Embed Size (px)
Citation preview
ASTHMA UPDATE 0889-8561/96 $0.00 + .20
COST AND COST-EFFECTIVENESS IN ASTHMA
Use of Pharmacoeconomics to Assess the Value of Asthma Interventions
Sean D. Sullivan, PhD
Substantial medical care costs to patients, their families, and society are incurred for the management of asthma and its related morbidity. Aside from the considerable expenditures for medical treatments, chronic illnesses like asthma impart additional economic consequences in terms of work and school absence, work productivity loss, caregiver costs, and premature mortality. Estimates of the economic burden of asthma reflect a chronic disease that is often costly to manage and disproportionately expensive in persons with severe illness.
The sizable economic impact of managing chronic disease has sensi- tized medical decision makers, public and private payers, and society to the problem of scarce resources and to the need to make more cost- efficient treatment choices. For the payer or provider operating within a limited budget, the scarcity of medical resources means that dollars spent on new treatments must be reallocated from other medical uses. Resources for new acute, chronic, or preventive treatments for asthma must be derived from other sources, either externally from additional medical benefits premiums or internally from other medical conditions and treatments. In the face of resource limitations physicians and other health care professionals are looking toward outcomes research and cost- effectiveness studies to assist in the adoption and selection of asthma management strategies. The choice of treatment strategy now must
From the Departments of Pharmacy and Health Services, University of Washington, Seattle, Washington
IMMUNOLOGY AND ALLERGY CLINICS OF NORTH AMERICA
VOLUME 16 * NUMBER 4 NOVEMBER 1996 819
820 SULLIVAN
balance the strain between providing all medical services that are techni- cally feasible or that patients desire and financing these services with limited resources.12
The results from cost-effectiveness studies are intended to improve the quality of clinical and financial decision-making on the part of health plans and treating clinicians by providing information on the relationship between treatment choices, health outcomes, and the overall cost of medical care. As part of health plans that actively manage patient care, the acceptance of medical innovation is determined increasingly by technology adoption committees that make use of drug and device formularies, practice and treatment guidelines, prior approval, and case and disease management programs.lq Health economic and outcomes studies support rational decision-making by informing the development and periodic refinement of these policies.
Decisions about the use of asthma treatments are likely to involve the need for data on costs and cost-effectiveness, necessitating a better understanding of the burden of asthma and the relative cost-effective- ness of various asthma treatments. These data are necessary to promote better clinical and financial decision-making. This article informs the reader about the nature and extent of the economic burden of asthma and describes the literature on the cost-effectiveness of many of the major treatment choices for asthma.
THE PRINCIPLES OF PHARMACOECONOMICS
It is now well known that consumers and purchasers of medical treatments are sensitive to the overall costs of medical care in relation to the health benefits that treatments confer. Both want value for money. Medical care purchasers and formulary committees acting as agents for the populations they serve are rightly focused on total medical care resource requirements for management of disease. Pharmacoeconomic studies can be used to determine and quantify the costs, clinical out- comes, and quality of life consequences of alternative treatment strate- gies for a given illness or condition, thereby informing the process of technology adoption." Integrating data on the costs and outcomes of therapy alternatives into a single and comprehensive analysis is the goal of pharmacoeconomic studies. From the perspective of the payer, the practical purpose of such studies is to estimate the additional cost of new technology relative to additional benefits. The evaluation of medical treatments should incorporate data on the clinical consequences (efficacy and safety) and the costs and relative cost-effectiveness of treatment alternatives.* Unfortunately, despite the obvious need for such informa- tion, little pharmacoeconomic evidence is,available on alternative asthma management strategies.
The particular research methods that comprise the evolving field of pharmacoeconomics are quite well described." Each provides certain information on the impact of disease or the relative value of treatments.
COST AND COST-EFFECTIVENESS IN ASTHMA 821
The following section describes each method in the context of asthma and asthma management.
Cost-of-Illness Approach
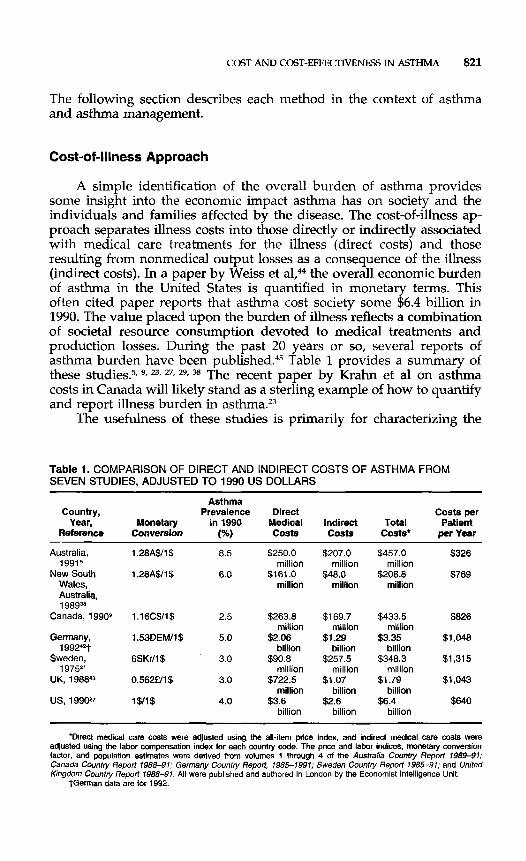
A simple identification of the overall burden of asthma provides some insight into the economic impact asthma has on society and the individuals and families affected by the disease. The cost-of-illness ap- proach separates illness costs into those directly or indirectly associated with medical care treatments for the illness (direct costs) and those resulting from nonmedical output losses as a consequence of the illness (indirect costs). In a paper by Weiss et a1,@ the overall economic burden of asthma in the United States is quantified in monetary terms. This often cited paper reports that asthma cost society some $6.4 billion in 1990. The value placed upon the burden of illness reflects a combination of societal resource consumption devoted to medical treatments and production losses. During the past 20 years or so, several reports of asthma burden have been published.45 Table 1 provides a summary of these studies? 9, 27, 29, 38 The recent paper by Krahn et a1 on asthma costs in Canada will likely stand as a sterling example of how to quantify and report illness burden in asthma.23
The usefulness of these studies is primarily for characterizing the
Table 1. COMPARISON OF DIRECT AND INDIRECT COSTS OF ASTHMA FROM SEVEN STUDIES, ADJUSTED TO 1990 US DOLLARS
Asthma Country, Prevalence Direct Costs per
Year, Monetary in 1990 Medical Indirect Total Patient Reference Conversion 1%) Costs Casts Costs* DerYear
Australia, 1.28A$/l$ 8.5 $250.0 $207.0 $457.0 $326
New South 1.28A$/l$ 6.0 $161.0 $48.0 $200.8 $769 19915 million million million
Wales, million million million Australia, 1 98g3*
Canada, 1990g 1.16C$/1$ 2.5 $263.8 $1 69.7 $433.5 $826
Germany, 1.53DEM/1$ 5.0 $2.06 $1.29 $3.35 $1,048
Sweden, 6SKr/l$ 3.0 $90.8 $257.5 $348.3 $1,315
million million million
1992-t billion billion billion
19752' million million million
million billion billion
billion billion billion
UK, 198843 0.562€/1$ 3.0 $722.5 $1.07 $1.79 $1,043
US, 1990'7 1$/1$ 4.0 $3.6 $2.6 $6.4 $640
"Direct medical care costs were adjusted using the all-item price index, and indirect medical care costs were adjusted using the labor compensation index for each country code. The price and labor indices, monetary conversion factor, and population estimates were derived from volumes 1 through 4 of the Australia Countiy Report 1989-91; Canada Country Report 1988-91; Germany Country Report, 1985-1991; Sweden Country Repoti 1985-91; and United Kingdom Country Report 198&91. All were published and authored in London by the Economist Intelligence Unit.
tGerrnan data are for 1992.
