Embed Size (px)
Citation preview

Cognitive Behavioral Therapy for Insomnia
April 14, 2012UC San Diego Moores Cancer CenterLa Jolla, California

Cognitive Behavioral Therapy for Insomnia
April 14, 2012UC San Diego Moores Cancer Center
La Jolla, California

Cognitive Behavioral Therapy for Insomnia April 14, 2012
Course Description This one-day course will teach practitioners how to get started with CBT-I, the components of CBT-I including sleep education, stimulus control, sleep restriction, sleep hygiene education, relaxation training and cognitive therapy, and helping patients sleep well over the long-term. In addition, normal sleep, consequences of insomnia, differential diagnoses with other sleep disorders, clinical evaluation of insomnia and pharmacological treatments will be covered. The goal of the conference is to provide up-to-date, clinically relevant information to assist you in delivering quality care for the patient with insomnia.
Course Objectives
At the conclusion of this course, the participants should be able to: • Describe the rationale and empirical support for treating insomnia with CBT-I. • Identify appropriate patients for CBT-I. • Appropriately apply concepts of CBT-I and pharmacological treatments with insomnia patients • Interpret and describe the latest research findings on cognitive deficits and neuroimaging
associated with different child neurological and psychiatric disorders • Assess long-term outcomes in children with perinatal brain insults • Examine the latest developments in computerized assessment instruments for children • Determine common cognitive profiles and behavioral changes in children who have suffered
traumatic brain injuries • Describe the latest research on different remediation and medication interventions for children
with neurocognitive disorders
Target Audience
This conference is specifically designed to provide in-depth knowledge for the psychologists, psychiatrists, primary care physicians, nurse clinician’s, social workers and other health professionals who encounter patients with insomnia in their clinical practice.
Needs Assessment Based on a review of recently published literature and faculty input, the planning committee has identified ongoing educational needs for psychologists, physicians and other related healthcare professionals involved in the evaluation and management of insomnia.
• Educational gaps o Few providers are trained in evidence-based treatment of insomnia o Few training opportunities in evidence-based treatment of insomnia are available. o Treatment options for patients are limited due to the lack of sufficient numbers of trained
professionals • Specific gaps in knowledge for providers include
o The latest advances in the diagnosis of insomnia o Understanding the co-morbidities associated with insomnia o Understanding the consequences of chronic insomnia o The latest advances in the behavioral and pharmacological treatments of insomnia
The faculty will fill these gaps by providing clear description of the assessment and treatment of insomnia across a broad spectrum of patient populations.

Accreditation Statement The University of California, San Diego School of Medicine is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
AMA: The University of California, San Diego School of Medicine designates this live activity for a maximum of 7.0 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
APA: (Full attendance is required) The University of California, San Diego School of Medicine, Department of Psychiatry is approved by the American Psychological Association to sponsor continuing education for psychologists. The University of California, San Diego School of Medicine, Department of Psychiatry maintains responsibility for this program and its content.
BBS: Course meets the qualifications for 7.0 hours of continuing education credit for MFTs and/or LCSWs as required by the California Board of Behavioral Sciences. (UCSD Provider Number PCE 683).
Evaluations and Certificates
To claim credit and evaluate this course: Please visit http://cme.ucsd.edu/evaluation to complete the evaluation for this course online. Use the access code INSOM2012 when prompted. Once you complete and submit your evaluation, your certificate will be available immediately for download. The last day to claim credit online is April 29, 2012. UC San Diego Continuing Medical Education P: 888-229-6263 E: [email protected]
Cultural Competency
California Assembly Bill 1195 requires continuing medical education activities with patient care components to include curriculum in the subjects of cultural and linguistic competency. It is the intent of the bill, which went into effect on July 1, 2006, to encourage physicians and surgeons, CME providers in the state of California, and the Accreditation Council for Continuing Medical Education to meet the cultural and linguistic concerns of a diverse patient population through appropriate professional development. The planners, speakers and authors of this CME activity have been encouraged to address issues relevant in their topic area. In addition, a variety of resources are available that address cultural and linguistic competency, some of which are included in your syllabus or handout materials. Additional resources and information about AB1195 can be found on our website at http://cme.ucsd.edu.

