Embed Size (px)
Citation preview
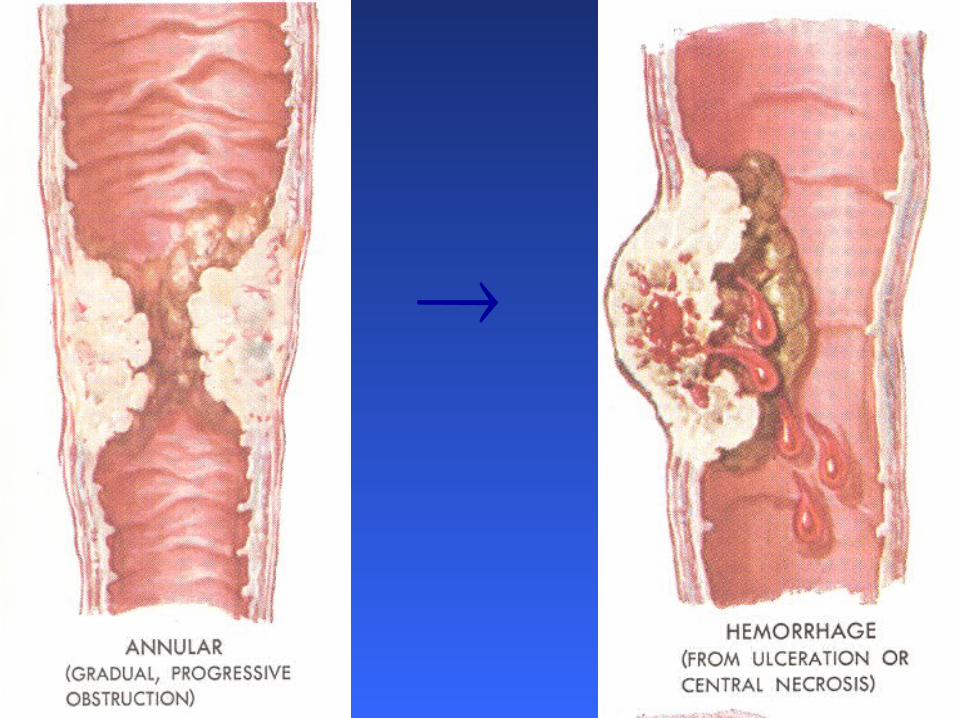
Colon-Rectal Cancer
Keith Bradley, MD
National Alliance of Research Associates Programs
NARAP
Colon-Rectal Cancer
• 2nd leading cause of cancer deaths in U.S.
Colon-Rectal Cancer
• 2nd leading cause of cancer deaths in U.S.
• complex interactions between inherited susceptibility and environmental risk factors
Risk Factors
• Inherited
• Acquired
Inherited Risk Factors
• age > 40
• personal hx of colon-rectal cancer
• Ulcerative colitis or Crohn’s disease
• family (parents or siblings) hx of
– colon-rectal cancer or – adenomas before age 60
• Familial polyposis
Acquired Risk Factors• diet
high in low in – saturated fat - calcium– protein - folate– calories– meat (both red and white)– alcohol
• sedentary lifestyle
• smoking cigarettes
Decreased Risk
• low-fat, high-fiber diet
• nonsteroidal anti-inflammatory drugs
• post menopausal female hormone use
• polyp removal
Colon-Rectal Cancer
• 2nd leading cause of cancer deaths in U.S.
