Embed Size (px)
Citation preview
Research in Social and Administrative Pharmacy
1 (2005) 408–429
Collaborative medication managementin a team-based primary care practice:An explanatory conceptual frameworkq
Jana M. Bajcar, B.Sc. Pharm., M.Sc. Pharm.,Ed.D., FCSHPa,b,*, Natalie Kennie, B.Sc. Pharm.,Pharm.D.a,b, Thomas R. Einarson, B.Sc. Pharm.,
M.S.(Pharm.), M.Ed., Ph.D.a
aLeslie Dan Faculty of Pharmacy, University of Toronto, Toronto, CanadabDepartment of Family and Community Medicine, St Michael’s Hospital, Toronto, Canada
Abstract
Background: In ambulatory practice many different health care professionals are
involved in the drug use process. The roles and functions of these individuals can bedifficult to define, because of a lack of a common ground for discussion. Deliberatingthe topic is important for developing a team approach to medication management.Objective: To describe a conceptual framework to create a platform that can be used
by different health care providers to identify, define, and discuss roles andresponsibilities in collaborative medication management.Methods: Authors reviewed and reflected upon their experiences as practitioners in
implementing a pharmaceutical care–based consulting practice within a familymedicine practice setting. Key roles and responsibilities relative to collaborativemanagement of medications were identified and described.
q This research was not supported by external funding of any kind. The authors have no
conflict of interest to disclose concerning this paper.
* Corresponding author. Leslie Dan Faculty of Pharmacy, University of Toronto, 19 Russell
Street Toronto, ON M5S 2S2, Canada. Tel.: C1 416 978 4241; fax: C1 416 978 8511.
E-mail address: [email protected] (J.M. Bajcar).
1551-7411/$ - see front matter � 2005 Elsevier Inc. All rights reserved.
doi:10.1016/j.sapharm.2005.06.003

409J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
Results: A conceptual framework subsequently developed, the Team Approach toMedicationManagement, consists of 3 primary components referred to asmedication-
related practices (medication prescribing, medication taking, and medicationdispensing). Each of these primary practices is supported by a team of health careprofessionals who have supportive roles and responsibilities. In the TeamApproach to
Medication Management framework, the patient’s medication-taking practice holdsa central and key positionwithin a collaborative approach tomedicationmanagement.Conclusions: The proposed Team Approach to Medication Management frameworkcan be used to guide discussions and decisions among the different health care
providers working in primary care to define both direct and indirect roles that healthcare practitioners and patients play in collaborative medication management.� 2005 Elsevier Inc. All rights reserved.
Keywords: Pharmaceutical care; Model; Pharmacy practice; Collaborative medication
management; Health care team; Primary care
1. Introduction
There is a growing global trend toward a more collaborative approach tomedication management.1 One particular area of interest is the managementof medications in the primary care (ambulatory care) setting. In this setting,many different health care providers are involved in the management ofpatients’ medications. In fact, health care providers around the world havebegun to work together as partners to develop, test, and evaluate new modelsof service delivery aimed at improving patients’ medication outcomes.1-5
In Canada, a recent national report on the direction of primary caredelivery has emphasized the need to improve theway inwhich the componentsof medicationmanagement are linked within primary health care.6 The reportsuggested that the effectiveness of prescription drugs could be optimizedthrough ongoing monitoring by teams and networks of health care providersworking with individual patients. In fact, various examples of innovativecollaborative health service models involving physicians, pharmacists, andnurses have been developed and tested in different parts of the world.1
A more collaborative approach to medication management is neededbecause medication use has become more complex, especially in patientswith chronic illnesses. Current best practices in the management of manychronic illnesses, such as diabetes mellitus and cardiovascular conditions,require the use of multiple medications.7,8 Therefore, in some chronicillnesses, polypharmacy has become the standard rather than something thatshould (or can) be avoided. In addition, there has been a rapid increase inthe volume of available information on optimal medication use, whichincreases the complexity of illness management.
Recent literature suggests that patients are experiencing high rates ofadverse events traceable to the method of medication use in the ambulatory

410 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
care setting.9-12 For example, one study reported that medications wereresponsible for 28% of emergency visits.13 It is important to try to addressthese problems because medication-related problems are believed to bepreventable in more than 50% of the cases.11,14
Such medication-related problems are caused by various factors such as(a) inappropriate care [eg, inadequate monitoring of the patient’s drugtherapy (67%) and inappropriate dose (51%)]; (b) medication errors; and (c)patient noncompliance (33%).9,11,12,14 Ninety-eight percent of patients hadmore than one preventable factor.14 The most common causes of theseproblems were adverse drug reactions, noncompliance, lack of patienteducation, and inappropriate prescribing and monitoring.15
To help patients achieve the maximum therapeutic benefits and reducepreventable factors that contribute to adverse events, different health careprofessionals need to address the complexity of medication management inan integrated manner. To do this, health care providers must betterunderstand one another’s roles and responsibilities, as well as those of thepatients themselves, with respect to medication use. Thus, the involvedprofessionals need to find ways of working together and coordinating theirefforts to optimize the benefits that medications can offer to patients.
One practice environment in which collaborative approaches tomedication management is growing is in family practice.16-19 For the last10 years, two authors of this study (JB, NK), both practicing pharmacists,have taken part in developing and implementing a practice model in whicha clinical pharmacist works within an academic physician–based primarycare office affiliated with a university teaching hospital.20,21 The practicemodel is located within the community at 2 separate sites. A pharmacistwith advanced clinical training works in collaboration with 16 staff familyphysicians, 6 nurses, 2 social workers, 3 addiction counsellors, 1 dietician,and 1 occupational therapist. The pharmacist’s practice within this office isbased on the established philosophy of pharmaceutical care, a philosophythat provided the foundation for shaping the development of thepharmacist’s role.22 Patient-related consultations and questions are referredto the pharmacist by any member of the health care team. At the time of theconsult or question, the pharmacist examines the nature of the consult andidentifies the task and the associated medication-related issue. Thepharmacist then determines what type of activities or service(s) would bemost appropriate for the patient, considering the needs of the patient, theteam, and time available to complete the task.
2. Impetus for the framework
During the development, implementation, and evaluation of this site-specific practice model, we encountered 2 issues requiring creative solutionsand resulting in the gradual development of a conceptual framework, which

411J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
is the focus of this article. The first issue we encountered was the extensivenumber of players involved in medication management in family practice.Along with the family physician, the team includes the medical specialist,family practice pharmacist, community pharmacist, nurse, nurse practition-er, dietician, social worker, home care workers and, of course, the patientand his/her family. Some of these players are physically present in onelocation whereas others practice at a distant location, eg, the medicalspecialist or the community pharmacist. Often, medication managementroles and specific functions are difficult to define and thus, challenging todiscuss and negotiate. Over the years, many health care providers have haddifferent ways of defining their responsibilities in medication managementand had varied perceptions of the roles and responsibilities of others in theteam. In addition, patients have varied in their desire and ability toparticipate in their medication management.
