Embed Size (px)
Citation preview

CBPRA-00443; No of Pages 16: 4C
Available online at www.sciencedirect.com
Cognitive and Behavioral Practice xx (2012) xxx-xxxwww.elsevier.com/locate/cabp
Collaborative Empiricism in Cognitive Therapy for Psychosis: A Practice Guide
Paul Hutton and Anthony P. Morrison, Greater Manchester West Mental Health NHS Foundation Trust andUniversity of Manchester
Keywtive t
1077© 20Publ
PleBeh
We outline our understanding of collaborative empiricism (CE) as used in cognitive therapy (CT) for psychosis. We discuss how CE can bethought of as a technique for facilitating cognitive change in the service of a client's goals, but also as an expression of respect for clientautonomy, recognizing the ethical imperative to empower clients by involving them in decisions about their care. Taking a CE approach istherefore consistent with user-led conceptualizations of recovery, and the related movements of “shared decision-making” and “evidence-based patient choice.”Wediscuss howCE can aid with engagement, assessment, formulation, and intervention inCT, illustrating this withcase material. We focus on how CE can help with distressing intrusive experiences and beliefs, and also consider its role in helping clientsachieve wider life goals. Adaptations to CE for working with people with problemswith learning, attention, andmemory are discussed, as areconsiderations for working with high conviction and conceptual disorganization.
C OLLABORATIVE empiricism (CE) has been a definingfeature of cognitive therapy (CT) ever since the
latter was invented (Beck, 1967). It forms a particularlyimportant part of CT for people with psychosis, where CEis the general approach taken when helping clientsevaluate the validity, reliability, and usefulness of theirappraisals, behavior, and wider belief systems (Chadwick,Birchwood,&Trower, 1996; Fowler,Garety,&Kuipers, 1995;Gumley & Schwannauer, 2006; Kingdon & Turkington,2005; Morrison, Renton, Dunn, Williams, & Bentall, 2004).According to Beck and Dozois, “Collaborative empiricismmeans that the patient and the therapist become co-investigators both in ascertaining the goals for treatmentand investigating the patient's thoughts. Methods ofguided discovery are used to help patients to test theirown thinking through personal observations and exper-iments rather than via cajoling or persuasion” (Beck &Dozois, 2011).
CE is particularly important for case conceptualizationin CT. According to Kuyken and colleagues, collaborationbetween therapist and client here involves “bringing theirrespective expertise together in the joint endeavour ofdescribing, explaining and helping resolve the client'spresenting issues,” while empiricism involves a synthesis of
ords: collaborative empiricism; schizophrenia; psychosis; cogni-herapy; cognitive behavioral therapy
-7229/12/xxx-xxx$1.00/012 Association for Behavioral and Cognitive Therapies.ished by Elsevier Ltd. All rights reserved.
ase cite this article as: Hutton & Morrison, Collaborative Empiricism iavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
theory, research, and observation, and a hypothesis-testingapproach to clinical decision-making (Kuyken, Padesky, &Dudley, 2008).
However, Tee and Kazantzis have drawn attention tosome uncertainty over the definition, noting that the term“collaborative empiricism” now means different things todifferent theorists (Tee & Kazantzis, 2011). These authorsoffer a fresh perspective on how CE leads to belief change,using the framework of self-determination theory. Theynote the lack of scrutiny ofCE, andmake a call for empiricalwork to examine, among other things, the components ofCE, the relationship of CE to other constructs and variables,and the effectiveness of CE in CT.
CEmay be therapeutically valuable in two important andcomplementary ways. First, it may be an aid to achieving theoverall goal of helping a client reduce their suffering andemotional distress. Clients with psychosis have reportedfinding it inherently engaging to be treated as an equalpartner (Kilbride et al., 2012), and they may be more likelyto consider the full range of evidence before them whenthey have taken at least an equal role in discovering it (Tee& Kazantzis, 2011). Second, helping clients form views ormake decisions based on evidence (and reason) may helpthemmakemore reliable and informed decisions, now andin the future (Stacey et al., 2011). Thus, CEmight be viewedas a process that helps to build and protect decision-makingcapacity which, in turn, may promote autonomy (Owen,Freyenhagen, Richardson, & Hotopf, 2009).
Our aim in this paper is to discuss the use of CE in CTwith people who have received a diagnosis of a psychoticillness. We first discuss why CE is a particularly important
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

2 Hutton & Morrison
feature of CT with this group, focusing on how CE can helpclients achieve cognitive change.We then outline examplesof CE in CT, illustrated using anonymized case material.
CE in CT for Psychosis
CE may be a particularly important aspect of CT forpsychosis, for several related reasons. First, adopting acollaborative stance can aid engagement with clients whoare more likely than others to be experiencing high levelsof suspiciousness. Awillingness to collaboratemight commu-nicate awillingness to cede control andpower, thus reducingthe extent to which the clinician is viewed as a threat.Collaboration from the outset may help to ensure the goalsof therapy are clearly defined and shared, reducing thelikelihood of disagreement and misunderstanding.
Second, people with psychosis tend to experiencerelatively greater coercion from mental health services toadhere to treatment, which all too often consists ofantipsychotic drugs alone (Burns et al., 2011; Monahan etal., 2005). However, there is good evidence that people withpsychosis wish to be involved in making decisions abouttheir care and treatment (Byrne, Davies, & Morrison, 2010;Hamann, Cohen, Leucht, Busch, &Kissling, 2005), and thatmany retain the capacity to do so (Grisso, Appelbaum, &Hill-Fotouhi, 1997; Stroup et al., 2005; Vollmann, Bauer,Danker-Hopfe,&Helmchen, 2003).Nonetheless, exclusionfrom these and other important decisions is not uncommon(Hamannet al., 2008). Thus, clientsmaybe very receptive toa clinician who takes a collaborative approach.
Third, adopting CE as an approach requires thatclinicians pay close attention to the evidence informingtheir client's fears and concerns, and that they avoidmakingassumptions about their truth. This means a client's values,experiences, and perspective are taken seriously and notsimply dismissed as delusions, meaningless symptoms, orepiphenomena. Experience suggests that clients are oftenquite preoccupied with not being believed and frequentlyfeel frustrated and isolated as a result. CE can protectagainst that frustration being directed at the therapist, thushelping to ensure engagement.
Fourth, there is evidence that delusional conviction isassociated with a general tendency to form conclusionsquickly based on limited evidence (Fine, Gardner, Craigie,& Gold, 2007; Garety et al., 2005; Startup, Freeman, &Garety, 2008), as well as a greater inflexibility in consideringalternative explanations (So et al., 2011). If developing “theability to question the way I look at things” (Greenwood et al.,2010) is a shared goal of therapy, then adopting a CEapproach, with its focus on considering evidence andgenerating explanations, may be well-placed to help. Itmight be argued that service-users are unlikely to ever adoptsuch a goal, particularly if they believe their existing way oflooking at things with complete conviction. On the otherhand, delusional conviction varies a great deal (Brett-Jones,
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
Garety, & Hemsley, 1987), while experience suggests thatthe formulation process can help clients recognize the linkbetween fluctuating conviction and intensity of emotionaldistress. There is someevidence that reasoning training andmetacognitive training focusedon addressing various biasescan be particularly effective (Aghotor, Pfueller, Moritz,Weisbrod, & Roesch-Ely, 2010; Moritz, Kerstan, et al., 2011;Moritz, Veckenstedt, Randjbar, Vitzthum, & Woodward,2011; Ross, Freeman, Dunn, & Garety, 2011), and there isno reason why aspects of these procedures cannot beincorporated into standard CT if the formulation suggestsso.
Overall, CE has much in common with other constructssuch as person-centered care, shared decision-making,evidence-based patient choice, and value-based practice(Fulford, 2011), all of which are appropriate responses tothe growing “recognition of the ethical imperative toproperly involve patients in decisions about their care”(Elwyn et al., 2010). Moreover, the emphasis on collabora-tion brought by CE makes it an approach that is consistentwith the philosophy and ideals of the recovery movement,where “choice, self-determination, and empowerment arefoundational values” (Deegan & Drake, 2006). In a recentqualitative study, Pitt and colleagues found recovery frompsychosis involved three themes: rebuilding self, rebuildinglife, and hope for a better future. If experiencing choice,self-determination, and empowerment are important pre-requisites for achieving these broader goals, and if CE canpromote these effectively, then CE may have a role to playin promoting recovery.
Wewill nowoffer someguidance as to howCEcanbest beimplemented in CT for psychosis, specifically focusing onthe assessment and treatment of cognitive factors involved inhallucinations and delusions, should these be identified byclients as obstacles to their recovery. However, symptomaticimprovement is often not necessary or sufficient for arecovery which is meaningful to service users. Therefore, wealso focus on how CE might help with wider life goals.
The Practice of CE in CT for Psychosis
Engagement
It is common to encounter clients who are locked in afrustrating battle of wills with their psychiatrist or caseworker. We find this is particularly likely when a client hasdecided not to take antipsychotic medication, which isoften the only treatment being offered. Indeed there issome evidence that shared decision-making (not dissimilarto CE in its ethos) matters more to clients who are dissat-isfied with their treatment (Hamann,Mendel, Reiter, et al.,2011). Such clients may believe that their mental healthprofessional is not taking their fears and values seriously;often, the mental health professional believes their client
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