• complex interactions between inherited susceptibility and environmental risk factors
• number of new cases and deaths due to colon-rectal cancer has been decreasing
Screening
• fecal occult blood test
• flexible sigmoidoscopy
• colonoscopy
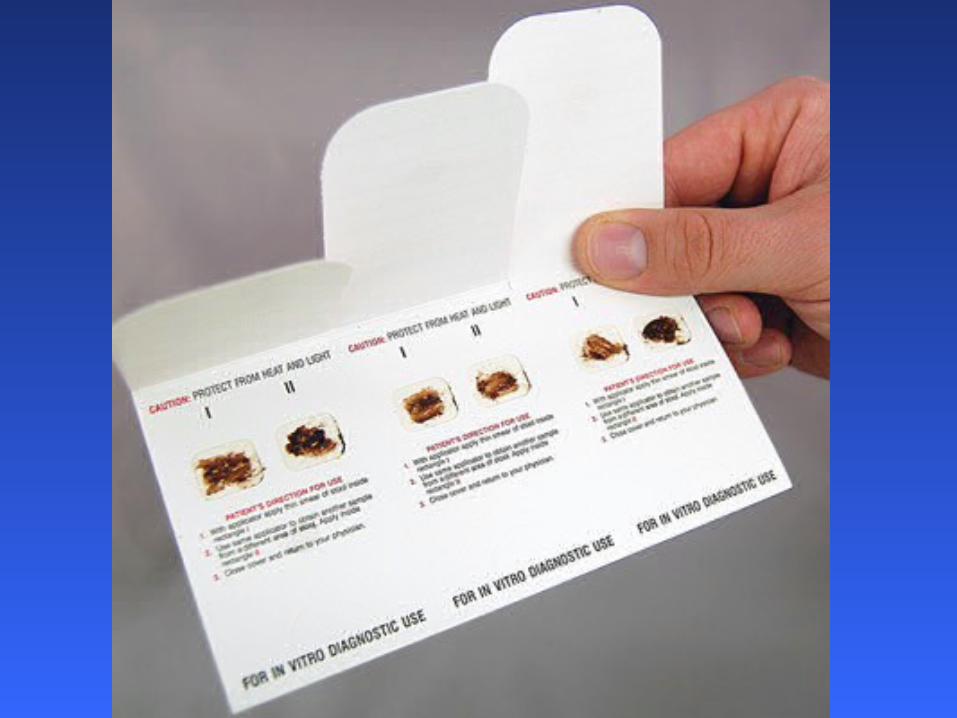
Fecal Occult Blood Test
• special cards are coated with a stool sample and returned to the physician or lab

Fecal Occult Blood Test
• special cards are coated with a stool sample and returned to the physician or lab
