Embed Size (px)
Citation preview

5/11/2013
1
Corrective Osteotomy of Distal Radius Malunion---New Horizons
I certify that, to the best of my knowledge, no aspect of my current personalor profession situation might reasonably be expected to affect significantlymy views on the subject on which I am presenting.
1. LOSS OF REDUCTION
2. DELAYED UNION AND NONUNION
3. MALUNION
4. DISTAL RADIOULNAR JOINT
WRIST FRACTURES
OSTEOARTICULAR COMPLICATIONS• Carpal ligaments
• Carpal fractures
• Nerves
• Tendons
• Combined soft tissues
• Vascular, compartment syndrome
ASSOCIATED LESIONS COMPLICATIONS
Carpal instability
Nonunion, malalignment
Neuropathy
Tendinitis, ruptures
Multifactorialfunctional deficit
RSD, Complex RegionalPain syndrome
WRIST FRACTURES
5/11/2013
2
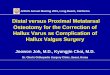
TIMING OF SURGERY
-absence of trophic changes-acceptable bone quality-adequate wrist function
as soon as possible, provided there is: NASCENT MALUNION
- immature callus
- established deformity (5 – 8 weeks
post-fracture )
MATURE MALUNION
- remodelled callus
- 4 to 6 months or morepost-fracture
ADVANTAGES OF EARLY CORRECTION
•easiness of radial and DRUJ re-alignment
•less soft tissue contractures and DRUJ dysfunction
•no need of structural corticocancellous bone graft
•considerably decrease of total disability
•early return to work
Jupiter JB, Ring D:A comparison of early and late r econstruction of malunited fracturesof the distal end of the radius. JBJS 78A: 739-
748, May 1996
corrective osteotomy of malunited Colles fracturesthrough a dorsal approach
preoperative planning is based on the radiographicmeasurements of the opposite wrist:
-ulnar inclination-ulnar variance-volar tilt
(for rotational deformity: comparative CT-scans)
Bindra RR,Cole RJ et al: Quantification of the radial torsion angle withcomputerized tomography in cadaver specimens JBJS 79A:833-837, 1997
SURGICAL TECHNIQUE

5/11/2013
3
preoperative planning dorsal approach
2.4 distal radius locking plates

5/11/2013
4

5/11/2013
5
5/11/2013
6

5/11/2013
7
correction of malunited Colles`fracturesthrough a volar approach:
SURGICAL TECHNIQUE
- Open wedge osteotomy, interpositional bone graftand volar plate fixation (U. Lanz, J.Orbay)
- Close wedge osteotomy, Darrach procedure andK-wire fixation (Posner, Garcia-Elias)
- Close wedge osteotomy and ulnar shortening
- Close wedge osteotomy and ulnar head prosthesis (D.L.Fernandez)

5/11/2013
8

5/11/2013
9
5/11/2013
10

5/11/2013
11

5/11/2013
12
open wedge osteotomy, bone graft and volar plate fi xation
Prommersberger KJ Lanz U.: Corrective osteotomy for malunited Colles‘fractures. Orthop Trauma 6: 75-87 , 1998.
Orbay JL, Indriago I, Badia A, Khouri RK, Gonzalez E, Fernandez DL: Corrective osteotomy of dorsally malunited fractures of the distal radiusvia the extended FCR approach.J Hand Surg 28B (Suppl 1): 2 ,2003
Lanz U, Kron W: Neue Technik zur Korrektur in Fehlstellung verheilterRadiusfrakturen. Handchir Mikrochir Plast Chir 8:203-206, 1976
L
Rsurgical technique