Acknowledgments
We would like to thank the following company for their generous educational grant.
Ferring Pharmaceuticals
Philips Resperonics

Disclosure Summary
Cognitive Behavioral Therapy for Insomnia
April 14, 2012
It is the policy of the University of California, San Diego School of Medicine to ensure balance, independence, objectivity and scientific rigor. All persons involved in the selection, development and presentation of content are required to disclose any real or apparent conflicts of interest. All conflicts of interest will be resolved prior to an educational activity being delivered to learners through one of the following mechanisms 1) altering the financial relationship with the commercial interest, 2) altering the individual’s control over CME content about the products or services of the commercial interest, and/or 3) validating the activity content through independent peer review. All persons are also required to disclose any discussions of off label/unapproved uses of drugs or devices. Persons who refuse or fail to disclose are disqualified from participating in the CME activity. Participants will be asked to evaluate whether the speaker’s outside interests reflect a possible bias in the planning or presentation of the activity. This information is used to plan future activities.
Speaker Name Name of Commercial Interest Nature of Relevant Relationship
Employee, Grants/Research Support recipient, Board Member, Advisor or Review Panel member, Consultant, Independent Contractor, Stock Shareholder (excluding
mutual funds), Speakers’ Bureau, Honorarium recipient, Royalty recipient, Holder of Intellectual Property Rights,
or Other Sonia Ancoli-Isreal Ferring Pharmaceuticals Inc.,
GlaxoSmithKline, Hypnocore, Johnson & Johnson, Merck, NeuroVigil, Inc., Pfizer, Phillips, Purdue Pharma LP, Sanofi-Aventis
Consultant
The following have no relevant financial relationships to disclose: Jennifer Martin The CME staff, meeting planners, planning committee and CME committee reviewers do not have any relevant financial relationships to disclose. This educational activity may contain discussion of unlabeled and/or investigational uses of agents that are not approved by the FDA. Please consult the prescribing information for each product. The views and opinions expressed in this activity are those of the faculty and do not necessarily reflect the views of the University of California, San Diego.

Cognitive Behavioral Therapy for Insomnia April 14, 2012
7:30-8:00 am Registration and Breakfast 8:00-8:05 Welcome and Introduction Sonia Ancoli-Israel, PhD, CBSM & Jennifer Martin, PhD, CBSM 8:05-8:20 What is Normal Sleep Anyway? Jennifer Martin, PhD, CBSM 8:20-9:00 Definition, Consequences, Co-morbidities of Insomnia Jennifer Martin, PhD, CBSM 9:00-9:30 OSA, RLS and CRSD Presenting as Insomnia Sonia Ancoli-Israel, PhD, CBSM 9:30-10:15 Clinical Evaluation of Insomnia Sonia Ancoli-Israel, PhD, CBSM 10:15-10:45 Break 10:45-11:15 Pharmacological Treatments Sonia Ancoli-Israel, PhD, CBSM 11:15-11:30 Q & A 11:30-12:25 pm Getting Started With CBT-I: Session 1 Jennifer Martin, PhD, CBSM 12:25-1:25 Lunch Components of CBT-I 1:25-2:15 Stimulus Control Sleep Restriction Sonia Ancoli-Israel, PhD, CBSM 2:15-3:00 Sleep Hygiene Relaxation Jennifer Martin, PhD, CBSM 3:00-3:30 Break 3:30-3:45 Q & A 3:45-4:15 Cognitive Therapy Long-term Sleep Habits Jennifer Martin, PhD, CBSM 4:15-4:45 Case Discussions Sonia Ancoli-Israel, PhD, CBSM & Jennifer Martin, PhD, CBSM 4:45-5:00 Q & A 5:00 Adjourn
4/10/2012
1
Cognitive Behavioral Therapy for Insomnia Conference
Sonia Ancoli-Israel, PhD
April 14, 2012
University of California, San DiegoJennifer L. Martin, PhD
University of California, San Diego
Disclosures
Sonia Ancoli-Israel Consultant: Astra Zeneca, Ferring Pharmaceuticals Inc., GlaxoSmithKline, Hypnocore, Johnson & Johnson, Merck, NeuroVigil, Inc., Pfizer, Philips, Purdue PharmaLP, sanofi-aventis, Astra Zenica
Jennifer MartinNo disclosures

