Embed Size (px)
DESCRIPTION
SGD Reference Material
Citation preview

Core Concepts: Meconium Aspiration Syndrome:Pathogenesis and Current ManagementTsu F. Yeh, MD, PhD*
Author Disclosure
Dr Yeh has disclosed
no financial
relationships relevant
to this article. This
commentary does
contain a discussion
of an unapproved/
investigative use of a
commercial product/
device.
AbstractAspiration of meconium produces a syndrome characterized by hypoxia, hypercapnia,and acidosis. Perinatal hypoxia, acute airway obstruction, pulmonary inflammation,pulmonary vasoconstriction, pulmonary hypertension, and surfactant inactivation allplay a role in the pathogenesis of meconium aspiration syndrome (MAS). Mostaspiration of meconium probably occurs before birth. Following aspiration, meco-nium can migrate to the peripheral airway, leading to airway obstruction and subse-quent lung inflammation and pulmonary hypertension. The presence of meconium inthe endotracheal aspirate automatically establishes the diagnosis of meconium aspira-tion. MAS can be diagnosed in any infant born with meconium staining of amnioticfluid who develops respiratory distress at or shortly after birth and has positiveradiographic findings. Prevention of intrauterine hypoxia, early cleaning (suctioning)of the airway, and prevention and treatment of pulmonary hypertension are essentialin the management of MAS. Recent studies suggest that avoidance of posttermdelivery may reduce the risk of intrauterine hypoxia and the incidence of MAS.Routine intrapartum naso- and oropharyngeal suction does not appear to affect theincidence and outcome of MAS. Endotracheal suction now is reserved only for infantswho are depressed or have respiratory distress at birth. Mortality of MAS hasimproved; the causes of death are related primarily to hypoxic respiratory failureassociated with irreversible pulmonary hypertension. Morbidity is affected mostly byperinatal hypoxia.
Objectives After completing this article, readers should be able to:
1. Characterize meconium aspiration syndrome (MAS).2. Explain the pathophysiology that occurs after meconium aspiration.3. Review prevention measures and treatment of MAS.
IntroductionMAS in the newborn is characterized by hypoxia, hypercap-nia, and acidosis. Although the pathophysiology of thissyndrome is not completely understood, recent advances inmanagement and respiratory care have decreased the mortal-ity rate substantially. Perinatal hypoxia, airway obstructionshortly after birth, and significant pulmonary vasoconstric-tion and hypertension are the three major causes of mortalityand morbidity. In this review, we focus on the pathogenesis,clinical manifestations, and current management of MAS.
Incidence of Meconium-stained Amniotic Fluidand MASThe incidence of meconium-stained amniotic fluid and MASvaries between populations and depends on such factors asthe socioeconomic status of the family, advances in prenatalcare, accessibility to medical care, effective regionalization ofperinatal care, and age of the mother at the birth of the first
*Chair and Professor of Pediatrics, China Medical University, Taichung, Taiwan; Senior Neonatologist, John Stroger Hospital ofCook County, Chicago, Ill.
Abbreviations
A-aDO2: alveolar-arterial oxygen gradientECMO: extracorporeal membrane oxygenationFRC: functional residual capacityHFOV: high-frequency oscillatory ventilationHFV: high-frequency ventilationiNO: inhaled nitric oxideMAS: meconium aspiration syndromeNO: nitric oxideOI: oxygenation indexPDE: phosphodiesterasePEEP: positive end-expiratory pressurePPHN: persistent pulmonary hypertension of the newbornSIMV: synchronized intermittent mandatory ventilation
Article pulmonology
NeoReviews Vol.11 No.9 September 2010 e503
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

child. In the United States, meconium-stained amnioticfluid occurs in as many as 10% to 15% of live births. Theincidence of MAS decreased dramatically as the numberof births occurring after 41 weeks’ gestation was re-duced. (1) In a prospective study of infants born after37 weeks’ gestation, MAS decreased from 5.8% to 1.5%during the period 1990 to 1997. (1) This was associatedwith a 33% reduction in births at more than 41 weeks’gestation.
Pathogenesis of MASMeconium Passage
Although the mechanisms of in utero passage of meco-nium are not understood completely, they depend onincreased intestinal peristalsis, relaxation of the analsphincter, and a gestational age greater than 34 to35 weeks. Before 34 weeks’ gestation, meconium usuallyis not in the descending colon and rectum. Increasedperistalsis may be caused by increased concentrations ofmotilin (2) or triggered by infection, (3) hypoxia, orvagal stimulation produced by sporadic or repetitive cordcompression, any of which also may result in sphincterdilation.
However, meconium may be passed spontaneously ina term or postterm fetus that has a mature gastrointesti-nal tract with no evidence of fetal distress or in babieswho experience only transient or sporadic intrauterinestress with adequate cardiovascular compensation.
