Embed Size (px)
Citation preview

Romanian Journal of Morphology and Embryology 2009, 50(4):707–712
CCAASSEE RREEPPOORRTT
Correct complete denture rehabilitation, a chance for recovering abused tissues IULIANA BABIUC1), MIHAELA PĂUNA1), MĂDĂLINA ADRIANA MALIŢA1),
SIMONA GEORGIANA ARITON1), MARIA DAMIAN2), VASILICA UNGUREANU2), ANCA PETRINI2)
1)Department of Removable Prosthodontics, Faculty of Dentistry, “Carol Davila” University of Medicine and Pharmacy, Bucharest
2)“Ion Cantacuzino” National Institute of Research–Development for Microbiology and Immunology, Bucharest
Abstract The prosthodontic treatment must provide for the edentulous patients bio-functional prosthetic restorations, bio-prophylactic for the surrounding tissues. In this aim, an edentulous patient must be submitted to a methodical clinical examination in order to establish the quality of hard and soft tissues, which will indicate the degree of difficulty of the prosthetic treatment. Additional investigation as a microbiologic examination and cephalometric radiographs can be useful in a modern investigation. In our daily practice, we are rarely confronted with a normal morphology of the denture bearing oral structures. The problem of managing abused tissues in a patient with morphologic abnormalities due to faulty prostheses is sometimes difficult to solve. Preventing the deterioration of oral status must be a condition in providing a chance for the success of the following rehabilitations, mainly in the situation when the complete edentulousness succeeds in a young or middle age patient. Keywords: abused oral tissues, conventional complete denture, tissue recovery.
Introduction
The prosthetic treatment with complete dentures must aim to improve the oral health-related quality of life of the patients. However, epidemiological studies of the edentulous population showed that most patients with complete dentures have pathologic tissue changes that require treatment and these changes have little relation to a patient’s perception of denture success or personal oral health status [1].
The success of a new denture requires the support of healthy tissues. Abnormalities, whether they are local, mechanical, or systemic in origin, must receive proper diagnosis and treatment. A comprehensive clinical examination and accurate dental history are essential to identify problems and take necessary corrective action. Successful recovery of abused tissue requires tissue conditioning [2].
