Embed Size (px)
DESCRIPTION
Challenging Cases in Cancer: Integration of Findings from ASCO 2007 into Clinical Practice Lung Cancer. Corey J. Langer, MD, FACP Medical Director, Thoracic Oncology Fox Chase Cancer Center Philadelphia, PA. Extensive Stage Small Cell Lung Cancer. Case 1 Extensive Stage SCLC. - PowerPoint PPT Presentation
Citation preview
Challenging Cases in Cancer:Integration of Findings from ASCO 2007
into Clinical Practice
Lung Cancer
Corey J. Langer, MD, FACP
Medical Director, Thoracic Oncology
Fox Chase Cancer Center
Philadelphia, PA
Extensive Stage Small Cell Lung Cancer
Case 1Extensive Stage SCLC
• 72-year-old WM former smoker (50 pack-years) presents with cough, DOE and hoarseness over a 6-week course
• CXR suggests a (L) para-hilar infiltrate
• He initially receives antibiotics, but symptoms worsen
• PE is notable for a (L) SCN measuring 2 cm, with focal wheezing in the (L) mid-lung field
• Liver edge extends 3 cm below the RCM with focal tenderness
Case 1Extensive Stage SCLC
• Follow-up CXR demonstrates worsening infiltrate
• CT shows a dense, coalescent mass in the (L) hilar area measuring 9 x 8 cm with prominent hilar and mediastinal adenopathy; multiple, bilateral pulmonary nodules; and hepatic masses ranging between 2-3 cm in size and occupying 15% of the hepatic volume
• FNA of an anterior hepatic mass demonstrates classical SCLC
• PS is 1
• CBC and chemistries are WNL
Case 1Extensive Stage SCLC
Which of the following is appropriate therapy for this patient?
1. Irinotecan + cisplatin
2. Etoposide + cisplatin
3. Irinotecan + carboplatin
4. Etoposide + carboplatin
5. All of the above
Case 1Extensive Stage SCLC
Which of the following is appropriate therapy for this patient?
1. Irinotecan + cisplatin
2. Etoposide + cisplatin
3. Irinotecan + carboplatin
4. Etoposide + carboplatin
5. All of the above
Recommended Approach: All of the options above are appropriate for this patient.
Case 1Extensive Stage SCLC
Bevacizumab has been proven in phase III trials to enhance therapeutic outcome in patients receiving cisplatin in combination with either irinotecan or etoposide
1. True
2. False
Case 1Extensive Stage SCLC
Bevacizumab has been proven in phase III trials to enhance therapeutic outcome in patients receiving cisplatin in combination with either irinotecan or etoposide
1. True
2. False
Answer: False, bevacizumab has not been proven in phase III trials to
enhance outcomes.
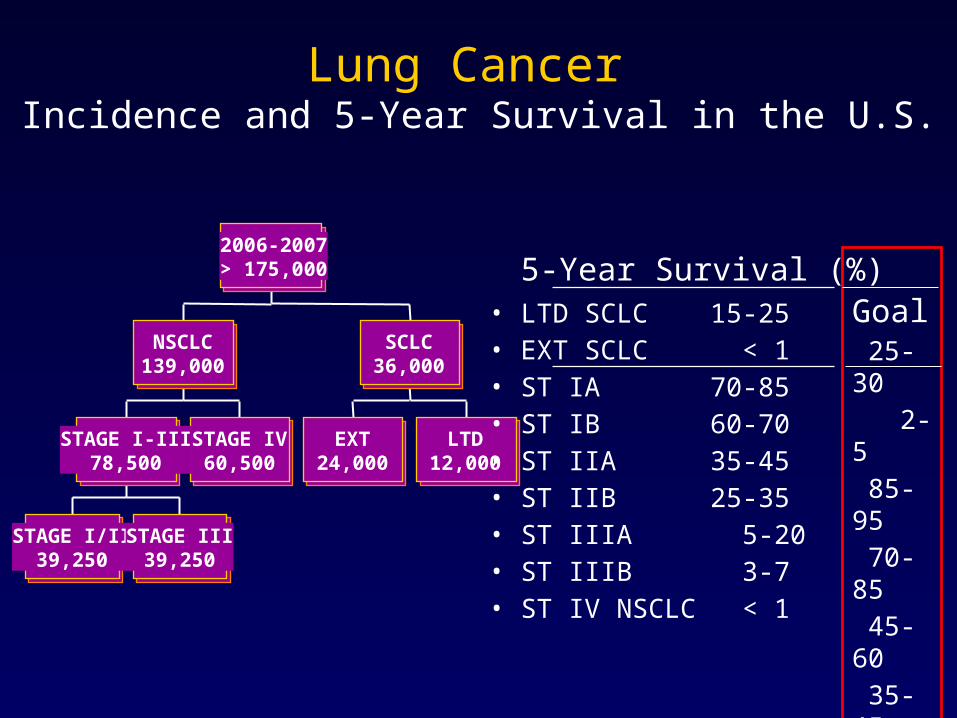
Lung Cancer Incidence and 5-Year Survival in the U.S.
STAGE I/II39,250
STAGE III39,250
STAGE I-III78,500
STAGE IV60,500
NSCLC139,000
EXT24,000
LTD12,000
SCLC36,000
2006-2007> 175,000 5-Year Survival (%)
• LTD SCLC 15-25• EXT SCLC < 1• ST IA 70-85• ST IB 60-70• ST IIA 35-45• ST IIB 25-35• ST IIIA 5-20• ST IIIB 3-7• ST IV NSCLC < 1
Goal 25-30 2-5 85-95 70-85 45-60 35-45 20-30 10-20 2-5
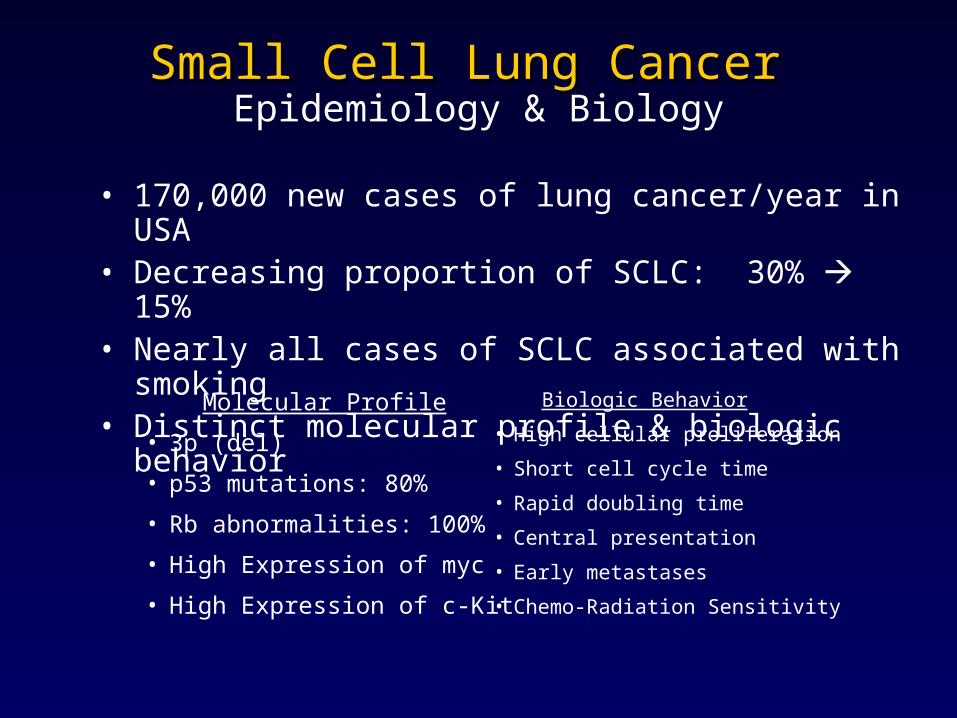
Small Cell Lung Cancer Small Cell Lung Cancer Epidemiology & Biology
Biologic Behavior
• High cellular proliferation
• Short cell cycle time
• Rapid doubling time
• Central presentation
• Early metastases
• Chemo-Radiation Sensitivity
Molecular Profile
• 3p (del)
• p53 mutations: 80%
• Rb abnormalities: 100%
• High Expression of myc
• High Expression of c-Kit
• 170,000 new cases of lung cancer/year in USA• Decreasing proportion of SCLC: 30% 15%• Nearly all cases of SCLC associated with smoking• Distinct molecular profile & biologic behavior
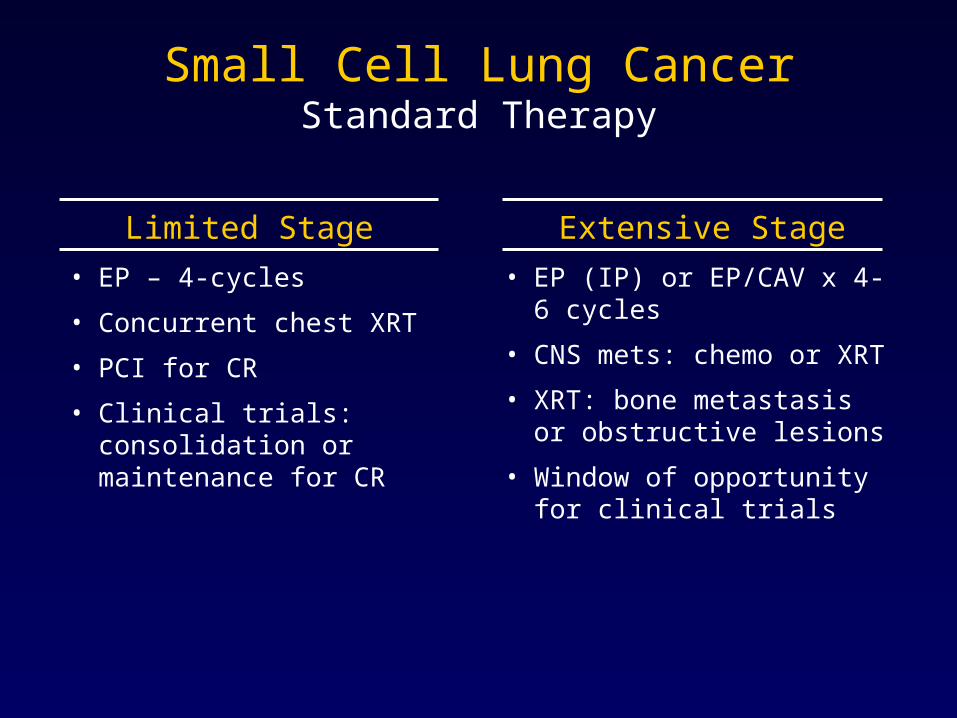
Small Cell Lung CancerStandard Therapy
Limited Stage
• EP – 4-cycles
• Concurrent chest XRT
• PCI for CR
• Clinical trials: consolidation or maintenance for CR
Extensive Stage
• EP (IP) or EP/CAV x 4-6 cycles
• CNS mets: chemo or XRT
• XRT: bone metastasis or obstructive lesions
• Window of opportunity for clinical trials
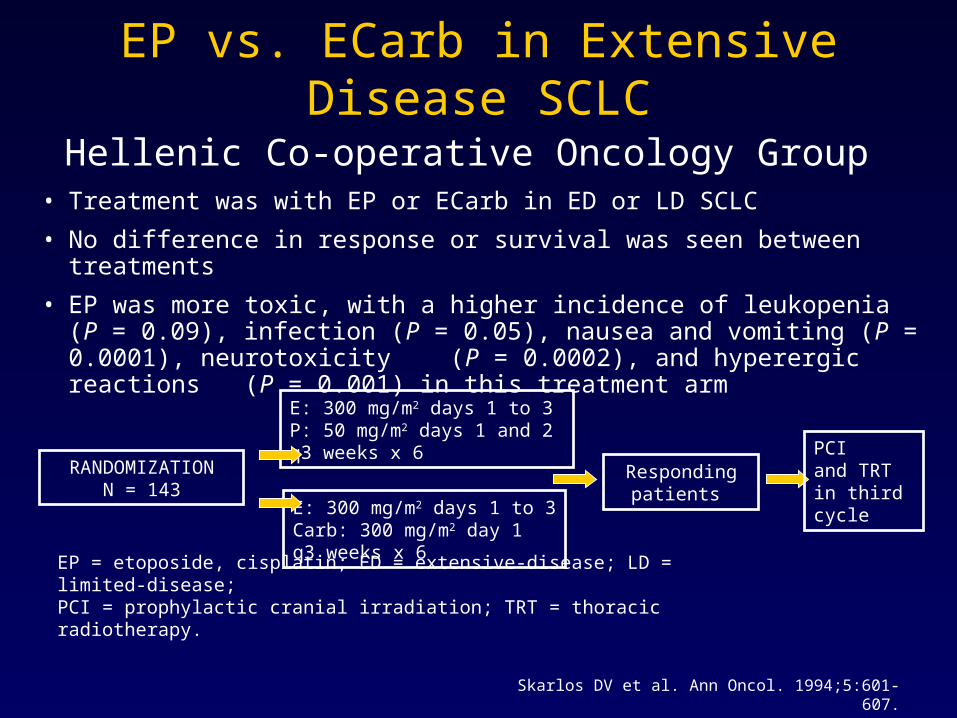
EP vs. ECarb in Extensive Disease SCLCHellenic Co-operative Oncology Group
EP = etoposide, cisplatin; ED = extensive-disease; LD = limited-disease; PCI = prophylactic cranial irradiation; TRT = thoracic radiotherapy.
