Embed Size (px)
Citation preview
Cognitive behavioural therapy self-help for depression:An overview
NICOLA RIDGWAY & CHRIS WILLIAMS
Institute of Health and Wellbeing, College of Medical, Veterinary and Life Sciences, University ofGlasgow, UK
AbstractBackground: The World Health Organisation suggests that 60–80% of those affected by depression canbe effectively treated using medication or psychotherapy within primary care. However, less than 50%of those affected actually receive such treatments. In practice, it remains a challenge to provide access topsychotherapy due to limited numbers of therapists combined with a growing number of treatmentguidelines recommending the delivery of evidence-based psychological therapies such as cognitivebehavioural therapy (CBT). One way to overcome this problem is to offer therapy in different ways –with so-called low-intensity (LI) working. One example of LI working is CBT self-help (CBT-SH).Aims: To provide an overview of the current literature surrounding the effectiveness of CBT-SH witha particular focus on depression and discuss the future directions for both research and policyimplementation.Conclusions: It is clear that self-help has a place within a healthcare framework but more work is neededto clarify where and how it should be delivered. The paper concludes that there appears to be enoughbenefits and sufficient evidence to argue for the introduction of LI working as an appropriate first stepfor most people facing depression and anxiety.
Keywords: bibliotherapy, guided CBT, depression, self-help, low intensity working
Background
Depression affects 121million peopleworldwide (WHO). It is the third leading contributor tothe global burden of disease and is expected to be the second leading contributor by 2020(World Health Organisation, 2004). Although the prevalence of depression is high andtrends suggest it will continue to rise, there are a number of treatment options ranging frompharmacotherapy to talking therapies (NICE, 2009). The WHO suggests that 60–80% ofthose affected can be effectively treated using medication or psychotherapy within primarycare. However, in 2004 Kohn et al. (2004) outlined that less than 50% of those affected re-ceived such treatments. This represented a significant treatment gap. With the introductionof the increasing access to psychological therapies (IAPT) programme within some areas oftheUK, it is hoped that this treatment gap will have been reduced. IAPT is still a recent endea-vour, however, so its true impact remains unclear at this stage.More importantly, this has onlybeen introduced in England so it seems fair to suggest that this large treatment gapmay remain
Correspondence: C. Williams, Institute of Health and Wellbeing, Administration Building, Gartnavel Royal Hospital, 1055 GreatWestern Road, Glasgow G12 0XH, UK. Tel: 0141 211-3912. E-mail: [email protected]
Journal of Mental Health, December 2011; 20(6): 593–603© 2011 Informa UK, Ltd.ISSN: 0963-8237 print / ISSN 1360-0567 onlineDOI: 10.3109/09638237.2011.613956
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.

in other regions. This article discusses the implementation of different treatment options thathave been proposed to reduce the treatment gap. The IAPT programme is discussed through-out the article as an example as it often adopts cognitive behavioural therapy (CBT).However,it is important to note, that IAPT also recommends/adopts other treatment options and doesnot just focus on a CBT framework. Issues considered throughout this paper are being dis-cussed and debated by policy-makers across the international arena. However, this paper par-ticularly focuses on changes aimed at adult populations predominantly within aUK setting. Inparticular, the paper assesses different resources of self-help with emphasis on varying types ofCBTself-help (CBT-SH) and their content rather than focusing onmore general forms of self-help such as support forums and internet chat rooms.
TheNational Institute ofHealth andClinical Excellence (NICE) recommends that for indi-viduals living with moderate-, severe- or treatment-resistant depression, CBT should be con-sidered as a treatment of choice (NICE, 2007, 2009). However, in practice, it remains difficultto provide access to CBT due to limited numbers of therapists combined with lengthy waitinglists (Shapiro et al., 2003). Layard (2006) has suggested that thewide access to CBT cannot beimplemented because Britain does not have sufficient therapists. One way to overcome thisproblem is to offer CBT in different ways – with so-called low-intensity (LI) working whereless practitioner time is allocated to treatment. That is, using LI approaches to enhancemental health and wellbeing on a community-wide basis, while using theminimum level of in-tervention necessary to create the maximum gain (Bennett-levy et al., 2010). This contrastswith the more traditional high-intensity (HI) delivery approaches which include longer (upto an hour) and more frequent treatment sessions (e.g. for 12–20 weeks) often led by ahighly trained and qualified specialist practitioner. The crucial difference, however, is that oftime – with less time in LI interventions and longer time in HI interventions. Also, a HIworker can offer bothHI and LI interventions. In contrast, LI workers do not have the compe-tencies to deliver specialist psychotherapeutic models such as CBT.
