
s gr
oss
resi
dual
tu
mor
, an
d -
mea
ns
that
no
sur
gery
w
as p
erfo
rmed
.
Low dose TBI for metastatic neuroblastoma 0 G.J. D’ANGIO AND A.E. EVANS 1963
1.0
0.9
0.8
0.7
50 100 150 200 250 rod
0.6
0.5
g 0.4
F:
Y K
LL :
0.3
5
z z!
0.2
0.1
\ \ \
i
\ \
Jlx200 --- NBL \
Do=113 fad \ n=l \
\
- Bhl Do = IO0 rod n= 1.65
Fig. 1. Illustrative single and multiple dose survival curves for human neuroblastoma cells and murine bone marrow stem cells, derived from references 10 and 11. These curves are only meant to demonstrate the advantages of multiple small doses in cell systems with favorably different n and Do characteristics, and the disadvantages of larger fractions. For the two cell types shown, doses of >200 rad result in higher cell kill for the normal than for the tumor cells.
CELL SURVIVAL BY DOSE AND FRACTION dren’s Hospital of Philadelphia (CHP) during the period March, 1980 to August, 1982. One of them, an infant with scanty bone involvement, was excluded from the pilot study because of her age (6 months) and because of the better prognosis for such infants. She remains well and free of disease nine months after three-drug chemo- therapy alone. There were no other exclusions. The patients ranged in age from 9 months (a boy with multiple bones affected) to 12 years (median of 30 months). In addition, a 4 year-old girl from St. Christopher’s Hospital for Children was included in this pilot investigation.
All children received triple-dose chemotherapy accord- ing to the standard CCSG regimen: cyclophosphamide, 700 mg/m’on day 1; DTIC, 250 mg/m2 on days l-5; and vincristine, I .5 mg/m* on day 5. These same drugs were given at 3-week intervals for 2 years. Radiation therapy was administered to the whole body on day 2 and day 4 of each chemotherapy cycle, 50 rad being delivered at each of two sessions at a rate of 8 rad/min.* This regimen was followed for the first 10 patients; thereafter, three daily doses of 50 rad have been given on days 2, 3 and 4 of the chemotherapy regimen. Six MeV beams with opposing lateral fields without compensating filters were used, the dose being specified at the mid-point at the level of the umbilicus. The target-to-axis distance was 370 cm.
The total doses of radiation and of chemotherapy have varied throughout the period of this pilot study. The first eight patients received 100 rad (50 rad q2d x 2) during each cycle of chemotherapy. The next two had irradiation according to the same schedule at 3 week intervals, but chemotherapy was dropped from the third and fifth courses because a pronounced thrombocytopenia was evident in all patients after the delivery of 300 or more rad. The next three patients were given 150 rad (50 rad qd x 3), the third and fifth cycles of chemotherapy being omitted, but the TBI dose for the third cycle has been reduced to 100 rad for the 14th child.