RANDOMIZATIONN = 143
E: 300 mg/m2 days 1 to 3 P: 50 mg/m2 days 1 and 2q3 weeks x 6
E: 300 mg/m2 days 1 to 3Carb: 300 mg/m2 day 1q3 weeks x 6
Responding patients
PCI and TRTin third cycle
• Treatment was with EP or ECarb in ED or LD SCLC
• No difference in response or survival was seen between treatments
• EP was more toxic, with a higher incidence of leukopenia (P = 0.09), infection (P = 0.05), nausea and vomiting (P = 0.0001), neurotoxicity (P = 0.0002), and hyperergic reactions (P = 0.001) in this treatment arm
Skarlos DV et al. Ann Oncol. 1994;5:601-607.
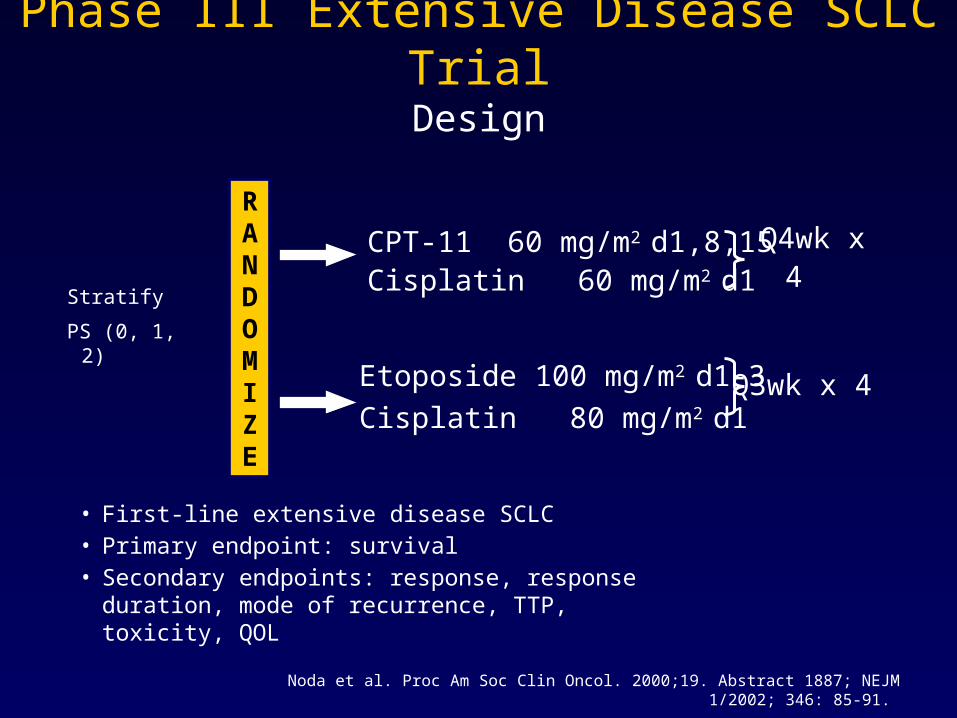
• First-line extensive disease SCLC• Primary endpoint: survival• Secondary endpoints: response, response duration,
mode of recurrence, TTP, toxicity, QOL
Phase III Extensive Disease SCLC TrialDesign
Noda et al. Proc Am Soc Clin Oncol. 2000;19. Abstract 1887; NEJM 1/2002; 346: 85-91.
Stratify
PS (0, 1, 2)
CPT-11 60 mg/m2 d1,8,15Cisplatin 60 mg/m2 d1
Etoposide 100 mg/m2 d1-3
Cisplatin 80 mg/m2 d1
Q4wk x 4
Q3wk x 4
RANDOMIZE
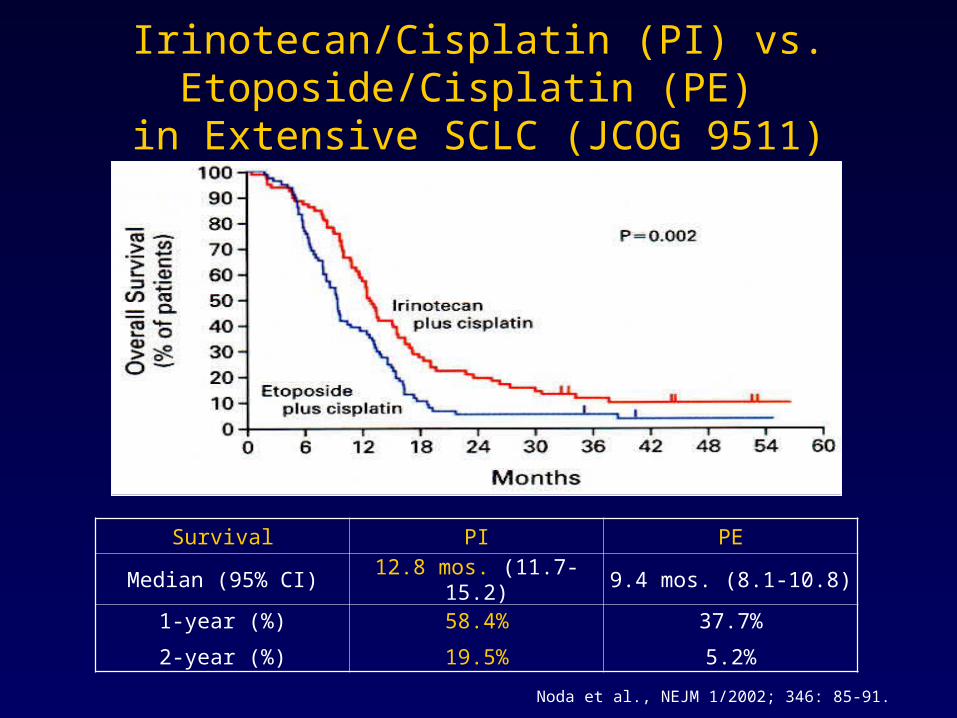
Irinotecan/Cisplatin (PI) vs. Etoposide/Cisplatin (PE) in Extensive SCLC (JCOG 9511)
Survival PI PE
Median (95% CI) 12.8 mos. (11.7-15.2) 9.4 mos. (8.1-10.8)
1-year (%)
2-year (%)
58.4%
19.5%
37.7%
5.2%
Noda et al., NEJM 1/2002; 346: 85-91.