Characteristics of Human MeconiumHuman meconium is a viscous and odorless substanceconsisting of water, lanugo, desquamated cells, vernix,amniotic fluid, pancreatic enzymes, and bile pigment.Meconium is a good medium for bacterial growth, par-ticularly for gram-negative bacilli. Several constituents ofmeconium, especially free fatty acids and bile salts, mayaffect the surface tension of alveoli by displacement orinhibition of surfactant.
Mechanisms of Meconium AspirationAspiration usually occurs in utero as a consequence ofhypoxia-induced gasping. Most infants who have MAS(�60%) are born by cesarean section, indicating thatthey aspirate meconium before birth. Some aspirationmay occur during the second stage of labor, when theshoulders and chest are delivered. It remains question-able, however, if there is a significant amount of meco-nium present in the oropharynx to cause MAS.
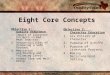
Pathophysiology After Aspiration of MeconiumGooding and associates (4) demonstrated the immediateeffects of meconium aspiration in an animal model(Fig. 1). Aspiration of a large amount of tenacious meco-nium led to acute cor pulmonale-induced heart failureand death. Aspiration of moderate amounts of meco-nium, however, was associated with a much better sur-vival rate. Meconium may migrate gradually (within 1 to2 hours) to the peripheral portions of the lungs. Acutecor pulmonale rarely is observed today in the clinicalsetting because infants usually undergo immediate resus-citation in the delivery room. However, meconium grad-ually migrates, either by spontaneous respiratory move-ments or by positive-pressure ventilation, to the smallairways. Thus, endotracheal suction should be per-formed as early as possible if the infant has respiratorydistress shortly after birth.
Figure 1. Upper A: Normal chest radiograph of newbornpuppy before injection of meconium. Upper B. One minuteafter injection of 2 mL of 50% meconium into the trachea, theright atrium has become markedly dilated. The puppy died ofacute cor pulmonale. Lower A. The injected tantalum-labeledmeconium is distributed throughout the tracheobronchialtree. Lower B. One hour later, the tantalum-labeled meconiumhas been cleared from the trachea and mainstem bronchi, butmaterial has also migrated peripherally. Reprinted with per-mission from Gooding CA, et al. (4)
pulmonology meconium aspiration syndrome
e504 NeoReviews Vol.11 No.9 September 2010
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

After migration to the lower airway, meconium mayblock the airway, either partially or completely, leadingto hyperaeration or atelectasis of the respiratory unit(Fig. 2). Meconium eventually is cleared from the lungsby macrophages (Fig. 3). During this stage, inflamma-tion plays an important role in the pathophysiologicchanges. MAS induces hypoxemia via five major effects:airway obstruction, pulmonary vasoconstriction and hy-pertension, surfactant dysfunction, infection, and possi-ble chemical pneumonitis.
Airway ObstructionThe most prominent effect of meconium aspiration, par-ticularly during the early course of the disease, is airwayobstruction. Depending on the physical characteristics ofmeconium and the amount aspirated, meconium maypartially or completely block the airway, leading to eitherhyperdistention or atelectasis of the alveoli. The gas thatis trapped may rupture into the pleura, resulting in airleaks, namely, pulmonary interstitial emphysema, pneu-momediastinum, and pneumothorax.
Pulmonary Vasoconstriction andPersistent Pulmonary Hypertension
Persistent pulmonary hypertension of the newborn(PPHN) frequently accompanies MAS, with right-to-leftshunting caused by increased pulmonary vascular resis-tance. Two-dimensional echocardiography should beused to evaluate pulmonary hypertension during thecourse of the illness. Significant pulmonary hypertension
with right-to-left shunting occurs in about 20% to 40% ofinfants who have MAS. PPHN in infants who have MAScould be due to: 1) hypertrophy or neomuscularizationof post-acinar capillaries as a result of chronic intrauterinehypoxia; (5) 2) pulmonary vasoconstriction as a result ofhypoxia, hypercarbia, or acidosis; or 3) pulmonary vaso-constriction as a result of lung inflammation.
Chronic intrauterine hypoxia can induce muscle hyper-trophy, causing thickening of the pulmonary vessels.PPHN usually presents in the subacute phase and aspersistent hypoxemia at 6 to 24 hours after birth. In ourstudy of MAS in newborn piglets, (6) we found that
pulmonary arterial pressure was bi-phasic, with the early phase startingfrom 2 to 6 hours, possibly due toairway obstruction, and the laterphase starting from 24 hours, pos-sibly because of lung inflammation.A good positive correlation wasseen between thromboxane B2 andleukotriene D4 in tracheal lavagefluids and mean pulmonary arterialpressure. The use of dexametha-sone reduced the concentrationsof thromboxane B2 and 6-keto-prostaglandin-1-alpha and signifi-cantly improved cardiac strokevolume. (6)
Spontaneous recovery usuallyoccurs within 3 to 4 days if theinfant survives, suggesting that vas-cular constriction plays a role in thepathogenesis.Figure 2. Pathogenesis of MAS. V/P�ventilation/perfusion.
