Embed Size (px)
Citation preview

COMPARISON OF BONE REGENERATION IN THE EXTRACTION SOCKETS WITH
AUTOLOGOUS PLATELET RICH FIBRIN GEL- AN IN VIVO STUDY
Dissertation submitted to
The Tamil Nadu Dr. M.G.R. Medical University
In partial fulfilment of the degree of
MASTER OF DENTAL SURGERY
BRANCH III
ORAL AND MAXILLOFACIAL SURGERY
2013-2016


ACKNOWLEDGEMENT
I extend my sincere and heartfelt gratitude to my teacher Dr. Mathew
Jose, Prof and HOD, under his able guidance and encouragement, I had the
opportunity of being taught and explained the surgical techniques, tips and
tricks of being an efficient surgeon. Vast experience of him has attributed in
unwinding the complex nature of many questions that took me through different
but difficult situation in my post graduate studies. I could not have asked for a
better mentor or guide for my post graduate studies.
I thank Dr. Dhineksh Kumar for the able guidance and support he has
provided me during the research and also post graduate studies. He with his
friendly talks, critical questions and sometimes being strict has made sure that I
am travelling in correct path of being a good surgeon. Best part of him always
approachable and ready to share the vast knowledge and experience he has
acquired in years.
I take this opportunity to thank our principal Dr. Elizabeth Koshi for
her help, support & patient guidance for finishing this work on the time bound
limits.
I express my sincere gratitude to my teacher Dr. Sajesh continually and
persuasively conveyed a spirit of adventure in regard to research and
scholarships, and an excitement in regards to teaching. He has always supported
me and his helpful nature has one of been the driving force for the fulfillment
of my research work.
I extend my deepest gratitude and thanks to Dr. Jomy Varghese who
has always been a great teacher and for us. He has taught us to have the right
kind of attitude a fellow surgeon need to have, he has tried to mold us into a
well behaved and classy professional with etiquette and moral and ethical
responsibilities.
I am indebted to my teacher Dr. Achuthan Nair who has tried to bring
the best out of me. He has motivated me to a mass knowledge and taught us
how learning process could be an enjoyable moments. He has been one of the
serious critics of my post graduate studies.
I extend my sincere thanks to Dr.Nandagopan for his contributions in
my thesis work. His humbleness and dedication to profession coupled with
tremendous skill had always been a fascination to me.
I am highly obliged Dr.Rajeev for being there always to clear my
doubts and guide me through the right path.
I would like to thank Dr. Murugan for supporting me through the hard
times and motivating me to study harder.
I would like to thank my super seniors Dr.Sivalinga Raja and Dr.Deepu
for teaching me the intimate skills of surgery.
I would like to thank my seniors Dr.Prem Anand and Dr.Thinakar
Babu for timely support and guidance.

I would like to thank my juniors Dr.Swaminathan, Dr.Shameem Jamal,
Dr.Harinee and Dr.Abirami for the support and enjoyable moments we had
during the post graduate life.
Above all I thank Almighty God, My parents Mr.A.Wilson and Mrs.A.Jansi
and my wife Dr.S.Shani Carmela for walking with me in each and every step of my
life and making this study to successful one.
SPECIAL ACKNOWLEDGEMENT
I take this opportunity to thank our chairman Dr.C.K.Velayudhan Nair
MS & Dr.Rema.V.Nair MD Director, Sree Mookambika Institute Of Dental
Sciences, Kulasekharam, TamilNadu for giving me an opportunity to utilize
the facilities available in this institution for conducting this study.

CONTENTS
SI.NO INDEX PAGE NO.
1 List of Abbreviations i
2 List of Tables ii
3 List of Graphs iii
4 List of Figures iv
5 Abstract v-vi
6 Introduction 1-5
7 Aims and Objectives 6
8 Review of literature 7-20
9 Platelet Rich Fibrin 21-22
10 Materials and Methods 23-33
11 Figures vii-xi
12 Results 34-36
13 Tables and Graphs 37-45
14 Discussion 46-52
15 Summary and Conclusion 53-54
16 Bibliography
17 Annexures
LISTS OF ABBREVIATIONS
PRF- Platelet Rich Fibrin
PRP- Platelet Rich Plasma
PPP- Platelet Poor Plasma
PDGF- Platelet Derived Growth Factor
TGF- Transforming Growth Factor
IGF- Insulin Derived Growth Factor
PDWHF- Platelet Derived Wound Healing Factor
AFA- Autologous Fibrin Adhesive
BMP- Bone Morphogenic Protein
bFGF- basic Fibroblast Growth Factor
EGF- Epidermal Growth Factor
PRGF- Platelet Rich Growth Factor
NBR- Natural Bone Regeneration
NTR- Natural Tissue Regeneration.
i
LISTS OF TABLES
Table 1 Demographic data of study population
Table 2 Mean bone density values of different groups at different post operative
periods
Table 3 Comparison of mean bone density values immediate between the
groups
Table 4 Comparison of mean bone density values 1 month between the groups
Table 5 Comparison of mean bone density values 3 month between the groups
Table 6 Comparison of mean bone density values 6 month between the groups
Table 7 Comparison of mean bone density values between the groups at
different time periods
Table 8 Comparison of mean bone density values within the groups at
immediate
Table 9 Comparison of mean bone density values within the groups at 1month
Table 10 Comparison of mean bone density values within the groups at 3 month
Table 11 Comparison of mean bone density values within the groups at 6 month
Table 12 Multiple comparison of mean bone density values within the groups at
different time periods
ii

LISTS OF GRAPHS
Graph 1
Demographic data of study population
Graph 2
Comparison of mean bone density values between the groups at
different time periods
Graph 3
Multiple comparison of mean bone density values within the
groups at different time periods
iii
LISTS OF FIGURES
Figure 1 Armamentarium for the preparation of platelet rich fibrin
Figure 2 Medico centrifuge
Figure 3 Withdrawal of blood
Figure 4 After centrifugation
Figure 5 Platelet rich fibrin gel
Figure 6 Extracted socket
Figure 7 Suture done after platelet rich fibrin placed in the extraction
socket
Figure 8 Grey level histogram value evaluation from Intraoral Periapical
radiograph
Figure 9 Intraoral periapical radiograph of postoperative periods
iv

Introduction
Page 1
Maxillofacial reconstruction, regenerative procedures and oral implants
etc. are depends on successful healing and regeneration . According to the clinical
research it is the most greatest challenge faced in development of bioactive surgical
additives which regulates inflammation and healing is increased. To improve the
quality of bone in Bone regenerative procedures graft materials, protein and barrier
membrane are mostly used. Tissue healing is mediated by variety of signalling
proteins. Platelets plays a vital role in wound healing.16
Repairing the bony tissue is a complex process which involves
mineralization of the defect and a number of cellular functions which is followed by
an inevitable remodelling the defects to achieve original structure1. In the platelet gel
therapeutic concept Platelet-rich fibrin (PRF) represents a new step with lacking of
artificial biochemical modification in a simplified process. 2 The platelet derived
growth factors are released abundantly by platelet concentrate which are essential
regulators for survival of mesenchymal cell lineages, migration and proliferation.3
Platelet concentrates used as the tools of regenerative medicine which is
specially designed for the local release of platelet growth factors into a wounded or
surgical site, in order to regeneration or stimulate tissue healing. Platelets are rich in
protein molecules like cytoskeleton regulatory proteins, signalling, cytokines,
membrane proteins, and other bioactive peptides which plays an essential role not
only in hemostasis but also in regulating and initiating which is the basic aspect in
wound healing.4 One of the greatest challenge in clinical research is the development
of bioactive surgical additives in regulating, enhancing healing and regeneration of
Introduction
Page 2
bone and tissues.5 Combination PRF along with fat grafts is more effective in
lipostructure surgery. 13
Platelet rich plasma (PRP), is the first generation autologous platelet
concentrate. The PRP is prepared by adding citrate to whole blood which binds the
ionized calcium and inhibit the clotting cascade. This is followed by two steps of
centrifugation in which the first step separates the white and red blood cells from
platelets and plasma and in the second step of centrifugation it further concentrates
the platelets and ultimately produces the PRP separate from poor plasma and platelet.
But the real efficacy of PRP is debatable. It is hypothesized that, just before the cell
outgrowth from the surrounding tissue, PRP releases growth factors quickly.
Platelet rich fibrin (PRF), is a second generation platelet concentrate is
a elementary process which represents a original measures in therapeutic concept and
absence of artificial biochemical modification such as the use of bovine thrombin6.
PRF is prepared by the immediate centrifugation of whole blood without any
anticoagulant with the formation of three biological phases like a bottom layer
consists of coagulated red cell, a elastic and rigid PRF gel as intermediate layer and a
supernatant serum. During centrifugation a rapid activation of coagulation cascade
and synthesis of thrombin take place this results in inducing the fibrin formation and
the platelet activation. The essential point of PRF synthesis is to accumulate platelets
and release the cytokines in a fibrin clot recompense by a natural polymerization
process during the centrifugation with release of growth factors and matrix
glycoproteins for more than 7 days.7
Introduction
Page 3
Recently, the platelet concentrates has suggested that it is an aid for
epithelial tissues and osseous regeneration in oral surgery.24 In 1974 the platelets
regenerative potential which shows better result in regenerative dentistry by Ross
et al.25
Platelet rich plasma is derived from concentrated human platelets which
is taken from plasma which have been explained to induce healing. PRF along bovine
porous it is a bone mineral which promotes bone regeneration during periodontal
defects.23
The process of wound healing is a complex mechanism which is
characterized by four phases; hemostasis, inflammation, proliferation and
remodelling they are coordinated by cell-cell interactions and by a soluble growth
factors which is released by various types of cells. The Platelets includes high
concentration of different types of growth factors with relatively low molecular
weight ranging from 6 to 45 kDa in their alpha granules which is extremely important
in regenerative process and the platelet cell membranes also play a important role in
wound healing through their growth factor receptor sites. The PRF have anti-
infectious activities.8 The platelet poor plasma have growth cells helpful to induce
differentiation of periodontal ligament and osteoblast mainly for periodontal
regeneration and bone regeneration.47 PRF shows more advantages such as surgical
time is less, good healing properties, few techniques elimination, resorption is very
less in healing.10

Introduction
Page 4
The production protocol of PRF clot and membrane often varies in
different literature. Choukroun et al2 advocated 3000 RPM for 10 minutes while kiran
et al 20119 used 2700 RPM for 12 minutes. Platelets plays an important role in
process of wound healing because platelets contain many growth factors like Insulin-
like Growth factor(IGF), platelet derived growth factors (PDGF) and also
transforming growth factor-ß (TGF-ß) which when secreted are responsible for
increasing cell mitosis, collagen production, initiating vascular in-growth and it
induce cell differentiation12. In degree of grade II furcation PRF plays important role
in healing.11
Fibrin matrix of PRF is elastic, flexible and very strong. Which consists
of weak thrombin which require equilateral junction. These junctions are connected
and permits the establishment of flexible and fine network which is capable of
supporting cellular migration and cytokines results in the increase of life spans of
cytokines. The concentration of platelet and growth factors differs in distinct
preparation protocol like disparity of tubes, gel inducing enzyme and centrifugation
force30. The topical application of PRF helpful for epithelialisation in donar site and
autografts of meshed-split thickness graft.48
A platelet proteome project reveals that more than 300 proteins which is
released by human platelets are responsible for thrombin activation and 190
membrane-associated, 262 phosphorylated proteins when identified via independent

Introduction
Page 5
proteomic and phosphoproteomic profiling.14 A progressive slow polymerization
mode may raised incorporation of circulating cytokines in fibrin meshes are released
in a relatively long-term and controllable way which helpful in soft tissue healing and
accelerates bone regeneration.15
This prospective clinical trail is designed to compare bone regeneration
with autologus platelet rich fibrin in bilateral extraction socket.

Aims & Objectives
Page 6
The aim of the study is to evaluate the comparison of bone regeneration in the
extraction socket with autologous platelet rich fibrin gel.

Review of Literature
Page 7
Matras et al 198517 described about fibrin glue which is derived from
blood product mainly used to stimulate healing and to seal wounds. It contains
concentrated fibrinogen polymerization induced by calcium and thrombin. By using
donar plasma it was prepared and used to improve skin wound healing in a rat model.
He who first described fibrin glue used as surgical adhesive which helpful for healing
process.
Knighton et al 198618 examined the efficacy of platelet derived
wound healing factors(PDWHF) which applied topically prepared with 2- step
centrifugation procedures. It was applied in 41 patients which left in place for 12
hours in 71 chronic non-healing cutaneous ulcers. He explained that PDWHF
stimulate chronically non-healing human wounds by granulation tissue formation and
epithelialization. There is no evidence of over healing like keloid formation or
hypertrophic scar.
Lynch et al 198719 suggested that at the site of injury platelet derived
growth factors (PDGF) plays an major role in the initiation of the wound healing
process.
Gibble et al 199020 found that fibrin glue is commercially available
products like beriplast, tisseel provided a consistent source of fibrinogen. The
preparation of fibrin glue contained aprotinin and bovine derived protease inhibitor
with anti-fibrinolytic activity.

