Embed Size (px)
Citation preview

No. 1829.
SEPTEMBER 18, 1858.
Course of LecturesON THE
PHYSIOLOGY & PATHOLOGYOF THE
CENTRAL NERVOUS SYSTEM.Illustrated by numerous Engravings, representing the
principal Experiments and Pathological Cases.
DELIVERED AT THE
ROYAL COLLEGE OF SURGEONS OF ENGLAND
IN MAY, 1858.BY
E. BROWN-SÉQUARD, M.D.
LECTURE VII.-(Continued.PATHOLOGICAL CASES SHOWING THAT THE CONDUCTORS OF
SENSITIVE IMPRESSIONS FROM THE TRUNK AND LIMBS DE-CUSSATE IN THE SPINAL CORD AND NOT IN THE ENCEPHA-LON, AND THAT THE CONDUCTORS OF THE ORDERS OF THEWILL TO MUSCLES DECUSSATE IN THE LOWER PART OF THEMEDULLA OBLONGATA AND NOT IN THE PONS VAROLII.
The decussation of the conductors of sensitive impressions, fromthe trunk and limbs, does not take place in the crura cerebri,neither in the pons Varolii, nor in the medulla oblongata.--Cases proving that this decussation takes place in the spinalcord.-Cases of loss of voluntary movement in one side of thebody, and of loss of sensibility in the opposite side. -The de-cussation ofthe conductors for voluntary movements does nottake place, as has been imagined, all along the basis of theencephalon. This decussation seems to take place almostentirely in the lower paJ’t of the medulla oblongata.-Symp-toms of alteration in a lateral half of the spinal cord, thelower part of the medulla oblongata, and the rest of the en-cephalon, as regards voluntary movements and sensibility.SOME of the cases, already mentioned to establish the exacti-
tude of my views concerning the decussation of the conductorsof sensitive impressions in the spinal cord, are far from being positive proofs of these views, no autopsy having shown thereal extent of the injury; but there are two reasons whichhave decided my relating them, as giving an additional evi-dence. The first of these reasons is, that the symptoms observedin these pathological facts (see Cases 32, 33, 34, and 35) arethe same as those which I have shown to exist in animals aftera section of a lateral half or some other injuries to the spinalcord, so that it seems quite certain that the same injuries ex-isted in this organ in these cases. The second reason is, thatthere is no theory able to explain all that we know of thesecases, except the theory we are now trying to prove. I add to
these reasons that in Cases 32 and 34 the direction of the swordand its shape and size were such that the injury must havebeen what we have already stated. It seems, therefore, thatof the seven cases (from 29 to 35) which we have related toground our theory, there are three (29, 30, 31) which are asdirect and as positive proofs as possible of the exactitude ofthis theory, and there are four (32 to 35) which have an indi-rect but a great value for the establishment of this doctrine.We will now relate two more cases, which, although they donot give a positive proof, are very interesting by the symptomsWhich they have offered, and because they afford an additionaltestimony of some value in support of the view that the con-ductors of sensitive impressions decussate in the spinal cord.
CASE 36.-A. young man received a blow of a quadrangularand acute poignard, which entered the neck below the left ear,being directed towards the beginning of the spinal cord. Imme-
diately all the parts below the head lost sensibility and motion.
LECTURE VII.-(Continued.PATHOLOGICAL CASES SHOWING THAT THE CONDUCTORS OF
SENSITIVE IMPRESSIONS FROM THE TRUNK AND LIMBS DE-CUSSATE IN THE SPINAL CORD AND NOT IN THE ENCEPHA-LON, AND THAT THE CONDUCTORS OF THE ORDERS OF THEWILL TO MUSCLES DECUSSATE IN THE LOWER PART OF THEMEDULLA OBLONGATA AND NOT IN THE PONS VAROLII.
The decussation of the conductors of sensitive impressions, fromthe trunk and limbs, does not take place in the crura cerebri,neither in the pons Varolii, nor in the medulla oblongata.--Cases proving that this decussation takes place in the spinalcord.-Cases of loss of voluntary movement in one side of thebody, and of loss of sensibility in the opposite side. -The de-cussation ofthe conductors for voluntary movements does nottake place, as has been imagined, all along the basis of theencephalon. This decussation seems to take place almostentirely in the lower paJ’t of the medulla oblongata.-Symp-toms of alteration in a lateral half of the spinal cord, thelower part of the medulla oblongata, and the rest of the en-cephalon, as regards voluntary movements and sensibility.SOME of the cases, already mentioned to establish the exacti-
tude of my views concerning the decussation of the conductorsof sensitive impressions in the spinal cord, are far from being positive proofs of these views, no autopsy having shown thereal extent of the injury; but there are two reasons whichhave decided my relating them, as giving an additional evi-dence. The first of these reasons is, that the symptoms observedin these pathological facts (see Cases 32, 33, 34, and 35) arethe same as those which I have shown to exist in animals aftera section of a lateral half or some other injuries to the spinalcord, so that it seems quite certain that the same injuries ex-isted in this organ in these cases. The second reason is, thatthere is no theory able to explain all that we know of thesecases, except the theory we are now trying to prove. I add to
these reasons that in Cases 32 and 34 the direction of the swordand its shape and size were such that the injury must havebeen what we have already stated. It seems, therefore, thatof the seven cases (from 29 to 35) which we have related toground our theory, there are three (29, 30, 31) which are asdirect and as positive proofs as possible of the exactitude ofthis theory, and there are four (32 to 35) which have an indi-rect but a great value for the establishment of this doctrine.We will now relate two more cases, which, although they donot give a positive proof, are very interesting by the symptomsWhich they have offered, and because they afford an additionaltestimony of some value in support of the view that the con-ductors of sensitive impressions decussate in the spinal cord.