Figure 3. Meconium is usually picked up by macrophages 2 to3 days after aspiration.
pulmonology meconium aspiration syndrome
NeoReviews Vol.11 No.9 September 2010 e505
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

Surfactant DysfunctionAnimal models of meconium aspiration have shown thatmeconium may inactivate surfactant function. Lung la-vage fluid from infants who have MAS demonstratehigher-than-normal concentrations of surfactant inhibi-tors such as total protein, albumin, and membrane-derived phospholipids. Several constituents of meco-nium, especially the free fatty acids (eg, palmitic, stearic,and oleic acid), have a higher minimal surface tensionthan surfactant and may displace it from the alveolarsurface, resulting in diffuse atelectasis, with decreasedlung volume, compliance, and oxygenation. Bile salts inmeconium may inhibit surfactant synthesis. The effect ofMAS on surfactant dysfunction usually occurs in thesubacute and late phase of the disease.
InfectionMeconium is a good medium for enhancing bacterialgrowth in vitro. Microscopic features characteristic ofpneumonia frequently are seen at autopsy in affectedinfants treated with mechanical ventilation. However, aclinical study carried out by our group revealed thatantibiotics are indicated only if there is a history ofperinatal infection or if the infants have undergone vig-orous resuscitation or are receiving mechanical ventila-tion. (7)
Chemical PneumonitisThe pH of meconium is approximately 7.10 to 7.20.Aspiration of meconium may cause airway irritation. Theenzymes and bile salts of meconium may cause a releaseof cytokines (eg, tumor necrosis factor-1-alpha andinterleukins-1B, -6, -8, -13), which can result in diffusetoxic pneumonitis. Chemical pneumonitis has been dem-onstrated in an animal model, but the role that chemicalpneumonitis plays in human MAS has not been clearlydefined.
Pulmonary FunctionThe most prominent feature of MAS during the first48 hours is high airway resistance. (8) Low compliancecan be caused by atelectasis. The time constant is usuallyhigh during the first 3 days.
Lung volume, as measured by the closed-circuit he-lium dilution technique, can be low, normal, or high.The relationship between lung volume and complianceduring the first 3 days is shown in Figure 4. Infants whohave MAS may have low functional residual capacity(FRC) and low compliance, suggesting partial or com-plete atelectasis, or they may have high FRC and lowcompliance, suggesting overdistension of the lung. The
discrepancy between lung aeration and poor compliancealso can be seen in the lung at different locations. Mal-distribution of ventilation and aeration is common inMAS. Arterial blood gases show a low PO2 and a highalveolar-arterial oxygen gradient (A-aDO2) due to in-trapulmonary shunting, uneven ventilation-perfusion ra-tio, or extrapulmonary shunting. Arterial PCO2 usually isin the normal range or lower. Increased PCO2 generallyindicates an air leak or the presence of PPHN.
Because of the increase in airway resistance and con-sequently the time constant, adequate expiratory timeshould be permitted for exhalation to avoid adversepositive end-expiratory pressure (PEEP) during me-chanical ventilation. Because of the abnormal air distri-bution and subsequent abnormal compliance in thelung, high-frequency oscillatory ventilation (HFOV)may be a better method of achieving good ventilationand oxygenation.
DiagnosisClinical Features
The diagnosis of MAS typically is based on the followingcriteria: 1) meconium-stained amniotic fluid or infant orboth, 2) respiratory distress at birth or shortly after birth,and 3) positive radiographic features. If the infant re-
Figure 4. The relationship between lung compliance (CL) andfunctional lung capacity (FRC) in healthy infants and infantswho have MAS during the first 3 postnatal days. The solid lineand dotted lines indicate mean and 95% confidence lines forhealthy infants. The solid circles represent infants who haveMAS. Infants who have MAS can either have high FRC and lowCL, indicating hyperaeration, or low FRC and low compliance,indicating atelectatic lung.
pulmonology meconium aspiration syndrome
e506 NeoReviews Vol.11 No.9 September 2010
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

quires intubation, the presence of meconium in endotra-cheal suctioning automatically establishes the diagnosis.
Infants who have MAS may present with yellowish-green-stained fingernails, umbilical cord, and skin. Post-mature infants may have evidence of peeling skin, longfingernails, and decreased vernix. Other findings of MASmay include tachypnea, retraction, grunting, and barrel-shaped chest. Auscultation reveals rales and rhonchi.Tricuspid regurgitation murmur with changing intensityover time may be audible in infants who have PPHN.Other clinical features associated with perinatal asphyxiaalso may be seen in infants who have MAS (Table).
Radiographic FeaturesEssentially, three major features can be seen in MAS:1) diffuse or local linear or patchy infiltrates, 2) consoli-dation or atelectasis, and 3) hyperaeration with or with-out air leaks (Fig. 5). The classic radiologic findings inMAS are diffuse, coarse, patchy infiltrates that may alter-nate with areas of hyperexpansion. The lungs of infantswho have severe MAS may show consolidation or atelec-tasis associated with hyperaeration, which most likely isdue to aspiration of large, tenacious meconium particles.These features are predictive of poor outcome comparedwith features of generalized infiltration. (9) Radio-graphic changes may resolve within 7 to 10 days, al-though they can persist for weeks. Cardiomegaly may beseen in infants who have MAS, particularly when accom-panied by pulmonary hypertension.