One example of LI working is CBT-SH. There is currently no agreed definition of self-helpbut Cuijpers et al. (2010) succinctly define it as “a psychological treatment, where the patienttakes home a standardised psychological treatment and works through it more or less indep-endently” (p. 1). Another definition is “the delivery of materials that employ a media-basedformat to treatment suchasbook, computeror video tape.Howeverdelivered, self-helpmaterialsaim to increase the users knowledge about a particular problem, and also to equip themwith skills to better self-manage their difficulties” (Williams, 2003, pp. 172–173). Suchstandardised self-help treatments can be delivered through various modalities such as books,DVDs, audiotapes and online. They can also be delivered independently (unguided orunsupported) or supported/guided by practitioner either with one-to-one support or within agroup/class setting.
Pros and cons of different modalities
The various modalities of delivering CBT-SH each have their own pros and cons but a keypoint is that it depends how people like to work, with everyone being different. Some peoplewill prefer to read written materials, others to use computers and for others to blend theirlearning using more interactive methods of learning (Williams & Morrison, 2010). It isimportant to consider the pros and cons of each method of delivery and match them to indi-vidual patients.
As well as the therapy being delivered using difference modalities, it is also important toconsider the associated support techniques that may go along with it. For example, supportcould be delivered over the telephone, email, internet forums, skype or using an internet
594 N. Ridgway & C. Williams
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.

bulletin board. However, it is important to balance personal preference with practicalitiessuch as internet access, speed of internet, cost of equipment and confidentiality, etc. Per-sonal preference and choice is an important consideration when investigating LI approaches.Preferences for one modality over another or even HI approaches compared with LI ap-proaches may vary across different ages and genders but this choice is individualised andcannot be generalised. For instance, although many may suggest that online resources maybe more suited to the younger population it does not mean that some older adults wouldnot be interested in accessing online resources. An individual approach is therefore neededto match people with their preferred modality. One factor that may influence this is the pre-ferred learning style of the user (Williams & Morrison, 2010).
Learning styles and allocation to LI or HI
A significant literature in the area of teaching and learning has confirmed the importance ofconsidering learning style – how people like to learn. (Please see Romanelli et al. (2009) for areview of learning styles, theories and their application.) If CBT is seen as ultimately aboutadult learning, then helping people consider how they use learning resources (books, com-puters, etc.) is important and an assessment of learning style is as important as an assessmentof depression (Williams & Morrison, 2010). Some will need significant additional prac-titioner time to help them learn and apply CBT principles, whereas for others they may beable to gain these skills using a self-help resource, and the practitioner support neededwould be less. Some patients may need HI work, but many can do well with LI like CBT-SH. The relationship between therapist support time and the intensity of working is detailedin Figure 1.
How do HI and LI models relate together?
Stepped care models provide a logical way of delivering high-capacity services while using ef-fectively the staff skills and competencies available. It aims to focus more highly skilled clin-icians for patients with the greatest needs in terms of chronicity and complexity plus thosewho do not get better with LI alone. In a true stepped care model, the majority of patientswould expect to use LI approaches as a first step.
The argument for this approach is that if two treatments have roughly equivalent out-comes, the lower cost and highest capacity alternative should be offered by default unlessthere is a reason for providing a more complex intervention. However, although in the
Figure 1. Therapist support time: HI versus LI approaches (Reproduced from Williams & Morrison, 2010).
CBT self-help a review 595
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.
wider NHS work force approaches such as CBT-SH are often acknowledged as useful tools,it appears most practitioners do not believe they are as effective as face-to-face interventions(Whitfield & Williams, 2004).
Practitioners here appear to equate LI working such as cCBT with mild to moderatesymptoms rather than for the sorts of more complex patients often seen. This is in spite ofevidence from research, guidelines and service delivery that many patients are complex,and that sometimes focused interventions are what is needed for complex patients. So,helping someone problem solve effectively can help those at high risk of repeated suicide at-tempts (Salkovskis et al., 1990) and improving sleep may be a highly impactful interventionin depression and anxiety (Van Straten & Cuijpers, 2009). Interestingly, practitioner atti-tudes towards the use of CBT-SH improve positively after training (Keeley et al., 2002).
Does CBT-SH work?
