Embed Size (px)
Citation preview

DISEASE OF THE MONTH
Congenital Nephrogenic Diabetes Insipidus
DANIEL G. BICHET,* ALEXANDER OKSCHE,t and WALTER ROSENTHALt
*Department of Medicine, Universit#{233} de Montr#{233}al and Research Centre, H#{244}pitaldu Sacr#{233}-Coeur de Montr#{233}al,
Montr#{233}al, Quebec, Canada; and tForschungsinstitut fir Molekulare Pharmakologie, Berlin, Germany.
Congenital nephrogenic diabetes insipidus (NDI) is a rare
disorder of the kidney characterized by the failure to concen-
trate urine despite normal or elevated plasma concentrations of the
antidiuretic hormone arginine vasopressin (AVP). The identifica-
tion, characterization, and mutational analysis of two different
genes, i.e., the AVP receptor 2 gene (AVPR2) and the vasopressin-
sensitive water channel gene (aquaporin-2 [AQP2]), provide the
basis for our understanding of two different hereditary forms of
ND!: X-linked ND! and autosomal recessive NDI. A majority
(>90%) of congenital ND! patients have AVPR2 mutations: Of
1 15 families with congenital ND! that were referred to our labo-
ratories in Montreal and Berlin, 105 families had A VPR2 muta-
tions and 10 had AQP2 mutations. When studied in vitro, most
AVPR2 mutations lead to receptors that are trapped intracellularly
and are unable to reach the plasma membrane. A minority of the
mutant receptors reach the cell surface but are unable to bind AVP
or to properly trigger an intracellular cAMP signal. Similarly,
AQP2 mutant proteins are misrouted and cannot be expressed at
the luminal membrane. The advances described in this review
provide diagnostic tools for physicians caring for these patients
and open the door for the development of therapeutic strategiesbased on gene transfer.
Cellular Actions of Vasopressin and MolecularBiology of ND!
The conservation of water by the human kidney is a function
of the complex architecture of renal tubules within the renal
medulla ( I ). The principal cells of the renal collecting tubules
are responsive to the neurohypophyseal antidiuretic hormone
AVP. The major action of AVP is to facilitate urinary concentra-
tion by allowing water to be transported passively down an
osmotic gradient between the tubular fluid and the surrounding
interstitium. The process of this counter multiplication system and
the action of AVP on principal collecting duct cells are repre-
sented in Figure 1.
The first step in the antidiuretic action of AVP is its binding
to the vasopressin V2 receptor (AVPR2 in Figure 1 ; a three-
dimensional model of the vasopressin V2 receptor where AVP
is docked is shown in Figure 2A) located on the basolateral
membrane of collecting duct cells. This step initiates a cascade
Correspondence to Dr. Daniel G. Bichet. Research Centre, H#{244}pitaldu Sacr#{233}-Coeur de Montr#{233}al,5400, Boulevard Gouin West. Montreal, Quebec, CanadaH4J 1C5.
1046-6673/0801 2-195 1$030010
Journal of the American Society of Nephrology
Copyright © 1997 by the American Society of Nephrology
of events-receptor-linked activation of G-protein (G.j, acti-
vation of adenylyl cyclase, production of cAMP, and stimula-
tion of protein kinase A-that leads to the final step in the
antidiuretic action of AVP, i.e., the exocytic insertion of spe-
cific water channels, AQP2, into the luminal membrane,
thereby increasing the water permeability of that membrane.
These water channels are members of a superfamily of integral
membrane proteins that facilitate water transport (4,5). Aqua-
porin-l (AQP1 ; also known as CHIP, channel-forming integral
membrane protein of 28 kD) was the first protein shown to
function as a molecular water channel and is constitutively ex-
pressed in mammalian red cells, renal proximal tubules, thin
descending limbs, and other water-permeable epithelia (6). At the
subcellular level, AQP1 is localized in both apical and basolateral
plasma membranes that may represent entrance and exit routes for
transepithelial water transport. In contrast to AQP2, limited
amounts of AQPI are localized in membranes of vesicles or
vacuoles. In the basolateral membranes, AQP1 is localized to both
basal and lateral infoldings. AQP2 is the vasopressin-regulated
water channel in renal collecting ducts. It is exclusively present in
principal cells and inner medullary collecting duct cells and is
diffusely distributed in the cytoplasm in the euhydrated condition,
whereas apical staining of AQP2 is intensified in the dehydrated
condition or after vasopressin administration. These observations
are thought to represent the exocytic insertion of preformed water
channels from intracellular vesicles into the apical plasma mem-
brane (the shuttle hypothesis) (Figure 1). AQP3 and AQP4 are the
water channels in basolateral membranes of renal medullary col-
lecting ducts.
