Embed Size (px)
Citation preview
Concussion: Current Concepts to Drive Evidence Based Evaluation and Management
Zac Lynch
Outline
• Concussion overview
• Epidemiology
• Pathophysiology
• Symptoms and Signs
• Assessment tools and clinical measures
• Management of the course of injury
• Concussion risk reduction
What is a concussion?1
• Concussion is classified as a brain injury comprised of complex physiological/functional injury with chemical alterations and not anatomical alterations
• Brain injury sustained from either impact forces or non-impact forces
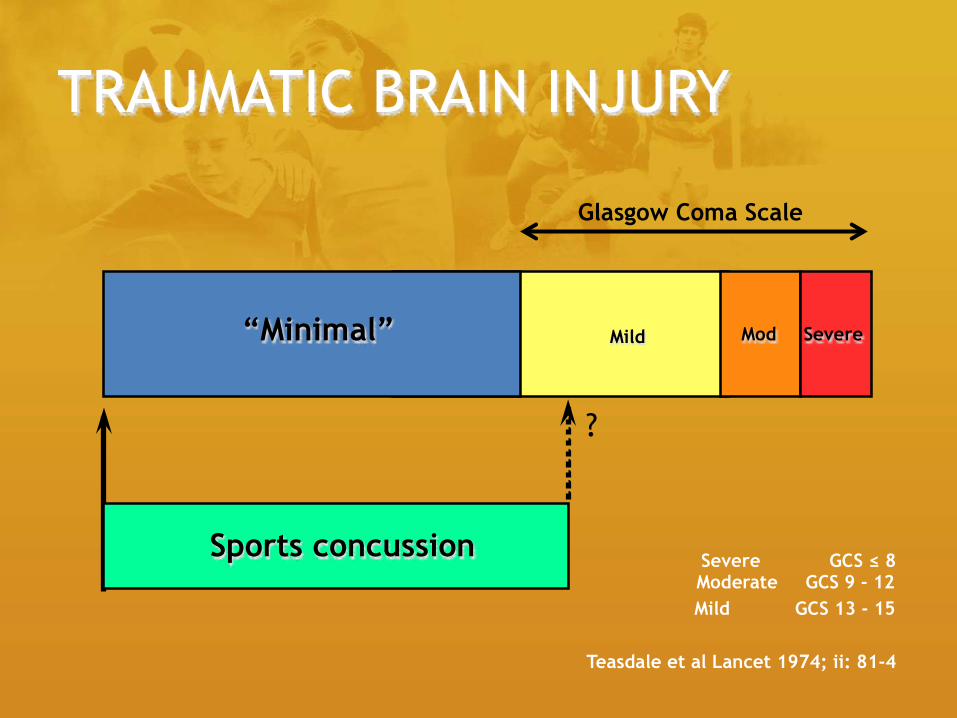
TRAUMATIC BRAIN INJURY
Mod Mild Severe
Severe GCS ≤ 8 Moderate GCS 9 - 12
Mild GCS 13 - 15
Teasdale et al Lancet 1974; ii: 81-4
Sports concussion
?
“Minimal”
Glasgow Coma Scale
Who gets these concussions, and are they really that important?3
• MOI: sports, car crash, falls, assault
• 1.5-8.0 million total reported concussion cases each year in U.S.