Review of Literature
Page 8
Knighton et al 199021 in his study chronic non-healing wounds in 32
patients were treated with platelet-derived wound healing formula (PDWHF). This
study shows a statistically highly significant effect of topically applied PDWHF for
the repair of chronic non-healing ulcers with epithelialisation of the wound.
Tayapongsak et al 199422 introduced mandibular reconstruction
using autologous fibrin adhesive (AFA) is the novel idea of reconstructive options.
Slater et al 199527 conducted a study to examine the efficacity of
concentrated human platelet as a eked out to basic medium in the functional and
proliferative activity of human osteoblastic like cells. The results shows that eked out
platelet medium stimulates the proliferation and maintains the activity of
differentiated function of human fetal osteoblast like cells.
Heldin et al 199733 presented a report on intracellular signal
transduction pathways which involves PDGF induced cell motility and growth also
discussed the fact that the inhibitory stimulatory pathways are parallely induced. He
also reported that the PDGF exert their effect by the binding of two protein tyrosine
kinase receptor which is structurally related.
Whitman et al 199726 used “platelet gel” derived from platelet
concentrate produced by a gradient density cell separator shown their clinical results
in reconstruction of oral and maxillofacial surgery. The authors considered the platelet
gel as a fibrin glue helpful for mandibular reconstruction, alveolar cleft procedure,

Review of Literature
Page 9
closure of oro antral and oro nasal communication and also show greater effect in
implant placement.
Green et al 199834 reported that platelet gel was used as wound
sealant. The presence of leukocytes and platelets in the formulation of antimicrobial
and hemostatic support which bring the growth factors and cytokines to the surgical
site.
Marx et al 199828 first introduced platelet rich plasma in dental studies
clinically. The platelet rich plasma is used to improve the graft incorporation in the
mandibular reconstruction to the patients who have received cancellous bone marrow
grafts after the tumor removal. In their study it have been showed that PRP contains a
concentrated platelets and growth factors. The PRP which was used with grafts
showed a evidence of radiographic maturation rate 1.6 to 2.16 times faster than the
grafts which was used without PRP. This data suggested strongly that by adding PRP
to bony grafts accelerates the degree and rate of bone formation.
Anitua et al 199931 performed a study in 20 patients for whom
extraction was done and subsequent implant placement was done. A biopsy in that
area was obtained without any additional discomfort, macroscopically there was a
evident of epitheliazation microscopically the bone was compact and mature and well
organized trabeculae was evident with normal physiology.
Review of Literature
Page 10
Heldin et al 199932 reported that the first growth factor was the PDGF
which shows chemotactic for migration of cells in the healing skin wound like
fibrolast, monocytes and neutrophils. He also proved that PDGF enhances not only
the proliferation of fibroblast and extracellular matrix production but also it stimulates
the fibroblast to contract collagen matrices and also induces the myofibroblast
phenotype which suggest a major role in healing of wound. Also he demonstrated that
the series of clinical and experimental studies about the useful effect of PGDF which
can be used in wound healing disorders.
Schuldiner et al 200035 examined the ability of eight growth factors
such as basic fibroblast growth factor(bFGF), activin-A, bone morphogenic protein 4
( BMP-4), ), transforming growth factor ß1 (TGF-ß1), epidermal growth factor(EGF),
hepatocyte growth factor(HGF), b nerve growth factor (bNGF) and retinoic acid(RA).
Anitua E (2001)36 conducted various studies to see the effect of
platelet rich in growth factors (PRGF) and proved it is a conventional methods to
accelerates soft tissue and bone regeneration in post extraction sockets.
Man et al 200129 described a new technique by preparing autologous
fibrin glue and platelet gel. They examined the effective stopping of capillary
bleeding in surgical flaps for the patients undergoing cosmetic surgery. Their finding
showed both products have effect in maintaining hemostasis and sealing of capillary
bleeding.

Review of Literature
Page 11
Soffler et al 200338 suggested that the fibrin sealants may enhance
overall outcome of the surgical intervention due to adhesive, hemostatic and healing
properties.
Lacoste et al 200339 quantified that the concentration of TGF-ß1,
bFGF, VEGF and PDGF-BB from the platelet concentrates and the whole blood
before and after there is addition of various concentrations such as calcium and
thrombin and also have been assessed that physiological importance of growth
factors on angiogenesis.
Weibrich et al 200337 studied the level of growth factors in PRP by
dispersion of cell separation method and also point of care method. It is also called as
‘buffy coat method’. From 115 healthy donars whole blood was drawn . The
increase in thrombocyte count was obtained in both of the methods which results in
higher TGF-ß1 levels while increase in the leukocyte count in curasan PRP shows
more PDGF-AB levels.
Anitua et al 2004 40showed that the platelets contains the storage
pools of growth factors such as VEGF, TGF-ß and PDGF and cytokines which
includes proteins like PF4 and CD40L. He also reported that the growth factors
attached to the platelets and/ or fibrin which results in enhanced activity over the
recombinant proteins, also he reviewed the various situation in the muscle/tendon
repair, orthopaedic surgery, hole repair in the eye surgery , reversal of skin ulcers and
cosmetic surgery where platelet accelerates the healing mechanism.

Review of Literature
Page 12
Dohan et al 200641 quantified the level of cytokine within PRF clot
exudates serum and platelet poor plasma supernatant : IL-1b, IL-4 , IL-6,VEGF and
TNF-alpha that was obtained with in plasma and in serum. He proved that PRF
shows a complex tridemsional architecture it makes a real platelet and also a
leukocyte rich fibrin biomaterial.
Li et al 200642 explained the pleiotropic function of TGF-ß which
signalling in T cells. It shown that T cell specific deletion in mice with of TGF-ß
receptor II which developed lethal inflammation and it is associated with T Cell
activation and differentiation.
Thor et al 200743 calculated that effect of platelet rich plasma on the
early stage and late stage bone healing after maxillary sinus grafting. There was
significantly more new bone were formed at platelet rich plasma treated sites when
compared to control group in 3 months of healing. He suggest that platlet rich plasma
have low regenerative capacity which influenced the bone healing in the early phase.
Diss et al 20085 studied that the radiographic changes occurs in the
apical portion the bone levels on the microthreaded implants when it is placed in
subsinus residual bone height it is according to a bone added osteotome the sinus floor
elevation technique with PRF is used as grafting material in 20 patients.

Review of Literature
Page 13
Lundquist et al 200846 platelet rich fibrin gives a sustained release
and also protection against the proteolytic degradation of the endogenous fibrogenic
factors which is most important for wound healing.
Su et al 200844 analyzed that growth factors release from the platelet
gels from 10 volunteers where the whole blood was collected along with
anticoagulant citrate dextrose(ACD). The estimation of growth factor from platelet
gel with releasate, platelet gel, releasate with thrombin at 5 , 60, 120, 300 minute
time points. TGF-ß1, PDGF-AB, EGF and VEGF increase was identified in platelet
gel with releasate of the PDGF-AB of 0.6x10-16 and also the TGF-ß1 of 0.9x10-16 per
PLT.
Sunitha et al 200845 concluded that the combination of growth factors
and bone grafts contained in platelet rich fibrin and platelet rich plasma may be
suitable to increase bone density. In experimental study the content such as growth
factor in platelet rich fibrin and platelet rich plasma was measured by using Elisa Kit.
Dohan et al 20097 estimated the growth factors from PRF initial
serum exudates and which was gently flushed out. The membrane was placed in an
significant volume of the culture medium (4ml) which protect the cell integrity of
leukocytes in the clot. He display that when these membranes were prepared with in
the PRF Box, PDGF-AB amounts were significantly higher at each experimental
time and the TGF-1 and VEGF amounts were significantly higher during the first 4
hours.

Review of Literature
Page 14
Gassling et al 200916 generated PRF and PRP from the whole blood
samples in ten patients. Human fibroblasts, human osteoblasts and human osteoblast-
derived osteosarcome cells which were used for the cell culture and shown the growth
factors IGF-1and TGF-ß1 and ß2 ,PDGF-AB and BB found that the cytokine
concentration were higher for PRP and PRF in the osteoblasts and also in Saos-2
cultures.
Mazor et al 200950 used platelet-rich fibrin as a sole filling material
during sinus lift and implantation which is stabilized a high volume of regenerated
natural bone in subsinus cavity till the tip of implants. According to Choukroun’s
platelet rich fibrin is an simple and inexpensive biomaterial used during a sinus lift ,
particularly it will protect the schneiderian membrane.
Su et al 200949 observed that the amount of growrh factors into
supernatant serum (SS) and PRF releastate (PRFR) after the preparation of PRF.
Growth Factor release was determined for 300 minutes over total period of time. It
covers the maximum time which needed for surgical procedures and also higher
quantity of transforming growth factor (TGF)-1 and PDGF-AB was released. He
concluded that the PRFR and SS should be mixed along with bone grafts the use of
patients blood helpful for tissue regeneration.
Simonperi et al 200951 showed platelet rich fibrin membranes were
particularly helpful for healing and maturation of periosteum. Thus the thick Peri-
Review of Literature
Page 15
Implant in gingival region show the result of several healing phases of platelet rich
fibrin membrane layer.
Gassling et al 201054 platelet rich fibrin is superior to collagen(Bio-
Gide) used as a scaffold membrane for human periosteal cellular proliferation.
Periosteal cell cultivation in bone tissue engineering Platelet Rich Fibrin membranes
plays a major role.
Gurbuzer et al 201055 platelet rich fibrin force not lead to lift bone
healing in the soft tissue impaction of mandibular third molar removal sockets after
4 weeks of surgery.
Lucarelli et al 201052 evaluated the growth factors present in PRFM
in vitro and shown their ability to accelerates the growth of mesenchymal stem cells
plays a major role in tissue repair. There mechanical properties and also the platelet
distribution were evaluated. Platelets found to be localized in one side of membrane.
In the first day the kinetics of release were more for VEGF, and in bFGF more
gradual release was seen. The concentration of the PDGF-AA, PDGF-AB,
VEGF,TGF-ß1,bFGF, EGF in PRFM conditioned media were greater in a day 1
when compared to other days.
Senger et al 201053 showed that both bFGF and VEGF will stimulate
the endothelial proliferation and also angiogenesis but VEGF transcripts encode and
directs active secretion of VEGF from the cell, and it is considered to be the
Review of Literature
Page 16
endothelial specific mitogen. The VEGF stimulates nitric oxide production it will
inhibits platelet activation and suggesting that the role of VEGF is to prevent
undesirable thrombosis.
Ahmed et al 201156 described about the autocrine pool between FGF
and PDGF-BB. It shown that the FGF transcriptionally activates PDGF receptors . It
is then reinforced to the membrane. PDGF and FGF trigger expression of PDGFR
and FGFR respectively and resulted in decrease in number of receptors residing in the
plasma membrane after internalization. There is a crosstalk about the proteins to
switch the expression of receptors to sensitize the cells to the respective ligands this
shows how both these factors regulates the neoplasticity metastasis and angiogenesis.
Kiran et al 20119 described method how to prepare PRP and their
clinical application and also the safety concerns of PRP. The evolution of PRF the
second generation platelet concentrate which is prepared by the blood is centrifuged
in centrifuge machine for 12 minutes at 2700 RPM. Then he reported PRF eliminates
adding anticoagulant as well as it needs to neutralize.
Lee et al 201161 did experiments in the animal model with peri-
implant of defect sized 3.0x5.0 mm (width x length) repaired successfully by
applying Platelet- Rich Fibrin alone.
Prakash et al 201158 explained with platelet-rich fibrin, though the
biomaterial appears to accelerate the physiologic healing, there is a numerous point
of view about Platelet Rich Fibrin have to be tested clinically.

Review of Literature
Page 17
Ruga et al 201159 combined the action of piezoelectric surgery and
Platelet Rich Fibrin which can be considered a fine and safe technique for alveolar
socket healing and third molar surgery.
Sammartino et al 201157 described L-Platelet Rich Fibrin is a safe
filling and also the hemostatic material it is a reliable therapeutic option which avoid
significant bleeding after extractions in dentistry without any suspension of
continuous anticoagulant therapy in cardiac patients.
Simonperi et al 201160 L-Platelet Rich Fibrin used as a sole filling
material during sinus-lift and implantation which is suitable surgical option for
promoting regeneration of natural bone.
Bambal et al73 2012 he describes the successful rate of platelet rich
fibrin while treating the periapical lesion which shows a better healing when
compared to the other.
Del corso et al 201266 showed that L-Platelet Rich Fibrin also
defining a new therapeutic principles: Natural tissue regeneration (NTR) for intra
bony lesion treatment in periodontal problem and the natural bone
regeneration(NBR)to reconstruct the alveolar ridges.
Dohan et al 201262 estimated that the slow release of growth factors
PDGF-AB, TGF-ß1, VEGF and matrix proteins from P-PRP gel membrane and L-

Review of Literature
Page 18
PRF in culture medium. He explained that the less than 5 days P-PRP gel
membranes dissolves completely in the culture medium, mean while the L-PRF
membranes are still intact after 7 days this implies that polymerization and the final
architecture of fibrin matrix influence the strength and the growth factor trapping/
release potential of the membrane.
Jankovic et al 201263 for 6 months he did randomized controlled
clinical study and compared the results with the use of a connective tissue grafts
(CTG) or platelet rich fibrin(PRF) membrane in the
gingival recession and clinically evaluated the impact of PRF on subjective patient
discomfort and early wound healing.
Ozdemir et al 201272 while used along with titanium barriers rate of
bone regeneration is increased due to growth factors present in the Platelet Rich
Fibrin(PRF).
Peck et al 201267 L-Platelet Rich Fibrin is newly developed platelet
concentrate and it is successfully used in the number of surgical procedures to induce
wound healing and also used to stimulate bone formation for ideal and successful
implants placement.
Tunah et al 201265 T-Platelet Rich Fibrin induce the formation of new
bone along with the new connective tissue in the rabbit model helpful for wound
healing in 30 days of treatment.

Review of Literature
Page 19
Vinayakumar et al 201264 platelet rich fibrin is a second generation
platelet concentrate mainly used widely used to increase soft and hard tissue healing.
Gassling et al 201370 due to the limits of study, lateral sinus window
were covered by two different absorbable membranes such as a conventional collagen
membrane or platelet rich fibrin.
Khiste et al 201368 described that the PRF starts the healing process
to increase predictability. It contains the thrombin concentrations is weak with
equilateral functions it permits to form a fine and flexible network which supports
the cytokines.,
Yosif et al 201369 illustrated the use of PRFM in the implant
osseointegration site. In this study thirty two adult rats, where the titanium implants
were inserted in the femur.PRF place on right side and left side taken as control
group along with screw implants only.
Mc Lellan et al 201471 in 12 healthy patients the PRF is evaluated
thoroughbred geldings and it is compared with the temporal release of the growth
factors to PRP. For five days four groups were analysed for slow and immediate
release PRP and PRF.
Kumar et al 2015 82 Platelet concentrates shown to have great scope
in reconstructive and regenerative medicine as well in dentistry. And PRF being the
Review of Literature
Page 20
recent of the Platelet Derivatives which is safer and simpler when compared to
previous PRP concentrates they are used clinically.
Reddy et al 2015 84 observed the healing of PRF membrane site
supports to accelerates the soft tissue healing. PRF membrane act as a bandage is an
efficacious approach which protect the open wound in palate helps to reduce healing
time and discomfort of the patient.
Raaj et al 2015 83 Platelet rich fibrin (PRF), is a second generation
platelet concentrate and shown to promote soft tissue healing because PRF contains
autologous growth factors and cytokines which responsible factors for the
regeneration of bone and also for the maturation of soft tissue.