Patient, Methods and Results
A female patient, aged 53 years, presented with two incorrect dentures, which led to a poor oral health and function.
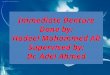
The upper denture was inappropriately designed in order to avoid the torus. As a result, the denture fractured due to the lack of resistance and poor fit. (Figure 1). The denture displayed a poor hygiene, with heavy deposits of plaque and calculus. The vertical dimension was decreased and the prosthesis displayed faulty occlusal relations, causing excessive and mis-directed forces applied to the residual ridges. All these
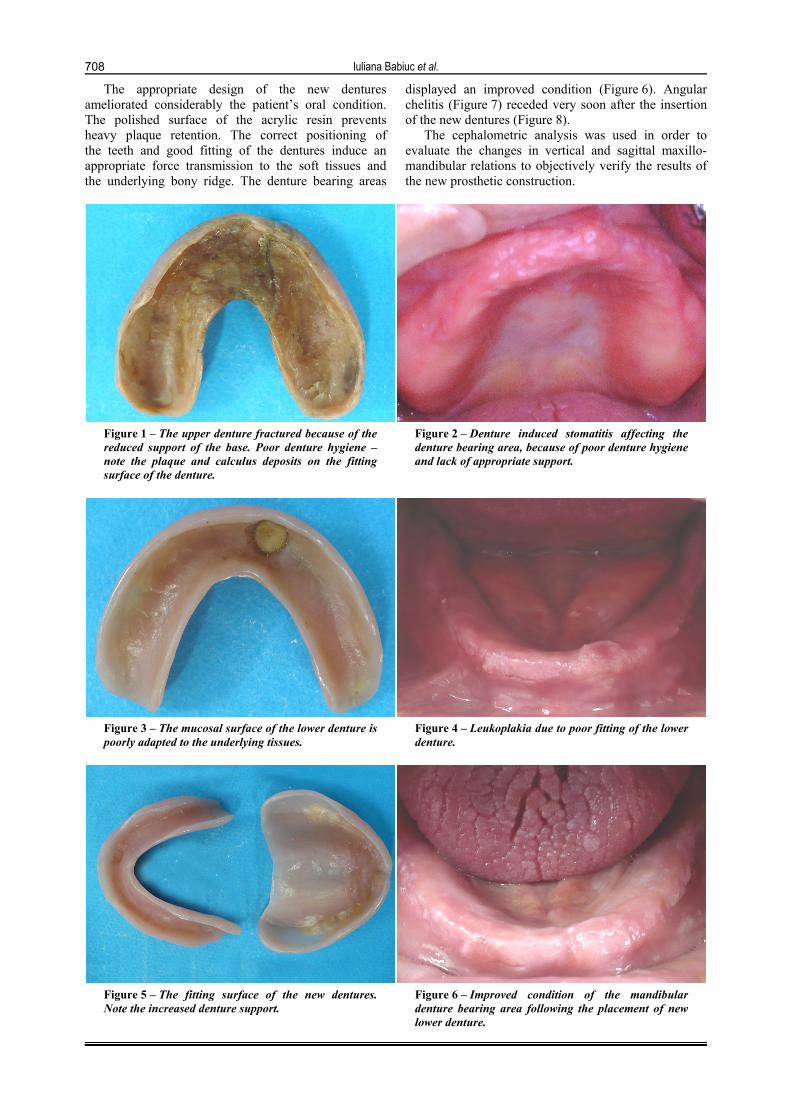
led to a denture-induced stomatitis affecting the denture bearing area (Figure 2). Microbiological analysis showed no pathological strains, leading to the conclusion that the stomatitis was solely related to the mechanical trauma caused by reduced support of the denture, poor fit, reduced vertical dimension and constant wearing of the denture.
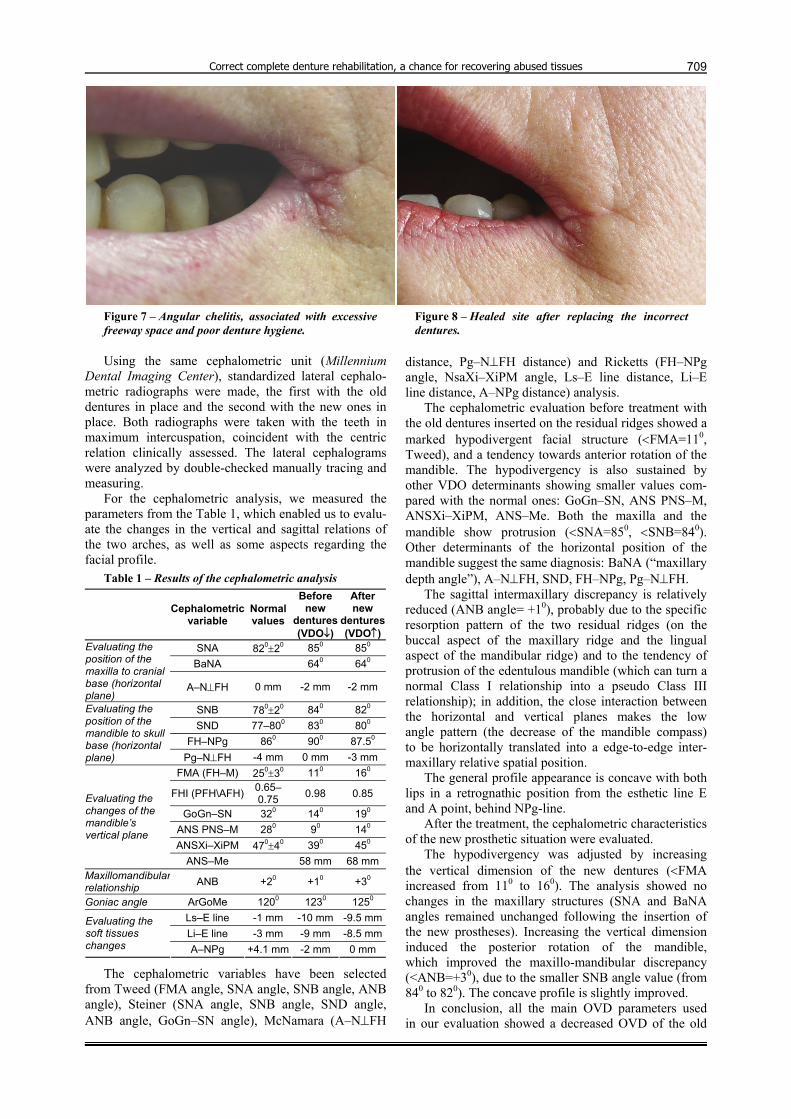
The lower denture was poorly adapted to the underlying tissues (Figure 3). One tooth was added later and this repair induced a leukoplakia in the correspond-ding tissue bearing area (Figure 4).
Angular chelitis was present and was associated with excessive freeway space and poor denture hygiene. Both dentures displayed very poor esthetics, a decreased vertical dimension and incorrect occlusal relations.
The patient was advised to leave the dentures out at nighttime, soaked in denture-cleaning agent in order to improve the tissue condition prior to inserting new dentures.
A new set of dentures (Figure 5) was made, which corrected the support, retention and esthetic problems. During the treatment, we encountered a series of difficulties such as the lack of appropriate impression trays for the atypical conformation of both the edentulous maxilla (very large) and the atypical mandible, where we needed to adapt a tray for dentate patients. The centric relation was registered by simple, non-stressing clinical methods. The increase of the vertical occlusal dimension was of utmost importance because it radically improved functionality, especially aesthetics.