• Over 1.6 million sport related concussion each year
• 6-10 per 100,000 result in death each year with only 2% of reported cases resulting in death when classifying concussion as the primary cause of death
• 15% experience PCS
Relation of concussion to sport3
• 7% of injuries in youth sport
• 9% of injuries in high school sport
• 6% of injuries in collegiate sport
• 53% of high school athletes have sustained a concussion before participation in high school sports
– 36% of collegiate athletes have a history of multiple concussions
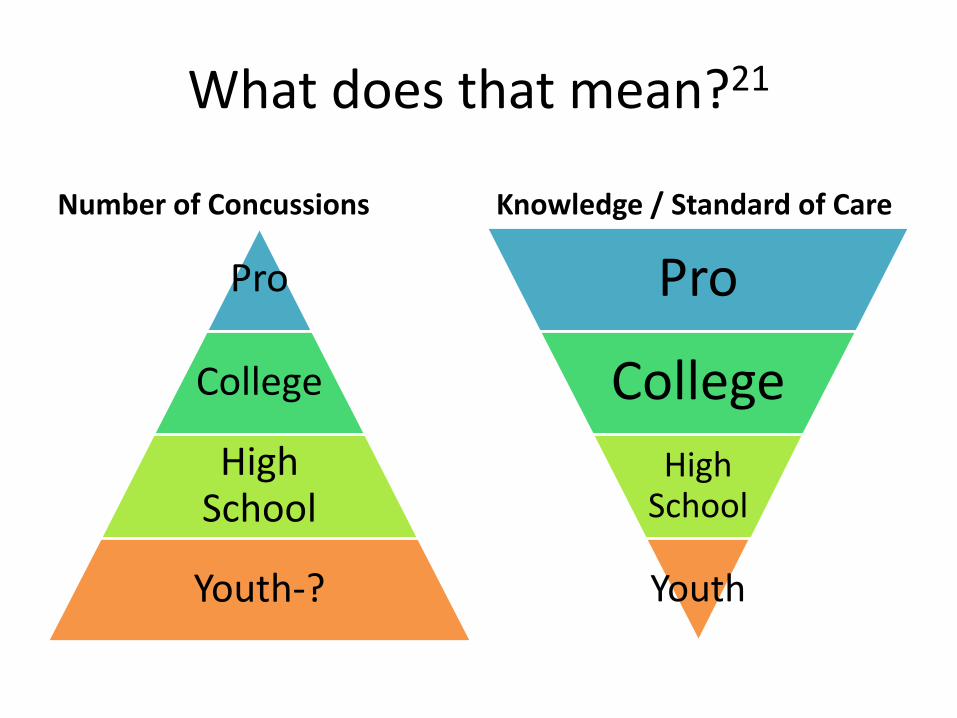
What does that mean?21
Number of Concussions
Pro
College
High School
Youth-?
Knowledge / Standard of Care
Pro
College
High School
Youth
The numbers large, classification mild, and pathology complex4,5
• The changes that occur within the neuronal mechanics are complex.
• What starts this whole process we know as a concussion?
– External forces causing trauma and shearing of internal neuronal dendrites causing sustained depolarization from specialized signals in the cerebrum in correlation with the lobe of injury
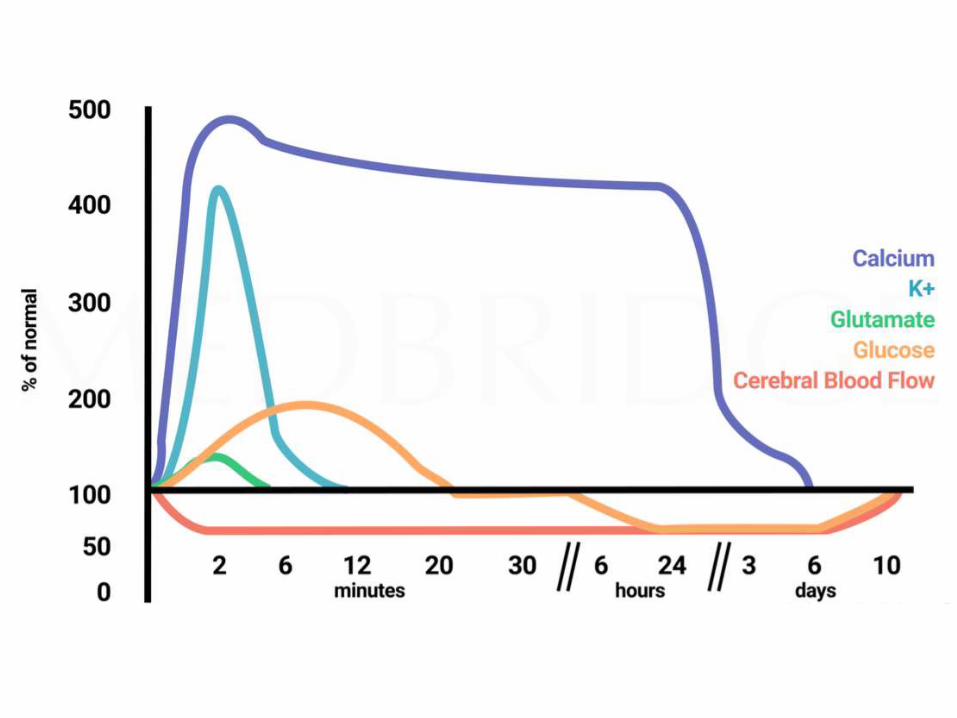
Physiology4,5
• Ionic changes• K+• Ca2+• Na-K-ATPase
• Neurotransmitters• Excitatory neurons (primarily
Glutamate) respond in association to the excited state of the lobes and in turn continue to interact and communicate with the corresponding distal cell