5/11/2013
13
post-opx-rays
12 weekspost-op
5/11/2013
14
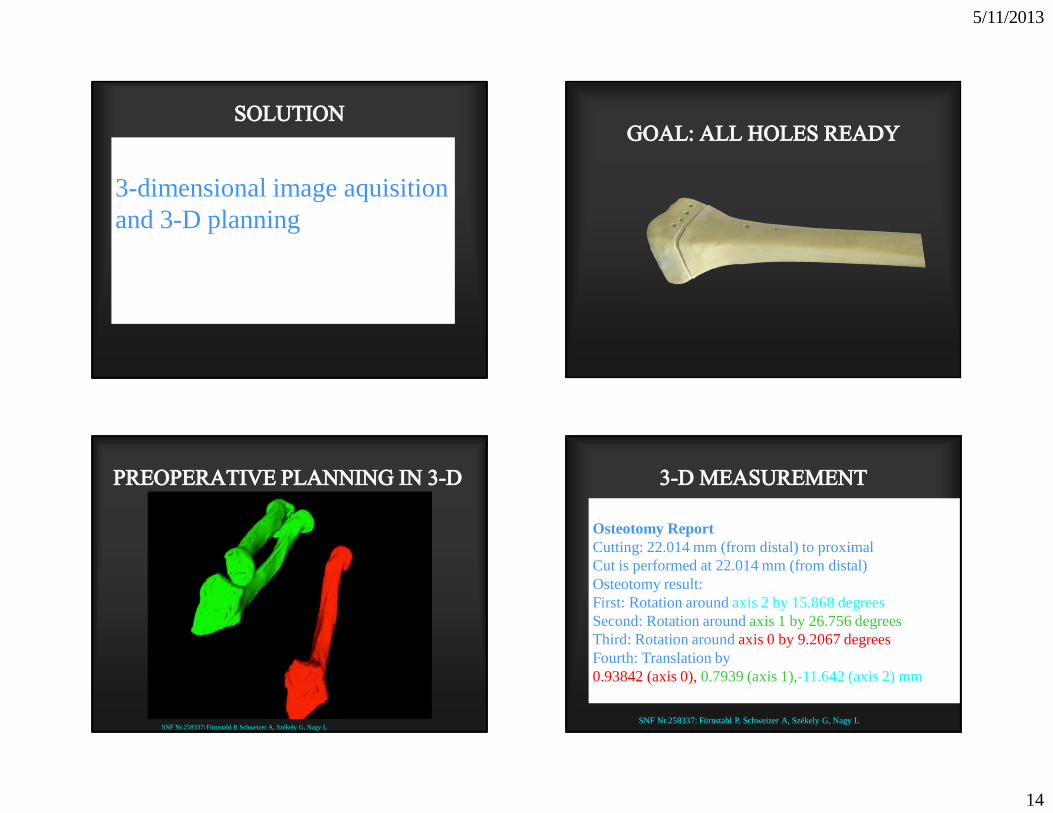
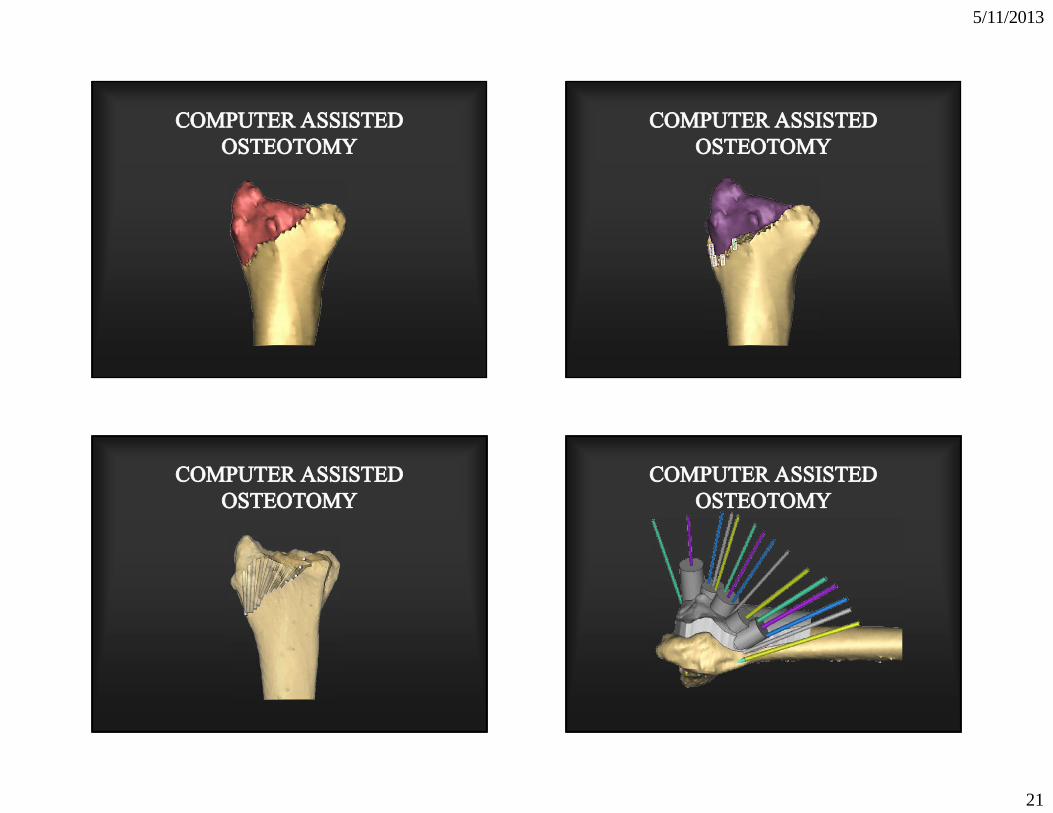
3-dimensional image aquisition and 3-D planning
SNF Nr.258337: Fürnstahl P, Schweizer A, Székely G, Nagy L
Osteotomy ReportCutting: 22.014 mm (from distal) to distalCut is performed at 22.014 mm (from distal)Osteotomy result:First: Rotation around axis 2 by 15.868 degreesSecond: Rotation around axis 1 by 26.756 