Iuliana Babiuc et al.
708
The appropriate design of the new dentures ameliorated considerably the patient’s oral condition. The polished surface of the acrylic resin prevents heavy plaque retention. The correct positioning of the teeth and good fitting of the dentures induce an appropriate force transmission to the soft tissues and the underlying bony ridge. The denture bearing areas
displayed an improved condition (Figure 6). Angular chelitis (Figure 7) receded very soon after the insertion of the new dentures (Figure 8).
The cephalometric analysis was used in order to evaluate the changes in vertical and sagittal maxillo-mandibular relations to objectively verify the results of the new prosthetic construction.
Figure 1 – The upper denture fractured because of the reduced support of the base. Poor denture hygiene – note the plaque and calculus deposits on the fitting surface of the denture.
Figure 2 – Denture induced stomatitis affecting the denture bearing area, because of poor denture hygiene and lack of appropriate support.
Figure 3 – The mucosal surface of the lower denture is poorly adapted to the underlying tissues.
Figure 4 – Leukoplakia due to poor fitting of the lower denture.
Figure 5 – The fitting surface of the new dentures. Note the increased denture support.
Figure 6 – Improved condition of the mandibular denture bearing area following the placement of new lower denture.
Correct complete denture rehabilitation, a chance for recovering abused tissues
709
Figure 7 – Angular chelitis, associated with excessive freeway space and poor denture hygiene.
Figure 8 – Healed site after replacing the incorrect dentures.
Using the same cephalometric unit (Millennium
Dental Imaging Center), standardized lateral cephalo-metric radiographs were made, the first with the old dentures in place and the second with the new ones in place. Both radiographs were taken with the teeth in maximum intercuspation, coincident with the centric relation clinically assessed. The lateral cephalograms were analyzed by double-checked manually tracing and measuring.
For the cephalometric analysis, we measured the parameters from the Table 1, which enabled us to evalu-ate the changes in the vertical and sagittal relations of the two arches, as well as some aspects regarding the facial profile.