ManagementPrepartum Prevention
The decreased incidence of MAS over the last decade hasbeen attributed to the reduction in postterm delivery,aggressive management of abnormal fetal heart ratemonitoring, and decreased number of infants who havelow Apgar scores. Continuous electronic fetal monitor-ing is indicated for pregnancies that are complicated bymeconium-stained amniotic fluid. Timely interventionshould be initiated in the presence of a nonreassuringfetal heart rate tracing such as a category III tracing. Fetalpulse oximetry is a new modality for antepartum fetalsurveillance, (1)(10)(11) but its effect on outcome re-mains questionable. Postterm delivery often is associatedwith intrauterine hypoxia and meconium-stained amni-otic fluid, and, as noted previously, the reduction inpostterm delivery has led to a reduction in the incidenceof MAS. (10)
Amnioinfusion may be an effective therapy for preg-nancies complicated by oligohydramnios and fetal dis-tress. Amnioinfusion dilutes the thickness of meconiumand may prevent umbilical cord compression and meco-nium aspiration. (12) However, studies have indicatedthat although this strategy decreases the amount of
Table. Commonly AssociatedFindings With MASCardiovascular Consequences of Asphyxia
● Hypoxemia-related pulmonary hypertension● Hypoxemia-related myocardial dysfunction
Pulmonary Consequences of Asphyxia
● Decreased surfactant● Pulmonary edema● Meconium aspiration syndrome
Renal Consequences of Asphyxia
● Tubular and medullary necrosis● Bladder paralysis
Central Nervous System Consequences of Asphyxia
● Hypoxic-ischemic encephalopathy● Intracranial hemorrhage
Figure 5. Chest radiographs of MAS. A. Mild linear infiltrates,usually indicating a small amount of thin meconium aspira-tion. B. Bilateral linear and patchy infiltrates, indicating amoderate amount of thin meconium aspiration. C. Bilateralgeneralized diffuse patchy infiltration, usually indicating alarge amount of thin meconium aspiration. D. Partial leftupper lobe atelectasis with hyperaeration of right lung, usuallyindicating large particles and thick meconium aspiration. Theinfant often develops respiratory failure and requires exten-sive respiratory therapy. Reprinted with permission from YehTF, et al. (9)
pulmonology meconium aspiration syndrome
NeoReviews Vol.11 No.9 September 2010 e507
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

meconium below the cords, in infants born to motherswho have meconium staining of amniotic fluid, it failsto reduce the risk of MAS. (13)(14) A recent multi-center study by Fraser and associates (15) concluded thatamnioinfusion did not reduce the risk of moderate-to-severe MAS and MAS-related perinatal death in infantsborn through thick meconium. There is also insufficientevidence that amnioinfusion reduces meconium-relatedneonatal morbidity. Accordingly, amnioinfusion is notrecommended for women who have meconium stainingof amniotic fluid alone unless there is evidence of severeoligohydramnios and fetal distress. Because infection andchorioamnionitis may be associated with severe MAS,early administration of broad-spectrum antibiotic ther-apy in cases of maternal chorioamnionitis may reduceneonatal morbidity.
Intrapartum PreventionOropharyngeal and nasopharyngeal suction soon afterdelivery of the head but before the delivery of shouldersand chest has been a common practice in the past 2 de-cades that was shown to decrease the incidence andseverity of MAS. (16)(17) However, a recent multicenterstudy showed that this strategy does not prevent MAS.(18) Researchers also showed that it does not reduce themortality rate, the duration of ventilation and oxygentreatment, or the need for mechanical ventilation. Ac-cordingly, such routine suctioning no longer is recom-mended, although it is recommended in specific cases,such as the presence of thick or copious meconium-stained fluid.
Postpartum PreventionEndotracheal intubation and suction is performed toremove the meconium in the upper airway before itmigrates to the lower airway. Meconium can migrate tothe peripheral airway through spontaneous respiratorymovement or positive-pressure ventilation. Therefore, itseems logical that endotracheal intubation and suctionshould be performed as early as possible after delivery, ie,before the baby takes the first breath or before activebreathing. Until recently, routine intubation and tra-cheal suction was recommended for most infants whohad meconium staining of amniotic fluid. (19) However,recent studies do not support universal aggressive suc-tion unless the infant’s respiration is depressed. Since2005, the American Heart Association and the NeonatalResuscitation Program have recommended tracheal suc-tioning only if the infant is not vigorous, has decreasedmuscle tone, or has a heart rate less than 100 beats/min.