822 SULLIVAN
underlying burden of illness and for amplifying the policy importance of a particular disease state. Benchmarking disease costs and underlying components of care can highlight the need for additional study and point to areas in which treatments and treatment strategies may be most effective. For instance, the Weiss et a1 report showed that more than 50% of all medical care expenditures for asthma were for emergent care. These data focused attention on the need to reduce the frequency of high cost hospital and emergency department use among asthmatic patients.
Importantly, cost-of-illness studies cannot be used to assess the impact of interventions or treatments on the costs of care. For this purpose, evaluative methods such as cost-benefit and cost-effectiveness analysis are needed.
Cost-Identification Method
The least complicated method of phannacoeconomic analysis is cost identification or cost minimization, which involves a comprehensive assessment of the costs of alternative treatment strategies. This technique is valid only when the health outcomes are so similar that a formal analysis of health outcomes would indicate no statistically or clinically significant difference among treatment groups. An example might be a cost comparison of two asthma drug treatments that are considered to be equally effective at relieving asthma symptoms, but one may be more expensive to deliver because of difficulty in titration or dose monitoring. In many cases, comparative cost-identification studies may not be appro- priate; costs may differ because of differences in compliance or utiliza- tion of expensive health care resources associated with differences in patient preferences or adverse consequences. Thus observed cost differ- ences often are a subtle consequence of differences in treatment effective- ness.
Cost-Benefit Analysis
Cost-benefit analysis allows for the identification, valuation, and comparison of the costs associated with the implementation or use of a medical program or technology and the benefits derived from its appl icat i~n.~~ Both costs and benefits are defined in monetary terms and time preference-adjusted to net present values. The results of these studies are usually reflective of a wider societal point of view. Thus the analysis considers both private and social costs and benefits. The ratio of monetary benefits to overall costs provides a way to determine whether the value produced by the technology is worth the cost strictly in financial terms: The intervention is said to be cost beneficial if the benefit-to-cost ratio exceeds a value of 1.0. Many technical, social, and ethical problems, however, are associated with expressing all health
COST AND COST-EFFECTIVENESS IN ASTHMA 823
outcomes in monetary terms. Difficulty arises when the benefits of the intervention are not amenable to economic valuation, such as years of life saved or improvements in psychosocial outcomes. In health eco- nomic problems it is often difficult to value health improvements in monetary terms. Economists rely on revealed preferences in actual mar- kets or on hypothetical estimations derived from willingness-to-pay studies.21 While analysts may prefer this technique from a conceptual point-of-view, cost-benefit analyses tend to be used less widely in the field of pharmacoeconomics because of numerous practical limitations.
Cost-Effectiveness Analysis
The most common health economic evaluation technique is cost- effectiveness analysis. This approach simultaneously considers the rela- tive costs and outcomes of two or more alternative medical technologies when used to treat a similar condition.43 Like cost-benefit analysis, the cost-effectiveness technique makes explicit the positive and negative costs and consequences of various medical technologies. Cost-effective- ness analysis differs from cost-benefit analysis, however, in that the health outcomes of treatments are expressed in "natural" units such as symptom-free days or quality-adjusted years of life saved and not in monetary terms. A cost-effectiveness evaluation requires estimation of two inputs from the comparator technologies: (1) a direct measure or proxy of absolute and comparative health outcome or effectiveness and (2) an estimate of total medical costs. From these data an incremental cost-effectiveness ratio can be estimated such that:
Cost (A) - Cost (B) Incremental Cost/Effectiveness Ratio = Effectiveness (A) - Effectiveness (B)
The incremental cost of treatment A compared with treatment B is determined in the numerator of the equation to reflect any additional medical care expenditures associated with the use of treatment A relative to B. A similar estimate is made of the incremental health benefit or effectiveness of treatment A compared with treatment B. The estimates of incremental cost and benefits attributable to the two treatments then are expressed as a ratio of cost to benefit. As will be seen later, a frequently produced cost-effectiveness ratio for the comparison of two asthma treatments is the incremental cost per symptom-free day gained.
In cost-effectiveness analysis, as in other economic evaluation tech- niques, costs are evaluated comprehensively and not limited solely to measurement of the cost of therapy. For example, if only the costs of medications are assessed in an evaluation of drug therapy for asthma, a number of important economic parameters will be disregarded. These may include the direct costs associated with the use of medical resources to treat sigruficant adverse reactions to the drug or the savings that result from averted hospitalization and emergency department visits due to improved clinical outcome. Furthermore, important noneconomic
824 SULLTVAN
factors, such as improvements in functional status and changes in quality of life, also will be ignored.
Cost-effectiveness analysis is grounded in the clinical effectiveness of the interventions; thus, the clinical effects of an intervention and its most likely alternatives must be understood clearly before cost- effectiveness hypotheses can be generated and tested. An important feature of cost-effectiveness analysis is its inherently comparative nature. One of the fundamental concepts underlying cost-effectiveness analysis is that of ”opportunity costs,” which states that the true economic cost of an intervention is the value of the alternative interventions that are foregone. This implies that choices always must be made among interventions and that an intervention can never be evaluated in isola- tion. At the very least, in a cost-effectiveness analysis, the intervention should be compared with usual care or “no treatment.”
Cost-Utility Analysis
Cost-utility analysis is a special form of the cost-effectiveness model in which the health outcomes are expressed in quality-adjusted life years (QALY) gained. The quality adjustment is derived from preference weights or health utilities.39a The advantages of a cost-utility study are (1) a QALY captures simultaneously changes in mortality and morbidity and is applicable to all disease states and treatments, (2) a QALY consid- ers patient preferences for health outcomes, and (3) important to ana- lysts, cost-utility analyses conform to normative theory of decision- making under uncertainty?’
These studies have a conceptual appeal to researchers and are the most ideal for use in decision-making because they capture important outcomes to clinicians and patients and because cost-utility results can be used to compare treatments across different disease states. Technical limitations in measurement of preferences and a lack of long-term data concerning asthma interventions, however, severely limit the use of this approach for the study of asthma treatments.
