Embed Size (px)
Citation preview

CRITICAL CAREMANAGEMENTOF ACUTEISCHEMIC STROKEAllyson R. Zazulia
ABSTRACT
Although most patients with acute ischemic stroke can be managed in aninpatient stroke ward or urgent care setting, about 15% to 20% will needadmission to an intensive care unit. These patients require attention to airway andrespiratory status, blood pressure, glucose, temperature, cardiac function, and insome cases, management of life-threatening cerebral edema. This review willdiscuss general principles in the critical care management of patients with acuteischemic stroke and apply these principles to common clinical scenarios.
Continuum Lifelong Learning Neurol 2009;15(3):68–82.
INTRODUCTION
Powerful evidence supports the benefitof organized inpatient stroke unit care toprevent complications and reduce therisk of death after acute ischemic stroke.Some stroke units are able to provide anintermediate level of care, such as that re-quired after thrombolytic administration,but about 15% to 20% of patients requireadmission to a critical care setting formore intensive monitoring or treatment.Thesemay include patients with difficult-to-control blood pressure, acute arrhyth-mias or myocardial infarction, impairedlevelof consciousness (or impaired lowercranial nerve function) resulting in in-ability to maintain an airway, or massivehemispheric or cerebellar infarction cre-ating risk for developing life-threateningcerebral edema, and those undergoingsome experimental treatments, such as
therapeutic hypothermia. New data haveemerged in recent years that havechanged the critical care management ofacute ischemic stroke, particularly in theareas of glycemic control and aggressivemanagement of cerebral edema.
Of course, patient and family valuesmust be considered before the decisionis made to admit a patient to the inten-sive care unit (ICU). Patients with ische-mic strokeareoftenelderly andmayhavean advanced directive that specifies thataggressive interventions be withheld. Inthis situation, ICU admission may not beconsistent with the patient’s wishes oran appropriate use of limited resources.
AIRWAY AND RESPIRATORYMANAGEMENT
Respiratory impairment may compli-cate ischemic stroke in three settings.
68
Relationship Disclosure: Dr Zazulia has nothing to disclose.Unlabeled Use of Products/Investigational Use Disclosure: Dr Zazulia has nothing to disclose.
Copyright # 2009, American Academy of Neurology. All rights reserved.
KEY POINT
A Patients with
ischemic stroke
who require
management in
an ICU setting
include those
with massive
hemispheric
infarction or large
cerebellar
infarction at risk
for developing
life-threatening
cerebral edema;
those with
respiratory failure,
hemodynamic
disturbance, or
cardiac
decompensation;
and those
undergoing some
experimental
treatments.
Note: Text referenced in the Quintessentials Preferred Responses, which appearlater in this issue, is indicated in yellow shading throughout this chapter.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

(1) It may occur as a direct result of le-sions impacting brainstem control of res-piration, with loss of pharyngeal tone aswell as cough, swallow, and gag reflexes.(2) Consciousness may be diminished,resulting in relaxation of the pharyngealmusculature and tongue and suppressionof cough and gag reflexes (Case 4-1).
The risk for respiratory impairmentin association with large hemispherestroke increases after a few days’ delay,as cerebral edema intensifies. With pro-gressive brainstem dysfunction due toherniation, a complete loss of controlof pharyngeal musculature and protec-tive reflexes is present. (3) Respiratory
69
Continuum Lifelong Learning Neurol 2009;15(3)
Case 4-1A 61-year-old woman was admitted to the neurologyfloor after the sudden onset of left-sided weakness,dysarthria, and confusion. Blood pressure was178/96 mm Hg, heart rate 80 beats per minute,and respiratory rate 16 breaths per minute with100% oxygen saturation on room air. She faileda bedside swallow evaluation because of coughingwith intake of liquids and solids and was notedto frequently need to clear her secretions. Overthe next 24 hours, she became less responsivewith sonorous respirations. Vital signs and oxygensaturation remained stable. Head CT showedhypodensity in the right middle cerebral artery(MCA) territory.
Comment. This patient with MCA infarctionhas signs of impaired airway protection withdepressed level of consciousness, difficulty managingsecretions, and impaired swallow. It is not prudentto wait for oxygen saturation to begin to fall beforeintervening. Initial airway management in ischemicstroke includes repeated assessments for sonorousrespirations and inability to manage oral secretions.If such signs develop, conservative measures,including proper positioning, frequent suctioning,and placement of an oral or nasal airway, areindicated. If conservative measures are ineffective,intubation may be necessary. In the setting of largehemispheric infarction with edema, care must betaken to avoid intracranial hypertension that cancomplicate the intubation process as a result ofhypoxia, hypercarbia, and direct tracheal stimulation(Table 4-1). IV lidocaine has been recommended toblock the response to tracheal stimulation, butdata supporting its use are lacking. Short-acting IVanesthetic agents such as etomidate or thiopentalalso block this response and additionally suppressbrain metabolic rate, theoretically improvingtolerance of a transient fall in cerebral perfusionpressure should it occur. Etomidate is generallypreferred over thiopental because it is less likelyto lower blood pressure.
TABLE 4-1 Sample IntubationProcedure for
Patients With IschemicStroke at Risk for ElevatedIntracranial Pressure
" Preoxygenation
100% oxygen forapproximately 5 minutes
" Induction
Etomidate 0.1 mg/kg to0.5 mg/kg or thiopental1 mg/kg to 5 mg/kg
" Intubation
Application of cricoidpressure (Sellick maneuver)
Laryngoscopy with intubation
" Confirmation of PlacementWith Auscultation, End-TidalCarbon Dioxide, and ChestX-ray
" Postintubation
Full ventilatory support(assist control or intermittentmandatory ventilation)
Hyperventilation (increaseminute ventilation to lowerarterial PCO2 to 25 mm Hgto 30 mm Hg) if acuteneurologic deteriorationor suspicion of increasedintracranial pressure is present
Sedation with short-actingagents such as fentanyl,midazolam, or propofol,as needed
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

compromise may be caused by aspira-tion or systemic complications such aspneumonia, pulmonary embolism, orpulmonary edema. These complicationsshould be considered any time a suddenchange in respiratory status occurs inpatients with acute ischemic stroke.
The mortality rate of patients withacute stroke who require intubation ishigh regardless of the reason for in-tubation, with only about 50% surviv-ing 30 days and 30% surviving 1 year(Milhaud et al, 2004). Predictors ofdeath include low Glasgow Coma Scalescore at intubation and absent pupillarylight reflexes. Patients who do survivemay achieve good functional outcome,however, with more than two-thirdsregaining normal activities of daily liv-ing with mild to moderate impairment(Santoli et al, 2001).