In congenital ND!, the renal collecting ducts are resistant to
the antidiuretic action of AVP or to its antidiuretic analog
l-desamino-8-D-arginine vasopressin (7,8). This is a rare, but
now well described, entity secondary either to mutations in the
AVPR2 gene (X-linked ND! [Online Mendelian Inheritance in
Man (OMIM), Johns Hopkins University, Baltimore, MD;
MIM No.: 3048001), which codes for the antidiuretic (V.,)
receptor, or to mutations in the AQP2 gene (autosomal reces-
sive ND! [OMIM, Johns Hopkins University; MIM No.:
222000]), which codes for the vasopressin-dependent water
channel (9-1 1). Of98 families with congenital NDI referred to
our laboratory in Montreal, 90 families have A VPR2 mutations
and eight have AQP2 mutations. Most of the affected pa-
tients (with AVPR2 or AQP2 mutations) have a full pheno-
type characterized by the inability to increase the urinary
osmolality value above the plasma osmolality value during
a pharmacological infusion of l-desamino-8-D-arginine Va-
sopressin (7). Only three AVPR2 mutations are characterized

Na�
,. K�
3Na� Principal cell of the
2K� collecting duct
AQP�
1120
AQP4
Inner medullarycollecting duct
1952 Journal of the American Society of Nephrology
Thick ascending limb of Henle
Thinlimb of Henle
�/“
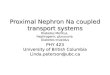
4�OOHFigure 1. Schematic representation of the nephron with selected areas involved in the urinary concentrating mechanism. (Top Left Panel) The
reabsorption of NaC1, but not water, from the ascending limbs of Henle, initiate countercurrent multiplication within the renal medulla. The
Na-K-2C1 cotransporter (inhibited by bumetanide) in the medullary thick ascending limb is shown. (Right Panel) Plasma arginine vasopressin
(AVP) increases water permeability in collecting ducts: The hormone is bound to the vasopressin V2 receptor (a G-protein linked receptor) on
the basolateral membrane. AVP activates adenylate cyclase, increasing the intracellular concentration of cAMP. The topology of adenylyl
cyclase is characterized by two tandem repeats of six hydrophobic putative transmembrane domains separated by a large cytoplasmic loop and
terminating in a large intracellular tail. Generation of cAMP follows receptor-linked activation of the heterometric G-protein (G�) and
interaction of the free G0�-chain with the adenylyl cyclase catalyst. A cAMP-dependent protein kinase A (PKA) is the target of the generated
cAMP. Cytoplasmic vesicles carrying the water channel proteins (represented as homotetrameric complexes) are fused to the luminal membrane
in response to vasopressin, thereby increasing the water permeability of this membrane. When vasopressin is not available, water channels are
retrieved by an endocytic process. and water permeability returns to its original low rate. Aquaporin-3 (AQP3) and AQP4 are expressed on the
basolateral membrane. Vasopressin also increases the permeability of the terminal part of the collecting duct to urea, resulting in movement
of urea into the medullary interstitium. This process is provided by urea transporters (represented here with 10 transmembrane domains). Both
the inner medullary collecting duct and thin descending limbs of short loops of Henle express a urea transporter (reprinted from reference 2
with permission).
by a mild phenotype with a less severe clinical disease and the
possibility of increasing urinary osmolality to approximately 400
mosmol/L during a dehydration test with a concomitant plasma
sodium concentration less than 150 mEq/L (12,13).
The human V, receptor gene AVPR2 is located in chromo-
some region Xq28 and has three exons and two small introns
(14, 15). The sequence of the cDNA predicts a polypeptide of
37 1 amino acids with a structure typical of guanine-nucleotide
(G) protein-coupled receptors with seven transmembrane, four
extracellular, and four cytoplasmic domains (16) (Figure 2A).
The human AQP2 gene is located in chromosome region
12ql3 and has four exons and three introns (10,1 1). It is predicted
to code for a polypeptide of 271 amino acids that is organized
into two repeats oriented at 1 80#{176}to each other and that has
six membrane-spanning domains, with both terminal ends
located intracellularly, and conserved asparagine-proline-

B
30 -
20 -
10 -
p% //-
Figure 2. (A) Ribbon representation of the AVP receptor 2 (AVPR2). This is a side view from a direction parallel to the cell membrane surface.