The Outcomes of Cost-Effectiveness Studies
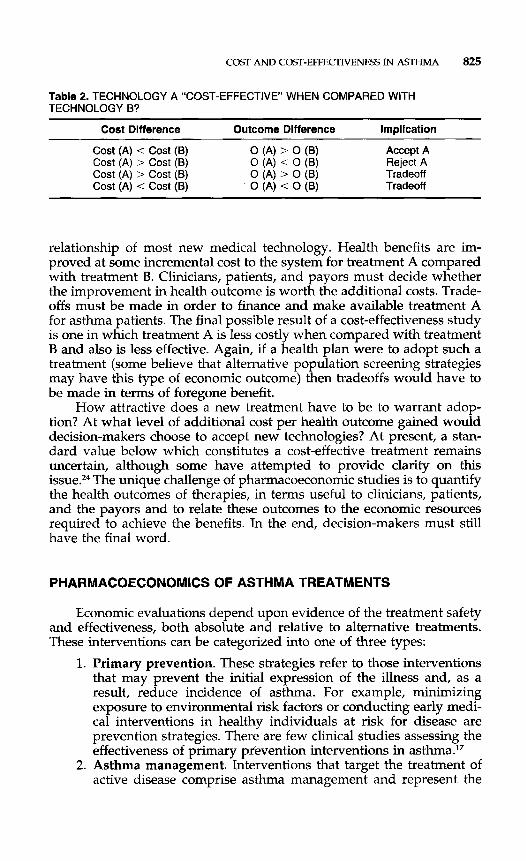
The possible outcomes of a cost-effectiveness study comparing asthma treatment A with asthma treatment B are illustrated in Table 2.13
When the overall cost of treatment A is less than treatment B and the health outcomes associated with treatment A are greater than for treat- ment B, treatment A is said to be ”dominant” and should be adopted by providers and purchasers. The introduction of these treatments is most desirable from a system efficiency standpoint, but is rarely found in practice. On the other hand, if treatment A is m6re costly and provides reduced health benefits when compared with treatment B, the new technology should be rejected. Most new asthma treatments are not like these two examples. The third row of Table 2 shows the cost-outcome
COST AND COST-EFFECTIVENESS IN ASTHMA 825
Table 2. TECHNOLOGY A “COST-EFFECTIVE’ WHEN COMPARED WITH TECHNOLOGY B?
Cost Difference Outcome Difference Implication ~~~ ~ ~
Accept A Reject A Tradeoff Trade off
Cost (A) < Cost (B) Cost (A) > Cost (B) Cost (A) > Cost (B) Cost (A) < Cost (B)
0 (A) ’ 0 (8) 0 ( 4 < 0 (B) 0 ( 4 > 0 (B) 0 (A) < 0 (B)
relationship of most new medical technology. Health benefits are im- proved at some incremental cost to the system for treatment A compared with treatment B. Clinicians, patients, and payors must decide whether the improvement in health outcome is worth the additional costs. Trade- offs must be made in order to finance and make available treatment A for asthma patients. The final possible result of a cost-effectiveness study is one in which treatment A is less costly when compared with treatment B and also is less effective. Again, if a health plan were to adopt such a treatment (some believe that alternative population screening strategies may have this type of economic outcome) then tradeoffs would have to be made in terms of foregone benefit.
How attractive does a new treatment have to be to warrant adop- tion? At what level of additional cost per health outcome gained would decision-makers choose to accept new technologies? At present, a stan- dard value below which constitutes a cost-effective treatment remains uncertain, although some have attempted to provide clarity on this issue.” The unique challenge of pharmacoeconomic studies is to quantify the health outcomes of therapies, in terms useful to clinicians, patients, and the payors and to relate these outcomes to the economic resources required to achieve the benefits. In the end, decision-makers must still have the final word.
PHARMACOECONOMICS OF ASTHMA TREATMENTS
Economic evaluations depend upon evidence of the treatment safety and effectiveness, both absolute and relative to alternative treatments. These interventions can be categorized into one of three types:
1. Primary prevention. These strategies refer to those interventions that may prevent the initial expression of the illness and, as a result, reduce incidence of asthma. For example, minimizing exposure to environmental risk factors or conducting early medi- cal interventions in healthy individuals at risk for disease are prevention strategies. There are few clinical studies assessing the effectiveness of primary prevention interventions in asthma.17
2. Asthma management. Interventions that target the treatment of active disease comprise asthma management and represent the
826 SULLIVAN
most studied area of asthma care, particularly from the clinical outcomes perspective. These interventions are designed to reduce the severity or duration of morbidity associated with asthma, principally the prevention of symptoms and exacerbations. The most notable treatment options available to clinicians are the pharmacotherapeutic agents. Other examples include asthma management and education programs directed at physicians and patients, medical devices such as spacers and peak flow meters, changes in the delivery of medical care for people with asthma, and environmental programs aimed at reducing exposure to known risks such as house-dust mites, secondary smoke, or cat dander. The "Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma" summarized most of the key clini- cal efficacy studies in the area of asthma management.30 The literature is dominated by placebo-controlled studies of medica- tions.
3. Emergency care. These interventions often imply the need for immediate, advanced, high-cost medical care treatments. Patients requiring these interventions present with status asthmaticus, respiratory failure, progressive lung deterioration, or some other form of life-threatening severe disease. Typically, these patients are treated in emergency departments or hospital settings where multiple technologies (e.g., mechanical ventilation, intensive care, drug therapy) are used.
The few resources expended for research on the economic impact of asthma interventions have been in the area of medications or for asthma education/management programs. No economic study has been conducted on primary prevention, and very few studies have been undertaken for emergency care strategies. Indeed, estimating the value of primary prevention strategies presents a unique challenge to research- ers. The outcomes and cost impact of prevention often require several years of observation and many patients. In addition, it is difficult to state with certainty that the poor health state actually was prevented. At the same time, the amount of resources required to implement large- scale prevention programs is considerable, especially in the first few years, but declines as efficiencies are gained.
THE ECONOMICS OF PHARMACOTHERAPY
Although relatively few economic evaluations of asthma pharmaco- therapy have been performed, there is increasing interest in this area, particularly by pharmaceutical manufacturers and health benefit payers. A major reason for this increased attention is the possible market advan- tage gained over a competitor if both clinical and economic benefits are established. In the case of the payer, clinical and resource decisions are likely to be improved with the availability of pharmacoeconomic
COST AND COST-EFFECTIVENESS IN ASTHMA 827
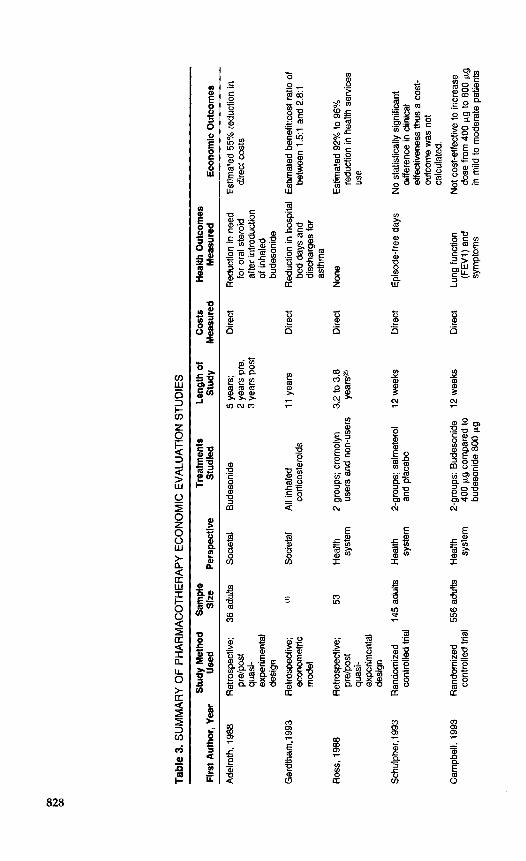
information. Table 3 summarizes the important pharmacoeconomic eval- uations of asthma pharmacotherapy.