Table 1 – Results of the cephalometric analysis
Cephalometric variable
Normal values
Before new
dentures (VDO↓)
After new
dentures (VDO↑)
SNA 820±20 850 850 BaNA 640 640
Evaluating the position of the maxilla to cranial base (horizontal plane)
A–N⊥FH 0 mm -2 mm -2 mm
SNB 780±20 840 820 SND 77–800 830 800
FH–NPg 860 900 87.50
Evaluating the position of the mandible to skull base (horizontal plane) Pg–N⊥FH -4 mm 0 mm -3 mm
FMA (FH–M) 250±30 110 160
FHI (PFH\AFH) 0.65–0.75 0.98 0.85
GoGn–SN 320 140 190 ANS PNS–M 280 90 140 ANSXi–XiPM 470±40 390 450
Evaluating the changes of the mandible’s vertical plane
ANS–Me 58 mm 68 mm Maxillomandibular relationship ANB +20 +10 +30
Goniac angle ArGoMe 1200 1230 1250 Ls–E line -1 mm -10 mm -9.5 mmLi–E line -3 mm -9 mm -8.5 mm
Evaluating the soft tissues changes A–NPg +4.1 mm -2 mm 0 mm
The cephalometric variables have been selected from Tweed (FMA angle, SNA angle, SNB angle, ANB angle), Steiner (SNA angle, SNB angle, SND angle, ANB angle, GoGn–SN angle), McNamara (A–N⊥FH
distance, Pg–N⊥FH distance) and Ricketts (FH–NPg angle, NsaXi–XiPM angle, Ls–E line distance, Li–E line distance, A–NPg distance) analysis.
The cephalometric evaluation before treatment with the old dentures inserted on the residual ridges showed a marked hypodivergent facial structure (<FMA=110, Tweed), and a tendency towards anterior rotation of the mandible. The hypodivergency is also sustained by other VDO determinants showing smaller values com-pared with the normal ones: GoGn–SN, ANS PNS–M, ANSXi–XiPM, ANS–Me. Both the maxilla and the mandible show protrusion (<SNA=850, <SNB=840). Other determinants of the horizontal position of the mandible suggest the same diagnosis: BaNA (“maxillary depth angle”), A–N⊥FH, SND, FH–NPg, Pg–N⊥FH.
The sagittal intermaxillary discrepancy is relatively reduced (ANB angle= +10), probably due to the specific resorption pattern of the two residual ridges (on the buccal aspect of the maxillary ridge and the lingual aspect of the mandibular ridge) and to the tendency of protrusion of the edentulous mandible (which can turn a normal Class I relationship into a pseudo Class III relationship); in addition, the close interaction between the horizontal and vertical planes makes the low angle pattern (the decrease of the mandible compass) to be horizontally translated into a edge-to-edge inter-maxillary relative spatial position.
The general profile appearance is concave with both lips in a retrognathic position from the esthetic line E and A point, behind NPg-line.
After the treatment, the cephalometric characteristics of the new prosthetic situation were evaluated.
The hypodivergency was adjusted by increasing the vertical dimension of the new dentures (<FMA increased from 110 to 160). The analysis showed no changes in the maxillary structures (SNA and BaNA angles remained unchanged following the insertion of the new prostheses). Increasing the vertical dimension induced the posterior rotation of the mandible, which improved the maxillo-mandibular discrepancy (<ANB=+30), due to the smaller SNB angle value (from 840 to 820). The concave profile is slightly improved.
In conclusion, all the main OVD parameters used in our evaluation showed a decreased OVD of the old

Iuliana Babiuc et al.
710
dentures, which was adjusted by the treatment. The results correspond with the clinical picture, where the new set of dentures with an increased vertical dimension led to an improved oral condition and esthetics.