Over recent years, there has been a significant expansion in the amount of research investi-gating the effectiveness of LI interventions such as self-help (Anderson et al., 2005; Bennett-Levy et al., 2010; McKendree-Smith et al., 2003; Proudfoot et al., 2004; Richards et al.,2003). Over 30 systematic reviews and meta-analyses also contribute to provide ample evi-dence that CBT-SH is effective for depression and anxiety (for a recent example, seeAndrews et al., 2010). A meta-analyses and meta-regression by Gellatly et al. (2007) goesone step further to investigate the factors that determine effectiveness of CBT-SH. Theyidentified 34 published studies covering 39 relevant comparisons in the treatment ofdepression and found that there was evidence for CBT-SH, but not for psycho-educationalmaterials. Overall, the effect of self-help interventions was found to be 0.43, which can beconsidered a medium effect (Gellatly et al., 2007). However, when the analysis was restrictedto only include guided self-help studies (self-help with some minimal therapist contact) theeffect increased and was concluded to be large (0.8). Gellatly identified that studies recruit-ing participants from non-clinical settings, patients with existing problems (rather than atrisk) and CBT techniques were all associated with greater effectiveness. Although thereare clear differences between the methods of delivery of self-help and the learning stylesassociated with them, overall Gellatly et al. (2007) found there were no significant differencesin the effects of written self-help (bibliotherapy) and online self-help. Studies have not to dateseparated out the relative impacts of support, individualisation of therapy and the effect of theCBT-SH resources themselves, and it has been assumed that the support aids application ofthe resources in the person’s life. Vernmark et al. (2010) have explored the concept of indi-vidualisation of therapy by comparing CBT-SH with minimal therapist input with individua-lised email therapy based on CBT principles. Both treatment interventions significantlyimproved outcome with no significant differences found between the two treatments. Vern-mark et al.’s (2010) findings suggest that in fact the individualisation of therapy may have lessof an impact than anticipated. However, it is important to interpret these findings cautiouslyas Vernmark et al. (2010) outline that their study was underpowered to detect differencesbetween the two treatment groups. The complex relationship between CBT, support andindividualisation of therapy needs to be tested in more elegant placebo controlled trialsthat control for the impact of support and individualisation.
Recent evaluations have reported “real-life” roll-outs of LI services – including those usingCBT-SH. Clark et al. (2009) outlined the outcome data from two IAPT demonstration sites(Doncaster and Newham) that received additional funds to rapidly roll-out access to CBT-related interventions. The paper outlined outcome data from roughly the first year of oper-ation at each of the two sites. Clark et al. (2009) summarised that clinical services in each
596 N. Ridgway & C. Williams
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.

site are guided by the NICE guidelines but each site had a slightly different emphasis.Doncaster had a high throughput and although HI interventions were available, greateremphasis was placed on LI work (behavioural activation for low moods and CBT-SH foranxiety). In contrast, Newham placed greater emphasis on HI working (CBT delivered byexpert practitioners). Comparison of these two sites allows a real-life examination of twodifferent ways of structuring services. Clark et al.’s (2009) findings highlighted that bothLI and HI approaches are effective. However, there were enormous differences in throughputand capacity with 3102 people completing the intervention in Doncaster (predominantly LI)compared with 369 completing in Newham (predominantly HI). It is important to note thatDoncaster IAPT were already established and running prior to the data collection periodwhereas Newham IAPT began form a “standing start” so processes were slower to get upand running. Despite this, it is clear that the throughput for LI processes was far larger. Itis worth noticing that a typical IAPT team of say 25 staff members offers treatment toaround 10,000 people a year. This is enormously different in terms of scale to that achievedby more traditionally delivered mental health services. A typical LI worker would have acurrent caseload of 60.
Comparisons between LI and HI approaches were directly done in a recent systematicreview and meta-analyses by Cuijpers et al. (2010). They conducted a meta-analysis of ran-domised controlled trials investigating guided self-help and compared effects directly withthose using face-to-face psychotherapies. Twenty-one studies were included covering 810participants (429 in face-to-face therapy studies and 381 in guided self-help studies). It isimportant to note that despite covering such a large number of participants, the qualityof the studies were not optimal with many providing insufficient information on method-ologies adopted. Notwithstanding this, the quality of the treatment interventions thatwere delivered was good in most studies (e.g. manualised treatments and specificallytrained therapists, etc.). Collectively, the results supported the findings of Clark et al.(2009) and indicated no significant differences between the effects of guided self-helpand face-to-face therapies. This finding is particularly pertinent as the meta-analysis waspowered to detect even small differences in effect. The Cuijpers et al. (2010) paper there-fore suggests that HI and LI therapies lead to equal mental health improvements. As withany meta-analyses, it is important to note that populations across studies will not alwayshave comparable patient groups so results should be considered cautiously. For example,of the 21 studies that Cuijpers et al. (2010) included, six were aimed at people withdepression, seven with panic, three with social phobia, two with specific phobias andthree with phobias in general. Cuijpers et al. (2010) compared depression and anxiety out-comes and used an established methodology to report their results. Overall, they concludedthat “guided self-help and face-to-face treatments for depression and anxiety have compar-able effects, and that there is no evidence that one or the other is significantly larger than theother” (p. 1953).