degreesThird: Rotation around axis 0 by 9.2067 degreesFourth: Translation by 0.93842 (axis 0),0.7939 (axis 1),-11.642 (axis 2) mm
SNF Nr.258337: Fürnstahl P, Schweizer A, Székely G, Nagy L
Osteotomy ReportCutting: 22.014 mm (from distal) to proximalCut is performed at 22.014 mm (from distal)Osteotomy result:First: Rotation around axis 2 by 15.868 degreesSecond: Rotation around axis 1 by 26.756 degreesThird: Rotation around axis 0 by 9.2067 degreesFourth: Translation by 0.93842 (axis 0),0.7939 (axis 1),-11.642 (axis 2) mm
5/11/2013
15
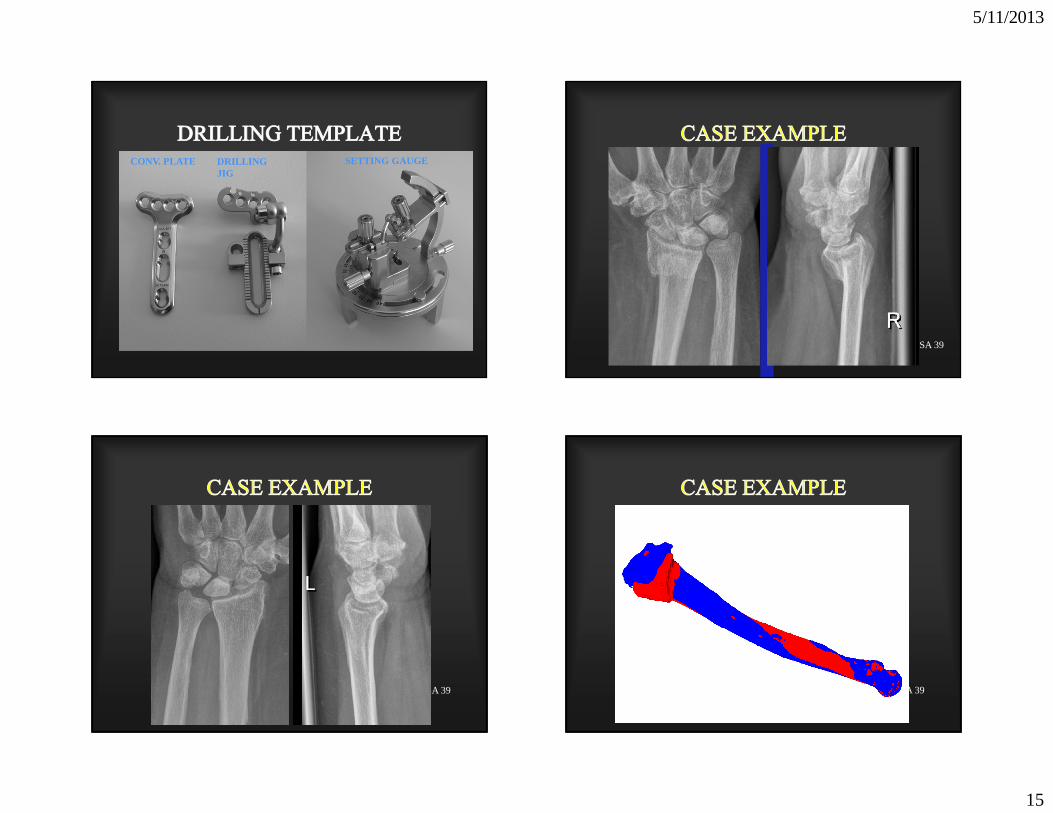
CONV. PLATE DRILLING JIG
SETTING GAUGE
SA 39
SA 39 SA 39
5/11/2013
16
SA 39 SA 39
SA 39
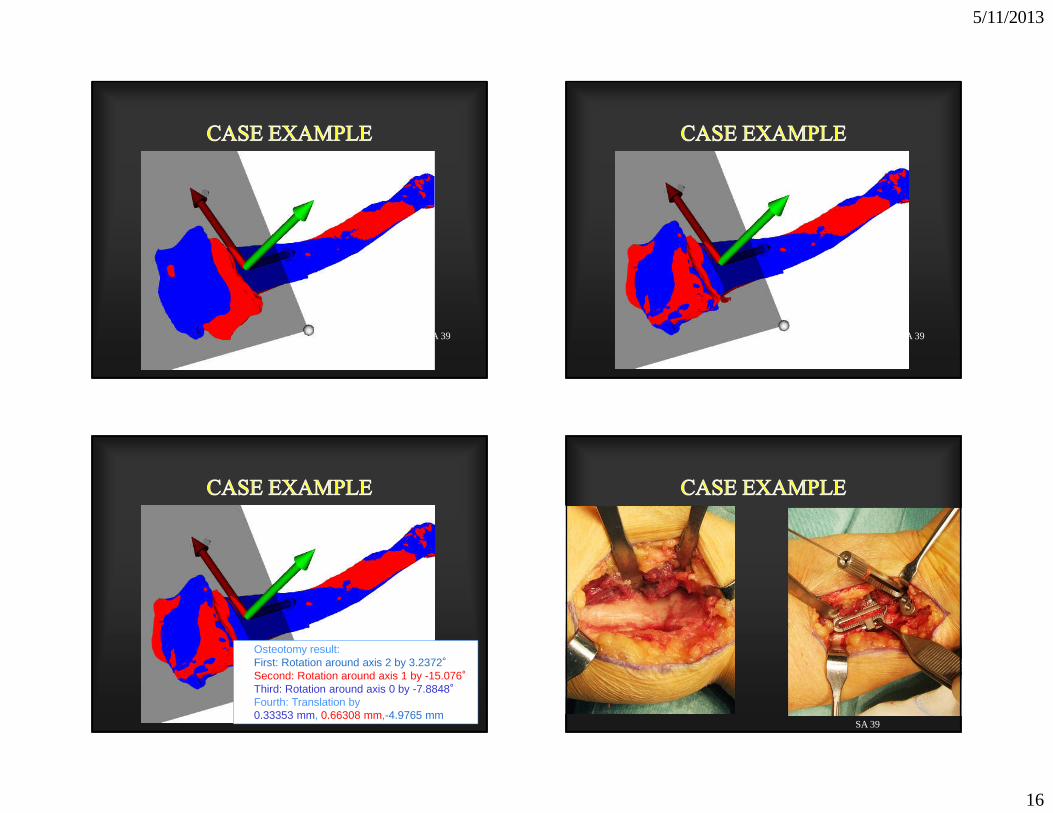
Osteotomy result:First: Rotation around axis 2 by 3.2372°Second: Rotation around axis 1 by -15.076°Third: Rotation around axis 0 by -7.8848°Fourth: Translation by0.33353 mm, 0.66308 mm,-4.9765 mm
SA 39