• Blood flow involvement• The area with trauma now has 40%
less blood flow• Less blood means less glucose/H20
being transported across the blood brain barrier
• Cellular energy impact
• Energy crisis• Less glucose means the less glucose
that gets transported to the neuronal cell mitochondria
• The less glucose for mitochondria means the less ATP that is produced
• The less ATP produces means prolonged dysfunction of the Na-K-ATPase pump b/c it is driven by ATP
• The lack of this pump working means prolonged cellular depolarization from the K and Ca, meaning that the Glutamate is still stimulated and acts to communicate with the corresponding cell which then means that the patient is still experiencing the symptoms from the Cerebral brain injury from the persistent specific informational impulses


Preparation planning5,6
• Rid the emotion
– Have a plan set so that you can appropriately screen an individual with impact from the game, family, etc.
• Age plays a factor in screening
– Age makes a difference on communication and the ability to openly discuss what they are truly feeling (eg. teenagers).
• Unconscious vs. conscious
Symptoms5,7
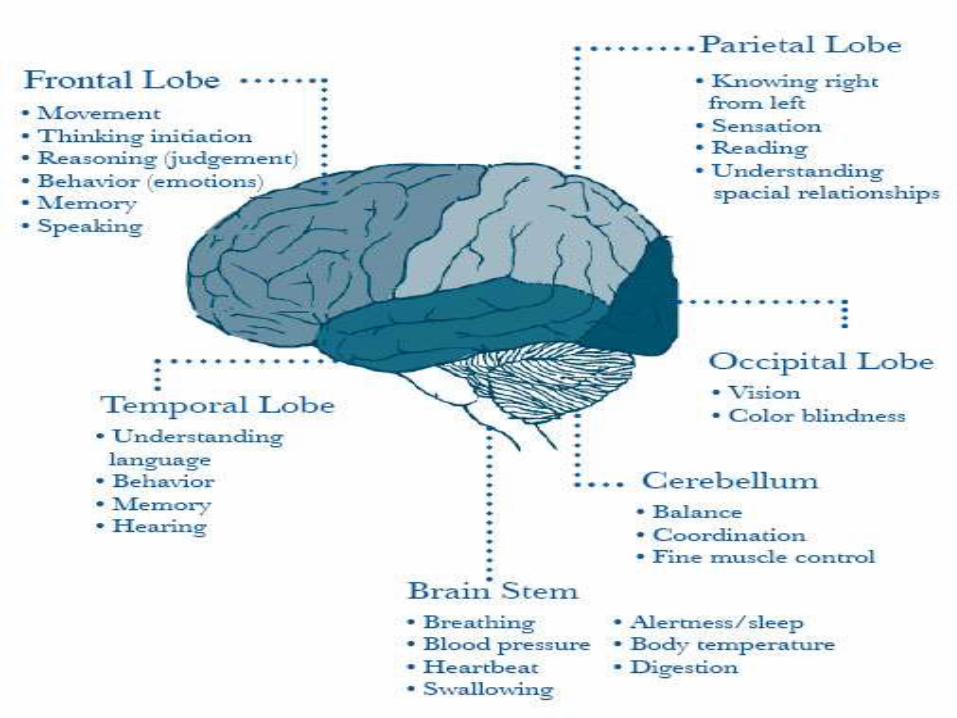
• Symptoms presentation correlates to the injured lobe of the brain, so the symptoms will be similar with the function of that lobe. The input of a stimulus to that lobe after a concussion is much more sensitive.