Overall, the question of whether LI or HI outcomes are equal is flawed by the lack ofpatient numbers (i.e. the comparisons are underpowered). To scientifically “prove” equival-ence a very large study would be needed at high cost and such studies are rarely done for anytreatment in the health service. What is usually carried out instead are “superiority” studies,which compare two or more treatments and examine whether one is better than the other orinstead whether a “no likely difference” conclusion should be reached. The evidence fromthe Cuijpers et al. paper is that for over 800 people included in the combined studies,there is not even a trend for HI (i.e. longer practitioner sessions, often by an expert) to besuperior to LI working for the treatment of anxiety and depression.
CBT self-help a review 597
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.
A possible criticism of papers investigating the effectiveness of self-help is that becausemany of the papers recruit participants using advertisements, the participants involved inthe study are therefore unrepresentative of those seen within the health service. An alternativeexplanation is that the participants, however recruited, were actually depressed or anxious andthat both LI and HI approaches helped them. Studies like those outlined previously show thatpeople who respond to adverts can do very well with these approaches. The fact that recruit-ment is by advert for some of the studies is a positive strength as it shows these approachescan be used both within and outside the formal health service – by recruiting people nototherwise receiving help. Martinez et al. (PhD in preparation) compared participantsrecruited using a free access CBT-SH website and recruited through the voluntary sector(Depression Alliance Scotland and Anxiety, UK) with participants referred for CBT-SHby general practitioners. The results indicated that those using the resources were remarkablysimilar in terms of severity and demographics, regardless of recruitment strategy. Thissimilarity has also been demonstrated in other mental health populations (e.g. bulimia;Pretorius et al., 2009).
Cuijpers et al.’s study is important when considering the so-called treatment gap (i.e. theproportion of people who have depression or anxiety and need treatment but do not receiveit). The treatment gap suggests that less than 50% of those needing treatment for depressionor anxiety actually receive it from the health service. This is why many now argue that weshould encourage self-referral to mental health services, and this approach is being widelyoffered in the IAPT services in England (www.iapt.nhs.uk).
Side-effects and criticisms of CBT-SH
Research summarised so far has outlined evidence for the effectiveness of CBT-SH in thetreatment of depression. Work has not thus far identified whether some patients do betterwith one-to-one specialist CBT, or LI CBT-SH – and if so how to predict these. It is notcurrently possible to answer the question whether response is related to severity, chronicityor co-morbidity. It is also unclear whether it relates to patient choice and preference, satisfac-tion and endorsement. Self-help overall may be just as effective as face-to-face therapy but is itas acceptable? Waller and Gilbody (2009) conducted a systematic review of quantitative andqualitative evidence investigating the barriers to computerised CBT. Results indicated that79% of participants who entered a trial completed it, suggesting a 21% dropout rate.Dropout was concluded to be twice as likely for those using computerised CBT comparedwith control interventions (many control interventions were HI approaches) but thispattern was not seen across all studies and was not significant. Dropout rates in self-helpstudies vary greatly with Kaltenthaler et al. (2008) concluding that they vary from 0% to75% with a mean dropout rate of 31.75%. Although, this may appear high, Kaltenthaleret al. suggest that it is comparable to dropout rates for other psychological therapies. In con-trast, Cuijpers et al. (2010) found that dropout rates for self-help were “somewhat” higher thanfor face-to-face therapy, but it is important to note that this was not statistically significant.
Although great variation appears to exist in current research about dropout rates for thoseusing self-help, it seems unjustified to suggest that dropout rates are an inevitable conse-quence of self-help. It is clear that some patients adhere well to such interventions andfind them highly acceptable. As with comparing LI and HI approaches in general or evendifferent types of LI approaches, it is likely that different approaches may suit differentpeople and how they like to work and learn.
Further criticisms levelled at self-help interventions are privacy and security concerns asnoted by Whitfield and Williams (2004) as well as social and peer pressures such as cyber
598 N. Ridgway & C. Williams
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.
bullying, particularly for online self-help approaches. Macleod et al. (2009) also foundevidence of a lack of detection of a worsening of the patient’s clinical state due to reducedtherapist contact when investigating CBT-SH. However, patients themselves seem lessworried about such issues as Waller and Gilbody (2009) concluded that participants ratedinterventions as high on clarity, content, usefulness and satisfaction.
Who is CBT self-help suitable for?
A survey of accredited CBT practitioners found that in general they endorsed LI interventionssuch as cCBTas being less effective than seeing a practitioner (Keeley et al., 2002). In Scotland,a practical guide to evidence-basedpractice (NHSEducationScotland, 2011) also reaffirms thispremise as it suggests that expert-ledHI approaches should be left for all thosewithmore severeproblems. However, this is out of accord with NICE (2009) guidelines. NICE (2009) suggestthat CBT-SHmay be adopted in the treatment of mild as well as moderately severe depression.