As a result, we needed a way to define a platform, which could be used togain greater clarification of the medication management needs of this settingand the roles and responsibilities of the members of the team including thepatient and his/her family. To avoid potential ‘‘turf conflicts,’’ it wasimportant to find a way to discuss medication management issues based ongeneric components of medication management that were not based onpredefined roles of the different health care providers.
The second issue surfaced when we wanted to design a comprehensiveapproach to assess the impact of the pharmacist within this collaborativesetting. We also wanted to identify any unmet needs that could be used toidentify new opportunities and to guide further development of thepharmacist’s role. We needed to find a way, if possible, to isolate theunique contribution of the pharmacist to a patient’s care and what outcomeswould be sensitive to that contribution as opposed to those of the othermembers of the team.
3. Generation of the framework
To address these 2 issues, we reflected and identified 2 guiding principlesthat we felt were essential to consider in collaborative medicationmanagement. The first principle was the complexity of modern medicationuse requiring that different health care providers support and complementeach other’s roles. We needed an approach that could be used to describe thepotential roles or contributions of different team members and not that ofthe pharmacist alone. The second principle was that many medication issuesobserved in family practice fall outside the sphere of health care providers’direct control, but reside rather primarily within the patient’s domain. Thereason is that, in this setting, patients have the ultimate control over theirmedication use.23 This sentiment was captured by Glasgow and Anderson,who stated as follows:
412 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
‘‘Patients are in control. No matter what we as health careprofessionals do or say, patients are in control of these importantself-management decisions. When patients leave the clinic or office,they can and do veto recommendations a health professionalmakes.’’24
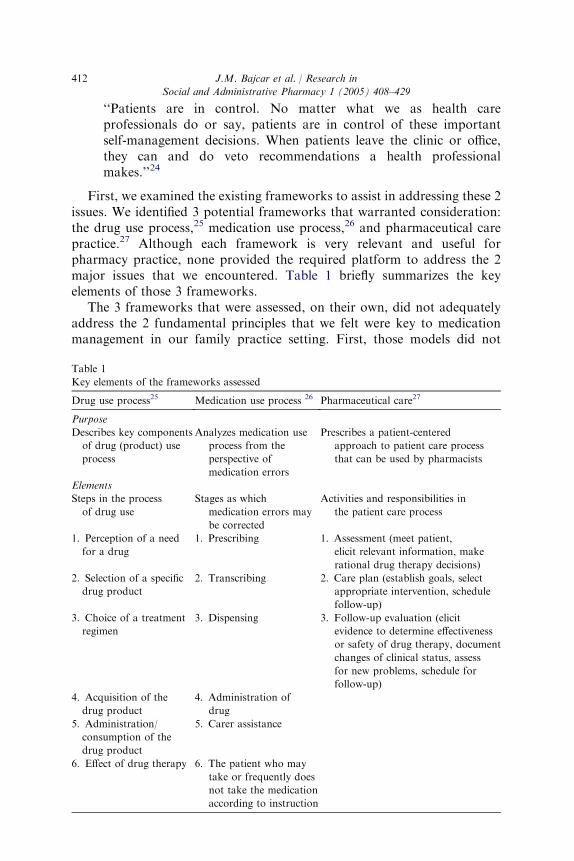
First, we examined the existing frameworks to assist in addressing these 2issues. We identified 3 potential frameworks that warranted consideration:the drug use process,25 medication use process,26 and pharmaceutical carepractice.27 Although each framework is very relevant and useful forpharmacy practice, none provided the required platform to address the 2major issues that we encountered. Table 1 briefly summarizes the keyelements of those 3 frameworks.
The 3 frameworks that were assessed, on their own, did not adequatelyaddress the 2 fundamental principles that we felt were key to medicationmanagement in our family practice setting. First, those models did not
Table 1
Key elements of the frameworks assessed
Drug use process25 Medication use process 26 Pharmaceutical care27
Purpose
Describes key components
of drug (product) use
process
Analyzes medication use
process from the
perspective of
medication errors
Prescribes a patient-centered
approach to patient care process
that can be used by pharmacists
Elements
Steps in the process
of drug use
Stages as which
medication errors may
be corrected
Activities and responsibilities in
the patient care process
1. Perception of a need
for a drug
1. Prescribing 1. Assessment (meet patient,
elicit relevant information, make
rational drug therapy decisions)
2. Selection of a specific
drug product
2. Transcribing 2. Care plan (establish goals, select
appropriate intervention, schedule
follow-up)
3. Choice of a treatment
regimen
3. Dispensing 3. Follow-up evaluation (elicit
evidence to determine effectiveness
or safety of drug therapy, document
changes of clinical status, assess
for new problems, schedule for
follow-up)
4. Acquisition of the
drug product
4. Administration of
drug
5. Administration/
consumption of the
drug product
5. Carer assistance
6. Effect of drug therapy 6. The patient who may
take or frequently does
not take the medication
according to instruction
413J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
adequately identify all the potential key players who contribute tomedication management. They instead focused on either the drug product,the medication use process from the perspective of medication errors, or onthe patient care process that should be used by the pharmacist. All 3perspectives are important, but they need to be supplemented withcomponents, which then must be integrated to address medicationmanagement in a comprehensive manner required for a team-based practice.For example, the focus on the drug product is in conflict with patient-centered practice. Limiting a model to medication errors ignores drugoutcomes such as effectiveness and patient preference. Using the viewpointof the pharmacist alone causes insufficient attention to be paid to the otherteam members.
Second, the frameworks were more process oriented. We required a focuson roles, responsibilities, and activities of the different players to facilitatea discussion of these roles within a multidisciplinary team. As well, theyneed to relate to the relevant patient care outcomes.
Third, these frameworks did not explicitly differentiate between primarycontrol/authority and the supportive roles. This differentiation is importantwhen we consider aspects of accountability and the approach that should beused to evaluate impact on medication use outcomes of one member of theteam, such as the pharmacist.
Fourth, the patient’s role in the medication management process needs tobe more specifically explicated and described beyond administration/consumption, passive following of instructions, or limited to providinginput into defining desired outcomes. Building on the pharmaceutical caremodel, and being patient-centered, we need to recognize and support thesignificant roles and responsibilities that patients and their families have inthe medication management process.
