Embed Size (px)
Citation preview
Comparison of Recurrence Rates AfterDirect-Current Cardioversion for New-
Onset Atrial Fibrillation in PatientsReceiving Versus Those Not Receiving
Rhythm-Control Drug TherapyHuagui Li, MD, PhD, Roger Riedel, MD, J. Bradley Oldemeyer, MD, Karen Rovang, MD,
and Tom Hee, MD
The AFFIRM investigators have recommended rate controlas the preferred strategy for recurrent atrial fibrillation(AF), but the appropriate strategy for new-onset persistentAF is uncertain. Our study evaluated the AF recurrence rateand the impact of rhythm-control drugs (class 1A, 1C, and3 antiarrhythmic drugs) on patients with new-onset persis-tent AF after successful direct-current (DC) cardioversion.Consecutive patients who underwent DC cardioversion ofAF from January 1, 1996 to December 31, 1999 werescreened for new-onset persistent AF, and 150 patientsmet the inclusion criteria. After the first DC cardioversion,50 patients received rhythm-control drugs (rhythm-controlgroup) and the other 100 did not (rate-control group). The2 groups had similar clinical characteristics except for alower ejection fraction (44 � 14% vs 49 � 14%, p <0.01)and a higher proportion of idiopathic dilated cardiomyop-athy (20% vs 1%, p � 0.03) in the rhythm-control groupversus the rate-control group. During the follow-up period
there was a trend toward a lower rate of early AF recur-rence at 24 hours after DC cardioversion in the rhythm-control group versus the rate-control group (6% vs 16%, p� 0.11), but there was a high recurrence rate of AF in bothgroups at 1 month (30% for the rhythm-control group vs41% for the rate-control group, p � 0.25). At the end of thefollow-up period, rhythm-control therapy was abandonedin 78% of the rhythm-control group patients after the fail-ure of 1 to 3 rhythm-control drugs. In the rate-controlgroup, rhythm-control therapy was attempted after AFrecurrence in 62 patients but was later abandoned in 48patients (77%) because of treatment failure. Therefore, thehigh incidence of treatment failure with rhythm-controltherapy suggests that rate control with anticoagulationshould be preferred in patients with new-onset persistentAF if AF recurs after DC cardioversion. �2003 by Ex-cerpta Medica, Inc.
(Am J Cardiol 2004;93:45–48)
Recent randomized trial results have suggested thatin patients with recurrent atrial fibrillation (AF),
ventricular rate control plus anticoagulation may bethe preferred initial strategy.1,2 In patients with new-onset AF, the optimal therapeutic strategy has notbeen systematically studied. It is generally acceptedthat new-onset paroxysmal AF may not need antiar-rhythmic drug prophylaxis because AF recurrencemay not be predictable. For patients with new-onsetpersistent AF that requires direct-current (DC) cardio-version, the AF recurrence rate is unknown. Further-more, recurrent AF may require repeat DC cardiover-sion that may involve hospitalization andtransesophageal echocardiography. Previous studiesof antiarrhythmic drug therapy after DC cardioversionof AF included heterogenous patients and did notspecifically address the subgroup of patients withnew-onset AF.3–6 Therefore, our study focused on the
AF recurrence rate and the impact of antiarrhythmicdrug prophylaxis in patients with new-onset persistentAF after DC cardioversion.
METHODSNew-onset persistent AF was defined as AF with
duration of �72 hours and absence of a history of AF.The study patients were identified from the databaseof DC cardioversion in our center from January 1,1996 to December 31, 1999. Only the medical recordsof patients who underwent the first DC cardioversionduring the study period were selected. Patients withany of the these were excluded: (1) history of previousparoxysmal AF, (2) DC cardioversion �1 month aftera cardiac surgery, (3) AF duration �72 hours, (4) AFthat occurred after hospital admission for other med-ical reasons, (5) AF with identified reversible etiolo-gies, and (6) unsuccessful DC cardioversion (definedas failure to terminate AF with electrical shocks at themaximal output of the defibrillator). Immediate recur-rence of AF after the electrical shock was consideredearly AF recurrence and was included in the finalanalysis. Patients with AF who were converted tosinus rhythm pharmacologically were automaticallyexcluded.
From The Cardiac Center of Creighton University, Omaha, Nebraska.Manuscript received June 27, 2003; revised manuscript received andaccepted September 4, 2003.