• Somatic • Cognitive • Emotional • Sleep
Signs1,5-8
• Appearance of dazed/confused
• Disorientation
• Forgets instruction
• Clumsiness/incoordination
• Delayed verbal expression
• LOC
• Mood changes
• Vacant stare
• Decreased attention
• Slurred speech
• Emotional lability
• Fatigue
• Difficulty reading
• Amnesia (retro vs ante)
• Short term memory impairment
What tools and strategies are needed to actually signify these S&S?9
• Preseason Baseline Testing
• Acute Management
• Sideline Management
• Clinical/Follow Up Management
Preseason Testing9-13
• Brief testing to measure balance, somatic and neurobehavioral symptoms, attention span, working memory, and reaction time.
– SCAT 3 (sections 3-8 only)
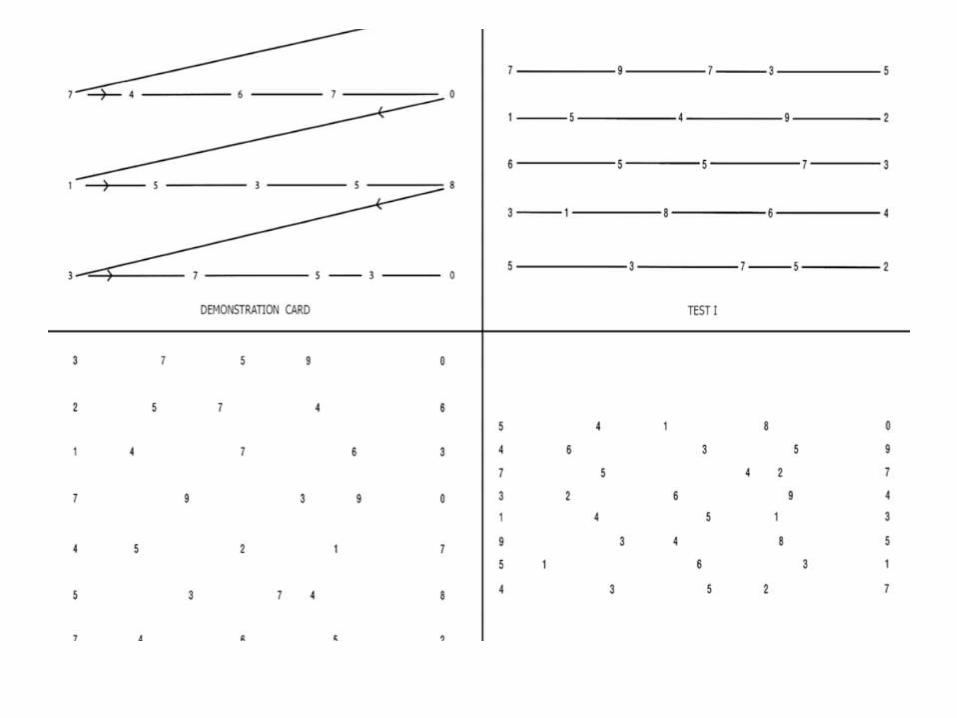
– King-Devick Test
– VOMS
– Clinical Reaction Time
– Agility times
– ImPACT Test
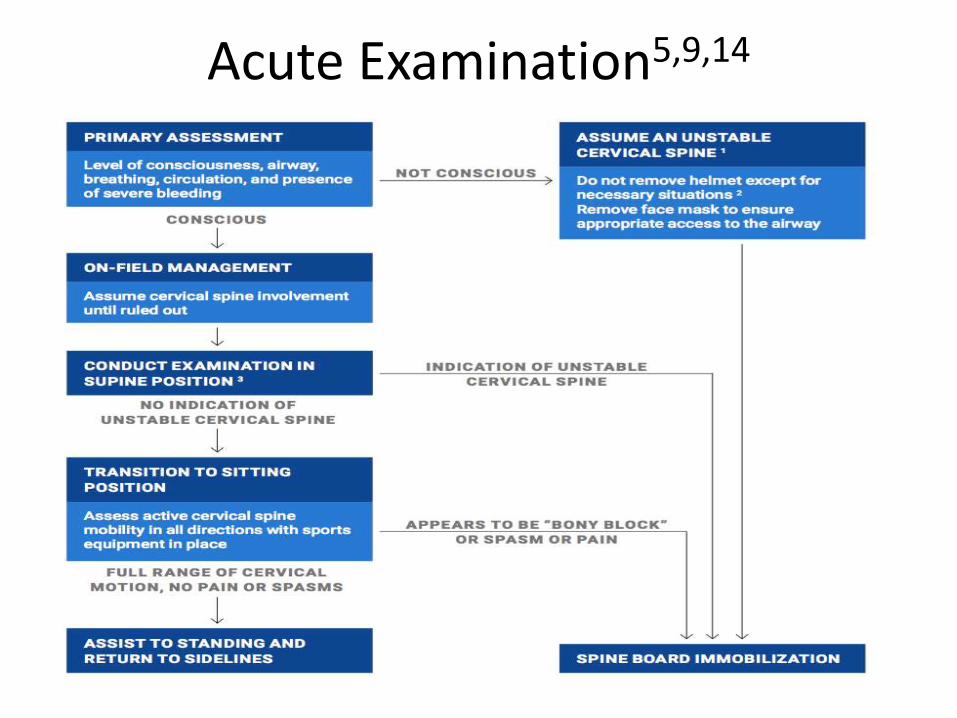
Acute Examination5,9,14
Once removed from activity5,9
• Next phase of examination begins only after a C-spine injury has been ruled out.