CASE 36.-A. young man received a blow of a quadrangularand acute poignard, which entered the neck below the left ear,being directed towards the beginning of the spinal cord. Imme-
diately all the parts below the head lost sensibility and motion.
He was brought home and put in bed, and there, amongst otherthings that the impediment to his respiration allowed him to say,he complained of being cold, and without any feeling he was burnton the thighs, the legs, and feet, in consequence of the applica-tion of a heated metallic vase to those parts. The left side ofthe body began for the first time to recover some feeling on theseventeenth day, and on the twentieth he began to move thetoes and fingers of the same side, and these two faculties in-creased graduallv until the thirtieth day in this side. Only onthe thirty-second day there was a return of some feeling in theright side of the body; movement also, but later, returnedslowly there. On the fortieth day there was sensibility andmovement everywhere, but not enough to allow the patient tostand up, and still less to walk. The recovery was so slow,that four months after the accident he was hardly beginning toget out of bed, and to walk as a child learning to walk; eventhen there was less power of movement and feeling in the rightthan in the left side. (Morgagni, "De Sedibus et Causis Mor-borum," &e. Nonaed., Lutetian, 1822, tomus sextus, p. 515-17.)
In this interesting case, we find that, although the woundmust have been more extensive in the left side of the spinalcord than in the right, the return of sensibility was quickerand greater in the corresponding side than in the right side ofthe body. It would not have been so if there was no decussa-tion of the conductors of sensitive impressions in the spinalcord. In this respect, therefore, this case is a good one in sup-port of my views; but how to explain that the power of volun-tary motion returned quicker in the side most injured than inthe other ? It would be easy to understand all the phenomenaobserved in admitting that the medulla oblongata, just abovethe crossing of the pyramids, was the part injured; but deathwould have been an immediate, or almost immediate, result ofsuch a wound, so that we must admit that the spinal cord isthe organ that was injured. In trying experiments on animalsto solve this difficulty, I have found that the introduction of aninstrument in the spinal cord, obliquely from the left to theright, and a little from behind forwards and from below up-wards, and dividing on the left side almost all the central greymatter, the posterior part of the lateral column, and a part ofthe posterior column, and, on the right side, part of the centralgrey matter and the parts of the right lateral column just atthe place where they approach the median line to make theircrossing just below the medulla oblongata, I produced a moreconsiderable loss of voluntary motion and sensibility in theright than in the left side. So that a greater injury to thegrey matter on the left than on the right side, and a greaterinjury to the lateral column (particularly to its decussatingpart) on the right than on the left side, are probably the causesof a greater loss of voluntary movement and sensibility in theright than in the left side in the case recorded by Morgagni.We must add, that the complete loss of sensibility and motionin the beginning, in that case, depended upon the existence ofsome haemorrhage, with pressure upon the whole spinal cord,besides the section of certain parts of this organ.The following case is less complicated than the preceding :-CASE 37.-Mrs. W- after a profuse haemorrhage, became
paralytic. Upon one side of the body there was a loss of sensi-bility, without, however, any corresponding diminution of
power in the muscles of volition. The breast, too, upon thatside partook of the insensibility, although the secretion of milkwas as copious as in the other. Upon the opposite side of thebody there was defective power of motion, without, however,any diminution of sensibility. The arm was incapable of sup-porting the child, the hand was powerless in its grasp, and theleg was moved with difficulty and with the ordinary rotatorymovement of a paralytic patient; but the power of sensationwas so far from being impaired that she constantly complainedof an uncomfortable state of heat, a painful tingling, and morethan the usual degree of tenderness from pressure, or othermodes of slight mechanical violence.Autopsy. -No positive disorganization of the brain could be
detected; the ventricles, however, contained more serum thanusual; and there were found thickening and increased vas-cularity of the membranes, with firm adhesion, in some parts;in others, an apparently gelatinous, transparent, and colourlessdeposit interposed between them. Unfortunately, the spinalcord was not examined.-(H. Ley, in a letter to Sir C. Bell, in" The Nervous System of the Human Body," 3rd ed., 1844,p. 245.)
This case acquires importance from the fact that there wasno alteration in the brain that could account for the symptoms,and from the similitude between the symptoms and those ob-served in animals after a section of a lateral half of the spmalcord.
He was brought home and put in bed, and there, amongst otherthings that the impediment to his respiration allowed him to say,he complained of being cold, and without any feeling he was burnton the thighs, the legs, and feet, in consequence of the applica-tion of a heated metallic vase to those parts. The left side ofthe body began for the first time to recover some feeling on theseventeenth day, and on the twentieth he began to move thetoes and fingers of the same side, and these two faculties in-creased graduallv until the thirtieth day in this side. Only onthe thirty-second day there was a return of some feeling in theright side of the body; movement also, but later, returnedslowly there. On the fortieth day there was sensibility andmovement everywhere, but not enough to allow the patient tostand up, and still less to walk. The recovery was so slow,that four months after the accident he was hardly beginning toget out of bed, and to walk as a child learning to walk; eventhen there was less power of movement and feeling in the rightthan in the left side. (Morgagni, "De Sedibus et Causis Mor-borum," &e. Nonaed., Lutetian, 1822, tomus sextus, p. 515-17.)