4/10/2012
2
Today’s schedule8:05-8:20 What is normal sleep?8:20-9:00 Insomnia definition, consequences & comorbidities9:00-9:30 OSA, RLS and CRSD presenting as insomnia9 30 10 15 Cli i l E l ti f I i9:30-10:15 Clinical Evaluation of Insomnia10:15-10:45 BREAK10:45-11:15 Pharmacological treatments11:15-11:25 Question/Answer11:25-12:15 Getting started with CBT-I12:15-1:15 LUNCH1:15-2:45 Components of CBT-I1:15-2:45 Components of CBT-I2:45-3:15 BREAK3:15-3:30 Question/Answer3:30-4:00 Components of CBT-I, continued4:00-4:30 Case discussions4:30-4:45 Evaluations
Housekeeping itemsPlease silence cell phones and pagersand pagersRestroomsBreaks/lunchEvaluations – please share your comments with us!

What is normal sleep?
Jennifer L. Martin, PhD CBSMAdjunct Assistant Professor
David Geffen School of MedicineUniversity of California, Los Angeles
Career Research Scientist and PsychologistVA Greater Los Angeles Health Care System
Certified, Behavioral Sleep Medicine
Neurophysiology of SleepThe cyclic alternations of waking and sleep are controlled by neuronal mechanisms interconnecting throughout the brain from the medulla to the cerebral cortex.Sleep is subdivided into two states: non-REM and REM sleep. Each have distinct anatomical, behavioral and electrophysiological features.
Adapted from Sleep Multimedia, 1998
Stage N1
Stage N2
Stage N3
Non-REM EEG

REM EEG
Summary of Sleep Stage
Brain Activity During Wake and Sleep
Awake NonREM REM
Adapted from Sleep Multimedia, 1998
Red = high metabolic activityPurple = low metabolic activity

Characteristics of REM and NREM Sleep
REM NREM EEG Mixed frequency,
fast Spindles,
K-complexes, Delta waves
EMG Absent Present but lowEOG Rapid Slow
Autonomic Nervous System
Variable Regular
Nocturnal Penile Tumescence
Present Absent
Respiration Variable Regular
Sleep Staging in a Young Adult
Adapted from Sleep Multimedia, 1998
Sleep (and the likelihood of falling asleep) is regulated by two key processes
Process S: homeostatic drive for sleep
Process C: circadian variation in alertness
2-Process Model of Sleep Regulation
Borbely, 1982;

Homeostasis - Daytime Sleepiness
Human Circadian Rhythms
Sleep-Wake CycleCircadian and Homeostatic Regulation of Sleep
Wake
Sleep
Wake Propensity
9 am 3 pm 9 pm 3 am 9 amAsleepAwake
Melatonin
Sleep Drive
Circadian Alerting
Signal
Adapted from Kilduff TS, Kushida CA. Circadian regulation of sleep. In: Chokroverty S, ed. Sleep Disorders Medicine: Basic Science, Technical Considerations, and Clinical Aspects. 2nd ed. Boston, Mass: Butterworth-Heineman; 1999. [Evidence Level C]. Kennaway DJ, Voultsios A. J Clin Endocrinol Metab. 1998;83:1013-1015. [Evidence Level C]

Sleep changes across the human lifespan, from infancy to old age.Some age-related changes in sleep are normal.Other changes reflect increasing rates of sleep disorders
Obstructive Sleep ApneaRestless Legs SyndromeCircadian Rhythm Sleep DisordersInsomniaREM Behavior Disorder
Sleep Across the lifespan
Distribution of Sleep in Human Development
Adapted from Basics of Sleep Behavior, 1993
Sleep and Age
Tota
l Sle
ep in
Min
utes
700
600
500
400
300
200
100
Age in Years10 20 30 40 50 60 70 80
Total time in bed
Awake in bedNREM 1
REM
NREM 2
NREM 3
Williams RL, et al. EEG of Human Sleep:ClinicalApplications. New York, NY: Wiley & Sons; 1974.