• fecal occult blood test
performed every 1 or 2 years
in people between the ages of 50-80 years decreases deaths due to colorectal cancer by 20 – 40%
Flexible Sigmoidoscopy• a thin, lighted tube (sigmoidoscope)
into rectum and only the descending colon• most often done
– in a doctor’s office or clinic– by a family practitioner (FP) or general internist
• patient remembers the procedure • polyps or other abnormal tissue
removed and biopsied• combined with FOBT every 3 years
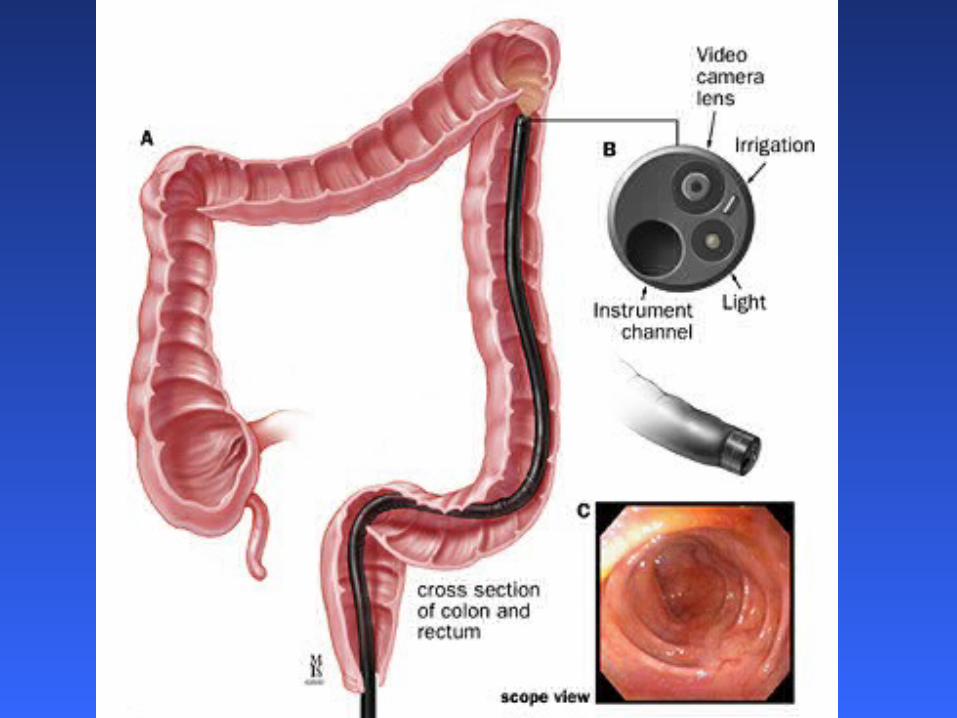
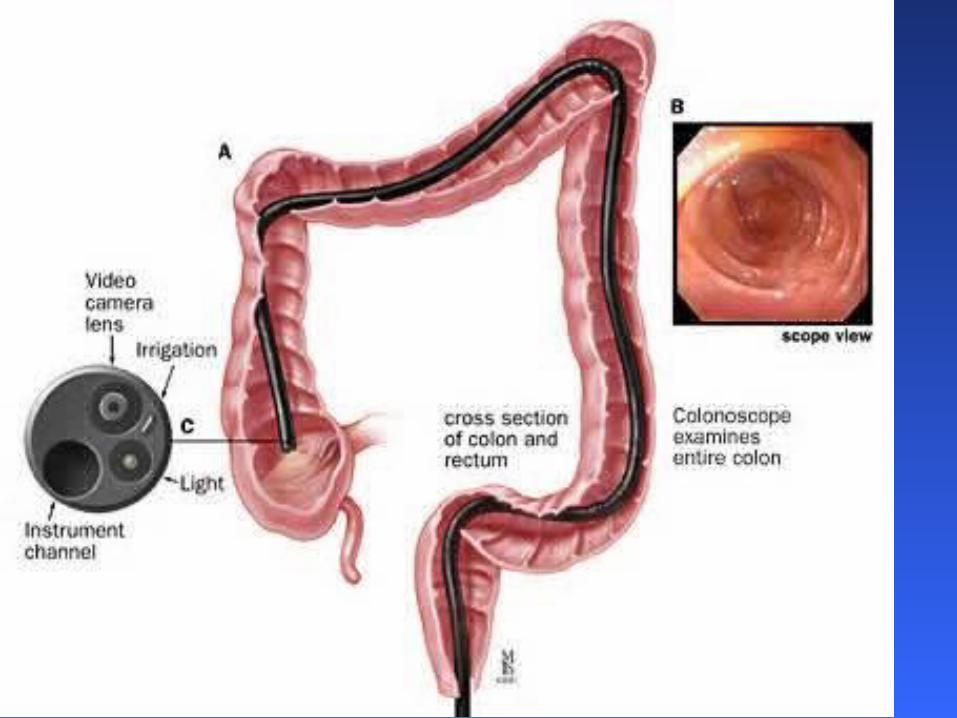
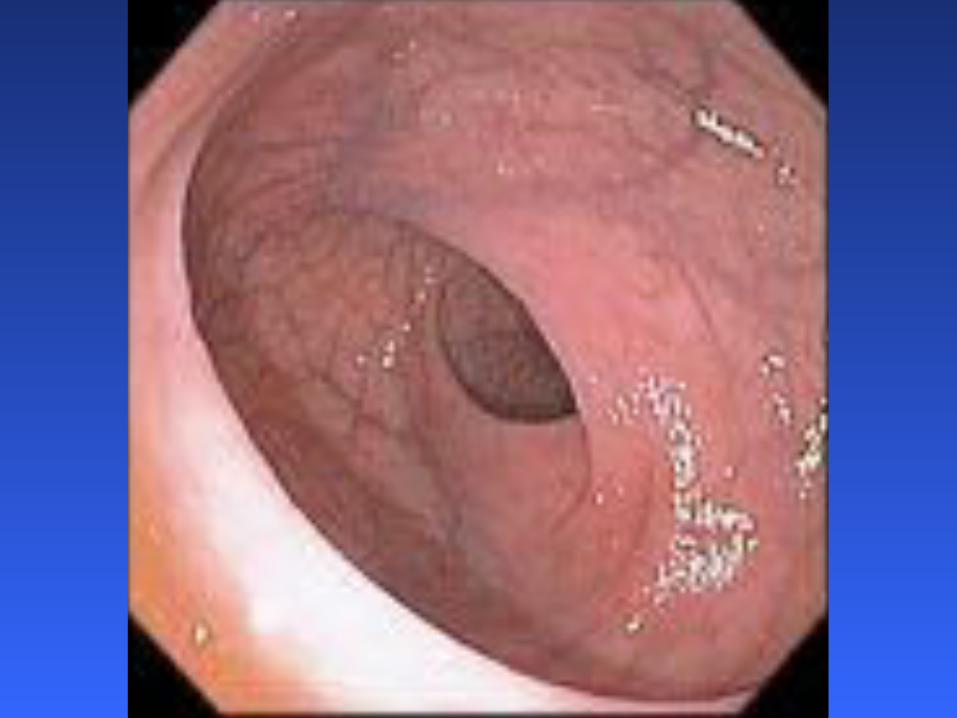
Colonoscopy
• a thin, lighted tube (colonoscope)
into rectum and through the entire colon• most often done
– in a hospital or specialized setting– by a gastroenterologist (but possibly a FP)
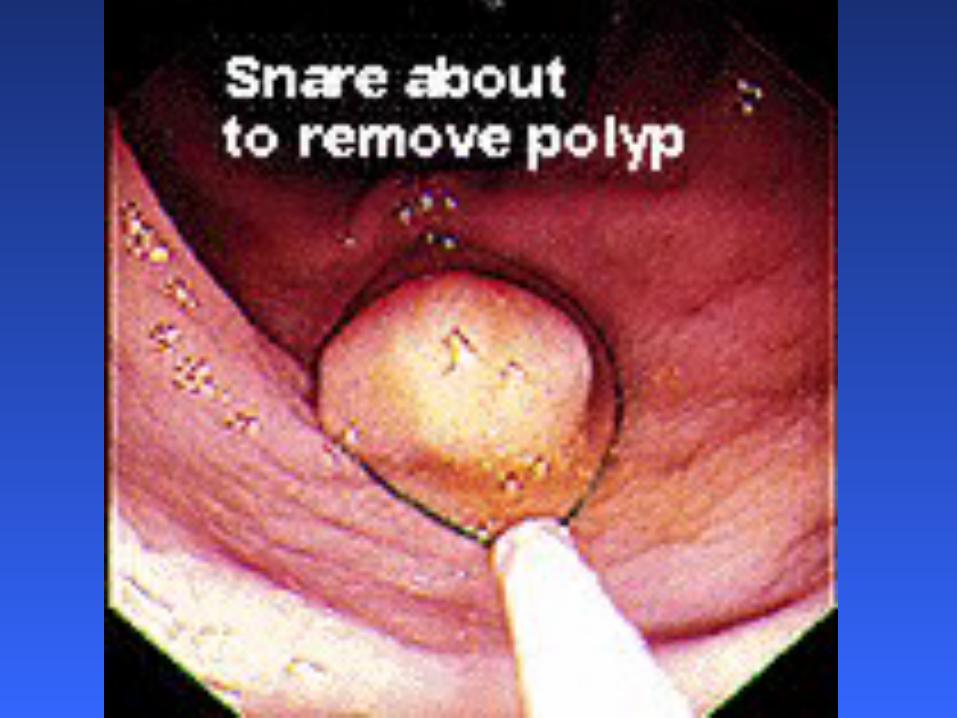
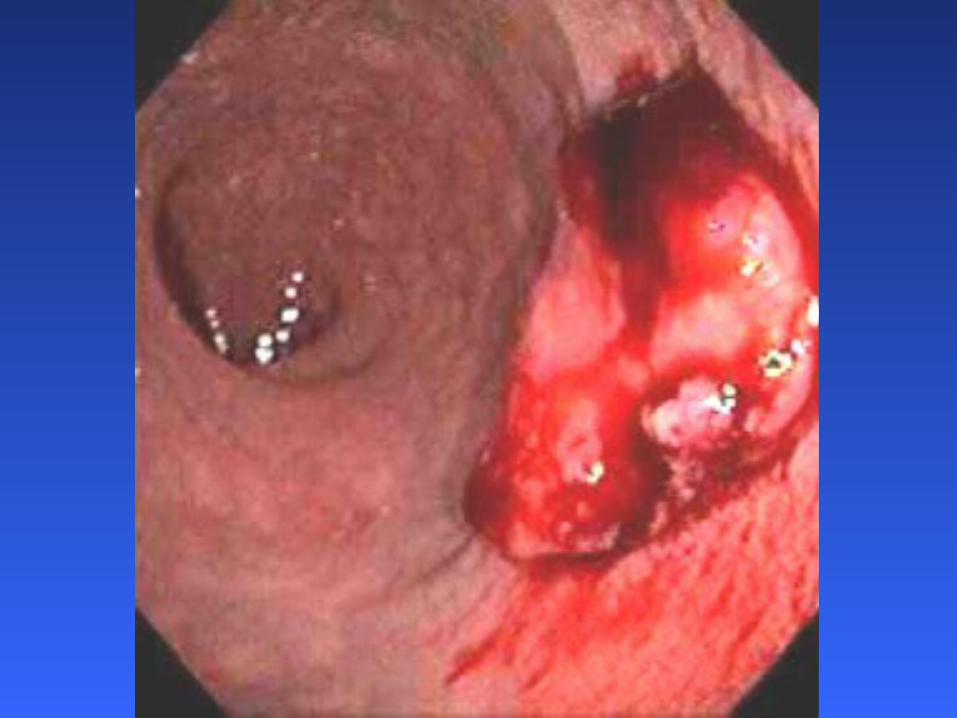
• under conscious sedation• polyps or other abnormal tissue
removed and biopsied