The initial findings comparing two IAPT sites in the Clark et al. (2009) study illustratedthat LI approaches may indeed be used for similar populations of similar severity as HI ap-proaches. More pertinently, when describing the population at each site and the initial sever-ity of the patient populations, 82% of those participating in Doncaster (LI) scored 10 orhigher on the PHQ-9 (the clinical cut-off for depression) with 34% scoring 20 or higher(therefore considered severe). Similarly, the population described at the Newham site (HI)had 76% scoring 10 or higher on the PHQ-9 and 28% scoring 20 or more. As outlined pre-viously, Clark et al. (2009) found that both approaches were effective. The similarity in theseverity of patient scores at these two sites demonstrates how LI approaches can be adoptedto treat higher and lower severity levels. Although, both treatment options may be effective intreating a broad range of severity, it is important to also consider complexity. Therefore,although both LI and HI options have been shown to be helpful for severe problems, itseems likely that at times HI approaches may be more suitable due to the need for abespoke and individualised approach, or to tease out suitable interventions based on a com-plicated clinical formulation. However, it is not known how to clearly identify such patients,and this stance does not seem to justify a conclusion that CBT-SH is appropriate for mildsymptoms alone. NICE (2009) suggest that four important factors should be taken intoconsideration to determine complexity and the appropriate step in the stepped care model.Care providers should evaluate whether there is evidence of risk, co-morbid mental healthproblems, complex social problems and past treatment history.
Optimising delivery of CBT-SH
Self-help interventions can be delivered in isolation or with support (guided). Support isoften provided by a trained therapist or mental health worker and is normally of a supportivenature designed to facilitate progression through the self-help programme. Gellatly et al.(2007) found that interventions that were offered with support reported a significantlyhigher effect size than those delivered with no support. Support can be offered in a varietyof ways from face to face, over the telephone or via email. Kenwright et al. (2005) illustratedthe effectiveness of telephone support and its importance alongside self-help therapy. In thisstudy, patients with obsessive compulsive disorder were randomised to receive either ninescheduled clinician initiated calls or to only receive calls when requested by the patient. Onaverage, patients in the scheduled support group received 76 min of support comparedwith 16 min for those in the requested support group. Results demonstrated that patientsin the scheduled support group dropped out less frequently and showed more improvements
CBT self-help a review 599
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.
in symptoms and disability. Although the use of support has been shown to be effective, moreresearch is still needed to investigate the optimal delivery of support. For example, optimaltime input for support and mode of support (telephone versus email versus face to face).
Incorporating CBT-SH into practice
In many existing clinical services, it is not currently clear where CBT-SH or other LI inter-ventions should fit in the health delivery algorithms. There appears to be more than sufficientevidence to justify widespread service redesign (Clark et al., 2009; Cuijpers et al., 2010; Gel-latly et al., 2007; NICE, 2009). Options for implementation include the setting up of new LIservices such as IAPT, or working with the existing workforce to train and introduce this wayof working (e.g. the SPIRIT Programme; Williams et al., 2011). However implemented,practitioner belief will be important and guide delivery.
The positioning of an intervention also affects take-up and use. So, services that place self-help as the “first step of treatment” (Bara-Carril et al., 2004) tend to have far higher take-up(78%) than situations where self-help is offered simply as an option if patients wish to take itup while waiting to see a practitioner (26%, Whitfield et al., 2006).
It is also important to consider how stepped care is implemented. Some current servicesroutinely choose to send most patients to an LI intervention. In contrast, others allocate veryfew, depending on the criteria/cut-offs in the service algorithms. The concept of matched careis widely used in services to decide who receives LI or HI treatments but there is no estab-lished widely agreed definitions to allow consistent matching of who needs HI and LI inter-ventions as the first step. This is because in matched care, who is allocated to each step isoften down to individual practitioner judgement. It is subjective and too easily informednot by patient needs, but by the expectations and preferences of the assessing practitioner.Although it sounds very justifiable and patient focused – the danger is it is biased by twofactors. One is that the assessment is often currently completed by mental health specialists– who often believe that HI working is “better” (Whitfield & Williams, 2004). The second ispatient expectation. Although in community settings self-help approaches are endorsedhighly by people (Jorm et al., 1997), there is still a lack of knowledge about what someaspects of LI working are like. As there are no differences in effectiveness between mainforms of CBT-SH, the choice of approach will be best decided by patient expectationsand choice (Gellatly et al., 2007). Are people sufficiently informed to make such choices?For example, Mitchell and Gordon (2007) found that the credibility of computerisedCBT was initially very poor among their sample of students. However, the proportion ofpeople expressing a preference for computerised CBT increased from below 10% to 30%after a simple intervention where content of the package was played. This has implicationsfor wider implementation as patients, referrers and staff may need some degree of familiar-isation with LI ways of working. Providing “taster” examples of different approaches, e.g.short excerpts of different materials, screenshots, handouts or short DVDs may be used.