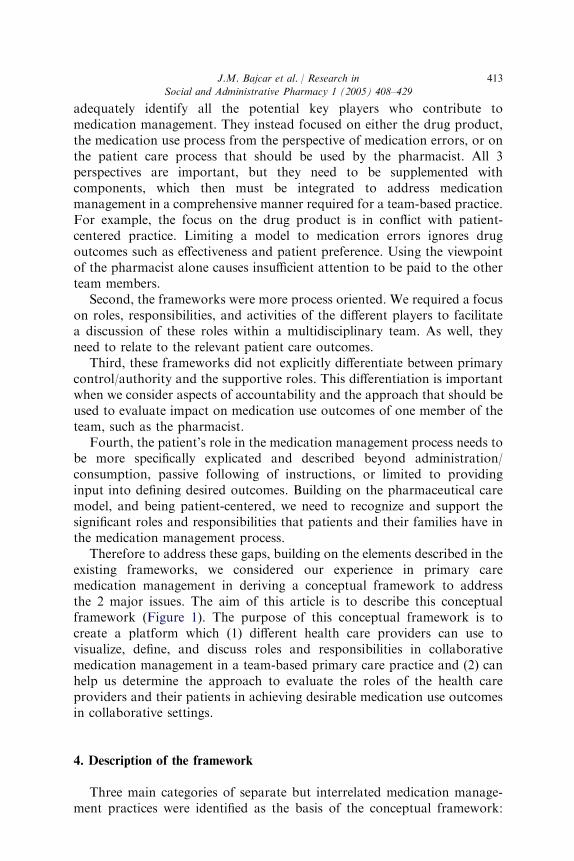
Therefore to address these gaps, building on the elements described in theexisting frameworks, we considered our experience in primary caremedication management in deriving a conceptual framework to addressthe 2 major issues. The aim of this article is to describe this conceptualframework (Figure 1). The purpose of this conceptual framework is tocreate a platform which (1) different health care providers can use tovisualize, define, and discuss roles and responsibilities in collaborativemedication management in a team-based primary care practice and (2) canhelp us determine the approach to evaluate the roles of the health careproviders and their patients in achieving desirable medication use outcomesin collaborative settings.
4. Description of the framework
Three main categories of separate but interrelated medication manage-ment practices were identified as the basis of the conceptual framework:
414 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
medication taking, medication prescribing, and medication dispensing.These practices represent the tasks and activities of individuals who in theprimary care setting have the ultimate control over taking, prescribing, anddispensing medication. Further, these medication practices have beenidentified in the medication error literature as key contributors to gaps inmedication use that must be addressed to reduce medication-relatedmorbidity and mortality.28-33
The 3 categories of medication practices describe components inmedication use where potential gaps can occur in the medication-relatedwork performed by individuals who have the direct authority over specificmedication-related tasks and the related activities. Because the tasks or
The prescriber:*
a) Makes the correct diagnosis; b) decides if drug therapy is indicated or needs to be continued; c) selects the best medication for an individual patient; d) selects the optimal dose for the individual patient; e) writesthe prescription for the selected medication regimen; f) monitors how well the medication is working and/or if it is causing any problems; g) instructs the patient about the prescribed regimen; h) evaluates and facilitates theongoing reordering of long-term medication outcomes.* The medication-prescribing practice is the primaryresponsibility of the individual clinical prescriber.
Supportive roles and functions provided by different members of the health-care team:
• Various individuals support the three primary medication-related practices • System level: create structures and processes that support individual
practices and facilitate team's work
The dispenser of the
medication:*
a) Assesses the medication order or prescription for authenticity and appropriateness in the patient’s clinical situation; b) creates appropriate labelling; c) compounds the medication (occasionally); d) explains the directions to the patient and provides the patient withinformation about the medication; and e) maintains an accurate medication profile.* In the ambulatory care setting, medication-dispensing practice is usually the primary responsibilityof the pharmacist.
The patient:*
a) Understands his or her medical illness and medications so that they make sense; b) makes informed choices about his or her medications; c) takes the medications appropriately; d) evaluates the status of the illness and monitors for medication problems; e) identifies problematic situations and knows the appropriate action to take; and f) accesses the medication or navigates systems to facilitate access.* In the ambulatory care setting, medication-taking practice is the primary responsibility of thepatient or the patient’s caregiver.
Medication-Dispensing PracticeMedication-
Prescribing Practice
Medication-TakingPractice
Figure 1. Conceptual framework for a Team Approach to Medication Management
(TeAMM Model).

415J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
activities that are performed as part of the 3 practices are numerous andoften complex, the framework also places other individuals in supportiveroles that contribute to effective medication management. Both types ofroles (primary and supportive), however, are key to the overall effective useof medications. Each medication-related practice has a set of activities thatneed to be performed by one or more individuals in the team. Einarson,34 inhis authority model, describes the complexity of the notion of authority andinfluencing factors in the drug use process. We found it useful to developand use our conceptual framework in organizing our thinking aboutdifferent roles, responsibilities, and activities that someone in the team mayneed to carry out with respect to medication management. Medicationmanagement is presented as collective dynamic work performed by thosewith different independent or shared roles and responsibilities. The roles andresponsibilities have to be defined for each patient care setting because theneeds in different settings will differ as will the members of the health careteam who are able and willing to work collectively toward patient care. Theconceptual framework proposed in this article serves as a platform toconsider the roles and responsibilities of members of the team whocontribute to medication management.
4.1. Medication-taking practice
Medication taking is a key component of the work performed by patientswith chronic illnesses and their family as part of medical management.35 Ofthe 3 medication-related practices, medication taking is probably the mostimportant component of collaborative medication management but oftenreceives the least attention.
In the ambulatory care setting, medication taking is the primaryresponsibility of the patient and/or the patient’s caregiver. It is estimatedthat between 20% and 70% of patients do not take their medications asprescribed (the average being approximately 50%), with the greatestproblems seen with long-term medication use in patients with chronicillnesses.33,36,37
How patients manage their medications can affect their health. Alandmark study done over 25 years ago identified that 10.5% of patientswere hospitalized in a general medicine ward secondary to problems causedby patients’ noncompliance with their medications.38 Preventable admis-sions to a medical unit were due to nonadherence to medication in 30% ofcases.29 One third of preventable hospital admissions for adverse drugreactions were associated with patient noncompliance.14 Sullivan et al39
estimated that 5.3% of hospitalizations were due to medication non-compliance. A substantial number of these incidents of noncompliance arebelieved to be intentional. Specifically, most patients (but not all) receivinglong-term medications make regular and conscious decisions about theirmedications. They engage in planned medication self-regulation practices,

416 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
often without consulting their physicians or other health care providers.40-47
Planned self-regulated medication may include reducing or increasing dailydoses, skipping a dose or taking an extra one under specific circumstances,or stopping the use of the drug completely. From the patient’s perspective,the purpose of such self-regulating practice is to assess whether (1) themedication is still needed, (2) an adequate benefit from the medication canbe obtained with lower doses, or (3) an undesirable side effect is beingcaused by the medication.