In this interesting case, we find that, although the woundmust have been more extensive in the left side of the spinalcord than in the right, the return of sensibility was quickerand greater in the corresponding side than in the right side ofthe body. It would not have been so if there was no decussa-tion of the conductors of sensitive impressions in the spinalcord. In this respect, therefore, this case is a good one in sup-port of my views; but how to explain that the power of volun-tary motion returned quicker in the side most injured than inthe other ? It would be easy to understand all the phenomenaobserved in admitting that the medulla oblongata, just abovethe crossing of the pyramids, was the part injured; but deathwould have been an immediate, or almost immediate, result ofsuch a wound, so that we must admit that the spinal cord isthe organ that was injured. In trying experiments on animalsto solve this difficulty, I have found that the introduction of aninstrument in the spinal cord, obliquely from the left to theright, and a little from behind forwards and from below up-wards, and dividing on the left side almost all the central greymatter, the posterior part of the lateral column, and a part ofthe posterior column, and, on the right side, part of the centralgrey matter and the parts of the right lateral column just atthe place where they approach the median line to make theircrossing just below the medulla oblongata, I produced a moreconsiderable loss of voluntary motion and sensibility in theright than in the left side. So that a greater injury to thegrey matter on the left than on the right side, and a greaterinjury to the lateral column (particularly to its decussatingpart) on the right than on the left side, are probably the causesof a greater loss of voluntary movement and sensibility in theright than in the left side in the case recorded by Morgagni.We must add, that the complete loss of sensibility and motionin the beginning, in that case, depended upon the existence ofsome haemorrhage, with pressure upon the whole spinal cord,besides the section of certain parts of this organ.The following case is less complicated than the preceding :-CASE 37.-Mrs. W- after a profuse haemorrhage, became
paralytic. Upon one side of the body there was a loss of sensi-bility, without, however, any corresponding diminution of
power in the muscles of volition. The breast, too, upon thatside partook of the insensibility, although the secretion of milkwas as copious as in the other. Upon the opposite side of thebody there was defective power of motion, without, however,any diminution of sensibility. The arm was incapable of sup-porting the child, the hand was powerless in its grasp, and theleg was moved with difficulty and with the ordinary rotatorymovement of a paralytic patient; but the power of sensationwas so far from being impaired that she constantly complainedof an uncomfortable state of heat, a painful tingling, and morethan the usual degree of tenderness from pressure, or othermodes of slight mechanical violence.Autopsy. -No positive disorganization of the brain could be
detected; the ventricles, however, contained more serum thanusual; and there were found thickening and increased vas-cularity of the membranes, with firm adhesion, in some parts;in others, an apparently gelatinous, transparent, and colourlessdeposit interposed between them. Unfortunately, the spinalcord was not examined.-(H. Ley, in a letter to Sir C. Bell, in" The Nervous System of the Human Body," 3rd ed., 1844,p. 245.)
This case acquires importance from the fact that there wasno alteration in the brain that could account for the symptoms,and from the similitude between the symptoms and those ob-served in animals after a section of a lateral half of the spmalcord.

296
Setting aside, in this lecture, what relates to temperature, westate that a transversal section of a lateral half of the spinalcord causes a loss of voluntary movement in the correspondingside of the body, and a loss of sensibility in the opposite side,and if, now, we look at the cases we have related to see howthey agree with this general result, we find the followingpoints :-
Setting aside, in this lecture, what relates to temperature, westate that a transversal section of a lateral half of the spinalcord causes a loss of voluntary movement in the correspondingside of the body, and a loss of sensibility in the opposite side,and if, now, we look at the cases we have related to see howthey agree with this general result, we find the followingpoints :-
If we add to these cases those in which we have no other reasonbut the analogy of symptoms with those observed in animals,such as Cases 33 and 37, we have two more instances of thiscurious but simple morbid manifestation-i. e., loss of movementin one side, loss of sensibility in the other. In animals, as Ihave often said and shown, the paralysed parts are in a stateof hyperaesthesia; in the cases I have related, hyperaesthesiahas been noted in Cases 32, 33, 35, and 37. It was so greatthat the least touch produced pain in Cases 32 and 35. Itwould have been found in the other cases, had the physicianswho attended the patients looked for it.The cases of loss of movement in one side of the body
with loss of sensibility in the opposite side are not so rareas a great many of my hearers probably think. That verylearned writer, Dr. Copland, says that the paralytic affectionin epilepsy occasionally consists " of loss of sensation in onelimb and of loss of movement in another, on the opposite side."("Diet. of Pract. Medicine," vol. i. 1844, p. 795). There is acase also in the" Ephemeridae Naturae Curios." cent. ii., obs.196; and Dr. J. Cooke ("History and Method of Cure ofPalsy," 1821, p. 19) says that Ramazzini speaks of a person inwhom one leg had lost its feeling, but not its power of motion,and the other its motion, but not its feeling. He also mentionsSênac as having related a case in which the most acute sensa-tion (hyperaesthesia) was experienced in one arm, which hadlost the power of motion; whilst in the other arm sensationwas lost, though motion remained perfect. Burserius, he adds,quotes a similar case from Heister. (I have vainly looked forthis case in Heister’s works.) In a recently-published work("Des Paralysies des Membres Inferieurs," 2de partie, 1857,p. 116, par R. Leroy d’EtioIles) there is a case of hysteric para-lysis, with loss of movement in one side and loss of sensibilityin the other. Lastly, Dr. R. Bright has recorded a case of thiskind, of which we will speak by and bye.
I shall not stop now to show that these cases, or at leastmost of them, are cases of alteration limited to a lateral halfof the spinal cord, as I shall have to treat of this subject againin a future lecture, in examining the symptoms of alterations ofvarious parts of the cerebro-spinal axis. I set aside also, forthe present, cases which might be considered as in oppositionto the theory I try to prove in this lecture, and I pass imme-diately to the second series of cases which I have to relate infavour of this theory. !