Inhaled Corticosteroids
Evidence is overwhelming for the positive clinical effects of combin- ing inhaled corticosteroids with bronchodilator therapy for the manage- ment of asthma? The therapeutic management guidelines of the Expert Panel Report recommend as initial treatment such combination therapy for persons with moderate-to-severe asthma.3O Adding expensive, in- haled corticosteroid medications to an existing regimen of inhaled or oral bronchodilator therapy, however, contributes sigruficantly to the overall cost of treating asthma in these patients. An important, and as yet not fully explored, research question is “Are inhaled corticosteroids in combination with bronchodilators cost effective compared with bron- chodilators alone when used to treat persons with either mild-to-moder- ate or moderate-to-severe asthma?”
The first evidence of the cost beneficial effects of inhaled budesonide on health services outcomes was reported in a letter by Adelroth and Thompson.’ The authors showed the relationship between use of high- dose inhaled budesonide (800 p,g/d) and asthma-related inpatient hospi- tal days in 36 oral steroid-dependent patients with asthma during a 5- year period. The analysis used a pre-post, quasi-experimental study design in which patients served as their own controls. A dramatic reduction in inpatient admissions, days, and costs was observed in patients on budesonide when compared with the previous 2 years on oral steroid therapy. Cost per patient declined by more than 55% per year for up to 3 years after the initiation of inhaled budesonide.
Gerdtham and colleagues16 built on Adelroth and Thompson’s initial work in Sweden by constructing a pooled, time-series economic model to determine the association between greater use of inhaled corticoste- roids and asthma-related hospital days in 14 counties over an ll-year period, again using a nonexperimental methodology. More than 80% of inhaled corticosteroid use during this time was with budesonide. Al- though not a true cost-benefit analysis, the authors did show a strong negative association between use of inhaled corticosteroids and hospital- bed-days for asthma. An approximate cost-benefit ratio was developed from the multivariate models suggestive of positive economic benefits in excess of costs on the order of between 1.5:l.O and 2.8:1.0, depending on the analytic model.
The lack of experimental design in the study by Gerdtham and colleagues and the very small sample size of the Adelroth and Thomp- son study restrict the internal validity and conclusions of these two studies. These studies make use of an alternative evaluation strategy, however, wherein the authors attempt to measure population effective- ness of the inhaled product in the absence of the constraints of a
i3 m
Tab
le 3. S
UM
MA
RY
OF
PH
AR
MA
CO
THE
RA
PY
EC
ON
OM
IC E
VA
LUA
TIO
N S
TUD
IES
Firs
t Aut
hor,
Year
U
sed
Siz
e P
ersp
ectiv
e S
tudi
ed
Stu
dy
Mea
sure
d M
easu
red
Eco
nom
ic O
utco
mes
S
tudy
Met
hod
Sam
ple
Trea
tmen
ts
Leng
th o
f C
osts
H
ealth
Out
com
es
Ade
lroth
, 198
8
Ger
dtha
m,l9
93
Ros
s, 1
988
Sch
ulph
er,l9
93
Cam
pbel
l, 19
93
Ret
rosp
ectiv
e;
36 a
dults
S
ocie
tal
Bud
eson
ide
pre/
post
qu
asi-
expe
rimen
tal
desi
gn
econ
omet
ric
corti
cost
eroi
ds
mod
el
Ret
rosp
ectiv
e;
OJ
Soc
ieta
l A
ll in
hale
d
Ret
rosp
ectiv
e;
53
Hea
lth
2 gr
oups
; cro
mol
yn
pre/
post
sy
stem
us
ers
and
non-
user
s qu
asi-
expe
rimen
tal
desi
gn
cont
rolle
d tri
al
syst
em
and
plac
ebo
Ran
dom
ized
14
5 ad
ults
H
ealth
2-
grou
ps; s
alm
eter
ol
Ran
dom
ized
55
6 ad
ults
H
ealth
2-
grou
ps: B
udes
onid
e co
ntro
lled
trial
sy
stem
40
0 pg
com
pare
d to
bu
deso
nide
800
pg
5 ye
ars;
2
year
s pr
e,
3 ye
ars
post
11 y
ears
3.2
to 3
.8
year
s",
12 w
eeks
12 w
eeks
Dire
ct
Dire
ct
Dire
ct
Dire
ct
Dire
ct
Red
uctio
n in
nee
d fo
r or
al s
tero
id
dire
ct c
osts
af
ter
intro
duct
ion
of in
hale
d bu
deso
nide
bed
days
and
di
scha
rges
for
asth
ma
Est
imat
ed 5
5% re
duct
ion
in
Red
uctio
n in
hos
pita
l E
stim
ated
ben
efit:
cost
ratio
of
betw
een
1.51
and
2.8
:l
Non
e
Epi
sode
-free
days
Lung
func
tion
(FE
W) a
nd
sym
ptom
s
Est
imat
ed 9
2% to
96%
re
duct
ion
in h
ealth
sew
ices
us
e
No
stat
istic
ally
sig
nific
ant
diffe
renc
e in
clin
ical
ef
fect
iven
ess
thus
a c
ost-
outc
ome
was
not
ca
lcul
ated
.
dose
from
400
Fg
to 8
00 p.g
in m
ild to
mod
erat
e pa
tient
s
Not
cos
t-effe
ctiv
e to
incr
ease
Con
nett,
199
3 R
ando
miz
ed
40 c
hild
ren
Soc
ieta
l co
ntro
lled
trial
Rut
ten-
van
MiT
lken,
R
ando
miz
ed
116
Soc
ieta
l 19
93
cont
rolle
d tri
al
child
ren
Rut
ten-
van
Mdl
ken,
R
ando
miz
ed
274
adul
ts
Soc
ieta
l 19
95
cont
rolle
d tri
al
Per
era,
199
5 U
ncon
trolle
d 86
chi
ldre
n S
ocie
tal
pre/
post
tria
l
2-gr
oups
: Bud
eson
ide
26 w
eeks
co
mpa
red
to p
lace
bo
2-gr
oups
: Bud
eson
ide
3 ye
ars(
3)
and
salb
utam
ol,
salb
utan
ol a
lone
3-gr
oups
: 2.
5 ye
ars
Bec
lom
etha
sone
an
d te
rbut
alin
e,
ipra
tropi
um a
nd
terb
utal
ine,
te
rbut
alin
e al
one
Bec
lom
etha
sone
, B
udes
onid
e
2-gr
oups
: 4
year
s
Dire
ct a
nd
indi
rect
Dire
ct a
nd
indi
rect
Dire
ct a
nd
indi
rect
Dire
ct
Lung
func
tion
(FE
VI)
, sy
mpt
oms,
sy
mpt
om-fr
ee
days
Lung
func
tion
(FE
W),
sym
ptom
- fre
e da
ys, s
choo
l ab
senc
es
Lung
func
tion
(FE
W, P
C20
), sy
mpt
om-fr
ee
days
Trea
tmen
t sa
tisfa
ctio
n, a
cute
se
vere
atta
cks,
br
eakt
hrou
gh
whe
ezin
g, a
nd
scho
ol lo
ss
Dom
inan
t the
rapy
; sav
ed
abou
t $9.