Discussion
Complete dentures are foreign objects in the oral cavity that are accepted and tolerated by the tissue to a certain degree. A biopsy study, conducted on individual patients prior to and after the application of complete dentures, showed that after wearing the dentures for three months, the underlying mucosa showed an increased amount of keratinization [3]. Wearing well-adapted dentures is not harmful to the epithelium and they can stimulate rather than irritate the underlying mucosa [4–6].
However, ill-fitting complete dentures can alter the character, condition and form of the underlying oral tissues. Abnormalities caused by local, mechanical, or systemic factors must receive proper diagnosis and treatment [2, 7]. Some forms of soft tissues pathology, as papillary hyperplasia of the palate and candidosis are common in associations with old dentures and can look alarming [8]. Clinicians should examine very carefully the entire mouth and the dentures in order to establish the condition of the supporting tissues and to identify any faults of the existing dentures. It is important for both the clinician and the patient to determine the cause of the existing pathology in order to correct it with the new dentures [9]. The physical condition of the patient and his cooperation during and after treatment were observed to be significant factors in the treatment of chronic denture stomatitis [10].
Denture stomatitis is a form of erythematous candi-diasis in which the diffuse redness and inflammation of the mucosa matches the area covered by the denture. It appears most often in the palate and might take an acute or chronic form [11, 12]. It is generally caused by a mixed microflora that includes Candida and pseudo-hyphae, associated with poor denture hygiene, tissue trauma from an ill-fitting denture, constant wearing of the denture, dry mouth, systemic diseases and defi-ciencies of the immune system [13]. Frequently, this form of stomatitis is not an actual infection, since the yeasts and the pseudohyphae are not evident in the epithelium of the biopsy specimens [14].
Excessive thickness of the mucosa causes movement during the use of a complete denture, which may impede a proper stability and encourage the hyperplasia of the fibrous connective tissue [15]. Old lesions may appear as a circumscribed mass of tissue varying in size [12]. Denture hyperplasia has a multi-factorial etiology, which includes wearing the denture day and night, poor denture hygiene, overextension of the denture and placement of arbitrary relief [16]. The small lesions usually recede in two months if the denture is reduced or if the patient does not wear the denture. Large lesions may require a surgical removal.
Moderate intermittent forces exerted on the bony ridge by a prosthesis may be stimulating and help
preserve rather than destroy the bony ridge. A good maintenance of the soft and hard tissues is given by a proper frequency, intensity, duration, direction of the forces [17]. Excessive pressure plays a role in the osteoclastic resorption of bone tissue, due to a circulatory disturbance in the periosteum or bone marrow. The main destructive mechanical factors in complete dentures are improper contour of the impression surface of the denture, improper coverage by the denture impression surface, insufficient interocclusal surface and occlusal disharmony [18].
Changes in color, firmness, contour, tone, and thickness of soft tissues were seen after the removal of ill-fitting dentures, with an average change of 0.136 mm [19]. Cross sections of casts before and after tissue recovery can show the extent of the deformation in tissue contours. Intraoral radiographs can also be used to evaluate the changes in the soft tissue and residual ridge after the removal of the dentures for 72 hours.
Cephalometric analysis can be used to evaluate the effect of prosthodontic rehabilitation on the supporting bony structures [20–27]. Cephalometric radiographs with dentures in place and markers in the molar and bicuspid regions make the contour tissue changes more exact to measure [28].
Before recording impressions for the new dentures, it is essential to improve the health of the denture-bearing areas. Without any preliminary treatment, any errors existing in the previous dentures could be perpetuated. Loss of retention or stability and occlusal relationship changes can be a cause of ill-fitting dentures and these discrepancies can be hidden because of the ability of soft tissues to accommodate. The existing dentures should be assessed whether they can be used as a reference for the new dentures.