Address for reprints: Huagui Li, MD, PhD, The Cardiac Center ofCreighton University, 3006 Webster Street, Omaha, Nebraska68131. E-mail: [email protected].
45©2003 by Excerpta Medica, Inc. All rights reserved. 0002-9149/04/$–see front matterThe American Journal of Cardiology Vol. 93 January 1, 2004 doi:10.1016/j.amjcard.2003.09.010

Patients: The study patients were divided into 2groups based on the use of rhythm-control drugs (de-fined as any of the class 1A, 1C, or 3 antiarrhythmicdrugs). The rhythm-control group included patientswho received rhythm-control drugs after the first DCcardioversion and the rate-control group included pa-tients who did not. Patients who did not initiallyreceive a rhythm-control drug after the first cardiover-sion but later had AF recurrence and received rhythm-control drugs after repeat DC cardioversion remainedin the rate-control group. The use of a rhythm-controldrug was at the discretion of the attending cardiolo-gists and was not randomized. Selection of a specificrhythm-control drug for each patient was mainlybased on the left ventricular ejection fraction (class 1drugs were not used if the ejection fraction was�40%). All patients treated with rhythm-controldrugs started the drug at least 1 day before DC car-dioversion. Only 1 rhythm-control drug was used at atime, with no patient receiving combined rhythm-control drugs.
All patients with risk factors for thromboembolismwere treated with warfarin with a targeted interna-tional normalized ratio of 2.0 to 3.0 for �3 weeksbefore the scheduled cardioversion. Transesophagealechocardiography was performed to rule out intra-atrial thrombus if the patient received warfarin for �3weeks or if the international normalized ratio was�2.0 at the time of the scheduled cardioversion. An-ticoagulation was continued for at least 1 month inpatients without AF recurrence and indefinitely inpatients with recurrent AF.
The primary end point of the study was the firstrecurrence of AF after the DC cardioversion. After theDC cardioversion, patients were followed in the outpa-tient clinic by 1 of the cardiologists at our center every 3to 6 months. For patients who died or were lost tofollow-up, data collection was up to the time of the lastclinic visit before the death or loss of follow-up.
Statistical analysis: Continuous data are presentedas mean � SD. Student’s t test was used to comparethe difference of means between the groups. Chi-square and Fisher’s exact tests were used to compareincidence rates between the groups. A p value �0.05was considered statistically significant.
RESULTSOne hundred fifty patients met study inclusion
criteria (50 in the rhythm-control group and 100 in therate-control group). The clinical characteristics of the2 groups of patients were comparable, except therewas a lower left ventricular ejection fraction andhigher proportion of patients with idiopathic dilatedcardiomyopathy in the rhythm-control group than inthe rate-control group (Table 1). The duration of AFranged from 72 hours to 6 months (median 3 months)and was not significantly different between the 2groups (p �0.05). All patients had symptoms duringAF that ranged from palpitation or fatigue to chestpain or dyspnea, but no patient had pulmonary edemaor hypotension. The use of initial antiarrhythmic drugsafter DC cardioversion is listed in Table 2. The use of
� blockers was not significantly different between the2 groups (52% vs 54%, p �0.05) if sotalol is consid-ered as a � blocker.