Intubated patients are at high riskof pneumonia via colonization of theoropharynx, sinuses, trachea, and gas-trointestinal tract or contaminationfrom hospital personnel or equipment.Appropriate measures should be takentominimize this risk. Daily oral care androutine use of chlorhexidine gluconatehelp reduce this risk.
BLOOD PRESSUREMANAGEMENT
Hypertension occurs commonly afterstroke. Even in patients without a his-tory of hypertension, blood pressure isoften elevated acutely and typically re-turns to baseline spontaneously overthe first week. A U-shaped relationshipbetween admission blood pressure anddeath has been found in some studies:both elevated and low blood pressuresare associated with high rates of earlyand late death (Castillo et al, 2004).Theoretical reasons in favor of loweringelevated blood pressure acutely are toreduce the formation of edema andlessen the risk of hemorrhagic trans-formation. Additionally, allowing bloodpressure to remain high risks acute
myocardial infarction, pulmonary ede-ma, and renal failure in a populationalready prone to cardiac and renaldisease. However, the acute treatmentof hypertension is controversial be-cause of concerns that impaired auto-regulation in the peri-infarct area willresult in further reduction of cere-bral blood flow (CBF) with loweringof blood pressure. In a recent reporton hypertensive patients studied withPET within the first week after stroke,focally impaired autoregulation to a15-mm Hg reduction in mean arterialpressure in the peri-infarct area wasnot seen. CBF did fall in some patientswith lowering of blood pressure, butthis was a global phenomenon likelyrelated to an upward shift of the auto-regulatory curve as a consequence ofchronic hypertension (Powers et al,2007). Larger blood pressure reduc-tions have been associated with earlyneurologic worsening, larger infarctvolumes, and higher rates of poor out-come and death (Castillo et al, 2004).
American Heart Association guide-lines for the early management ofischemic stroke (Adams et al, 2007)recommend treating systolic bloodpressures greater than 220 mm Hg ordiastolic blood pressures greater than120 mm Hg. But because of the risk ofexceeding an upwardly shifted lowerlimit of autoregulation in the setting ofpoorly controlled chronic hyperten-sion, it would be prudent to use anyknown information on prestroke bloodpressure status in treatment decisions.
On the other end of the spectrumis the use of induced hypertensionto increase CBF, a practice that issupported by experimental data. Pre-liminary studies suggest that theadministration of vasopressors in care-fully selected patients may improveneurologic and radiographic outcome(Hillis et al, 2003), but data from largeclinical trials are not available, andthe safety of induced hypertension in
70
Continuum Lifelong Learning Neurol 2009;15(3)
KEY POINTS
A Impaired airway
protection may
occur with
ischemic stroke
due to impaired
pharyngeal
reflexes,
depressed
consciousness, or
cardiopulmonary
complications.
Sonorous
respirations or
inability to
manage oral
secretions should
prompt
intervention.
A Blood pressure
management
after ischemic
stroke is
controversial.
Blood pressure
should be
lowered when
there is coexisting
acute myocardial
infarction,
pulmonary
edema, or
renal failure.
Otherwise,
decisions should
take into account
prestroke blood
pressure control.
"ACUTE ISCHEMIC STROKE
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

acute ischemic stroke has not beenestablished.
Blood Pressure ManagementAfter Thrombolysis
To reduce the risk of symptomatichemorrhagic transformation after ad-ministration of recombinant tissue-typeplasminogen activator (rt-PA), manage-
ment of blood pressure in this settingfollows stricter parameters. The guide-lines for monitoring of blood pressureafter treatment with rt-PA as used in theNational Institute of Neurological Dis-orders and Stroke (NINDS) tissue plas-minogen activator (t-PA) trial as well assuggested choice of agents (modifiedfrom those recommended in theNINDSt-PA trial) are listed in Table 4-2.
GLUCOSE MANAGEMENT
Hyperglycemia in the acute phase af-ter ischemic stroke is common, oc-curring in most or all patients witha history of diabetes mellitus and inone-third to one-half of nondiabeticpatients. Hyperglycemia is more com-mon in severe strokes and in thoseinvolving the insular cortex, support-ing at least some role for an underly-ing stress response that may involveautonomic dysregulation.
Early hyperglycemia is associatedwith larger infarct volume in experi-mental stroke models. In humans,hyperglycemia on admission is asso-ciated with increased cerebral edemavolume, higher rates of hemorrhagictransformation, lower likelihood of re-canalization and clinical benefit withthrombolytic therapy, and worse neu-rologic outcome. Although retrospectivedata suggested that early normalizationof blood glucose reduced mortalitynearly fivefold, the multicenter random-ized UK Glucose Insulin in Stroke Trial(GIST-UK) failed to show improved 90-day outcome with IV glucose-potassium-insulin infusions for 24 hours after acuteischemic stroke (Gray et al, 2007). Be-cause glucose-potassium-insulin therapywas associated with significantly lowerblood pressure, the authors hypothe-sized that the blood pressure loweringmay have counterbalanced any possi-ble benefit of glucose lowering. Treat-ment achieved only modest reductionsin mean plasma glucose concentration
71
TABLE 4-2 Management ofBlood Pressure
After Treatment WithRecombinant Tissue-TypePlasminogen Activator
" Monitor Blood Pressure
Every 15 minutes during andfor 2 hours after treatment
Then every 30 minutesfor 6 hours
Then every hour for 16 hours
" Treat if Systolic BloodPressure Is Greater Thanor Equal to 180 mm Hg orDiastolic Blood Pressure IsGreater Than or Equal to105 mm Hg
" Choice of Agents
Labetalol 10 mg IV over 1 to2 minutes, may repeat every5 to 10 minutes
Nicardipine infusion, 5 mg/h,titrate up to desired effectby increasing 2.5 mg/h every5 minutes to maximum of15 mg/h
Hydralazine 10 mg to20 mg IV, may repeat every15 minutes
Enalapril 1.25 mg IV over5 minutes, may repeat every20 minutes to maximum of5 mg in 6 hours
Adapted with permission from Adams HP Jr,Adams RJ, Brott T, et al. Guidelines for the earlymanagement of patients with ischemic stroke: ascientific statement from the Stroke Council ofthe American Stroke Association. Stroke 2003;34(4):1056–1083.