5/11/2013
17
SA 39 SA 39
SA 39 SA 39
Skyline view

5/11/2013
18
SA 39 6W
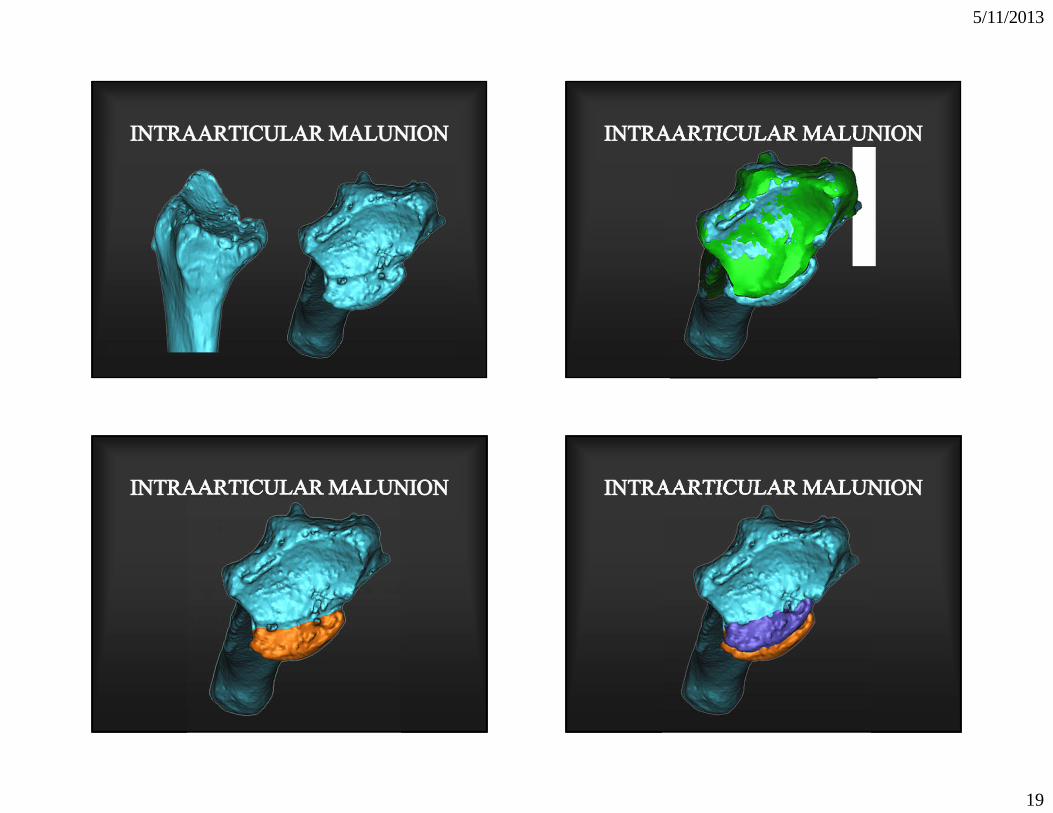
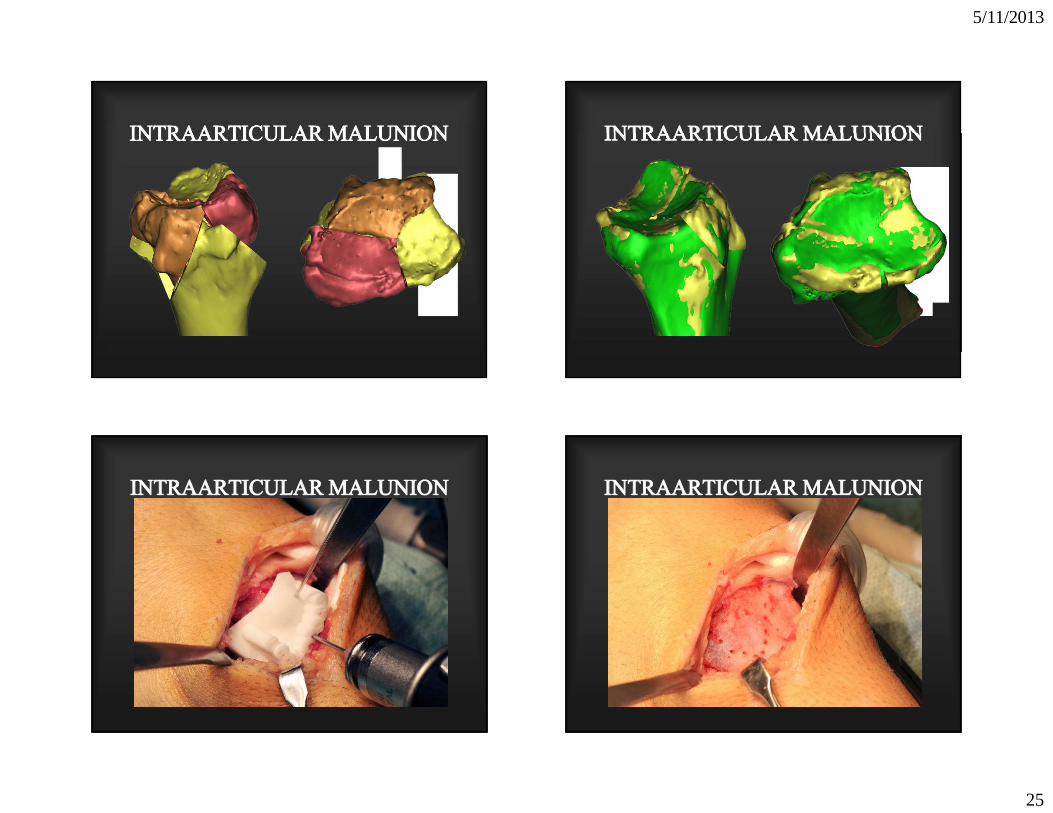
INTRARTICULAR MALUNION
intra-articular malunion results after failure to r ecognize
potentially unstable articular disruption, or insuf ficient
reduction and fixation during surgical treatment
5/11/2013
19