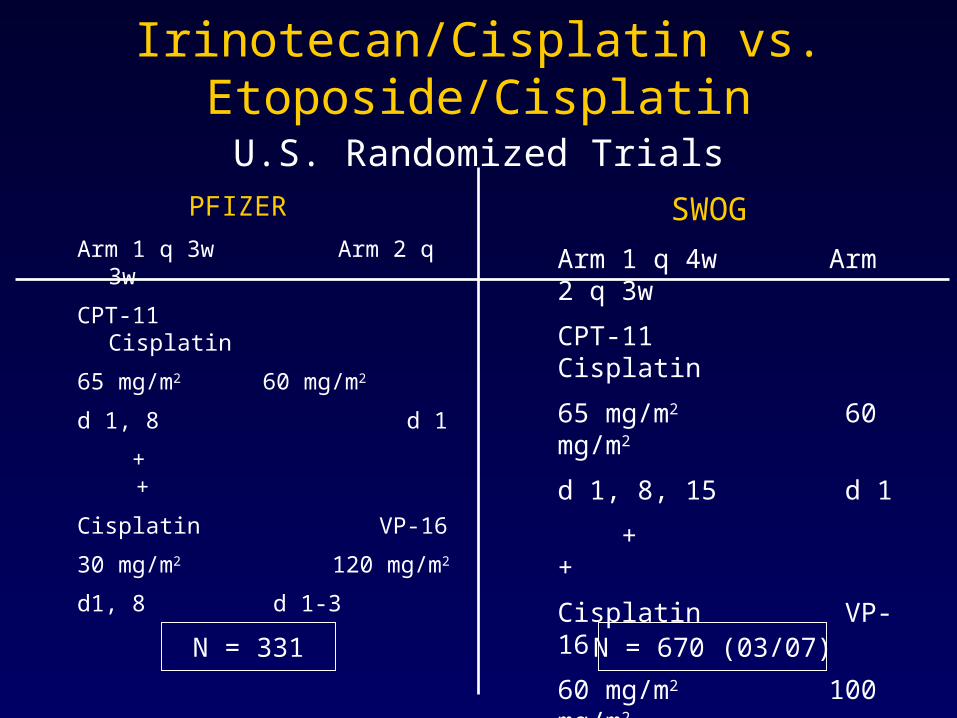
Irinotecan/Cisplatin vs. Etoposide/Cisplatin U.S. Randomized Trials
SWOG
Arm 1 q 4w Arm 2 q 3w
CPT-11 Cisplatin
65 mg/m2 60 mg/m2
d 1, 8, 15 d 1
+ +
Cisplatin VP-16
60 mg/m2 100 mg/m2
d1 d 1-3
PFIZER
Arm 1 q 3w Arm 2 q 3w
CPT-11 Cisplatin
65 mg/m2 60 mg/m2
d 1, 8 d 1
+ +
Cisplatin VP-16
30 mg/m2 120 mg/m2
d1, 8 d 1-3
N = 331 N = 670 (03/07)
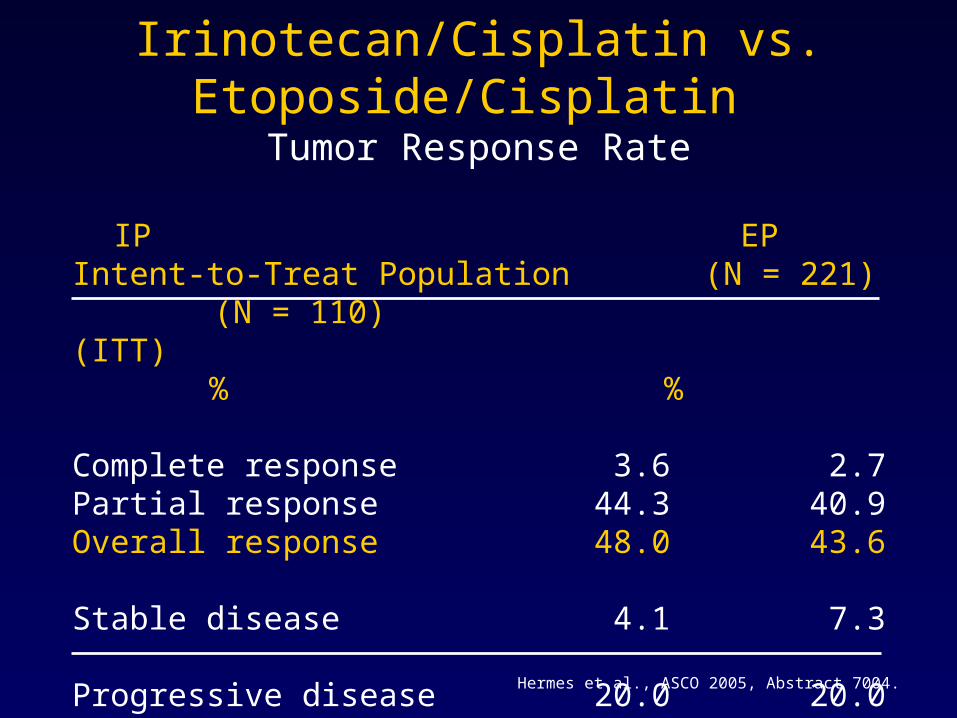
Irinotecan/Cisplatin vs. Etoposide/Cisplatin Tumor Response Rate
IP EPIntent-to-Treat Population (N = 221) (N = 110)(ITT) % %
Complete response 3.6 2.7Partial response 44.3 40.9Overall response 48.0 43.6
Stable disease 4.1 7.3
Progressive disease 20.0 20.0Not evaluable 28.1 29.1
Hermes et al., ASCO 2005, Abstract 7004.
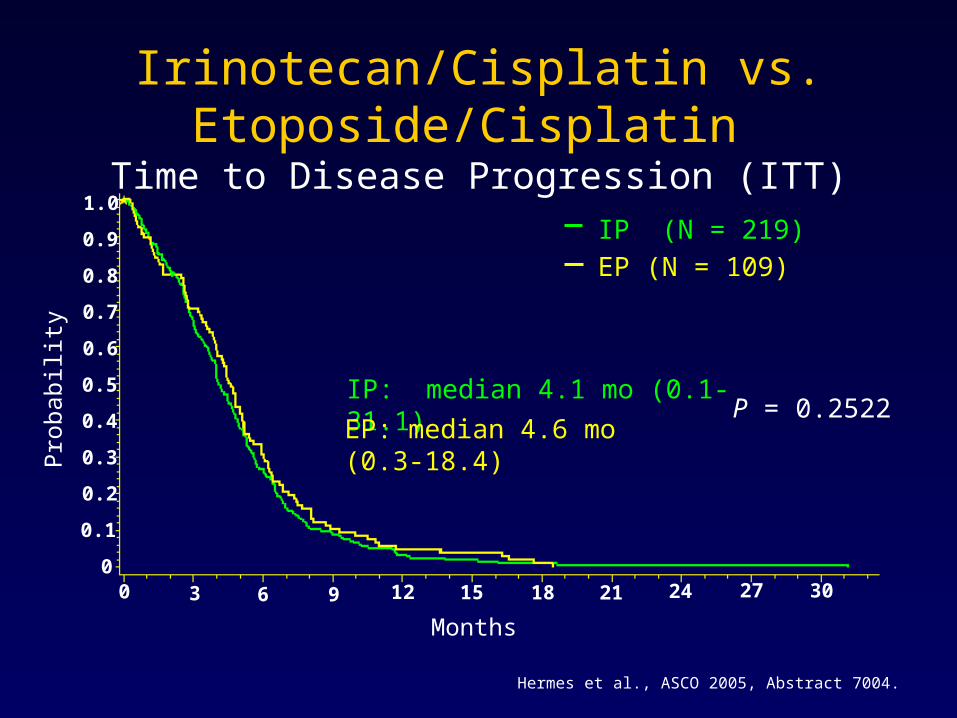
Irinotecan/Cisplatin vs. Etoposide/Cisplatin Time to Disease Progression (ITT)
Months
Pro
babi
lity
IP: median 4.1 mo (0.1-31.1)
EP: median 4.6 mo (0.3-18.4)P = 0.2522
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 3 6 9 12 15 18 21 24 27 30
IP (N = 219)
EP (N = 109)
Hermes et al., ASCO 2005, Abstract 7004.
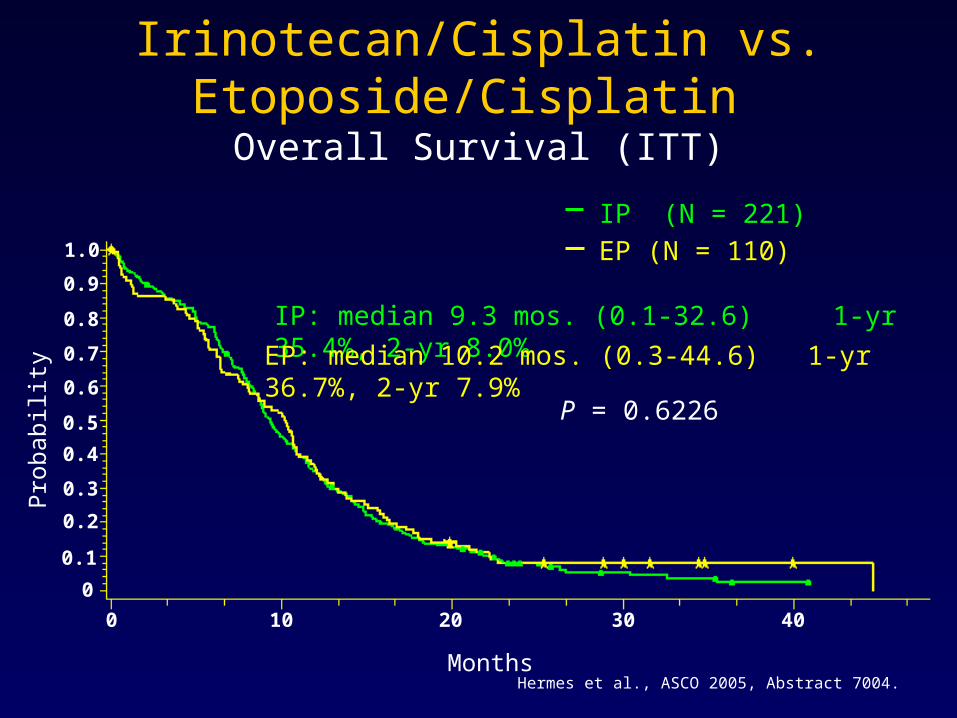
Irinotecan/Cisplatin vs. Etoposide/Cisplatin Overall Survival (ITT)
Months
IP: median 9.3 mos. (0.1-32.6) 1-yr 35.4%, 2-yr 8.0%
EP: median 10.2 mos. (0.3-44.6) 1-yr 36.7%, 2-yr 7.9%
Pro
babi
lity
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
0 10 20 30 40
IP (N = 221)
EP (N = 110)
P = 0.6226
Hermes et al., ASCO 2005, Abstract 7004.
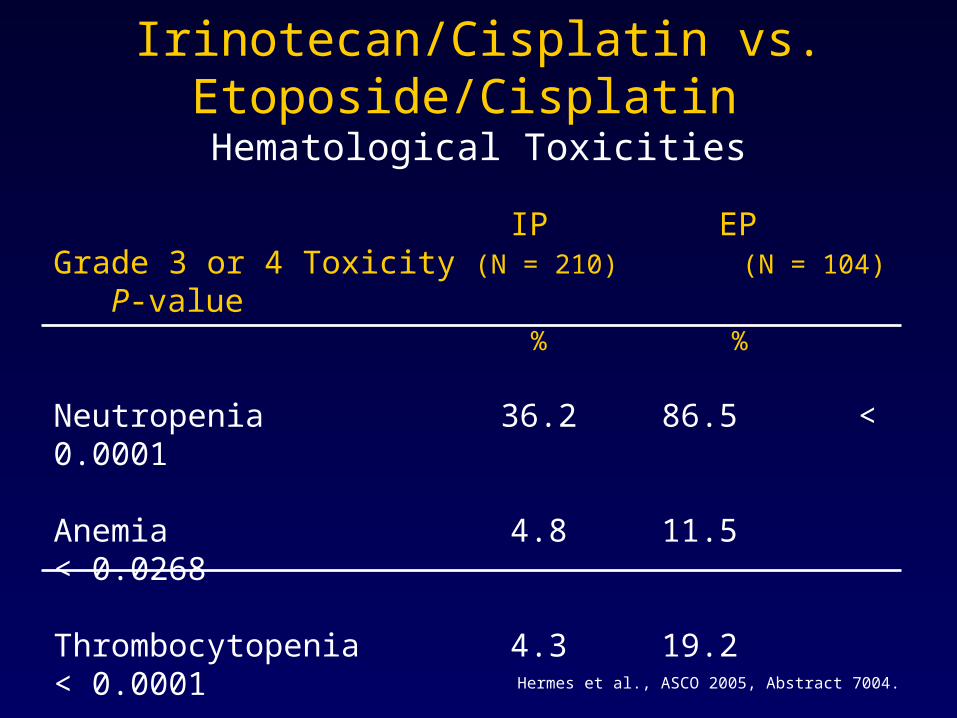
Irinotecan/Cisplatin vs. Etoposide/Cisplatin Hematological Toxicities
IP EPGrade 3 or 4 Toxicity (N = 210) (N = 104) P-value
% %
Neutropenia 36.2 86.5 < 0.0001
Anemia 4.8 11.5 < 0.0268
Thrombocytopenia 4.3 19.2 < 0.0001
Hermes et al., ASCO 2005, Abstract 7004.