For self-help to be successfully integrated into service implementation we need prac-titioners to be happy to move to self-referral and from current research, we know this willtake time (Keeley et al., 2002). An alternative to introducing LI models would be insteadto put more and more training resources and staff into HI services. Factors that causepressure for this to occur are often waiting lists for specialist services. However, it is doubtfulthat HI services will ever meet the needs of the wider population and the danger is that HIservices narrow their service remits to focus on only the more complex and long-termcases. Therefore, if LI approaches were not introduced then less complex cases wouldbecome neglected as HI approaches would not be able to accommodate them.
600 N. Ridgway & C. Williams
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.
Currently less than half of all people with depression/anxiety receive any level of healthservice input. Of those that do, most are in primary care. A combined LI (majority) andHI (minority) service makes sense pragmatically, but also from the perspective of the individ-ual person with depression. IAPT data outcomes have shown that such an approach can beeffective (Clark et al., 2009). Instead of facing waiting lists, they can receive rapid access in atimely manner and with flexible support that fits their lives (i.e. phone based as well as face toface). The danger is that attempts to solve access problems using HI models alone will fail,and lead to a restricted focus on wider access to care.
Conclusion
From the evidence presented in this paper, it is clear that CBT-SH has a place within ahealthcare framework but more work is needed to clarify for whom, how to recruit andalso how to introduce and support the approach. Importantly, we need to learn moreabout which modality of delivery (e.g. books, DVDs, online, etc.) suits which people.Clearly, patients work and learn in different ways and self-help therapies need to accommo-date this. A large-scale RCT comparing LI resources, delivered using different modalitieswould help us to learn “who” suits the different delivery methods (Table 1). A study likethis would allow us to explain characteristics of responders to different modalities. More
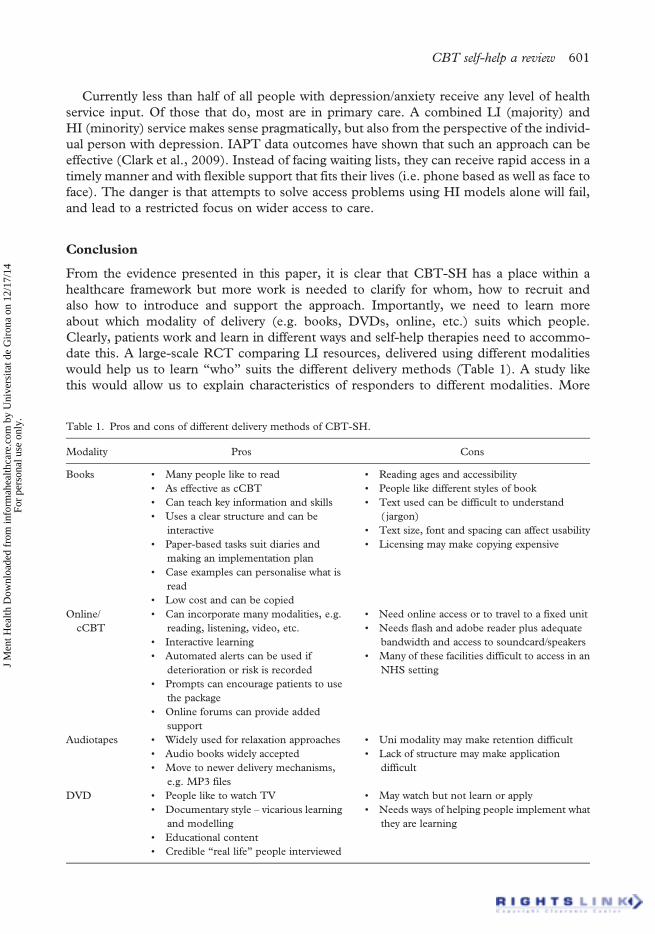
Table 1. Pros and cons of different delivery methods of CBT-SH.
Modality Pros Cons
Books • Many people like to read• As effective as cCBT• Can teach key information and skills• Uses a clear structure and can be
interactive• Paper-based tasks suit diaries and
making an implementation plan• Case examples can personalise what is
read• Low cost and can be copied
• Reading ages and accessibility• People like different styles of book• Text used can be difficult to understand
( jargon)• Text size, font and spacing can affect usability• Licensing may make copying expensive
Online/cCBT
• Can incorporate many modalities, e.g.reading, listening, video, etc.