3Collaborative Empiricism in CT for Psychosis
“lacks insight”—a judgment that only furthers their client'sfrustration. Not surprisingly, a preoccupying question forsuch clients entering therapy is, Whose side are you on? Thetherapist's response, whether implicit or explicit, can be amake-or-break moment for engagement. CE combinedwith value-based practice (Fulford, 2011) might help here.In practice, this means we tend to respond that we are notyet able to have an informed view on the matter, since weare not in possession of enough information, and that wewould find it useful to carefully go through the evidencewith them, but only if doing so is something that fits withtheir goals.
High levels of suspiciousness can also threaten engage-ment. For example, occasionally clients may suspect theirtherapist of conspiring with their persecutor. Again, CEin combination with awareness of the client's goals andvalues can help here. Working together to draw up a listof evidence for and against their suspicions is useful inestablishing why they have these concerns. Dependingon what this reveals, we may then encourage clients toexamine our office, speak to our colleagues, check ourprofessional qualifications, and read references fromprevious patients. Encouraging clients to consider therapyas a form of experiment in trusting others is also helpful.Eliciting regular feedback from the client regarding theirsuspiciousness is essential, as it allows any potential issuesto be addressed before they become critical. If such con-cerns are revealed, these can be used to demonstrate theutility of the cognitive model by examining them in termsof an event-thought-feeling-behavior cycle and the selec-tion of an appropriate change strategy. For example, if aclient interprets the therapist clearing their throat asevidence of involvement in a conspiracy and a signal tosomeone to follow the client home, then this could beanalyzed as follows:
Event
Please cite this artBehavioral Practice
Thought
icle as: Hutton &(2012), http://d
Feeling
Morrisonx.doi.org
Behavior
Therapist clearsthroat
“It's a signal”
Anxiety Act suspiciouslyTherapist startschecking diaryon phone
“He'sinvolved”
Anger
Look for moreevidence to supportappraisalThis could, according to the client's preferences andstage of therapy, result in a discussion of the evidence,consideration of the advantages and disadvantages ofappraising it in this way, consideration of alternativeexplanations for throat clearing or using therapy atten-dance as an experiment; all of these are examples of CE inaction. Even at this early stage, the client and therapistjointly decide what to focus on. Hypotheses are formedtogether, tested together, and then evaluated together.One caveat here is that the therapist will often not have agreat deal of time in which to ensure engagement.
, Collaborative Empiricism i/10.1016/j.cbpra.2012.08.003
Suspiciousness of the therapist can, if not addressed,mean that the client might not return.
Assessment and Formulation
Cognitive behavioral assessment of people with psycho-sis benefits a great deal from the use of CE. Sharing theprocess of information-gathering from the outset demon-strates to the client that, in CT at least, they are an equalpartner. We suggest that CE is first used to establish, ingeneral terms, what problems the client is seeking helpfor, and their goals in relation to these problems. These canbe operationalized in more detail later as the case concep-tualization progresses. Establishing general problems andgoals at the outset, prior to more detailed assessment, servesat least two important functions: First, it introduces con-straints on the assessment process almost straight away,helping to ensure it is focused, structured, time-efficient,and relevant. Second, it communicates quite clearly to theclient that what takes primacy are their concerns andpreferences. This is particularly important in psychosis,where the problems for which a client seeks help canbe very different from those identified by mental healthprofessionals or concerned relatives (Byrne et al., 2010).For example, while psychiatric services might defineremission from schizophrenia as the relative absence ofpositive symptoms (Andreasen et al., 2005), often help--seeking individuals simply wish to have greater controlover psychotic experiences or their impact on their lives(Byrne et al.; Pitt, Kilbride, Nothard, Welford, & Morrison,2007). A significant proportion of people derive at leastsome meaning or companionship from these experiencesand would prefer not to lose them (Daalman et al., 2011;Jackson & Fulford, 1997; Jenner, Rutten, Beuckens,Boonstra, & Sytema, 2008; Morrison, Nothard, Bowe, &Wells, 2004; Romme, Honig, Noorthoorn, & Escher, 1992).Many others are at least ambivalent, and ambivalence aboutpsychotic experiences has recently been shown to beassociated with refusal of antipsychotic medication (Moritzet al., 2012).
Once general goals are established, we encourage theclient to take an active role in information gathering,working collaboratively with them to identify whichvariables may be important to assess and how best toassess them. Repeated analyses of recent events areperhaps most useful for generating shared hypothesesabout key appraisals and responses (both cognitive andbehavioral). Idiosyncratic monitoring sheets can be pro-duced to help identify triggers for experiences, togetherwith their frequency, intensity, and duration. These canalso be used to track conviction in particular appraisals,measure day-to-day fluctuation in emotion and identify keycognitive and behavioral responses (Morrison, Renton,et al., 2004).
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

Box 1Using collaborative empiricism to guide a case con-ceptualization and action plan.
James was a 25-year old former student whohad left university due to increased fears thatother people could read his mind and were trans-mitting their thoughts to him. He was completelyconvinced this was happening, although he waswilling to re-examine the evidence if this couldhelp reduce his distress and allow him to return touniversity. He prioritized examining his fears thatpeople could readhismind, as he thought tacklingthis would help him feel less anxious, whichwould in turn help him achieve his goal ofreturning to university.
In the early sessions of therapy, James and thetherapist went through several recent eventswhen the problem occurred. James agreed tokeep a daily record of antecedent events, as wellas a recordof thenumberof hoursof sleephehad,his mood and his anxiety. Careful discussionrevealed that James often experienced an in-crease in the loudness of his thoughts when hewas in a public area. He then worried that otherpeople could hear them, which led to anxiety. Healso began to worry that he was “going mad,”which led to even more anxiety and a furtherincrease in the loudness of his thoughts. Hebegan to stare at people, trying to figure outwhether they were listening and could hear.When they stared back, he interpreted this asevidence confirming his fears. He then left thesituation as soon as possible, and stayed at homeworrying.
By gathering information about possible trig-gers, he realized that this experience was muchmore likely to happenwhen he had not slept andwas already feeling anxious or worried. He alsorealized that he was much more anxious whenhe was having what he regarded as unaccept-able thoughts. James and the therapist agreed itwould be useful to find out how people wouldnormally react to being stared at, as well asdevelop other ways of testing his belief theycould hear his thoughts (e.g., by thinking thingsthat would provoke a reaction, such as therebeing a fire, or thinking his bank account securitycode). He also agreed it might be useful to findoutmore about intrusive thoughts, as he seemedunaware other people had these or that theywere linked to anxiety. Finally, James and thetherapist agreed to work together to plan a
survey, asking peoplewhether they experiencedan increase in the volume of their thoughtswhenthey were stressed and/or sleep-deprived.
Box 1 (continued)
4 Hutton & Morrison
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
If the client identifies voice-hearing or unusual beliefsas their main problem, then our assessment and caseconceptualization would normally be guided by a cogni-tivemodel of psychosis (Morrison, 2001b), which proposesthat delusions can be conceptualized instead as culturallyunacceptable and/or catastrophic appraisals of relativelynormal intrusive experiences, maintained by safety-seekingbehaviors and threat-related attentional biases, and in-formed by preexisting negative core beliefs about self,others, and the world, as well as positive and negativemetacognitive beliefs concerning the usefulness, uncontrol-lability and dangerousness of paranoia and other cognitiveprocesses (Morrison, 2001b; Morrison et al., 2010). Similarappraisal-based models have also been applied to under-standing and treating persecutory delusions (Freeman,Garety, Kuipers, Fowler, & Bebbington, 2002), distressingvisual hallucinations (Collerton & Dudley, 2004), grandiosedelusions (Knowles, McCarthy-Jones, & Rowse, 2011) andmania (Mansell,Morrison, Reid, Lowens, &Tai, 2007). If themain problem identified by the client is related to an emo-tional disorder (e.g., panic, depression, social anxiety, etc.),which are all very common in people with psychosis(Freeman & Garety, 2003), then we would be guided bythe appropriate cognitive model.
Although the therapist might have all these models todraw upon, the client normally only has their own uniqueexperience. Working collaboratively with the client togenerate a meaningful formulation and set of hypothesesregarding their difficulties is essential. The models de-scribed above are held in mind, but the results from theclient's own empirical work take precedence. A simple caseconceptualization normally emerges from the process ofrepeated analyses of recent events, and is often sufficient toplan an initial successful intervention. A case example of asimple CE-informed case conceptualization and derivedaction plan is given in Box 1.
If a client identifies wider life goals as their priority, suchas returning to work or study, having a relationship, orimproving existing relationships, then much the sameprocess applies. Client and therapist work together to makethese goals “SMART” (Specific, Measurable, Achievable,Realistic, Time-based), following which they jointly investi-gate the factorsmaintaining the problemor preventing goalachievement. The role of self-defeating beliefs (e.g., “If youcannot do something well, there is little point in doing itat all”) has been examined recently in relation to difficul-ties some clients may have with experiencing pleasure,
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