The positioning of transmembrane domains I through 7 is counterclockwise when viewed from the extracellular surface of the receptor. The
transmembrane helices are shown in red, and the intracellular and extracellular loops are shown in purple. The model is oriented such that the
extracellular side is at the top of the image. This hypothetical model of interaction between AVP and its V, receptor is constructed according
to the model published by Mouillac et a!. (3) pertaining to the �, receptor. AVP is supposed to be completely embedded into a 1 5 to 20 A
cleft defined by the transmembrane helices 2 through 7 of the receptor. The localization of the R 137 residue is represented. This image wasproduced using the MidasPlus program (Computer Graphics Laboratory, University of California. San Francisco. CA: supported by National
Institutes of Health Grant RR-01081). (B) Expression of the R137H mutant in L cells. The R137H mutant had unaltered affinity for tritiated
AVP but failed to stimulate adenylate cyclase (28). Inset shows the localization of the missense amino acid in a planar representation. Only
the first three transmembrane domains are represented.
I I I11 10 9 8 7 6
AVP (-log M)
Congenital ND! 1953
I
I
alanine (Asn-Pro-Ala) boxes (Figure 3). These features are char-
acteristic of the major intrinsic protein family. There is 48%
amino acid sequence identity between AQP2 and AQPI (I I).
Clinical Characteristics of A VPR2 Mutations,Incidence, Population Genetics, AncestralMutation and de novo Mutations, andMechanisms of A VPR2 Mutations
The AVPR2 gene is located in chromosome region Xq28
and, as a result, males who have an A VPR2 mutation have a
phenotype characterized by early dehydration episodes, hyper-
natremia, and hyperthermia as early as the first week of life.
The dehydration episodes can be so severe that they lower
arterial blood perfusion pressure to a degree insufficient to
sustain adequate oxygenation to the brain, kidneys. and other
organs. Mental and physical retardation and renal failure are
the classical “historical” consequences of a late diagnosis and
lack of treatment. Heterozygous females exhibit variable de-
grees of polyuria and polydipsia because of skewed X chro-
mosome inactivation. The onset and severity of the clinical
manifestations of autosomal recessive ND! are similar to those
of X-linked ND!.

Ri 870
Loop E
extracellular T 26M
68M
R85X
. S216Pintracellular
G64RLoop B
1 271
NH2
Figure 3. Schematic representation of the AQP2 protein and identification of 10 AQP2 mutations. A monomer is represented with six stretches
of hydrophobic sequences that are suggestive of six transmembrane helices. The major intrinsic proteins of lens (see text) share an NPA
(Asn-Pro-Ala) motif in each ofthe two prominent loops. AQP1 (and by analogy AQP2) is a homotretamer containing four independent aqueous
channels.
1954 Journal of the American Society of Nephrology
The early symptomatology of the nephrogenic disorder and
its severity in infancy is clearly described by Crawford and
Bode ( I 7). The first manifestations of the disease could be
recognized during the first week of life. The infants are irrita-
ble, cry almost constantly, and, although eager to suck, will
vomit milk soon after ingestion unless prefed with water. The
history given by the mothers often includes persistent consti-
pation; erratic. unexplained fever; and failure to gain weight.
Even though the patients characteristically show no visible
evidence of perspiration, increased water loss during fever or
in warm weather exaggerates the symptoms.
Unless the condition is recognized early, children will ex-
perience frequent bouts of hypertonic dehydration, sometimes
complicated by convulsion or death. Mental retardation is a
frequent consequence of these episodes. The intake of large
quantities of water, combined with the patient’s voluntary
restriction of dietary salt and protein intake, leads to hypoca-
loric dwarfism beginning in infancy. Affected children fre-
quently develop lower urinary tract dilatation and obstruction.
probably secondary to the large volume of urine produced ( I 8).
Dilatation of the lower urinary tract is also seen in primary
polydipsic patients and in patients with central (neurogenic)
diabetes insipidus ( 19.20). Chronic renal insufficiency may
occur by the end of the first decade of life and could be the
result of episodes of dehydration with thrombosis of the gb-
merular tufts (17).
Generally, X-linked ND! is a rare disease with an estimated
prevalence of approximately four per 1 million males and a
carrier frequency of 7.4 X lO_6; these figures are based on the
number of patients with X-linked ND! known in Quebec (21).