Continuum Lifelong Learning Neurol 2009;15(3)
KEY POINT
A In the 24 hours
after tissue
plasminogen
activator
administration,
blood pressure
should be kept
below 180/105
mm Hg to
minimize the risk
of hemorrhage.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

(less than 18 mg/dL difference betweenthe treatment and control groups); thusthis trial did not address the potentialbenefit ofmore intensive insulin therapy.However, a recent meta-analysis ofintensive glucose lowering in criticallyill patients found that tight glucosecontrol did not reduce hospital mortalitycompared with standard glucose man-agement but was associated with amarkedly increased risk of hypoglycemia(Wiener et al, 2008). Because hypo-glycemia itself may lead to brain injury,this situation certainly should be avoidedafter stroke. Several other studies ofglucose modulation in acute stroke areongoing. Untilmore conclusive evidencebecomes available, it seems prudentnot to aggressively lower glucose butrather to target moderate glucose levelsafter acute ischemic stroke. The ap-propriate level of blood glucose thatshouldprompt intervention is unknown,but a reasonable approach is to targetcontrol of glucose levels at 100 mg/dLto 150 mg/dL.
MANAGEMENT OF FEVER ANDTHERAPEUTIC HYPOTHERMIA
Fever
Fever is quite common in the earlyphase after ischemic stroke, occurringin more than half of patients (Hajatet al, 2000). The most common causeof fever after stroke is systemic infec-tion, but in some patients the cause isnot readily apparent, leading to theassumption of a central origin. Aconsiderable body of evidence suggestsa negative effect of fever on outcome inexperimental stroke. Data have notbeen as consistent in humans, but ameta-analysis of nine studies totaling3790 patients (in which the definitionof fever ranged from greater than37.08C to greater than or equal to38.08C) found a 19% increase in mor-tality for febrile stroke patients (confi-dence interval, 0.99-1.43) (Hajat et al,
2000). Combining the probability val-ues of the individual studies, fever wasassociated with significantly highermorbidity and mortality. Conversely,lowbody temperature on admission is anindependent predictor of good short-term outcome. The mechanism(s) for adetrimental effect of fever on outcomeare postulated to include increasedmetabolic demands, free radical pro-duction, and increased release of excit-atory neurotransmitters.
American Heart Association guide-lines recommend that sources of feverbe treated and antipyretic medicationsbe administered to febrile patients withstroke (Adams et al, 2007); however,the optimal treatment regimen is un-known, and the effectiveness of reduc-ing fever in improving outcome has notbeen established. Several small clinicaltrials have reported modest success inachieving normothermia with aspirin,ibuprofen, acetaminophen, and intra-vascular or surface cooling. One trialevaluated the utility of acetaminophenin afebrile patients with stroke andfound that, while treatment may resultin a small reduction in body tempera-ture, the effects were unlikely to haverobust clinical impact (Kasner et al,2002). The effect of prophylactic anti-biotic administration to febrile patientswith severe stroke has also been evalu-ated. A 4-day course of prophylacticmezlocillin plus sulbactam resulted inlower body temperature, reduced in-cidence of infections, and improved90-day outcome in one study (Schwarzet al, 2008).
Therapeutic Hypothermia
Lowering body temperature via hy-pothermic therapy has been demon-strated to have a neuroprotective effectin experimental stroke models, and itsearly introduction has been shown toimprove neurologic outcome after car-diac arrest. Hypothermia can be insti-tuted via surface or intravascular cooling.
72
Continuum Lifelong Learning Neurol 2009;15(3)
KEY POINTS
A Current data
support standard
care in the
management of
hyperglycemia
after stroke. A
reasonable
approach is to
target blood
glucose levels
of 100 mg/dL to
150 mg/dL.
A Sources of fever
should be treated
and antipyretic
medications
administered to
febrile patients
with stroke;
however, the
optimal treatment
regimen is
unknown, and
the effectiveness
of reducing fever
in improving
outcome has not
been established.
"ACUTE ISCHEMIC STROKE
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Surface cooling is typically achievedwith a combination of cooling blan-kets, ice water, and alcohol packs. Thismethod is uncomfortable, induces avigorous shivering response, and mayrequire elective intubation, neuromus-cular paralysis, and sedation, thus re-ducing eligibility for treatment to a verysmall subset of patients with massivestrokes. Newer devices designed toenhance contact with skin are moreeffective at lowering temperature; how-ever, they still induce shivering. Morelocalized cooling with a cooling hel-met is being investigated. Alternatively,an IV heat exchange system can beused, which involves circulating warmor cool saline through a central ve-nous catheter. This method is bettertolerated than surface body coolingwith potentially less of a shivering re-sponse and less need for intubationand paralysis.
Patients treated with hypothermiamust be monitored in an intensive caresetting where clinical status can bemonitored and hemodynamic parame-ters controlled. Potential complicationsinclude arrhythmia, hypotension, infec-tion, electrolyte abnormalities, throm-bocytopenia, and coagulopathy and areseen more with profound levels ofhypothermia (less than 308C) than withmild to moderate hypothermia (328C to368C). In addition, a rebound increasein intracranial pressure (ICP) may oc-cur with rewarming after hypothermia,which can result in fatal herniation.Controlled slow rewarming (0.18C to0.58C per hour) reduces this risk.
The optimal level of body temper-ature has not been determined. Sev-eral small pilot studies on the safetyand feasibility of therapeutic hypother-mia in acute ischemic stroke haverecently been published, most of themtargeting a temperature of 328C to338C. This degree of temperature re-duction requires aggressive sedation,which increases the risk of complica-
tions and reduces eligibility for thetreatment. One study of surface cool-ing with the ‘‘forced air’’ method for aperiod of 6 hours in acute strokeshowed that a more modest target of35.58C to 36.08C allowed cooling with-out heavy sedation and was not as-sociated with an increased frequencyof complications or increased mortal-ity (Kammersgaard et al, 2000). Tworandomized controlled trials of mild tomoderate hypothermia within 6 hoursof stroke onset are ongoing.