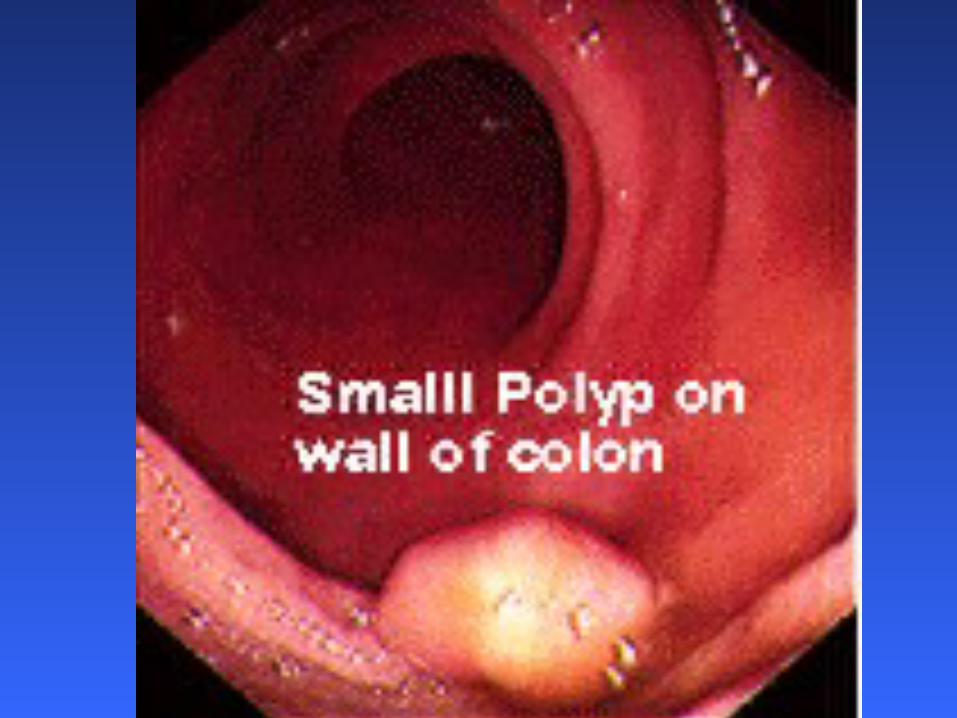
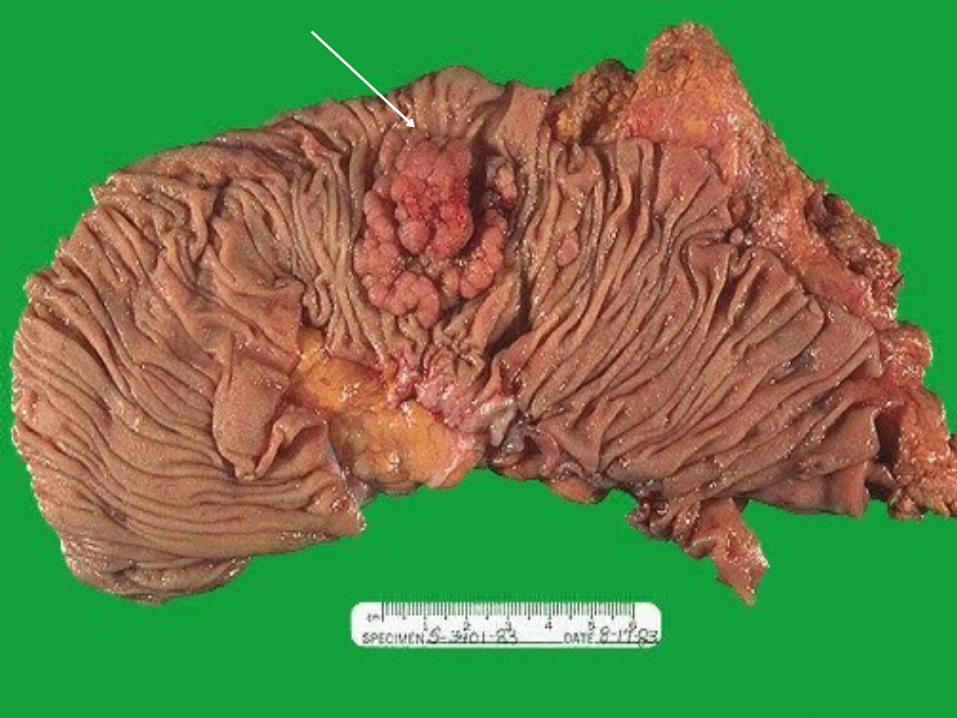
Polyps
• adenomas = precursors for vast majority of colorectal cancer
• most of these adenomas are polypoid

Colon-Rectal Cancer Screening
Fewer than 50% over age 50 get screened
Colon-Rectal Cancer Screening
Fewer than 50% over age 50 get screened
In a survey,
respondents who had never had a colonoscopy
said they would rather give up three months of life
than have the test.
United States Preventive Services Task Force(USPSTF) Recommendations
• Adults, beginning at age 50 years and continuing until age 75 years
• Options– annual screening with a sensitive FOBT – flexible sigmoidoscopy every 5 years
with a mid-interval sensitive FOBT – colonoscopy every 10 years



























![Chassin's Operative Strategy in Colon and Rectal Surgery,(2006) [UnitedVRG]](https://img.dokumen.tips/doc/110x75/56d6c06f1a28ab30169a63d7/chassins-operative-strategy-in-colon-and-rectal-surgery2006-unitedvrg.jpg)
