Embed Size (px)
Citation preview
1533
the case if, because of inadequacies in the methods applied, it
appears that Eldorado has been attained.
University Department Medicine,General Infirmary,Leeds LS1 3EX THOMAS PULLAR
Centre for Rheumatic Diseases,Glasgow Royal Infirmary,Glasgow HILARY A. CAPELL
1. Pullar T, Capell HA. Can treatment really influence the radiological progression ofrheumatoid arthritis? Br J Rheumatol 1986; 25: 2-6.
2. Pullar T, Capell HA. Selection of suitable patients for second-line therapy mrheumatoid arthritis. Br J Rheumatol 1986; 25: 276-81.
3. Scott DL, Spector TD, Pullar T, McConkey B. What should we hope to achieve whentreating rheumatoid arthritis? Ann Rheum Dhs 1989; 48: 256-61.
4. Richards IM1, Fraser SM, Hunter JA, Capell HA. Comparison of phenytoin and goldas second line drugs m rheumatoid arthritis. Ann Rheum Dis 1987; 46: 667-69.
5. Belch JJF, Madhok R, McArdle B, et al. The effect of increasing fibrinolysis in patientswith rheumatoid arthritis: a double blind study of stanozolol. Q J Med 1986; 225:19-27.
COVERAGE OF MMR VACCINE
SiR,—Combined measles, mumps, and rubella (MMR) vaccinewas introduced into the UK childhood immunisation schedule in
October, 1988.1 The Cover of Vaccination Evaluated Rapidly(COVER) scheme which is run by the Communicable DiseaseSurveillance Centre of the Public Health Laboratory Service, hasprovided timely statistics of coverage for diphtheria, pertussis, andmeasles in England and Wales since 1987. MMR was included inthe scheme in October, 1988, and preliminary results are nowavailable.MMR coverage by 15 months of age was assessed in nineteen
health districts in England and Wales from November, 1988. Thedata were obtained with a standard programme from the statistical
package of the child health system.3 MMR coverage was evaluatedis six consecutive monthly cohorts of children bom between July 1and Dec 31, 1987. Each monthly cohort was studied shortly afterthe youngest member had reached 15 months of age. For example,children bom in July, 1987, were evaluated in November, 1988.Evaluations of subsequent cohorts were conducted between
December, 1988, and April, 1989. For comparison, measlescoverage by age 15 months was evaluated in six consecutive
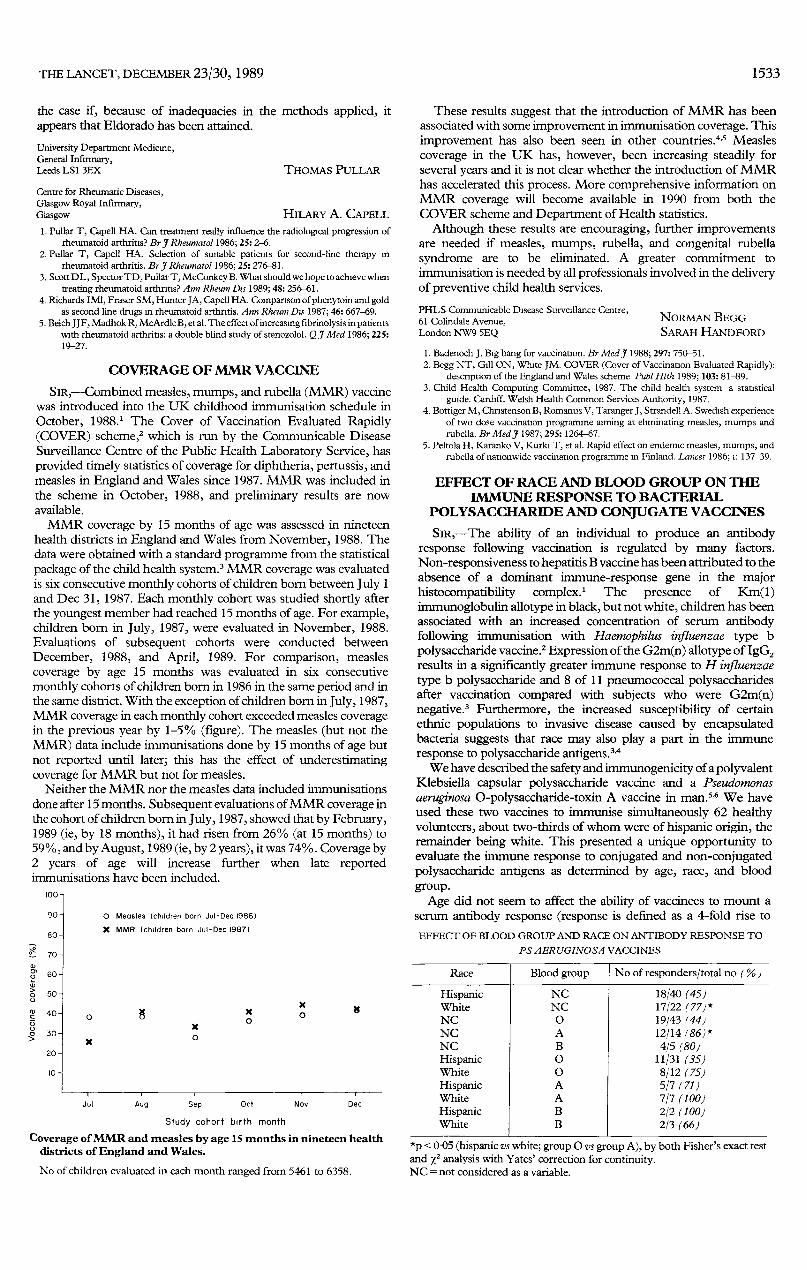
monthly cohorts of children born in 1986 in the same period and inthe same district. With the exception of children born in July, 1987,MMR coverage in each monthly cohort exceeded measles coveragein the previous year by 1-5% (figure). The measles (but not theMMR) data include immunisations done by 15 months of age butnot reported until later; this has the effect of underestimatingcoverage for MMR but not for measles.