Reported Hours Slept Older vs. Younger American Adults
6.7 7.66.9 7.17.1 7.27 7.1
6.2
6.4
6.6
6.8
7
7.2
7.4
7.6
7.8
Week Nights Weekends
Hou
rs
18-54 55-64 65-84 55-84
2003 NSF Sleep in America Poll
Time use on an average work day for employed persons ages 25-54 with children
SOURCE: Bureau of Labor Statistics, American Time Use Survey (2010)
How Much Sleep Do You Need?The amount that permits you to be wide awake, alert and energetic throughout the dayThe average sleep need is about 7-8 hoursSleep need varies considerably from person to person and is likely genetically determined

Definitions, consequences and comorbidities
Jennifer L. Martin, PhD CBSMAdjunct Assistant Professor
David Geffen School of MedicineUniversity of California, Los Angeles
Career Research Scientist and PsychologistVA Greater Los Angeles Health Care System
Certified, Behavioral Sleep Medicine
Definition of Insomnia
DefinitionConsequencesComorbidites
Insomnia: Diagnosis
Review of diagnostic criteriaAPA’s Diagnostic and Statistical Manual –Forth Edition (DSM-IV)International Classification of Sleep Disorders – Revised (ICSD)Research Diagnostic Criteria for Insomnia (RDC)
Jennifer L. Martin, PhDAmerican Psychological Association 1994; American Academy of Sleep Medicine 2005 ; Edinger et al. 2004 ;

A. The predominant complaint is difficulty initiating or maintaining sleep for at least 1 month
B. The sleep disturbance (or associated daytime fatigue) causes clinically significant distress or impairment in social, occupational or other important areas of functioning
DSM-IV Primary Insomnia
American Psychological Association 1994
C. The sleep disturbance does not occur exclusively during the course of narcolepsy, breathing-related sleep disorder, circadian rhythm sleep disorder or a parasomnia
D. The sleep disturbance does not occur exclusively during the course of another mental disorder (e.g., major depressive disorder, generalized anxiety disorder, a delirium)
E. The disturbance is not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition.
DSM-IVPrimary Insomnia
American Psychological Association 1994
A. A complaint of difficulty initiating sleep, difficulty maintaining sleep, or waking up too early or sleep that is chronically nonrestorative or poor in quality.*
B. The above sleep difficulty occurs despite adequate opportunity and circumstances for sleep.
ICSD - RevisedInsomnia
American Academy of Sleep Medicine 2005
*In children, the sleep difficulty is often reported by the caretaker and may consist of observed bedtime resistance or inability to sleep independently.

C. At least one of the following forms of daytime impairment related to the nighttime sleep difficulty is reported by the patient:i. Fatigue or malaiseii. Attention, concentration or memory impairmentiii. Social or vocational dysfunction or poor school performanceiv. Mood disturbance or irritabilityv. Daytime sleepinessvi. Motivation, energy, or initiative reductionvii. Proneness for errors or accidents at work or while drivingviii. Tension, headaches or gastrointestinal symptoms in response to
sleep lossix. Concerns or worries about sleep
ICSD-RevisedInsomnia
American Academy of Sleep Medicine 2005
Adjustment insomnia (acute insomnia)Psychophysiological insomniaParadoxical insomniaIdiopathic insomniaInsomnia due to a medical disorderInadequate sleep hygieneBehavioral insomnia of childhoodInsomnia due to drug or substanceInsomnia due to medical conditionInsomnia not due to substance or known physiological condition, unspecified (nonorganic insomnia, NOS)Physiological (organic) insomnia, unspecified
ICSD-RevisedInsomnia subtypes
American Academy of Sleep Medicine 2005
A. The patient’s symptoms meet the criteria for insomnia.B. The insomnia is present for at least 1 month.C. The patient has evidence of conditioned sleep difficulty
and/or heightened arousal in bed as indicated by one or more of the following:i. Excessive focus on and heightened anxiety about sleepii. Difficulty falling asleep in bed at the desired bedtime or during
planned naps, but no difficulty during other monotonous activities when not intending to sleep
iii. Ability to sleep better away from home than at homeiv. Mental arousal in bed characterized by intrusive thoughts or
perceived inability to stop sleep-preventing mental activityv. Heightened somatic tension in bed reflected by a perceived
inability to relax the body sufficiently to allow the onset of sleep
ICSD-RevisedPsychophysiological insomnia
American Academy of Sleep Medicine 2005