• The athlete will be questioned subjectively with a strong emphasis on objective questions, rather than close-ended and questions that give minimal feedback.
Sideline Examination5,10,11,14,15
• King-Devick test
• VOMS
• SCAT 3 with modifications discussed during preseason testing
• Cranial nerves II, III, IV, VII, XI
• Evaluate progression of symptoms and possible red flags from the ACE.
ACE Red Flags16
• HA that worsens
• Seizures
• Focal neurological signs
• Very drowsy; cannot be awakened
• Repeated vomiting
• Slurred speech
• Cannot recognize people or places
• Progression of confusion or irritability
• Weakness/numbness in any extremity
• Neck pain
• Behavioral change
• State of consciousness change
•
Can the athlete return to play?1,2,5
• The only way to athlete will return to play on the same day is if no S&S were ever present on the field or on the sideline. If S&S were negative during exertion testing, then the athlete MAY return to play.
Education Provided After the Game1,5,17,18
• Sleep as much as possible, do not be afraid to go to sleep
• Avoid electronic stimulation• Minimize educational work• Take rest breaks• Use ice pack • Avoid pain medication, but continue normal
medication you normally take• Avoid alcohol• Avoid driving
Follow-Up Examination
Follow-Up Examination5
• Intake questionnaire
• Subjective examination
– Who hit them; what was score; do they remember what happened
– Dizziness and amnesia post-concussion result in longer resolution times