5Collaborative Empiricism in CT for Psychosis
motivation and emotions generally (Beck, Grant, Huh,Perivoliotis, & Chang, 2011; Couture, Blanchard, &Bennett, 2011; Grant & Beck, 2009; Rector, Beck, & Stolar,2005). Such beliefsmay be a particular obstacle to subjectiveempowerment, a key feature of service-user conceptualiza-tions of recovery (Deegan & Drake, 2006; Pitt et al., 2007).Recent empirical work suggests cognitive therapy whichfocuses on collaborative reexamination of these beliefs ismore effective than standard care in improving functioningin clients who are particularly struggling (Grant, Huh,Perivoliotis, Stolar, & Beck, 2012). Although this specializedtype of CT holds promise in helping people move towards ameaningful recovery, it is currently not known whether andtowhat extent CE is a necessary ingredient. Nonetheless, CEis a prominent part of the CT approach which was tested,although the authors acknowledge implementing this is notalways easy:
Key components of collaborative empiricism are expressed inattitudes of equality, teamwork, shared responsibility for change,unconditional positive regard and nonjudgmentalisam. Thespirt and approach of collaborative empiricismmay be harder tomaintain when the patient is extremely paranoid, expressingmore bizarre delusional beliefs, incoherent due to substantivethought disorder, or exceedingly reticent due to overarchingnegative symptoms. The key is for the therapist to maintain astance of flexibility and patience, and recognize that although itmay be difficult to understand some aspects of the person'spresentation, many other aspects will be readily understandable,and understanding improves with time and persistence. (Beck,Rector, Stolar, & Grant, 2009)
Interventions
NormalizingClients very often believe their intrusive experiences are
abnormal and a sign of impending mental catastrophe(Morrison, Nothard, et al., 2004). These appraisals maylead to increased salience, preoccupation, and anxiety,which may, directly or indirectly, make the experiencesmore frequent or intense (Varghese et al., 2011). Fear ofmadness and the perceived stigma of having a diagnosis of apsychotic illness may discourage clients from questioningtheir own explanations which, if unrealistic, distressing, andheld with high conviction, are likely to be classified asdelusions by mental health professionals.
Thus, an important early task (Session 1 or 2) is often tohelp clients test out their abnormality-related appraisals.Referred to asnormalizing, this approach is a key componentof CT for psychosis (Garrett, Stone, & Turkington, 2006;Morrison & Barratt, 2010; Morrison, Renton, et al., 2004). Itoften involves providing clients with the results of studiesthat have examined the prevalence of psychotic-likeexperiences and beliefs in different populations (mostcommonly in the nonclinical, healthy population). Thereare many such studies now, all of which provide strong
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
support for the notion that supposedly unusual experiencesand beliefs are in fact remarkably common (Nuevo et al.,2012; Pechey & Halligan, 2011, in press), supporting theidea of a psychosis continuum(British Psychological Society,2000; Strauss, 1969). One recent multinational study of256,000 healthy individuals found around 1 in 8 reported atleast one psychotic symptom, while a recent UK study of1,000 people found 26% endorsed supposedly bizarrebeliefs (Pechey & Halligan, 2011), with 48% reportingthey experienced psychotic-like experiences at least some-times or often (Pechey&Halligan, in press). Although thereare still somedissenting voices (David, 2010), the continuummodel of psychosis is now commonly accepted (van Os,Hanssen, Bijl, & Ravelli, 2000; van Os, Linscott, Myin-Germeys, Delespaul, & Krabbendam, 2009).
Use of CE can help people with distressing psychosis toexplore the meaning of these findings and reflect on whatthis means for them personally. It is important, however,to ensure that normalizing information is provided in arespectful manner, and is consistent with the goals of theclient, in order to avoid minimizing their difficulties.
Depending on the question being investigated, wemightalso encourage clients to construct surveys which we theninvite our colleagues to complete anonymously, perhapsusing online questionnaires. Here, client and therapistagree upon a question to ask as well as a method of ratingresponses. Collaboration is essential; without it there is anincreased chanceofmisunderstanding, risking the eventualresults being meaningless to the client. An example of atypical survey question is provided in Box 2. Such surveysare very useful tools for normalizing and destigmatizingwhat clients believe are unusual, frightening, or shamefulexperiences. They are also a good example of CE inpractice. Such surveys can also be conducted by the clientthemselves, if they feel sufficiently safe in doing so; forexample, a person who believes that others can hear theirthoughts may trust particular family and friends enough toask them about this.
While providing clients with empirical normalizingevidence is important, so is helping clients realize theimpact of their appraisals on their distress and behavioralresponses. Thus, we suggest normalizing should always becarried out within the context of a basic formulation, andthat the degree of conviction in the abnormality-relatedappraisal, as well as degree of related emotional distress, ismeasured before and after the provision of information,perhaps using a simple 0–100 scale. Regular monitoringof these variables can help clients begin to appreciate thelinks between cognition and emotional distress.
Examining the Advantages and Disadvantages of Appraisalsand Core Beliefs
Normally, one of the first things we do is encourageclients to consider the various nonempirical ormotivational
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

Box 2Sample survey question
If a person you met and liked told you they heard voices, would this *alone* makeyou feel reluctant to develop a friendship with them?
Yes, I would not want to be friends with someone who heard voices
No, the fact they hear voices has no bearing on my decision to be friends with
them I don't know
Other (please specify)
6 Hutton & Morrison
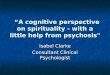
reasons for and against holding their particular appraisalsand beliefs. Carrying out an analysis of the advantages anddisadvantages of a particular belief or experience can behelpful, using either a simple 2-column approach ororthogonal continua, as shown in Figure 1. This analysiscan help clients appreciate that we often believe things forreasons other than the truth, introducing the idea thatmotivational factors might lead to attentional biases and areluctance to consider alternative explanations. However,the main reason for such an analysis is to seek informedconsent to reexamine their beliefs and explore alternativeexplanations. This is especially important given theambivalence that many clients report in relation to theirpsychotic experiences and the potential benefits that theyderive. For example, it has been suggested within specificcognitive models that delusions such as persecutory ideas(Bentall, Corcoran, Howard, Blackwood, & Kinderman,2001) and grandiosity (Knowles et al., 2011) may help toprotect self-esteem, and it is well documented thatexperiences such as voice hearing can provide benefitssuch as companionship (Miller, O'Connor, & DiPasquale,1993). Recent cognitive models have highlighted theself-protective function of withdrawal, avolition, anhedonia,and other negative symptoms (Perivoliotis & Cather, 2009).
There is a school of thought that the therapist shouldinvest effort in ensuring more disadvantages thanadvantages are elicited and written down, on the basisthat clients can sometimes be swayed into reexaminingtheir beliefs by the simple appearance of there being moredisadvantages. Whether this and other such tactics fitswith CE is a matter for debate. An alternative approach isto discuss the advantages and disadvantages in as honest,collaborative, and exhaustive a way as possible, based onthe assumption that this will provide both client andtherapist with the most accurate understanding of themotivational architecture surrounding the belief, andallow clients to make a truly informed choice as towhether they wish to proceed. Of course, this approachmay increase the risk that clients may not agree toexamining their beliefs. Indeed many people, when
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
asked, may prefer to live in a world they know and arefamiliar with, regardless of whether it is fictional (DeBrigard, 2010; Festinger, Riecken, & Schachter, 1956). Itcan, therefore, be extremely helpful to ask clients whether,if there was a way of looking at things that kept theadvantages of the existing appraisal or belief but had fewerof the disadvantages, this is something they would like toconsider. Emphasizing that they can determine the pace ofdeveloping this alternative perspective can help to reducetheir anxiety about the uncertainty they might have toendure. If a client chooses not to proceed to evaluate theirbelief, then it may be possible to negotiate an attempt toobtain the advantages in some other manner and thenrevisit the cost-benefit analysis; for example, if self-esteem isprotected by a delusional belief, use ofCT strategies derivedfrom a cognitive approach to self-esteem (Fennell, 1997)may be beneficial.
If andwhen some reasonable alternative explanations aredeveloped, then these can also be subject to an advantages-disadvantages analysis, thus hopefully demonstrating thatthe new perspective is worth considering inmore detail. Thepotential disadvantage of this strategy is that it risks implicitlylegitimizing the formation of beliefs on motivationalgrounds, rather than on empirical observation and rationalenquiry. However, as it is the client who will have to livewith the long-term consequences of any belief change, it isimportant that they fully participate in the decision as towhether to subject a particular belief to detailed evidentialanalysis. Again, this process should be explicitly linked totheir goals.
Generating Alternatives and Examining the EvidenceThere is good evidence that delusions are associated
with a tendency to form judgments quickly based on limitedevidence (Fine et al., 2007), difficulty producing alternativeexplanations (Freeman et al., 2004) and, therefore, greater“belief inflexibility” (Garety et al., 2005). Interventionsdesigned, among other things, to encourage people togenerate more alternative explanations show promise inreducing delusions and positive symptoms generally(Aghotor et al., 2010; Moritz, Kerstan, et al., 2011; Moritz,Veckenstedt, et al., 2011; Ross et al., 2011), and there is anexpert consensus that they are a particularly importantcomponent of CBT for psychosis (Morrison & Barratt,2010).
When carrying out this exercise, the therapist canprovide knowledge of the range of possible causes forparticular experiences (e.g., stress, sleep deprivation,anxiety, depression, trauma, use of alcohol or drugs,suggestibility, coincidence, etc.), or, in the spirit of CE,refer the client to investigate these topics for themselves viathe Internet. They can also help to focus the discussion ofsuch information if it begins to wander unproductively, andutilize Socratic questioning/guided discovery to help the
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

Can't keep information secret Helps to explain things
People may use information for their own gain Means I'm not 'mad' or 'mentally ill'People may judge my thoughts negatively May mean I'm special
DISADVANTAGES ADVANTAGES
Means I don't know what's going on? Can keep information secret
Means I might worry I'm mentally ill Means others have less power over meMeans I'm less important or special? Can have private thoughts like everyone else
IF TRUE
IF FALSE
Figure 1. Advantages and disadvantages of James’ belief that other people can read his mind.
7Collaborative Empiricism in CT for Psychosis
person to reflect on this information and draw their ownconclusions. Once a list of alternatives is produced, theevidence for and against each one can then be examined.Evidential analysis should be completed as collaborativelyas possible; the aim here is not to change the client's mind.Rather, the aim is to help clients learn a process that willimprove their general ability to consider the full range ofevidence available to them.
Nonetheless, it is helpful to ask the client to rate theirconviction in their appraisal and level of distress, before andafter the exercise. As with normalizing, this can help themappreciate the relationship between appraisal convictionand distress, as well as demonstrate the potential benefits ofthis process. A reduction in conviction may help clientsrealize their current strategies are not necessarily helpingthem to establish the whole truth, while no or minimalreduction may suggest the presence of other importantfactors, as yet unconsidered. As clients becomemore skilledat this process, they can be encouraged to increase their useof it in situations outside of therapy. We describe how thiswas used with one of our clients in Box 3.
Behavioral ExperimentsBehavioral experiments in CT for psychosis exemplify
CE and have many advantages as a strategy for achievingcognitive change (Bennett-Levy, 2004). There is a consen-sus that they are an important component of CT for psy-chosis (Morrison & Barratt, 2010; Wykes, Steel, Everitt, &
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
Tarrier, 2008), and we believe they are probably the mosteffective way of helping clients evaluate their existingappraisals and beliefs.
Most importantly, they help clients discover the impactof changing their behavior on their appraisals, while thecompelling experiential learning they offer is best-placed tocounter the negative experiential learning that has oftencontributed to the development of problematic appraisals.Behavioral experiments also tend to generate new empiricalobservations, which can lead to new explanations and dis-coveries for both client and therapist. Moreover, if clientscan learn to conduct their own behavioral experiments,then they will learn an important transferable skill. Theprocess of planning, conducting, and interpreting behav-ioral experiments in CBT for psychosis has been discussedin depth elsewhere (Morrison, Renton, Dunn, et al., 2004).Here we present a transcript (a composite of variousanonymized cases) that illustrates the use of CE to plan abehavioral experiment in order to test a client's belief thatthey have no control over their voices:
n C
THERAPIST: Can I just check that your goal is still toincrease your sense of control over your voices to50%, from what it is currently — 0% I think yousaid? Or has your goal changed at all?
CLIENT: Yeah, I'd be happy with 50% control.
ognitive Therapy for Psychosis: A Practice Guide, Cognitive and