5/11/2013
20
5/11/2013
21

5/11/2013
22

5/11/2013
23

5/11/2013
24
5/11/2013
25

5/11/2013
26
The indication of osteotomy for an intra-articularmalunion depends on:
1) the fracture pattern
2) the extent of cartilage damage
3) the chronology
4) presence of fixed carpal malalignment
5) the soft tissue condition
INTRA-ARTICULAR OSTEOTOMIES

5/11/2013
27
CONTRAINDICATIONS
1) severe cartilage damage
2) radiographic degenerative changes
3) chronic synovitis
4) significant soft tissue andcapsular contractures (post RSD)
5) complex fracture pattern andfixed carpal malalignment
TREATMENT RECOMMENDATIONS
- simple intra-articular disruption
- as soon as possible
- minimal cartilage damage (chondromalacia)
- adequate pre-operative function
- complient, cooperative patient
otherwise a limited carpal fusion (RSL or RL) is preferable
INTRA-ARTICULAR MALUNION

5/11/2013
28
ARTHROSCOPIC ASSISTED TREATMENT OF DISTAL RADIUS MALUNION
Francisco del Piñal et al: Arthroscopically guided osteotomyfor management of intra-articular distal radius malunions.
J Hand Surg 35A: 392-397, 2010
del Piñal, F , Garcia Bernal FJ, et al: Correction of malunited intra-articular distal radius fractures with an inside-out
osteotomy technique. J Hand Surg 31A: 1029-1034, 2006
Courtesy: Dr Francisco del Piñal, Santander,Spain

5/11/2013
29
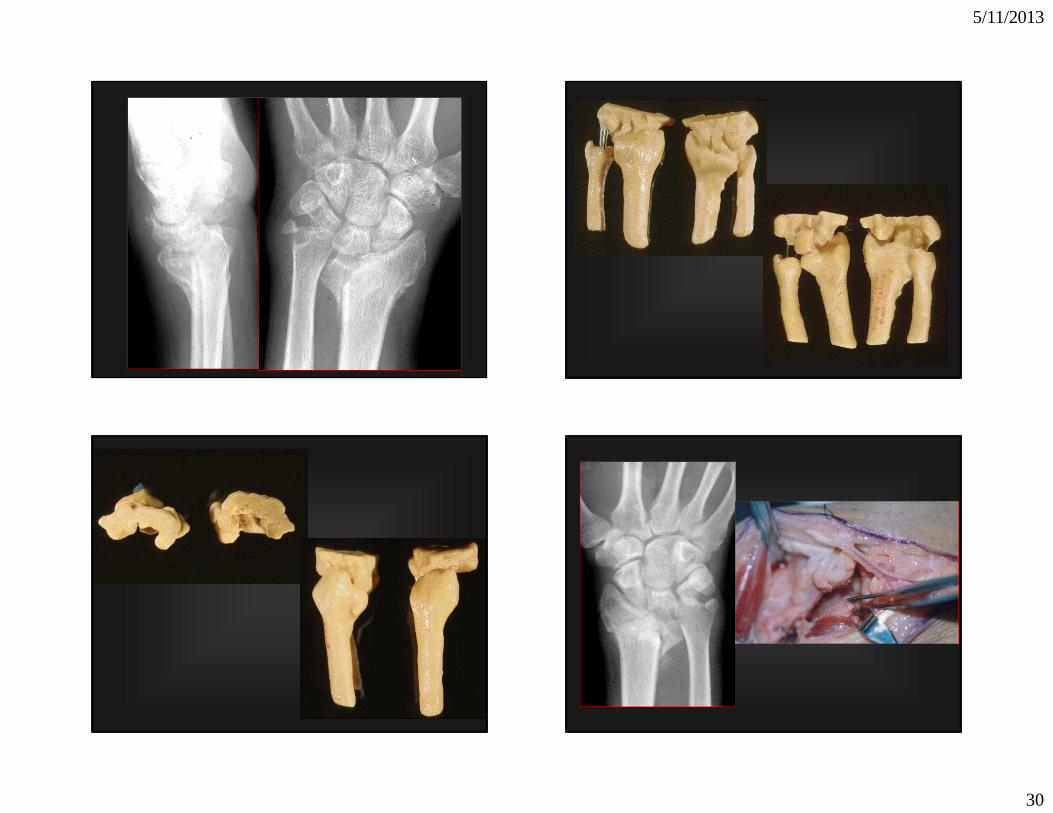
Combined Intra- and Extra-Articular Distal Radius Malunion
5/11/2013
30
118
119
5/11/2013
31
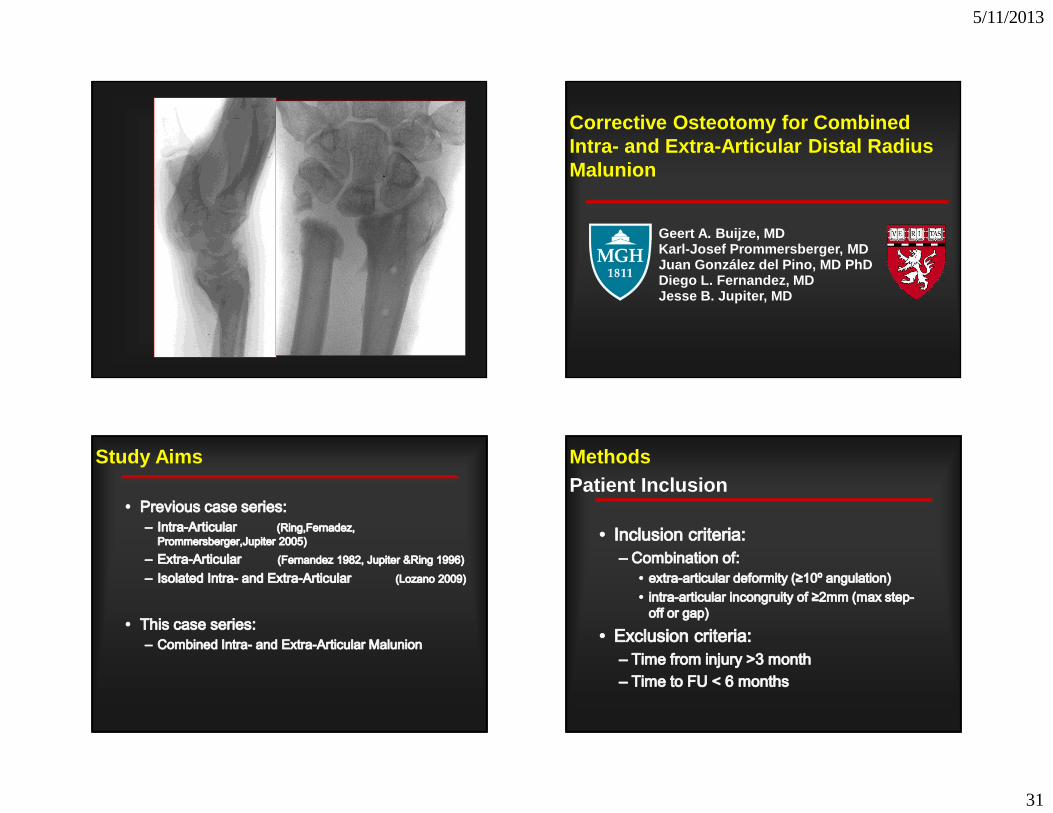
Geert A. Buijze, MDKarl-Josef Prommersberger, MDJuan González del Pino, MD PhDDiego L. Fernandez, MDJesse B. Jupiter, MD
Corrective Osteotomy for Combined Intra- and Extra-Articular Distal Radius Malunion
Study Aims MethodsPatient Inclusion