Management of PPHNOnce the infant develops MAS, management is pri-marily supportive. Maintenance of adequate oxygen-ation; good systemic blood pressure; and correction ofacidosis, hypoglycemia, or other metabolic disorders arethe mainstays of treatment. The infant should be caredfor in a neutral thermal environment and watchedclosely. Gentle care is essential; excessive handling andagitation should be avoided. An umbilical arterial cathe-ter or radial arterial catheter should be inserted in infantswho have moderate-to-severe MAS to monitor bloodgases and blood pressure without disturbing the infant.We rarely use vasodilators for PPHN.
Infants who have MAS with low blood pressure maypresent with clinical features of PPHN. It is, therefore,important to maintain adequate systemic blood pressurein infants who have moderate-to-severe MAS. In addi-tion to maintaining intravenous fluids, volume expanderssuch as normal saline and albumin are needed if patientshave low blood pressure. Blood transfusion is indicatedto keep hematocrit greater than 40% (0.40). Continuousintravenous infusions of dopamine (2 to 20 mcg/kg perminute), dobutamine (2 to 25 mcg/kg per minute), orepinephrine (0.01 to 0.03 mg/kg per minute) often areused separately or in combination. For infants who haveintrauterine hypoxia and sustained hypotension, physio-logic replacement with hydrocortisone may help over-come possible adrenal insufficiency and may stabilize theblood pressure. (20)(21)
Because hypoxia, acidosis, and hypercapnia mayincrease pulmonary vascular resistance, oxygen andventilator therapy should be administered to maintainappropriate blood gas values and acid-base balance. Be-cause infants who have PPHN are very labile during theacute phase of the disease, we prefer to maintain thearterial PO2 near or above 100 mm Hg. Arterial bloodgases should be monitored frequently and oxygen andventilator support weaned gradually until the acute stageis over and the infant’s condition stabilizes. We attemptto maintain the PCO2 at 40 to 45 mm Hg and the pHaround 7.35 to 7.45.
Early use of high-frequency ventilation (HFV), in-haled nitric oxide (iNO), or both may be needed tomaintain appropriate blood gas values and acid-base bal-ance. This approach may prevent the subsequent devel-opment of PPHN.
Patients who have PPHN are very sensitive to stimu-lation or excessive handling. Term infants may becomeagitated during intubation, and synchronization of theinfant’s breathing with mechanical ventilation may notbe possible. Analgesia and anesthesia often are needed.
pulmonology meconium aspiration syndrome
e508 NeoReviews Vol.11 No.9 September 2010
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

We prefer to begin with fentanyl at a dose of 1 to5 mcg/kg per hour or midazolam at a dose of 10 to60 mcg/kg per hour. An increased dose may be neededafter several days of treatment because of the develop-ment of tolerance. Occasionally, a continuous intrave-nous infusion of morphine 100 to 150 mcg/kg over1 hour followed by 10 to 20 mcg/kg per hour may begiven. Muscle relaxants such as pancuronium 0.1 mg/kgper dose can be provided for unsynchronized ventilationbut rarely are needed.
Ventilator ManagementApproximately 30% of infants who have MAS requireventilator support. Such infants tend to breathe on theirown, so some degree of sedation may be necessary.Airway obstruction and a prolonged time constant arethe major features during the early course of the disease,which necessitates an adequate expiration time duringthe expiratory phase. (8) For this reason, caution shouldbe taken to avoid increasing the inspiration time orreversing the inspiratory-to-expiratory ratio during me-chanical ventilation. For similar reasons, during HFV,the rate should be kept below 15 Hz, if possible. Thisstrategy may prevent adverse PEEP and air leaks. HFV isprobably most appropriate to achieve good pulmonaryventilation and gas exchange in MAS. Clinical trials haveshown that HFV reduces the need for extracorporealmembrane oxygenation (ECMO) treatment and de-creases the incidence of air leaks in infants who havePPHN. We initially use synchronized intermittent man-datory ventilation (SIMV). If infants require high posi-tive inspiratory pressure or high FiO2 or are at a risk ofdeveloping air leak, we switch to HFOV. We allowcrossover treatment because some babies respond differ-ently. Clark and associates (22) showed that amongpatients who had severe respiratory disease, 63% whofailed SIMV responded to HFOV.
Surfactant TherapySurfactant can be administered as bolus or as lavage. In arandomized, controlled study, Findlay and colleagues(23) concluded that surfactant replacement with threedoses of 150 mg/kg (6 mL/kg) within 6 hours afterbirth improved oxygenation and reduced the incidenceof air leaks, the severity of pulmonary morbidity, theneed for ECMO treatment, and duration of hospitaliza-tion. Other studies have shown similar findings. Acuteadverse effects of surfactant therapy include transientoxygen desaturation and endotracheal tube obstructionoccurring during bolus administration. The dose of sur-factant administered by bolus or slow infusion is not
defined. We administer 100 mg/kg to infants who havesevere MAS via an intratracheal indwelling catheterthrough the side hole of an endotracheal tube.
There is no evidence that surfactant therapy influencesthe mortality rate of infants who have MAS. The use ofsurfactant to lavage the airway may be more effectivethan single surfactant instillation, although no controlledstudy has been performed in neonates. It is reasonable toassume that surfactant therapy would be more effectiveafter airway obstruction has been relieved.