Box 3Case example of a 53-year-old woman with perse-cutory delusions and a diagnosis of paranoid schizo-phrenia, illustrating the benefits of helping clientsgenerate alternative explanations.
Janet was a 53-year-old women who did nothave fixed accommodation. She slept in her carmost nights, or in a local women's hostel. Sherefused all offers of tenancy from the localauthorities. She had been given a diagnosis ofparanoid schizophrenia some 20years ago, butwould not engage with medical staff andtherefore was not taking antipsychotic medica-tion. Janet did, however, accept financial andlegal assistance from social care staff. She alsoagreed to begin a course of cognitive therapy,although it soon became clear that she wasambivalent about this—mainly because shebelieved her paranoia kept her safe (which itmay have). Although Janet had complex beliefsabout being persecuted by various governmentdepartments, she prioritized controlling every-day anger as a therapy goal.
Janet struggled a great dealwith attention andmemory, and had to be continually prompted toattend therapy sessions. She would spend mostof the early sessions shouting angrily about thepersecution she had received that week. Shewould flit from topic to topic as her affectincreased in the session, and sheactively resistedagenda-setting.
Nonetheless, she and the therapist wereable to produce a simply event-thought-feeling-behavior diagram of the anger, and an analysisof the advantages and disadvantages of it. Theythen spent several sessions practicing gener-ating alternative explanations for recent anger-inducing events, which Janet found useful.Initially the therapist had to take the lead on gen-erating situational attributions, as Janet tendedto focus on blaming others. They discussed howthis tendency might fuel her anger and paranoia,which led to a review of the advantages anddisadvantages of the latter. As with anger,the advantages were centered around stayingsafe and not being weak. Generating alternativeexplanations was acceptable to Janet as shefound that it enhanced her ability to accuratelyanticipate threat, rather than reduce it. SoonJanet was practicing this in her daily life inrelation to both anger and paranoia-inducingevents. She felt a greater sense of control as a
8 Hutton & Morrison
Please cite this article as: Hutton & Morrison, Collaborative Empiricism in CBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
x 3 (continued)
sult, and there was a noticeable decrease invels of affect in the sessions, and she wasuch more able to stay focused on the “list ofings to discuss.”
relemth
Bo
THERAPIST: And we've discussed whether theremight be a link between what you do to cope withthe voices, and your belief that you have no controlover them — although we're not totally sure?
CLIENT: Yeah, I know what you're saying makessense, but I just don't know…
THERAPIST: And we also discussed how there mightbe a link between believing you have no control,your anxiety, and the frequency of your voices — ifyou remember we discussed this sort of unhelpful“loop” that seems to take place [points to diagram].
CLIENT: Yeah, this is what happens. I start panickingthat I've lost control, and then this vicious cycle sortof develops and before I know it the voices arereally loud and I feel really confused…
THERAPIST: Okay, so I wonder … how would you feelabout testing some of this out? If it turned out thatsome of the things you are currently doing to copeare actually working against you, do you think thatwould be useful to know? I know I would find ituseful, as it would help me understand what's goingon a bit better. But what do you think?
CLIENT: Yeah, but how do we do that?
THERAPIST: Well, let's have a look at what you'redoing. We've got it written down here that youoften try and push the voices away in your mind —you tell them to shut up or try really hard to ignorethem. Can you think of an alternative approach?
CLIENT: No, not really. I just get so frustrated andangry sometimes.
THERAPIST: I completely understand, and I thinkyour response to them is very understandable. Iwonder … have you ever tried to simply observe thevoices in a detached way, as if you were watchingsomething happening in the street outside yourwindow; just observing and not getting involved?
ognitive Therapy for Psychosis: A Practice Guide, Cognitive and

9Collaborative Empiricism in CT for Psychosis
PB
CLIENT: No, I think I always try and argue with them.Or when I've had enough I shout at them. When it'sreally bad I'll just get drunk.
THERAPIST: Yes, you mentioned your alcohol usebefore and how it helps in the short-term, but notthe day after? Have I got that right? [client nods].Going back to this, how would you feel about tryingout this new approach just now? Are you hearingvoices as we speak?
CLIENT: I am, yeah … Okay, I'll give it a go — but I'mnot really sure what I need to do.
THERAPIST: That's okay, I'll talk you through it. Can Ijust ask: if it turns out that shouting at the voicesand engaging with them is making them worse,what are the implications of that for you?
CLIENT: Well, it would mean I had some control …
THERAPIST: And you currently believe you have nocontrol? [client nods]. Ok, so would you be willingto compare your old approach to the new one Imentioned?
CLIENT: Sure …
THERAPIST: And how we will measure the voices? Doyou want to look at frequency, loudness, number ofvoices, or something else?
CLIENT: Loudness is the main issue for me.
THERAPIST: Right, and what do you think will happento the loudness of the voices if you stop trying toshout at them and observe them in a detached wayinstead?
CLIENT: Well, when I've tried this in the past they'vegot louder, so I've just started shouting at themagain. But I guess I'm pretty quick to give up on notshouting [laughs].
THERAPIST: Right, so one possibility is they'll getlouder to start with. If that started to happen, wouldyou be willing to persist with the new approach a bitlonger than you have in the past?
CLIENT: Okay, I'll try.
THERAPIST: Also, before we start — if it turns out thevoices do get louder the louder you shout, howwould you make sense of that?
lease cite this article as: Hutton & Morrison, Collaborative Empiricism iehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
CLIENT: Don't know …
THERAPIST: Okay, let's imagine for a second they gotreally quiet when you whisper to yourself … whatwould that mean, do you think?
CLIENT: Mmmm … [long pause]. I guess it mightmean the voices are me, or a part of me? Like it saysin that book you gave me.
THERAPIST: Right, okay. And if that were the case,how would you make sense of that?
CLIENT: It would mean I could control them! I'd berelieved.
THERAPIST: Okay, sounds like that would fit with youroverall goal then? Let's come back to this. Beforewe go ahead with our experiment, tell me; howwould you like to measure “loudness”?
CLIENT: I don't know, maybe use some sort of scale …
THERAPIST: Great idea — what sort of scale?
This illustrates several key aspects of experiment-planning that we believe are important: The experimentmust be in the service of the client's goals, and normallyserve as a test of hypotheses arising from the formulationthat both client and therapist agree would be importantand beneficial to test.
The planning must also be as collaborative as far aspossible (depending on the client's familiarity with theprocess), and predictions and implications normally needto be elicited before running the experiment.Moreover, allrelevant variables need to be operationalized and measur-able. There are a wide range of possible behavioral experi-ments that can be used in psychosis (Morrison, Renton, etal., 2004), but often the therapist and client will need to usetheir creativity to devise their own. Once the experimenthas been completed, then socratic questioning can be usedto work with the client to explore the implications of thenew information on the case conceptualization, as well asthe treatment plan.
Socratic QuestioningSocratic questioning has been defined as “a method of
guided discovery in which the therapist asks a series ofcarefully sequenced questions to help define problems,assist in the identification of thoughts and beliefs, examinethe meaning of events, or assess the ramifications ofparticular thoughts or behaviors” (Beck & Dozois, 2011).Others describe it as a process involving “…(1) gatheringdata, (2) looking at this data in different ways with the
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

10 Hutton & Morrison
client, (3) inviting the client to devise his own plans for whatto do with the information examined . . .” (Padesky, 1993),suggesting Socratic questioning and CE are closely linkedconcepts.
Experience suggests some adaptations need to be madeto Socratic questioning when working with psychosis.Concentration, memory problems and distracting voicescan mean it might take longer to explore an issue, and if aperson is suffering from conceptual disorganization orexperiencing “flight of ideas,” then it can be advisable tointroduce more structure than you might otherwise.Exploring one question at a time (e.g., the advantages ordisadvantages of a particular behavior) can help here, as itprovides a point of return for the conversation if it starts toveer off. Taking a CE approach to planning how to deal withunproductive departures may also help. This might involveasking the client howheor she thinks these departures couldbest be understood and managed, and then testing this out.
Work Between SessionsThe use of CE in CT for psychosis is also very important
in the development and implementation of work betweensessions, which is of vital importance in maximizing gainsfrom therapy (Dunn, Morrison, & Bentall, 2002; Dunn,Morrison, & Bentall, 2006; Morrison & Barratt, 2010;Morrison, Renton, Dunn, et al., 2004). Helping a clientchoose when and how to evaluate the accuracy of theirbeliefs and the utility of particular cognitive and behavioralresponses outside of therapy sessions is an essential elementof CE in CT.
However, therapists should be aware of the risk ofsuggesting an unequal “teacher-pupil” relationship whenplanning this work. We suggest considering terminologycarefully. “Homework” carries particular implications ofschoolwork, and might be best avoided. “Home tasks,”“things to try for next time,”or “workbetween sessions”maybe more acceptable terms. Providing a very clear rationalefor engaging in suchwork is very important, asmany peoplewith psychosis struggle withmotivation, memory, attention,and concentration (Dunn et al., 2002; Kilbride et al., 2012;Rector, 2007).
It can be helpful to explain to clients, in the first sessionand then again at the end of the first few sessions, thatengaging in such work will make it more likely theywill achieve their goals. We advise that people tend to “getout what they put in.” If clients seem reluctant, we wouldencourage them to consider doing work outside the ses-sions as an experiment. Detailed guides to between-session work in CT are available elsewhere, outliningideas for both the process and the content of such work(Kazantzis, 2005; Morrison, Renton, et al., 2004; Rector,2007). A range of helpful tasks are outlined by Rector,covering the whole period of therapy from engagement todischarge planning.
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
Suffice it to say, one of the best ways to ensure thatbetween-session work is planned in a collaborative andmeaningful way is to set aside sufficient time. A goalshould be agreed on, thus providing the client with arationale for the subsequent task. It is also important thatbetween-session work takes place from the first or secondsession; otherwise, it can be easy for both therapist andclient to fall into the trap of avoiding it. Between-sessionwork is not just for clients, of course, and oneway to developthe sense of therapist and client being co-investigators is toagree on tasks for the therapist aswell. Perhaps the therapistcan ask the client to suggest things for him or her to do?An advantage of this is that it makes it more likely the clientwill persist with his or her plans.
An important development in the last few years hasbeen the publication of several self-help books for psychosis.It is entirely fitting with a CE approach for a client to beencouraged to read, between sessions, a chapter or twofrom one of these books, which at present cover paranoia(Freeman, Freeman,&Garety, 2006) andpsychosis generally(Morrison, Renton, French, & Bentall, 2008; Turkingtonet al., 2009). Clients who struggle to read may find itmore acceptable to listen to audio recordings of importantinformation instead (French et al., 2010).
Focusing on Recovery and Functioning
CE in CT for psychosis is not limited to focusing onproblematic experiences like hallucinations and paranoia.In line with the recovery approach, an emphasis on CE inCT can help people work out and overcome the obstaclesthey might face in relation to other goals, such as startingcollege, going to work, and having a relationship.
We discussed earlier how cognitive approaches haveposited a major role for self-defeating beliefs in lowfunctioning, low motivation, and other so-called negativesymptoms in psychosis (Rector et al., 2005). The develop-ment of such beliefs can pre-date formal transition topsychosis (Perivoliotis, Morrison, Grant, French, & Beck,2009), and therefore may be a consequence of the earlyadversity we know many people with psychosis haveendured (Varese et al., 2012). However adversity oftencontinues oncepeople receive a diagnosis.While symptoms,stigma, and social exclusion have been linked to disem-powerment (Brohan et al., 2010; Strack & Schulenberg,2009), the impact of coercive treatment, in many ways theantithesis of CE, has also come under the spotlight (Burnset al., 2011; Grealish, Tai, Hunter, & Morrison, 2011; Strack& Schulenberg, 2009; Zigmond, 2011).
We are not aware of research examining how use ofCE relates to subjective empowerment and recovery gen-erally, although a majority of clients in a recent service-userled qualitative study discussed benefits from CBT relatingto “sharing control,” “reappraising psychological diffi-culties through evidence-gathering,” and “achievement,
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