MANAGEMENT OFCARDIAC ISSUES
Cardiac ischemia and arrhythmias arenot only risk factors for ischemic strokebut are also potential complicationsafter ischemic stroke. Coronary athero-sclerosis and myocardial infarction arehighly prevalent in patients with fatalischemic stroke: among patients whodied a median of 12 days after stroke,the percentage with coronary plaques,coronary stenosis, and myocardial in-farction was 74%, 39%, and 44%, re-spectively (Gongora-Rivera et al, 2007).Two-thirds of the cases of myocardialinfarction were clinically silent. Esti-mates of the risk of coronary events inthe acute period after ischemic strokeprimarily come from stroke treatmenttrials, where the risk of fatal myocardialinfarction ranges from 2% to 5%. Theserates could be an underestimate be-cause healthier patients tend to beenrolled in such trials, but they mayoverestimate risk among patients with-out a history of heart disease.
Elevation of cardiac troponin levelson serial measurements can be foundin approximately 10% of patients withacute ischemic stroke (Jensen et al,2007) and is variably associated withan increased incidence of death. In-creased troponin levels occur mostfrequently in older patients with othercomorbidities (heart and/or renal fail-ure) and more severe strokes. EKG
73
Continuum Lifelong Learning Neurol 2009;15(3)
KEY POINT
A Therapeutic
hypothermia
holds promise as
a neuroprotective
technique but
remains
investigational in
acute ischemic
stroke. Because
of the risk of
systemic
complications
and rebound
intracranial
hypertension
upon rewarming,
patients must be
monitored in an
ICU setting.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

changes such as prolonged QT interval,inverted T waves, ST segment abnor-malities, and abnormally prominent Uwaves are very common after ischemicstroke as are cardiac arrhythmias, par-ticularly atrial fibrillation and prema-ture atrial or ventricular contractions.Fortunately, malignant arrhythmias arerare, but sudden death may occur. Areasonable screen for cardiac ischemiain acute ischemic stroke is an EKGand two cardiac troponin levels ob-tained 8 to 12 hours apart, with con-tinued measurement of any elevatedtroponin until it begins to decrease.Routine Holter monitoring will identifyoccult atrial fibrillation in about 5% ofpatients with acute ischemic stroke(Liao et al, 2007). Serial EKGs overthe first few days may improve thisdetection rate.
The mechanisms underlying cardiacevents in the setting of acute strokeare unknown but may involve distur-bances in the autonomic system. Thishypothesis is supported by the factthat patients with infarctions involv-ing insular cortex (particularly on theright) have an increased risk of cardiaccomplications and sudden death, andthe insula is the most important cor-tical area that controls cardiovascularregulation.
Atrial fibrillation with rapid ventricu-lar response is typically managed withcardioselective beta-blockers or calciumchannel blockers (Table 4-3). Theantiarrhythmic drug amiodarone hasatrioventricular node-blocking proper-ties and can be used when other agentsare contraindicated or ineffective. Ina hemodynamically unstable patient,cardioversion is required (Case 4-2).There is no apparent benefit of acuteheparin administration on the risk ofearly recurrent stroke since the in-crease in hemorrhagic stroke it pro-duces entirely offsets the decrease inischemic stroke. However, heparin isindicated if cardioversion is performed
after more than 48 hours of atrialfibrillation.
Management strategies in acute myo-cardial infarction focus on achievingreperfusion, reducing blood pressureand heart rate to decrease myocardialoxygen demand, and limiting furtherthrombosis with antithrombotic ther-apy. Blood pressure goals in the setting
74
TABLE 4-3 Management ofAcute AtrialFibrillation
" Assess for HemodynamicInstability
Hypotension
Heart rate greater than100 beats per minute
Pulmonary edema
Acute myocardial infarction
" If Hemodynamically Unstable
Adenosine 6 mg to 12 mgIV bolus or
Direct-current cardioversion
" If Rapid Heart Rate GreaterThan100 Beats Per Minute
Cardioselective beta-blocker
Metoprolol 5 mg to 15 mgIV bolus or
Esmolol 0.5 mg/kg IV over1 minute, then 0.05 mg/kg/min to 0.1 mg/kg/min IV
Calcium channel blocker
Diltiazem 0.25 mg/kg IVbolus, then 10 mg/hour IVinfusion or
Verapamil 2.5 mg to 5 mgIV bolus, then 0.05 mg/minto 0.2 mg/min IV infusion
Class III antiarrhythmic
Amiodarone 5 mg/kg IVover 30 to 60 minutes,then 1.2 g to 1.8 g IV over24 hours
Continuum Lifelong Learning Neurol 2009;15(3)
KEY POINTS
A Serial cardiac
troponin levels
and an EKG are
indicated after
acute ischemic
stroke because
of the frequent
occurrence of
cardiac ischemia
and arrhythmia.
A Atrial fibrillation
with rapid
ventricular
response
warrants
treatment with
rate-controlling
agents and, if
producing
hemodynamic
instability,
direct-current
cardioversion.
"ACUTE ISCHEMIC STROKE
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

of acute myocardial infarction are of-ten at odds with these goals in thesetting of acute ischemic stroke, re-sulting in difficult management deci-sions. Consultation with a cardiologistis typically indicated to determine if anacute intervention, such as angioplasty,is indicated.
MANAGEMENT OFCEREBRAL EDEMA
When blood flow is restored to infarct-ed brain tissue, the dead cells swell,causing an increased mass within thebrain. Edema starts to develop withinhours of stroke onset, peaks at 2 to5 days, and then gradually resolves(Shaw et al, 1959). With large infarcts,the swelling can damage and displacebrain structures, increase ICP, and inabout 2% to 3% of cases, cause brainherniation and death. However, rou-
tine ICP monitoring is not helpful inthe management of patients with largehemispheric stroke because by thetime global ICP rises to critical values,clinical and radiographic signs of her-niation are already present. In fact,most patients who herniate do so witha normal global ICP. Not surprisingly,the time course of fatal transtentorialherniation parallels that of edema, andherniation from space-occupying cere-bral edema is the leading cause ofdeath within the first week afterischemic stroke (Silver et al, 1984).