Platelet Rich Fibrin
Page 21
Platelet rich fibrin is a platelet concentrates. It is single fibrin mesh which
contains all constituents of blood products helpful for healing and immunity. The recent
biomaterial is autologous matrix which has cicatricial properties, like fibrin glue or like
platelet concentrate.59 Fibrin is activated from fibrinogen. This molecule is present in plasma
and in platelet alpha granules plays a major role in hemostatis by the aggregation of
platelets.25,38
Platelets is a major constituents obtained from blood. The structure is
discoidal and a nuclear structure. The diameter is 2-4µm. Megacaryocytes of bone marrow is
the main source for platelet production. The lifespan become 8-10days.11 There are so many
growth factors seen in platelets. They are listed below,
Transforming growth factor ß-1 it is a fibrosis agent. It is considered as inflammatory
regulator which induce fibrous cicatrisation.
Platelet derived growth factor it is a stimulant of mesenchymal lineages. It is a
essential regulators helpful for migration, survival of mesenchymal cell lineages and
proliferation.
The insulin like growth factor is a cell protective agent. 11
Platelet rich fibrin prepared by centrifugation of blood without add any
anticoagulant. It contain fibrin matrix which is polymerized into tetra molecular structure,
cytokines, platelets, circulating stem cells and leukocytes include into it. Platelet gel can also

Platelet Rich Fibrin
Page 22
used as an membrane. Fibrin gel can also used along with bone grafts which helpful for
healing, bone regeneration and also achieve haemostasis.59
Choukroun et al first developed platelet rich fibrin specifically used in oral
surgery. In this technique no need to require any anticoagulant. Patients own blood is
centrifuged so there is no possible of spreading any blood borne diseases.25
The blood is collected without any anticoagulant and immediately
centrifuged for 10 minutes in 3000rpm. Due to absence of anticoagulant most of the platelets
activated in few minutes in contact with tube walls the coagulation cascades released. Fibrin
clot obtained between red blood corpuscles and a cellular plasma. A cellular plasma is the
top layer, fibrin is the middle layer and the red blood corpuscles is the bottom layer.25
The secret of the success present on faster blood collection and immediately
transfer to centrifuge. Prolonged time make chance of failure in process.
Platelet rich fibrin induce soft tissue healing, bone regeneration and it is
mixed with graft material. Platelet rich fibrin used in treating residual extraction sockets.34 It
can also used to treat gingival recession and protect the root platelet rich fibrin used in sinus
lift and dental implant procedure.72

Materials & Methods
Page 23
The patients with bilateral extraction in dental arch were selected
for the study from the out patient department of oral and maxillofacial surgery, Sree
Mookambika Institute Of Dental Science, Kulasekharam. The patients were divided
into two groups for this study. In Study group Platelet-Rich Fibrin was placed after
extraction in the extracted socket. In Control group patients there is no intervention
after extraction in the extracted socket. Before commerencing the study we got
approval from Institutional research committee and Institutional human ethical
committee, Sree Mookambika Institute Of Dental Science, Kulasekharam. All the
patients who were included in the study agreed for the study protocol and written
informed consent was submitted. All patients were recalled for suture removal in 7th
day and reviewed in 1st, 3rd , 6th month postoperatively.
Total duration of the study: 6 months
Number of groups: Two groups
Description of groups:
30 patients were taken for dental extraction. Total 60 extraction (30 in
case and 30 in control) One is case group and other is control group. Atraumatic
extraction carried in the right and left quadrant of the same jaw and same teeth. One
side taken as case and other side as control.

Materials & Methods
Page 24
Group A- Platelet rich fibrin placed
Group B- No intervention
Sample size of each group:
According to this formula 22
1 22 the sample size of each group may be 30.
Inclusion Criteria:
• Patient of age group 18 to 55 years will be selected irrespective of religion, socio-
economic status, caste and sex.
• Patients in whom bilateral extraction is indicated.
• Patients who were agreed for this study protocol/consent.
Exclusion Criteria:
• Allergic to local anaesthesia.
• Chain smoker
• Uncontrolled systemic illness.[on h/o]
• Immunodeficiency pathology [on h/o]
• Bone disorders
• Patient with psychiatric problem
• Patients who were not willing for post operative follow-up
• Platelet disorders
• hematological disorders.
Materials & Methods
Page 25
• Chemotherapy and radiotherapy
• Stress situations
The subjects were informed of the study after the screening
procedure. They were explained that their selection was made since they met the
inclusion and exclusion criteria. The subjects were ensured that their participation is
voluntary and that they have the right to withdraw at any time during the course of the
study without giving reasons. Informed consent was obtained from the volunteers.
ARMAMENTARIUM
• Medical centrifuges
• Tourniquet
• 5ml disposable syringe with 24 gauge needle
• Surgical gloves
• Cotton gauze
• Spirit swabs
• Blood collecting glass tubes
• Nasal dressing forceps
• Scissors
• Stop watch
Materials & Methods
Page 26
PROCEDURE IN DETAIL:
Patient was prepared for the extraction. One side taken as case and
other side taken as control in same patient with bilateral extraction. Under aseptic
condition instruments were arranged, patients was draped. Intraorally inferior alveolar
nerve, long buccal nerve block, lingual nerve block were given for mandibular
extractions and posterior superior alveolar nerve block, middle superior nerve block,
anterior superior alveolar nerve block, greater palatine nerve block and nasopalatine
nerve block were given for maxillary extractions by injecting 2% solution of
lignocaine hydrochloride along with 1:80000 adrenaline. (LIGNOX 2 %). [3ml
Syringe with 24 gauze needle]
SURGICAL TECHNIQUE:
Full thickness mucoperiosteal flap was reflected to achieve adequate
exposure of the surgical site by periosteal elevator. Tooth was delivered using
appropriate forceps. After extraction bony spicules which is sharp and with rough
edges of extracted socket was trimmed and smoothened with bone file and bone
rounger. The hemostasis were achieved. Now after this procedure the prepared
Platelet rich fibrin was placed in the extracted socket for the side of case group . With
the help of 3-0 silk suture material, the extracted socket were sutured. The opposite
side extraction carried after 1 week taken as control.

Materials & Methods
Page 27
PREPARATION OF PLATELET RICH FIBRIN:
A tourniquet was tied on patient’s arm. In the aseptic conditions, for
about 4ml blood was withdrawn and it was collected in the 5ml capacity blood
collection tube which was pre-sterilized without any anticoagulant and it was
centrifuged immediately for 10 minutes at 3000rpm. After centrifugation following
three layers were formed.
1. Topmost layer consists of a cellular platelet with poor plasma
2. Middle layer contains Platelet rich fibrin clot
3. Bottom layer is Red blood corpuscles
Now from the centrifugation tube platelet rich fibrin clot was
withdrawn using a nasal dressing forceps with long and narrow beak. After
withdrawal of platelet rich fibrin clot, the red blood corpuscles clot which was seen is
attached to the base of platelet rich fibrin clot. Using scissors this was separated. Now
the platelet rich fibrin clot is ready to place in the socket.
ROUTINE POST OPERATIVE CARE:
• The post operative instructions were given to the patients which includes a 30minutes
firm pressure with a sterile gauze pack and to take semisolid or cold liquid diet for
first 24 hours and to avoid rinsing.
• After every meals patients were advised to rinse with warm saline rinse and 0.2%
chlorhexidine rinses twice daily after 24 days for 1 week.
• Postoperatively antibiotics and analgesics were prescribed for 5 days.
• On 7th postoperative day the suture was removed.

Materials & Methods
Page 28
FOLLOW-UP:
• Post-operative follow done in case group after 24 hours to check the stability of
platelet rich fibrin in socket.
• After 7 days suture removal was done. Succeeding follow-up was done at 1st month,
3rd month and 6th month postoperatively for the evaluation of radiographic
parameters.
PARAMETERS EVALUATED
BONE DENSITY ANALYSIS
With the help of HP Scan Jet 7400C scanner all the IOPA images were
digitalized. “Adobe Photoshop 7.0” which is a digital software programme is used to
analyse the Bone density and it enlarges the standard IOPA radiograph for better
resolution.
The grey level histogram value was measured in immediate
postoperative IOPA and the graph was marked.. This interpretation of bone density
appears white for dense bone and it appears black on empty defect in radiograph.
The bone density analysis was done and compared postoperatively by using software
measured by grey level histogram value in 1st month, 3rd month and 6th month post-
operative period and the value were compared.

Materials & Methods
Page 29
STATISTICAL TOOLS EMPLOYED:
The study was analyzed by statistical package for social
sciences(SPSS 16.0) version. Unpaired t test applied to find the significant between
the groups. P value less than 0.05(p<0.05) considered statistically significant at 95%
confidence interval.
The grey level in histogram value is used to evaluate bone density by
using Wilcoxon rank-sum test to compare between two groups. The Friedman test
is used to compare within the group.
Materials & Methods
Page 30
SREE MOOKAMBIKA INSTITUTE OF DENTAL SCIENCE, KULASEKHARAM
DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY
CASE RECORD
DATE: OP NO.
PERSONAL DATA:
Name:
Age:
Sex:
Address:
History:
Cheif complaints:
History of present illness.
Materials & Methods
Page 31
Medical history:
Dental history:
Personal history:
Family history
EXAMINATIONS:
Extra oral examination:
Face:
Tmj:
Lymphnodes:

Materials & Methods
Page 32
Intraoral examination:
Soft tissue examination:
Buccal/labial mucosa:
Tongue:
Alveolar mucosa:
Floor of the mouth:
Hard tissue examination:
Teeth present:
PROVISIONAL DIAGNOSIS:

Materials & Methods
Page 33
TREATMENT PLAN:
POSTOPERATIVE EVALUATION:
RADIOGRAPHIC EVALUATION
Findings Review
Grey level histogram values
Immediate post-op Date:
1st month post-op Date:
3rd month post-op Date:
6th month post-op Date:
Guide/ Co-guide signature

Figures
Page vii
FIG: 1 ARMAMENTARIUM FOR THE PREPARATION OF PLATELET
RICH-FIBRIN
FIG:2 MEDICO CENTRIFUGE

Figures
Page viii
FIG:3 WITHDRAWAL OF BLOOD
FIG:4 AFTER CENTRIFUGATION

Figures
Page ix
FIG:5 PLATELET RICH FIBRIN GEL
FIG:6 EXCTRACTED SOCKET

Figures
Page x
FIG:7 SUTURE DONE AFTER PLATELET RICH FIBRIN PLACED IN THE
EXTRACTION SOCKET
FIG:8 GREY LEVEL HISTOGRAM VALUE EVALUATION FROM
INTRAORAL PERIAPICAL RADIOGRAPH
Figures
Page xi
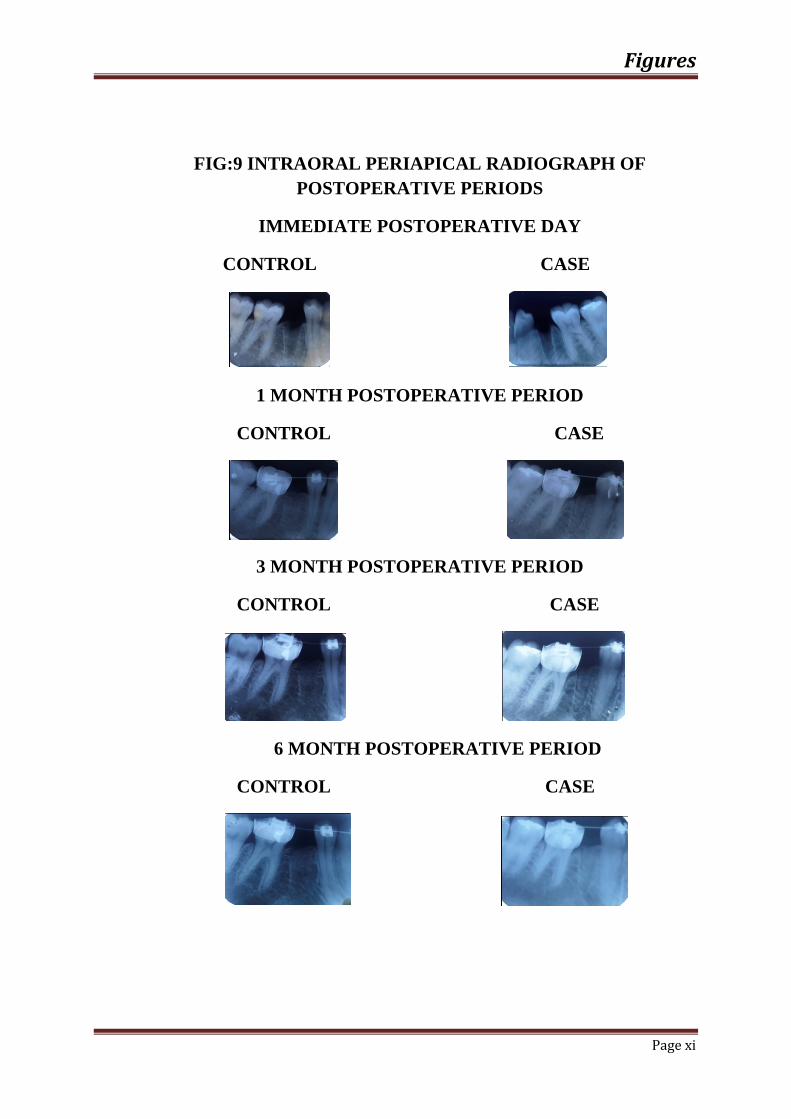
FIG:9 INTRAORAL PERIAPICAL RADIOGRAPH OF POSTOPERATIVE PERIODS
IMMEDIATE POSTOPERATIVE DAY
CONTROL CASE
1 MONTH POSTOPERATIVE PERIOD
CONTROL CASE
3 MONTH POSTOPERATIVE PERIOD
CONTROL CASE
6 MONTH POSTOPERATIVE PERIOD
CONTROL CASE

Results
Page 34
The present study was designed to evaluate the efficacy of Autologous
platelet rich fibrin in bone regeneration after extraction. The study was undertaken on
30 patients with bilateral extraction from the outpatient department of oral and
maxillofacial surgery in Sree Mookambika Institute Of Dental Science,
Kulasekharam.
The age, sex and date of procedure were recorded. Grey level histogram
value recorded from IOPA in immediate postoperative day, 1 month, 3 month and 6
months postoperatively of all patients of the case and control groups has been
tabulated.
By statistical analysis the results obtained were given below,
Total 30 patients were selected for this study, among 30 patients 12 patients
were males(40%) and 18 patients were females (60%). The male to female
ration was 1:1.5.
The mean age of the 30 patients were 29.37 years (Table:1, Graph 1)
The mean bone density values become 47.53 and 47.50 of control and case of
immediate postoperative, 58.73 and 60.85 of control and case in 1st month
postoperative, 66.70 and 69.46 of control and case in 3rd month postoperative,
74.23 and 77.30 of control and case in 6th month postoperative period.
(Table:2).