Box 4Ideas to facilitate collaborative empiricism in thecontext of very high conviction (no particular order).
• Empathize as much as possible with theclient's distress,maintaining an agnostic “neu-tral” position, but modeling an inquisitive andhypothesis-testing approach.
• Try keeping the shared goals as explicit aspossible. If a client challenges you over whetheryou believe them or not, being very clear thatyour aim is to help themachievewhatever goal itis they have set themselves can legitimize theprocess and motivate the patient to continuewith it. If a person does not have clear goalswhich legitimize the formulation, then you areprobably formulating the wrong thing.
• Ensure you have examined and understood allthe advantages and disadvantages of high-conviction appraisals.
• Limit direct discussion of the high-convictionbelief and instead focus on understandingproblem maintenance at the metacognitivelevel (i.e., worry about worry), or focus onimproving self-esteem.
• If a client cares a great deal about you acceptingtheir belief as true, then consider examiningwhy.Formulate and address their concerns about notbeing believed.
• Agree to respectfully disagree, drawattention tobenefits and prevalence of divergent views,emphasize that not sharing a belief does notmean you think they are less intelligent orinferior, help them think about times they haveexperienced a positive relationship despite notsharing a particular view, help clients considerpeople who can work well together on sharedgoals despite divergent views, outline thebenefits of therapist taking a “critical friend” or“devil's advocate” role.
• Share the dilemma with the client. Let themknow that you are trying to help, but you areworried that not sharing their belief is going tojeopardize engagement.
• Wait. Focus on something less “hot” andwait fora timewhere the person is simplymore amenableto taking a CE approach in relation to a particularbelief. Conviction fluctuates a great deal in psy-chosis and there will be times when a patientexperiences considerable dissonance. They maythenbewilling to standback fromtheir beliefs andconsider them as hypotheses rather than facts.
11Collaborative Empiricism in CT for Psychosis
empowerment and indepedence in recovery” (Kilbrideet al., 2012). Some studies have also examined the impact oftraining patients and staff in shared decision-making, acousin of CE (Tee & Kazantzis, 2011), on various outcomes(Deegan, 2010; Deegan, Rapp, Holter, & Riefer, 2008;Duncan, Best, & Hagen, 2010; Hamann, Mendel, Meier,et al., 2011), with results indicating that patients whoreceived the training were more interested and motivatedto be involved in treatment decisions afterwards (Hamann,Mendel, Meier, et al., 2011). However, psychiatrists ratedpatients who received the training as more difficult to treat,while patients rated their psychiatrists as less trustworthyand becamemore skeptical about the benefits of treatment.Such outcomes are not incompatible with service userconcepts of recovery, where qualitative user-led researchhas identified “a collaborative approach,” “protection ofharm from professionals,” “alternatives to the medicalmodel” as key themes (Pitt et al., 2007).
Challenges in Using CE in Psychosis
A potential obstacle to taking a CE approach might bethe level of education clients have received, as well as theircurrent cognitive resources. Problems with memory,attention, and concentration are well-observed in psychosis,and can affect the ability of people to fully engage intherapeutic work. However, we do not wish to give theimpression that CE is only possible with college-educatedclients with intact cognitive functioning. While minimizingthe complexity of the formulation and intervention planmay benefit clients with fewer years of education orcognitive difficulties, this should not affect the general CEapproach. Staying focused on one topic at a time, providingclients with clear written summaries, and encouraging themto listen to tape recordings of sessions are strategies thatmight help with CT in general.
Working collaboratively with people who are completelyconvinced by their particular explanations can also be verychallenging. There is evidence that CT might be lessbeneficial for those with low belief flexibility (Garety et al.,1997) or high conviction (Brabban, Tai, & Turkington,2009), although other work suggests baseline degree of“psychological orientation to problems” may be a moreimportant factor in determining who engages in fulltherapy (Freeman et al., 2012). Successfully taking a CEapproach with these clients depends to a large extent ontheir goals, the quality of the therapeutic relationship, andthe motivational architecture that supports the client'sbelief system. In Box 4 we outline a variety of strategies thatmight help therapists useCEwhenworkingwith clients withhigh conviction.
Conceptual disorganization presents another potentialchallenge to using CE, in so far as it has a negative effect oncommunication. Conceptual disorganization includes,among other things, derailment of ideas and flow of
Please cite this article as: Hutton & Morrison, Collaborative Empiricism in Cognitive Therapy for Psychosis: A Practice Guide, Cognitive andBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003

12 Hutton & Morrison
speech, tangentiality, drifting from topic under discus-sion, incoherence and illogicality (Beck et al., 2009).There are many possible causes for these difficulties, butthere is evidence that high levels of affect and personaldisclosure (Docherty, Evans, Sledge, Seibyl, & Krystal,1994; Docherty, Hall, & Gordinier, 1998; Haddock,Wolfenden, Lowens, Tarrier, & Bentall, 1995; Shimku-nas, 1972; Tai, Haddock, & Bentall, 2004), trauma (Read,Agar, Argyle, & Aderhold, 2003), childhood maltreat-ment (Toth, Pickreign Stronach, Rogosch, Caplan, &Cicchetti, 2011), intrusive thoughts and memories(Harrow, Lanin-Kettering, Prosen, & Miller, 1983),difficulty understanding the needs of listeners (Sarfati& Hardy-Bayle, 1999), and problems with working andsemantic memory (Beck et al., 2009; Bentall, 2003;McKenna & Oh, 2005) may contribute.
If disorganized speech or thought is proving a barrierto CE then, in the spirit of CE, the therapist might con-sider sharing their dilemma with the client. Conceptualdisorganization is rarely continuous, and moments ofclarity can be used to explore ways in which therapist andclient canmanage the issue. Encouraging clients to listen toa recording of their speech may lead to useful insights(Harrow & Prosen, 1978). For example, after listening toa recording, one of our clients volunteered that when shefelt emotionally exposed—or bored—she automatically“switched the channel” in her mind. Further discussionsuggested this meant she disengaged from what was cur-rently happening, and stopped monitoring her speech—something she had learned to do when coping withtrauma in the past. This led to a further discussion of theadvantages and disadvantages of this strategy now, andcollaborative generation of alternative strategies. Theseincluded scheduling short breaks and agreeing on asignal they could use to indicate when a change of topicwas required. As outlinedbyBeck and colleagues, therapistsand client can jointly try to identify what appraisals lead toincreases in emotional arousal and subsequent problemswith communication.
A client's interest in being involved in decision-makingabout the process of therapy may be another variableimpacting on use of CE. For instance, Hamann andcolleagues found that clients who judged their owndecision-making to be poor or who were poorly educateddid not wish to take part in shared decision-makingtraining regarding medical treatment, particularly if theywere not dissatisfied with their treatment (Hamann,Mendel, Reiter, et al., 2011). Whether this means theywould not have benefitted had they received the trainingis unclear, as is the extent to which these patientsendorsed defeatist beliefs about their own ability. Furtherresearch examining the link between self-defeatingbeliefs, perception of cognitive impairment and desireto engage in either collaborative empiricism and/or
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
shared decision-making would be useful, particularlygiven such beliefs may mediate the impact of cognitiveimpairment on functioning (Grant & Beck, 2009).
Summary and Conclusion
Our aim was to discuss the use of CE in CT forpsychosis. We offered some thoughts on the nature of CEand why it is particularly important when working withthis often marginalized and disempowered group. Finally,we offered some suggestions and guidance on how best toimplement CE in CT for psychosis.
One particular theme to emerge from this article isthat CE enters into almost every part of CT for psychosis.We did not discuss evaluation or relapse prevention, butsuffice it to say, CE is an essential part of these therapycomponents too. Another theme readers may havenoticed is that there seem to be few differences betweenCT for emotional disorders and CT for psychosis. Fewadaptations are required, in our view, although we concurwith others that maintaining a CE approach perhaps canrequire greater investment at times (Beck et al., 2009).However, unless a person is particularly unwell, then CEin CT proceeds in a similar manner to CE in CT foranxiety and depression. We also hope we have shown whyCE is essential for achieving cognitive change in CT forpsychosis. In our experience, it is difficult to engage,assess, or work with highly suspicious people, or peoplewith high levels of conviction or preoccupation, withoutusing a CE approach.
The particular approach we present in this article is in-formed by considerations of research on expert views re-garding the key elements of CT for psychosis (Morrison &Barratt, 2010), qualitative studies of service-users’ experi-ences of CT for psychosis, recovery, and psychiatric treat-ment generally (Byrne et al., 2010;Dunn et al., 2002; Kilbrideet al., 2012; Pitt et al., 2007), empirical studies suggestingthe overall approach toCT is benefical (Morrison, French, etal., 2004; Morrison, Renton, Williams, et al., 2004; Morrisonet al., 2011; Morrison et al., 2012), and clinical experience(Hutton, Morrison, & Taylor, 2012; Morrison, 2001a).Nonetheless, many of our thoughts about CE and recom-mendations for its use need further empirical investigation,and should be taken as such. As outlined by Tee andKazantzis,muchwork needs to be done in understandingCEin CT generally (Tee & Kazantzis, 2011).
We also discussed how best to conceptualize CE. Weargued it can be viewed as both a technique in CT and anexpression of respect for patient autonomy. It would beuseful if future attempts to achieve consensus among CTfor psychosis experts could incorporate some discussionof the value and purpose of CE, and how best to assess it.It would also be of interest to investigate further serviceuser views on the importance or otherwise of CE in CT.Establishing whether there are links between cognitive
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