As illustrated in the literature, patients play a pivotal role in themedication management process. Ambulatory care patients and/or theirhome caregivers are the last link in the chain leading to optimal medicationuse.30 Medication-taking practice in our conceptual framework refers totasks and activities of medication management that are performed by eitherthe users of medications or their home caregivers (eg, family, friends).
From our analysis of the practice and the literature, several themesemerged that describe what the patient and his/her family should be ableand willing to do if they are to create a safe and effective medication-takingpractice. These themes include the following: (a) understanding theirmedical illness and medications so that they make sense to them,44,48-50 (b)making informed choices about their medications,40 (c) taking theirmedications appropriately,25,26 (d ) evaluating the status of the illness andmonitoring for medication problems,23 (e) effectively identifying anyproblematic situation that arises and knowing the appropriate action totake, 23 and ( f ) accessing the medications or navigating systems to facilitateaccess.25
The conceptual framework draws importance to the medication-takingpractice of patients and places this practice at the core of the collaborativemedication management framework. A person’s medication-taking practicewill ultimately and directly determine (to a large extent) whether thatindividual will benefit from the medications. The literature clearly describesthat patients create medication-taking practices that differ from what thehealth care provider may have had in mind.33,36,37 In fact, there is a growingbody of literature indicating that most patients with chronic illnesses willmodify and test their medications before fully accepting them.44 Thepatients’ objective in testing or self-regulating the medications is todetermine for themselves if (a) they still need the drug, (b) an adverse effectmay be due to the medication, or (c) they could use a lower dose.41,44,50
To effectively self-regulate medications, patients need adequate knowl-edge and understanding of their medications. But, it is well documented thatpatients have gaps in their understanding of their pharmacotherapy, andthese gaps will affect their decisions regarding the self-regulation of theirdrugs and interpretation of the medication-taking experiences, which canlead to drug-related problems. For example, Gilbert et al51 observed that20% of the drug-related problems identified in the community setting wasrelated to the patient’s lack of knowledge about the medications. Kennie
417J.M. Bajcar et al. / Research in
and Bajcar20 noted that, in 92% of drug-related problems identified ina medication check-up program, the patient had some gaps in medicationknowledge, and half of the patients had additional questions about theirmedications. Patients recognize their need for more information from theirhealth care providers, including information that differs in type from whatthey usually receive, so patients can become better-informed medicationtakers.52-54 Therefore, it is essential that patients are considered as membersof the team and therefore they need to be included more explicitly in thecollaborative approach to medication management because there are healthand cost implications if patients develop medication-taking practices thatare unsafe or not aligned with their health care provider’s prescribingpractice.14,39,55
4.2. Medication-prescribing practice
The second component of the conceptual framework is medication-prescribing practice of health care providers who have been grantedauthority to prescribe. With the increase in the number of medicationsintroduced into the market over the last few years and the focus onevidence-based prescribing of medications, this practice has also becomemore complex.
Various studies have identified gaps in medication-prescribing practice. Ithas been estimated that 1-2% of patients admitted to US hospitals areharmed as a result of medication errors, most of which are errors inprescribing.26,55,56 It is estimated that errors occur in up to 11% of allprescriptions.57 Sanders57 found that gaps in medication prescribing aremainly related to issues of dose and medication selection. Sellors et al5
observed that in family practice the most common prescription error issueswere related to the patients not receiving a required drug, medicationselection, and inadequate dose of the medication. Roughead et al58 notedsimilar results, but in addition they reported that one in three people in thecommunity setting required additional monitoring.
Based on our experience in the family practice setting, specifically fromour action-based research in teaching medical residents therapeutics, andreview of the literature, several tasks and activities emerged as part ofmedication-prescribing practice.59,60 It is necessary that the prescriber (a)makes the correct diagnosis, (b) decides if drug therapy is indicated or needsto be continued, (c) selects the best medication for a particular patient ata given time, (d) selects the optimal dose for an individual patient, (e) writesthe prescription for the selected medication regimen, (f) effectively monitorshow well the medication is working and/or if it is causing any problems, (g)instructs patients about the prescribed medication, and (h) evaluates andfacilitates the ongoing reordering of long-term medications.
Over the last few years in different countries, different health careprofessionals, not only physicians and dentists, but also nurse practitioners,
Social and Administrative Pharmacy 1 (2005) 408–429

418 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
midwives, pharmacists, physician assistants, and chiropractors, have beenauthorized to prescribe or coprescribe. Medication prescribing can bea challenge because these prescribers must be aware of the latest therapeutictreatment options and integrate the best available evidence into theirdecision making, at the same time involving the patient and considering thepatient’s preferences.
4.3. Medication-dispensing practice
Dispensing of medication is the third component of medicationmanagement. As with the other medication practices described above, gapsin primary or community-based care can also occur at this level. Theseinclude dispensing the wrong drug, wrong strength or formulation,providing an incorrect label, or giving the prescribed medication to thewrong patient. The literature on medication-dispensing errors is moreabundant for hospital pharmacy practice than community pharmacypractice. However, Chua et al61 reported that, in 4 primary care pharmaciesin the United Kingdom, 56 dispensing errors or ‘‘near misses’’ occurred forevery 10,000 items dispensed. The most common errors were related toincorrect strengths of the drugs.61
Based on medication-dispensing standards of practice, the following aresome of the key responsibilities and activities to be performed for effectiveand safe dispensing of medications62: (a) assessing the prescription forauthenticity and appropriateness in the patient’s clinical situation (consid-ering, for example, dose, drug interaction, duplicates, and allergies), (b)developing an appropriate prescription label to ensure that the patient isable to understand which medication should be taken and how much, how,when, and for how long, (c) transfering the medication to an appropriatecontainer, (c) (occasionally) compounding of the medication, (d ) explainingthe directions to the patient and providing the patient with informationabout the medication, and (e) maintaining an accurate medication profile.
In the ambulatory care setting, medication-dispensing practice is usuallythe primary responsibility of the pharmacist. Medication dispensing isbecoming more automated and facilitated by the use of various technologiesto increase efficiency and reduce errors, and sometimes responsibility may beshifted to more senior technicians. This shift has provided the opportunityfor pharmacists in the community setting to expand their clinical roles.
4.4. Supportive functions and systems
The proposed conceptual framework suggests that a collaborative effortis required to address the complexities associated with modern medicationmanagement. Many medication management elements must be addressedwithin each medication-related practice and executed within the highlycomplex health care system. Therefore, in addition to the primary roles

419J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
described, additional supportive roles need to be played by members of theteam if we are to achieve and sustain optimal use of medications. Theframework identifies where and how different health care professionals needto collaborate and support the practices of medication prescribing,medication taking, and medication dispensing. This interrelationship ofroles is described below.