Second Series of Cases proving that the Conductors of S’ensitiveImpressions make their Decussation in the Spinal Cord.
I begin this series by a most important case indeed, fromwhich many physiological and practical deductions may bedrawn. It has been recorded by an able American physician,Dr. Samuel Annan.CASE 38.-S. G-, aged twenty-eight, was, on the 14th of
May, suddenly seized with an acute pain in the right side ofthe head, and fell down in a state of inst nsibility, remainingso for twenty-four hours. On recovering, she found she hadlost the power of moving her left arm, and, in a great degree,that of moving the leg of the same side. The right side wasunaffected, except the face, the muscles of which were paralysed;those of the left side of the face retained their power. Sensi-
bility of the left side of the body was destroyed, and likewisethat of the right side of the face. She could not hear with theright ear. The right eye became inflamed several weeks be-fore her death, and the cornea was slightly ulcerated; theupper eyelid was constantly raised. Her muttering was
scarcely intelligible; paralysis of all the parts affected becamecomplete; deglutition and mastication performed with greatdifficulty.
Autopsy, twelve hours after death.-A fibrous, semi-carti-laginous tumour was found on the right side of the tuberannulare and the medulla oblongata, seated in the substance of
If we add to these cases those in which we have no other reasonbut the analogy of symptoms with those observed in animals,such as Cases 33 and 37, we have two more instances of thiscurious but simple morbid manifestation-i. e., loss of movementin one side, loss of sensibility in the other. In animals, as Ihave often said and shown, the paralysed parts are in a stateof hyperaesthesia; in the cases I have related, hyperaesthesiahas been noted in Cases 32, 33, 35, and 37. It was so greatthat the least touch produced pain in Cases 32 and 35. Itwould have been found in the other cases, had the physicianswho attended the patients looked for it.The cases of loss of movement in one side of the body
with loss of sensibility in the opposite side are not so rareas a great many of my hearers probably think. That verylearned writer, Dr. Copland, says that the paralytic affectionin epilepsy occasionally consists " of loss of sensation in onelimb and of loss of movement in another, on the opposite side."("Diet. of Pract. Medicine," vol. i. 1844, p. 795). There is acase also in the" Ephemeridae Naturae Curios." cent. ii., obs.196; and Dr. J. Cooke ("History and Method of Cure ofPalsy," 1821, p. 19) says that Ramazzini speaks of a person inwhom one leg had lost its feeling, but not its power of motion,and the other its motion, but not its feeling. He also mentionsSênac as having related a case in which the most acute sensa-tion (hyperaesthesia) was experienced in one arm, which hadlost the power of motion; whilst in the other arm sensationwas lost, though motion remained perfect. Burserius, he adds,quotes a similar case from Heister. (I have vainly looked forthis case in Heister’s works.) In a recently-published work("Des Paralysies des Membres Inferieurs," 2de partie, 1857,p. 116, par R. Leroy d’EtioIles) there is a case of hysteric para-lysis, with loss of movement in one side and loss of sensibilityin the other. Lastly, Dr. R. Bright has recorded a case of thiskind, of which we will speak by and bye.
I shall not stop now to show that these cases, or at leastmost of them, are cases of alteration limited to a lateral halfof the spinal cord, as I shall have to treat of this subject againin a future lecture, in examining the symptoms of alterations ofvarious parts of the cerebro-spinal axis. I set aside also, forthe present, cases which might be considered as in oppositionto the theory I try to prove in this lecture, and I pass imme-diately to the second series of cases which I have to relate infavour of this theory. !
Second Series of Cases proving that the Conductors of S’ensitiveImpressions make their Decussation in the Spinal Cord.
I begin this series by a most important case indeed, fromwhich many physiological and practical deductions may bedrawn. It has been recorded by an able American physician,Dr. Samuel Annan.CASE 38.-S. G-, aged twenty-eight, was, on the 14th of
May, suddenly seized with an acute pain in the right side ofthe head, and fell down in a state of inst nsibility, remainingso for twenty-four hours. On recovering, she found she hadlost the power of moving her left arm, and, in a great degree,that of moving the leg of the same side. The right side wasunaffected, except the face, the muscles of which were paralysed;those of the left side of the face retained their power. Sensi-
bility of the left side of the body was destroyed, and likewisethat of the right side of the face. She could not hear with theright ear. The right eye became inflamed several weeks be-fore her death, and the cornea was slightly ulcerated; theupper eyelid was constantly raised. Her muttering was
scarcely intelligible; paralysis of all the parts affected becamecomplete; deglutition and mastication performed with greatdifficulty.