43 p
er s
ympt
om-
free
day
gain
ed
Cos
t-effe
ctiv
e; $
83 p
er 1
0%
impr
ovem
ent i
n F
EV
I, $4
.75
per s
ympt
om-fr
ee d
ay
gain
ed
Cos
t-effe
ctiv
e; $2
01 p
er 1
0%
impr
ovem
ent i
n F
EW
, $5
per
sym
ptom
-free
day
ga
ined
Est
imat
ed a
n 82
% r
educ
tion
in m
ean
mon
thly
trea
tmen
t co
sts
(1) U
nit o
f an
alys
is is
cou
ntie
s an
d no
t per
sons
. The
stu
dy r
epre
sent
s a
tota
l of
71%
of
the
Sw
edis
h po
pula
tion.
(2)
Cro
mol
yn u
sers
con
tribu
ted
3.2
year
s of
dat
a an
d no
nuse
rs o
f cro
mol
yn c
ontri
bute
d 3.
8 ye
ars
of d
ata.
(3)
The
stu
dy h
ad a
pla
nned
3 y
ear f
ollo
w-u
p bu
t onl
y 39
pat
ient
s re
ache
d a
follo
w-u
p pe
riod
of 2
2 m
onth
s.
830 SULLIVAN
clinical study design. The strength of the conclusions by Gerdtham and colleagues lies in the longitudinal and generalizable nature of the data.
The results from these two studies suggest a favorable economic impact of budesonide. Similar reductions in inpatient care have been associated with use of high-dose inhaled beclomethasone dipropionate in people with chronic asthma.22 This study lacked any direct economic valuation, however.
Six recent economic studies have used experimental research de- signs to investigate the cost-effectiveness of inhaled corticosteroids. Campbell and coworkers7 reported on the cost-effectiveness of increasing the daily dose of inhaled budesonide from 400 to 800 pg after 6 weeks in patients with mild-to-moderate asthma. Data from a 12-week random- ized trial of 556 patients ages 14 to 84 years were used in the analysis. The efficacy of increasing the dose of inhaled budesonide in these patients was reported elsewhere and indicated that 800 pg/d of bude- sonide failed to further improve lung function or reduce symptoms when compared with 400 The total cost of treatment (medication only) was estimated to be f3,108 (about $4,660 US) in the 400 pg/d group (12 weeks) compared with €4,662 (about $6,993 US) in both the 400 pg/d (6 weeks) and 800 Fg/d (6 weeks) groups. The authors concluded that increasing the dose of budesonide from 400 to 800 pg/d is not a cost-effective strategy in patients with mild-to-moderate asthma.
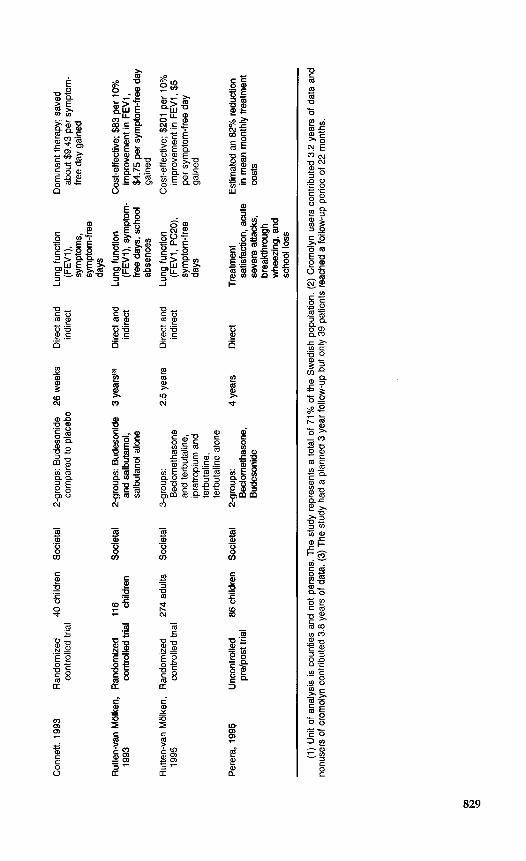
In a somewhat longer study, Connett and colleagues1o studied the cost-effectiveness of inhaled budesonide compared with placebo in a 6- month randomized trial of 40 children 1 to 3 years of age with asthma with persistent symptoms. The outcome results indicated that budeson- ide produced a favorable clinical response, increasing symptom-free days when compared with placebo (195 vs. 117 days). Direct medical costs (including the cost of budesonide) and indirect costs were tabu- lated for the numerator of the cost-effectiveness ratio. The results sug- gested that budesonide is a dominant therapy, that is, compared with placebo, budesonide increases overall effectiveness and reduces overall costs by €6.33 (about $9.45 US) per symptom-free day gained.
Rutten-van Molken and associatesN reported on the cost-effective- ness of adding inhaled corticosteroid to as-needed beta,-agonist com- pared with as-needed beta2-agonist alone in a 12-month randomized trial of 116 children 7 to 16 years of age with asthma.34 The investigators evaluated FEV, as the primary outcome. Frequency of symptom-free days and the number of school absences were included as secondary outcome measures. Patients randomized to inhaled corticosteroid plus as-needed beta,-agonist experienced significantly better lung function (FEV,), increased symptom-free days and reduced days missed from school relative to as-needed beta,-agonist alone. Computation of the cost-effectiveness ratio indicated that, when compared with beta2-agonist alone, beta,-agonist plus inhaled corticosteroid increased FEV, by 10% at an additional total cost of about $83 US. The additional cost of beta,- agonist plus inhaled corticosteroid was about $4.75 US per symptom- free day gained. In this study, addition of inhaled corticosteroid to a
COST AND COST-EFFECTIVENESS IN ASTHMA 831
treatment regimen of inhaled beta,-agonist was more effective than beta,-agonist alone but at an additional cost, the value of which de- pended on whether the outcome was improved lung function (FEV,) or better symptom control.
In the largest and most comprehensive study to date, Rutten-van Molken and analyzed data from a randomized trial of 274 adult participants (ages 18 to 60 years) in an effort to investigate the costs and effects of adding inhaled anti-inflammatory therapy to existing inhaled beta,-agonist. Patients were selected for inclusion if they met the age criteria and had diagnosed moderately severe obstructive airway disease defined by pulmonary function criteria. The patients were of mixed diagnosis and could be enrolled if they had either asthma or chronic obstructive pulmonary disease. Patients were randomized to fixed-dose inhaled terbutaline plus inhaled placebo (BA + PL), inhaled terbutaline plus 800 pg/d of inhaled beclomethasone (BA+CS), or in- haled terbutaline plus inhaled ipratropium bromide 160 pg/d (BA + AC). Patients were followed for up to 2.5 years or until premature withdrawal.