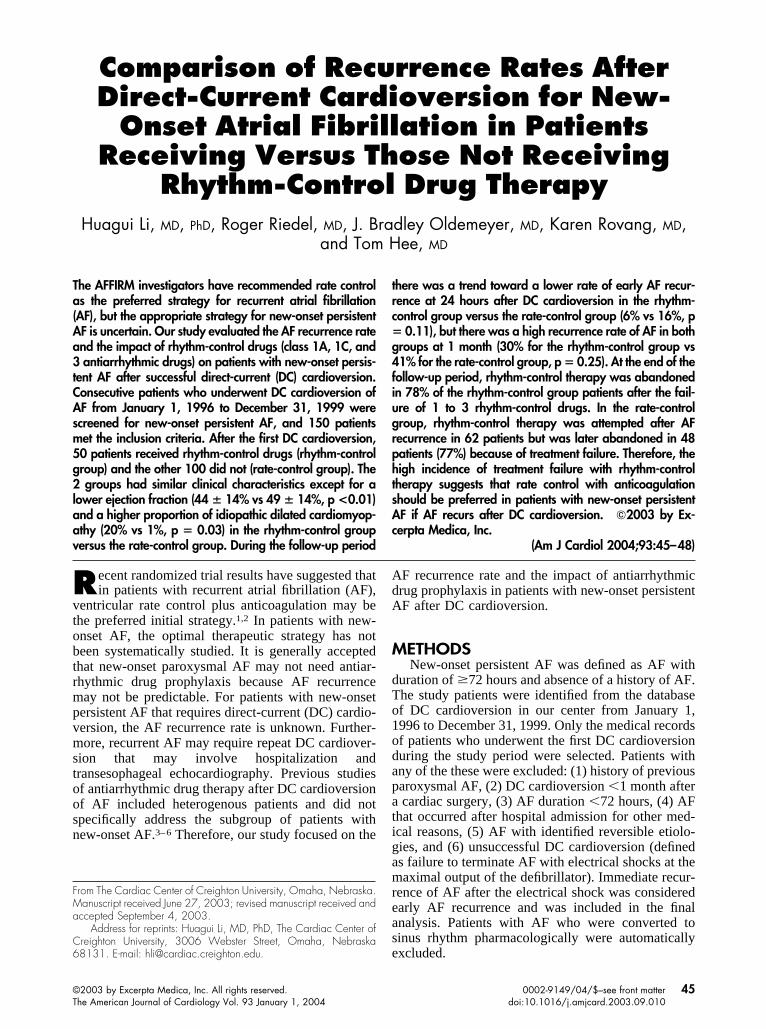
Mean follow-up duration was 20 � 15 months forthe rhythm-control group and 17 � 1 months for therate-control group (p �0.05). Two (4%) and 4 patients(4%) were lost to follow-up in the rhythm-control andrate-control groups, respectively (p �0.05). The firstAF recurrence after DC cardioversion is depicted inFigure 1. Although statistically the rhythm-controlgroup had a lower recurrence rate than the rate-controlgroup, the overall AF recurrence was very high inboth groups. At 24 hours after the DC cardioversion,there was a trend toward a lower incidence of early AFrecurrence in the rhythm-control group than in therate-control group (6% vs 16%, p � 0.11). At 1month, there was a clinically impressive recurrence ofAF in both groups (30% for the rhythm-control groupvs 41% for the rate-control group, p � 0.25). Thestatistical difference in AF recurrence between the 2groups became apparent at 6 months. The curve of AFrecurrence-free survival continued to drop during thefollow-up period in both groups. Of the patients in therhythm-control group with a follow-up duration of upto 48 months, about 20% were free of AF recurrence.
In the rate-control group, the rhythm-control strat-
TABLE 1 Clinical Characteristics of the Rhythm-control andRate-control Group
Rhythm-controlGroup
Rate-controlGroup
(n � 50) (n � 100)
Age (yrs) 69.4 � 11.2 71.3 � 11.2Men/women 35/15 64/36Coronary artery disease 15 (30%) 45 (45%)Hypertension 26 (52%) 51 (51%)Idiopathic dilated cardiomyopathy 10 (20%) 1 (1%)*Valvular disease 10 (20%) 19 (19%)Diabetes mellitus 12 (24%) 17 (17%)Left atrial size (mm) 45.5 � 6.9 45.9 � 7.2Left ventricular EF (%) 44.1 � 14.2 49.3 � 13.6†
*p �0.01; †p � 0.03.EF � ejection fraction.
TABLE 2 Comparison of Antiarrhythmic Drug Use After theFirst Direct-current (DC) Cardioversion
Drug
Rhythm-controlGroup
Rate-controlGroup
(n � 50) (n � 100)
Digoxin 26 (52%) 45 (45%)Regular � blocker 15 (30%) 54 (54%)*Calcium blocker† 8 (16%) 20 (20%)Amiodarone 18 (36%) 0Propafenone 15 (30%) 0Sotalol 11 (24%) 0Procainamide 2 (4%) 0Disopyramide 2 (4%) 0Qunidine 1 (2%) 0Flecainide 1 (2%) 0
*p �0.01.†Calcium blocker refers to only verapamil or diltiazem in this study.