D. The sleep disturbance is not better explained by another sleep disorder, medical condition, mental disorder, medication use or substance use disorder
ICSD-RevisedPsychophysiological insomnia
American Academy of Sleep Medicine 2005
A. The individual reports one or more of the following complaints:1. difficulty initiating sleep 2. Difficulty maintaining sleep3. Waking up too early or4. Sleep that is chronically nonrestorative or poor in quality
B. The above sleep difficulty occurs despite adequate opportunity and circumstances for sleep
Research Diagnostic Criteriafor Insomnia Disorder
Edinger et al, 2004
Insomnia ≠ Sleep Deprivation
InsomniaSleep Deprivation
Sleep Opportunity Adequate Reduced
Sleep Ability Reduced Adequate

Insomnia ≠ Sleep Deprivation
Insufficient opportunity for sleep (i.e., not spending enough time in bed)Inadequate circumstances for sleep (e.g., homelessness)Accompanied by daytime sleepiness or drastic measures to counteract sleepiness (e.g., overuse of stimulants)Effects reversed if opportunity lengthend and/or circumstances are improved
Prevalence of Chronic Insomnia in the General Adult Population
Ford , Kamerow . JAMA. 1989;262:1479-1484. Ohayon et al. Compr Psychiatry. 1998;39:185-197. Ohayon , Roth . J Psychosom Res. 2001;51:745-755. Ancoli-Israel , Roth . Sleep. 1999;22(suppl 2):S347-S353. Ishigooka et al. Psychiatry Clin Neurosci. 1999;53:515-522. Simon , VonKorff . Am J Psychiatry. 1997;154:1417-1423.; Leshner et al. NIH State-of-the-Science Conference Statement, June 15, 2005.
10.2
17.7 16.8
9
11.710
0
5
10
15
20
Percen
t (%)
Ancoli‐Israel1999
Ford1989
Ohayon1998
Ohayon2001
Ishigooka1999
Simon1997
Insomnia = sleep disturbance every night for >2 weeks, or similarly stringent criteria
30% of the general population has disturbed sleep10% of the general population meet diagnostic criteria50% of patients under clinical care meet diagnostic criteria
Reid et al, Am J Geriatr Psychiatry, 2006, 14:860‐866
Insomnia Is Under-reported
Number of Sleep Complaints Endorsed (n=1503, age 60-100y) 69% endorsed at least one sleep problem40% endorsed >2 sleep problems45% endorsed symptoms of insomniaBUT Identified in medical chart only 19% of time
26% ‐ Discussed sleep during visit for other purpose
5% ‐ Visited specifically to discuss sleep problem
69% ‐Never
discussed
Percent of insomniacs who discussed sleep problems with their physicians
Ancoli-Israel S, Roth T. Sleep. 1999;22(suppl 2):S347-S353

The Interplay of Sleep and Illness
Psychiatric/Medical Illness
Direct Influence on Sleep Architecture
Medications for Illness Influence Sleep
Sleep Disruption
Exacerbates
Comorbid conditions and insomnia…
Most likely, there is a BI-DIRECTIONAL relationship between insomnia and comorbid conditions
Medical and psychiatric conditions increase risk of insomniaInsomnia exacerbates symptom severity and increases risk of relapse
Insomnia itself is associated with multiple negative consequences.
Mechanism Linking Sleep and HealthIn the laboratory setting, short-term sleep restriction leads to
a variety of adverse physiologic sequelae, includingImpaired glucose controlIncreased cortisolIncreased blood pressureSympathetic activationIncreased markers of inflammationDecreased leptin level
These data suggest that chronic sleep restriction may have long-term health consequences
Zee PC, et al. Arch Intern Med. 2006;166:1686-1688.