The economic objective of this study was to determine if additional treatment costs of the combination therapies were outweighed or justified by additional clinical benefits and reduced utilization of other health care services. The clinical results suggested that addition of the inhaled corticosteroid to fixed-dose terbutaline led to a significant im- provement in pulmonary function (FEV, and PC20) and symptom-free days, whereas addition of the inhaled ipratropium bromide to fixed- dose terbutaline produced no significant clinical benefits over placebo. The average annual monetary savings associated with the use of inhaled corticosteroid were not offset by the increase in costs from the average annual price of the inhaled product. The incremental cost-effectiveness ratio for inhaled corticosteroid was $201 per 10% improvement in FEV, and $5 per symptom-free day gained. It was not appropriate to evaluate the incremental cost effectiveness of ipratropium bromide because of the lack of clinical benefit relative to placebo. In many ways, this study represents a model for pharmacoeconomic analysis in asthma. The re- source and cost estimates are clear and precise, the study period is sufficiently long, and the analytic techniques are appropriate. The mixed population of asthma and chronic obstructive pulmonary disease pa- tients, however, limits the utility of these data for decision-making for asthma treatment.
In a paper by Perera;, 86 moderate-to-severe asthmatic children previously unexposed to inhaled steroid were assigned randomly to either inhaled beclomethasone dipropionate or inhaled budesonide and followed for clinical efficacy and economic outcomes for 4 years. Patients served as their own controls in the quasi-experimental study, and none of the patients were lost to follow-up during the period of the study. Statistically significant improvements in breakthrough wheezing, hospi- tal admissions, acute severe attacks, and loss of school days were ob- served in both treatment groups when compared with pretreatment
832 SULLIVAN
values. Cost impact was estimated using a pre/post cost-of-illness ap- proach. That is, average costs were determined for the period prior to treatment and for a similar period following inhaled steroid use. As expected, the average cost of care per patient was reduced substantially, in some cases by more than 1000% from baseline.
The Perera study highlights the need to standardize cost-effective- ness methods for the purpose of economic evaluation of asthma treat- ments. This study used some very important research design features (e.g./ active comparators, long-term follow-up, multiple and relevant outcome measures) from the perspective of economic evaluation. Several important limitations, however, reduce the usefulness of this work for decision-making. The lack of a control group, incorrect application of economic methods, and failure to report an incremental cost-effective- ness ratio are but a few of the major limitations.
Controlled clinical trials are necessary to investigate the efficacy and safety of pharmacotherapy. It is not clear whether such rigorous study designs are necessary for economic evaluation. Two of the economic studies just described show that inhaled corticosteroids reduced asthma- related morbidity in low doses (400 &d) and that the economic benefits either offset or add to overall treatment costs. The study by Campbell and coworkers7 was brief in duration, measured only medication costs, and focused on clinical measures of pulmonary function, whereas most primary care clinicians and health plans are interested in total costs and outcomes important to patients, such as symptoms. The studies by Connett and colleagueslO and Rutten-van Molken and associates34, 35 were somewhat longer in duration, measured total costs, and evaluated symptom-free days as the primary outcome measure. All three studies determined that inhaled corticosteroids improved symptom-free days compared with the beta,-agonist alone, but each arrived at a different economic conclusion. The study by Connett and colleagueslO included an estimate of indirect costs, which increased the estimate of overall economic benefit. Both studies by Rutten-van Molken and associates34, 35 valued only medical care costs and showed that adding inhaled cortico- steroid to a regimen of inhaled beta2-agonist improved clinical outcomes and increased the overall cost of care.
These studies highlight the need for standardization of study de- sign, selection of comparator therapy, and standardization and valuation of economic and outcome measures. Without standardization, decision- makers are likely to be confused by conflicting results.
Long-acting Beta,-Agonists
Long-acting bronchodilators such as formoterol and salmeterol rep- resent a relatively new approach to prophylactic and symptomatic treat- ment for asthma. Only one published study has evaluated simultane- ously the impact of a long-acting agent on clinical and economic outcomes for patients with In this paper, the authors reported
COST AND COST-EFFECTIVENESS IN ASTHMA 833
on a retrospective cost-effectiveness analysis of a clinical trial of 145 patients diagnosed with asthma and randomized to receive 12 weeks of maintenance therapy with either long-acting formoterol or short-acting albuterol. The primary clinical outcome measure was cumulative symp- tom-free days during the 12-week period. The authors concluded that there were no statistically significant differences in symptom-free days between the two treatment groups. Because of these results, no incre- mental cost-effectiveness ratio was calculated. For illustrative purposes, the authors simulated a range of possible clinical benefits and cost- effectiveness ratios by respecifying the symptom-free composite score to include or not include adverse events.
Inhaled Cromolyn Sodium
Ross and made use of patient and health services re- cords in one large group practice to estimate the economic consequences of including cromolyn sodium in the treatment regimen of asthma patients. A total of 53 patients were identified retrospectively from medical records and categorized into two groups: those who received cromolyn sodium for at least 1 year (n = 27) and those who received no cromolyn sodium as part of the treatment regimen (n = 26). Patients receiving cromolyn sodium provided an average of 3.2 years of health service utilization data, and those in the comparison group provided 3.8 years of data. Medication costs for patients on cromolyn sodium were slightly higher ($27.90 per month) than for the control group ($25.20 per month). Emergency department and hospital costs were lower, however, for cromolyn sodium patients; after the change in medication, they experienced a 96% reduction in the rate of emergency department visits and a 92% reduction in the rate of hospital admissions. The authors made no direct measurement of outcomes of therapy and did not control for symptom severity or other baseline confounding that might partly explain differences in the results. Thus this study is not a true cost- effectiveness analysis; rather, it is a cost comparison of two retrospective cohorts of asthma patients on two different treatment regimens.
Other Pharmaceuticals
The remaining economic studies of asthma medications identified in this review were not full cost-effectiveness evaluations. Tierce and colleagues39 performed a retrospective cost-identification study compar- ing use of inhaled albuterol with use of inhaled metaproterenol in 1463 Michigan Medicaid patients. Asthma-related medications, physician and emergency department visits, and hospital care were assessed and val- ued using Medicaid prices. The authors concluded that the overall cost of care was significantly lower in the albuterol group compared with
834 SULLIVAN
the metaproterenol group. Because this study was not randomized, questions remain about baseline comparability of the two groups.
A modest number of papers exist on the impact of other beta,- agonists on health services utilization,’* methylprednisolone use in the emergency or aerosolized versus metered-dose inhaler delivery of beta,-agonists.”, 37 Three of the studies did not attempt to value the intervention benefits in monetary terms; rather, these studies expressed outcomes in terms such as number of visits. Further, one was not considered because of a mixed study sample that included patients without asthma among the evaluable patients.
ECONOMICS OF ASTHMA EDUCATION PROGRAMS
The economics of health education have been assessed, and the economic benefits appear to be clear. The earliest study of an educational intervention for asthma included a discussion of the economic outcomes of the program.18 In the last decade, a number of educational programs have been developed for asthma based on theories of behavior change.6 The stated goals of asthma patient education programs are to reduce morbidity and mortality by (1) improving knowledge among patients with asthma and their caregivers to produce better self-management behavior, (2) increasing compliance with therapy, (3) improving relations and interaction with health care providers, and (4) increasing confidence among people with asthma with regard to controlling and managing symptoms.