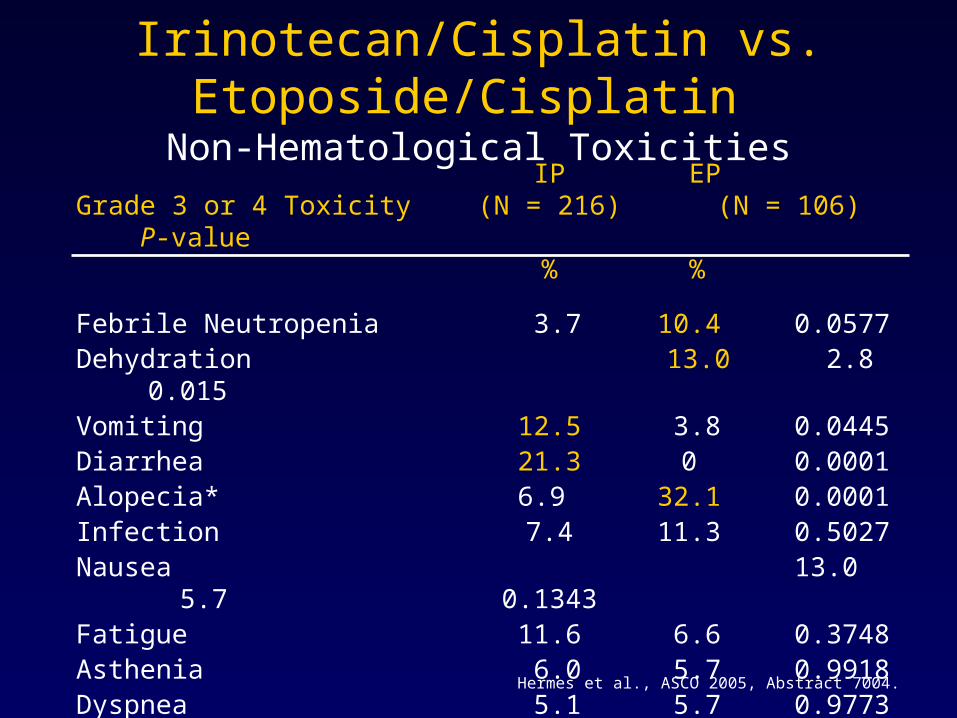
Irinotecan/Cisplatin vs. Etoposide/Cisplatin Non-Hematological Toxicities
IP EPGrade 3 or 4 Toxicity (N = 216) (N = 106) P-value
% %
Febrile Neutropenia 3.7 10.4 0.0577Dehydration 13.0 2.8 0.015Vomiting 12.5 3.8 0.0445Diarrhea 21.3 0 0.0001Alopecia* 6.9 32.1 0.0001Infection 7.4 11.3 0.5027Nausea 13.0 5.7 0.1343Fatigue 11.6 6.6 0.3748Asthenia 6.0 5.7 0.9918Dyspnea 5.1 5.7 0.9773Anorexia 5.6 1.9 0.3164
*Grade 2
Hermes et al., ASCO 2005, Abstract 7004.
Irinotecan/Cisplatin vs. Etoposide/Cisplatin Conclusions
• Treatment with this regimen of IP results in similar efficacy outcomes when compared with EP– Response Rates– Time to Progression– Overall Survival
• IP results in statistically significant lower rates of – Neutropenia and neutropenic fever– Anemia and thrombocytopenia
• IP results in statistically significant higher rates of – Diarrhea, vomiting and dehydration
Hermes et al., ASCO 2005, Abstract 7004.
Irinotecan/Cisplatin vs. Etoposide/Cisplatin Conclusions (cont.)
• The dose intensity of Irinotecan delivered on this trial was higher compared to the JCOG trial
• The explanation(s) for the differences in outcomes between this effort and the JCOG trial remain speculative; they may be accounted for by: – Pharmacogenomic disparities– Platinum dose and schedule changes– Patient characteristic differences in the study populations
Hermes et al., ASCO 2005, Abstract 7004.
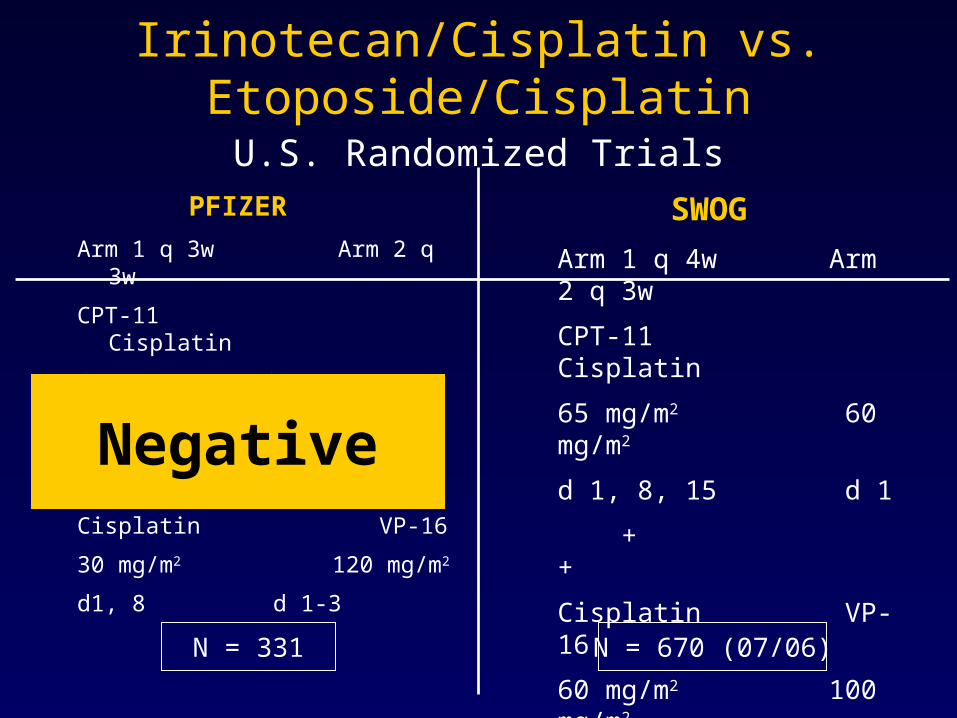
Irinotecan/Cisplatin vs. Etoposide/Cisplatin U.S. Randomized Trials
SWOG
Arm 1 q 4w Arm 2 q 3w
CPT-11 Cisplatin
65 mg/m2 60 mg/m2
d 1, 8, 15 d 1
+ +
Cisplatin VP-16
60 mg/m2 100 mg/m2
d1 d 1-3
PFIZER
Arm 1 q 3w Arm 2 q 3w
CPT-11 Cisplatin
65 mg/m2 60 mg/m2
d 1, 8 d 1
+ +
Cisplatin VP-16
30 mg/m2 120 mg/m2
d1, 8 d 1-3
N = 331 N = 670 (07/06)
Negative
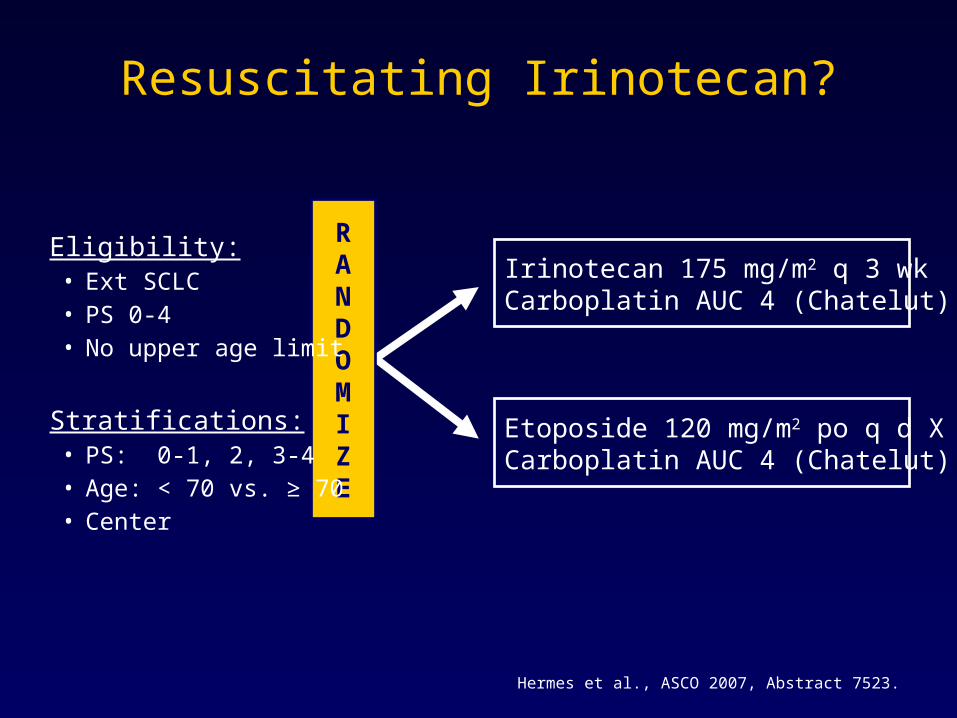
Resuscitating Irinotecan?
Hermes et al., ASCO 2007, Abstract 7523.