• Interactive learning• Automated alerts can be used if
deterioration or risk is recorded• Prompts can encourage patients to use
the package• Online forums can provide added
support
• Need online access or to travel to a fixed unit• Needs flash and adobe reader plus adequate
bandwidth and access to soundcard/speakers• Many of these facilities difficult to access in an
NHS setting
Audiotapes • Widely used for relaxation approaches• Audio books widely accepted• Move to newer delivery mechanisms,
e.g. MP3 files
• Uni modality may make retention difficult• Lack of structure may make application
difficult
DVD • People like to watch TV• Documentary style – vicarious learning
and modelling• Educational content• Credible “real life” people interviewed
• May watch but not learn or apply• Needs ways of helping people implement what
they are learning
CBT self-help a review 601
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.

specifically, studies comparing book-based and computerised CBT and LI with HI interven-tions for patient groups with differing clinical complexity are required. Time needs to bedirected into implementing LI working into the current health framework so it is notviewed as a “second-class” option after HI approaches. However, considering the currentstate of research, there appears to be enough benefits and sufficient evidence to argue forthe introduction of LI working as an appropriate first step for most people facing depressionand anxiety and to do this widely across the health service.
Declaration of Interest: A range of CBT-SH materials have been written by ProfessorChris Williams.
References
Anderson, L., Lewis, G., Araya, R., Elgie, R., Harrison, G., Proudfoot, J., et al. (2005). Self-help books fordepression: How can practitioners and patients make the right choice? British Journal of General Practice, 55,387–392.
Andrews, G., Cuijpers, P., Craske, M.G., McEvoy, P., & Titov, N. (2010). Computer therapy for the anxiety anddepressive disorders is effective, acceptable and practical health care: A meta-analysis. PloS One, 5 (10), e13196.doi:10.1371/journal.pone.0013196
Bara-Carril, N., Williams, C.J., Pombo-Carril, M.G., Reid, Y., Murray, K., Aubin, S., et al. (2004). A preliminaryinvestigation into the feasibility and efficacy of a CD-ROM based cognitive-behavioural self-help intervention forbulimia nervosa. International Journal of Eating Disorders, 35, 538–548.
Bennett-Levy, J., Richards, D., Farrand, P., Christensen, H., Griffiths, K., Kavanagh, D., et al. (2010).Oxford guideto low intensity CBT interventions. Oxford: Oxford University Press.
Clark, D.M., Layard, R. Smithies, R., Richards, D.A., Suckling, R., & Wright, B. (2009). Improving access topsychological therapy: Initial evaluation of two UK demonstration sites. Behavioural Research and Therapy, 47,910–920.
Cuijpers, P., Donken, T., Van Straten, A., Li, J., & Andersson, G. (2010). Is guided self-help as effective as face-to-face psychotherapy for depression and anxiety disorders? A systematic review and meta-analysis of comparativeoutcome studies. Psychological Medicine, 40(12), 1943–1957.
Gellatly, J., Bower, P., Hennessy, S., Richards, D., Gilbody, S., & Lovell, K. (2007). What makes self-help interven-tions effective in the management of depressive symptoms? Meta-analysis and meta-regression. PsychologicalMedicine, 37, 1217–1228.
Jorm, A.F., Korten, A.E., Jacomb, P.A., Christensen, H., Rodgers, B., & Pollitt, P. (1997). Helpfulness of interven-tions for mental disorders: Beliefs of health professionals compared with the general public. British Journal of Psy-chiatry, 171, 233–237.
Kaltenthaler, E., Sutcliffe, P., Parry, G., Beverley, C., Rees, A., & Ferriter, M. (2008). The acceptability to patientsof computerized cognitive behaviour therapy for depression: A systematic review. Psychological Medicine, 38,1521–1530.
Keeley, H., Williams, C.J., & Shapiro, D. (2002). A United Kingdom survey of accredited cognitive behaviour thera-pists’ attitudes towards and use of structured self-help materials. Behavioural and Cognitive Psychotherapy, 30,191–201.
Kenwright, M., Marks, I., Graham, C., Franses, A., &Mataix-Cols, D. (2005). Brief scheduled phone support froma clinician to enhance computer-aided self-help for obsessive-compulsive disorder: Randomized controlled trial.Journal of Clinical Psychology, 61(12), 1499–1508.
Kohn, R., Saxena, S., Levov, I., & Saraceno, B. (2004). The treatment gap in mental health care. Bulletin of the WorldHealth Organisation, 82(11), 811–890.
Layard, R. (2006). The Depression Report. A new deal for depression and anxiety disorders. London School of Economics,The Centre for Economic Performance’s Mental Health Group.
MacLeod, M., Martinez, R., Williams, & C. (2009). Cognitive behaviour therapy self-help: Who does it help andwhat are its drawbacks? Behaviour and Cognitive Psychotherapy, 37, 61–72.
McKendree-Smith, N., Floyd, M., & Scogin, F. (2003). Self administered treatments for depression: A review.Journal of Clinical Psychology, 59, 275–288.