First, patients’ medication-taking practices must be supported throughformal and informal network of individuals (including health careprofessionals and nonhealth care professionals). Many health care providerscurrently are developing roles and services to help patients manage theirmedications effectively. For example, in ambulatory care settings, varioushealth care providers such as pharmacists, physicians, and nurses performthis role. This support is required from all health care professionals involvedin medication management because each profession contributes in differentways to assist the patient in developing and maintaining a safe and effectivemedication-taking practice. Several activities that support a patient’smedication-taking practice emerged from our reflection of the patients inour practice and were confirmed from the description of activities in theliterature. These activities may include the following: (a) developing a systemthat helps patients access their medications which may include identifyingsources of financial support or delivery of medication for those who are notmobile, (b) offering medication adherence strategies and tools to supportmedication administration,63 (c) providing patients with information aboutmedications to help them understand the method of taking medication,64
(d ) providing advice on medication options and consequences helpingpatients decide about their medications,23 and (e) educating patients todevelop self-management skills to attain a high level of understanding oftheir illness and medication so they can play an active role in theirmedication management.23
The literature clearly demonstrates a need for collaboration betweenhealth care professionals who support the medication-prescribing practice ofthe prescriber. Medication prescribing is a complex act.65 Many studies havedocumented the gaps and challenges that exist in medication prescribing.5,57
This is not surprising because effective medication prescribing depends on(a) accurate and timely access to comprehensive patient medicationhistory,60 (b) access to up-to-date evidence-based therapeutic information,(c) an understanding of how drug and dose selection need to be tailored toindividual patient characteristics, concurrent illnesses, and concurrent use oftheir medications,60 (d ) accurate communication of the intended medicationregimen, including interpretation of it, to the health care professional whodispenses the medication, and (e) a means of monitoring the outcomes of themedications. In the modern health care setting, it is often challenging forone health care provider to address each of these aspects.60 Thus, there isa growing need for additional health care practitioners to support themedication-prescribing practice.

420 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
Medication-prescribing practice is supported by medical specialists,pharmacists, nurses, or nurse practitioners. The supportive functions mayinclude (a) providing a second opinion on a diagnosis by another physician,(b) offering advice on selection of drugs or doses, (c) conducting a fullmedication review or pharmaceutical care assessment to help select a drugor a dose,27 (d ) completing a full medication history,27 (e) monitoring theillness and medications,27 ( f ) providing general drug information, ( g)providing continuing professional education, and (h) creating a system thatfacilitates the reordering of medications, and/or supplemental prescribingunder preauthorized protocols.66 The features of the input or advice canvary, depending on the practice setting and the nature of the collaborationthat has been established between the health care practitioners.
With respect to medication-dispensing practice, the health care providerwho dispenses (ie, the pharmacist) is usually supported in this role bypharmacy technicians and by various dispensing-related technologies.Common medication-dispensing supporting functions may include technicalfunctions such as67 (a) receiving prescriptions, (b) entering prescriptioninformation into computers, (c) preparing pharmaceutical products, and (d )general support of distribution and quality assurance activities. Theexpanded role of the pharmacy technician has provided greater support topharmacists allowing them to focus more on clinical functions that supportthe medication-prescribing and medication-taking practices. In manycountries, the pharmacy technician’s role is becoming more formalized.68
Pharmacists may also support the medication-dispensing practices of otherpharmacists by sharing information about the patient or helping the patientobtain a medication.
Therefore, the 3 primary medication-related practices are supportedthrough formal and informal networks of health care professionals whoprovide other individuals in the team with (a) information (eg, simple factsabout the drug and disease), (b) advice (eg, recommendations on how totreat), (c) education (ie, creation of an environment in which the learner cancreate meaning from the information that is provided), (d ) strategies (eg,medication-prescribing protocols) and tools (eg, medication adherenceaids), or (e) system support (eg, helping patients access medications).
5. Summary of the conceptual framework
Figure 1 illustrates the relationship among the 3 principal components ofmedication management and the supportive roles. The 3 principal practicesform the backbone of the proposed conceptual frameworkdTeamApproach to Medication Management (TeAMM). Two of the medica-tion-related practices fall directly within the responsibility of health careproviders and the third falls under the patient’s control. In each practice,a responsible person or persons must competently execute various elements.
421J.M. Bajcar et al. / Research in
Thus to achieve optimal medication use, we need to achieve the following 3specific goals: (a) the prescriber must have a safe and effective medication-prescribing practice, (b) the dispenser (usually the pharmacist) must havea safe and effective medication-dispensing practice, and (c) the patient musthave a safe and effective medication-taking practice (which extends to theactivities of the home caregiver). The framework places the patient’smedication-taking practice in a prominent position because in theambulatory care setting the patient plays a critical role in the entiremedication management process.
5.1. Case example
A case example is provided in Appendix 1 to illustrate the 3 medication-related practices that form the principal components of the TeAMMframework and how they relate to each other within a family practicecontext. The case illustrates not only that the patient and his/hermedication-taking practice is front and center, but also that there is a needfor extension of the involvement of multiple health care professionals, someof whom play principal roles and others supporting roles, but that all rolesare essential.
This case illustrates the outcome of the combined effort of 4 health careprofessionals (physician, pharmacist, nurse, dietician) working together withthe patient as a key member of the team. The clinical pharmacist in thisscenario supports effective and safe medication-taking and medication-prescribing practices. The case also demonstrates the importance ofconsidering and focusing on the patients’ medication-taking practicebecause the support given to the patients by their various health careproviders helped them develop a more effective and safer medication-takingpractice that was key to acheiving the final outcome.
In addition to describing the 3 basic medication-related practices, the casedemonstrates that health care professionals who are part of a primary careteam must also perform various supportive roles and functions thatinfluence the 3 practices (medication prescribing, medication taking, andmedication dispensing). It is through the performance of these supportiveroles that true collaboration occurs, which potentially can enhance the useof medications and optimize their benefit to patients.
6. Discussion and conclusions
The TeAMM framework for medication management consists of 3primary medication-related practices, each supported by a team of healthcare professionals and a system. The framework delineates potential roles,responsibilities, and activities that relate to medication management.Because medication management has become highly complex, the roles
Social and Administrative Pharmacy 1 (2005) 408–429

422 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
and functions of different members of the health care team in primary careneed to be integrated into a network of health care professional supportsystems that enhance, optimize, and connect each of the 3 practices.Therefore, additional supportive components are required within collabo-rative medication managementdcomponents that are as important as theinitial 3 principal practices of medication prescribing, medication taking,and medication dispensing. The TeAMM framework can help define thedirect and indirect roles that different members of the team can play inmedication management. The framework provides a platform upon whichthe different health care providers can begin discussion on the differentdirect or supportive roles in medication management. Different practicesettings and clinical patient situations may require a change in how theseroles are defined. However, the framework may help any one of themembers of the team reflect upon the role and describe the practice andfunctions so they can be communicated to others.