Autopsy, twelve hours after death.-A fibrous, semi-carti-laginous tumour was found on the right side of the tuberannulare and the medulla oblongata, seated in the substance of
the dura mater and other membranes. It extended from thepoint where the fifth pair of nerves arises from the tuberannulare, covered the origin of this nerve and the whole of theright side of the tuber below this, and passed down along two-thirds of the medulla oblongata, and adhered to the right sideof the basilar artery. The right vertebral artery was enclosedin the tumour, which was about two inches long. The surfaceof the root of the right crus cerebelli on which it pressed wassoftened, as was also that part of the tuber annulare on whichit lay. It was incorporated with the substance of the rightside of the medulla oblongata, and had produced softening asfar as it reached. This softening extended through the pos-terior tract, but became less as it approached the posteriorsurface. The anterior tract was a pulpy mass. Neither theanterior nor the posterior tract of the left side was perceptiblyaffected. The tumour pressed upon the roots of the fifth,seventh, eighth, and ninth pairs of nerves.-(S. Annan, in theAmerican Journal of the Medical Sciences, vol. ii., July, 1841,p. 105.)The author justly says: "The right side of the medulla
oblongata was softened to the extent of complete disorganiza-tion : there was complete paralysis both of motion and sensa-tion on the left side. The decussation of the fibres of the-corpora pyramidalia explains the loss of motion in the opposite-side, but as we have no facts proving a similar interlacementof the fibres of the posterior or sensory tract, it is not easy to-discover how it happened that the right side was not deprivedof sensation. Motion and sensation were unimpaired in theextremities of the side diseased; they were both destroyed inthe same parts of the opposite or left side. Are we not justifiedfrom this in making the inference that there is a decussationof the fibres for sensation as well as those for motion ?" Cer-tainly this is a very proper inference; but this question re-mains : Where does the decussation of the " fibres for sesation"take place ? Is it in the lower part of the medulla oblongata,where exists the decussation of the anterior pyramids, or-inthe spinal cord ? Lately, Messrs. Vulpian and Philipeaux(Comptes rendus de la Soci6ti de Biologie, Mars, 1858) haveshown that there are in the anterior pyramids fibres originatingfrom the posterior horns of grey matter, and decussating withthe other decussating fibres of these pyramids; and they suggestthat a crossing for sensation probably exists there. Admittingthat they are right, these conductors of sensitive impressionswould pass into the anterior pyramids, and they themselvesstate that it must be so. We will show, in the lecture on themedulla, oblongata, that this view is in opposition to positivefacts, and particularly the celebrated case of alteration of theanterior pyramids which has been recorded by our friend Pro.fessor Lebert.We think that the case of Dr. Annan, if we take into account
the extent of the injury in the medulla oblongata, bears cutclearly that most if not all of the conductors of sensitive im-pressions from the trunk and limbs make their decussation inthe spinal cord. But the importance of this case is not limitedto this demonstration: it shows at once the radical differencebetween the symptoms of an alteration of a lateral half of themedulla oblongata above the crossing of the pyramids, and analteration of a lateral half of the spinal cord either in the cer-vical or in another region. In this last case, as we have showna moment ago, there is loss of movement in one side and lossof sensibility in the opposite side; while in a case of alterationabove the crossing of the pyramids, we find that the loss ofmovement and of sensibility are both in the opposite side.This case is also excellent to show that the functions attributedto the restiform body as a conductor of sensitive impressions,and to the cerebellum as either a centre of perception of theseimpressions, or as a regulator of our voluntary movements, oras a centre for the guiding sensation, whether by a reflex actionor otherwise, are not performed by these parts, as the commu-nication between the cerebellum and the right side of the bodythrough the right side of the medulla oblongata was almostimpossible, a small part of the right restiform body remaining,and sensibility and voluntary movements being preserved inthis side.
In the following case, which is related by Broussais, we find,with less detail, many of the features of the preceding one.CASE 39.-An officer, recovered for some time, after having
been attacked with stupor, vomiting, &c.; but, five monthsafterwards, hemiplegia gradually appeared in the right side :the leg could support him a little ; the arm lost both movementand feeling. Soon after, the lift eye lost its transparency andbecame atrophied; the left eyelids were paralysed. A fewweeks after, walking was still more difficult, and speech moreimpeded, and death occurred after coma.
the dura mater and other membranes. It extended from thepoint where the fifth pair of nerves arises from the tuberannulare, covered the origin of this nerve and the whole of theright side of the tuber below this, and passed down along two-thirds of the medulla oblongata, and adhered to the right sideof the basilar artery. The right vertebral artery was enclosedin the tumour, which was about two inches long. The surfaceof the root of the right crus cerebelli on which it pressed wassoftened, as was also that part of the tuber annulare on whichit lay. It was incorporated with the substance of the rightside of the medulla oblongata, and had produced softening asfar as it reached. This softening extended through the pos-terior tract, but became less as it approached the posteriorsurface. The anterior tract was a pulpy mass. Neither theanterior nor the posterior tract of the left side was perceptiblyaffected. The tumour pressed upon the roots of the fifth,seventh, eighth, and ninth pairs of nerves.-(S. Annan, in theAmerican Journal of the Medical Sciences, vol. ii., July, 1841,p. 105.)The author justly says: "The right side of the medulla
oblongata was softened to the extent of complete disorganiza-tion : there was complete paralysis both of motion and sensa-tion on the left side. The decussation of the fibres of the-corpora pyramidalia explains the loss of motion in the opposite-side, but as we have no facts proving a similar interlacementof the fibres of the posterior or sensory tract, it is not easy to-discover how it happened that the right side was not deprivedof sensation. Motion and sensation were unimpaired in theextremities of the side diseased; they were both destroyed inthe same parts of the opposite or left side. Are we not justifiedfrom this in making the inference that there is a decussationof the fibres for sensation as well as those for motion ?" Cer-tainly this is a very proper inference; but this question re-mains : Where does the decussation of the " fibres for sesation"take place ? Is it in the lower part of the medulla oblongata,where exists the decussation of the anterior pyramids, or-inthe spinal cord ? Lately, Messrs. Vulpian and Philipeaux(Comptes rendus de la Soci6ti de Biologie, Mars, 1858) haveshown that there are in the anterior pyramids fibres originatingfrom the posterior horns of grey matter, and decussating withthe other decussating fibres of these pyramids; and they suggestthat a crossing for sensation probably exists there. Admittingthat they are right, these conductors of sensitive impressionswould pass into the anterior pyramids, and they themselvesstate that it must be so. We will show, in the lecture on themedulla, oblongata, that this view is in opposition to positivefacts, and particularly the celebrated case of alteration of theanterior pyramids which has been recorded by our friend Pro.fessor Lebert.We think that the case of Dr. Annan, if we take into account
the extent of the injury in the medulla oblongata, bears cutclearly that most if not all of the conductors of sensitive im-pressions from the trunk and limbs make their decussation inthe spinal cord. But the importance of this case is not limitedto this demonstration: it shows at once the radical differencebetween the symptoms of an alteration of a lateral half of themedulla oblongata above the crossing of the pyramids, and analteration of a lateral half of the spinal cord either in the cer-vical or in another region. In this last case, as we have showna moment ago, there is loss of movement in one side and lossof sensibility in the opposite side; while in a case of alterationabove the crossing of the pyramids, we find that the loss ofmovement and of sensibility are both in the opposite side.This case is also excellent to show that the functions attributedto the restiform body as a conductor of sensitive impressions,and to the cerebellum as either a centre of perception of theseimpressions, or as a regulator of our voluntary movements, oras a centre for the guiding sensation, whether by a reflex actionor otherwise, are not performed by these parts, as the commu-nication between the cerebellum and the right side of the bodythrough the right side of the medulla oblongata was almostimpossible, a small part of the right restiform body remaining,and sensibility and voluntary movements being preserved inthis side.