Objective pulmonary function measures (such as FEV,) alone have not been shown to be improved by health education programs. Research has established, however, that in some settings and in some populations, health education programs reduce other asthma-related morbidity. An extensive and critical review of asthma patient education programs has been undertaken by Boulet and colleagues.6
Asthma patient education programs have been targeted at both adults and children. Windsor and colleagues,% in a randomized cost- effectiveness t ia l of 267 adults with asthma, showed that inhaler, drug, and total medical adherence improved in the experimental group rela- tive to the control group at an additional cost of $28 per person. No direct measures of health outcomes were attempted, and the costing protocol failed to account for potential economic benefits related to reductions in health services use.
A study by Muhlhauser and associatesB reported on the efficacy of a 3-year structured asthma teaching and treatment program (ATTP) in Germany for adults with moderate-to-severe asthma. The program fo- cused on better asthma control through self-monitoring and patient awareness and reported favorable effects on health services utilization and days missed from work. Trautner and colleaguesrn carried the analy- sis further by estimating the cost benefit of the ATTP program. From the perspective of the German health authorities, the program produced
COST AND COST-EFFECTNENESS IN ASTHMA 835
monetary benefits in excess of costs at a ratio of 2.7 to 1. When estimated from the perspective of society, the program appeared even more favor- able, with a benefit-cost ratio of 5.0 to 1.
Bolton and associates4 evaluated the cost-effectiveness of a 12-month asthma self-management program in a sample of 241 adults who pre- sented to an emergency department with asthma symptoms. When compared with the usual control group, the intervention group had fewer emergency department visits (39 per 100 patients vs. 16 per 100 patients) and fewer days with activity limitations. Physician and hospital visits did not differ statistically between the two groups. The economic analysis showed that the $82 per person cost for the patient education program was offset by an estimated $628 per person reduction in emer- gency department visit charges.
In a mixed population of 62 adults and children with asthma, Sondergaard and c011eagues~~ estimated the costs and benefits of a 6- month patient education program administered by a team of health professionals consisting of a physician, a nurse, and a pharmacist. The goal of the program was to improve disease awareness, medication compliance, and self-monitoring using peak flow meters. Among the economic evaluations in health education reviewed here, this study takes the most comprehensive approach to valuing costs and benefits, including program materials, personnel, and transportation costs. In addition, the study attributed monetary values to the benefits from reducing all health services utilization and work absenteeism. Changes from baseline in use of resources, work productivity, and health status were measured in both the experimental and usual care groups. The results suggest that experimental patients experienced more physician and drug costs and fewer emergency care visits and days missed from work. These results suggest predictable patterns of substitution of care-physician and drug services as substitutes for emergency care. In this case, however, the overall costs of the intervention (€6,546) exceeded the benefits (€4,528).
In children with asthma, there are three noteworthy economic evalu- ations of patient education programs. In the first, Fireman and associ- a t e ~ ’ ~ targeted a comprehensive health education program for both the affected child and the parent. When compared with a usual care group, the experimental group showed improvement in compliance and reduc- tions in asthma exacerbations, lost school days due to asthma, and emergency and hospital visits. The cost-benefit analysis suggested that savings from health service utilization offset costs by about 2 to 1, or about $225 per affected child.
In the second, Lewis and colleaguesz randomly assigned 76 children and their parents at the Los Angeles Kaiser Permanente facility to the Asthma Care Training program or usual care. Results indicated that disease knowledge improved equally in both groups. Medication adher- ence was greater, and emergency department visits and days of hospital- ization were fewer in the experimental group. Overall, the effect of the
836 SULLIVAN
program on the experimental children represented a $180 savings per year per child when both program costs and benefits were accounted.
The third was a larger study by Clark and coworkers* on the costs and benefits of health education in low-income families with children with asthma (n = 310). This evaluation study found no statistically significant difference in emergency department visits and hospitaliza- tions. When the analysis was restricted to individuals with a recent history of hospitalization, however, the experimental group was found to have reduced frequency of health services utilization compared with the usual care group. The economic evaluation determined that, overall, benefits were less than costs by a ratio of 0.6 to 1. When considering only the subgroups of individuals with previous hospitalization, however, the benefits exceed costs by a ratio of 11.2 to 1, suggesting the obvious that targeting interventions to certain subgroups with greater baseline illness costs may elicit more favorable economic results.
These eight studies provide mixed evidence of the economic value of asthma education programs in both adults and children. More favor- able results are reported when the program is targeted to high-risk or more costly patients. These high-risk patients include those who are more severely ill, young, from an ethnic minority, from a low-income family, and those who have frequent compliance problems. The ability to generalize from these studies is minimal because the patient education programs are not comparable in terms of goals and scope, and the outcome measurements and follow-up periods vary across studies. More research is needed to understand the effectiveness and economic benefits of these programs in different high-risk populations. In addition, it would be important to determine which components of the asthma patient education programs are most cost-effective. Based on present knowledge, it would be difficult for decision-makers with limited re- sources to choose among these programs.
SUMMARY
Health care decision-makers are interested in using rational ap- proaches to allocating resources among patients with chronic disease. Some policy-makers may view cost-effectiveness analyses as a means to justify rationing, but others embrace economic evaluation methods for improving decision-making about, for example, limits on insurance cov- erage for specific interventions, formulary development, quality im- provement programs, and appropriate utilization of services. Before sound decisions can be made on appropriate selection and use of inter- ventions, however, more comparative data on the economic value of the treatments and management strategies are needed.
Too few studies as yet adequately characterize the economic impact of the large number of interventions currently being used to manage asthma. There is no standard approach to evaluating the economic costs and benefits of medical treatments used to treat asthma or for comparing
COST AND COST-EFFECTIVENESS IN ASTHMA 837
the clinical and economic benefits of alternative treatments. Researchers conduct studies with varying lengths of follow-up, use different outcome measures, include different costs in the calculation of total cost, and evaluate different mixes of patients. These inconsistencies hinder efforts by decision-makers to compare clinical and economic benefits.
Despite the many shortcomings, economic evaluations of asthma treatments need to be encouraged and nurtured. Substantial improve- ments and standardization are needed in the study design, study dura- tion, sample size determination based on economic and health status endpoints, selection of appropriate comparison therapies, and selection and evaluation of costs and outcomes.
References
1. Adelroth E, Thompson S: Advantages of high-dose inhaled budesonide. Lancet 1:476, 1988
2. Banta HD, Luce BR: Health Care Technology and Its Assessment. New York, Oxford University Press, 1993
3. Barnes PJ, Pedersen S Efficacy and safety of inhaled corticosteroids in asthma. Am Rev Respir Dis 148:Sl-S26, 1993
4. Bolton MB, Tilley BC, Kuder J, et a1 The cost and effectiveness of an education program for adults who halie asthma. J Gen Intern Med 6401-407, 1991
5. Boston Consulting Group: The Costs of Asthma in the Federal Republic of Germany. Boston, The Boston Consulting Group, 1995
6. Boulet LP, Chapman KR, Green LW, FitzGerald JM. Asthma education. Chest 106(suppl 4):1845-1965, 1994
7. Campbell LM, Simpson RJ, Turbitt ML, et al: A comparison of the cost-effectiveness of budesonide 400 &day and 800 pg/day in the management of mild-to-moderate asthma in general practice. Br J Med Econ 667-74,1993
8. Clark NM, Feldman CH, Evans D, et al: The impact of health education on frequency and cost of health care use by low income children with asthma. J Allergy Clin Immunol78:108-115, 1986
9. Clark TJH The Occurrence and Cost of Asthma. West Sussex, UK, Cambridge Medical Publications, 1990
10. Connett GJ, Lenney W, McConchie SM: The cost-effectiveness of budesonide in severe asthmatics aged one to three years. Br J Med Econ 6:127-134,1993
11. Drummond MF, Stoddart GL, Torrance G W Methods for the Economic Evaluation of Health Care Programmes. New York, Oxford University Press, 1987