Complete MCA territory infarctionwith massive brain edema (‘‘malignant’’MCA infarction) is associated with amortality rate as high as 80% with con-servative therapy (Hacke et al, 1996).Early identification of patients likely todevelop massive edema is essential inplanning a rational approach to man-agement. These patients typically have
75
Continuum Lifelong Learning Neurol 2009;15(3)
Case 4-2A 75-year-old woman with a history of hypertension, diabetes, andcoronary artery disease was admitted with left hemiparesis andhemianesthesia and right hemianopia. Blood pressure on presentationwas 186/92 mm Hg. MRI revealed infarcts in the anterior superficial rightMCA territory and the superficial left posterior cerebral artery territory.Later that day, she developed palpitations and dyspnea and was foundon telemetry to have atrial fibrillation. EKG confirmed the atrial fibrillationwith a ventricular rate of 120 beats per minute and demonstratedT wave inversions in the lateral leads. She was transferred to the ICUand treated with diltiazem. When rate control was not achieved, a loadingdose of amiodarone was begun. During the bolus, blood pressure fellto 90/60 mm Hg and she became confused. The infusion was stopped butthe blood pressure did not improve. Emergent direct-current synchronizedcardioversion with 200 joules was performed, resulting in prompt reversionback to sinus rhythm with a rate of 80 beats per minute and blood pressureof 160/85 mm Hg. Neurologic status improved. Troponin I peaked at4.0 ng/mL (reference: less than 0.24 ng/mL) 24 hours later.
Comment. This patient with multifocal cerebral infarcts was found tohave an acute myocardial infarction and atrial fibrillation with rapidventricular response shortly after admission. Rate control was attemptedwith diltiazem followed by amiodarone. Amiodarone is associated witha number of potential adverse effects, including hypotension, whichoccurred in this patient. Once she became hemodynamically unstable,direct-current cardioversion was indicated.
KEY POINTS
A Ischemic cerebral
edema peaks 2
to 5 days after
stroke onset and
can lead to brain
herniation and
death. Routine
intracranial
pressure (ICP)
monitoring is not
helpful, however.
A Conservatively
managed
complete middle
cerebral artery
(MCA) territory
infarction with
massive brain
edema
(‘‘malignant’’
MCA infarction)
is associated
with a high
mortality rate.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

a complete hemispheric syndrome onpresentation with hemiplegia, hemi-anesthesia, global aphasia (dominant
hemisphere) or neglect (nondominanthemisphere), forced gaze deviation,and hemianopia (Case 4-3). CT scan
76
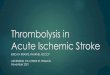
Case 4-3A 38-year-old man had a sudden onset of right-sided weakness and fell to the ground. Onexamination in the emergency department, blood pressure was 160/90 mm Hg, and he was alertwith dysarthria and reduced speech output. He followed simple, but not two-step, commands.He had a forced left gaze and right visual field cut. Strength in the right arm and leg wasantigravity only, and sensation was diminished on that side. Head CT showed a hyperdense leftMCA sign. He received IV t-PA 150 minutes after symptom onset and was admitted to the ICU formonitoring. The examination remained unchanged over the subsequent 16 hours, but at thatpoint blood pressure climbed to 190/100 mm Hg and he began to complain of headache, hadepisodes of emesis, and became progressively less alert. The right side became flaccid. Head CTshowed a persistent hyperdense left MCA sign as well as hypodensity in the entire left MCAterritory with 8 mm of midline shift, subfalcine herniation, and compression of the suprasellarcistern (Figure 4-1). Six hours later, he was noted to have a 7-mm unreactive left pupil.
Comment. The large size of this patient’s infarct was predicted by the extent of his deficitsat onset. Just 16 hours after symptom onset, he already had signs of increased ICP due tocerebral edema. Given that edematypically reaches a maximum at 2 to5 days, it is likely that he will continueto deteriorate for at least another2 days. It should be remembered thatyounger patients may have earliermanifestations of developing edemabecause without the added spaceafforded by preexisting cerebralatrophy, herniation will occur sooner.Subfalcine and uncal herniation aremost commonly seen with massiveanterior circulation infarcts. As theexpanding temporal lobe shifts theuncus and hippocampal gyrus overthe lateral edge of the tentoriumcompressing the oculomotor nerve,an ipsilateral dilating pupil develops.Ipsilateral hemiparesis may follow asthe opposite cerebral peduncle iscompressed against the edge of thetentorium contralateral to the infarct.
As in Case 4-1, this patient requiresairway management. With progressive decline in level of consciousness, loss of control ofpharyngeal and tongue musculature and cough and gag reflexes occur. If intubation is performed,care should be taken to avoid further increases in ICP. Immediate reversal of herniation is indicated.Hyperventilation is a temporizing measure to reduce ICP until more definitive treatment can beinstituted. Reducing arterial PCO2 through hyperventilation constricts cerebral arterioles, decreasingcerebral blood volume and thus ICP; however, it does so at the expense of decreasing CBF, which risksworsening cerebral ischemia. In any case, despite a continued reduction in PCO2 with sustainedhyperventilation, the effect on the cerebral vasculaturewanes after a period of about 4 hours (Raichleand Plum, 1972), and rapidweaningof sustainedhyperventilation can cause a rebound increase in ICP.
FIGURE 4-1 Head CT obtained 18 hours after strokeonset in the patient in Case 4-3demonstrating hypodensity involving the
entire left middle cerebral artery territory with hemorrhagicconversion in the basal ganglia, 8-mm horizontal shift of theseptum pellucidum, subfalcine herniation, and compression ofthe suprasellar cistern.
Continuum Lifelong Learning Neurol 2009;15(3)
"ACUTE ISCHEMIC STROKE
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

within the first few hours often showsloss of gray/white matter distinctionand sulcal effacement in the involvedterritory, and hyperdensity within thedistal internal carotid artery (ICA) and/or proximal MCA, indicative of throm-bus. The so-called carotid-T occlusion,in which acute occlusion extends fromthe supraclinoid portion of the ICAinto the proximal segments of themiddle and anterior cerebral arteries,has high specificity but low sensitivityto predict fatal brain edema. Clinicaland radiographic predictors of fatalbrain edema include high baselineNIH Stroke Scale (NIHSS) score, earlynausea and vomiting, 12-hour systolicblood pressure greater than or equal to180 mm Hg, early hypodensity ofgreater than 50% of the MCA territoryon CT, diffusion lesion volume greaterthan 82 mL within 6 hours of onset,involvement of additional vascular ter-ritories, elevatedwhite blood cell count,and history of hypertension or heartfailure (Kasner et al, 2001). The typicalpathologic pattern for the developmentof malignant MCA infarction is carotidocclusion with abnormal circle ofWillis ipsilaterally. Patients with malig-nant MCA infarction tend to beyounger, and there is a small but signifi-cant female predominance ( Jaramilloet al, 2006).
Although frequently used in thepast to treat stroke-induced cerebraledema, corticosteroids do not im-prove outcome and have fallen outof favor (Qizilbash et al, 2000).