The tissue conditioning can be easily achieved with the rest of the underlying tissue. Abused and deformed soft tissues should be allowed to recover and return as closely as possible to normal form before impressions for new dentures are made. Healthy tissues are also important while recording inter-arch relations, because if these were made on deformed tissues, occlusal errors would be perpetuated on the new denture. Dentures, which have been constructed on abused tissues, impinge on the freeway space [29]. The recovery of the underlying tissues can be achieved by the complete removal of the dentures from the mouth for 48 to 72 hours. If the dentures cannot remain out of the mouth for that period of time, they should be left out of the mouth overnight, and all the excessive pressure areas of the denture should be relieved [18].
Tissue conditioners can be placed in the denture to treat an irritated underlying mucosa. Initially, they display a plastic phase, which allows them to adapt to the changing shape of distorted tissue as the tissues recover and become healthy. Soft lining materials act to distribute functional stress uniformly [30].
It is important to adjust the vertical dimensions of the old dentures. A decreased vertical dimension may lead to excessive or misdirected forces applied to the residual ridges and to the soft tissues. Acrylic can be added on the occlusal surface of the old denture in order

Correct complete denture rehabilitation, a chance for recovering abused tissues
711
to assess the extent of the vertical dimension increase. Proper occlusion is probably the most important
factor in maintaining tissue health. Occlusal errors will distort alveolar mucosa and cause soft tissue discomfort. A clinical remount procedure is necessary when occlusal discrepancies are suspected, to restore occlusal harmony and establish proper distribution of the forces over the tissue bearing area.
Edentulous patients show a low intake of fiber, vitamin C and other important nutrients [12]. A nutritional deficiency can produce a number of oral symptoms such as atrophy, edema, xerostomia, and reduced healing capability. If nutritional deficiencies are suspected, it may be necessary to obtain a medical consultation to identify and correct the specific deficiency.
It is essential for the patient to develop good oral and denture hygiene habits in order to achieve oral tissue health, esthetics, control of malodor, affirmation of patient’s sense of well being. Significant reduction in inflammation occurred with brushing although no significant reduction in plaque score was found [31]. Candida albicans is known to colonize denture surfaces as well as the underlying soft tissues and can cause candidiasis. It is essential to treat both the tissue and the denture; they should be cleaned thoroughly with a brush. Candida albicans can infiltrate both into the porous acrylic and in the soft lining material [32–34]. Antifungal agents should be used.
Oral massage can stimulate the tissues by increasing the vascularity and thus can help restore the health of the tissue. The massage can be performed with a soft brush, digitally with gauze dipped in warm saline, or by chewing a large bolus of bubble gum.
In case the lesion persists, the inflammatory hyperplasia should be surgically removed, in which case it is recommended to perform a pathological exami-nation of the biopsy specimen, to analyze the potential neoplastic changes in the tissue. The patient may be left with a flat alveolar process with muscle attachments approaching the crest of the ridge, which can cause a limited extension and thereby reduced retention and stability of a complete denture. Vestibuloplasty and ridge augmentation could be considered [15].
Our patient showed a variety of symptoms caused by faulty dentures and it is a good example of how a well conducted treatment can improve the oral condition in a very short period of time.
The maxillary stomatitis extended to the entire denture-bearing area and although it had an inflamma-tory aspect, the microbiological analysis revealed no pathological strains, just as Rossie K et al. showed in their study [14]. We believe it was caused by mecha-nical factors, mainly incorrect occlusal relations, a reduced vertical dimension and a reduced support of the denture. Once these faults were corrected with the new denture, the tissue condition improved considerably.
The reduced vertical dimension and the excessive freeway space caused the angular chelitis. A proper vertical dimension and a proper repositioning of the peri-oral tissues led to the healing of the site in a very short period of time.
The replacement of the lower denture improved the aspect of the leukoplakia present on the alveolar crest of the lower arch. It was probably caused by the denture repair, which might have affected the structure of the acrylic, and also by a poor fit of the denture.
Before taking impressions for the new dentures, we allowed the underlying tissues to rest. The patient was advised to leave the dentures out at nighttime, soaked in denture-cleaning agent.