Nitric Oxide TherapyNitric oxide (NO) is a potent vasodilator. iNO can bedelivered to the alveoli through a ventilator, resulting inselective pulmonary vasodilatation. Once in the blood-stream, NO is metabolized by hemoglobin and, thus, haslimited systemic effects. In general, iNO (20 ppm) isinitiated when the oxygenation index (OI) exceeds 25.Although brief exposure to higher doses (40 to 80 ppm)appears to be safe, sustained treatment with 80 ppm iNOincreases the risk of methemoglobinemia. The lowesteffective initial dose of iNO in term newborns who havePPHN has not been determined, but sustained improve-ment in oxygenation has been demonstrated with doseslower than 10 ppm. (24)(25)
Methemoglobin and nitrogen dioxide concentra-tions should be monitored for 4 to 12 hours. Serialechocardiography is useful in monitoring the pressuregradients and myocardial function. Patients usually aremaintained on low-dose iNO (5 to 20 ppm) for 2 to6 days, then gradually weaned to avoid rebound hypox-emia. The combination of HFOV and iNO therapy canbe more successful than treatment with HFOV or iNOalone in patients who have PPHN and respiratory distresssyndrome or MAS as the underlying disease. (26)(27)
SteroidsSteroids are used in the treatment of MAS for severalreasons: 1) they can stabilize the blood pressure, partic-ularly in infants who suffer from intrauterine hypoxia andadrenal insufficiency; 2) they can inhibit chemical pneu-monitis; 3) they can inhibit inflammation and decreasecytokine-induced vasoconstriction, and, therefore, maybe beneficial for infants who have PPHN; and 4) dexa-methasone can increase cardiac stroke volume and im-prove overall cardiopulmonary function. A double-blindtrial of hydrocortisone use, however, did not show abeneficial effect. (28) Hydrocortisone may be useful forinfants who have unstable blood pressure. The anti-inflammatory effect of dexamethasone in the treatmentor prevention of PPHN has not been studied.
pulmonology meconium aspiration syndrome
NeoReviews Vol.11 No.9 September 2010 e509
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

Phosphodiesterase (PDE) Inhibitors:Sildenafil and Milrinone
Sildenafil inhibits cGMP-specific PDE type 5, increasescGMP concentrations, and may result in pulmonary vaso-dilation or the enhancement of NO activity. Because PDE5is primarily distributed within the arterial wall smooth mus-cle of the lungs and penis, sildenafil acts selectively in boththese areas without inducing vasodilation in other areas ofthe body. Sildenafil is only available in enteral form. Thedrug was approved by the United States Food and DrugAdministration for the treatment of pulmonary hyperten-sion in adults, but data are limited in neonates. Baquero andassociates (29) reported that oral sildenafil improves the OIin infants who have severe PPHN. The recommended doseis 0.3 to 1 mg/kg via orogastric tube every 6 to 12 hours.Potential adverse effects include worsening of oxygenation,systemic hypotension, and bleeding tendency. Milrinone isa specific PDE3 inhibitor that increases cAMP concentra-tions and decreases pulmonary vascular resistance.
Extracorporeal Membrane OxygenationThe use of adjunctive therapies has dramatically decreasedthe need for ECMO therapy, (30) but some infants whohave MAS and PPHN still develop persistent respiratoryfailure despite optimal medical treatments. (22) ECMOprovides cardiopulmonary support while allowing the un-derlying pulmonary or cardiac dysfunction to resolve with-out the risk of further injury from barotrauma or hyperoxia.ECMO treatment increases the survival rate of infants whohave MAS and PPHN from 80% to 94%.
The selection criteria for ECMO include: 1) more than34 weeks’ gestation, 2) birthweight more than 2,000 g,3) lack of major coagulopathy or active bleeding, 4) nomajor intracranial bleeding, 5) mechanical ventilation ofless than 10 to 14 days’ duration and reversible lung disease,6) failure of optimal medical management, and 7) infantswho have a high predicted mortality rate.
OI and A-aDO2 are used commonly to predict thelikelihood of mortality. A mortality rate of 80% is associ-ated with an OI of 40 or greater, an A-aDO2 greater than600 mm Hg, or both.
Potential Therapy for PPHNA number of vasodilators are under investigation, in-cluding calcium channel blockers (nifedipine, diltiazem,verapamil), prostacyclin analogs (epoprostenol, trepros-tinil, iloprost), and endothelin receptor antagonists(bosentan, sitaxsentan, ambrisentan).
Outcome of MASThe mortality rate associated with MAS-related illnesshas declined markedly over the past few decades: 4.2%
during 1973 to 1987 in the United States to 2.5% during1995 to 2002 in Australia and New Zealand. (1)(10)Perinatal deaths are related to perinatal depression (as-phyxia), airway obstruction, and development of PPHN.