Hyperosmolar Therapy
Osmotic agents such as mannitol andhypertonic saline lower elevated ICPand can reverse transtentorial hernia-tion, effects that appear to be achievedprimarily via extraction of water fromthe intracellular and interstitial spaces,resulting in temporary brain shrinkage.They may also improve cerebral perfu-sion through reduced viscosity or al-
tered red blood cell rheology (Andrewset al, 1993). Despite their widespreaduse in treating stroke-induced cerebraledema, few investigations of hyper-osmolar therapy in ischemic strokehave been done. In some experimentalmodels of ischemic stroke, mannitol,primarily when administered within 6hours after stroke onset, reducesinfarct size, edema, and neurologicdeficit (Karibe et al, 1995; Paczynskiet al, 1997). Data from observationalstudies and retrospective reviews inpatients with ischemic stroke suggestthat, while mannitol may transientlyreduce elevated ICP, it does not clearlyimprove outcome (Candelise et al,1975; Santambrogio et al, 1978). Evenfewer studies have addressed the useof hypertonic saline for the treatmentof poststroke edema. While it mayparadoxically increase brain water andinfarct volume in experimental stroke(Toung et al, 2002), data from humanischemic stroke suggest that it caneffectively treat ‘‘mannitol-resistant’’stroke-induced intracranial hyperten-sion (Suarez et al, 1998). The impactof hypertonic saline on outcome isunknown. While noting the lack ofconvincing evidence of efficacy, theAmerican Heart Association guidelines(Adams et al, 2007) and others recom-mend the use of osmotic agents totreat poststroke edema.
The optimal dose and timing of treat-ment with osmotic agents in ischemicstroke are uncertain. Mannitol is typi-cally administered as a bolus at a doseof 0.5 g/kg to 1.0 g/kg every 4 to 6hours. Hypertonic saline is typically ad-ministered as a bolus (23.4% concentra-tion) in roughly equi-osmolar doses tomannitol or as a continuous infusion(up to 3% concentration). No head-to-head comparisons have been done be-tween the two agents or among differentdoses, however. Similarly, no studieshave addressed the prophylactic use ofthese agents to treat stroke-associated
77
Continuum Lifelong Learning Neurol 2009;15(3)
KEY POINTS
A Osmotic agents
such as mannitol
and hypertonic
saline lower
elevated ICP and
can reverse
transtentorial
herniation. The
optimal dosing
regimen is
uncertain.
A Clearance
of mannitol
between doses
should be
monitored with
the osmolal gap,
and urine output
should be
replaced with
isotonic fluids
to reduce risk
of rebound
intracranial
hypertension
and renal failure.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

swelling and tissue shifts prior to theonset of intracranial hypertension.
In addition to their osmotic effects,these agents produce hemodynamiceffects that necessitate close monitor-ing of cardiac and fluid status. The mostcommon complications are fluid andelectrolyte imbalances and pulmonaryedema. Although rebound intracranialhypertension and renal failure are of-ten cited as major limitations to theuse of mannitol, these effects appearto be an issue primarily if the drug isnot completely cleared from the bloodbetween administrations and urine out-put is not adequately replaced, leadingto hypovolemia. Monitoring the clear-ance of mannitol between administra-tions is most effectively achieved withthe osmolal gap (the difference be-tween osmolality and osmolarity, calcu-lated using the formula [2� sodium] +[blood urea nitrogen/3] + [glucose/18]) rather than simple osmolality sinceonly the former correlates well withmannitol levels (Garcia-Morales et al,2004).
DecompressiveHemicraniectomy
Decompressive surgery for large hemi-spheric infarction involves removing alarge frontotemporal-parietal bone flap
and opening the dura ipsilateral to theside of infarction to allow outwardherniation of the brain, thus loweringICP and alleviating or preventing down-ward herniation (Figure 4-2). Severalnonrandomized studies have suggestedthat decompressive hemicraniectomywith duroplasty lowers mortality inpatients with malignant MCA infarctionwithout increasing the number of sev-erely disabled survivors. A preplannedpooled analysis of three Europeanrandomized controlled trials of de-compressive hemicraniectomy (De-compressive Craniectomy in MalignantMiddleCerebralArtery Infarcts [DECIMAL],Decompressive Surgery for the Treat-ment of Malignant Infarction of theMiddle Cerebral Artery [DESTINY], andHemicraniectomy After MCA Infarc-tion with Life-threatening Edema Trial[HAMLET]) compared with conserva-tive treatment confirmed the beneficialeffect of surgery suggested by earliercase series (Vahedi et al, 2007). Impor-tant eligibility criteria for the pooledanalysis included age 18 to 60; NIHSSgreater than 15; decrease in level ofconsciousness to a score of greaterthan or equal to 1 on item 1a of theNIHSS; CT hypodensity involving atleast 50% of the MCA territory; ab-sence of bilaterally fixed, dilated pu-pils; and inclusion within 45 hours ofstroke onset. Surgery within 48 hoursof stroke onset increased the chancesof a favorable outcome (modifiedRankin scale [mRS] score of 1 to 4)from 24% to 75%. Surgery doubled theprobability of survival with an mRSscore of 3 or less without increasingrisk of very severe disability (mRS scoreof 5); however, the risk of survival withmoderately severe disability (ie, needfor assistance with walking and attend-ing to bodily needs) was increasedmore than 10-fold. Whether this is adesirable outcome requires discussionwith the patient and family in eachindividual case.
78
Continuum Lifelong Learning Neurol 2009;15(3)
FIGURE 4-2 CT scan obtained after decompressivehemicraniectomy of the patient in Case 4-2demonstrating herniation of brain through
the skull defect and resultant lessening of midline shift andbasilar cistern compression.
KEY POINT
A Decompressive
hemicraniectomy
within 48 hours
of malignant
MCA infarction
increases the
chances of a
favorable
dichotomized
outcome
(modified Rankin
Scale score of 4
or less), but this
includes a 10-fold
greater risk of
surviving with
moderately
severe disability.
"ACUTE ISCHEMIC STROKE
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

The North American-Hemicraniectomyand Durotomy for DeteriorationFrom Infarction Relating Swelling Trial(HeaDDFIRST), which has only beenpublished in abstract form (Frank,2003), showed a benefit of surgery inimproving survival at 21 days, but thesurvival benefit did not persist at 3 and6 months, and there was no improve-ment in functional outcome at 6months. Major differences in eligibilitycriteria for this trial compared with theEuropean pooled analysis are thatHeaDDFIRST permitted enrollment ofolder patients (up to age 75) as well asthose who developed severe edema aslate as 96 hours after stroke onset. Thislonger time window means that pa-tients in HeaDDFIRST were more likelyto have clinically deteriorated by thetime surgery was performed.