13Collaborative Empiricism in CT for Psychosis
impairment, defeatist beliefs and preferences for taking aCE approach may have implications for understandingand minimizing early discontinuation from CT (Freemanet al., 2012).
Finally, a recent qualitative, user-led study that examinedthe subjective experience of receiving CT for psychosishighlights the importance to clients of both collaborationand empiricism (Kilbride et al., 2012), as the followingquotations illustrate:
“It was very much a partnership between myself and thepsychologist, it was really put to me as team work, which Ithought was great. It wasn't that someone else has anagenda…it was centred aroundme which I'd not come acrossbefore in anything really in medicine or psychiatry”
“I think the evidence thing's kind of good, sort of it is realand you have to sort of work out well, is it likely to be real. Likeif you think, say, people taking thoughts out of my head, anderm, it's sort of well what's the proof that they are”
References
Aghotor, J., Pfueller, U., Moritz, S., Weisbrod, M., & Roesch-Ely, D.(2010). Metacognitive training for patients with schizophrenia(MCT): Feasibility and preliminary evidence for its efficacy.Journal of Behavior Therapy and Experimental Psychiatry, 41, 207–211.http://dx.doi.org/10.1016/j.jbtep. 2010.01.004
Andreasen, N. C., Carpenter,W. T., Jr., Kane, J. M., Lasser, R. A., Marder,S. R., & Weinberger, D. R. (2005). Remission in schizophrenia:Proposed criteria and rationale for consensus. American Journal ofPsychiatry, 162, 441–449. http://dx.doi.org/10.1176/appi.ajp. 162.3.441
Beck, A. T. (1967). Depression: Clinical, experimental and theoretical aspects.New York, NY: Harper and Row.
Beck, A. T., & Dozois, D. J. (2011). Cognitive therapy: Current statusand future directions. Annual Review of Medicine, 62, 397–409.http://dx.doi.org/10.1146/annurev-med-052209-100032
Beck, A. T., Grant, P. M., Huh, G. A., Perivoliotis, D., & Chang, N. A.(2011). Dysfunctional attitudes and expectancies in deficit syn-drome schizophrenia. Schizophrenia Bulletin. http://dx.doi.org/10.1093/schbul/sbr040
Beck, A. T., Rector,N. A., Stolar, N.M.,&Grant, P.M. (2009). Schizophrenia:Cognitive theory, research, and therapy. New York, NY: Guilford Press.
Bennett-Levy, J. (2004). Oxford guide to behavioural experiments in cognitivetherapy. New York, NY: Oxford University Press.
Bentall, R. P. (2003). Madness explained: Psychosis and human nature.London, England: Penguin.
Bentall, R. P., Corcoran, R., Howard, R., Blackwood, R., & Kinderman, P.(2001). Persecutory delusions: A review and theoretical integration.Clinical Psychology Review, 22, 1–50.
Brabban, A., Tai, S., & Turkington, D. (2009). Predictors of outcome inbrief cognitive behavior therapy for schizophrenia. SchizophreniaBulletin, 35, 859–864. http://dx.doi.org/10.1093/schbul/sbp065
Brett-Jones, J., Garety, P., & Hemsley, D. (1987). Measuring delusionalexperiences: A method and its application. British Journal of ClinicalPsychology, 26, 257–265.
British Psychological Society (2000). Recent advances in understandingmental illness and psychotic experiences. Leicester: British PsychologicalSociety.
Brohan, E., Elgie, R., Sartorius, N., Thornicroft, G., Group, G. A. -E. S.,Arteel, P., . . . Pievskaya, J. (2010). Self-stigma, empowerment andperceived discrimination among people with schizophrenia in 14
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
European countries: The GAMIAN-Europe study. SchizophreniaResearch, 122, 232–238.
Burns, T., Yeeles, K., Molodynski, A., Nightingale, H., Vazquez-Montes,M., Sheehan, K., & Linsell, L. (2011). Pressures to adhere totreatment ('leverage') in English mental healthcare. British Journalof Psychiatry, 199, 145–150. http://dx.doi.org/10.1192/bjp.bp.110.086827
Byrne, R. E., Davies, L., & Morrison, A. P. (2010). Priorities andpreferences for the outcomes of treatment of psychosis: A serviceuser perspective. Psychosis, 2, 210–217.
Chadwick, P. D., Birchwood, M. J., & Trower, P. (1996). Cognitive therapyfor delusions, voices and paranoia. Chichester: Wiley.
Collerton, D., & Dudley, R. (2004). A cognitive behavioural frameworkfor the treatment of distressing visual hallucinations in olderpeople. Behavioural and Cognitive Psychotherapy, 32, 443–455.
Couture, S. M., Blanchard, J. J., & Bennett, M. E. (2011). Negativeexpectancy appraisals and defeatist performance beliefs andnegative symptoms of schizophrenia. Psychiatry Research, 189,43–48. http://dx.doi.org/10.1016/j.psychres.2011.05.032
Daalman, K., Boks, M. P., Diederen, K. M., de Weijer, A. D., Blom, J. D.,Kahn, R. S., & Sommer, I. E. (2011). The same or different? Aphenomenological comparison of auditory verbal hallucinationsin healthy and psychotic individuals. Journal of Clinical Psychiatry,72, 320–325. http://dx.doi.org/10.4088/JCP.09m05797yel
David, A. S. (2010). Why we need more debate on whether psychoticsymptoms lie on a continuum with normality. Psychological Medicine,40, 1935–1942. http://dx.doi.org/10.1017/S0033291710000188
De Brigard, F. (2010). If you like it, does it matter if it's real?Philosophical Psychology, 23, 43–57.
Deegan, P. E. (2010). A web application to support recovery and shareddecision making in psychiatric medication clinics. PsychiatricRehabilitation, 34, 23–28. http://dx.doi.org/10.2975/34.1.2010.23.28
Deegan, P. E., & Drake, R. E. (2006). Shared decision making andmedication management in the recovery process. Psychiatric Services,57, 1636–1639. http://dx.doi.org/10.1176/appi.ps.57.11.1636
Deegan, P. E., Rapp, C., Holter, M., & Riefer, M. (2008). Best practices:A program to support shared decision making in an outpatientpsychiatric medication clinic. Psychiatric Services, 59, 603–605.http://dx.doi.org/10.1176/appi.ps.59.6.603
Docherty, N. M., Evans, I. M., Sledge, W. H., Seibyl, J. P., & Krystal, J. H.(1994). Affective reactivity of language in schizophrenia. Journal ofNervous and Mental Disease, 182, 98–102.
Docherty, N.M., Hall, M. J., &Gordinier, S.W. (1998). Affective reactivityof speech in schizophrenia patients and their nonschizophrenicrelatives. Journal of Abnormal Psychology, 107, 461–467.
Duncan, E., Best, C., & Hagen, S. (2010). Shared decision makinginterventions for people with mental health conditions. CochraneDatabase, CD007297. http://dx.doi.org/10.1002/14651858.CD007297.pub2
Dunn, H., Morrison, A. P., & Bentall, R. P. (2002). Patients' experiencesof homework tasks in cognitive behavioural therapy for psychosis: Aqualitative analysis. Clinical Psychology and Psychotherapy, 9, 361–369.
Dunn, H., Morrison, A. P., & Bentall, R. P. (2006). The relationshipbetween patient suitability, therapeutic alliance, homework compli-ance and outcome in cognitive therapy for psychosis. ClinicalPsychology and Psychotherapy, 13, 145–152.
Elwyn, G., Laitner, S., Coulter, A., Walker, E., Watson, P., & Thomson, R.(2010). Implementing shared decision making in the NHS. BritishMedical Journal, 341. http://dx.doi.org/10.1136/bmj.c5146
Fennell, M. J. V. (1997). Low self-esteem: A cognitive perspective.Behavioural and Cognitive Psychotherapy, 25, 1–26.
Festinger, L., Riecken, H. W., & Schachter, S. (1956).When prophecy fails.Minneapolis: University of Minnesota Press.
Fine, C., Gardner, M., Craigie, J., & Gold, I. (2007). Hopping, skipping orjumping to conclusions? Clarifying the role of the JTC bias indelusions. Cognitive Neuropsychiatry, 12, 46–77. http://dx.doi.org/10.1080/13546800600750597
Fowler, D., Garety, P., & Kuipers, E. (1995). Cognitive-behaviour therapy forpsychosis: Theory and practice. Chichester: Wiley.
Freeman, D., Dunn, G., Garety, P., Weinman, J., Kuipers, E., Fowler, D.,Jolley, S., & Bebbington, P. (2012). Patients' beliefs about the
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