Results
Page 35
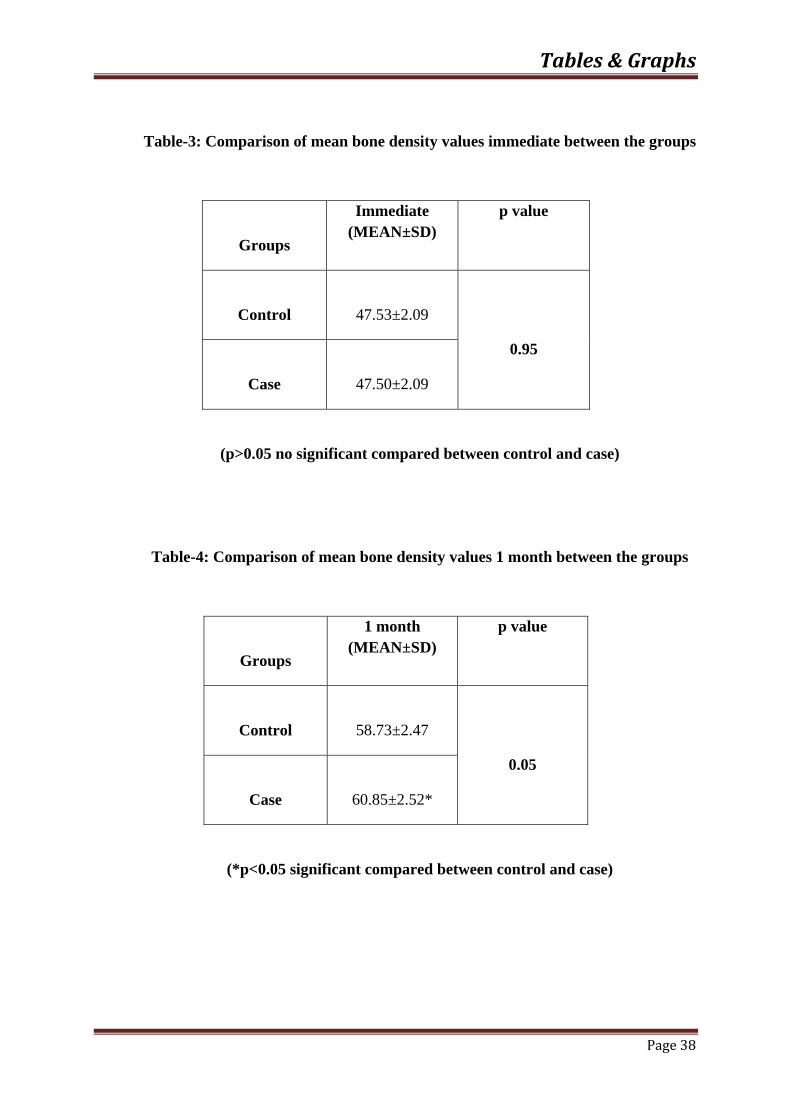
The mean bone density values of immediate postoperative become no
significant between control and case (Table:3)
The mean bone density values of 1st month postoperative period become
significant between control and case(Table:4)
The mean bone density values of 3rd month postoperative become significant
between control and case(Table:5)
The mean bone density values of 6th month postoperative period between
control and case become significant. (Table:6)
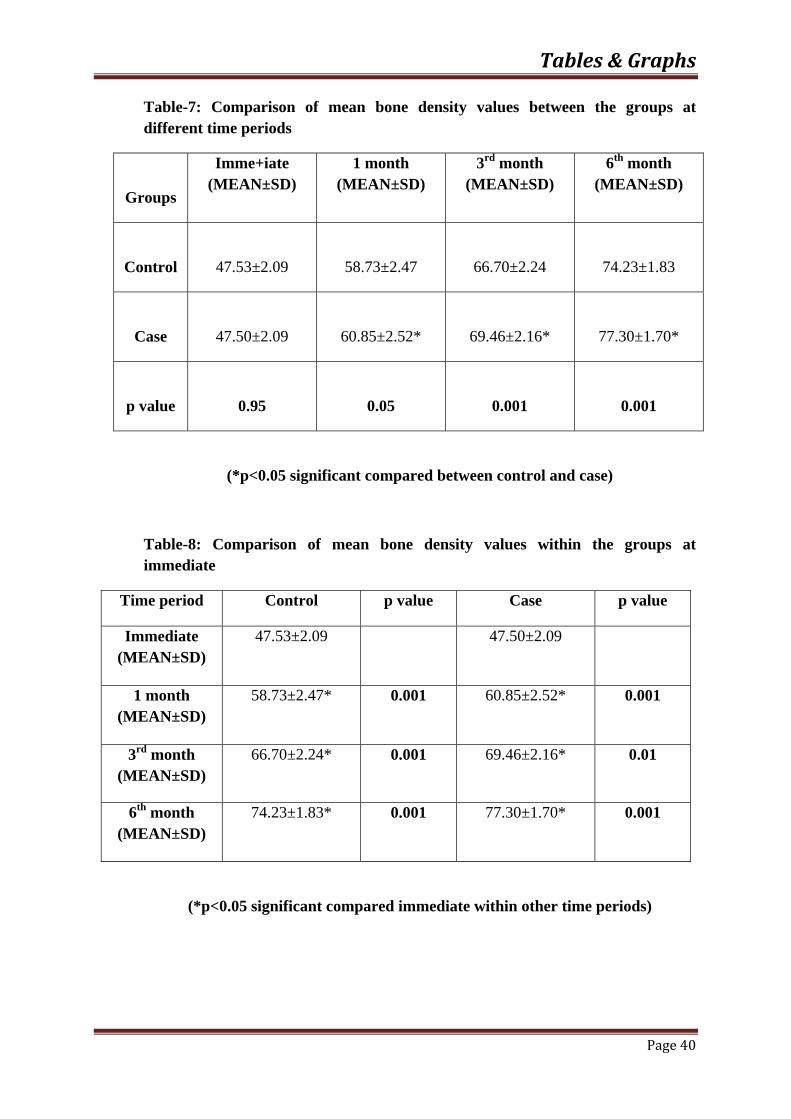
The comparison of mean bone density values between the groups at different
time periods become significant.(Table:7, Graph 2)
The mean bone density values within the group at immediate postoperative day
is significant when compared within other time periods.(Table:8)
The mean bone density values within the groups at 1 month postoperative
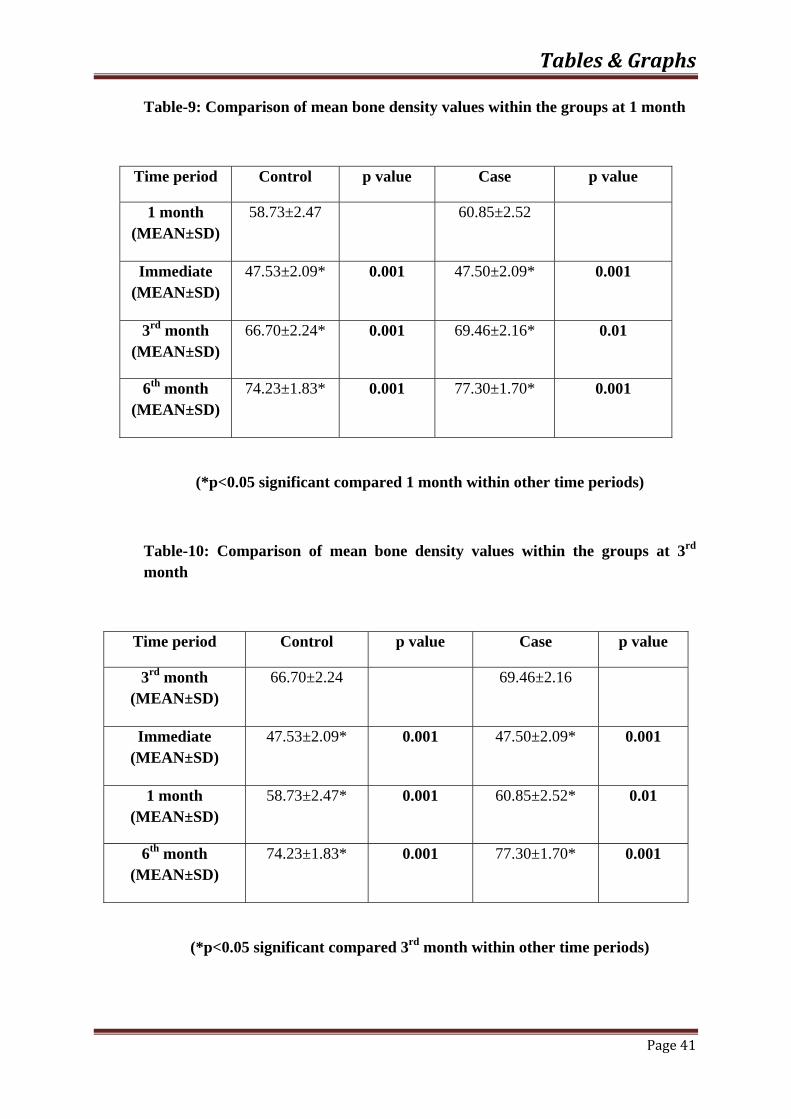
period is significant within other time periods(Table:9)
There is significant values of mean bone density within the groups at 3rd month
postoperative within other time periods.(Table:10)
Results
Page 36
The mean bone density values within the groups at 6th month postoperative is
significant within other time periods.(Table 11)
The multiple comparison of mean bone density values within the groups at
different time periods is significant compared immediate with other time
periods, 1st month with other time periods and 3rd month with other time
periods.(Table:12, Garph 3)
The bone density value is higher in case treated with Autologous
Platelet Rich Fibrin gel compared with control group which has been not treated with
Autologous Platelet Rich Fibrin gel.

Tables & Graphs
Page 37
Table-1: Demographic data of study population
Demographic data
Age
(MEAN±SD)
Gender
Male
Female
Number Percentage (%)
Number Percentage (%)
Groups
29.37±8.26
12
40.00
18
60.00
Table-2: Mean bone density values of different groups at different post operative periods
Groups
Immediate (MEAN±SD)
1 month (MEAN±SD)
3rd month (MEAN±SD)
6th month (MEAN±SD)
Control
47.53±2.09
58.73±2.47
66.70±2.24
74.23±1.83
Case
47.50±2.09
60.85±2.52
69.46±2.16
77.30±1.70
Tables & Graphs
Page 38
Table-3: Comparison of mean bone density values immediate between the groups
Groups
Immediate (MEAN±SD)
p value
Control
47.53±2.09
0.95
Case
47.50±2.09
(p>0.05 no significant compared between control and case)
Table-4: Comparison of mean bone density values 1 month between the groups
Groups
1 month (MEAN±SD)
p value
Control
58.73±2.47
0.05
Case
60.85±2.52*
(*p<0.05 significant compared between control and case)

Tables & Graphs
Page 39
Table-5: Comparison of mean bone density values 3rd month between the groups
Groups
3rd month (MEAN±SD)
p value
Control
66.70±2.24
0.001
Case
69.46±2.16*
(*p<0.05 significant compared between control and case)
Table-6: Comparison of mean bone density values 6th month between the groups
Groups
6th month (MEAN±SD)
p value
Control
74.23±1.83
0.001
Case
77.30±1.70*
(*p<0.05 significant compared between control and case)
Tables & Graphs
Page 40
Table-7: Comparison of mean bone density values between the groups at different time periods
Groups
Imme+iate (MEAN±SD)
1 month (MEAN±SD)
3rd month (MEAN±SD)
6th month (MEAN±SD)
Control
47.53±2.09
58.73±2.47
66.70±2.24
74.23±1.83
Case
47.50±2.09
60.85±2.52*
69.46±2.16*
77.30±1.70*
p value
0.95
0.05
0.001
0.001
(*p<0.05 significant compared between control and case)
Table-8: Comparison of mean bone density values within the groups at immediate
Time period Control p value Case p value
Immediate (MEAN±SD)
47.53±2.09 47.50±2.09
1 month (MEAN±SD)
58.73±2.47* 0.001 60.85±2.52* 0.001
3rd month (MEAN±SD)
66.70±2.24* 0.001 69.46±2.16* 0.01
6th month (MEAN±SD)
74.23±1.83* 0.001 77.30±1.70* 0.001
(*p<0.05 significant compared immediate within other time periods)
Tables & Graphs
Page 41
Table-9: Comparison of mean bone density values within the groups at 1 month
Time period Control p value Case p value
1 month (MEAN±SD)
58.73±2.47 60.85±2.52
Immediate (MEAN±SD)
47.53±2.09* 0.001 47.50±2.09* 0.001
3rd month (MEAN±SD)
66.70±2.24* 0.001 69.46±2.16* 0.01
6th month (MEAN±SD)
74.23±1.83* 0.001 77.30±1.70* 0.001
(*p<0.05 significant compared 1 month within other time periods)
Table-10: Comparison of mean bone density values within the groups at 3rd month
Time period Control p value Case p value
3rd month (MEAN±SD)
66.70±2.24 69.46±2.16
Immediate (MEAN±SD)
47.53±2.09* 0.001 47.50±2.09* 0.001
1 month (MEAN±SD)
58.73±2.47* 0.001 60.85±2.52* 0.01
6th month (MEAN±SD)
74.23±1.83* 0.001 77.30±1.70* 0.001
(*p<0.05 significant compared 3rd month within other time periods)