In the following case, which is related by Broussais, we find,with less detail, many of the features of the preceding one.CASE 39.-An officer, recovered for some time, after having
been attacked with stupor, vomiting, &c.; but, five monthsafterwards, hemiplegia gradually appeared in the right side :the leg could support him a little ; the arm lost both movementand feeling. Soon after, the lift eye lost its transparency andbecame atrophied; the left eyelids were paralysed. A fewweeks after, walking was still more difficult, and speech moreimpeded, and death occurred after coma.

297
Autopsy.-The left hemisphere was softened; cerebellumnormal. At the upper part of the medulla oblongata, in theinterior of the left pyramidal body there was a canceroustumour, the size of a chesnut, in continuity with the surround-ing nervous tissue. (Broussais, in "Traité des PhlegmasiesChroniques," troisime ed.; 1822, p. 420.)The state of sensibility of the right lower extremity is not
mentioned, but we find that there was loss of feeling in theright upper limb, and a tumour in the right upper extremity,showing that the decussation of the conductors of sensitive im-pressions must have taken place below the point injured-i. e.,in the spinal cord or the lower part of the medulla oblongata.Now, as there is no proof that there is such a decussation inthis part of this nervous centre ; and as, on the contrary, thereare facts in opposition to the view that there is such a cross-ing, we must admit that it exists in the spinal cord. The samething may be concluded from a case of M. Carre (Archives de-kgdecii2e, p. 234, vol. v., 1834), in which a cancerous tumourin the left half of the pons Varolii, extending several lines in themedulla oblongata and the crus cerebri, had produced paralysisof movement and sensibility on the right side of the body, theleft side remaining in the normal state. Nearly the same thingexisted in a case of Friedreich, (" Beitraege zur Lehre von denideschwiilsten iunerhalb der Schaedelhohle," 1853, p. 29). Thefollowing case leads also to the same conclusions :
CASE 40.-A young Pole, after a nervous fever, became para-lysed of sensibility and movement in the left side of the body,.and in the right side of the face.Autopsy.-The right side of the pons Varolii is twice its
Tiormal size; it extends forwards and backwards, where itpasses under the right olive, compressing the neighbouringparts. The enlargement was due to a very large clot of bloodin the right half of the pons. (M. H. Romberg, in Ee7irbue7tder Nervenkrankheiten, 1851, vol. i., part 2, pp. 198-202, andthird edition, 1857, third part, p. 923.)
In many cases of alteration of a lateral half of the ponsVarolii, the medulla oblongata not being injured, we find, also,the paralysis of movement and sensibility only in the oppositeside (excepting, however, the face, which is paralysed on thesame side.) Such cases are recorded by Gendrin, Charcellay,Greuzard, Friedreich (loco cit., p. 15), Cruveilhier,§ Dr. R.Bright, Dr. J. W. Ogle, &c. In many other cases, in which’one .half of the pons was more altered than the other, there wasparalysis and anaesthesia, in the two sides of the body, but at a,greater degree in the side opposite to the half of the pons mostinjured. Cases of this kind are recorded by Cruveilhier, Dr.R. Bright, Abercrombie (loco cit., p. 235), Hermann Romberg,*- whom we must not take for the great neuro-pathologist,Moritz Heinrich Romberg,-Grenet, Poisson, Tacheron,§§Dr. T. Inman, I1II &c.These cases assuredly show that the decussation of the con-
ductors of sensitive impressions does not take place in the ponsVarolii, and that it has taken place before they reach thisorgan, and therefore that it occurs either in the spinal cord orthe medulla oblongata-a question which is solved by the facts"we have mentioned relating to these organs. But there is.another consequence to be drawn from many of these cases : ifthe pons Varolii were a place of passage of only a part of the .conductors of sensitive impressions, most of these conductorspassing into the cerebellum from the posterior columns of thespinal cord and their continuation, the restiform bodies, wecertainly should see but a diminution, and not a complete loss,of sensibility in those cases in which an alteration is limited tothe central parts of the pons Varolii, and not interfering withthe cerebellum and its peduncles. It is usually, however, aoomplete loss of sensibility which is observed, and not a diminu-tion. The case of Greuzard, already mentioned, is particularlyinteresting in this respect: there was a softening, irregular inits shape, large, like an almond, and rose-coloured, in the in-ferior and middle part of the right half of the pons Varolii, andthe anaesthesia and paralysis of the right side of the body hadbeen complete. In a case still more interesting, and which Ishall have to relate by-and-bye for another object, there was atumour in the left half of the pons Varolii, with complete loss
* Hist. Anatom. des Inflammations, vol. ii., p. 155.t In Ollivier, loco cit., vol. ii., p. 315.Archives de Medecine, 1834, vol. v., p. 458.§ Anatomic Pathologique, livre 21.