5/11/2013
32
MethodsPatient Inclusion
MethodsPatient Characteristics
Surgical TechniqueExtra-Articular Malunion
Surgical TechniqueIntra-Articular Malunion

5/11/2013
33
Surgical Technique
1
1
2
3
3
2
Surgical Technique
Surgical Technique Surgical Technique

5/11/2013
34
Eleven years FU CONCLUSIONS
- malunion remains the most common complication of closed reduction and plaster immobilisation of unst able
extra-articular fractures
- intra-articular malunion results after failure to recognize potentially unstable articular disruption, or insuf ficient
reduction and fixation during surgical treatment
- if symptomatic extra-articular malunion occurs, ra dialosteotomy offers better function,improves the exter nal
appearance and normalizes carpal kinematics
-intra-articular malunion deserves early correction in orderto restore the functional – anatomic integrity of th e jointbefore the onset of symptoms and cartilage damage
-our experience has shown that with:
careful patient selection
correct indication and
refinements of surgical technique
over 80% of excellent and good results can be expected
CONCLUSIONS
Complications and failures are commonly caused eith erby technical errors, or by improper patient selecti on with:
degenerative changes
trophic disturbances
partial joint stiffness
severe osteoprosis
fixed type of DISI malaligment
and failure to assess and simultaneously treatassociated disorders of the distal radioulnar joint
CONCLUSIONS

5/11/2013
35
THANK YOU