Tables & Graphs
Page 42
Table-11: Comparison of mean bone density values within the groups at 6th month
Time period Control p value Case p value
6th month (MEAN±SD)
74.23±1.83 77.30±1.70
Immediate (MEAN±SD)
47.53±2.09* 0.001 47.50±2.09* 0.001
1 month (MEAN±SD)
58.73±2.47* 0.001 60.85±2.52* 0.01
3rd month (MEAN±SD)
66.70±2.24* 0.001 69.46±2.16* 0.001
(*p<0.05 significant compared 6th month within other time periods)
Table-12: Multiple comparison of mean bone density values within the groups at different time periods
Time period Control Case
Immediate (MEAN±SD)
47.53±2.09 47.50±2.09
1 month (MEAN±SD)
58.73±2.47* 60.85±2.52*
3rd month (MEAN±SD)
66.70±2.24*,# 69.46±2.16*,#
6th month (MEAN±SD)
74.23±1.83*,#,$ 77.30±1.70*,#,$
(*p<0.05 significant compared immediate with other time periods, #p<0.05 significant compared 1 month with other time periods, $p<0.05 significant compared 3rd month with other time periods)

Graph-1: D
1
1
1
1
1
2
Num
ber
Demograph
0
2
4
6
8
10
12
14
16
18
20
hic data of
Male
study popu
e
G
ulation
Gender
Tab
Femal
bles & Gr
le
raphs
Page 43

Graph
0
10
20
30
40
50
60
70
80
Mea
n
h-2: Mean
Immed
bone densi
diate 1
ity values ooperative p
1 month
Ti
Control
of different periods
3rd mo
ime
Case
Tab
groups at
nth 6th
bles & Gr
different p
h month
raphs
Page 44
ost

Graph-3: Mdifferent ti
0
10
20
30
40
50
60
70
80
90
Mea
n
Multiple coime period
Immed
omparison s
diate
of mean bo
1 month
Control
one density
3rd m
Case
Tab
y values wi
month
bles & Gr
ithin the gr
6th mont
raphs
Page 45
roups at
th
Discussion
Page 46
Bone tissue repair is a complex process helpful for cellular
functions and mineralization of defects to remodelling the surgical defect to regain
the original structure.74 In future protecting wound and regain the bone will become
standard care for all extractions. Platelet-rich fibrin is new step in platelet therapeutic
concept helpful for artificial biochemical modification.8 Platelet-Rich Fibrin is a
autologous fibrin which contain huge amount of platelet and leukocyte cytokines41.
Wound healing involves a sequence of physiological events which
restore and replace the damaged tissue functions. After extraction have been done the
healing is explained in coagulative phase, proliferative phase and osteogenic-
remodelling phase. The coagulative phase starts from immediately after the extraction
and last until 3days which involves filling the socket with clot and inflammatory
process initiation. In this phase platelets, endothelium and fibroblast begins to release
a numerous growth factor. After this the proliferative phase starts and last until 20
days to 2 months following postoperative period . After this the blood clot become
dissolved, connective tissue matrix is formed, there is a supply of blood to the wound
the osteoblastic activity and osteoclastic activity is initiated, the last and the longest
phase is osteogenic-remodelling phase. The healing of the extracted socket last from
weeks till months. This phase involves mineralization of the matrix, secretion of
osteoid and bone remodelling.
The platelets helpful for blood clotting by hemostatic plug
formation. By using platelet concentrate it helpful for natural clot formation which
induce wound healing and bone regenerative process.34 The PRFM creates a gel like
substance which contain functional, nonactivated, intact platelets present in the fibrin

Discussion
Page 47
matrix which release growth factors over the period of 7 days.75 It mainly used as a
protective layer for scheniderian membrane in sinus lift procedure to fill the material.6
Bone morphogenic was first identified in the year 1965 . the bone
formation is induced when demineralised bone matrix is placed. There is a wide
evidence which supports there role as bone induction regulators repair and
maintenance also being critical determinants of embryological development of
mammalian organisms. In differentiation, growth inhibition, proliferation and arrest of
wide variety of maturation cells BMP plays a major role depending on cellular
microenvironment and interaction with other regulatory factors. Some of the demerits
of BMP are poor distribution, large dose requirement, high cost and short half life. In
order to overcome these demerits alternative methods like promoting bone
regeneration and formation.76
The initial coagulative phase contains a series of physiological
process, they are proliferation, cellular migration and differentiation, initiation of
vascular in-growth and increased collagen production. In order to bring efficient and
timely prepare of wounds many type of cell, other proteins and growth factors interact
with one another.
Several studies made in last 10 years in animal and in vivo
conclude polypeptide growth factors helpful for soft tissue and bony healing.
Transforming growth factor (TGF)ß1 and ß2 helpful to inhibit bone resorption. It
helpful for faster maturation of collagen in wounds. Platelet derived growth

Discussion
Page 48
factor(PDGF) helpful to increase the wound healing cells which helpful for increase
wound healing properties. 34,77
The main advantages in using platelet rich fibrin may be34
Helpful for tissue healing
Regenerate the bone defects
Maintain hemostasis
Simple chair side procedure
With drawl of patients own blood
No chance of cross infection
No need of any anticoagulants.
The platelet rich plasma is first generation platelet concentrate
contain various growth factors such as platelet derived growth factor, vascular
endothelial growth factor and transforming growth factor obtained from freshly drawn
venous blood. Fibrin, fibronectin and vitronectin are the three proteins present which
helpful for epithelial migration and osteoconduction.
The second generation platelet concentrate is platelet rich fibrin is
centrifuged without any anticoagulants.25 It contains various growth factors which
helpful for wound healing and bone regeneration process. When compared to platelet
rich plasma no need of add any anticoagulants. Platelet rich fibrin release cytokines in
a fibrin clot. In this study we used platelet rich fibrin to regenerate the bony defects in
the extraction sockets.

Discussion
Page 49
PRF and oral surgery:
To restore the bone loss so many regenerative medicine technique
are applied in dentistry. In Choukroun’s PRF the blood collected without
anticoagulant and centrifuged immediately. The natural coagulation process helpful
for easy collection of PRF clot. To induce bone regeneration in sinus lift procedure to
achieve good implant placement it plays major role to achieve good results. L-PRF
act as sole filling material in sinus lift and implantation is a good option to promote
natural bone regeration.50,60,66
PRF based membrane used to cover the alveolar ridge
augmentation in several in vivo study. PRF appears superior to collagen (Bio-Gide)
used as scaffold membrane. PRF membrane is suitable for cultivation of Periosteal
cells in bone tissue engineering.54
Due to inadequate bone in the alveolar ridge implant failure is the
major problem in implant dentistry. Implant success is based on ideal anatomical
position to maintain functional and aesthetic results. It is not always possible due to
bone tissue loss. L-prf is a platelet concentrate used with success in most of the
surgical procedures to obtain wound healing and new bone formation.59,67 PRF is used
along with Bio-Oss as a graft material in maxillary sinus augmentation in severe bone
atrophy.78

Discussion
Page 50
PRF for facial plastic surgery:
Platelets plays a major role in homeostasis, but recent studies
shows improve in wound healing. Platelet concentrate induce wound healing. Platelet
rich fibrin matrix helpful for fat transfer supplementation and volume augmentation.
The prf produce natural and autologous platelet concentrate releases growth factors
which stimulates regeneration of surrounding tissues for cosmetic application.79
There are several studies regarding Platelet Rich Fibrin were
applied in Oral and Maxillofacial surgery,
Choukroun et al11,12,25 used autologous platelet rich fibrin to
improve bony healing in the implant dentistry. Platelet rich fibrin combined with the
material freeze-dried bone allograft(FDBA) helpful for sinus floor elevation to
induce bone regeneration. Simonpieri et al concluded hat there is good results when
Platlet rich fibrin used along with FDBA.
Jankovic et al80 concluded platelet rich fibrin is potential for root
coverage in gingival recession cases which promote wound healing, graft
stabilization, bone regeneration , wound sealing and to achieve hemostasis.The major
disadvantage of this platelet rich fibrin will be large amount of blood collected for
larger defects.
Discussion
Page 51
In this study, according to Choukroun et al2 platelet rich fibrin
was prepared from 4 ml blood sample from same patient without any anticoagulant
collected in test tubes. It centrifuged immediately for 10 min in 3000 rotations. Su et
al joined with Choukroun et al shown the importance of rapid handling of blood
sample. In this study conventional medico centrifuge machine is used.
Platelet rich fibrin taken out from the tube and placed in the
extracted socket. The remaining PPP and RBCs were discarded. After extraction the
platelet rich fibrin is placed in the intra bony defects in different time intervals the
assessment was made for bone density.
By using “adobe photoshop 7.0” software program bone density
were analysed. The IOPA were taken immediate postoperative period, 1month
postoperative period, 3 month postoperative period, 6month postoperative period to
measure the bone density according to this software. By using grey level histogram
value the bone density were analysed. Grey level for each pixels were increase for
white and decrease for black image. The graph were interpreted for bone density and
the dense bone shows white and empty space appears black in intra oral periapical
radiograph jansen et al81
Bone density analysis of immediate postoperative day was
performed on the day of extraction and values were recorded. The mean value become
equal in case and control group. It is not significant the mean value become(p>0.05).
The mean value of grey level histogram were evaluated by IOPA in case group and
control group in 1st month, 3rd month and 6th month postoperative period. The IOPA
Discussion
Page 52
were digitalized by using HP scanner. It was significant in 1st month, 3rd month and
6th month postoperative period the mean value become(p<o.o5). According to my
study the extracted socket treated with platelet rich fibrin shows more bone density
when compared to the normal extraction socket. The results of these study coincide
with Diss et al5 and Chang et al24 study.
The present study to evaluate the bone regeneration in the
extraction socket by using platelet rich fibrin. Bilateral extraction of same tooth in a
patients is choosen for this study one side taken as control and another it was taken as
case. When comparing the case with control the bone regeneration is higher in case
than control. So the patients treated with Platelet rich fibrin gel shows more bone
regeneration than the patients not treated with platelet rich fibrin gel Rao et al1
The limitations of study were listed below,
Bone width and bone height were not assessed
Longer follow up is needed for better results
Platelets quality, quantity and its growth factor were not assessed.

Summary & Conclusion
Page 53
In this clinical study to evaluate the effect of autologous platelet rich
fibrin used in extraction socket for bone regeneration. This study clearly indicates the
improvement in bone regeneration in the extraction socket compared with extracted
socket not treated with platelet rich fibrin.
Patients with bilateral extraction were chosen for this study. Inclusion
and exclusion criteria of this study followed strictly. The benifits of platelet rich fibrin
were taken to the knowledge of the patients. Bilateral extraction were performed at
different appointments. One side is taken as case and other side taken as control.
Extracted socket treated with platelet rich fibrin were taken as case and other
extraction socket taken as control. Bone density were analysed by using intraoral
periapical radiograph at different time intervals. The immediate bone density were
measured on the day of procedure. Patients advised to review after 1 week for suture
removal. Further bone density analysis done at 1st month, 3rd month and 6th month
postoperative period.
IOPA were digitalized using HP scanner 7400C by using “Adobe
photoshop 7” the grey level histogram value were evaluated for bone generation in
case and control group. Black image denotes less bone density and white image
denotes high bone density in the extraction socket. In statistical analysis there no
significant in immediate postoperative between case and control group. But in later
period of 1st month, 3rd month and 6th month postoperative period shows a significant
between case and control group in bone regeneration.

Summary & Conclusion
Page 54
The procedure for the preparation of platelet rich fibrin is simple chair
side procedure, patients own blood, very low cost, time consuming is very less and
shows good results. In this study bone generation in the extraction socket is analysed
in different time intervals. There is significant changes seen in the extracted socket
treated with platelet rich fibrin when compared to the socket not treated with platelet
rich fibrin.
Concluded that the platelet rich fibrin plays major role in bone
regeneration process in the extracted socket when compared to the non treated platelet
rich fibrin socket. It also helpful for osseous regeneration in other post surgical
defects, implant placement, mandibular reconstruction, ridge augmentation, graft for
bone substance etc.

Bibliography
1. Rao SG, Bhat P , Nagesh KP, Gundu H.R.Rao. Bone regeneration in extraction
socket with autologous platelet rich fibrin gel. J.maxillofac.surg (jan-mar 2013)
12 (1) 11-16
2. Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, Gogly B.
Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part I:
technological concepts and evolution. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2006; 101:e37-44
3. Andrae j, gallini r, betsholtz c: role of platelet derived growth factor in
physiology and medicine. Genes dev 2008:22:1276-1312
4. Weyrich AS, Schwertz H, Kraiss LW, Zimmerman GA. Protein synthesis by
platelets: historical and new perspectives. Journal of thrombosis and haemostasis
2009(2): 241-46
5. Diss A, Dohan MD, Mouhyi J, Mahler P. Osteotome sinus floor elevation using
choukroun’s platelet rich fibrin as graft material: A 1-year prospective pilot study
with microthreaded implants. Oral surg oral med oralpathol radiol endod 2008:
105; 572-579
6. Dohan Ehrenfest DM, Marco Del Corso, Antoine Diss, Jaafar Mouhyi, Jean-
Baptiste Charrier. Three Dimensional A rchitecture and cell composition of a
choukroun’s platelet rich fibrin clot and membrane. J Periodontol 2010; 81:546-
55.