Irinotecan 175 mg/m2 q 3 wkCarboplatin AUC 4 (Chatelut)
Etoposide 120 mg/m2 po q d X 5Carboplatin AUC 4 (Chatelut)
RANDOMIZE
Eligibility:• Ext SCLC• PS 0-4• No upper age limit
Stratifications:• PS: 0-1, 2, 3-4• Age: < 70 vs. ≥ 70• Center
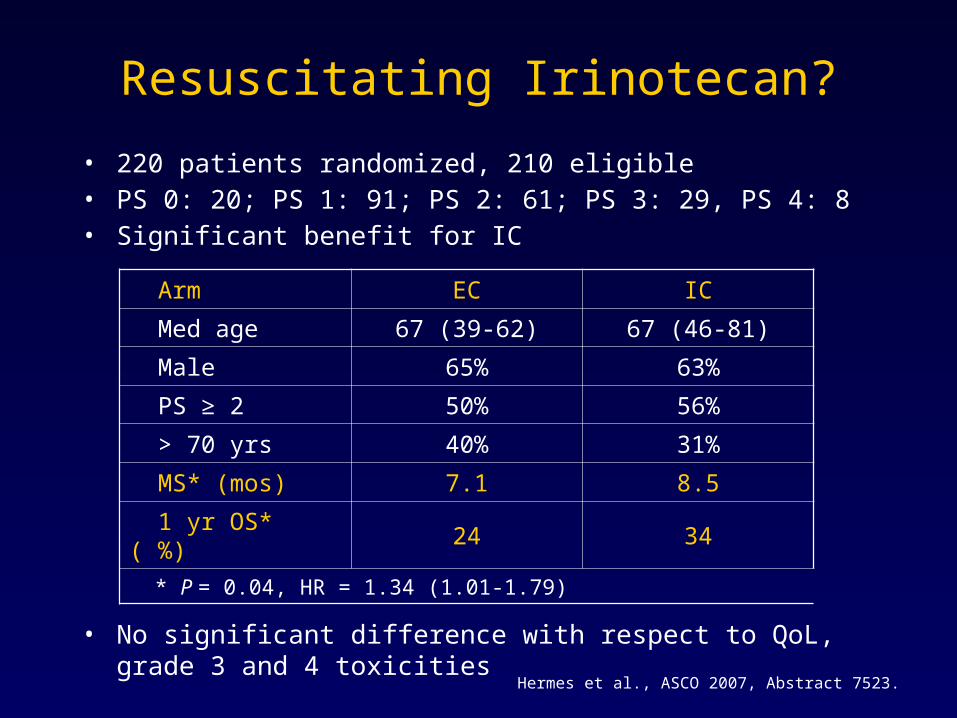
Resuscitating Irinotecan?
• 220 patients randomized, 210 eligible• PS 0: 20; PS 1: 91; PS 2: 61; PS 3: 29, PS 4: 8• Significant benefit for IC
• No significant difference with respect to QoL, grade 3 and 4 toxicities
Arm EC IC
Med age 67 (39-62) 67 (46-81)
Male 65% 63%
PS ≥ 2 50% 56%
> 70 yrs 40% 31%
MS* (mos) 7.1 8.5
1 yr OS* ( %) 24 34
* P = 0.04, HR = 1.34 (1.01-1.79)
Hermes et al., ASCO 2007, Abstract 7523.
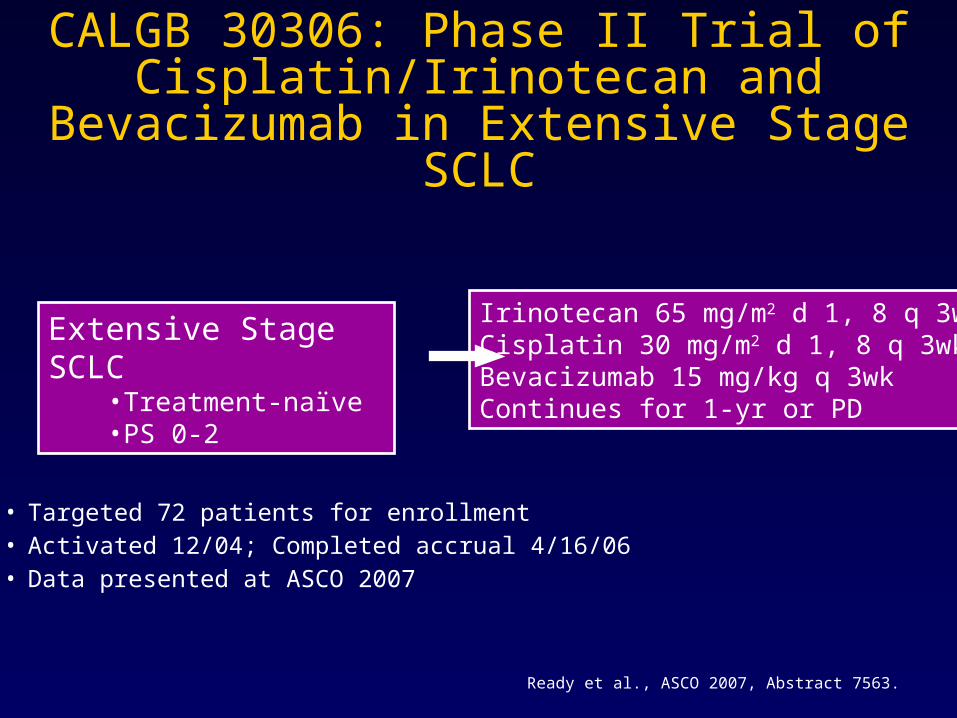
CALGB 30306: Phase II Trial of Cisplatin/Irinotecan and Bevacizumab in
Extensive Stage SCLC
• Targeted 72 patients for enrollment• Activated 12/04; Completed accrual 4/16/06• Data presented at ASCO 2007
Extensive Stage SCLC•Treatment-naïve •PS 0-2
Irinotecan 65 mg/m2 d 1, 8 q 3wkCisplatin 30 mg/m2 d 1, 8 q 3wkBevacizumab 15 mg/kg q 3wkContinues for 1-yr or PD
Ready et al., ASCO 2007, Abstract 7563.
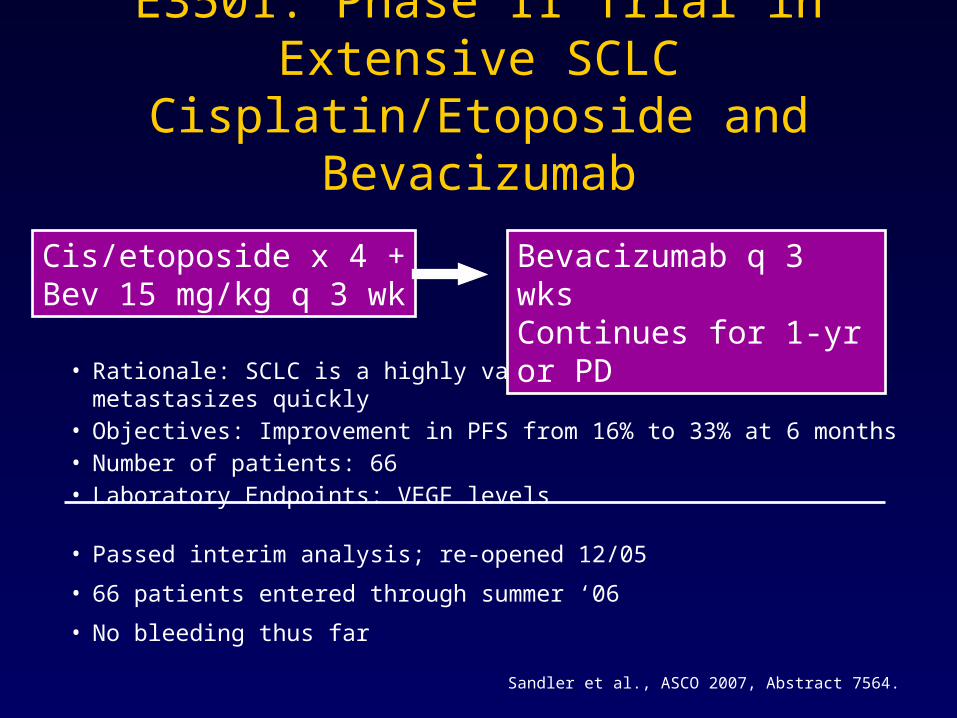
E3501: Phase II Trial in Extensive SCLC Cisplatin/Etoposide and Bevacizumab
• Rationale: SCLC is a highly vascularized tumor which metastasizes quickly• Objectives: Improvement in PFS from 16% to 33% at 6 months• Number of patients: 66• Laboratory Endpoints: VEGF levels
• Passed interim analysis; re-opened 12/05
• 66 patients entered through summer ‘06
• No bleeding thus far
Cis/etoposide x 4 +Bev 15 mg/kg q 3 wk
Bevacizumab q 3 wksContinues for 1-yr or PD
Sandler et al., ASCO 2007, Abstract 7564.
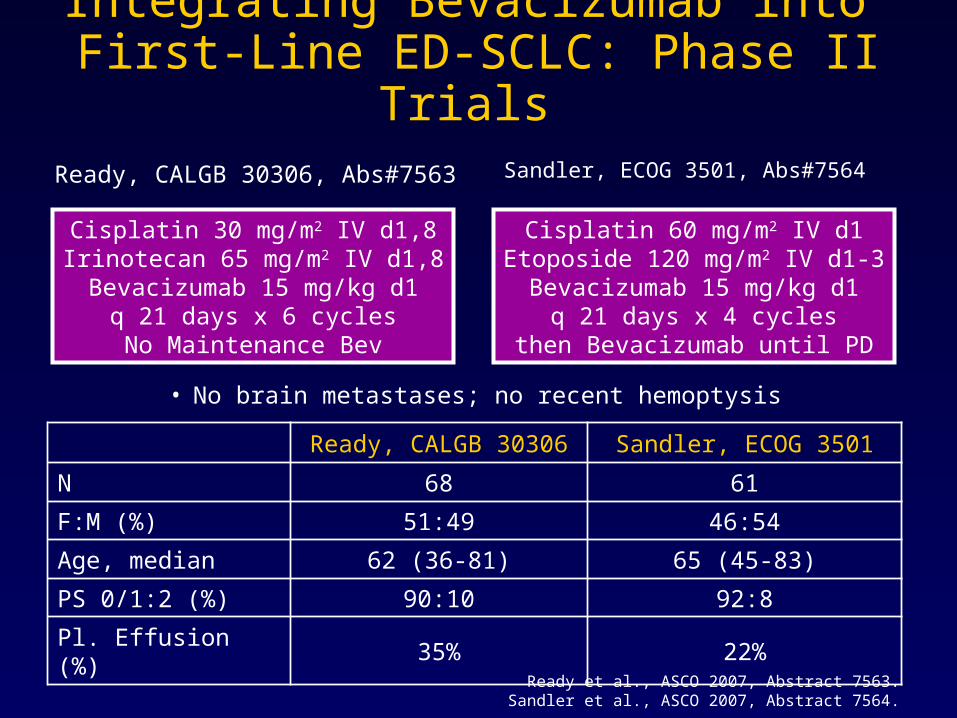
Integrating Bevacizumab into First-Line ED-SCLC: Phase II Trials
Ready, CALGB 30306, Abs#7563 Sandler, ECOG 3501, Abs#7564
Cisplatin 30 mg/m2 IV d1,8Irinotecan 65 mg/m2 IV d1,8Bevacizumab 15 mg/kg d1
q 21 days x 6 cyclesNo Maintenance Bev
Cisplatin 60 mg/m2 IV d1Etoposide 120 mg/m2 IV d1-3
Bevacizumab 15 mg/kg d1q 21 days x 4 cycles
then Bevacizumab until PD
Ready, CALGB 30306 Sandler, ECOG 3501
N 68 61
F:M (%) 51:49 46:54
Age, median 62 (36-81) 65 (45-83)
PS 0/1:2 (%) 90:10 92:8
Pl. Effusion (%) 35% 22%
• No brain metastases; no recent hemoptysis
Ready et al., ASCO 2007, Abstract 7563.Sandler et al., ASCO 2007, Abstract 7564.