Pulmonary sequelae are common among infants whohave severe MAS. Nearly 50% of all affected infantsdevelop reactive airway diseases during the first 6 monthsafter birth. Mild airway obstruction or exercise-inducedasthma often present in the children at 6 to 8 years of age(31)(32)
The long-term neurologic outcomes of infants who haveMAS depend on the underlying disorders. The neurologicoutcomes are related to the presence or absence of intra-uterine asphyxia, hypoxic-ischemic encephalopathy, andPPHN. Infants who require ECMO treatment tend to havemore complications than infants who do not.
References1. Yoder BA, Kirsch EA, Barth WH, Gordon MC. Changingobstetric practice associated with decreasing incidence of meco-nium aspiration syndrome. Obstet Gynecol. 2002;99:731–7392. Mahmoud EL, Benirschke K, Vaucher YE, Poitras P. Motilinlevels in term neonates who have passed meconium prior to birth.J Pediatr Gastroenterol Nutr. 1988;7:953. Piper HM, Newton ER, Berkus MD, Peairs WA. Meconium: amarker for peripartum infection. Obstet Gynecol. 1998;91:741–7744. Gooding CA, Gregory GA, Taber P, Wright RR. An experimen-tal model for the study of meconium aspiration of newborn. PediatrRadiology. 1971;100:137–1415. Roine J, Hislep AA, Redington AN, Haworth SG, ShinebourneEA. Fetal persistent pulmonary hypertension presenting late in theneonatal period. Arch Dis Child. 1991;66:398–4026. Wu JM, Yeh TF, Wang JY, et al. The role of pulmonary inflam-mation in the development of pulmonary hypertension in newbornwith meconium aspiration syndrome. Pediatr Pulmonol Suppl.1999;18:205–208
American Board of Pediatrics Neonatal-PerinatalMedicine Content Specifications• Know the significance and obstetrical
management of meconium-stainedamniotic fluid.
• Know the current recommendationsregarding suctioning meconium from theairway during and following delivery.
• Know the pathogenesis, pathophysiology, pathologic features,and risk factors of meconium aspiration syndrome.
• Know how to manage meconium aspiration syndrome.• Know the clinical, laboratory, and imaging features of
meconium aspiration syndrome.• Know the management of persistent pulmonary hypertension,
including assisted ventilation, pharmacologic approaches, andECMO.
pulmonology meconium aspiration syndrome
e510 NeoReviews Vol.11 No.9 September 2010
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

7. Lin HC, Su BH, Tsai CH, Lin TW, Yeh TF. Role of antibioticsin the management of non-ventilated cases of meconium aspirationsyndrome without risk factors for infection. Biol Neonate. 2005;87:51–558. Yeh TF, Barathi A, Lilien LD, Pildes RS. Lung volume, dynamiclung compliance, and blood gases during the first 3 days of post-natal life in infants with meconium aspiration syndrome. Crit CareMed. 1982;10:588–5929. Yeh TF, Harris V, Srinivasan G, Lilien L, Pyati S. Roentgeno-graphic findings in infants with meconium aspiration syndrome.JAMA. 1979;242:60–6310. Dargaville PA, Copnell B; for the Australian and New ZealandNeonatal Network. The epidemiology of meconium aspirationsyndrome: incidence, risk factors, therapies, and outcome. Pediat-rics. 2006;17:1712–172111. Shaw K, Clark S. Reliability of intrapartum fetal heart ratemonitoring in the postterm fetus with meconium passage. ObstetGynecol. 1988;72:886–88912. Wenstrom K, Parson MT. The prevention of meconium aspira-tion in labor using amnioinfusion. Obstet Gynecol. 1989;73:647–65113. Eriksen NL, Hostetter M, Parisi VM. Prophylactic amnioinfu-sion in pregnancies complicated by thick meconium. Am J ObstetGynecol. 1994;171:1026–103014. Spong CY, Ogundipe OA, Ross MG. Prophylactic amnio-infusion for meconium-stained amniotic fluid. Am J Obstet Gynecol.1994;171:931–93515. Fraser WD, Hofmeyr J, Lede R, et al. Amnioinfusion for theprevention of the meconium aspiration syndrome. N Engl J Med.2005;353:909–91716. Gregory GA, Gooding CA, Phibbs RH. Meconium aspirationin infants: a prospective study. J Pediatr. 1974;85:848–85317. Carson BS, Losey RW, Bowes WA. Combined obstetric andpediatric approach to prevent meconium aspiration syndrome.Am J Obstet Gynecol. 1976;126:712–71718. Vain NE, Szyld EG, Prudent LM, Wiswell TE, Aguilar AM,Vivas NI. Oropharyngeal and nasopharyngeal suctioning ofmeconium-stained neonates before delivery of their shoulders: mul-ticentre, randomised controlled trial. Lancet. 2004;364:597–60219. Kattwinkel J, ed. Neonatal Resuscitation Program. Elk GroveVillage, Ill: American Academy of Pediatrics; 200020. Fernandez EF, Watterberg KL. Relative adrenal insufficiencyin preterm and term infants. J Perinatol. 2009;29:S44–S49