Bibliography
7. Dohan Ehrenfest DM, De Peppo GM, Doglioli P, Sammartino G. Slow release of
growth factors and thrombospondin-1 in choukroun’s platelet rich fibrin(PRF): a
gold standard to achieve for all surgical platelet concentrates technologies.growth
factors 2009; 27:63-69.
8. Moojen DJ, Everts PA, Schure RM et al. Antimicrobial activity of platelet
leukocyte gel against staphylococcus aureus. J Orthop Res 2008;26:404-410.
9. Kiran NK, Mukunda KS, Tilak Raj TN. Platelet concentrates: A promising
innovation in dentistry. Journal of dental sciences and research 2011; 2(1):50-61.
10. Simon BI, Gupta P, Tajbakhsh S. Quantitative evaluation of extraction socket
healing following the use of autologous platelet rich fibrin matrix in humans. Int
J Periodontics Resorative Dent 2011;31(3):285-95.
11. Sharma A, Pradeep AR. Autologous platelet rich fibrin in the treatment of
mandibular degree II furcation defects. A randomized clinical trial. J periodontal
2011;82:1396-1403
12. Dohan DM, Choukroun J, Diss A, Dohan SL, Simonpieri A, Girard MD platelet
rich fibrin(prf): a second generation platelet concentrate part IV: Clinical effects
on tissue healing. Oral surg oral med oral pathol radiol endod 2006;101:E56-60.

Bibliography
13. Keyhan SO, Hemmat S, Badri AA, Abdeshahzadeh A, Khlabani K. Use of
platelet rich fibrin and platelet rich plasma in combination with fat graft: which is
more effective during facial lipostructure? J Oral Maxillofac Surg 2013;7(3):
610-21.
14. Qureshi AH, Chaoji V, Maiguel D. Proteomic and phosphor-proteomic profile of
human platelets in basal, resting state; insights into integrin signalling. PLoS one
2009; 4(10) ; Article ID e7627.
15. Ling H, Ye L, Xiulian H,Zhang Y, Wu H. A comparative study of platelet –rich
fibrin (PRF) and platelet-rich plasma(PRP) on the effect of proliferation and
differentiation of rat osteoblasts in vitro. Oral Surg Oral Med Pathol Oral Radiol
Endod 2009; 108: 707-713.
16. Gassling VL, Acil Y, Springer IN et al (2009) Platelet-rich plasma and platelet-
rich fibrin in human cell culture. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod 108:48–55
17. Matras H. Fibrin seal: the state of the art. J Oral Maxillofac Surg.
1985;43(8):605-11
18. Knighton DR, Ciresi KF, Fiegel VD, Austin LL, Butler EL.Classification and
treatment of chronic nonhealing wounds. Successful treatment with autologous
platelet-derived wound healing factors (PDWHF). Ann Surg 1986; 204(3):
322-30

Bibliography
19. Lynch SE, Nixon JC, Culvin RB, Antoniades HN. Role of platelet-derived
growth factor in wound healing. Synergistic effects with other growth factors.
Proc.Natl.Acad.Sci.USA 1987;84:7696-7700
20. Gibble JW, Ness PM. Fibrin glue: the perfect operative sealant? Transfusion
1990;30(8):741-47.
21. Kington DR, Ciresi K, Fiegel VD, Schumerth S, Butler E, Cerra F. Stimulation
of repair in chronic, nonhealing, cutaneous ulcers using platelet-derived wound
healing formula. Surg. Gynecol. Obstet 1990; 170(1):56-60.
22. Tayapongsak P, O’Brien DA, Monteiro CB, Arceo-Diaz LY. Autologous fibrin
adhesive in mandibular reconstruction with particulate cancellous bone and
marrow. J Oral Maxillofac Surg 1994;52(2):161-165.
23. Whitman DH, Berry RL, Green DM. Platelet gel: an autologous alternative to
fibrin glue with applications in oral and maxillofacial surgery. J.Oral Maxillofac
Surg 1997;55(11):1294-99.
24. Chang YC, Wu KC, Zhao JH. Clinical application of platelet rich fibrin as the
sole grafting material in periodontal intrabony defects. J Dent Sciences
2011;6:181-188.
Bibliography
25. Ross R, Glomset J, Kariya B, Harker L. A Platelet dependent serum factor that
stimulates the proliferation of arterial smooth muscle cells in vitro. Proc Natl
Acad Sci Usa 1974;71:1207-10.
26. Whitman DH, Berry RL, Green DM. Platelet gel: An autologous alteration in
oral and maxillofacial surgery. J Oral Maxillofac Surg 1997;55:1294
27. Slater M, Patava J, Kingham K. Involvement of platelets in stimulating
osteogenic activity. J Ortho Res 1995;13: 655-663
28. Marx RE, Carlson ER, Eichstaedt RM. Platelet rich plasma: Growth factor
enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Oral
Endod 1998;85:638-646.
29. Man, Daniel, Plosker, Harvey, Winland B, Jill E. The use of autologous platelet
rich plasma (Platelet gel) and autologous platelet poor plasma (fibrin glue) in
cosmetic surgery. Plast reconstr surg 2001;107(1):238-39.
30. MazzucoL, Balbo V, Cattana E, Guaschino R, Borzini P. Not every PRP-gel is
born equal. Evaluation of growth factor availability for tissues through four PRP-
gel preparations : fibrinet, regen PRP-kit, platelets and one manual procedure.
Vox sang 2009; 97(2):110-18

Bibliography
31. Anitua E. Plasma rich in growth factors: preliminary results of use in the
preparation of future sites for implants. Int. J. Oral Maxillofac Implants
1999;14:529-35.
32. Heldin CH, Westermark B. Mechanism of action and in vivo role of platelet-
derived growth factor. Physiol Rev 1999;79:1283-316.
33. Heldin CH. Simultaneous induction of stimulatory and inhibitory signals by
PDGF. FEBS Lett 1997;410:17-21.
34. Green, David M, Klink B. Platelet gel as an intraoperatively procured platelet-
based alternative to fibrin glue. Plast Recon Surg 1998;61:101
35. Schuldiner M, Yanuka O, Eldor JI, Melton DA, Benvenisty N. Effects of eight
growth factors on the differentiation of cells derived from human embryonic
stem cells. PNAS2000;21:11307-12.
36. Anitua E. The use of platelet rich growth factors(PRGF) in oral surgery.
PracProcedAesthet Dentistry 2001;13:487-93.
37. Weibrich G, Kleis WK, Hafner G, Hitzler WE, Wagner W. Comparision of
platelet, leukocyte and growth factor levels in point of care platelet enriched
plasma, prepared using a modified cursan kit, with preparations received from a
local blood bank. Clin Oral Implants Res 2003;14:357-62.

Bibliography
38. Soffler E, Ouhayoun JP, Anagnostou F. Fibrin sealants and platelet preparations
in bone and periodontal healing. Oral Surg oral med oral pathol oral radiol endod
2003;95:521-528.
39. Lacoste E, Martineau I, Gagnon G, Platelet concentrates: Effects of calcium and
thrombin on endothelial cell proliferation and growth factor release. J Periodontal
2003;74:1498-507
40. Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT. Autologous platelet as a
source of proteins for healing and tissue regeneration. Thromb haemost
2004;91:4-15
41. Dohan DM, Choukroun J, Diss A, Dohan AJ, Mouhyi J et al. Platelet rich
fibrin(PRF): a second generation platelet concentrate. Part III: leucocyte
activation: a new feature for platelet concentrate? Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 2006;101(3):51-55.
42. Li MO, Sanjabi S, Flavell RA. Transforming growth factor-beta controls
development, homeostasis and tolerance of T cells by regulatory T cell dependent
and independent mechanisms. Immunity 2006;25:455-71.
43. Thor AV, Stenport F, Johanson CB, Rasmusson L. Early bone formation in
human bone grafts treatment with platelet-rich plasma; preliminary
histomorphometic result. Int J Oral Maxillofac Surg 2007;36:1164-1171.
Bibliography
44. Su CY,Kuo YP, Nieh HL, Tseng YH, Burnoff T. Quantitative assessment of the
kinetics of growth factors release from platelet gel. Transfusion 2008;48:
2414-20.
45. Sunitha RV, Munirathnam NE. Platelet rich fibrin. Evolution of a second
generation platelet concentrate. Ind J Of Dent Res 2008;19(1):42-46.
46. Lundquist R, Dziegel MH, Agren MS. Bioactivity and stability of endogenous
fibrogenic factors in platelet rich fibrin. Wound repair regen 2008;16:356-63.
47. Schmidmaier G, Hermann S, Green J et al. Quantitative assessment of growth
factors in reaming aspirate, iliac crest and platelet preparation. Bone
2006;39:1156-1163.
48. Danielsen P, Jorgensen B, Karlsmark T, Jorgensen LN, Agren MS. Effect of
topical autologous platelet rich fibrin versus no intervention on epithelialisation
of donor sites and meshed split thickness skin autografts: a randomized clinical
trial, plast reconst surg 2008; 122(5):1431-40.
49. Su CY, Kuo YP, Tseng YH, Su CH, Burnouf T. In vitro release of growth factors
from platelet rich fibrin(PRF): a proposal to optimize the clinical applications of
PRF. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:56-61.

Bibliography
50. Mazor Z, Horowitz RA, Del Corso M, Prasad HS, Rohrer MD, DohanEhrenfest
DM. Sinus floor augmentation with simultaneous implant placement using
choukroun’s platelet rich fibrin as the sole grafting material: A Radiographic and
histologic study at 6 months. J periodontal 2009;80:2056-64.
51. Simonpieri A,Del Corso M, Sammartino G, Dohan Ehrenfest DM. The relevance
of choukroun’s platelet rich fibrin and metronidazole during complex maxillary
rehabilitations using bone allograft. Part II: Implant surgery, prosthodontics and
survival, Implant Dent 2009;18:220-29.
52. Lucarelli E, Beretta R, Dozza B, Tazzari PL, O’Connell SM, Ricci F, Pierini M
et al. A recently developed bifacial platelet rich fibrin matrix. Eur cell mater
2010;20:13-23.
53. Senger DR. Vascular endothelial growth factor: much more than an angiogenesis
factor. Mol Biol Cell 2010;21:377-9.
54. Gassling V, Douglas T, Warnke PH, Acil Y, Wiltfang J, Becker ST. Platelet rich
fibrin membranes as scaffolds for periosteal tissue engineering. Clin Oral
Implants Res 2010;21:543-9.
55. Gurbuzer B, Pikdoken L, Tunali M, Urhan M, Kucukodaci Z, Ercan F.
Scintigraphic evalution of osteoblastic activity in extraction sockets treated with
platelet rich fibrin. J Oral Maxillofac Surg 2010;68:980-9

Bibliography
56. Ahmed SS et al. Investigating the potential role of platelet derived growth factor
(PDGF). Biotechnology and Molecular Biology Review 2011:6(6):133-41
57. Sammartino G, Dohan Ehrenfest DM, Carile F, Tia M, Bucci P. Prevention of
hemorrhagic complications after dental extractions into open heart surgery
patients under anticoagulant theraphy: the use of leukocyte and platelet rich
fibrin. J Oral Implantol 2011;37:681-90
58. Prakash S, Thakur A. Platelet concentrates: past,present and future. J Maxillofac
Oral Surg 2011;10:45-9
59. Ruga E, Gallesio C, Boffano P. Platelet rich fibrin and piezoelectric surgery: a
safe technique for the prevention of periodontal complications in third molar
surgery. J Craniofac Surg 2011;22:1951-55
60. Simonpieri A, Choukroun J, Del Corso M, Sammartino G, Dohan Ehrenfest DM.
Simultaneous sinus-lift and implantation using microthreaded implants and
leukocyte and platelet rich fibrin as sole grafting material: a six year experience
Implant Dent 2011;20:2-12.
61. Lee JW, Kim SG, Kim JY, Lee YC, Choi JY, Dragos R. Reconstruction of a
peri-implant defect by platelet rich fibrin. Oral Surg Oral Med Oral Pthol Oral
Radiol endod 2011.

Bibliography
62. Dohan Ehrenfest DM, Bielecki T, Jimbo R, Barbe G, Del Corso M, Inchingolo F
et al. Do the fibrin architecture and leukocyte content influence the growth factor
release of platelet concentrates. An evidence based answer comparing a pure
platelet rich plasma(P-PRP) gel and a leukocyte and platelet rich fibrin(L-PRF).
Curr Pharm Biotechnlol 2012;13:1145-52.
63. Jankovic S, Aleksic Z, Milinkovic I, Dimitrijevic B. The coronally advanced flap
in combination with platelet rich fibrin(PRF) and enamel matrix derivative in the
treatment of gingival recession: a comparative study. Eur J Esthet Dent
2010;5:260-73.
64. Vinaya kumar R, Shubhashini N. Platelet rich fibrin: A new paradigm in
periodontal regeneration cell tissue bank 2012.
65. Tunali M, Ozdemir H, Kucukodaciz Z, Akman S, Firath E. In vivo evalution of
titanium prepared platelet rich fibrin: A new platelet concentrate. Br. J Oral
Maxillofac Surg 2012.
66. Del Corso M, Vervelle A, Simonpieri A, Jimbo R, Inchingolo F, Sammartino G.
Current knowledge and perspectives for the use of platelet rich plasma(PRP) and
platelet rich fibrin(PRF) in oral and maxillofacial surgery part I: Periodontal and
dentoalveolar surgery. Curr Pharm Biotechnol 2012;13:1207-30.