In this study, the framework was capable of being used to reflect uponthe existing pharmacy practice within the family practice setting and thatthe support of a patient’s medication-taking practice was underdevelopedand unstructured was identified. Most of the systematic practice de-velopment focused on supporting medication-prescribing practice throughpharmaceutical care assessments and by providing drug information.Although there were a variety of activities that occurred in support of thepatients’ medication-taking practice, in relation to the other roles thesewere a lot less structured, less studied, and not as well defined. Thisobservation has led to a series of practice research studies and practiceenhancement projects to improve and structure the pharmacists’ approachto supporting patients’ medication-taking practice in our family practicesetting.
The TeAMM framework indicates that each component is essential ifcollaborative medication management is to result in optimal medication use.Patients can develop significant medication-related problems or negativeclinical outcomes if there are gaps in any of the 3 primary medication-related practices. This suggests that the ultimate responsibility for theoverall outcomes of the therapy depends on a coordinated and integratedeffort of the team, and not on one member of the team alone. Therefore, theconceptual framework may be useful when health care providers are facedwith the difficult task of evaluating the effectiveness of any one member ofthe team, especially if the specific health care professional primarily providesa supportive clinical role, versus the outcomes that can be measured asa result of the collaborative work of the entire team. The notion of primarymedication-related practices and supportive practices indicates that we needto identify levels of intermediate medication use outcomes that relatespecifically to each of the 3 medication-related practices. A pharmacistwhose main role and responsibility is to support medication-prescribingpractice and medication-taking practice should be assessed to the extent to

423J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
which the activities that are carried out by the pharmacists effectively fulfillthis supportive function. For example, to assess the degree to which thepharmacist supports the patient in his/her medication-taking practice maybe measured by assessing the patient’s degree of change in understanding themedication, the ability to accurately set up the correct medication schedule,the ability to describe how a medication dose is adjusted in specificcircumstances, and/or the ability to demonstrate how an administrationdevice is used. Specific measurement instruments will need to be furtherdeveloped to measure these changes in understanding and abilities. But,even if patients have these understanding and abilities, the transfer toeffective daily medication-taking may not occur and thus changes in clinicaloutcomes may not be observed. Therefore clinical outcomes such asfunctional status, laboratory measures of disease control, and hospital-izations should be considered as distant and indirect outcome measuresbecause they can be influenced by many different individuals and actionsthat are not directly related to the pharmacist’s supportive functions.
Lastly, a key aspect of the TeAMM framework is that in the ambulatorycare setting, it is the patient who has the ultimate responsibility and controlover how medications are used. Therefore, in the TeAMM framework thepatient and his/her medication-taking practice occupy a central and keyposition and indicate that the patients’ use of medications must beconnected to safe and appropriate medication-prescribing and medication-dispensing practices.
The limitation of the conceptual framework proposed in this article isthat the specific roles and responsibilities are context dependent, meaningthat it is not possible to prespecify completely all the roles andresponsibilities to fit every practice setting. Different clinical practices willrequire a different complement of individuals and the different individualsmay take on a different repertoire of activities that are within their scope ofpractice but which are in synchrony with roles and responsibilities of theother members of the team. It is important to point out that the patient andthe patient’s family are equal members of the team.
On the other hand, because the framework does not pre-prescribe theseroles and responsibilities it offers a platform that can be used in differentclinical setting to identify the potential key players and the actual roles andfunctions that need to be addressed within that setting. No 2 practices arethe same and we need to develop different practice models to align withpatient needs. Also the specific players and their roles may be influenced andlimited by the specific nature of the health care system and the paymentsystem.
The framework was developed based on our team’s experience ina clinical practice that is a single payer system, which can facilitate theimplementation of collaborative medication management. Thus anotherlimitation of the framework is that it does not directly address the specificdynamics and feasibility in different payer systems. However, the framework
424 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
can help define different activities that need to be performed and that couldthen be negotiated within a multipayer system. The incentive to work asa team and thus to collaborate may, however, be different in a multipayersystem than in a single payer system.
In conclusion, the proposed TeAMM framework can be a useful tool toreflect on an existing practice (as in our setting) or can be used whenconsidering the development of a new collaborative pharmacy practicebecause it provides a platform that may enhance communication aboutmedication management among the players. As a framework it is relevantfor a discussion about the roles and responsibilities of the different healthcare providers who are involved in medication management. It also helps todefine different practitioners’ roles and illustrates the complexities ofevaluation of a specific health care provider involved in medicationmanagement. In addition and according to this conceptual framework, weneed to minimize preventable adverse medication events by achievingalignment between effective and safe medication-taking practices of patients,effective and safe medication-prescribing practices of prescribers, andeffective and safe medication-dispensing practices of pharmacists. TheTeAMM framework proposes that in addition to aiming for alignmentamong these 3 practices, a network of team members must support andenhance all 3 medication use practices.
Appendix 1: Case example
A middle-aged man, Mr Loke (a fictitious name), was referred by thefamily physician to the clinical pharmacist for a consultation regarding hisdiabetes. The physician was concerned because the patient was alreadyreceiving 2 oral hypoglycemics and his blood sugar was not well controlled.The physician asked if anything further could be done with the oral diabeticmedications or if there was no other choice but to switch Mr Loke to insulin.The physician was also concerned about Mr Loke’s medication adherence.Therefore, the initial referral received by the pharmacist was to providesupport in the domain of medication-prescribing practice and assessment ofthe patient’s medication-taking practice.
The clinical pharmacist met with the patient for an initial interview toconduct a complete medication history and to collect information todetermine why Mr Loke’s diabetes was not well controlled. The pharmacistconsidered issues such as intentional or unintentional medication non-adherence, drug-related causes of elevated glucose, nonadherence to dietand exercise, and whether alternative therapy was required to managediabetes at this time.
During the interview, the pharmacist discovered that Mr Loke washaving difficulty remembering to take his medications as a result of a generallack of interest in his care, lack of knowledge of the disease, and poor

425J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
understanding of the role he needed to play in his disease management.Therefore, he was missing doses and taking medications at inappropriatetimes. He was not eating well and, despite seeing a dietitian the year before,he had made very few changes to his diet. He was also not self-monitoringhis glucose regularly. It became apparent that the main reason for his poordiabetes control lay in the domain of the patient’s medication-takingpractice. This aspect of the problem needed to be addressed first before anyfurther decisions could be made in the domain of medication-prescribingpractice.
