Embed Size (px)
Citation preview

70 Indian Dermatology Online Journal - January-April 2012 - Volume 3 - Issue 1
Letters to the Editor
4. Nigam PK, Singh G. Mucosal and genital lesions in histoid leprosy. Int J Dermatol 1990;29:207-8.
5. Parikh DA, Parikh AC, Ganapati R. Penile and scrotal lesions in leprosy: Case reports. Lepr Rev 1989;60:303-5.
6. Kumar B, Kaur I, Rai R, Mandal SK, Sharma VK. Involvement of male genitalia in leprosy. Lepr Rev 2001;72:70-7.
7. Ghorpade A. Penile shaft lesion in reactional borderline tuberculoid leprosy: A case report. Indian J Dermatol Venereol Leprol 2003;69:411-2.
8. Desikan KV, Iyer CG. Histoid variety of lepromatous leprosy: A histopathologic study. Int J Lepr Other Mycobact Dis 1972;40:149-56.
9. Mansfield RC. Histoid leprosy. Arch Pathol 1969;87:580-5. 10. Rodriguez JN. The histoid leproma. Its characteristics and significance.
Int J Lepr Other Mycobact Dis 1969;37:1-21.
Cutis laxa with pulmonary artery stenosis Sir,A 9-month-old female patient presented with cough andbreathlessnessof1week’sduration.Shewasfoundtohaveloose,saggingskinalloverthebodysincebirth.Childwasbornofnon-consanguinousmarriageandwasdeliveredfull-term..Her developmental milestones were normal and she had no past history of major illness.. At the time of presentation she had moderate respiratory distress with a respiratory rate of 38/min,apulse rateof132/min,and temperatureof100°F.Onexamination,apart fromrightupperzonecrapitations,adiastolic murmur was heard.
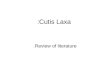
Theskinoftheentirebodywasextremelyloose,hanginginfolds,softandinelastic.Thechangeswereremarkableonface,neck,andflexures.Droopingofcornersofmouthandlooseskin around eyes gave her “blood hound” facial appearance [Figures1and2].The lax skin couldbeeasily pulled fromunderlying tissue and when released would return slowly to its initialposition.Nootherapparentabnormalityofnails,mucosa,orgentialiawasevident.Nocyanosis,edema,orpurpurawereobserved. No hernia or palpable lymph nodes were present. Hermotorandsensoryreflexeswerenormal.
OninvestigationhertotalWBCcountwas16,000/cmmwith84%neutrophils.Other investigations includingESR, liverfunctiontests,andrenalfunctiontestswerenormal.ThetestforTORCHantibodydidnot showanyelevated titre.X-raychest showed right and left upper zone patchy opacity with normalheartshadow.X-rayskull,clavicle,andcarpalboneswerenormal.USGabdomendidnotshowanyabnormality.2-Dechocardiogram showed right pulmonary artery stenosis with normal valves suggesting acyanotic congenital heart defects. Skin biopsy was not done as clinical diagnosis was obvious and parents did not give consent for the biopsy.
Her pedigree chart was made which showed two distant
relatives of the same generation affected with similar skin changes suggesting autosomal recessive (AR) inheritance[Figure3].Nootherdetailsregardinganysystemicabnormalityin other affected family members could be obtained.