Bibliography
67. Peck MT, Marnewick J, Stephen LX, Singh A, Patel N, Majeed A. The use of
leukocyte and platelet rich fibrin to facilitate implant placement in bone-deficient
sites: A repot of two cases. SADJ 2012;67:54-6,58-9.
68. Khiste SV, Naik Tari R. Platelet rich fibrin as a biofuel for tissue regeneration.
ISRN Biomaterials 2013; Article ID 627367:6 Pages.
69. Yosif A, Al-Hijazi A. Evaluation of the effect of autologous platelet rich fibrin
matrix on osseointegration of the titanium implant immunohistochemical
evaluation for PDGF-I and IGF-A. J Bagh college Dentistry 2013;25(1):70-5.
70. Gassling V, Purcz N, Braesen JH, Will M, Gierloff M, Behrens E. Comparision
of two different absorbable membranes for the coverage of lateral osteotomy
sites in maxillary sinus augmentation: A Preliminary study. J Craniomaxillofac
Surg 2013;41:76-82.
71. McLellan J, Sarah Plevin. Temporal release of growth factors from platelet rich
fibrin(PRF) and platelet rich plasma(PRP) in the horse: A comparative in vitro
Analysis. Intern J Appl Res Vet Med 2014;12(1)
72. Ozdemir H, Ezirganli S, Isa Kara M, Mihmanli A, Baris E. Effects of platelet
rich fibrin alone used with rigid titanium barrier. Arch Oral Biol 2013;58:537-44.
73. Bambal D, Manwar NU, Chandak M, Rudagi K. A Comparitive evaluation of the
healing ability of bilateral periapical lesions treated with and without the use of
platelet rich fibrin. Todays FDA 2012;24:54-7.
Bibliography
74. Oda T.,Kinshita and Ueda M.:effect of cortical bone perforation on periosteal
Destruction. J Maxillofacial Surg 2009; 67 (7)1478-85.
75. Carroll RJ, Arnoczky SP, Graham S, O’Connell SM. Characterization of
autologous growth factors in cascade platelet rich fibrin matrix(PRFM).
Musculoskeletal Transplant Foundation. Edison NJ 2005.
76. Nikitas S and Lynne AO. Bone morphogenic proteins (BMPs): How do they
function what can they offer the clinician? J Oral Sci 2003;45:57-73.
77. Carlson NE, Roach RB. Platelet rich plasma clinical applications in dentistry.
JADA 2002;133:1383-1386.
78. Tatullo M, Marrelli M, Cassetta M, Pacifici A, Stefanelli LV, Scacco S et al.
Platelet rich fibrin in reconstructive surgery of atrophied maxillary bones; clinical
and histological evaluations. Int. J med Sci 2012 Nov 9(10):872-80.
79. Sclafani AP. Platelet rich-fibrin matrix for improvement of deep nasolabial folds.
J Cosmet Dermatol. 2010 Mar;9[1]:66-71
80. Jankovic S, Aleksic Z, Klokkevold P, Lekovic V, Dimitrijevic B, Kenny EB,
Camargo P. Use of platelet rich fibrin membrane following treatment of gingival
recession: a randomized clinical trial. Int J Periodontics Restrorative Dent
2012;32(2):e41-50

Bibliography
81. Jansen RC, Reinink K, Vander Heijden GWAM. Analysis of grey level
histograms by using statistical methods for mixture of distributions. Pattern
recognition letters 1993;14:585-590.
82. Kumar VR, Gangadharan G. Platelet rich fibrin in dentistry: A review of
literature. Int J Of Med 2015;3(2):72-76
83. Raaj V, Gautam A, Abhishek, Kumari P. Platelet Rich Fibrin(PRF): A New
Generation Platelet Concentrate. Int J Dent Med Res 2015;1(6):164-67
84. Reddy S, Prasad MGS, Singh S, Krishnanand P, Bhowmik N. Enhancing palatal
wound healing by using platelet rich fibrin membrane as fibrin bandage. Int. J Of
App. Dent. Sci. 2015;1(4):02-04.


CONSENT FORM
PART 1 OF 2 INFORMATION FOR PARTICIPANTS OF THE STUDY
1. Name of the Principal Investigator:
Dr.A.W.GODWIN SAJI,
Post Graduate student,
Department of Oral and Maxillofacial surgery,
SreeMookambika Institute of Dental Sciences,
Kulasekharam, Kanyakumari District-629161
2. Name of the Guide: Dr. Mathew Jose,
Head of the department,
Department Of Oral and Maxillofacial Surgery.
SreeMookambika Institute of Dental Sciences,
Kulasekharam, Kanyakumari District-629161
Dear Volunteers, We welcome you and thank you for your keen interest in participation in this research
project. Before you participate in this study, it is important for you to understand why this research
is being carried out. This form will provide you all the relevant details of this research. It will
explain the nature, the purpose, the benefits, the risks, the discomforts, the precautions and the
information about how this project will be carried out. It is important that you read and understand
the contents of the form carefully. This form may contain certain scientific terms and hence, if you

3. Name of the Co-Guide: Dr.N.Dhineksh Kumar,
Professor,
Department Of Oral and Maxillofacial Surgery,
SreeMookambika Institute of Dental Sciences,
Kulasekharam, Kanyakumari District-629161
4. Institute:
SreeMookambika Institute of Dental Sciences,
V.P.M Hospital complex, Padanilam, Kulasekharam,
Kanyakumari – 629161
Tamil Nadu.
5. Title of the study :
“COMPARISION OF BONE REGENERATION IN THE EXTRACTION
SOCKETS WITH AUTOLOGOUS PLATELET RICH FIBRIN GEL - AN
INVIVO STUDY
6. Background information: Platelet concentrates for surgical use are tools of regenerative medicine designed for the local
release of platelet growth factors into a surgical or wounded site, in order to stimulate tissue
healing or regeneration. PRF preparation is very simple wherein the blood is collected without
any anticoagulant and immediately centrifuged at 3000 rpm for 10 minutes. Growth factors are
proteins or polypeptides capable of initiating the proliferation of cells that are in a quiescent
state by stimulating deoxyribose nucleic acid synthesis and progression of the cell cycle. They
are a class of multifunctional biologic mediators which regulate connective tissue cell migration,
proliferation, synthesis of proteins and capable of affecting all growth, differentiation,
angiogenesis, inflammation, tissue repair and immune response. The present study is aimed at
the comparison of bone regeneration in extraction sockets with autologous platelet rich fibrin gel.
7. Aim and objectives:
To evaluate the effects of autologous platelet rich fibrin gel on bone regeneration in extraction socket
8. Scientific justification of the study:
Platelets are a nucleate cytoplasmic fragments derived from bone marrow
megakaryocytes and measure 2–3 micron in diameter. The alpha granules are spherical or
oval structures with diameters ranging from 200 to 500 nm each enclosed by a unit
membrane. They form an intracellular storage pool of proteins vital to wound healing,
including platelet-derived growth factor (PDGF), transforming growth factor beta (TGFb),
and insulin-like growth factor (IGF-I).7These growth factors promote cell proliferation,
collagen synthesis, osteoid production etc.7 PRF is an autologous platelet concentrate that can
be effectively used in repair and regeneration of the periodontal tissues.
9. Procedure for the study:
• Under aseptic condition local anesthesia given
• Extraction done with appropriate forceps
• 4ml venous blood drawn from patient
• PRF has been prepared by centrifugation with 3000rpm for 10 min.
• PRF has been placed in extraction socket.
• Post-op record has been maintained to measure the bone regeneration.
10. Expected risks for the participants:
The needle stick for drawing the blood might cause pain,bleeding and thrombophlebitis at
injected site.
11. Expected benefits of research for the participants:
The blood will be used only for research which will better our understanding of PRF and
for advancement of medical knowledge. Benefit for prosthetic rehabilitation.
12. Maintenance of confidentiality:

• You have the right to confidentiality regarding the privacy of your medical
information(Personal details, results of physical examinations, investigations, and your
medical history).
• By signing this document, you will be allowing the research team investigators, other
study Personnel, sponsors, institutional ethics committee and any person or agency
required by law to view your data, if required.
• The results of clinical tests and therapy performed as part of this research may be
included in your medical record.
• The information from this study, if published in scientific journals or presented at
scientific meetings, will not reveal your identity.
13. Why have I been chosen to be in this study?
a. Chosen because of grouping under the inclusion and exclusion criteria
b. Need of good sampling size
c. Minimal radiation exposure that will notharm your health and helps inderiving the
normal facial proportions which will be useful as a guide for orthognathic surgery
for the society
d. To improve the aesthetic appearance.
14. How many people will be in the study? 30 individuals
15. Agreement of compensation to the participants (In case of a study related
injury): Patient will be taken care in case of complication and medical treatment will be provided in the
institution at the expense of the principal investigator.
16. Anticipated prorated payment, if any, to the participant(s) of the study: For your cooperation to the study, the expenses for the routine blood investigations for which
you originally visited the clinic will be settled by the principal investigator.
17. Can I withdraw from the study at any time during the study period?

The participation in this research is purely voluntary and you have the right to withdraw
from this study at any time during the course of the study without giving any reasons.
18. If there is any new findings/information, would I be informed? Yes
19. Expected duration of the participant’s participation in the study: 1 day
20. Any other pertinent information : No other information
21. Whom do I contact for further information?
Place: signature of principal investigator
Date:
Signature of the participant
For any study related queries, you are free to contact:
Dr.A.W.GODWIN SAJI
Post Graduate student.
Department of Oral & Maxillofacial Surgery,
SreeMookambika Institute of Dental Sciences,
Kulasekharam, Kanyakumari District-629161.
Mobile No: 08344841644
CONSENT FORM
PART 2 OF 2
PARTICIPANTS CONSENT FORM
The details of the study have been explained to me in writing and the details have been
fully explained to me. I am aware that the results of the study may not be directly beneficial to
me but will help in the advancement or medical sciences. I confirm that I have understood the
study and had the opportunity to ask questions. I understand that my participation in the study is
voluntary and that I am free to withdraw at any time, without giving any reason, without the
medical care that will normally be provided by the hospital being affected. I agree not to restrict
the use of any data or results that arise from this study provided such a use is only for scientific
purpose(s). I have been given an information sheet giving details of the study. I fully consent to
participate in the study titled
“COMPARISION OF BONE REGENERATION IN THE EXTRACTION
SOCKETS WITH AUTOLOGOUS PLATELET RICH FIBRIN GEL”
Serial no / Reference no :
Name of the participant :
Address of the participant :
Contact number of the participant :
Signature / thumb impression of the participant / Legal guardian
Witnesses:
1.
2.
Date: Place:

xg;Gjy; gbtk;
gFjp1-2
Ma;tpy; gq;Nfw;gtUf;fhd gbtk;
Ma;thsh;
kU.m.tp. fhl;tpd; r[p
KJfiy gl;ljhhp
tha; kw;Wk; KfrPuikg;G gphpT
= %fhk;gpfh gy; kUj;Jtkid
fy;Y}hp
FyNrfuk;
fd;dpahFkhp khtl;lk;
topfhl;b
kU.Nkj;A N[h];
Nguhrphpah; jiyikahsh;
tha; kw;Wk; KfrPuikg;G gphpT
= %fhk;gpfh gy; kUj;Jtkid
kjpg;gpw;Fhpa jd;dhu;tyNu
jhq;fs; ,e;j Ma;tpy; gq;Nfw;f te;jikf;F ed;wp. ,e;j
Ma;tpy; gq;Nfw;gjw;F Kd; ,e;j Ma;tpd; KOtpguq;fisAk;
cq;fSf;F njhptpf;Fk; Ma;tpy; gq;Nfw;gjw;F Kd; ,e;jgbtj;ij
KOtJk; gbj;J Ghpe;J nfhz;l gpd; gq;Nfw;f Ntz;Lk;. ,e;j
gbtj;jpy; rpy kUj;Jt kw;Wk; mwptpay; nrhw;fs; cs;sd.
Mjyhy; VNjDk; re;Njfq;fs; Vw;gl;lhy;. ,e;j gbtj;jpd; ,Wjpapy;
Fwpg;gpl;Ls;s eghplk; Ma;tpy; gq;Nfw;gjw;F Kd; njspT ngw
Ntz;Lk;.
fy;Y}hp
FyNrfuk;
fd;dpahFkhp khtl;lk;
Jiztopfhl;b
kU.jpNd~;f; Fkhh;
Nguhrphpah;
tha; kw;Wk; KfrPuikg;G gphpT
= %fhk;gpfs gy; kUj;Jtkid
fy;Y}hp
FyNrfuk;
fd;dpahFkhp khtl;lk;
Ma;T epiyak;
= %fhk;gpfh gy; kUj;Jtkid
fy;Y}hp
FyNrfuk;
fd;dpahFkhp khtl;lk;
1. jiyg;G :
gy; vLj;j gFjpapy; gp.Mh;v/ itj;Jk; gp.Mh;. v/
itf;fhkYk; vYk;G cUthFjiy xg;gpLjy;.
2. Ma;tpd; gpd;gyk;:
gpNyl;yl; itj;J fhag;gl;l rij Fzg;gLj;Jjy;, vYk;G
cUthf itj;jy; Nghd;w ed;ikfs; cz;L.

,e;j Muha;rpapd; %yk; gp.Mh;. v/ gy; vLj;j ,lj;jpy;
itj;J vYk;G cUthf itj;jy;.
3. FwpNfhs;:
Ma;tpy; gq;Nfw;NghUf;F gy; vLj;j gFjpapy; cs;s vYk;G
gw;whf;Fiwia gp.Mh;.v/ %yk; rhp nra;jy;.
4. mwptpay; gpd;fyk; :
Kd; fhyq;fspy; elj;jg;gl;l Ma;tpy; fhag;gl;l rij gFjp
,oe;j vYk;G gFjp gp.Mh;.v/ itg;gjpd; %yk; rhp nra;tJ
epUgpf;fg;gl;Ls;sJ.
5. nray; Kiw:
• jhq;fs; ,e;j Ma;tpy; gq;F ngw;w gpd; jdp ,yf;f vz;
nfhLf;fg;gLk;.
• ,e;j Ma;tpd; tpsf;f Kiw czh;j;jg;gl;L gpd; xg;Gjy;
gbtk; ifnahg;gk; ngwg;gLk;.
• gy; vLj;j gFjpapy; ,oe;j vYk;G gFjpia gp.Mh;.v/ itj;J
rhpnra;jy;.
• vYk;G cUthFjy; fjph;tPr;R glk; %yk; cWjp nra;ag;gLk;.
6. vjph;kiw tpisTfs;- ,y;iy
7. Vw;gLk; ed;ikfs;
• ,oe;j vYk;G gFjp cUthf;fg;gLk;
• fhag;gl;l rij gFjp rPf;fpuk; rhp nra;jy;
8. jftypd; ghJfhg;G
• cq;fSila jfty;fs; midj;Jk; ghJfhf;fgLk; ve;j
epiyapYk; ntspaplg;glhJ.