To support the patient’s medication-taking practice, during the first visitthe pharmacist created a medication calendar for the patient (a list ofmedications and times of day to take them) and began to educate the patientabout the need for, and role of, all his medications. The patient was alsoasked to return to meet with the pharmacist for additional visits to furtherassess his response to drug therapy. Over the next few visits the pharmacistspent time with Mr Loke to teach him more about his diabetes, how hismedications work, how to organize his medications throughout the day, andhow to monitor his response to drug therapy (ie, a supporting role to enhancepatient’s medication-taking practice). The patient gradually started to playa more active role in his medication management and began to monitor hisblood glucose daily. The pharmacist referred the patient to the nurse forinstructions on how to use a glucometer (in this setting, it was negotiatedthat this function was to be part of the nurse’s role) and also the patientagreed to revisit the dietician. These referrals by the pharmacist expandedthe composition of the team that would be able to support the patient in hismedication-taking practice. To help facilitate the work of the other healthcare professionals, the pharmacist discussed the education-related needs ofMr Loke with the nurse and dietician because the patient was respondingwell to simple instructions and coaching and expressed that he liked thisapproach.
The pharmacist discussed the case with the physician and maderecommendations to change the patient’s doses of his oral medication forhis diabetes to improve his diabetes control (ie, the supporting role ofmedication-prescribing practice). The pharmacist also contacted Mr Loke’scommunity pharmacist to relay specific medication changes (ie, medication-dispensing practice) and to assist the community pharmacist in reinforcingthe dosing changes with the patient (ie, supporting patient’s medication-taking practice). The interaction between the 2 pharmacists helped thecommunity pharmacist in her medication-dispensing practice and alsobrought the community pharmacist into the team approach to medicationmanagement.
Over a period of several weeks, the pharmacist, the physician, and thepatient were able to make a few changes in the patient’s oral diabetic agentsand lower his blood sugar to the target without the need for insulin(medication assessment supporting medication-prescribing practice). Mr
426 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
Loke also lost more than 3 kg (7 pounds), was actively monitoring his bloodsugars, and had begun to play an active role in his care. Mr Loke himselfexpressed that he appreciated and needed a team approach and a supportsystem to assist his medication management.
References
1. Woodend K. Medication management: the future of pharmaceutical care? Can Pharm J.
2003;136:29–31.
2. Gilbert AL, Roughead EE, Beilby J, Mott K, Barratt JD. Collaborative medication
management services: improving patient care. Med J Aust. 2002;177:189–192.
3. Achieving Positive Outcomes through collaborative pharmaceutical care: The KPNW
Medication Management Program. Permanente J. 2000;4.
4. Watman GP, Jepson M. Patient screening by a community pharmacist located in a GP
practice. J Soc Admin Pharm. 2001;18:97–102.
5. Sellors J, Kaczorowski J, Sellors C, et al. A randomized controlled trial of a pharmacist
consultation program for family physicians and their elderly patients. Can Med Assoc J.
2003;169:17–22.
6. Commission on the Future of Health Care in Canada. Building on Values: The Future of
Health Care in Canada. Ottawa: The National Library of Canada; 2002.
7. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National
Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure:
The JNC report. JAMA. 2003;289:2560–2572.
8. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian
Diabetes Association 2003 clinical practice guidelines for the prevention and management
of diabetes in Canada. Can J Diabetes. 2003;27:S37–S42.
9. Pappas G, Hadden WC, Kozak LK. Potentially avoidable hospitalizations: inequal-
ities in rates between US socio-economic groups. Am J Public Health. 1997;87:
811–816.
10. Billings J, Anderson GM, Newman LS. Recent findings on preventable hospitalizations.
Health Aff (Millwood). 1996;15:239–249.
11. Winterstein A, Sauer B, Hepler CD, Poole C. Preventable drug-related hospital admissions.
Ann Pharmacother. 2002;36:1238–1248.
12. Einarson TR. Drug-related hospital admissions. Ann Pharmacother. 1993;27:832–840.
13. Patel P, Zed PJ. Drug-related visits to the emergency department: how big is the problem?
Pharmacotherapy. 2002;22:915–923.
14. McDonell PJ, Jacobs MR. Hospital admissions resulting from preventable adverse drug
reactions. Ann Pharmacother. 2002;36:1331–1336.
15. Tafreshi MJ, Melby MJ, Kaback KR, Nord TC. Medication-related visits to the emergency
department: a prospective study. Ann Pharmacother. 1999;33:1252–1257.
16. Farris KB, Cote I, Feeny D, et al. Enhancing primary care for complex patients.
Demonstration project using multidisciplinary teams. Can Fam Physician. 2004;50:998–
1003.
17. Klockars SJ, Blair MM, Ragucci K. Survey of clinical pharmacy services in a family
medicine clinic. Am J Health Syst Pharm. 2003;60:485–486.
18. Martin-Misener R, McNab J, Sketris IS, Edwards L. Collaborative practice in health
systems change: the Nova Scotia experience with the Strengthening Primary Care Initiative.
Can J Nurs Leadersh. 2004;17:33–45.
19. Collaborative working relationships between pharmacists and physicians: an exploratory
study. J Am Pharm Assoc. 2004;44:358–365.
427J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
20. Kennie N, Bajcar JM. Development of pharmacist-managed preventive medication
assessment program in a family physician office setting: the medication checkup. Can J
Hosp Pharm. 2002;55:320–328.
21. Bajcar J, Vaillancourt R. Integrated delivery of pharmaceutical care in family practice.
Pharmacy Connection. 1996;3:26–33.
22. Winslade NE, Strand LM, Pugsley JA, Perrier DG. Practice functions necessary for the
delivery of pharmaceutical care. Pharmacotherapy. 1996;16:889–898.
23. Bodenheimer T, Lorig K, Holman H, Grumbach K. Patient self-management in primary
care. JAMA. 2002;288:2469–2475.
24. Glasgow RE, Anderson RM. In diabetes care, moving from compliance to adherence is not
enough. Diabetes Care. 1999;22:2090–2092.
25. Drug use (Chapter 3). In: Smith MC, Knapp DA, eds. Pharmacy, Drugs and Medical Care.
5th ed. Baltimore, MD: Williams and Wilkins; 1992.
26. Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential
adverse drug events: implications for prevention. JAMA. 1995;274:29–34.
27. Cipolle RJ, Strand LM, Morley PC. Pharmaceutical Care Practice. New York: McGraw-Hill;
1998.
28. Gurwitz JH, Field TS, Harrold LR. Adverse drug events common, preventable in older
outpatients. JAMA. 2003;289:1107–1116.
29. Howard RL, Avery AJ, Howard PD, Partridge M. Investigation into the reasons for
preventable drug related admissions to a medication admission unit: observational study.
Qual Safe Health Care. 2003;12:280–286.
30. Forster AJ, Clark HD, Menard A, et al. Adverse events among medical patients after
discharge from hospital. Can Med Assoc J. 2004;170:345–349.
31. Stiell A, Forster AJ, Stiell IG, van Walraven C. Prevalence of information gaps in the
emergency department and the effect on patient outcomes. Can Med Assoc J.
2003;169:1023–1028.
32. Baker GR, Norton PG. Adverse events and patient safety in Canadian health care. Can
Med Assoc J. 2004;170:353–354.