14 Hutton & Morrison
causes, persistence and control of psychotic experiences predicttake-up of effective cognitive behaviour therapy for psychosis.Psychological Medicine, 1–9. http://dx.doi.org/10.1017/S0033291712001225
Freeman, D., Freeman, J., & Garety, P. A. (2006). Overcoming paranoidand suspicious thoughts. London: Robinson.
Freeman, D., & Garety, P. A. (2003). Connecting neurosis and psychosis:The direct influence of emotion on delusions and hallucinations.Behavior Research and Therapy, 41, 923–947. doi:S0005796702001043[pii].
Freeman, D., Garety, P. A., Fowler, D., Kuipers, E., Bebbington, P. E., &Dunn, G. (2004). Why do people with delusions fail to choose morerealistic explanations for their experiences? An empirical investiga-tion. Journal of Consulting and Clinical Psychology, 72, 671–680.
Freeman, D., Garety, P. A., Kuipers, E., Fowler, D., & Bebbington, P. E.(2002). A cognitive model of persecutory delusions. British Journalof Clinical Psychology, 41, 331–347.
French, P., Hutton, P., Barratt, S., Byrne, R., Parker, S., Shryane, N., &Morrison, A. P. (2010). Provision of online normalising informationto reduce stigma associated with psychosis: Can an audio podcastchallenge negative appraisals of psychotic experiences? Psychosis:Psychological, Social and Integrative Approaches, 3, 52–62.
Fulford, K. W. (2011). Bringing together values-based and evidence--based medicine: UK Department of Health Initiatives in the'Personalization' of Care. Journal of Evaluation in Clinical Practice,17, 341–343. http://dx.doi.org/10.1111/j.1365-2753.2010.01578.x
Garety, P., Fowler, D., Kuipers, E., Freeman, D., Dunn, G.,Bebbington, P., Hadley, C., & Jones, S. (1997). London-EastAnglia randomised controlled trial of cognitive-behaviouraltherapy for psychosis. II: Predictors of outcome. British Journalof Psychiatry, 171, 420–426.
Garety, P. A., Freeman, D., Jolley, S., Dunn, G., Bebbington, P. E., Fowler,D. G., Kuipers, E., & Dudley, R. (2005). Reasoning, emotions, anddelusional conviction inpsychosis. Journal of Abnormal Psychology, 114,373–384. http://dx.doi.org/10.1037/0021-843X.114.3.373
Garrett, M., Stone, D., & Turkington, D. (2006). Normalizing psychoticsymptoms. Psychology and Psychotherapy, 79, 595–610.
Grant, P. M., & Beck, A. T. (2009). Defeatist beliefs as a mediator ofcognitive impairment, negative symptoms, and functioning inschizophrenia. Schizophrenia Bulletin, 35, 798–806.
Grant, P. M., Huh, G. A., Perivoliotis, D., Stolar, N. M., & Beck, A. T.(2012). Randomized trial to evaluate the efficacy of cognitivetherapy for low-functioning patients with schizophrenia. Archives ofgeneral psychiatry, 69, 121–127. http://dx.doi.org/10.1001/archgenpsychiatry.2011.129
Grealish, A., Tai, S., Hunter, A., & Morrison, A. P. (2011). Qualitativeexploration of empowerment from the perspective of young peoplewith psychosis. Clinical Psychology and Psychotherapy. http://dx.doi.org/10.1002/cpp. 785
Greenwood, K. E., Sweeney, A., Williams, S., Garety, P., Kuipers, E.,Scott, J., & Peters, E. (2010). CHoice of Outcome In Cbt forpsychosEs (CHOICE): The development of a new service user-ledoutcome measure of CBT for psychosis. Schizophrenia Bulletin, 36,126–135. http://dx.doi.org/10.1093/schbul/sbp117
Grisso, T., Appelbaum, P. S., & Hill-Fotouhi, C. (1997). The MacCAT-T:A clinical tool to assess patients' capacities to make treatmentdecisions. Psychiatric Services, 48, 1415–1419.
Gumley, A., & Schwannauer, M. (2006). Staying well after psychosis.Chichester: Wiley.
Haddock, G., Wolfenden, M., Lowens, I., Tarrier, N., & Bentall, R. P.(1995). The effect of emotional salience on the thought disorderof patients with a diagnosis of schizophrenia. British Journal ofPsychiatry, 167, 618–620.
Hamann, J., Cohen, R., Leucht, S., Busch, R., & Kissling, W. (2005). Dopatients with schizophrenia wish to be involved in decisions abouttheir medical treatment? American Journal of Psychiatry, 162,2382–2384. http://dx.doi.org/10.1176/appi.ajp. 162.12.2382
Hamann, J., Mendel, R., Meier, A., Asani, F., Pausch, E., Leucht, S., &Kissling, W. (2011). "How to speak to your psychiatrist": Shareddecision-making training for inpatients with schizophrenia.Psychiatric Services, 62, 1218–1221. http://dx.doi.org/10.1176/appi.ps.62.10.1218
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
Hamann, J., Mendel, R., Reiter, S., Cohen, R., Buhner, M., Schebitz, M.,Diplich, S., Kissling, W., & Berthele, A. (2011). Why do somepatients with schizophrenia want to be engaged in medical decisionmaking andothersdonot? Journal of Clinical Psychiatry, 72, 1636–1643.http://dx.doi.org/10.4088/JCP.10m06119yel
Hamann, J., Mendel, R. T., Fink, B., Pfeiffer, H., Cohen, R., & Kissling,W.(2008). Patients' and psychiatrists' perceptions of clinical decisionsduring schizophrenia treatment. Journal of Nervous and MentalDisease, 196, 329–332. http://dx.doi.org/10.1097/NMD.0b013e31816a62a0
Harrow, M., Lanin-Kettering, I., Prosen, M., & Miller, J. G. (1983).Disordered thinking in schizophrenia: Intermingling and loss ofset. Schizophrenia Bulletin, 9, 354–367.
Harrow, M., & Prosen, M. (1978). Intermingling and disordered logicas influences on schizophrenic 'thought disorders'. Archives ofGeneral Psychiatry, 35, 1213–1218.
Hutton, P., Morrison, A. P., & Taylor, H. (2012). Brief cognitive-behavioural therapy for hallucinations: Can it help people whodecide not to take antipsychotic medication? A case report.Behavioural and Cognitive Psychotherapy, 40, 111–116.
Jackson, M., & Fulford, K. W. M. (1997). Spiritual experience andpsychopathology. Philosophy, Psychiatry and Psychology, 1,41–65.
Jenner, J. A., Rutten, S., Beuckens, J., Boonstra, N., & Sytema, S. (2008).Positive and useful auditory vocal hallucinations: prevalence,characteristics, attributions, and implications for treatment. ActaPsychiatrica Scandinavica, 118, 238–245. http://dx.doi.org/10.1111/j.1600-0447.2008.01226.x
Kazantzis, N. (2005). Using homework assignments in cognitive behaviortherapy. New York, NY: London: Routledge.
Kilbride, M., Byrne, R., Price, J., Wood, L., Barratt, S., Welford, M., &Morrison, A. P. (2012). Exploring service users’ perceptions of cognitivebehavioural therapy for psychosis: A user led study.Manuscript submittedfor publication.
Kingdon, D., & Turkington, D. (2005). Cognitive therapy for schizophrenia.New York, NY: Guilford Press.
Knowles, R., McCarthy-Jones, S., & Rowse, G. (2011). Grandiosedelusions: A review and theoretical integration of cognitiveand affective perspectives. Clinical Psychology Review, 31, 684–696.http://dx.doi.org/10.1016/j.cpr.2011.02.009
Kuyken, W., Padesky, C. A., & Dudley, R. (2008). The science andpractice of case conceptualization. Behavioural and CognitivePsychotherapy, 36, 757–768. http://dx.doi.org/10.1017/S1352465808004815
Mansell, W., Morrison, A. P., Reid, G., Lowens, I., & Tai, S. (2007). Theinterpretation of, and responses to, changes in internal states: Anintegrative cognitive model of mood swings and bipolar disorders.Behavioural and Cognitive Psychotherapy, 35, 515–539.
McKenna, P. J., & Oh, T. M. (2005). Schizophrenic speech: Making sense ofbathroots and ponds that fall in doorways. Cambridge: CambridgeUniversity Press.
Miller, L. J., O'Connor, E., & DiPasquale, T. (1993). Patients'attitudes to hallucinations. American Journal of Psychiatry, 150,584–588.
Monahan, J., Redlich, A.D., Swanson, J., Robbins, P. C., Appelbaum, P. S.,Petrila, J., . . . McNiel, D. E. (2005). Use of leverage to improveadherence to psychiatric treatment in the community. PsychiatricServices, 56, 37–44. http://dx.doi.org/10.1176/appi.ps.56.1.37
Moritz, S., Favrod, J., Andreou, C., Morrison, A. P., Bohn, F., Tonn, P.,& Karow, A. (2012). Beyond the usual suspects: positive attitudestowards positive symptoms predict medication noncompliance inpsychosis. Schizophrenia Bulletin, in press.
Moritz, S., Kerstan, A., Veckenstedt, R., Randjbar, S., Vitzthum, F.,Schmidt, C., Heise, M., &Woodward, T. S. (2011). Further evidencefor the efficacy of a metacognitive group training in schizophrenia.Behavior Research and Therapy, 49, 151–157. http://dx.doi.org/10.1016/j.brat.2010.11.010
Moritz, S., Veckenstedt, R., Randjbar, S., Vitzthum, F., & Woodward, T. S.(2011). Antipsychotic treatment beyond antipsychotics:Metacognitiveintervention for schizophrenia patients improves delusional symp-toms. Psychological Medicine, 41, 1823–1832. http://dx.doi.org/10.1017/S0033291710002618
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