Reports of Med. Cases, vol. ii., part 1.Edinburgh Monthly Journal of 3ledicine, March, 1855.Quasdam de Ponte Varolii, 1838, p. 17.
tt Gaz. Hebd. de Medee., Xo. 38, Sept. 1856.Bulletins de la Societe Anatom., Mai et Juin, 1855.
§§ Rech. Anat.-Pathol, sur la Medeeine Pratique, 1823 vol. iii., p. 450.Edinburgh Medical and Surgical Journal, .01. 64, 1845, p. 294.
Autopsy.-The left hemisphere was softened; cerebellumnormal. At the upper part of the medulla oblongata, in theinterior of the left pyramidal body there was a canceroustumour, the size of a chesnut, in continuity with the surround-ing nervous tissue. (Broussais, in "Traité des PhlegmasiesChroniques," troisime ed.; 1822, p. 420.)The state of sensibility of the right lower extremity is not
mentioned, but we find that there was loss of feeling in theright upper limb, and a tumour in the right upper extremity,showing that the decussation of the conductors of sensitive im-pressions must have taken place below the point injured-i. e.,in the spinal cord or the lower part of the medulla oblongata.Now, as there is no proof that there is such a decussation inthis part of this nervous centre ; and as, on the contrary, thereare facts in opposition to the view that there is such a cross-ing, we must admit that it exists in the spinal cord. The samething may be concluded from a case of M. Carre (Archives de-kgdecii2e, p. 234, vol. v., 1834), in which a cancerous tumourin the left half of the pons Varolii, extending several lines in themedulla oblongata and the crus cerebri, had produced paralysisof movement and sensibility on the right side of the body, theleft side remaining in the normal state. Nearly the same thingexisted in a case of Friedreich, (" Beitraege zur Lehre von denideschwiilsten iunerhalb der Schaedelhohle," 1853, p. 29). Thefollowing case leads also to the same conclusions :
CASE 40.-A young Pole, after a nervous fever, became para-lysed of sensibility and movement in the left side of the body,.and in the right side of the face.Autopsy.-The right side of the pons Varolii is twice its
Tiormal size; it extends forwards and backwards, where itpasses under the right olive, compressing the neighbouringparts. The enlargement was due to a very large clot of bloodin the right half of the pons. (M. H. Romberg, in Ee7irbue7tder Nervenkrankheiten, 1851, vol. i., part 2, pp. 198-202, andthird edition, 1857, third part, p. 923.)
In many cases of alteration of a lateral half of the ponsVarolii, the medulla oblongata not being injured, we find, also,the paralysis of movement and sensibility only in the oppositeside (excepting, however, the face, which is paralysed on thesame side.) Such cases are recorded by Gendrin, Charcellay,Greuzard, Friedreich (loco cit., p. 15), Cruveilhier,§ Dr. R.Bright, Dr. J. W. Ogle, &c. In many other cases, in which’one .half of the pons was more altered than the other, there wasparalysis and anaesthesia, in the two sides of the body, but at a,greater degree in the side opposite to the half of the pons mostinjured. Cases of this kind are recorded by Cruveilhier, Dr.R. Bright, Abercrombie (loco cit., p. 235), Hermann Romberg,*- whom we must not take for the great neuro-pathologist,Moritz Heinrich Romberg,-Grenet, Poisson, Tacheron,§§Dr. T. Inman, I1II &c.These cases assuredly show that the decussation of the con-
ductors of sensitive impressions does not take place in the ponsVarolii, and that it has taken place before they reach thisorgan, and therefore that it occurs either in the spinal cord orthe medulla oblongata-a question which is solved by the facts"we have mentioned relating to these organs. But there is.another consequence to be drawn from many of these cases : ifthe pons Varolii were a place of passage of only a part of the .conductors of sensitive impressions, most of these conductorspassing into the cerebellum from the posterior columns of thespinal cord and their continuation, the restiform bodies, wecertainly should see but a diminution, and not a complete loss,of sensibility in those cases in which an alteration is limited tothe central parts of the pons Varolii, and not interfering withthe cerebellum and its peduncles. It is usually, however, aoomplete loss of sensibility which is observed, and not a diminu-tion. The case of Greuzard, already mentioned, is particularlyinteresting in this respect: there was a softening, irregular inits shape, large, like an almond, and rose-coloured, in the in-ferior and middle part of the right half of the pons Varolii, andthe anaesthesia and paralysis of the right side of the body hadbeen complete. In a case still more interesting, and which Ishall have to relate by-and-bye for another object, there was atumour in the left half of the pons Varolii, with complete loss
* Hist. Anatom. des Inflammations, vol. ii., p. 155.t In Ollivier, loco cit., vol. ii., p. 315.Archives de Medecine, 1834, vol. v., p. 458.§ Anatomic Pathologique, livre 21.
Reports of Med. Cases, vol. ii., part 1.Edinburgh Monthly Journal of 3ledicine, March, 1855.Quasdam de Ponte Varolii, 1838, p. 17.
tt Gaz. Hebd. de Medee., Xo. 38, Sept. 1856.Bulletins de la Societe Anatom., Mai et Juin, 1855.