Impaired cognitive functioning1
Negative quality-of-life measures1
Increased incidence of bodily pain, poorer general health1-3
Increased future risk of psychiatric disorders4
Decreased job performance, increased absenteeism1
Increased risk of accidents5
Increased health care costs6,7
Impaired cognitive functioning1
Negative quality-of-life measures1
Increased incidence of bodily pain, poorer general health1-3
Increased future risk of psychiatric disorders4
Decreased job performance, increased absenteeism1
Increased risk of accidents5
Increased health care costs6,7
1. Zammit GK, et al. Sleep. 1999;22 Suppl 2:S379-S385.2. Bixler EO, et al. Life Sci. 1979;25(16):1379-1388.3. Mellinger GD, et al. Arch Gen Psychiatry. 1985;42(3):225-232.4. Breslau N, et al. Biol Psychiatry. 1996;39(6):411-418.5. Balter MB, Uhlenhuth EH. J Clin Psychiatry. 1992;53 Suppl:34-39; discussion 40-42.6. Simon GE, VonKorff M. Am J Psychiatry. 1997;154(10):1417-1423.7. Ford DE, Kamerow DB. JAMA. 1989;262(11):1479-1484.
Impairments Associated with Insomnia
Quality of Life in Insomnia
SF-3
6 Sub
scale
Sco
re
Control, n=101 Insomnia, n=261
* ** *
**
*
*
**P<0.0001Zammit GK, et al. Sleep. 1999;22(suppl):S343-S412.
0102030405060708090
100
Body Pain GeneralHealth
Mental Health EmotionalRole
Physical Role SocialFunctioning
PhysicalFunctioning
Vitalityworse
Primary vs. Comorbid InsomniaPrimary
Insomnia(15%)
Other SleepDisorders
(10%)
Other Illnesses,Medications, etc
(25%)
PsychiatricDisorders
(50%)
Ford DE, et al. JAMA. 1989;262:1479-1484.

Psychiatric disorders associated with insomnia
Mood disordersMood disordersMajor depressionMajor depressionDysthymicDysthymic disorderdisorderBipolar affective disorderBipolar affective disorder
Anxiety disordersAnxiety disordersGeneralized anxiety disorderGeneralized anxiety disorderPanic disorderPanic disorderPTSDPTSD
Psychotic disordersPsychotic disordersSchizophreniaSchizophrenia
Substance use disordersSubstance use disordersDiagnostic and Statistical Manual of Psychiatric Disorders, Fourth Edition, Text Revision. American Psychiatric Association, 2000.
n=580Adapted from: Ford DE, Kamerow DB. JAMA. 1989:262:1479-1484.
Comorbid Psychiatric Disorders Among Patients with Insomnia
0% 10% 20% 30% 40% 50% 60%
Drug Abuse
Other psychiatric disorders
Alcohol abuse
Dysthymia
Major depression
Anxiety disorder
No psychiatric disorder
4.2%
5.1%
7.0%
8.6%
14.0%
23.9%
59.5%
Insomnia Is a Risk Factor for Psychiatric Disorders
* 95% CI for odds ratio excludes 1.0.Breslau N et al. Biol Psychiatry. 1996;39:411‐418.
Inci
denc
e (%
) Ove
r 3.5
Yea
rs
**
*
0
5
10
15
20
Depression Anxiety Alcohol Abuse Drug Abuse
Insomnia, n=240 No Insomnia, n=739