Follow-Up Exam Continued…5,10,11,19
• SCAT-3
• Neurological exam
• Musculoskeletal exam
• VOMS
– Assess subjective symptoms of headache, dizziness, nausea, fogginess prior to administering this assessment, as well as after each component

Follow-Up Exam Continued…12,13,20
• ImPACT
• Clinical Reaction Time
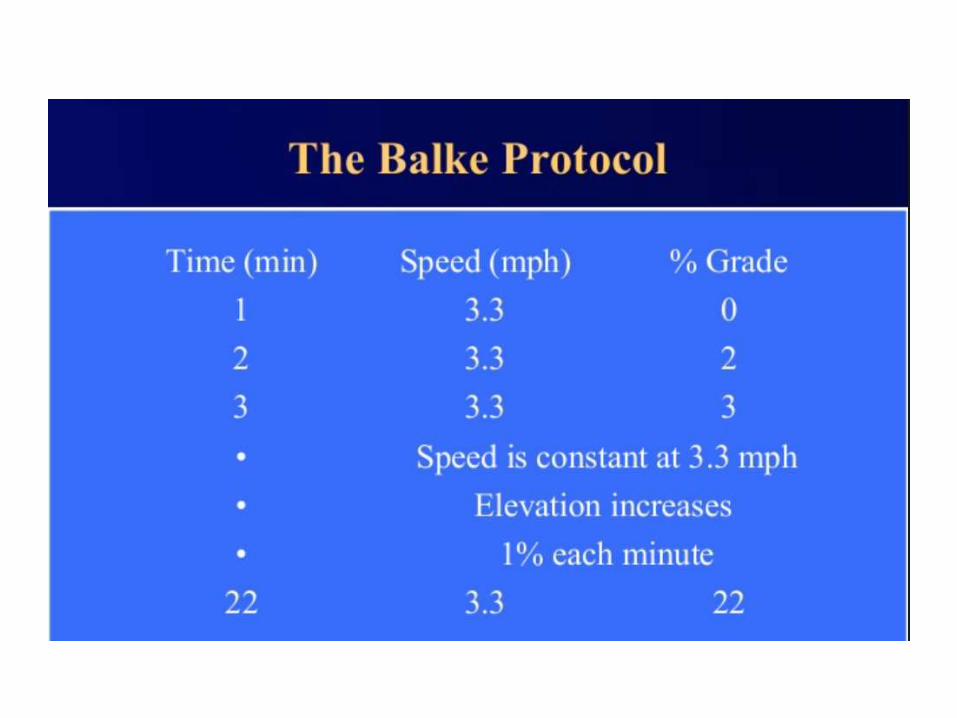
• Balke Treadmill Protocol
– Determine symptom threshold exercise tolerance
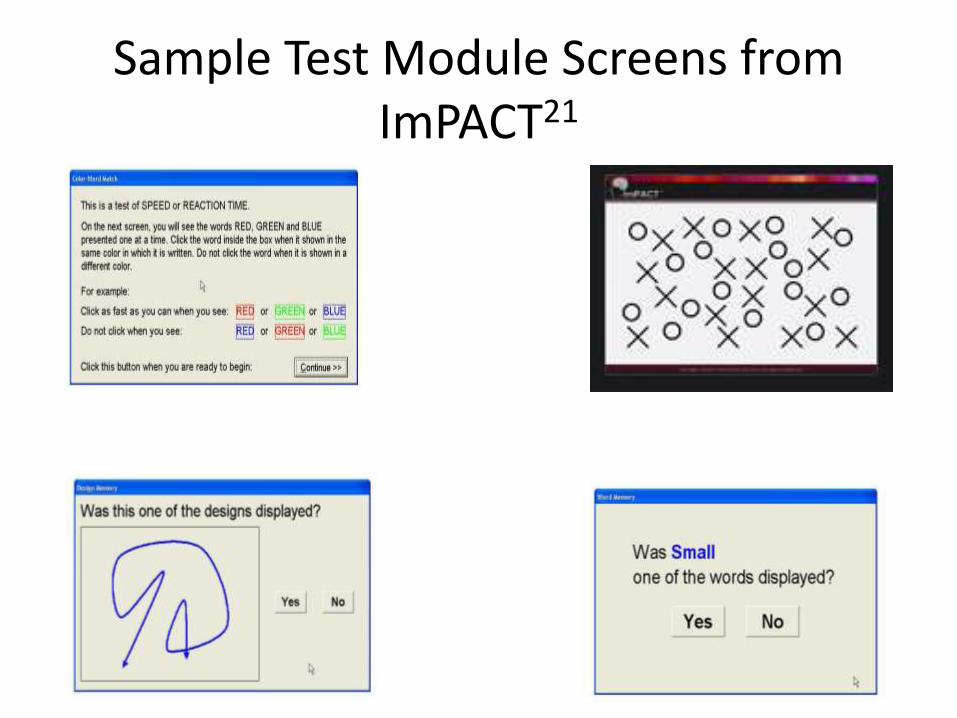
Sample Test Module Screens from ImPACT21
Education Provided after Follow-Up Evaluation5,7,9
• Concussion education
• Reassurance
• Education on how to manage symptoms
• Educate on return to play guidelines
• Rest until symptoms cease, then activity protocol begins – Research shows that more than 3 days of solitary
rest can prolong symptoms and keep athletes out even longer
Rehabilitation and Return to Play1,2,5,22
• These MUST be met before return to play is even considered
– Symptom resolution
– Normal neurologic exam
– Neurocognitive testing return to baseline
– Exertion
• Graduated physical activity protocol with absolutely ZERO return of symptoms
Return to Learn1,5,10
• Neurocognitive testing determines ability to return to academics.
– If they do poorly on the NC testing, it is correlated with poor academic performance.
• Use accommodations.
– Limit reading if ocular symptoms.
– Limit physical exertion (PE class, choir, band, drams) in its entirety until cleared.