15Collaborative Empiricism in CT for Psychosis
Morrison, A. P. (2001a). Cognitive therapy for auditory hallucinationsas an alternative to antipsychotic medication: A case series. ClinicalPsychology and Psychotherapy, 8, 136–147.
Morrison, A. P. (2001b). The interpretation of intrusions in psychosis:An integrative cognitive approach to hallucinations and delusions.Behavioural and Cognitive Psychotherapy, 29, 257–276.
Morrison, A. P., & Barratt, S. (2010). What are the components of CBTfor psychosis? A Delphi study. Schizophrenia Bulletom, 36, 136–142.http://dx.doi.org/10.1093/schbul/sbp118
Morrison, A. P., French, P., Stewart, S. L., Birchwood, M., Fowler, D.,Gumley, A. I., . . . Dunn, G. (2012). Early detection andintervention evaluation for people at risk of psychosis: multisiterandomised controlled trial. British Medical Journal, 344, e2233.http://dx.doi.org/10.1136/bmj.e2233
Morrison, A. P., French, P., Walford, L., Lewis, S. W., Kilcommons, A.,Green, J., Parker, S., & Bentall, R. P. (2004). Cognitive therapy forthe prevention of psychosis in people at ultra-high risk: Randomisedcontrolled trial. British Journal of Psychiatry, 185, 291–297.
Morrison, A. P., Gumley, A. I., Ashcroft, K., Manousos, R., White, R.,Gillan, K., Wells, A., & Kingdon, D. (2010). Metacognition andpersecutory delusions: Tests of a metacognitive model in a clinicalpopulation and comparisons with non-patients. British Journal ofClinical Psychology, 50, 223–233. http://dx.doi.org/10.1348/014466510X511141.
Morrison, A. P., Hutton, P., Wardle, M., Spencer, H., Barratt, S.,Brabban, A., . . . Turkington, D. (2011). Cognitive therapy forpeople with a schizophrenia spectrum diagnosis not takingantipsychotic medication: an exploratory trial. Psychological Medicine,1–8. http://dx.doi.org/10.1017/S0033291711001899
Morrison, A. P., Nothard, S., Bowe, S. E., & Wells, A. (2004).Interpretations of Voices in Patients with Hallucinations andNon-Patient Controls: A comparison and predictors of distress inpatients. Behaviour Research and Therapy, 42, 1315–1323.
Morrison, A. P., Renton, J. C., Dunn, H., Williams, S., & Bentall, R. P.(2004). Cognitive therapy for psychosis. East Essex: Brunner-Routledge.
Morrison, A. P., Renton, J. C., French, P., & Bentall, R. P. (2008). Thinkyou're crazy? Think again: A resource book for cognitive therapy for psychosis.London: Routledge.
Morrison, A. P., Renton, J. C., Williams, S., Dunn, H., Knight, A., Kreutz,M., Nothard, S., Patel, U., & Dunn, G. (2004). Delivering cognitivetherapy to people with psychosis in a community mental healthsetting: an effectiveness study. Acta Psychiatrica Scandinavica, 110,36–44. http://dx.doi.org/10.1111/j.1600-0447.2004.00299.x
Nuevo, R., Chatterji, S., Verdes, E., Naidoo, N., Arango, C., &Ayuso-Mateos, J. L. (2012). The continuum of psychoticsymptoms in the general population: A cross-national study.Schizophrenia Bulletin, 38, 475–485. http://dx.doi.org/10.1093/schbul/sbq099
Owen, G. S., Freyenhagen, F., Richardson, G., & Hotopf, M. (2009).Mental capacity and decisional autonomy: An interdisciplinarychallenge. Inquiry: An Interdisciplinary Journal of Philosophy, 52,79–107. http://dx.doi.org/10.1080/00201740802661502
Padesky, C. A. (1993). Socratic questioning: Changing minds or guideddiscovery? Keynote address delivered to European Congress ofBehavioural and Cognitive Therapies, London.
Pechey, R., & Halligan, P. (2011). The prevalence of delusion-like beliefsrelative to sociocultural beliefs in the general population. Psychopa-thology, 44, 106–115. http://dx.doi.org/10.1159/000319788
Pechey, R., & Halligan, P. (in press). Prevalence and correlates ofanomalous experiences in a large non-clinical sample. Psychologyand Psychotherapy: Theory, Research and Practice.
Perivoliotis, D., & Cather, C. (2009). Cognitive behavioral therapyof negative symptoms. Journal of Clinical Psychology, 65, 815–830.http://dx.doi.org/10.1002/jclp. 20614
Perivoliotis, D., Morrison, A. P., Grant, P. M., French, P., & Beck, A. T.(2009). Negative performance beliefs and negative symptomsin individuals at ultra-high risk of psychosis: a preliminarystudy. Psychopathology, 42, 375–379. http://dx.doi.org/10.1159/000236909
Pitt, L., Kilbride, M., Nothard, S., Welford, M., & Morrison, A. P. (2007).Researching recovery from psychosis: A user-led project. PsychiatricBulletin, 31, 55–60.
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
Read, J., Agar, K., Argyle, N., & Aderhold, V. (2003). Sexual andphysical abuse during childhood and adulthood as predictors ofhallucinations, delusions and thought disorder. Psychology andPsychotherapy, 76, 1–22.
Rector, N. A. (2007). Homework use in cognitive therapy for psychosis: A caseformulation approach. Cognitive and Behavioral Practice, 14, 303–316.
Rector, N. A., Beck, A. T., & Stolar, N. (2005). The negative symptomsof schizophrenia: A cognitive perspective. Canadian Journal ofPsychiatry, 50, 247–257.
Romme, M. A., Honig, A., Noorthoorn, E. O., & Escher, A. D. (1992).Coping with hearing voices: an emancipatory approach. BritishJournal of Psychiatry, 161, 99–103.
Ross, K., Freeman, D., Dunn, G., & Garety, P. (2011). A randomizedexperimental investigation of reasoning training for people withdelusions. Schizophrenia Bulletin, 37, 324–333. http://dx.doi.org/10.1093/schbul/sbn165
Sarfati, Y., & Hardy-Bayle, M. C. (1999). How do people withschizophrenia explain the behaviour of others? A study of theoryof mind and its relationship to thought and speech disorganiza-tion in schizophrenia. Psychological Medicine, 29, 613–620.
Shimkunas, A. (1972). Demand for intimate self-disclosure andpathological verbalizations in schizophrenia. Journal of AbnormalPsychology, 80, 197–205.
So, S. H., Freeman, D., Dunn, G., Kapur, S., Kuipers, E., Bebbington, P.,Fowler, D., & Garety, P. A. (2011). Jumping to conclusions, a lackof belief flexibility and delusional conviction in psychosis: Alongitudinal investigation of the structure, frequency, andrelatedness of reasoning biases. Journal of Abnormal Psychology,129–139. http://dx.doi.org/10.1037/a0025297
Stacey, D., Bennett, C. L., Barry, M. J., Col, N. F., Eden, K. B.,Holmes-Rovner, M., . . . Thomson, R. (2011). Decision aids for peoplefacing health treatment or screening decisions. Cochrane Database,CD001431. http://dx.doi.org/10.1002/14651858.CD001431.pub3
Startup, H., Freeman, D., & Garety, P. A. (2008). Jumping toconclusions and persecutory delusions. European Psychiatry, 23,457–459. http://dx.doi.org/10.1016/j.eurpsy.2008.04.005
Strack, K. M., & Schulenberg, S. E. (2009). Understanding empow-erment, meaning, and perceived coercion in individuals withseriousmental illness. Journal of Clinical Psychology, 65, 1137–1148.http://dx.doi.org/10.1002/jclp. 20607
Strauss, J. S. (1969). Hallucinations and delusions as points on continuafunction: Rating scale evidence. Archives of General Psychiatry, 21,581–586.
Stroup, S., Appelbaum, P., Swartz, M., Patel, M., Davis, S., Jeste, D., . . .S Lieberman, J. (2005). Decision-making capacity for researchparticipation among individuals in the CATIE schizophrenia trial.Schizophrenia Research, 80, 1–8. http://dx.doi.org/10.1016/j.schres.2005.08.007
Tai, S., Haddock, G., & Bentall, R. (2004). The effects of emotionalsalience on thought disorder in patients with bipolar affectivedisorder. Psychological Medicine, 34, 803–809.
Tee, J., & Kazantzis, N. (2011). Collaborative empiricism in cognitivetherapy: A definition and theory for the relationship construct.Clinical Psychology: Science and Practice, 18, 47–61. http://dx.doi.org/10.1111/j.1468-2850.2010.01234.x
Toth, S. L., Pickreign Stronach, E., Rogosch, F. A., Caplan, R., &Cicchetti, D. (2011). Illogical thinking and thought disorder inmaltreated children. Journal of the American Academy of Child &Adolescent Psychiatry, 50, 659–668. http://dx.doi.org/10.1016/j.jaac.2011.03.002
Turkington, D., Kingdon, D., Rathod, S., Wilcock, S. K. J., Brabban, A.,Cromarty, P., . . . Weiden, P. J. (2009). Back to life, back to normality:Cognitive therapy, recovery and psychosis. Cambridge, UK: CambridgeUniversity Press.
van Os, J., Hanssen, M., Bijl, R. V., & Ravelli, A. (2000). Strauss (1969)revisited: A psychosis continuum in the normal population?Schizophrenia Research, 45, 11–20.
vanOs, J., Linscott, R. J.,Myin-Germeys, I., Delespaul, P., &Krabbendam, L.(2009). A systematic review and meta-analysis of the psychosis con-tinuum: Evidence for a psychosis proneness-persistence-impairmentmodel of psychotic disorder. Psychological Medicine, 39, 179–195.http://dx.doi.org/10.1017/S0033291708003814
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and

16 Hutton & Morrison
Varese, F., Smeets, F., Drukker, M., Lieverse, R., Lataster, T.,Viechtbauer, W., . . . Bentall, R. P. (2012). Childhood adversitiesincrease the risk of psychosis: A meta-analysis of patient-control,prospective- and cross-sectional cohort studies. SchizophreniaBulletin. http://dx.doi.org/10.1093/schbul/sbs050
Varghese, D., Scott, J., Welham, J., Bor, W., Najman, J., O'Callaghan, M.,Williams, G., & McGrath, J. (2011). Psychotic-like experiences inmajor depression and anxiety disorders: A population-based survey inyoung adults. Schizophrenia Bulletin, 37, 389–393. http://dx.doi.org/10.1093/schbul/sbp083
Vollmann, J., Bauer, A., Danker-Hopfe, H., & Helmchen, H. (2003).Competence of mentally ill patients: A comparative empiricalstudy. Psychological Medicine, 33, 1463–1471.
Wykes, T., Steel, C., Everitt, B., & Tarrier, N. (2008). Cognitive behaviortherapy for schizophrenia: Effect sizes, clinical models, andmethodological rigor. Schizophrenia Bulletin, 34, 523–537.
Please cite this article as: Hutton & Morrison, Collaborative Empiricism iBehavioral Practice (2012), http://dx.doi.org/10.1016/j.cbpra.2012.08.003
Zigmond, T. (2011). Pressures to adhere to treatment: observations on'leverage' in English mental healthcare. British Journal of Psychiatry,199, 90–91. http://dx.doi.org/10.1192/bjp.bp. 111.091876
Disclosure statement. The authors report no conflicts of interest.
Address correspondence to Paul Hutton, Greater ManchesterWest Mental Health NHS Foundation Trust, Psychosis Research Unit,Bury New Road, Prestwich, M25 3BL, United Kingdom; e-mail:[email protected].
Received: January 26, 2012Accepted: August 14, 2012Available online xxxx
n Cognitive Therapy for Psychosis: A Practice Guide, Cognitive and