33. Vermeire E, Hearnshaw H, Van Royen P. Patient adherence to treatment: three decades of
research. A comprehensive review. J Clin Pharmacol Ther. 2001;26:331–342.
34. Einarson TR. The Authority/Pharmacotherapy Care Model: an explanatory model of the
drug use process. Res Soc Admin Pharm. 2005;1:101–117.
35. Corbin J, Strauss A. Unending Work and Care: Managing Chronic Illness at Home. San
Francisco, CA: Jossey-Bass Publishers; 1988.
36. Andreasen BF, Damsgaard EM. Drug therapy in the elderly: what doctors believe and
patients actually do. Br J Clin Pharm. 2001;51:615–622.
37. Hayes RB, McDonald H, Garg AX, Montague P. Interventions for helping patients to
follow prescriptions for medications (Cochrane Review). Available from: http://gateway1.
ovid.com/ovidweb.cgi 2002. Accessed 29.09.04.
38. McKenney JM, Harrison WL. Drug-related hospital admission. Am J Hosp Pharm.
1976;33:792–795.
39. Sullivan DD, Kreling DH, Hazlet TK. Noncompliance with medication regimens and
subsequent hospitalization: a literature analysis and cost of hospitalization estimate. J Res
Pharm Econ. 1990;2:19–33.
40. Chewning B, Boh L, Widerholt J, et al. Does the concordance concept serve patient
medication management? Int J Pharm Pract. 2001;9:71–79.
41. Conrad P. The meaning of medications: another look at compliance. Soc Sci Med.
1985;20:29–37.
42. Conrad P. The noncompliant patient in search of autonomy. Hastings Cent Rep.
1987;17:15–17.
43. Donovan JL, Blake DR. Patient non-compliance: deviance or reasoned decision-making?
Soc Sci Med. 1992;34:507–513.
428 J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
44. Dowell J, Hudson H. A qualitative study of medication-taking behavior in primary care.
Fam Pract. 1997;14:369–375.
45. Hunt LM, Arar NH. An analytical framework for contrasting patient and provider views of
the process of chronic disease management. Med Anthropol Q. 2001;15:347–367.
46. Johnson MJ. Adherent and non-adherent medication-taking in elderly hypertensive
patients. Clin Nurs Res. 1999;8:318–335.
47. Campbell R, Pound P, Pope C, et al. Evaluating meta-ethnography: a synthesis of
qualitative research on lay experiences of diabetes and diabetes care. Soc Sci Med.
2003;56:671–684.
48. Development of a needs-driven theory-based model for medication-taking education with
plans for implementation and evaluation. Doctoral dissertation, Nova Southeastern
University, North Miami, FL; 2003.
49. Bajcar J. Learner characteristics and patient goals for medication-taking education:
patients’ perspectives on the learning environment that supports patient’s mediation-taking
practice (Abstract). Can J Clin Pharmacol. 2003;10:158.
50. Leventhal H, Nerenz DR, Steel DJ. Illness representation and coping health threats. In:
Baum A, Singer J, eds. A Handbook of Psychology and Health. Hillsdale. NJ: Erlbaum
Associates; 1984, p. 219–252.
51. Gilbert J, Murray G, Corbin R. Consumerism and healthcare in Ontario: are patients
becoming consumers? The Change Foundation.www.changefoundation.com. Accessed 10.
03.04.
52. Smith F, Francis S, Rowley E. Group interviews with people taking long-term medications:
comparing the perspectives of people with arthritis, respiratory disease and mental health
problems. Int J Pharm Pract. 2000;8:88–96.
53. Nair K, Dolovich L, Cassels A, et al. What patients want to know about their medications.
Can Fam Physician. 2002;48:104–110.
54. Ziegler DK, Mosier MC, Beuenaver M, Okuyemi K. How much information about
adverse effects of medications do patients want from physicians? Arch Intern Med.
2001;161:706–713.
55. Barber ND, Dean BS. The incidence of medication errors and ways to reduce them. Clinical
Risk. 1998;4:103–106.
56. Leappe LL, Bates DW, Cullen DJ, et al. Systems analysis of adverse drug events. JAMA.
1995;274:35–43.
57. Sanders J, Esmail A. The frequency and nature of medical error in primary care:
understanding the diversity across studies. Fam Pract. 2003;20:231–236.
58. Roughead EE, Barratt JD, Gilbert AL. Medication-related problems commonly occurring
in Australian community settings. Pharmacoepidemiol Drug Saf. 2004;13:83–87.
59. Dovey SM, Meyers DS, Philips RL, et al. A preliminary taxonomy of medical errors in
family practice. Qual Saf Health Care. 2002;11:233–239.
60. Carmichael JM, O’Connell MB, Devine B, et al. Collaborative Drug Therapy Management
by Pharmacists. Pharmacotherapy. 1997;17:1050–1061.
61. Chua SS, Edmonson H, Allen C, et al. A feasibility study for recording of dispensing errors
and ‘near misses’ in four UK primary care pharmacies. Drug Saf. 2003;26:803–813.
62. Ontario College of Pharmacists. Standards of practice 2003 for community and hospital
pharmacists.http://www.ocpinfo.com. Accessed 14.12.04.
63. Raynor DK, Booth TG, Blenkinsopp A. Effects of computer generated reminder charts on
patients’ compliance with drug regimens. BMJ. 1993;306:1158–1161.
64. Berger BA. Communication Skills for Pharmacists: Building Relationships and Improving
Care. Washington, DC: American Pharmaceutical Association; 2002.
65. Barber N, Rawlings M, Franklin D. Reducing prescribing error: competence, control, and
culture. Qual Saf Health Care. 2003;12:29–32.
66. Pearson G, Yuksel N, Card D, Chin T, Gray M, Howboldt J, Jackevicius C, Slavik R,
Thompson A. An information paper on pharmacist prescribing within health care facility.
429J.M. Bajcar et al. / Research in
Social and Administrative Pharmacy 1 (2005) 408–429
Canadian Society of Hospital Pharmacist Statement on Pharmacist Prescribing.www.cshp.
ca. Accessed 14.12.04.
67. Ontario College of Pharmacists.. Competency profile for pharmacy technicians. Pharmacy
Connection. 2003;9:8–17.
68. Balestrini S. Pharmacy technician expanded role to support pharmacists. Pharmacy
Connection. 2003;9:6–17.
















![Medication Supply in Closed Loop Medication Conceptual ...ceur-ws.org/Vol-2001/paper3.pdf · repackaged unit doses from hospital pharmacies or other businesses [3]. ID-marked unit](https://img.dokumen.tips/doc/110x75/5f03da457e708231d40b156a/medication-supply-in-closed-loop-medication-conceptual-ceur-wsorgvol-2001.jpg)