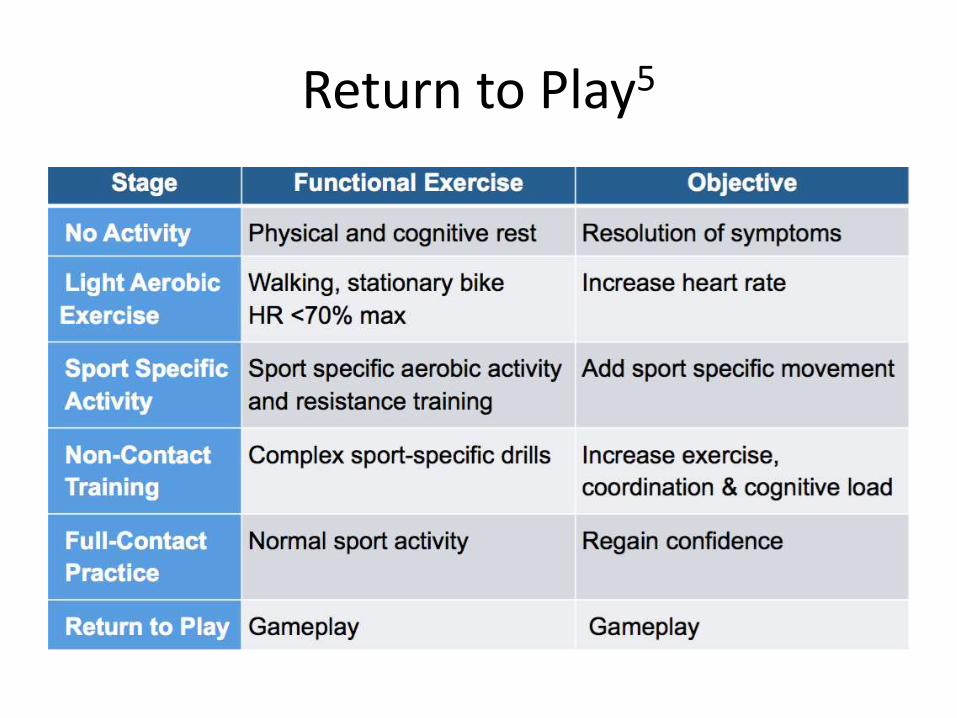
Return to Play5
About the Graduated Protocol5
• Concussions respond in a relatively short amount of time, given if the treatment and modifications are appropriate.
• If symptoms onset, regress a stage in the physical activity protocol and begin again.
• Goal is to have the athlete remain at each stage for 24 hours before progression to the next stage.
Why such a strenuous protocol for return to play? What if they need their star player back for the final minutes
of a rivalry game?1,5,23
What are the consequences?1,2,22-24
• Second Impact Syndrome– Head trauma during occurring during the initial healing process
• Commonly seen in adolescents
– Cerebral swelling causing vascular engorgement leads to increased intracranial pressure and can cause brain herniation leading to soft tissue death of brain matter
– Can also cause subdural hematoma• Morbidity level 95%
• Post-Concussive Syndrome– Typically (in 80-90% of cases) symptoms resolve in 7-10 days with the
proper care and guidelines about return to play, but in some instances the symptoms are prolonged and last beyond the natural recovery period.
– The onset of this syndrome can be due to previous concussions, excessive stimulus during the recovery stage, recurrent trauma during recovery stage, inadequate rest during recovery stage.
Concussion Risk Reduction Programming5,25-27
• Some correlation to weakness of neck musculature and posterior chain musculature to risk of concussion, but no strong current evidence. – Consistent use of helmets to prevent skull injury– Helmets need to be able to protect from impacts resulting in a head
change in velocity of up to 10 m/s in
• Eliminate body checking in ice hockey, and also eliminating forceful and aggressive actions in football/soccer/basketball.
• Educate athlete on importance of reporting all instances of dizziness, grogginess, and headaches during the game to prevent serious injury.
• Pre-season education provided to athletes in regard to the expectations and consequences of concussion, as well as the procedure they will go through and the return to play protocol.