Sites of disease measuring 5 cm or more in greatest diameter were ‘debulked’ surgically or with radiation
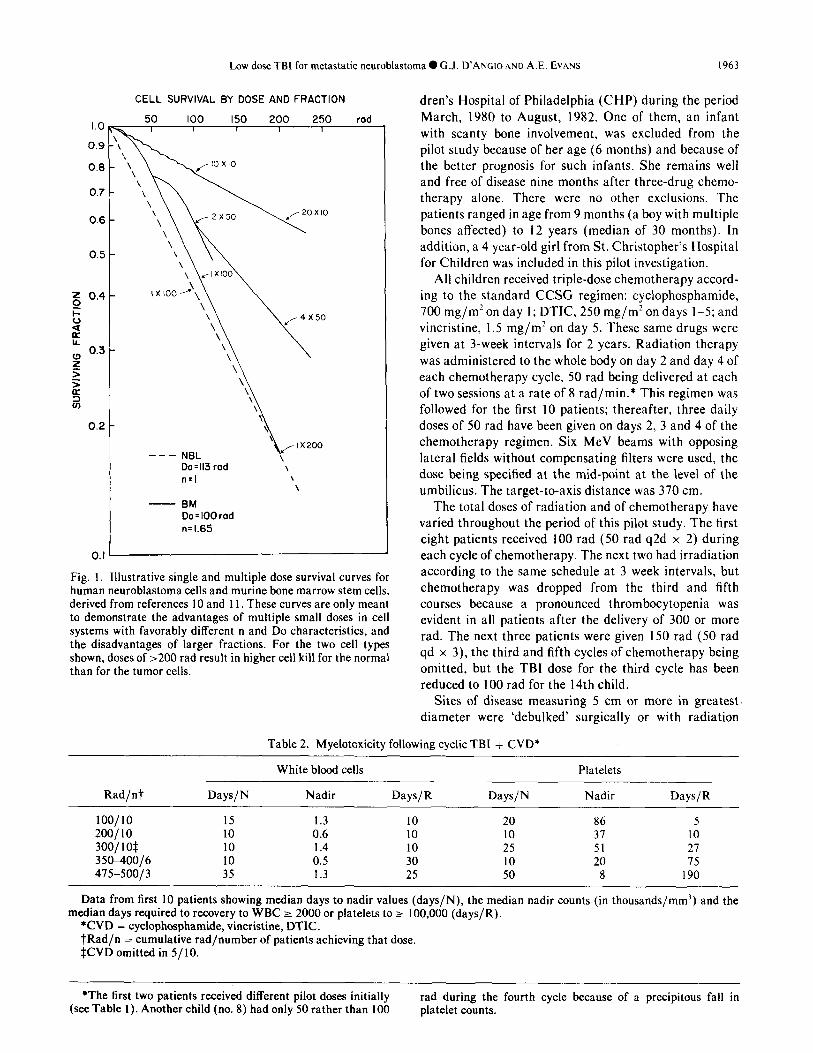
Table 2. Myelotoxicity following cyclic TBI + CVD*
White blood ceils Platelets
Rad/nt Days/N Nadir Days/R Days/N Nadir Days/R
100/10 15 1.3 10 20 86 5 ZOO/l0 10 0.6 10 10 31 10 300/I O$ 10 1.4 10 25 51 21 35&400/6 10 0.5 30 10 20 15 415-50013 35 1.3 25 50 8 190
Data from first 10 patients showing median days to nadir values (days/N), the median nadir counts (in thousands/mm’) and the median days required to recovery to WBC 2 2000 or platelets to zz 100,000 (days/R).
*CVD = cycIophosphami,de, vincristine, DTIC. tRad/n = cumulative rad/number of patients achieving that dose. $CVD omitted in 5/ 10.
*The first two patients received different pilot doses initially rad during the fourth cycle because of a precipitous fall in (see Table 1). Another child (no. 8) had only 50 rather than 100 platelet counts.
1964 Radiation Oncology 0 Biology 0 Physics
therapy. Local but generous irradiation fields were used and 200 rad/day for five successive days or 250 rad/d x 4 was delivered to each affected area. Residual tumor, after surgical attempts at debulking soft tissue masses, was treated in a similar fashion. The timing of such debulking maneuvers varied, but in general they took place after the second or third TBI cycle.
Patients whose bone marrows were tumor-free at diag- nosis, or those whose bone marrow was ‘cleared’ by treatment, had bone marrow ‘harvested’ and cryopre- served for possible later use, should they fail the low-dose TBI regimen.
RESULTS
All 14 children exhibited prompt and gratifying objec- tive and subjective improvement after the first course of therapy, but also exhibited pronounced pancytopenia after the second and subsequent cycles. The major prob- lem was thrombocytopenia, which became more pro- longed with each treatment cycle. Platelet transfusions were necessary in most patients and were given whenever platelet counts dropped below 2O,OOO/cu mm. Compiled data detailing hematological toxicity are shown in Table 2. Despite low absolute neutrophil counts, as well as low platelet levels, most patients remained in surprisingly good health. Hospitalization for these reasons was rare. However, the accelerated dose, 150 rad/course, has pro- duced even more problems with toxicity. Two patients succumbed to intracranial hemorrhage four months and six months after initiation of therapy, at a time when they appeared to be free of tumor. Autopsies were not obtained, so that microscopic residual disease at the time of demise cannot be excluded.