In defined regions of North America, however, the prevalence
is much higher. It is assumed that the patients in these regions
are progeny of common ancestors. An example is the Mormon
pedigree, with its members residing in Utah (Utah families);
this pedigree was originally described by Cannon (22,23). The
“Utah mutation” is a missense mutation (L3 12X) predictive of
a receptor that lacks transmembrane domain 7 and the intra-
cellular C terminus (23). The largest known kindred with
X-linked ND! is the Hopewell family, named after the Irish
ship Hopewell that arrived in Halifax, Nova Scotia, in 1761
(24). Aboard the ship were members of the Ulster Scot clan,
descendants of Scottish Presbyterians who migrated to the
Ulster Province of Ireland in the 17th century and left Ireland
for the new world in the 1 8th century.

Congenital NDI 1955
Whereas families arriving with the first emigration wave
settled in northern Massachusetts in 17 1 8, the members of a
second emigration wave, passengers of the Hopewell, settled in
Colchester County, Nova Scotia. According to the “Hopewell
hypothesis” (24), most NDI patients in North America are
progeny of female carriers from the second emigration wave.
This assumption is based mainly on the high prevalence of ND!
among descendants of the Ulster Scots residing in Nova Scotia.
In two villages with 2500 inhabitants, 30 patients have been
diagnosed, and the carrier frequency has been estimated at 6%
(2 1 ). Given the numerous mutations found in North American
X-linked ND! families, the Hopewell hypothesis cannot be
upheld in its originally proposed form. However, among X-
linked ND! patients in North America, the W7IX mutation is
more common than another AVPR2 mutation. It is a null
mutation (W71X; 23,25) (Figure 4) predictive of an extremely
truncated receptor consisting of the extracellular N terminus,
intracellular
the first transmembrane domain, and the N-terminal half of the
first intracellular loop. Because the original carrier cannot be
identified (21), it is not clear whether the Hopewell mutation
was brought to North America by Hopewell passengers or by
other Ulster Scot immigrants. Seventy-two different putative
disease-causing mutations in the AVPR2 gene have now been
reported in 102 unrelated families with X-linked NDI (Figure
4). The diversity of AVPR2 mutations found in many ethnic
groups (Caucasians, Japanese, African-Americans, Africans)
and the rareness of the disease are consistent with an X-linked
recessive disease that in the past was lethal for male patients
and was balanced by recurrent mutations. In X-linked ND!,
loss of mutant alleles from the population occurs because of the
higher mortality of affected males compared with healthy
males, whereas gain of mutant alleles occurs by mutation. If
affected males with a rare X-linked recessive disease do not
reproduce and if mutation rates are equal in mothers and
extracellular
Figure 4. Schematic representation of the V2 receptor and identification of 72 A VPR2 mutations, which include 36 missense, 10 non-sense, 18
frameshift, two inframe deletions, one splice-site, and five large deletion mutations. The four large deletions are characterized incompletely and
are not included in the figure. Predicted amino acids are given as the one-letter code. Solid symbols indicate the predicted location of the
mutations; an asterisk indicates two different mutations in the same codon. The names of the mutations were assigned according to the
conventional nomenclature. The extracellular (E1 to E1,,,), cytoplasmic (C1 to C1�), and transmembrane domains (TM1 to TM�11) are labeled from
the N terminus to the C terminus, according to Sharif and Hanley (40). E1: 98del28. 98ins28, 1 l3delCT. TM1: L44F, L44P, L53R, L62P. TM3
and C1: 253del35, 255del9. C1: 274insG, W71X. TM13: H8OR, L83P, D85N, V88M, 337delCT, P95L. E13: R1O6C, 4O2delCT, Cl l2R, RI 13W.
TM111: QI l9X, YI24X, SI26F, Y128S, AI32D. C11: R137H, RI43P, 528de17, 528delG. TM1�: Wl645, SI67L, S167T. E331: R181C, G185C,
R202C, T204N, 684delTA, Y205C, V206D. TM�: L219R, Q225X, 753insC. C111: E231X, 763delA, 786delG, E242X, 8O4insG, 8O4delG,
834delA, 855delG. TM�1: V277A, V278, Y280C, W284X, A285P, P286L, P286R, L292P, W293X. E,,,,: 977delG, 982-2A--*G. TM�11:
L312X, P322H, P322S, W323R. C3�: R337X. Whereas deletions and insertions can be attributed to slipped mispairing during DNA replication
favored by direct repeats, complementary repeats and symmetric sequences in the vicinity of the mutation (more than 50% of the single-base
substitutions) can be explained by mutations in CpG dinucleotides, which are hot spots for genetic disease and which are relatively common
in the human V2 receptor gene (26).