12. Eisenberg J M Clinical economics: A guide to economic analysis of clinical practices.
13. Ellwood P: Outcomes management: A technology of patient experience. N Engl J Med 318:1549-1556, 1988
14. Emerman CL, Cydulka RK, Effron D, et al: A randomized, controlled comparison of isoetharine and albuterol in the treatment of acute asthma. Ann Emerg Med 201090-1093,1991
15. Fireman P, Friday GA, Gira C, et al: Teaching self-management skills to asthmatic children and their parents in an ambulatory care setting. Pediatrics 68341-348, 1981
16. Gerdtham UG, Hertzman P, Boman G, et al: Impact of Inhaled Corticosteroids on Asthma Hospitalization in Sweden: A Pooled Regression Analysis. Stockholm, Re- search Report of the Ekonomiska Forskningsinstitutet, Center for Health Economics, Stockholm School of Economics, 1993
17. Grampian Asthma Study of Integrated Care (GRASSIC): Integrated care for asthma: A clinical, social, and economic evaluation. BMJ 308:559-564, 1994
JAMA 2622879-2886, 1989
838 SULLIVAN
18. Green LW Toward cost-benefit evaluations of health education: Some concepts, methods, and examples. Health Educ Monog 23444,1974
19. Grimes DA: Technology follies: The uncritical acceptance of medical innovation. JAMA 269303&3033,1993
20. Jasper AC, Mohsenifar Z, Kahan S, et al: Cost-benefit comparison of aerosol bronchod- ilator delivery methods in hospitalized patients. Chest 91:614-618, 1987
21. Johannesson M, Weinstein MC: Designing and conducting cost-benefit analyses. In Spilker B (ed): Quality of Life and Pharmacoeconomics in Clinical Trials, ed 2. Philadelphia, Lippincott-Raven Publishers, 1996
22. Karalus NC, Harrison AC: Inhaled high-dose beclomethasone in chronic asthma. N Z Med J 100:306-308, 1987
23. Krahn MD, Berka C, Langlois P, Detsky As: Direct and indirected costs of asthma in Canada, 1990. Can Med Assoc J 154:821-831,1990
24. Laupacis A, Feeny D, Detsky AS, Tugwell PX How attractive does a new technology have to be to warrant adoption and utilization? Tentative guidelines for using clinical and economic evaluations. Can Med Assoc J 146:473481,1992
25. Lewis CE, Rachelefsky G, Lewis MA, et al: A randomized trial of ACT (asthma care training) for kids. Pediatrics 74:47&486, 1984
26. Littenburg B, Gluck E H A controlled trial of methylprednisolone in the emergency treatment of acute asthma. N Engl J Med 3143150-152, 1986
27. Mellis CM, Peak JK, Bauman AE, Woolcock AJ: The cost of asthma in New South Wales. Med J Aust 155:522-528, 1991
28. Muhlhauser I, Richter B, Kraut D, et a1 Evaluation of a structured treatment and teaching programme on asthma. J Intern Med 230:157-164, 1991
29. National Asthma Campaign: Report on the Cost of Asthma in Australia. National Asthma Campaign, 1992
30. National Heart, Lung, and Blood Institute: Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma. Bethesda, US Department of Health and Human Services, NIH publication No. 91-3042,1991
31. Perera BJC: Efficacy and cost effectiveness of inhaled steroids in asthma in a devel- oping country. Arch Dis Child 73312-316,1995
32. Rees TI', Lennox B, Timney AP, et al: Comparison of increasing the dose of budeson- ide to 800 @g/day with a maintained dose of 400 &day in mild to moderate asthmatic patients. Eur J Clin Res 4:67-77, 1993
33. Ross RN, Morris M, Sakowitz SR, Berman BA Cost-effectiveness of including cromo- lyn sodium in the treatment program for asthma: A retrospective, record-based study. Clin Ther 10188-203, 1988
34. Rutten-van Molken MP, Van Doorslaer EK, Jansen MC, et al: Cost-effectiveness of inhaled corticosteroid plus bronchodilator therapy versus bronchodilator monother- apy in children with asthma. PhannacoEconomics 4257-270,1993
35. Rutten-van Molken MP, Van Doorslaer EK, Jansen MC, et al: Costs and effects of inhaled corticosteroids and bronchodilators in asthma and chronic obstructive pulmonary disease. Am J Respir Crit Care Med 151:975-982, 1995
35a. Sculpher M, Buxton MJ: The episode-free day as a composite measure of effectiveness. Pharmacoeconomics 4:345-352, 1993
36. Sondergaard B, Davidsen F, Kirkeby B, et a1 The economics of an intensive education program for asthmatic patients: A prospective controlled trial. PharmacoEconomics
37. Summer W, Elston R, Tharpe L, et al: Aerosol bronchodilator delivery methods: Relative impact on pulmonary function and cost of respiratory care. Arch Intern Med 149:618423, 1989
1~207-212,1992
38. Thompson S On the social cost of asthma. Eur J Respir Dis 136185-191, 1984 39. Tierce JC, Meller W, Berlow B, Gerth WC: Assessing the cost of albuterol inhalers in
the Michigan and California Medicaid programs: A total cost-of-care approach. Clin Ther 11:53-61, 1989
39a. Torrance G W Measurement of health state utilities for economic appraisal: A review. J Health Econ 51-30,1986
COST AND COST-EFFECTIVENESS IN ASTHMA 839
40. Trautner C , Richter B, Berger M: Cost-effectiveness of a structured treatment and teaching programme on asthma. Eur Respir J 614851491, 1993
41. von Neumann J, Morgenstern 0 Theory of Games and Economic Behaviour. Princeton, Princeton University Press, 1994
42. Warner KE, Luce BR Cost-Benefit and Cost-effectiveness Analysis in Health Care: Principles, Practice, and Potential. Ann Arbor, MI, Health Administration Press, 1982
43. Weinstein MC, Stason WB: Foundations of cost-effectiveness analysis for health and medical practices. N Engl J Med 296716-721, 1977
44. Weiss KB, Gergen PJ, Hodgson TA. An economic evaluation of asthma in the United States. N Engl J Med 326:862-866, 1992
45. Weiss KB, Sullivan SD: The economic costs of asthma: A review and conceptual model. PharmacoEconomics 4:14-30,1993
46. Windsor RA, Bailey WC, Richards JM Jr, et al: Evaluation of the efficacy and cost effectiveness of health education methods to increase medication adherence among adults with asthma. Am J Public Health 801519-1521, 1990
Address reprint requests to
Sean D. Sullivan, PhD Department of Pharmacy
Box 357630 University of Washington
Seattle, WA 98195





