• Ready et al., CALGB 30306– No grade 3-5 hemoptysis– One patient died w/thromboembolic CVA, secondary bleeding– Other treatment-related mortality due to FN, sepsis or PNA
• Sandler et al., ECOG 3501– No serious hemoptysis reported– Two treatment related deaths
• Mutli-organ failure• Infection with grade 3/4 neutropenia
• Grade 5 toxicities seen at similar or higher rate with chemo alone as well (e.g., Noda, NEJM 2002 & Hanna JCO 2006)
• Central location does not appear to be correlated with bleeding risk on bevacizumab in Tx of SCLC (vs. squamous histology)
Integrating Bevacizumab into First-Line ED-SCLC: Phase II Trials
Toxicity Results
Ready et al., ASCO 2007, Abstract 7563.Sandler et al., ASCO 2007, Abstract 7564.
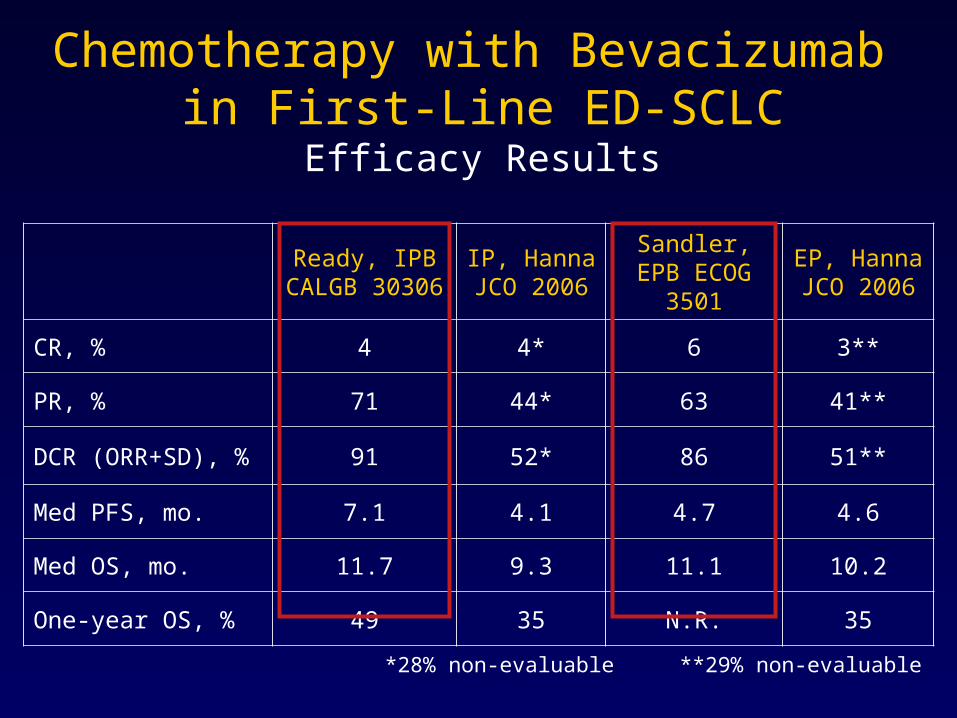
Ready, IPB CALGB 30306
IP, Hanna JCO 2006
Sandler, EPB ECOG 3501
EP, Hanna JCO 2006
CR, % 4 4* 6 3**
PR, % 71 44* 63 41**
DCR (ORR+SD), % 91 52* 86 51**
Med PFS, mo. 7.1 4.1 4.7 4.6
Med OS, mo. 11.7 9.3 11.1 10.2
One-year OS, % 49 35 N.R. 35
*28% non-evaluable **29% non-evaluable
Chemotherapy with Bevacizumab in First-Line ED-SCLC
Efficacy Results
• Neither trial reached the median survival of 12.8 months for cisplatin-irinotecan in Noda, NEJM 2002
• Results of SWOG 0124 still pending
• Both regimens are feasible, with few treatment-related deaths and no evidence of serious hemoptysis
• Encouraging results with bevacizumab vs. US-based historical controls, but phase II trials typically exceed broader experience
• Phase III study of chemo ± bevacizumab is an appropriate consideration
Chemo with Bevacizumab in ED-SCLC Conclusions
Case 1 Extensive Stage SCLC
• Patient receives 4 cycles of systemic therapy with etoposide 100 mg/m2 days 1, 2, and 3 along with carboplatin (AUC 5) every three weeks
– Enters a near CR with complete resolution of the hepatic and pulmonary metastases and SCN
– 80% regression of the primary lung mass and mediastinal adenopathy
• You elect to radiate the remaining volume of tumor in the chest
Case 1Extensive Stage SCLC
Is there a role for PCI in this patient?
1. Yes
2. No
Case 1Extensive Stage SCLC
Is there a role for PCI in this patient?
1. Yes
2. No
Recommended Approach: Yes, this patient should be treated with PCI to improve
outcomes.
Prophylactic Cranial Irradiation (PCI)
• Decreases brain relapse
– Dose related
• Survival advantage of 5%*
– Does not appear dose related
• Neurotoxicity < 10 %
– Found pre-Rx; ± PCI in 50% !
• Timing and dose less certain
*Auperin et al. NEJM(1999) 341: 476-84.
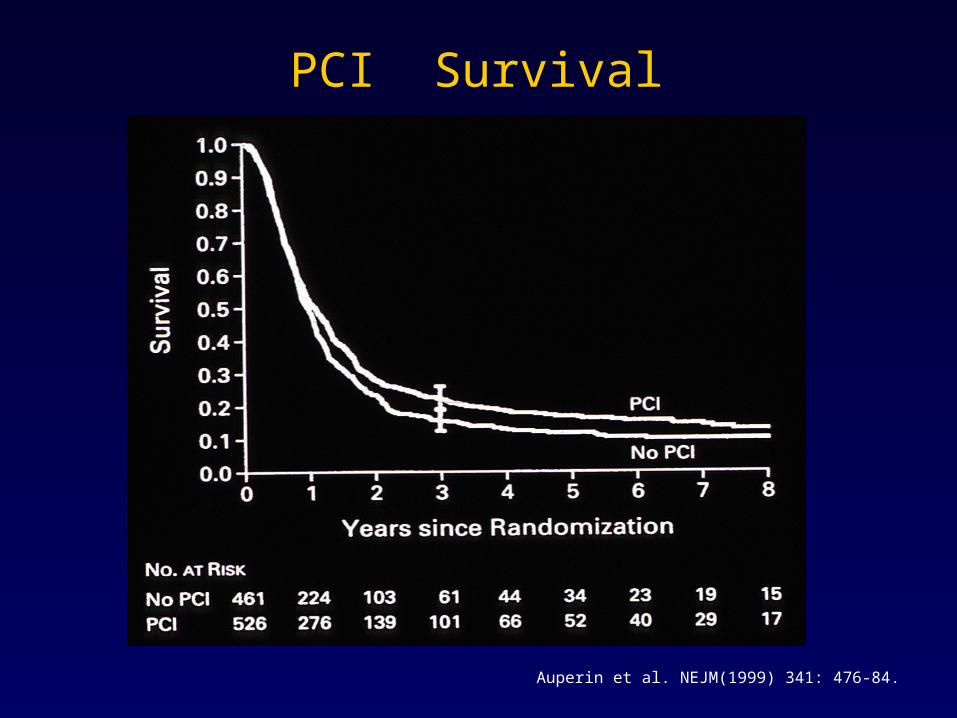
PCI Survival
Auperin et al. NEJM(1999) 341: 476-84.