The optimal timing of surgery re-mains unknown. Operating prior to thedevelopment of signs of herniationmay result in the greatest chance atbenefit but means that some patientswill undergo surgery needlessly. Atleast one study reported lower mortal-ity and improved functional outcomeamong those operated on within 24hours compared with historical con-trols operated on after 24 hours ofonset (Schwab et al, 1998). However,a systematic review of studies (Guptaet al, 2004) found that time to surgerydid not predict outcome, and sub-group analysis from the pooled datacited above revealed no difference inoutcome between patients assigned toearly (less than 24 hours) versus later(24 to 48 hours) surgery. Nevertheless,early neurosurgical consultation (ie,prior to the development of signs ofherniation) is warranted for any patientin whom decompressive hemicraniec-tomy is being considered.
Two categories of patients who de-serve special mention are older adultsand those with dominant hemisphereinfarction. Age is nearly uniformly the
strongest predictor of outcome afterhemicraniectomy. Survival rates areclearly lower for those over age 60compared with those under 60, andwhile surgery may improve survival inthe older population, functional out-come remains poor (ie, no survivorsover age 60 achieved a Barthel Indexscore greater than 60 or an mRS scoreof less than 4 in one series) (Yao et al,2005). The age difference betweenpatients in HeaDDFIRST and the Euro-pean pooled analysis likely contributedto the discrepancy in results betweenthe two patient groups.
Offering decompressive hemicrani-ectomy to patients with malignant in-farction of the dominant hemisphereremains controversial because of abias among clinicians that quality of lifeis heavily dependent on the ability tocommunicate; thus surgery for nondom-inant hemisphere infarction outpacessurgery for dominant hemisphere infarc-tion fourfold. In fact, the available datado not suggest a worse functional out-come for patients who undergo decom-pression of the dominant hemisphere(Gupta et al, 2004), and a recent reportdocumented significant recovery fromaphasia after hemicraniectomy, especiallyin younger patients (Kastrau et al, 2005).
Edema Associated WithCerebellar Infarct
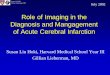
When cerebellar infarcts swell, life-threatening brainstem and fourthventricular compression may occur.There may be upward herniation ofthe cerebellar vermis and hemispheresthrough the tentorial opening ordownward tonsilar herniation throughthe foramen magnum. Radiographicsigns of mass effect develop in up to38% of cerebellar infarcts (Figure 4-3),and among these, about half are as-sociated with neurologic deteriora-tion (Koh et al, 2000), which mayinclude cranial nerve dysfunction,
79
Continuum Lifelong Learning Neurol 2009;15(3)
KEY POINTS
A The benefit of
decompressive
hemicraniectomy
extends to
patients with
dominant
hemisphere
infarction but
probably not to
patients over
age 60.
A Edema associated
with cerebellar
infarcts may
produce life-
threatening
brainstem and
fourth ventricular
compression.
The first sign of
medullary
compression with
tonsilar herniation
may be rapidly
progressive
bradycardia,
respiratory arrest,
and death.
A In the setting of
acute obstructive
hydrocephalus,
placement of an
external
ventricular drain
can rapidly lower
intracranial
pressure.
Suboccipital
craniotomy can
relieve both
obstructive
hydrocephalus
and brainstem
compression.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

hemiplegia or quadriplegia, posturing,or depressed consciousness. In addi-tion, it is critical to remember that thefirst sign of medullary compressionwith tonsilar herniation may be rapidlyprogressive bradycardia, respiratoryarrest, and death. Thus, patients withlarge cerebellar infarcts, particularlythose involving the full territory ofthe posterior inferior cerebellar arteryor superior cerebellar artery, shouldbe monitored closely in an ICU with
consideration of early neurosurgicalconsultation.
In the setting of acute obstructivehydrocephalus, placement of an exter-nal ventricular drain can rapidly lowerintracranial pressure. Suboccipital cra-niotomy can relieve both obstructivehydrocephalus and brainstem com-pression. Neither of these treatmentshas been compared with medicalmanagement (or with each other) ina randomized controlled trial.
REFERENCES
Adams HP Jr, del Zoppo G, Alberts MJ, et al. Guidelines for the earlymanagement of adults with ischemic stroke: a guideline from the AmericanHeart Association/American Stroke Association Stroke Council, ClinicalCardiology Council, Cardiovascular Radiology and Intervention Council, andthe Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes inResearch Interdisciplinary Working Groups: the American Academy of Neurologyaffirms the value of this guideline as an educational tool for neurologists. Stroke2007;38(5):1655–1711.
Andrews RJ, Bringas JR, Muto RP. Effects of mannitol on cerebral blood flow,blood pressure, blood viscosity, hematocrit, sodium, and potassium. Surg Neurol1993;39(3):218–222.
80
Continuum Lifelong Learning Neurol 2009;15(3)
FIGURE 4-3 Fluid-attenuated inversion recovery MRI obtained 3 days after acute-onsetheadache, vertigo, and nausea in a 58-year-old woman that demonstratesa large region of increased signal in the medial right cerebellum, consistent
with right posterior inferior cerebellar artery territory infarct (A). There is marked mass effect withcompression of the cerebral aqueduct and posterior brainstem (B) and narrowing of the fourthventricle (not shown). Prominence of the lateral ventricles and transependymal edema aresuggestive of acute obstructive hydrocephalus (C ).
"ACUTE ISCHEMIC STROKE
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Candelise L, Colombo A, Spinnler H. Therapy against brain swelling in strokepatients: a retrospective clinical study on 227 patients. Stroke 1975;6(4):353–356.
Castillo J, Leira R, Garcia MM, et al. Blood pressure decrease during the acutephase of ischemic stroke is associated with brain injury and poor stroke outcome.Stroke 2004;35(2):520–526.
Frank JI. Hemicraniectomy and durotomy upon deterioration from infarction relatedto swelling trial (HeaDDFIRST) first public presentation of the primary study findings.Neurology 2003;60(suppl 1):A426.
Garcia-Morales EJ, Cariappa R, Parvin CA, et al. Osmole gap in neurologic-neurosurgicalintensive care unit: its normal value, calculation, and relationship with mannitolserum concentrations. Crit Care Med 2004;32(4):986–991.