§§ Rech. Anat.-Pathol, sur la Medeeine Pratique, 1823 vol. iii., p. 450.Edinburgh Medical and Surgical Journal, .01. 64, 1845, p. 294.
of sensibility in the right side of the body. -(Stuart Cooper, in" Bulletins de la Soc. Anat.," 1846, p. 68.)In our Lecture on the Functions of the Medulla Oblongata
and Pons Varolii, we shall have to treat at length of the placeof decussation of the conductors of the orders of the will tomuscles; but we must now point out the following charac-teristic features of alterations limited to one lateral half ofthose parts :-lst, the spinal cord ; 2nd, the medulla oblongata,at the place of the crossing of the pyramids; 3rd, the ence-phalon, above this crossing.
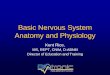
In Fig. 20 may be seen what we think to be proved by pa-thological cases in this respect:-1st. In the spinal cord analteration in a lateral half produces hyperxsthesia and para-lysis of movement in the corresponding side, behind the placeof the alteration, and the loss of sensibility, without loss ofmovement, in the opposite side. (See 3, Fig. 20.) 2nd. In thelower part of the medulla oblongata, diminution of movementin the two sides of the body, hyperaesthesia on the side altered,anaesthesia in the opposite side. (See 2, Fig. 20.) 3rd. Abovethe crossing of the pyramids, loss of movement and sensibilityin the opposite side, and hyperaesthesia with conservation ofmovement in the side of the alteration. (See 1, Fig. 20.)
of sensibility in the right side of the body. -(Stuart Cooper, in" Bulletins de la Soc. Anat.," 1846, p. 68.)In our Lecture on the Functions of the Medulla Oblongata
and Pons Varolii, we shall have to treat at length of the placeof decussation of the conductors of the orders of the will tomuscles; but we must now point out the following charac-teristic features of alterations limited to one lateral half ofthose parts :-lst, the spinal cord ; 2nd, the medulla oblongata,at the place of the crossing of the pyramids; 3rd, the ence-phalon, above this crossing.
In Fig. 20 may be seen what we think to be proved by pa-thological cases in this respect:-1st. In the spinal cord analteration in a lateral half produces hyperxsthesia and para-lysis of movement in the corresponding side, behind the placeof the alteration, and the loss of sensibility, without loss ofmovement, in the opposite side. (See 3, Fig. 20.) 2nd. In thelower part of the medulla oblongata, diminution of movementin the two sides of the body, hyperaesthesia on the side altered,anaesthesia in the opposite side. (See 2, Fig. 20.) 3rd. Abovethe crossing of the pyramids, loss of movement and sensibilityin the opposite side, and hyperaesthesia with conservation ofmovement in the side of the alteration. (See 1, Fig. 20.)
This flgure represents the decussation of the conductors forvoluntary movements, and those for sensations. a r, anteriorroots and their continuation in the spinal cord, and decussa-tion at the lower part of the medulla oblongata. m o, p r,the posterior roots and their continuation and decussation inthe spinal cord. g, g, the ganglions of these roots. Thearrows indicate the direction of the nervous action. r, theright side. l, the left side. 1, 2, 3, indicate places of altera-tion in a lateral half of the spino-cerebral axis, to show theinfluence on the two kinds of conductors in the three placesmentioned in the text.
This flgure represents the decussation of the conductors forvoluntary movements, and those for sensations. a r, anteriorroots and their continuation in the spinal cord, and decussa-tion at the lower part of the medulla oblongata. m o, p r,the posterior roots and their continuation and decussation inthe spinal cord. g, g, the ganglions of these roots. Thearrows indicate the direction of the nervous action. r, theright side. l, the left side. 1, 2, 3, indicate places of altera-tion in a lateral half of the spino-cerebral axis, to show theinfluence on the two kinds of conductors in the three placesmentioned in the text.
I ELECTRICITY I:Y SURGICAL OPERATIONS.-It may beinteresting to our readers to hear that some observations havebeen made during the last few days, by Mr. Marshall, at theUniversity College Hospital, on the efficacy of the electric cur-rent in benumbing parts submitted to surgical operations bythe knife,-the idea involved in these trials being, of course,derived from its alleged advantages in tooth-drawing. As
many as nine operations requiring incisions of various kinds,including cases of abscess, carbuncle, and the removal of anadipose tumour, have been performed between the 9th and14th of September. Excepting where the current employedappeared to be too strong, the pain of the incisions appears onthe whole to have been so modified as to be more bearable thanis usually the case. In one instance, that of the adiposetumour, the cuts were very slightly painful. There was noinstance, however, of complete anaesthesia; and it would bepremature to flatter ourselves that, in regard to the effects ofelectricity in cutting operations, anything more than a modi-fving influence had yet been certainly obtained
I ELECTRICITY I:Y SURGICAL OPERATIONS.-It may beinteresting to our readers to hear that some observations havebeen made during the last few days, by Mr. Marshall, at theUniversity College Hospital, on the efficacy of the electric cur-rent in benumbing parts submitted to surgical operations bythe knife,-the idea involved in these trials being, of course,derived from its alleged advantages in tooth-drawing. As
many as nine operations requiring incisions of various kinds,including cases of abscess, carbuncle, and the removal of anadipose tumour, have been performed between the 9th and14th of September. Excepting where the current employedappeared to be too strong, the pain of the incisions appears onthe whole to have been so modified as to be more bearable thanis usually the case. In one instance, that of the adiposetumour, the cuts were very slightly painful. There was noinstance, however, of complete anaesthesia; and it would bepremature to flatter ourselves that, in regard to the effects ofelectricity in cutting operations, anything more than a modi-fving influence had yet been certainly obtained