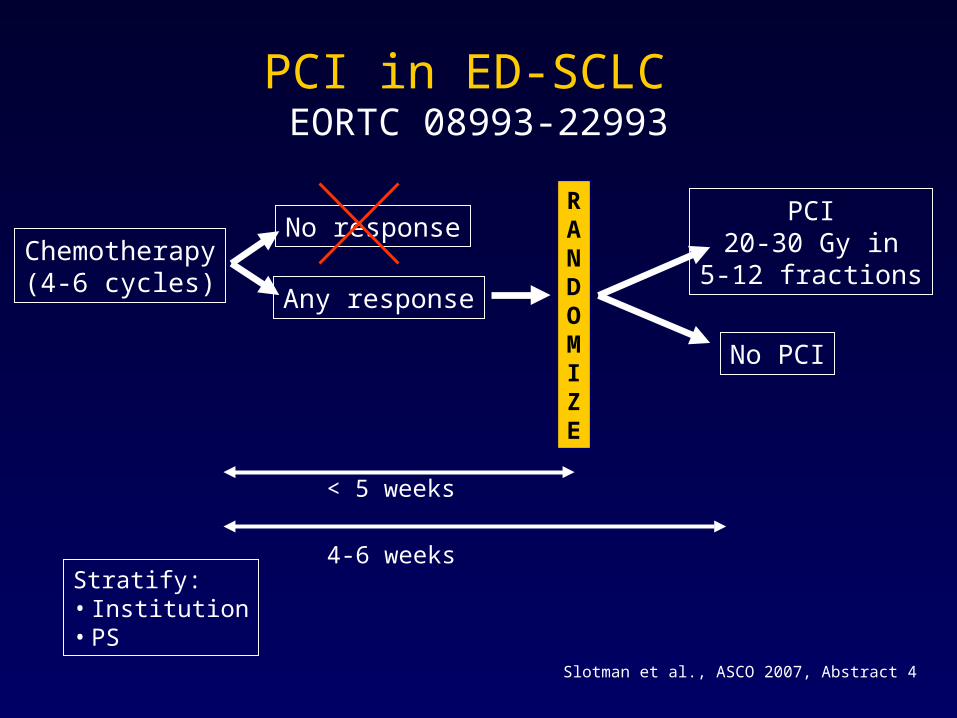
PCI in ED-SCLC EORTC 08993-22993
Chemotherapy(4-6 cycles)
No response
Any response
PCI20-30 Gy in
5-12 fractions
RANDOMIZE
No PCI
Stratify:• Institution• PS
< 5 weeks
4-6 weeks
Slotman et al., ASCO 2007, Abstract 4
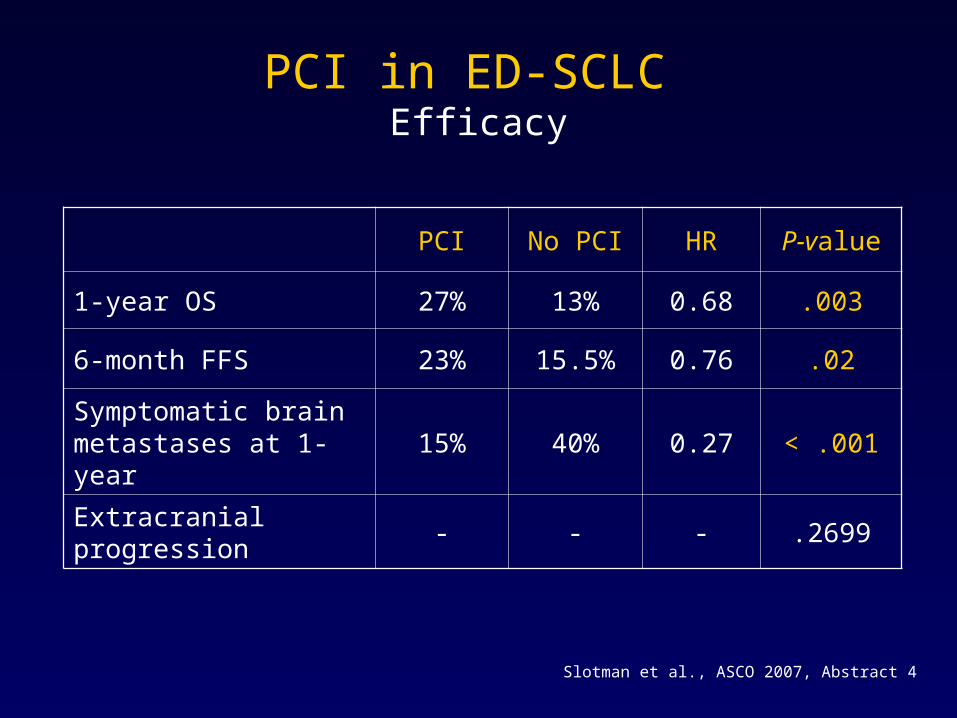
PCI in ED-SCLC Efficacy
PCI No PCI HR P-value
1-year OS 27% 13% 0.68 .003
6-month FFS 23% 15.5% 0.76 .02
Symptomatic brain metastases at 1-year
15% 40% 0.27 < .001
Extracranial progression - - - .2699
Slotman et al., ASCO 2007, Abstract 4
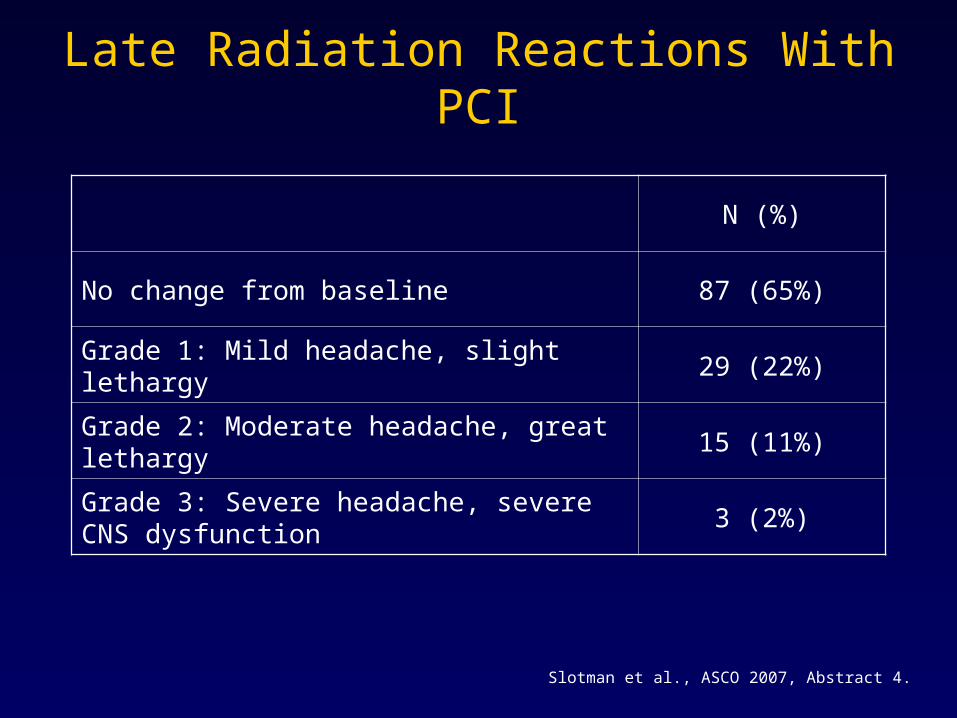
Late Radiation Reactions With PCI
Slotman et al., ASCO 2007, Abstract 4.
N (%)
No change from baseline 87 (65%)
Grade 1: Mild headache, slight lethargy 29 (22%)
Grade 2: Moderate headache, great lethargy 15 (11%)
Grade 3: Severe headache, severe CNS dysfunction
3 (2%)
Case 1Extensive Stage SCLC
• Patient receives PCI and does well
• After 9 months, he ultimately relapses in the chest and liver
Case 1Extensive Stage SCLC
Which of the following agents is FDA-approved for chemo-sensitive relapse of SCLC?
1. Oral topotecan
2. Intravenous topotecan
3. Oral etoposide
4. Intravenous etoposide
5. Paclitaxel
Case 1Extensive Stage SCLC
Which of the following agents is FDA-approved for chemo-sensitive relapse of SCLC?
1. Oral topotecan
2. Intravenous topotecan
3. Oral etoposide
4. Intravenous etoposide
5. Paclitaxel
Answer: Intravenous topotecan is the only FDA-approved agent for
second-line SCLC.
Salvage Therapy for SCLC
• Topotecan: de facto standard
– Not very popular (in US)
• Other options
– Taxanes
– Gemcitabine
– Oral etoposide
– Phase I approaches
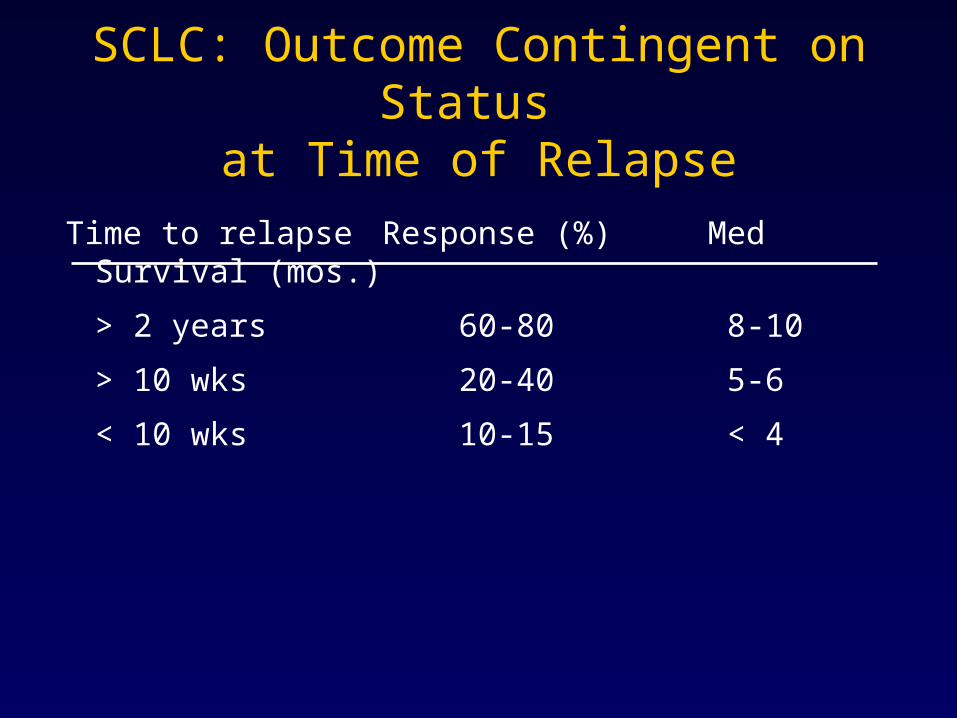
SCLC: Outcome Contingent on Status at Time of Relapse
Time to relapseResponse (%) Med Survival (mos.)
> 2 years 60-80 8-10
> 10 wks 20-40 5-6
< 10 wks 10-15 < 4
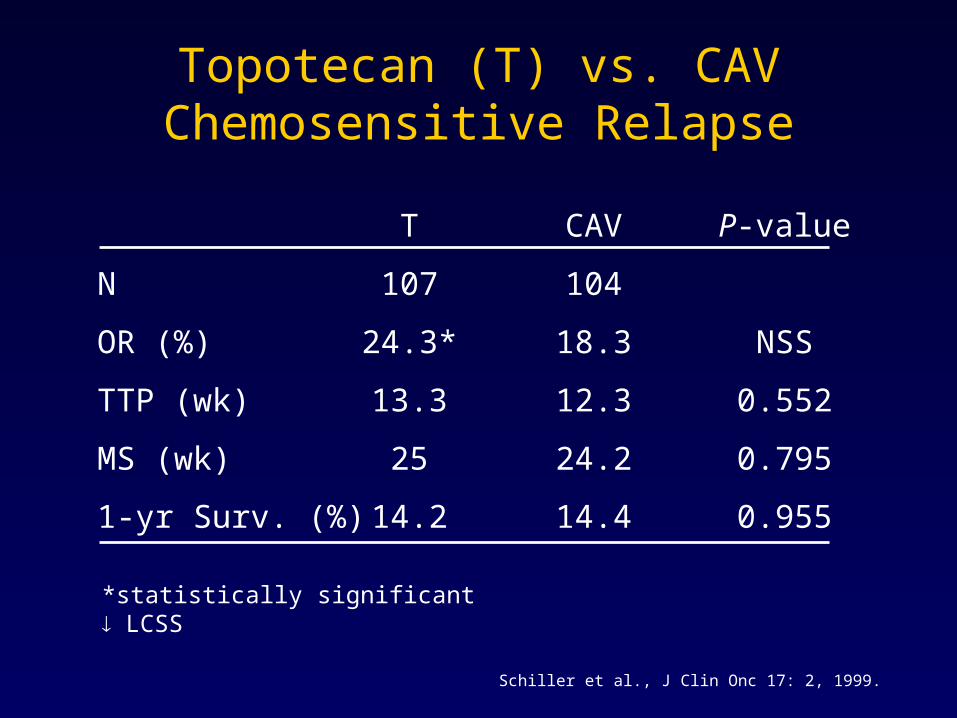
Topotecan (T) vs. CAVChemosensitive Relapse
T CAV P-value
N 107 104
OR (%) 24.3* 18.3 NSS
TTP (wk) 13.3 12.3 0.552
MS (wk) 25 24.2 0.795
1-yr Surv. (%) 14.2 14.4 0.955
*statistically significant LCSS
Schiller et al., J Clin Onc 17: 2, 1999.