46 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 93 JANUARY 1, 2004
egy was abandoned due to treatment failure (AF re-currence [15], intolerable side effects [3]) in 18 pa-tients (18 of 50 [36%]) after the first trial with arhythm-control drug. These patients subsequently re-mained in permanent AF and were treated with ratecontrol. The rhythm-control drug was abandoned dueto treatment failure (AF recurrence [10], intolerableside effects [2]) in another 12 patients (12 of 50[24%]) after a second drug trial. The rhythm-controldrug was abandoned in another 7 patients (7 of 50[14%]) after failure of a third drug trial (all due to AFrecurrence). At the end of the follow-up, only 9 pa-tients (18%) continued to receive a rhythm-controldrug (amiodarone [5], sotalol [2], flecainide [1],propafenone [1]) and were in sinus rhythm.
In the rate-control group, 38 patients never re-ceived any rhythm-control drug and 6 of them (6 of 38[27%]) had no AF recurrence. The other 62 patientsdid not receive a rhythm-control drug after the firstDC cardioversion but later received trials of 1 to 3rhythm-control drugs because of AF recurrence. Thir-ty-five patients tried 1 rhythm-control drug and 25 (25of 35 [71%]) abandoned the therapy due to drugfailure (AF recurrence [20], intolerable side effects[5]). Twenty-two patients tried 2 rhythm-control drugsand 18 (18 of 22 [82%]) abandoned the therapy due todrug failure (AF recurrence [16], intolerable side ef-fects [2]). Five patients tried 3 rhythm-control drugsand all abandoned the therapy due to drug failure (AFrecurrence [4], intolerable side effects [1]). At the endof the follow-up, only 20 patients (20%) remained insinus rhythm, 14 were receiving rhythm-control drugs(amiodarone [8], sotalol [3], propafenone [2], flecain-ide [1]), and 6 were not.
Amiodarone was used in 72% of patients (36 of 50)in the rhythm-control group and in 65% of patients (40of 62, p �0.05) in the rate-control group. The all-cause mortality was not significantly different be-tween the 2 groups during the follow-up period (8%for the rhythm-control group [n � 4] vs 7% for therate-control group [n � 7], p �0.05). The cause ofdeath was cardiac in 2 and 4 patients in the rhythm-control and rate-control groups, respectively (p
�0.05). Cardiac death occurred while receiving arhythm-control drug for 1 of 2 patients in the rhythm-control group and for 3 of 4 patients in the rate-controlgroup. Because of the retrospective nature of ourstudy, we could not further differentiate sudden fromnonsudden cardiac death. More patients in the rhythm-control group received permanent pacemaker implan-tation than in the rate-control group (10% [n � 5] vs2% [n � 2], p � 0.03).
DISCUSSIONNew-onset persistent AF accounts for a sizable
portion of the AF population (about 25% of patientswho underwent DC cardioversion of AF at our insti-tution, unpublished data) and its appropriate manage-ment strategy remains uncertain. Our study focused onsuch a subgroup of patients with AF and demonstrateda high recurrence rate of AF similar to that of patientswith recurrent AF.7 Such a high AF recurrence ratemay be due to a few reasons. First, when an AFepisode persisted and did not convert spontaneously,underlying electrophysiologic abnormalities werelikely present. Second, although every effort wasmade to exclude patients with a history of AF, some ofour patients may have had asymptomatic paroxysmalAF before they presented for DC cardioversion ofpersistent AF. Therefore, these patients would have asimilar natural history as those with recurrent AF.Third, because patients with pharmacologic conver-sion were excluded, those who required DC cardio-version may automatically indicate difficult cases withhigh recurrence rates.
The outcome of the rhythm-control group patientsdemonstrates that the use of a rhythm-control drugmay statistically reduce the early recurrence rate ofAF after DC cardioversion. This was the case, al-though the rhythm-control drugs were prescribed topatients who were predicted to have a high probabilityof AF recurrence, as demonstrated by the fact that therhythm-control group patients had a lower ejectionfraction and higher proportion of idiopathic dilatedcardiomyopathy. This observation is consistent withprevious studies.3–6 However, the impact of rhythm-control drugs on AF recurrence was relatively time-limited. AF recurrence continued to increase in pa-tients receiving rhythm-control drugs during thefollow-up period. By 24 months, the AF recurrence-free survival rate was �40%. Therefore, it appearsthat the use of a rhythm-control drug after DC cardio-version serves to delay the recurrence of AF for about6 to 12 months.