Gongora-Rivera F, Labreuche J, Jaramillo A, et al. Autopsy prevalence of coronaryatherosclerosis in patients with fatal stroke. Stroke 2007;38(4):1203–1210.
Gray CS, Hildreth AJ, Sandercock PA, et al. Glucose-potassium-insulin infusions inthe management of post-stroke hyperglycaemia: the UK Glucose Insulin in StrokeTrial (GIST-UK). Lancet Neurol 2007;6(5):397–406.
Gupta R, Connolly ES, Mayer S, Elkind MS. Hemicraniectomy for massive middlecerebral artery territory infarction: a systematic review. Stroke 2004;35(2):539–543.
Hacke W, Schwab S, Horn M, et al. ‘‘Malignant’’ middle cerebral artery territoryinfarction: clinical course and prognostic signs. Arch Neurol 1996;53(4):309–315.
Hajat C, Hajat S, Sharma P. Effects of poststroke pyrexia on stroke outcome: ameta-analysis of studies in patients. Stroke 2000;31(2):410–414.
Hillis AE, Ulatowski JA, Barker PB, et al. A pilot randomized trial of induced bloodpressure elevation: effects on function and focal perfusion in acute and subacutestroke. Cerebrovasc Dis 2003;16(3):236–246.
Jaramillo A, Gongora-Rivera F, Labreuche J, et al. Predictors for malignant middlecerebral artery infarctions: a postmortem analysis. Neurology 2006;66(6):815–820.
Jensen JK, Kristensen SR, Bak S, et al. Frequency and significance of troponin Televation in acute ischemic stroke. Am J Cardiol 2007;99(1):108–112.
Kammersgaard LP, Rasmussen BH, Jorgensen HS, et al. Feasibility and safety of inducingmodest hypothermia in awake patients with acute stroke through surface cooling: acase-control study: the Copenhagen Stroke Study. Stroke 2000;31(9):2251–2256.
Karibe H, Zarow GJ, Weinstein PR. Use of mild intraischemic hypothermia versusmannitol to reduce infarct size after temporary middle cerebral artery occlusion inrats. J Neurosurg 1995;83(1):93–98.
Kasner SE, Demchuk AM, Berrouschot J, et al. Predictors of fatal brain edema in massivehemispheric ischemic stroke. Stroke 2001;32(9):2117–2123.
Kasner SE, Wein T, Piriyawat P, et al. Acetaminophen for altering body temperature inacute stroke: a randomized clinical trial. Stroke 2002;33(1):130–134.
Kastrau F, Wolter M, Huber W, Block F. Recovery from aphasia afterhemicraniectomy for infarction of the speech-dominant hemisphere. Stroke2005;36(4):825–829.
81
Continuum Lifelong Learning Neurol 2009;15(3)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Koh MG, Phan TG, Atkinson JL, Wijdicks EF. Neuroimaging in deterioratingpatients with cerebellar infarcts and mass effect. Stroke 2000;31(9):2062–2067.
Liao J, Khalid Z, Scallan C, et al. Noninvasive cardiac monitoring for detectingparoxysmal atrial fibrillation or flutter after acute ischemic stroke: a systematicreview. Stroke 2007;38(11):2935–2940.
Milhaud D, Popp J, Thouvenot E, et al. Mechanical ventilation in ischemic stroke.J Stroke Cerebrovasc Dis 2004;(4):183–188.
Paczynski RP, He YY, Diringer MN, Hsu CY. Multiple-dose mannitol reduces brainwater content in a rat model of cortical infarction. Stroke 1997;28(7):1437–1443.
Powers WJ, Zazulia AR, Videen TO, Diringer MN. Effect of blood pressurereduction on regional cerebral flow in acute ischemic stroke. Stroke 2007;38(2):506.
Qizilbash N, Lewington SL, Lopez-Arrieta JM. Corticosteroids for acute ischaemicstroke. Cochrane Database Syst Rev 2000;(2):CD000064.
RaichleME, Plum F. Hyperventilation and cerebral blood flow. Stroke 1972;3(5):566–575.
Santambrogio S, Martinotti R, Sardella F, et al. Is there a real treatment forstroke? Clinical and statistical comparison of different treatments in 300 patients.Stroke 1978;9(2):130–132.
Santoli F, De Jonghe JB, Hayon J, et al. Mechanical ventilation in patients with acute ischemicstroke: survival and outcome at one year. Intensive Care Med 2001;27(7):1141–1146.
Schwab S, Steiner T, Aschoff A, et al. Early hemicraniectomy in patients with completemiddle cerebral artery infarction. Stroke 1998;29(9):1888–1893.
Schwarz S, Al-Shajlawi F, Sick C, et al. Effects of prophylactic antibiotic therapy withmezlocillin plus sulbactam on the incidence and height of fever after severe acuteischemic stroke: theMannheim infection in stroke study (MISS). Stroke 2008;39(4):1220–1227.
Shaw CM, Alvord EC Jr, Berry RG. Swelling of the brain following ischemicinfarction with arterial occlusion. Arch Neurol 1959;1:53–69.
Silver FL, Norris JW, Lewis AJ, Hachinski VC. Early mortality following stroke: aprospective review. Stroke 1984;15(3):492–496.
Suarez JI, Qureshi AI, Bhardwaj A, et al. Treatment of refractory intracranialhypertension with 23.4% saline. Crit Care Med 1998;26(6):1118–1122.
Toung TJ, Hurn PD, Traystman RJ, Bhardwaj A. Global brain water increases afterexperimental focal cerebral ischemia: effect of hypertonic saline. Crit Care Med2002;30(3):644–649.
Vahedi K, Hofmeijer J, Juettler E, et al. Early decompressive surgery in malignantinfarction of the middle cerebral artery: a pooled analysis of three randomisedcontrolled trials. Lancet Neurol 2007;6(3):215–222.
Wiener RS, Wiener DC, Larson RJ. Benefits and risks of tight glucose control in criticallyill adults: a meta-analysis [published erratum appears in JAMA 2009;301(9):956].JAMA 2008;300(8):933–944.
Yao Y, Liu W, Yang X, et al. Is decompressive craniectomy for malignant middle cerebralartery territory infarction of any benefit for elderly patients? Surg Neurol2005;64(2):165–169.
82
Continuum Lifelong Learning Neurol 2009;15(3)
"ACUTE ISCHEMIC STROKE
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.