• ePq;fs; ,e;j Ma;tpy; gq;Nfw;wgpd; vq;fsJ Ma;thsh;
cq;fSila jfty;fis njhpe;J nfhs;s KbAk;. NkYk;
Njit Vw;gl;lhy; vj;jpf;fy; fkpl;baplKk; fhz;gpf;fg;gLk;.
• Ma;tpd; Kbtpd; cq;fSila kUj;Jt jfty; gbtj;jpy;
(Nfhg;gpy;) gjpT nra;ag;gLk;.
• ,e;j Ma;T KbT ntspaplgLk; nghOJ cq;fsJ jfty;fs;
ntspaplg;glhJ.
9. ,e;j Ma;tpy; ePq;fs; Nrh;tjw;fhd fhuzk;?
• ePq;fs; ,e;j Ma;tpd; Nrh;g;G kw;Wk; tpLg;G tFg;Gfspd;
cs; mikg;gLtjhy;
• Ma;tpd; Njitahd khjphpf;fhfTk;
• r%fj;jpd; kw;Wk; kUj;Jt Kd;Ndw;wj;jpw;fhf
10. Ma;tpd; khjphp vz;zpf;if : 30
11. e~;laPL :
Ma;tpy; Vw;gLk; khw;wq;fSf;fhd rpfpl;ir Ma;T epiyaj;jpy;
toq;fg;gLk;.
12. e~;;;;laPL gzk; :gzk; vJTk; toq;fglhJ
13. Ma;tpy; ,Ue;J ve;j Neuj;jpYk; ve;j fhuzKk; ,d;wp tpyfyhk;
14. Ma;tpd; Kd;Ndw;wj;jpy; Vw;gLk; khw;wq;fs; njhptpf;fg;gl Ntz;Lk;.
15. Ma;tpd; fhy mtfhrk;: MW khjk;
16. NtW ve;j jfty;fSk; Njit ,y;iy.

17.
,lk;:FyNrfuk; Ma;thsh; ifnahg;gk;
Njjp:
gq;FngWgth; ifnahg;gk;
kU. .m.tp.fhl;tpd; r[p
KJfiy gl;ljhhp
tha; kw;Wk; KfrPuikg;G gphpT
= %fhk;gpfh gy; kUj;Jtkid
fy;Y}hp
FyNrfuk,; fd;dpahFkhp khtl;lk;
njhiyNgrp vz;:8344841644
kpd; mQ;ry; - [email protected]
Xg;Gjy; gbtk;
gFjp-2
gq;FngWgthpd; xg;Gjy; gbtk;
,e;j Ma;tpd; KO tpguq;fSk; vOj;J %ykhfTk; tphpthfTk;
vd;dplk; $wg;gl;lJ. vdf;F ,e;j Ma;tpd; tpisTfs; ve;j
gaDk; jutpy;iy vd;whYk; kUj;Jt mwptpaypd; Nkk;ghl;bw;fhf
gad;gLj;jg;gLk; vd;W mwpNtd;. ehd; ,e;j Ma;tpy; ve;j
eph;ge;jKk; ,y;yhky; gq;F ngWfpNwd;. NkYk; ,e;j Ma;tpd;
vy;yh tpjpfs; kw;Wk; tpjpKiwfisAk; mwpNtd;. ve;j
re;Njhfj;jpw;Fk; Nfs;tp Nfl;fNth my;yJ Ma;tpy; ,Ue;J
tpyfNth vy;yh chpikfSk; vdf;F cz;L vd;W mwpNtd;. ,e;j
Ma;tpd; tpisTfs; ve;j mwptpay; gad;ghl;bw;Fk; gad;gLj;j
vdf;F jilapy;iy. vdf;F ,jw;F Kd;ghf Ma;tpd; jfty;
gbtk; nfhLf;fg;gl;lJ. vdf;F ,e;j Ma;tpy; gq;Fngw KO
rk;kjk;.
Ma;tpd; ngah;
gy; vLj;j gFjpapy; gp.Mh;.v/ itj;Jk; gp.Mh;.v/ itf;fhkYk;
vYk;G cUthFjiy xg;gpLjy;.
Fwpg;G vz;:
ngah;:
Kfthp:
njhiyNgrp vz;:
rhl;rp 1: ifnahg;gk;
2.
,lk;:FyNrfuk;
Njjp:
k½X ]{Xw
`mKw þ 1
]T\hpambn klIcn¡p¶ hyànIfpsS Adnhntebv¡v
{]nbs¸« k¶² tkhI³ / tkhI,
R§Ä \n§sf kzmKXw sN¿p¶p. AtXmsSm¸w Cu ]T\hpambn klIcn¡m\pÅ k¶²XtbmSv \μn tcJs¸Sp¯p¶p. \n§Ä Cu ]T\¯n ]s¦Sp¡p¶Xn\p ap³]v Cu ]T\w F´n\mWv \S¯s¸Sp¶Xv F¶v Andtb−Xp−v. AXn\m Cu t^md¯n KthjW ]T\¯nsâ hnhc§fpw aäpw hniZambn tcJs¸Sp¯nbncn¡p¶p. Cu ]T\¯nsâ coXn, Dt±iw, {]tbmP\w, A]ISkm²yX, t¢iw, ap³IcpXÂ, F§s\ Cu ]T\w ap³t]m«p sIm−pt]mIp¶p F¶n§s\ FÃm hnhc§fpw t^md¯n tcJs¸Sp¯nbncn¡p¶p. kZbw Cu hnhc§Ä hmbn¨p a\Ênem¡phm³ A`yÀ°n¡p¶p. Cu hnhc§fn imkv{X]camb ]Z§Ä DÅXn\m kwib\nhmcW¯n\p {][m\ ]T\IÀ¯mhnt\mtSm Xmsg tcJs¸Sp¯n bncn¡p¶ hyànItfmtSm t^mdw H¸nSp¶Xn\p ap³t]m Asæn Cu ]T\¯nsâ Imemh[n Xocp¶Xphtctbm kao]n¡mhp¶XmWv.
1. apJy KthjI³ : tUm. F. hn. KmUvhn³ kPn t]mÌp{KmPpthäv Un¸mÀ«vsaâv Hm^v amIvkntemt^jy kÀPdn {io aqImw_nI C³Ìnäyq«v Hm^v sUâ kb³kv, IpetiJcw þ 629 161.
2. amÀ¤ ZÀin : tUm.amXyq tPmkv s{]m^kÀ & slUv Hm^v Zn Un¸mÀ«vsaâv,
Un¸mÀ«vsaâv Hm^v amIvkntemt^jy kÀPdn {io aqImw_nI C³Ìnäyq«v Hm^v sUâ skâÀ, IpetiJcw 3 kl amÀ¤ZÀin : tUm. Znt\jvIv IpamÀ
{]m^kÀ Un¸mÀ«vsaâv Hm^v amIvkntemt^jy kÀPdn {io aqImw_nI C³Ìnäyq«v Hm^v sUâ kb³kkv, IpetiJcw.
4. C³Ìnäyq«v : {io. aqImw_nI C³Ìnäyq«v Hm^v sUâ kb³kkv ]S\new, IpetiJcw, I\ymIpamcn þ 629 161. Xangv\mSv.

5. ]T\¯nsâ ioÀjIw :
]sÃSp¯ `mK¯n ]n.BÀ.F^v. h¨n«pw ]n.BÀ.F^v ssh¡msXbpw FÃm−mIp¶ Afhnsâ XmcXays¸Sp¯Â 6. ]Ým¯e hnhcw ? t¹äpseäv h¨v apdnhp`mK¯v icnbm¡p¶Xpw FÃp−mIp¶ \·Ifpw km[yamWv. Cu ]T\¯n ]n.BÀ.F^vþs\ ]sÃSp¯Øe¯v FÃv hfcm³ sN¿pI. 7. e£y§fpw Dt±i§fpw ]T\¯n ]s¦Sp¯hÀ¡v ]sÃSp¯ Øe¯pÅ FÃnsâ hfÀ¨ Ipdhns\ ]n.BÀ.F^v h¨v icnbm¡p¶Xv.
8. KthjWw \S¯m\pÅ \ymboIcWw CXn\p ap³]pÅ ]T\¯n apdnhpÅ Øe¯pw FÃp IpdhpÅ Øe¯pw ]n.BÀ.F^v. h¨v FÃnsâ hfÀ¨ \nco£n¨n«p−v.
9. KthjWcoXn • Cu KthjWhpambn klIcn¡p¶hÀ¡v Hcp \¼À \ÂIp¶XmWv.
• Cu KthjW coXn t_m[n¸n¨n«v AhcpsS ssI¿n \n¶pw k½X]{Xw hm§p¶XmWv.
• ]sÃSp¯ `mK¯v IpdhpÅ FÃp`mK¯n ]n.Bcv.F^v ssh¡Â.
• FÃv hfÀ¨ FIvkvtd aptJ\ Adnbmhp¶XmWv.
10. {]Xo£n¡p¶ A]IS km²yXIÄ þ CÃ
11. Cu ]T\¯n ]s¦Sp¡p¶XpsIm−v F\n¡v Fs´¦nepw D]tbmKapt−m ? t\cn«v {]tbmP\§Ä H¶pw CÃ. F¶ncp¶mepw IpdhpÅ FÃp`mK¯v ]n.BÀ.F^v hbv¡p¶Xpaqew FÃnsâ Ipdhv \nhÀ¯n sN¿m³ km[n¡p¶p. 12. Xm¦sf ]änbpÅ hnhc§Ä FÃmw clkyambn kq£n¡p¶XmtWm ? XoÀ¨bmbpw kq£n¡p¶XmWv. 13. Fs¶ F´psIm−v Cu ]T\¯n DÄs¸Sp¯n ? Xm¦Ä Cu KthjW¯n ]s¦Sp¡p¶Xn\v tbmKyXbmbXpsIm−v Xm¦sf R§Ä Cu ]co£W¯n\v hnt[bam¡n. 14. Ft¸mÄ thWsa¦nepw F\n¡v Cu ]T\¯n \n¶v ]n³amdmtam Xm¦Ä¡v Cu ]co£W¯n ]¦p sImÅp¶Xn\pw ]n·mdp¶Xn\pw ]qÀ®hImiap−v. ]co£W¯n ]¦psImÅp¶Xn\pw CSbn ]n·mdp¶Xnepw Xm¦fpsS NnInÕbv¡v GXphn[ _p²nap«pIfpw GÀs¸Sp¶XÃ.

15. Cu KthjW¯nsâ ^eambn ]pXnb Fs´¦nepw Is−¯epIfps−¦n AXv Fs¶ Adnbn¡ptam ? Cu ]T\¯nsâ Is−¯epIÄ ]T\ Ahkm\w XoÀ¨bmbpw \n§sf Adnbn¡p¶Xmbncn¡pw. 16. Cu ]co£W¯n GsX¦nepw ]pXnbXmbn I−p]nSn¡s¸«m Fs¶ Andbn¡ptam ? AsX Cu ]co£W¯nsâ Ahkm\w GsX¦nepw ]pXnbXmbn I−p]nSn¨m AXv XoÀ¨bmbpw Xm¦sf Adnbn¡p¶XmWv. 17. Cu ]T\¯nsâ kab ssZÀLyw F{XbmWv ? Bdp amkw 18. Cu ]T\¯nsâ F{Xt]cmWv ]s¦Sp¡p¶Xv. 30 t]À 19. Cu KthjW¯n ]s¦Sp¡p¶hÀ¡v Fs´¦nepw B\pIqeyw e`n¡ptam ? KthjW sNehv ]qÀ®ambpw KthjI³ sNehp hln¡p¶XmWv. 20. Cu KthjW¯n ]s¦Sp¡p¶hÀ¡v \ã ]cnlmcw e`n¡ptam ? Cà 18. IqSpX hnhc§Ä¡mbn Xmsg ]dbp¶hsc \n§Ä¡v _Ôs¸Smhp¶XmWv. tUm. F. hn. KmUvhn³ kPn t]mÌp{KmPpthäv Un¸mÀ«vsaâv Hm^v amIvkntemt^jy kÀPdn {io aqImw_nI C³Ìnäyq«v Hm^v sUâ kb³kv, IpetiJcw þ 629 161. skÂ:8344841644 C.sabnÂ: [email protected] Øew: IpetiJcw XobXn :

k½X]{Xw
`mKw þ 2
Cu ]T\s¯ ]änbpÅ FÃm Imcy§fpw F\n¡v ]dªv a\Ênem¡n XcnIbpw AXnsâ Hcp ]IÀ¸v F\n¡p \ÂIpIbpw sNbvXn«p−v. Cu ]T\w KthjW¯n\mbn DÅXmsW¶pw F\n¡v CXn \n¶v t\cn«v Hcp ^ehpw D−mInsöpw Rm³ a\Ênem¡p¶p. Cu ]T\¯nsâ coXnbpw Dt±ihpw F\n¡v a\Ênem¡n X¶n«p−v. AXp t]mse F\n¡v kwib§Ä tNmZn¡m³ Ahkc§Ä e`n¨n«pap−v. CXn ]s¦Sp¡m\pw ]s¦Sp¡mXncn¡m\pw DÅ AhImiw F\n¡ps−¶pw AXpt]mse ]T\¯nsâ GXp L«¯nepw CXn \n¶v ]n³h§m\pÅ kzmX{´yhpw F\n¡ps−¶v Rm³ a\Ênem¡p¶p. Cu ]T\¯n ]s¦Sp¡p¶XpsImt−m, ]s¦Sp¡m¯XpsImt−m Fsâ aäp NnInÕIsf _m[n¡p¶Xsöv Rm³ Andbp¶p.
“FsÃSp¯ `mK¯n ]n.BÀ.F^v. h¨n«pw ]n.BÀ.F^v ssh¡msXbpw FÃm−mIp¶ Afhnsâ XmcXays¸Sp¯Â .” F¶ KthjW¯n ]s¦Sp¡p¶Xn\pw CXnsâ ^e§Ä imkv{XteJ\¯n {]kn²oIcn¡p¶Xn\pw F\n¡v k½XamsW¶v Rm³ CXn\m Andbn¨psImÅp¶p.
kocnb \¼À / d^d³kv \¼À :
]s¦Sp¡p¶ Bfnsâ t]cv :
taÂhnemkw :
t^m¬ \¼À :
H¸v / hnceSbmfw
km£n :
Øew :
XobXn





