1956 Journal of the American Society of Nephrology
fathers, then, at genetic equilibrium, one-third of new cases of
affected males will be due to new mutations. We and others
have described ancestral mutations, de navo mutations, and
potential mechanisms of mutagenesis (26). These data are
reminiscent of those obtained from patients with late-onset
autosomal-dominant retinitis pigmentosa. In one-fourth of
these patients, the disease is caused by mutations in the light
receptor rhodopsin. Here, too. many different mutations (ap-
proximately 100). spread throughout the coding region of the
rhodopsin gene, have been found (27).
The basis of loss of function or dysregulation of 28 different
mutant V, receptors (including non-sense, frameshift, deletion,
or missense mutations) has been studied using in vitro expres-
sion systems (Figure 2B). Most of the mutant V, receptors
tested were not transported to the cell membrane and were
thus retained within the intracellular compartment (8).
Schoneberg and coworkers (29) pharmacologically rescued
truncated V, receptors by coexpression of a polypeptide
consisting of the last 130 amino acids of the V, receptor.
Four of the six truncated receptors (E242X, 8O4delG,
834delA, and W284X) regained considerable functional ac-
tivity as demonstrated by an increase in the number of
binding sites and stimulation of adenylate cyclase activity.
These in vitro results are potentially promising avenues for
the gene therapy of AVPR2 mutations.
AQP2 MutationsThe AQP2 gene is located in chromosome region l2ql3.
Males and females affected with congenital NDI have been
described who are homozygous for a mutation in the AQP2
gene �r who carry two different mutations (9,10,12,30,31)
(Figure 3). Functional expression studies showed that Xe-
flO/)U5 oocytes injected with mutant cRNA had abnormal
coefficient of water permeability, whereas Xenopus oocytes
injected with both normal and mutant cRNA had coefficient
of water permeability similar to that of normal constructs
alone. These findings provide conclusive evidence that ND!
can be caused by homozygosity for mutations in the AQP2
gene. More recently, we obtained evidence in three ances-
trally independent families to suggest that both autosomal
dominant and autosomal recessive ND! phenotypes could be
secondary to novel mutations in the AQP2 gene. Reminis-
cent of expression studies done with AVPR2 proteins, Deen
and coworkers also demonstrated that the major cause un-
derlying autosomal recessive NDI is the misrouting of
AQP2 mutant proteins (3 1,32).
Carrier, Perinatal Testing, and PerspectivesOver the past few years, it has become clear that congenital
NDI is caused by an inactivating mutation of a G-protein-
coupled receptor (V, receptor) or a water channel (AQP2). The
time of onset of the disease (shortly after birth) and the clinical
symptoms do not differ between the two forms. However, the
two forms can be distinguished by clinical testing: Whereas
desmopressin elicits extrarenal (coagulation and vasodilatory)
responses in patients with autosomal recessive NDI. patients
with X-linked ND! lack extrarenal response to desmopressin
(9,33,34).
Identification of the molecular defects underlying congenital
NDI is of immediate clinical significance. allowing diagnosis
by gene analysis. We encourage physicians who follow fami-
lies with X-linked and non-X-linked ND! to recommend mo-
lecular genetic analysis. because early diagnosis and treatment
of affected infants can avert the physical and mental retardation
associated with episodes of dehydration. Diagnosis of X-linked
ND! was accomplished by mutation testing of a sample of cord
blood in five of our patients. These patients were immediately
treated with abundant water intake, a low-sodium diet, and
hydrochlorothiazide. They never experienced episodes of
dehydration, and their physical and mental development is
normal. Gene analysis should be performed in newborns
with a family history of NDI and in patients of all age
groups with a firm diagnosis of congenital ND!, with or
without a family history. It may also be considered in babies
presenting with continuing fever of unknown origin, vom-
iting, constantly low urine osmolality, and failure to thrive.
Gene analysis is also important for the identification of
nonobligatory female carriers in families with X-linked
ND!. Most females heterozygous for a mutation in the V,
receptor do not present with clinical symptoms; few are
severely affected (35.36) (D.G. Bichet. unpublished obser-
vations).