The support of the new dentures was increased and they were well fitted to the underlying tissues, to provide a proper distribution of the forces. The increased vertical dimension corrected the hypo-divergent pattern of the profile (as shown by the cephalometric analysis), improved aesthetics and helped resolve the symptoms displayed by the oral tissues.
The new dentures displayed a high polish of the surfaces in order to reduce the plaque accumulation. The patient was instructed to clean both the dentures and the tissues thoroughly with a brush and to use denture-cleaning agents.
Conclusions
Faulty prostheses can alter the character, condition and form of the underlying oral tissues. The patholo-gical changes must be carefully examined and resolved, prior to the beginning of the new prosthetic rehabili-tation.
Our patient was treated by correct conventional dentures. The oral health-related quality of life improved considerably following a well conducted prosthetic treatment.
Acknowledgements This article was partially supported by CNCSIS–
UEFISCSU in the No. 254/2007 “Ideas” Research Project entitled: “Improving the restoring conditions and the quality of life of geriatric edentulous patient by preventing the deterioration of oral status”.
References [1] BLOEM T. J., RAZZOOG M. E., An index for assessment of
oral health in the edentulous population, Spec Care Dentist, 1982, 2(3):121–124.
[2] DANDO W. E., BARKER W. S., Tissue conditioning, Clinical Update, 2000, 22(5):11–12.
[3] KAPUR K., SHKLAR G., The effect of complete dentures on alveolar mucosa, J Prosthet Dent, 1963, 13(6):1030–1037.
[4] JONES P. M., Complete dentures and the associated soft tissues, J Prosthet Dent, 1976, 36(2):136–149.
[5] KRAJICEK D. D., DOONER J., PORTER K., Observations on the histologic features of the human edentulous ridge. Part I: Mucosal epithelium, J Prosthet Dent, 1984, 52(4):526–531.
[6] KRAJICEK D. D., DOONER J., PORTER K., Observations on the histologic features of the human edentulous ridge. Part II: Connective tissue, J Prosthet Dent, 1984, 52(5):682–687.
[7] SALINAS T. J., Treatment of edentulism: optimizing outcomes with tissue management and impression techniques, J Prosthodont, 2009, 18(2):97–105.
[8] LAMB D. J., Problems and solution in complete dental prosthetics, Quintessence Publishing, 1993, 20–34.
[9] RAHN A. O., HEARTWELL C. M., Textbook of complete dentures, 5th edition, Lea & Febiger, Philadelphia, 1993, 419–424.
[10] ZAKHARI K. N., MCMURRY W. S., Denture stomatitis and methods influencing its cure, J Prosthet Dent, 1977, 37(2):133–140.

Iuliana Babiuc et al.
712
[11] GIRARD B. JR., LANDRY R. G., GIASSON L., Denture stomatitis: etiology and clinical considerations, J Can Dent Assoc, 1996, 62(10):808–812.
[12] ALLEN P. F., MCCARTHY S., Complete dentures: from planning to problem solving, 1st edition, Quintessence Publishing, 2003, 13–35.
[13] WEBB B. C., THOMAS C. J., WILLCOX M. D., HARTY D. W., KNOX K. W., Candida-associated denture stomatitis. Aetiology and management: a review. Part 2. Oral diseases caused by Candida species, Aust Dent J, 1998, 43(3):160–166.
[14] ROSSIE K., GUGGENHEIMER J., Oral candidiasis: clinical manifestations, diagnosis and treatment, Pract Periodontics Aesthet Dent, 1997, 9(6):635–641; quiz 642.
[15] DESJARDINS R. P., TOLMAN D. E., Etiology and management of hypermobile mucosa overlying the residual alveolar ridge, J Prosthet Dent, 1974, 32(6):619–638.
[16] ETTINGER R. L., The etiology of inflammatory papillary hyperplasia, J Prosthet Dent, 1975, 34(3):254–260.
[17] TAUTIN F. S., Should dentures be worn continuously?, J Prosthet Dent, 1978, 39(4):372–374.