References1. Mccrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th International
Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. 2013;47(5):250-8.2. Zurich Concussion Conference. [PowerPoint]. 4th International Conference on Concussion in Sport held in
Zurich; November 2012. 3. Centers for Disease Control and Prevention. Nonfatal Traumatic Brain Injuries Related to Sports and Recreation
Activities Among Persons Aged ≤19 Years — United States, 2001–2009. MMWR 2011; 60(39):1337–1342.4. Signoretti; Lazzarino; Tavazzi; Vagnozzi. The Pathophysiology of Concussion. American Academy of Physical
Medicine and Rehabilitation. Vol. 3, October 2011.5. Todd Arnold. SCS Prep Course – Concussion in Sport. Medbridge. Accessed 09/22/2015. 6. Smith D, Hoogenboom B. Emergency care basics for the sports physical therapist. International Journal of Sports
Physical Therapy. 2011; 6(1): 59-62. 7. Broglio SP., et al. National Athletic Trainers’ Association Position Statement: Management of Sport Concussion.
Journal of Athletic Training. 2014; 49(2): 245-265.8. Mucha, Anne. Concussion Management Fact Sheet.. American Physical Therapy Association, Section of
Neurology. 9. Stewart GW, Mcqueen-borden E, Bell RA, Barr T, Juengling J. Comprehensive assessment and management of
athletes with sport concussion. Int J Sports Phys Ther. 2012;7(4):433-47.10. SCAT3. Br J Sports Med. 2013;47(5):259.11. Galetta; Brandes; et al. The King-Devick and sports-related concussion: Study of a rapid visual screening tool in a
collegiate cohort. Journal of the Nuerological Sciences (2011). 12. Eckner JT, Kutcher JS, Broglio SP, Richardson JK. Effect of sport-related concussion on clinically measured simple
reaction time. Br J Sports Med. 2014;48(2):112-8.13. Lovell, Mark. ImPACT: An Evidenced-Based and Comprehensive Concussion Management Program. ImPACT
Research Report, 2015.
References14. Giza, C.C., et al. (2013). Summary of evidence-based guideline update: evaluation and management of
concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology, Jun.; 80(24):2250-7. doi: 10.1212/WNL.0b013e31828d57dd.
15. Reynolds, E., Collins, M.W., Mucha, A., et al. (2014). Establishing a clinical service for the management of sports-related concussion. Neurosurgery, Oct; 75 Suppl. 74(4), 571-580.
16. Littleton, Ashley; Guskiewics, Kevin. Current concepts in sport concussion management: A multifaceted approach. Journal of Sport and Health Science, 2013.
17. Willer, Barry; Leddy, John. Management of Concussion and Post-Concussion Syndrome. Psychiatric Manifestations of Neurologic Disease.
18. Post-Concussion Syndrome Management Guidelines. Fowler Kennedy; St. Joseph’s Health Care. 19. Mucha A. et al. A Brief Vestibular / Ocular Motor Screening (VOMS) Assessment to Evaluate Concussions:
Preliminary Findings. American Journal of Sports Medicine. 2014; 42(10): 2479-2486.20. Pollock ML, Bohannon RL, Cooper KH, et al. A comparative analysis of four protocols for maximal treadmill
stress testing. Am Heart J. 1976;92(1):39-46.21. Johnston, Brian. [PowerPoint] Concussion in 2014. An update and review of current research and
recommendations. 22. Leddy JJ, Sandhu H, Sodhi V, Baker JG, Willer B. Rehabilitation of Concussion and Post-concussion Syndrome.
Sports Health. 2012;4(2):147-54.23. Kent, Janet. Post-Concussive Syndrome. South Short Hospital.24. Bey T, Ostick B. Second impact syndrome. West J Emerg Med. 2009;10(1):6-10.25. Benson BW, Mcintosh AS, Maddocks D, Herring SA, Raftery M, Dvorák J. What are the most effective risk-
reduction strategies in sport concussion?. Br J Sports Med. 2013;47(5):321-6.26. Collins CL, Fletcher EN, Fields SK, et al. Neck strength: a protective factor reducing risk for concussion in high
school sports. J Prim Prev. 2014;35(5):309-19.27. Committee on Sports-Related Concussions in Youth; Board on Children, Youth, and Families; Institute of
Medicine; National Research Council; Graham R, Rivara FP, Ford MA, et al., editors. Sports-Related Concussions in Youth: Improving the Science, Changing the Culture. Washington (DC): National Academies Press (US); 2014 Feb 4. 6, Protection and Prevention Strategies. Available from: http://www.ncbi.nlm.nih.gov/books/NBK185338/.