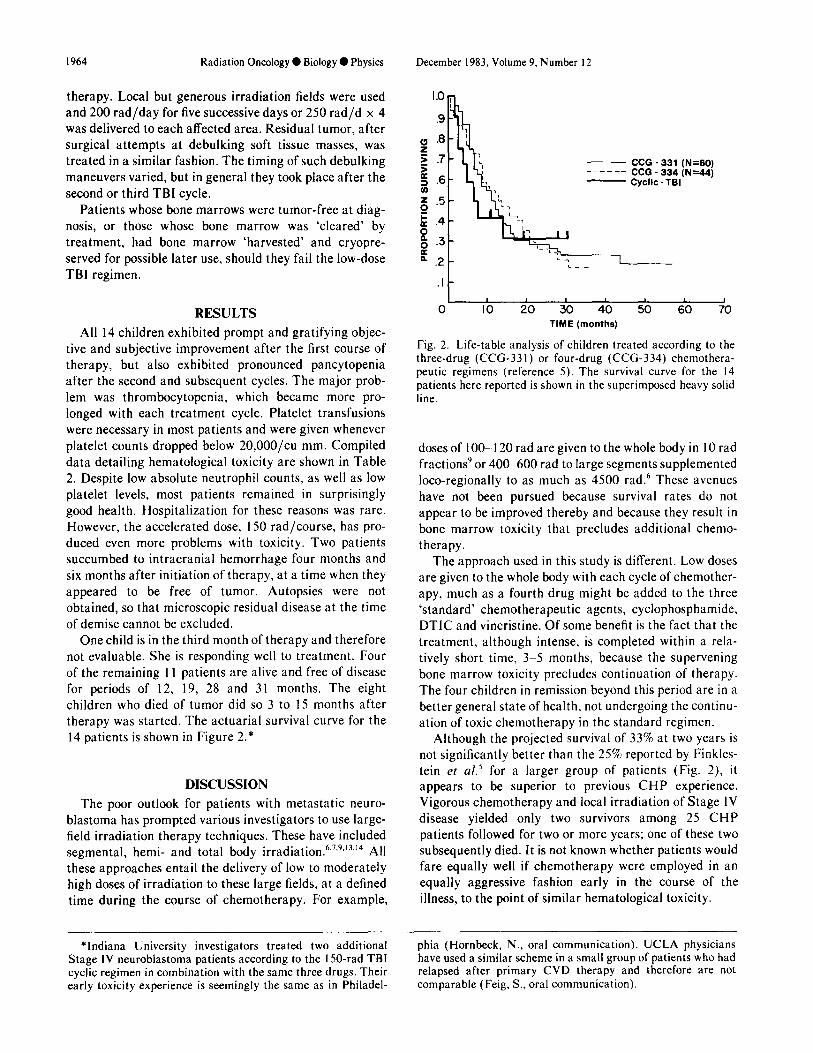
One child is in the third month of therapy and therefore not evaluable. She is responding well to treatment. Four of the remaining 11 patients are alive and free of disease for periods of 12, 19, 28 and 31 months. The eight children who died of tumor did so 3 to 15 months after therapy was started. The actuarial survival curve for the 14 patients is shown in Figure 2.*
DISCUSSION
The poor outlook for patients with metastatic neuro- blastoma has prompted various investigators to use large- field irradiation therapy techniques. These have included segmental, hemi- and total body irradiation.6.7,9.‘3,‘4 All these approaches entail the delivery of low to moderately high doses of irradiation to these large fields, at a defined time during the course of chemotherapy. For example,
December 1983, Volume 9, Number I2
- CCG - 331 (N=BO) ------ CCG - 334 (N=44) - Cyclic - TBI
I I 1 I I 1 I
0 IO 20 30 40 50 60 70 TIME (months)
Fig. 2. Life-table analysis of children treated according to the three-drug (CCG-331) or four-drug (CCG-334) chemothera- peutic regimens (reference 5). The survival curve for the I4 patients here reported is shown in the superimposed heavy solid line.
doses of 100-l 20 rad are given to the whole body in 10 rad fractions’or 400-600 rad to large segments supplemented loco-regionally to as much as 4500 rad.6 These avenues have not been pursued because survival rates do not appear to be improved thereby and because they result in bone marrow toxicity that precludes additional chemo- therapy.
The approach used in this study is different. Low doses are given to the whole body with each cycle of chemother- apy, much as a fourth drug might be added to the three ‘standard’ chemotherapeutic agents, cyclophosphamide, DTIC and vincristine. Of some benefit is the fact that the treatment, although intense, is completed within a rela- tively short time, 3-5 months, because the supervening bone marrow toxicity precludes continuation of therapy. The four children in remission beyond this period are in a better general state of health, not undergoing the continu- ation of toxic chemotherapy in the standard regimen.
Although the projected survival of 33% at two years is not significantly better than the 25% reported by Finkles- tein et al.’ for a larger group of patients (Fig. 2), it appears to be superior to previous CHP experience. Vigorous chemotherapy and local irradiation of Stage IV disease yielded only two survivors among 25 CHP patients followed for two or more years; one of these two subsequently died. It is not known whether patients would fare equally well if chemotherapy were employed in an equally aggressive fashion early in the course of the illness, to the point of similar hematological toxicity.