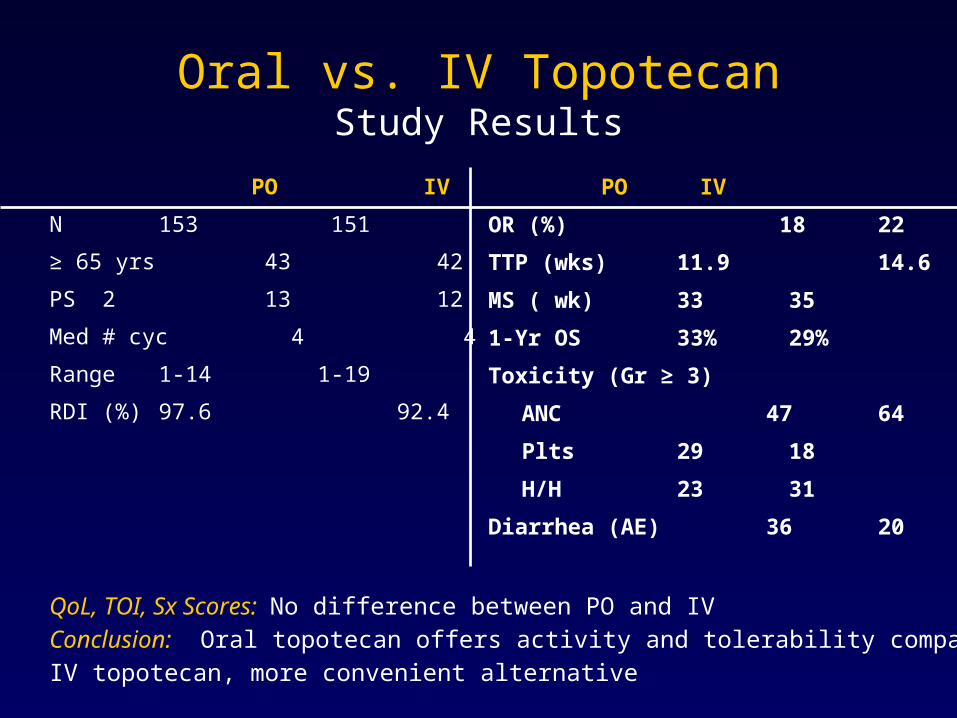
Oral vs. IV TopotecanStudy Results
PO IV
N 153 151
≥ 65 yrs 43 42
PS 2 13 12
Med # cyc 4 4
Range 1-14 1-19
RDI (%) 97.6 92.4
PO IV
OR (%) 18 22
TTP (wks) 11.9 14.6
MS ( wk) 33 35
1-Yr OS 33% 29%
Toxicity (Gr ≥ 3)
ANC 47 64
Plts 29 18
H/H 23 31
Diarrhea (AE) 36 20
QoL, TOI, Sx Scores: No difference between PO and IVConclusion: Oral topotecan offers activity and tolerability comparable to IV topotecan, more convenient alternative
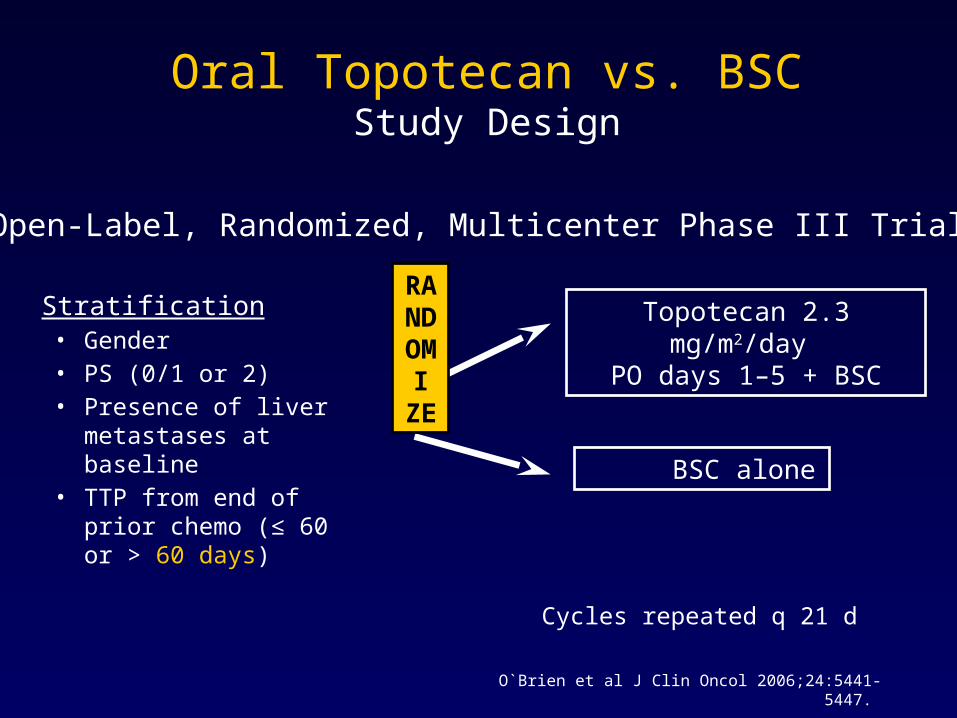
Stratification • Gender • PS (0/1 or 2)• Presence of liver
metastases at baseline • TTP from end of prior
chemo (≤ 60 or > 60 days)
Cycles repeated q 21 d
RANDO
M I ZE
Topotecan 2.3 mg/m2/day PO days 1–5 + BSC
BSC alone
Open-Label, Randomized, Multicenter Phase III Trial
Oral Topotecan vs. BSCStudy Design
O`Brien et al J Clin Oncol 2006;24:5441-5447.
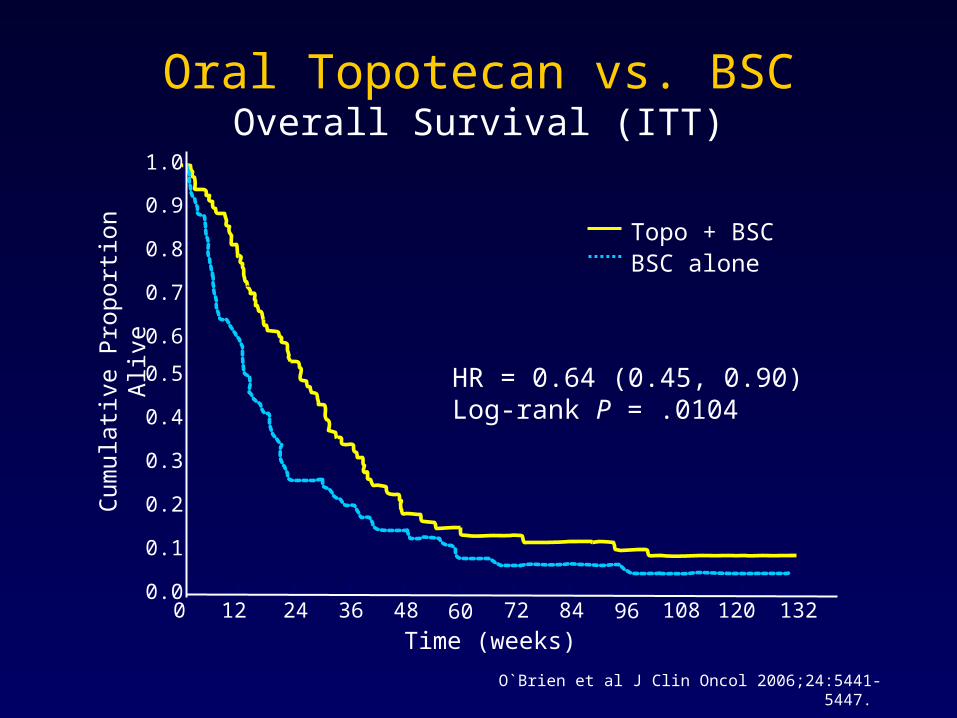
Oral Topotecan vs. BSCOverall Survival (ITT)
0 12 24 36 48 60 72 84 96 108 120 1320.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
HR = 0.64 (0.45, 0.90)Log-rank P = .0104
Time (weeks)
Cum
ulat
ive
Pro
port
ion
Aliv
e Topo + BSCBSC alone
O`Brien et al J Clin Oncol 2006;24:5441-5447.
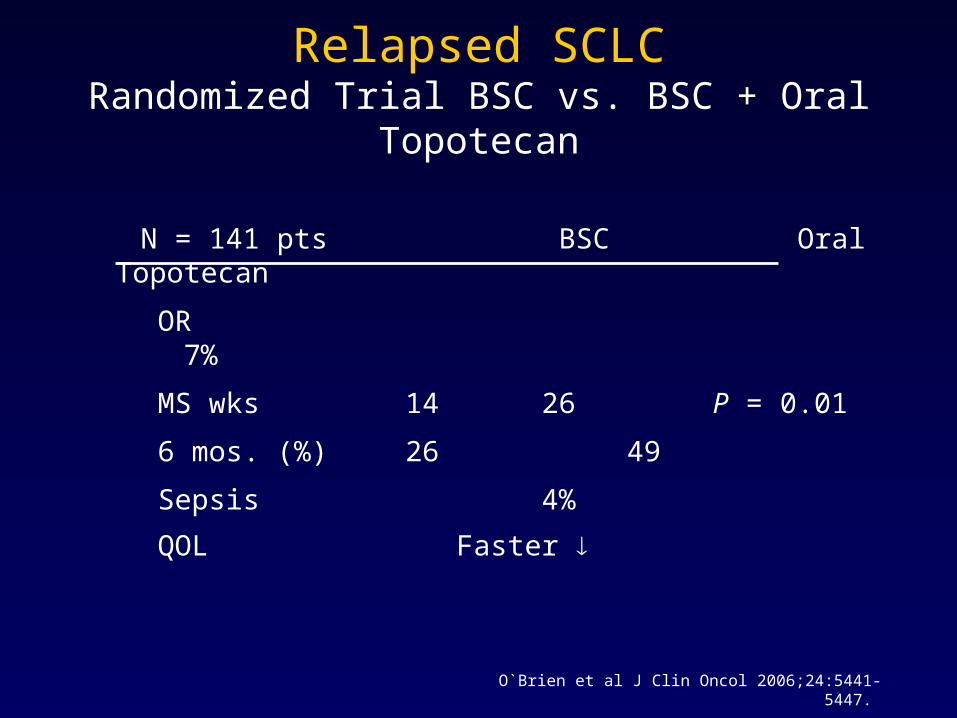
Relapsed SCLCRandomized Trial BSC vs. BSC + Oral Topotecan
N = 141 pts BSC Oral Topotecan
OR 7%
MS wks 14 26 P = 0.01
6 mos. (%) 26 49
Sepsis 4%
QOL Faster
O`Brien et al J Clin Oncol 2006;24:5441-5447.
ASCO 2007 – SCLC
Commentary





![Tabellen und Gleitobjekte - start [Unix-AG-Wiki] · Beispiel Dies ist Fließtext, langer, langer Text der sich immer wieder wiederholt. Dies ist Fließtext, langer, langer Text der](https://img.dokumen.tips/doc/110x75/5d5c45f788c99317558b63e9/tabellen-und-gleitobjekte-start-unix-ag-wiki-beispiel-dies-ist-fliesstext.jpg)