Mitchell, N., & Gordon, P.K. (2007). Attitudes towards computerized CBT for depression amongst a student popu-lation. Behavioural and Cognitive Psychotherapy, 35, 421–430.
602 N. Ridgway & C. Williams
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.

NHS Education Scotland. (2011). Matrix: A guide to delivering evidence-based psychological therapies in Scotland.Retrieved September 20, 2011, from http://www.nes.scot.nhs.uk/media/425354/psychology_matrix_2011s.pdf.
NICE. (2007). Depression: Management of depression in primary and secondary care, Clinical Guideline 23. London:National Institute for Clinical Excellence.
NICE. (2009). Depression: The treatment and management of depression in adults. London: National Institute forClinical Excellence.
Pretorius, N., Arcelus, J., Beecham, J., Dawson, H., Doherty, F., Eisler, I., et al. (2009). Cognitive behaviouraltherapy for adolescents with bulimic symptomatology: The acceptability and effectiveness of internet-based de-livery. Behaviour Research and Therapy, 47, 729–736.
Proudfoot, J., Ryden, C., Everitt, B., Shapiro, D., Goldberg, D., Mann, A., et al. (2004). Clinical efficacy of com-puterised cognitive-behavioural therapy for anxiety and depression in primary care: Randomised controlled trial.British Journal of Psychiatry, 185, 46–54.
Richards, A., Barkham, M., Cahill, J., Richards, D., Williams, C., & Heywood, P. (2003). PHASE: A randomisedcontrolled trial of supervised self-help cognitive behavioural therapy in primary care. British Journal of GeneralPractice, 53, 764–770.
Romanelli, F., Bird, E., & Ryan, M. (2009). Learning styles: A review of theory, application, and best practices.American Journal of Pharmaceutical Education, 73(1), 1–5.
Salkovskis, P.M., Atha, C., & Storer, D. (1990). Cognitive behavioural problem solving in the treatment of patientswho repeatedly attempt suicide. A controlled trial. The British Journal of Psychiatry, 157, 871–876.
Shapiro, D., Cavangh, K., & Lomas, H. (2003). Geographic inequity in the availability of cognitive behaviouraltherapy in England and Wales. Behavioural and Cognitive Psychotherapy, 31, 185–192.
Van Straten, A., & Cuijpers, P. (2009). Self-help therapy for Insomnia: A meta-analysis. Sleep Medicine Reviews,13(1), 61–71.
Vernmark, K., Lenndin, J., Bjährehed, J., Carlsson, M., Karlsson, J., Öberg, J., et al. (2010). Internet administeredguided self-help versus individualized E-Mail therapy: A randomized trial of two version of CBT for majordepression. Behaviour Research and Therapy, 48, 368–376
Waller, R., & Gilbody, S. (2009). Barriers to uptake of computerized cognitive behavioural therapy: A systematicreview if the quantitative and qualitative evidence. Psychological Medicine, 39, 705–712.
Whitfield, G., &Williams, C. (2004). If the evidence is so good –Why doesn’t anyone use them? A national survey ofthe use of computerised cognitive behavioural therapy. Behavioural and Cognitive Psychotherapy, 32, 57–65.
Whitfield, G., Hinshelwood, R., Pashley, A., Campsie, L., & Williams, C. (2006). The impact of a novel compu-terised CBT CD Rom (overcoming depression) offered to patients referred to clinical psychology. Behaviouraland Cognitive Psychotherapy, 34, 1–11.
Williams, C. (2003). New technologies in self-help: Another effective way to get better? European Eating DisordersReview, 11, 170–182.
Williams, C., & Morrison, J. (2010). A new language for CBT: New ways of working require new thinking as well as newwords. In J. Bennett-Levy, D. Richards, P. Farrand, H. Christensen, K. Griffiths, D. Kavanagh, B. Klein, M.A.Lau, J. Proudfoot, L. Ritterband, J. White, & C. Williams (Eds.) Oxford guide to low intensity CBT interventions.(pp. 69–83) Oxford: Oxford University Press.
Williams, C., Martinez, R., Dafters, R., Ronald, L., & Garland, A. (2011). Training the wider workforce in cognitivebehavioural self-help: The SPIRIT (Structured Psychosocial InteRventions in Teams) training course. Behav-ioural and Cognitive Psychotherapy, 39, 139–149.
World Health Organisation. (2004). Depression: What is depression? Retrieved September 20, 2011, from http://www.who.int/mental_health/management/depression/definition/en/.
CBT self-help a review 603
J M
ent H
ealth
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
12/
17/1
4Fo
r pe
rson
al u
se o
nly.





