*Indiana University investigators treated two additional Stage IV neuroblastoma patients according to the l50-rad TBI cyclic regimen in combination with the same three drugs. Their early toxicity experience is seemingly the same as in Philadel-
phia (Hornbeck, N., oral communication). UCLA physicians have used a similar scheme in a small group of patients who had relapsed after primary CVD therapy and therefore are not comparable (Feig. S., oral communication).

Low dose TBI for metastatic neuroblastoma 0 G.J. D’ANGIOAND A.E. EVANS I965
The hazards of the regimen are clear, in that the practical and may be of assistance in the management of children are vulnerable to infections and to life-threaten- patients with widely disseminated radioresponsive ing hemorrhagic episodes. Careful surveillance and sup- tumors. This approach needs to be perfected, including portive measures are needed for such complications. the choice of adequate time-dose-fractionation schemes,
It has been concluded that the delivery of fractionated, and the timing of surgical and radiotherapeutic debulking low-dosage total body irradiation given in 3 week cycles is maneuvers.
REFERENCES
1.
2.
3.
4.
5.
6.
I.
Abrams, R.A., Simon, R., Glaubiger, D., Lichter, A.. Deisseroth, A.B.: Haemopoietic recovery in Ewing’s sar- coma after intensive combination therapy and autologous marrow infusion. Lancet 2: 3855389, 1980. Carabell, S.C., Chaffey, J.T., Rosenthal, D.S., Moloney, W.C., Hellman, S.: Results of total body irradiation in the treatment of advanced non-Hodgkin’s lymphomas. Cancer 43: 994-1000,1979. del Regato. J.A.: Total body irradiation in the treatment of chronic lymphogenous leukemia. Am. J. Roentgenol. 120: 504-520, 1974. Evans, A.E.: Natural history of neuroblastoma. In Advances in Neuroblastoma Research, (Ed.). New York, Raven Press. 1980, pp. 3-l 2. Finkelstein, J.Z., Klemperer, M.R., Evans, A.E., Bernstein, I., Leikin, S., McCreadie, S., Grosfeld, J., Hittle, R., Weiner, J., Sather, H., Hammond, D.: Multiagent chemo- therapy for children with metastatic neuroblastoma. Med. Pediatr. Oncol. 6: 179-l 88, 1979. Green, A.A., Hustu, H.O., Palmer, R., Pinkel, D.: Total- body sequential segmental irradiation and combination chemotherapy for children with disseminated neuroblasto- ma. Cancer 38: 2250-2257. 1976. Helson, L., Jereb, B., Vogel, R.: Sequential hemi-body irradiation in treatment of advanced neuroblastoma: A pilot study. Int. J. Radiat. Oncol. Biol. Phys. 7: 53 I-534, 198 I.
8.
9.
IO.
11.
12.
13.
14.
Johnson, R.E.: Radiation therapy of generalized lympho- cytic lymphomas. Am. J. Roentgenol. 117: 50-53, 1973. Kun, L.E., Casper, J.T., Kline, R.W., Piaskowski, V.D.: Fractionated total body irradiation for metastatic neuro- blastoma. Int. J. Radiat. Oncol. Biol. Phys. 7: 1599-I 602, 1981.
McCulloch, E.A., Till, J.E.: The sensitivity of cells from normal mouse bone marrow to gamma radiation in vitro and in vivo. Radint. Res. 16: 822-832. 1962. Ohnuma, N., Kasuga, T., Nojiri. I., Furuse. T.: Radiosensi- tivity of human neuroblastoma cell line (NB-I ). Gun 68: 71 I-712, 1977.
Osgood, E.E.: Titrated, regularly spaced radioactive phos- phorus or spray roentgen therapy of leukemias. AMA Arch. Intern. Med. 87: 329-348, I95 I
Sagerman, R.H.: Primary management of disseminated neuroblastoma by sequential segmental irradiation. Radiol- ogy 90: 352-353, 1968.
Wharam, M.D., Kaizer, H., Leventhal, B.G., Munoz, L.. Tutschka, P.J., Santos, G.W., Elfenbein, G.J.. Order, S.E.: Systemic irradiation for selected Stage IV and recurrent pediatric solid tumors: Method, toxicity, and preliminary results. Int. J. Radiat. Oncol. Biol. Phys. 6: 217-223, 1980.