21. Seri I, Tan R, Evans J. Cardiovascular effects of hydrocortisonein preterm infants with pressure resistant hypotension. Pediatrics.2001;107:1070–107422. Clark RH, Yoder BA, Sell MS. Prospective, randomized com-parison of high-frequency oscillation and conventional ventilationin candidates for extracorporeal membrane oxygenation. J Pediatr.1994;124:447–45423. Findlay RD, Taeusch HW, Walther FJ. Surfactant replacementtherapy for meconium aspiration syndrome. Pediatrics. 1996;97:48–5224. Roberts JD, Polaner DM, Pang P, Zapol WM. Inhaled nitricoxide in persistent pulmonary hypertension of the newborn. Lancet.1992;340:818–81925. Clark RH, Kueser TJ, Walker MW, et al. Low-dose nitric oxidetherapy for persistent pulmonary hypertension of the newborn.N Engl J Med. 2000;342:469–47426. Konduuri G, Solimano A, Sokol GM, et al for the NINO StudyGroup. A randomized trial of early versus standard inhaled nitricoxide therapy in term and near-term newborn infants with hypoxicrespiratory failure. Pediatrics. 2004;113:559–56427. Kinsella JP, Truog WE, Walsh WF, et al. Randomized, multi-center trial of inhaled nitric oxide and high-frequency oscillatoryventilation in severe, persistent pulmonary hypertension of thenewborn. J Pediatr. 1997;131:55–6228. Yeh TF, Srinivasan G, Harris V, Pildes RS. Hydrocortisonetherapy in meconium aspiration syndrome: a controlled study.J Pediatr. 1977;90:140–14329. Baquero H, Soli A, Neira F, Venegas ME, Sola A. Oral sil-denafil in infants with persistent pulmonary hypertension of thenewborn: a pilot randomized blinded study. Pediatrics. 2006;117:1077–108330. Hintz SR, Suttner DM, Sheehan AM, Rhine WD, VanMeurs KP. Decreased use of neonatal extracorporeal membraneoxygenation (ECMO): how new treatment modalities have affectedECMO utilization. Pediatrics. 2000;106:1339–134331. Macfarlane PI, Heaf DP. Pulmonary function in children afterneonatal meconium aspiration syndrome. Arch Dis Child. 1988;63:36832. Swaminathan S, Quinn J, Stabile MW, et al. Long-term pul-monary sequelae of meconium aspiration syndrome. J Pediatr.1989;114:356
pulmonology meconium aspiration syndrome
NeoReviews Vol.11 No.9 September 2010 e511
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

NeoReviews Quiz
10. The incidence of meconium aspiration syndrome (MAS) decreased from 5.8% to 1.5% of births from 1990through 1997, as reported by Yoder and associates. Of the following, this decline in the incidence of MASis most attributed to the:
A. Enhancement of prenatal counseling.B. Implementation of regionalized perinatal care.C. Improvement in socioeconomic status of the families.D. Increase in access to cesarean section deliveries.E. Reduction in births past 41 weeks’ gestation.
11. Meconium aspiration syndrome induces hypoxemia by several pathophysiologic effects of the aspiratedmeconium. Of the following, the most prominent effect of aspirated meconium, especially during the earlycourse of the disease, is:
A. Airway obstruction.B. Chemical pneumonitis.C. Nosocomial infection.D. Pulmonary vasoconstriction.E. Surfactant dysfunction.
pulmonology meconium aspiration syndrome
e512 NeoReviews Vol.11 No.9 September 2010
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

DOI: 10.1542/neo.11-9-e5032010;11;e503NeoReviews
Tsu F. YehManagement
Core Concepts: Meconium Aspiration Syndrome: Pathogenesis and Current
ServicesUpdated Information &
http://neoreviews.aappublications.org/content/11/9/e503including high resolution figures, can be found at:
Referenceshttp://neoreviews.aappublications.org/content/11/9/e503#BIBLThis article cites 31 articles, 7 of which you can access for free at:
Subspecialty Collections
_subhttp://neoreviews.aappublications.org/cgi/collection/respiratory_tractRespiratory Tractbhttp://neoreviews.aappublications.org/cgi/collection/pulmonology_suPulmonologynfant_subhttp://neoreviews.aappublications.org/cgi/collection/fetus:newborn_iFetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://neoreviews.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://neoreviews.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from

DOI: 10.1542/neo.11-9-e5032010;11;e503NeoReviews
Tsu F. YehManagement
Core Concepts: Meconium Aspiration Syndrome: Pathogenesis and Current
http://neoreviews.aappublications.org/content/11/9/e503located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1526-9906. 60007. Copyright © 2010 by the American Academy of Pediatrics. All rights reserved. Online the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,it has been published continuously since . Neoreviews is owned, published, and trademarked by Neoreviews is the official journal of the American Academy of Pediatrics. A monthly publication,
at Philippines:AAP Sponsored on August 17, 2015http://neoreviews.aappublications.org/Downloaded from