The outcome of the rate-control group patients showsthat a few patients were free of AF recurrence without arhythm-control drug after DC cardioversion, suggestingthat 1 attempt of DC cardioversion may be beneficial atleast in a small number of patients. However, patientswho undergo initiation of a rhythm-control drug withrepeat cardioversion at the time of AF recurrence appar-ently have the same challenge as the rhythm-controlgroup patients. Again, even if a rhythm-control drug wasadded, AF recurrence continued to increase during thefollow-up period. Furthermore, failure with 1 drug ap-
FIGURE 1. Kaplan-Meier curve AF recurrence-free survival in the2 groups of patients is shown.
ARRHYTHMIAS AND CONDUCTION DISTURBANCES/ RHYTHM CONTROL FOR NEW-ONSET PERSISTENT AF 47

parently was associated with an increased failure ratewith another drug. There appeared to be little chance ofmaintaining sinus rhythm in a patient in whom 2 drugshave failed.
Our study indicates that the management strategyshould be planned before DC cardioversion in patientswith new-onset persistent AF. Our results are consistentwith previous reports that the efficacy of rhythm-controldrugs on prevention of AF recurrence is limited1,2 andcontinued search for better therapy (pharmacologic andnonpharmacologic) of AF is needed. The rate-controlstrategy seems to be a reasonable option for many pa-tients with new-onset persistent AF that requires DCcardioversion. DC cardioversion without a rhythm-con-trol drug may be attempted once. If AF recurs, therate-control strategy may be preferred over repeat car-dioversion with the addition of a rhythm-control drug.As an alternative, a curative therapy such as catheterablation may be offered to patients with severe AFsymptoms and few risk factors for stroke.
1. The Atrial Fibrillation Follow-up Investigation of Rhythm Management(AFFIRM) Investigators. A Comparison of rate control and rhythm control inpatients with atrial fibrillation. N Engl J Med 2002;347:1825–1833.2. Van Gelder IC, Hagens VE, Bosker HA, Kingma JH, Kamp O, Kingma T,Said SA, Darmanata JI, Timmermans AJM, Tijssen JGP, Crijns JGM, for theRate Control versus Electrical Cardioversion for Perisistent Atrial FibrillationStudy Group. A comparison of rate control and rhythm control in patientswith recurrent persistent atrial fibrillation. N Engl J Med 2002;347:1834 –1840.3. Van Gelder IC, Crijns HJGM, van Gilst WH, van Wijk LM, Hamer HPM, LieKI. Efficacy and safety of flecainide acetate in the maintenance of sinus rhythmafter electrical cardioversion of chronic atrial fibrillation or atrial flutter. Am JCardiol 1989;64:1317–1321.4. Juul-Moller S, Edvardsson N, Rehnqvist-Ahlberg N. Sotalol versus quinidinefor maintenance of sinus rhythm after direct current conversion of atrial fibrilla-tion. Circulation 1990;82:1932–1939.5. Gosselink ATM, Crijns HJGM, van Gelder IC, Hillige H, Wiesfeld ACP, LieKI. Low-dose amiodarone for maintenance of sinus rhythm after cardioversion ofatrial fibrillation or flutter. JAMA 1992;267:3289–3293.6. Stroobandt R, Stiels B, Hoebrechts R, on behalf of the Propafenone AtrialFibrillation Trial Investigators. Propafenone for conversion and prophylaxis ofatrial fibrillation. Am J Cardiol 1997;79:418–423.7. Van Gelder IC, Crijns HJ, Tieleman RG, Brugemann J, De Kam PJ, GosselinkAT, Verheugt FW, Lie KI. Chronic atrial fibrillation. Success of serial cardio-version therapy and safety of oral anticoagulation. Ann Intern Med 1996;156:2585–2592.
48 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 93 JANUARY 1, 2004









![Rate versus rhythm control in atrial fibrillation and ... · maintaining sinus rhythm with electrical cardioversion and/or antiarrhythmic agents) [5]. Rhythm control mainte-nance](https://img.dokumen.tips/doc/110x75/5f3fa535a6a94664fc482e5c/rate-versus-rhythm-control-in-atrial-fibrillation-and-maintaining-sinus-rhythm.jpg)



