All complications of congenital ND! are prevented by an
adequate water intake. Thus, patients should be provided with
unrestricted amounts of water from birth to ensure normal
development. In addition to a low-sodium diet, the use of
diuretics (thiazides) or indomethacin may reduce urinary out-
put. This advantageous effect has to be weighed against the
side effects of these drugs (thiazides: electrolyte disturbances;
indomethacin: reduction of glomerular filtration rate and gas-
trointestinal symptoms). With the identification of the genes
responsible for congenital NDI, a causative treatment based on
gene transfer has become possible.
Two prerequisites crucial for gene therapy seem to be ful-
filled in both forms of congenital ND!. (1) The defect in the
kidney appears to be restricted to water reabsorption with no
other functional or histological defects. Unlike central diabetes
insipidus (37), retinitis pigmentosa (see above), and many
other diseases, a deterioration of kidney function due to
progressive structural changes is not observed. Thus, organ
integrity seems to be preserved. (2) Recent experiments with
rats show that adenoviral-mediated gene transfer to the
tubular system of the kidney can be achieved either by
selective perfusion of the renal artery or by retrograde
infusion through a catheter placed into the pelvic cavity
(38). Depending on the route, expression of the reporter
gene (/3-galactosidase) is observed in proximal tubule cells
(kidney perfusion via renal artery) or tubular cells of the
papilla and medulla (retrograde infusion).
The mutations in the V, receptor associated with X-linked
NDI were the first naturally occurring mutations found in the
very large group of G-protein-coupled hormone receptors.
Within the past few years. however, a number of diseases were

Congenital NDI 1957
shown to be caused by mutations in genes encoding G-protein-
coupled receptors. In addition to retinitis pigmentosa and X-
linked ND!, examples of such diseases/symptoms include:
stationary night blindness, color blindness/altered color per-
ception, primary adrenocortical deficiency, hypocalciuric hy-
percalcemia/hyperparathyroidism, hypercalcemia/metaphyseal
chondrodysplasia, hypocalcemia, male precocious puberty,
male pseudohermaphroditism, hyperfunctioning thyroid ade-
noma, and Hirschsprung’s disease (reviewed in reference 39).
The main defect of many inactivating mutations is the reduced
expression of mutant receptors on the cell surface. Here, the
loss of receptor function occurs regardless of the remaining
biological activity of the individual protein. At present, little is
known about the cellular routing of 0-protein-coupled recep-
tors. Progress in this field will be crucial for the understanding
of the clinical phenotypes of receptor diseases on a molecular
level and for the development of therapeutic strategies based
on gene transfer.
AcknowledgmentsDr. Bichet is a Career Investigator of the Fonds de Ia Recherche en
Sante du Qu#{233}bec.This work was supported by Grant MT-8 126 fromthe Medical Research Council of Canada, by the Canadian KidneyFoundation, and by the Fonds de Ia Recherche en Sant#{233}/Hydro-
Qu#{233}bec.
References1 . Knepper MA, Rector FC Jr: Urine concentration and dilution. In:
The Kidney, 5th Ed., edited by Brenner BM .Philadelphia, W. B.
Saunders, 1996, pp 532-570
2. Bichet DG: Nephrogenic diabetes insipidus and vasopressin re-
ceptor. In: Coiztemporarv Endocrino!ogv: G-Proteins, Recep-
tors. and Disease, edited by Spiegel, AM, Totowa, NJ, Humana,
1997, p 170
3. Mouillac B, Chini B, Balestre M-N. Elands I, Trumpp-Kallm-
eyer S. Hofiack J, Hibert M, Jard 5, Barberis C: The binding site
of neuropeptide vasopressin V 1a receptor: Evidence for a major
localization within transmembrane regions. J Bio! Chei�i 270:
25771-25777, 1995
4. Walz T, Hirai T, Murata K, Heymann JB, Mitsuoka K, FujiyoshiY, Smith BL, Agre P, Engel A: The three-dimensional structure
ofaquaporin-l. Nature 387: 624-627, 1997
5. Cheng A, van Hock AN, Yeager M. Verkman AS. Mitra AK:
Three-dimensional organization of a human water channel. Na-
ture 387: 627-630, 1997
6. Agre P, Preston GM, Smith BL, Jung JS, Raina 5, Moon C,
Guggino WB, Nielsen 5: Aquaporin CHIP: The archetypal mo-
lecular water channel. Am J Phvsio! 34: F463-F476, 1993
7. Bichet DG: Nephrogenic diabetes insipidus. In: O.�ford Textbook
of Clinical Nep/irologv. 2nd Ed., Vol. 2, edited by Cameron iS,
Davison AM, Grfinfeld JP, Kerr DNS, Ritz E. New York, Oxford
University Press, 1997, pp 1095-1 1 12
8. Fujiwara MT. Morgan K, Bichet DG: Molecular analysis of
X-linked nephrogenic diabetes insipidus. Ear J Endocrino! 134:
675-677, 1996
9. Deen PMT, Verdijk MAJ, Knoers NVAM. Wieringa B, Mon-nens LAH, van Os CH. van Oost BA: Requirement of human
renal water channel aquaporin-2 for vasopressin-dependent con-
centration of urine. Scie,zce 264: 92-95. 1994
10. van Lieburg AF, Verdijk MAJ, Knoers NVAM. van Essen Al.