Cutis laxa (CL) is an acquired or inherited skin disorder
Figure 2: Skin of the trunk can be easily pulled
PROBAND (9 MONTHS) 11YEAR 9YEAR
Figure 3: Pedigree chart showing distant relatives affected
Figure 1: Skin of the whole body including face showing characteristic changes of CL
[Downloaded free from http://www.idoj.in on Wednesday, August 27, 2014, IP: 14.97.93.24] || Click here to download free Android application for this journal

Indian Dermatology Online Journal - January-April 2012 - Volume 3 - Issue 1 71
characterizedbywrinkled,inelasticskin.Inbornerrorsofelastinsynthesis and structural defects of extracellular matrix proteins lead todecreasedelasticityand redundant, saggingskin inaffected patients.[1]
The inherited forms of CL are rather uncommon. Autosomal dominant (AD), autosomal recessive (AR), and X-linkedrecessive(XRCL)formsofdisorderareknown.IntheADformskin and connective tissue symptoms manifest at birth or early childhood. Associated features include cardiac valve anomalies andhernias.Earlyemphysemamayoccur,butgastrointestinalsymptoms are uncommon. X-linked CL present at birthwith distinct facial features and severe systemic symptoms includingfailuretothriveduetomalabsorption,urethralandbladderdiverticulae,andcongenitalhydronephrosis.Variousskeletal anomalies such as coxa valga, pelvic exostosis,kyphosis,etcandcardiovascularanomaliessuchastortuouscarotidarteries,orthostatichypertensionalsooccur.ARformsare the most severe of all. The clinical spectrum of ARCL is heterogenous with respect to both organ involvement and severity.ARCL I is a life-threateningdisorderwith cardiac,pulmonary, gastrointestinal, genitourinary, and vascularanomalies. ARCL II is a spectrum of clinical entities with variable severity of CL, abnormal growth, developmentaldelay, and skeletal abnormalities. The classical phenotypeincludesgeneralizedloose,redundantskinwithslowreturnonstretching.Widefontenelles,frontalbossing,downwardslantedpalpebralfissures,reversedVeyebrows,anddentalcarriesarecharacteristic.Inguinalhernia,pigeonchest,scoliosis,etc.arecommonfindings.Thewrinkledskinsyndrome,theDeBarsysyndrome,Cantusyndrome,etc.arephenotypicvariantsofARform of CL.[2] All inherited forms of CL are very rare. Precise dataontheirexactincidenceareunavailable.Fewerthan200families with various inherited forms are reported.[2,3]
Differential diagnoses include Ehlers-Danlos syndrome,pseudoxanthomaelasticum,leprechaunism,etc.DiagnosisofCLissuggestedbyfindinglooseskinwhichrecoilsonlyslowlyafterstretchingmaybeconfirmedbyhistology.
The diagnosis of a CL syndrome is based on clinical assessment of the typical skin features and the associated extracutaneous findings.Inourpatient,therewasahistoryofsimilarproblemin other family members of the same generation suggesting AR inheritance. She had no history of developmental delay or any joint laxity as described for Type II recessive CL; our patient probably suffered from the Type I recessive form. She had the characteristic cutaneous abnormalities described in all thevarietiesofCL.Additionally,shehadstenosisoftherightpulmonary artery. Cardiopulmonary abnormalities are common in Type I recessive CL and are the main factors to determine theprognosisandlifeexpectancy.Pulmonaryemphysema,corpulmonale,andright-sidedheartfailurecausedbypulmonarydisease have been commonly described. Pulmonary artery
stenosis has been occasionally described in the literature in association with AR CL.[4,5]
Inconclusion,wereportacaseofCLwithassociatedcardiacdefects and AR inheritance. Cardiac conditions require continuous monitoring and specialized treatment. The diffuse elastic changes have devastating effects on patients and their relatives.Identificationofassociatedsystemicmanifestationsis essential at an early date to prevent further complications fromlife-threateningconsequences.Geneticcounselingfortheaffected family is essential. We continue to closely follow up the patient in view of development of other features of ARCL.
Krina B. Patel, Ruchin Patel Department of Dermatology, Smt. S. C. L. Hospital,
Ahmedabad, Gujarat, India
Address for correspondence: Dr. Krina B. Patel, Department of Dermatology, Smt. S. C. L. Hospital,
Saraspur, Ahmedabad, Gujarat, India. E-mail: [email protected]
Access this article online
Quick Response Code:
Website: www.idoj.in
DOI: 10.4103/2229-5178.93487
REFERENCES
1. Urban Z, Gao J, Pope FM, Davis EC. Autosomal dominant cutis laxa with severe lung disease: Synthesis and matrix deposition of mutant tropoelastin. J Invest Dermatol 2005;124:1193-9.
2. Morava E, Guillard M, Leefeber DJ, Wevers RA. Autosomal recessive cutis laxa syndrome revisited. Eur J Hum Genet 2009;17:1099-110.
3. Mauskar A, Shanbag P, Ahirrao V, Nagotkar L. Congenital cutis laxa. Ann Saudi Med 2010;30:167-9.
4. Andiran N, Sarikayalar F, Saraçlar M, Cağlar M. Autosomal recessive form of congenital cutis laxa: More than the clinical appearance. Pediatr Dermatol 2002;19:412-4.
5. Hayden JG, Talner NS, Klaus SN. Cutis laxa associated with pulmonary artery stenosis. J Pediatr 1968;72:506-9.
Linear psoriasis: A rare presentation Sir,A70-year-oldfemalepresentedwithoccasionalmildlypruriticlinear lesionsover leftupper limbof10yearsduration.Thelesions initially started on the left forearm and progressed proximally over the left armanddistally up to the firstweb
Letters to the Editor
[Downloaded free from http://www.idoj.in on Wednesday, August 27, 2014, IP: 14.97.93.24] || Click here to download free Android application for this journal