Neither the MMR nor the measles data included immunisationsdone after 15 months. Subsequent evaluations of MMR coverage inthe cohort of children born in July, 1987, showed that by February,1989 (ie, by 18 months), it had risen from 26% (at 15 months) to59%, and by August, 1989 (ie, by 2 years), it was 74%. Coverage by2 years of age will increase further when late reportedimmunisations have been included.
too-,
Jul Aug Sep Oct Nov Dec
Study cohort birth month
Coverage of MMR and measles by age 15 months in nineteen healthdistricts of England and Wales.
No of children evaluated in each month ranged from 5461 to 6358.
These results suggest that the introduction of MMR has beenassociated with some improvement in immunisation coverage. Thisimprovement has also been seen in other countries.4,s Measlescoverage in the UK has, however, been increasing steadily forseveral years and it is not clear whether the introduction of MMRhas accelerated this process. More comprehensive information onMMR coverage will become available in 1990 from both theCOVER scheme and Department of Health statistics.
Although these results are encouraging, further improvementsare needed if measles, mumps, rubella, and congenital rubellasyndrome are to be eliminated. A greater commitment to
immunisation is needed by all professionals involved in the deliveryof preventive child health services.
PHLS Communicable Disease Surveillance Centre,61 Colindale Avenue,London NW9 5EQ
NORMAN BEGGSARAH HANDFORD
1. Badenoch J. Big bang for vaccination. Br Med J 1988; 297: 750-51.2. Begg NT, Gill ON, White JM. COVER (Cover of Vaccination Evaluated Rapidly):
description of the England and Wales scheme Publ Hlth 1989; 103: 81-89.3. Child Health Computing Committee, 1987. The child health system a statistical
guide. Cardiff. Welsh Health Common Services Authority, 1987.4. Bottiger M, Chnstenson B, Romanus V, Taranger J, Strandell A. Swedish experience
of two dose vaccination programme aiming at eliminating measles, mumps andrubella. Br Med J 1987; 295: 1264-67.
5. Peltola H, Karanko V, Kurki T, et al. Rapid effect on endemic measles, mumps, andrubella of nationwide vaccination programme m Finland. Lancet 1986; 1: 137-39.
EFFECT OF RACE AND BLOOD GROUP ON THEIMMUNE RESPONSE TO BACTERIAL
POLYSACCHARIDE AND CONJUGATE VACCINES
SiR,—The ability of an individual to produce an antibodyresponse following vaccination is regulated by many factors.
Non-responsiveness to hepatitis B vaccine has been attributed to theabsence of a dominant immune-response gene in the majorhistocompatibility complex.! The presence of Km(l)immunoglobulin allotype in black, but not white, children has beenassociated with an increased concentration of serum antibodyfollowing immunisation with Haemophilus influenzae type b
polysaccharide vaccine.2 Expression of the G2m(n) allotype of IgG2results in a significantly greater immune response to H influenzaetype b polysaccharide and 8 of 11 pneumococcal polysaccharidesafter vaccination compared with subjects who were G2m(n)negative.3 Furthermore, the increased susceptibility of certainethnic populations to invasive disease caused by encapsulatedbacteria suggests that race may also play a part in the immuneresponse to polysaccharide antigens. 3,4We have described the safety and immunogenicity of a polyvalent
Klebsiella capsular polysaccharide vaccine and a Pseudomonasaeruginosa 0-polysaccharide-toxin A vaccine in man. 5,6 We haveused these two vaccines to immunise simultaneously 62 healthyvolunteers, about two-thirds of whom were of hispanic origin, theremainder being white. This presented a unique opportunity toevaluate the immune response to conjugated and non-conjugatedpolysaccharide antigens as determined by age, race, and bloodgroup.
Age did not seem to affect the ability of vaccinees to mount aserum antibody response (response is defined as a 4-fold rise to
EFFECT OF BLOOD GROUP AND RACE ON ANTIBODY RESPONSE TO
PS AERUGINOSA VACCINES
I 1-
*p < 0-05 (hispanic vs white; group 0 vs group A), by both Fisher’s exact testand X2 analysis with Yates’ correction for continuity.NC = not considered as a variable.





