Proesmans W. Mallmann R, Monnens LAH. van Oost BA, van
Os CH. Deen PMT: Patients with autosomal nephrogenic diabe-tes insipidus homozygous for mutations in the aquaporin 2 water-
channel gene. Aiiz J Hum Genet 55: 648-652, 1994I I . Agre P. Brown D, Nielsen 5: Aquaporin water channels: Unan-
swered questions and unresolved controversies. Curr Opin Ce!!
Bio! 7: 472-483 1995
I 2. Vargas-Poussou R, Forestier L. Dautzenberg MD. Niaudet P.
D#{233}chauxM. Antignac C: Mutations in the vasopressin V2 recep-
tor and aquaporin-2 genes in 12 families with congenital neph-
rogenic diabetes insipidus. J Aiii Soc Nepliro! 1997, in press
13. Sadeghi H, Robertson GL, Bichet DG, Innamorati G, Birn-
baumer M: Biochemical basis of partial NDI phenotypes. Mo!
Endocrino! 1998. in press
14. Birnbaumer M, Seibold A, Gilbert S. Ishido M, Barberis B,
Antaramian A, Brabet P. Rosenthal W: Molecular cloning of the
receptor for human antidiuretic hormone. Nature 357: 333-335.
1992
15. Seibold A, Brabet P. Rosenthal W, Birnbaumcr B: Structure and
chromosomal localization of the human antidiuretic hormone
receptor gene. Am J Hum Gene! 5 1 : 1078 -1083. 1992
16. Watson 5, Arkinstall 5: The G protein linked receptor Facts-
Book. In: FactsBook Series, London, Academic. 1994. pp 1-42717. Crawford ID. Bode HH: Disorders of the posterior pituitary in
children. In: Endocrine and Genetic Diseases of Childhood and
Ado!esce,ice, edited by Gardner LI. Philadelphia. W. B. Saun-
ders, 1975, pp 126-158
18. Streitz JM Jr. Streitz JM: Polyuric urinary tract dilatation with
renal damage. J Uro! 139: 784-785. 1988
19. Boyd SD, Raz D, Ehrlich RM: Diabetes insipidus and nonob-structive dilation of urinary tract. Urology 26: 266-269, 1980
20. Gauthier B, Thieblot P. Steg A: M#{233}gauret#{232}re.m#{233}gavessie Ct
diab#{232}teinsipide familial. Scm Hop 57: 60-61. 1981
21. Bichet DG, Hendy GN, Lonergan M, Arthus MF, Ligier S.
Pausova Z. Kluge R, Zingg H, Saenger P. Oppenheimer E,
Hirsch DI, Gilgenkrantz S. Salles JP. Oberl#{233}1. Mandel JL.
Gregory MC, Fujiwara TM, Morgan K, Scriver CR: X-linked
nephrogenic diabetes insipidus: From the ship Hopewell to re-
striction fragment length polymorphism studies. Am J Hu??l
Genet 51 : 1089-1 102, 1992
22. Cannon IF: Diabetes insipidus clinical and experimental studieswith consideration of genetic relationships. Are/i Interii Med 96:
215-272, 1955
23. Bichet DG, Arthus MF, Lonergan M. Hendy GN, Paradis Al.
Fujiwara TM, Morgan K, Gregory MC, Rosenthal W, Didwania
A, Antaramian A, Birnbaumer M: X-linked nephrogenic diabetesinsipidus mutations in North America and the Hopewell hypoth-
esis. J C!in Invest 92: 1262-1268, 1993
24. Bode HH, Crawford ID: Nephrogenic diabetes insipidus in NorthAmerica: The Hopewell hypothesis. N Eng! J Med 280: 750-
754, 1969
25. Holtzman EJ, Kolakowski LF, O’Brien D, Crawford ID, Aus-
iello DA: A null mutation in the vasopressin V2 receptor gene
(AVPR2) associated with nephrogenic diabetes insipidus in theHopewell kindred. Hum Mo! Genet 2: 1 201-1 204. 1993
26. Bichet DG, Birnbaumer M, Lonergan M. Arthus MF, Rosenthal
W, Goodyer P. Nivet H, Benoit 5, Giampietro P. Simonetti S.Fish A, Whitley CB. Jaeger P. Gertner I, New M, DiBona FJ,
Kaplan BS, Robertson GL, Hendy GN, Fujiwara TM. Morgan K:
Nature and recurrence of AVPR2 mutations in X-linked neph-
rogenic diabetes insipidus. Am J Huiiz Genet 55: 278-286. 1994
27. Vaithinathan R. Berson EL. Dryja TP: Further screening of the

1958 Journal of the American Society of Nephrology
rhodopsin gene in patients with autosomal dominant retinitis
pigmentosa. Genomics 2 1 : 46 1-463, 1994
28. Rosenthal W. Antaramian A, Gilbert 5, Birnbaumer M: Neph-
rogenic diabetes insipidus. JBio! them 268: 13030-13033, 1993
29. Schoneberg T. Yun I. Wenkert D, Wess I: Functional rescue of
mutant V2 vasopressin receptors causing nephrogenic diabetes
insipidus by a coexpressed receptor polypeptide. EMBO J 15:1283-1291, 1996
30. Hochberg Z. van Lieburg A, Even L. Brenner B. Lanir N. van
Oost BA, Knoers NVAM: Autosomal recessive nephrogenic
diabetes insipidus caused by an aquaporin-2 mutation. J Clii,
Endocrino! Metab 82: 686-689, 1997
3 1 . Mulders SB, Knoers NVAM, van Lieburg AF, Monnens LAH.
Leumann E. WUhl E, Schober E, Rijss JPL. van Os CH. Deen
PMT: New mutations in the AQP2 gene in nephrogenic diabetes
insipidus resulting in functional but misrouted water channels.
J An: Soc Nephro! 8: 242-248. 1997
32. Deen PMT. Croes H, van Aubel RAMH. Ginsel LA, van Os CH:
Water channels encoded by mutant aquaporin-2 genes in neph-rogenic diabetes insipidus are impaired in their cellular routing.
J C!in latest 95: 2291-2296, 1995
33. Bichet DG. Razi M. Lonergan M. Arthus MF. Papukna V. Kortas
C, Barjon IN: Hemodynamic and coagulation responses to I-desaminoi8-n-arginine]vasopressin (dDAVP) infusion in pa-
tients with congenital nephrogenic diabetes insipidus. N Eng!
JMed3l8: 881-887, 1988
34. Knoers N. Monnens LAH: A variant of nephrogenic diabetes
insipidus: V2 receptor abnormality restricted to the kidney. Eur
J Pediatr 150: 370-373, 1991
35. Oksche A, Dickson I, SchUlein R, Seyberth HW, Muller M,
Rascher W. Birnbaumer M, Rosenthal W: Two novel mutations
in the vasopressin V2 receptor gene in patients with congenital
nephrogenic diabetes insipidus. Biochem Biophvs Res �ommun
205: 552-557, 1994
36. van Lieburg AF, Verdijk MAJ. Schoute F, Ligtenberg MJL, van
Oost BA, Waldhauser F, Dobner M, Monnens LAH, Knoers
NVAM: Clinical phenotype of nephrogenic diabetes insipidus in
females heterozygous for a vasopressin type 2 receptor mutation.
Hum Genet 96: 70-78, 1995
37. Rittig R, Robertson GL, Siggaard C, Kov#{225}csL, Gregersen N,
Nyborg I, Pedersen EB: Identification of 13 new mutations in the
vasopressin-neurophysin II gene in 17 kindreds with familial
autosomal dominant neurohypophyseal diabetes insipidus. Am J
Hun, Genet 58: 107-1 17, 1996
38. Moullier P. Friedlander G, Calise D, Ronco P. Pemcaudet M,
Ferry N: Adenoviral-mediated gene transfer to renal tubular cells
in i’is’o. Kidney hit 45: 1220-1 225, 1994
39. Coughlin SR: Expanding horizons for receptors coupled to G-
proteins: Diversity and disease. Curr Bio! 6: 191-197. 1994
40. Sharif M, Hanley MR: Peptide receptors: Stepping up the pres-
sure. Nature 357: 279-280, 1992