[18] LYTLE R. B., Complete denture construction based on a study of the deformation of the underlying soft tissues, J Prosthet Dent, 1959, 9(3):539–551.
[19] DUKES B. S., An evaluation of soft tissue responses following removal of ill-fitting dentures, J Prosthet Dent, 1980, 43(3):251–253.
[20] CIFTÇI Y., KOCADERELI I., CANAY S., SENYILMAZ P., Cephalo-metric evaluation of maxillomandibular relationships in patients wearing complete dentures: a pilot study, Angle Orthod, 2005, 75(5):821–825.
[21] PĂUNA M. R., Studiul rapoartelor mandibulo-maxilare la edentatul total protezat prin analiză cefalometrică asistată de calculator, PhD thesis, U.M.Ph. Bucharest, 1995.
[22] TUNCAY O. C., THOMSON S., ABADI B., ELLINGER C., Cephalometric evaluation of the changes in patients wearing complete dentures. A ten-year longitudinal study, J Prosthet Dent, 1984, 51(2):169–180.
[23] MONTEITH B. D., A cephalometric method to determine the angulation of the occlusal plane in edentulous patients, J Prosthet Dent, 1985, 54(1):81–87.
[24] MONTEITH B. D., Cephalometrically programmed adjustable plane: a new concept in occlusal plane orientation for complete-denture patients, J Prosthet Dent, 1985, 54(3):388–394.
[25] SOFOU A. M., DIAKOYIANNI-MORDOHAI I., EMMANOUEL I., MARKOVITSI H., PISSIOTIS A. L., Using cephalometry to evaluate maxillomandibular relationships in complete den-ture construction, Int J Prosthodont, 1993, 6(6):540–545.
[26] MONTEITH B. D., Evaluation of a cephalometric method of occlusal plane orientation for complete dentures, J Prosthet Dent, 1986, 55(1):64–69.
[27] KELLY E., Changes caused by a mandibular removable partial denture opposing a maxillary complete denture, J Prosthet Dent, 1972, 27(2):140–150.
[28] WILSON W., Tissue conditioning utilizing dynamic adaptive stress, J Prosthet Dent, 1961, 11(5):804–815.
[29] LYTLE R. B., The management of abused oral tissues in complete denture construction, J Prosthet Dent, 1957, 7(1):27–42.
[30] KAWANO F., TADA N., NAGAO K., MATSUMOTO N., The influence of soft lining materials on pressure distribution, J Prosthet Dent, 1991, 65(4):567–575.
[31] CHAMBERLAIN B. B., BERNIER S. H., BLOEM T. J., RAZZOOG M. E., Denture plaque control and inflammation in the edentulous patient, J Prosthet Dent, 1985, 54(1):78–81.
[32] WEBB B. C., THOMAS C. J., WILLCOX M. D., HARTY D. W., KNOX K. W., Candida-associated stomatitis. Aetiology and management: a review. Part 1. Factors influencing distri-bution of Candida species in the oral cavity, Aust Dent J, 1998, 43(1):45–50.
[33] PEREIRA-CENCI T., DEL BEL CURY A. A., CRIELAARD W., TEN CATE J. M., Development of Candida-associated denture stomatitis: new insights, J Appl Oral Sci, 2008, 16(2):86–94.
[34] RADFORD D. R., CHALLACOMBE S. J., WALTER J. D., Denture plaque and adherence of Candida albicans to denture-base materials in vivo and in vitro, Crit Rev Oral Biol Med, 1999, 10(1):99–116.
Corresponding author Iuliana Babiuc, DDS, PhD candidate, Department of Removable Prosthodontics, Faculty of Dentistry, “Carol Davila” University of Medicine and Pharmacy, 37 Dionisie Lupu Street, 020021 Bucharest, Romania; Phone +40724–776 020, e-mail: [email protected] Received: August 25th, 2009
Accepted: October 20th, 2009