The Treatment of Insomnia Comorbid with Depression Improves Outcome: Fluoxetine + Eszopiclone vs Fluoxetine + Placebo
(N=545)
Fava M et al. Biol Psychiatry. 2006.
*
** *
**
240
270
300
330
360
390
420
-1 0 1 2 3 4 5 6 7 8
Placebo + FluoxetineEszopiclone + Fluoxetine
Tota
l Sle
ep T
ime
(Min
)
Weeks
*P<.0001
Insomnia Efficacy
P<.001 P<.01
Improvement in HAM-D17 Excluding Insomnia Items
% Remitters(HAM-D17≤7)
Significant Effect on Depression Response
43
55
0
10
20
30
40
50
60
End of Study
Pcbo+
Flu
ESZ+
Flu
9.5
11.1
0
2
4
6
8
10
12
14
End of Study
Pcbo+Flu
ESZ+Flu
Residual Insomnia After Treatment for Depression
0 20 40 60 80
Mood
Interest
Weight
Sleep
Fatigue
Guilt
Concentration
Percent with residual symptom
Threshold
Subthreshold
Nierenberg, 1999. J Clin. Psych
Medical disorders and conditions associated with insomnia
CardiovascularCongestive heart failure
PulmonaryCOPDAsthma
Renal and genitourinaryChronic renal failureProstatic hypertrophy
GastrointestinalGastroesophageal reflux disease
MusculoskeletalFibromyalgiaOsteoarthritisRheumatoid Arthritis
EndocrineHyperthyroidism
NeurologicalParkinson’s DiseaseCerebrovascular disease
OtherMenopause
Consider all causes of pain, breathing difficulty, impaired mobility

Many Medical Conditions Disturb Sleep
HeadachesNeurodegenerative Processes
Arthritic Pain
CAD/ CHFGI changes (GERD, Dyspepsia)
Benign prostatichypertrophy & Nocturia
Orofacial Pain/ TMJ
Peripheral Neuropathy with Pain
COPD
Nocturia and sleep
Particularly among older patients, nocturia is a common comorbidityImportant to assess frequency of urination at night during initial evaluationIn some cases, treatment of insomnia will lead to more consolidated sleepIn some cases, nocturia will require further evaluation and separate treatment
Nocturia and Disturbed Sleep
Survey study of 1506 adults aged 55-84 yearsThose with nocturia were more likely to define themselves as having:
Bliwise, D et al. Nocturia and disturbed sleep in the elderly. Sleep Med, 2008, in press.
Nocturia No Nocturia p-valueInsomnia 22.5% 13% <0.0001Poor sleep quality 27.3% 16.7% <0.0001

Nocturia and Disturbed Sleep
Nocturia and poor sleep are independently related to each other (n=2081)
Independent of other medical conditionsCongestive heart failureDiabetesDiuretics
Rembratt et al. et Nocturia and associated morbidity… BJU Int 2003, 92:726-30
Prevalence of Insomnia in Chronic Medical Conditions
0
10
20
30
40
50
60 InsomniaSevere insomnia
Adapted from Katz DA, McHorney CA. Arch Intern Med. 1998;158:1099-1107.
Tota
l Res
pond
ents
(%)
N = 3,445
Hip MI COPD Angina Prostate CHF DiabetesImpairment Problems
Sleep Problems and Multiple Medical Conditions
01020304050607080
< 6 hr sleep Any Insomnia EDS
Perc
ent
0 1 2 or 3 4 or more
Foley, Ancoli-Israel, Bitz, Walsh, J Psychosom Res. 2004, 56(5):497-502.

Medications and substances associated with insomnia
AlcoholAlcoholAcute useAcute useWithdrawalWithdrawal
CaffeineCaffeine
NicotineNicotine
AntidepressantsAntidepressantsSSRISSRISNRI, atypicalSNRI, atypical
CorticosteroidsCorticosteroids
DecongestantsDecongestantsPseudoephedrinePseudoephedrine
ββ agonists, agonists, theophyllinetheophyllinederivativesderivatives
ββ antagonistsantagonists
StatinsStatins
StimulantsStimulants
Dopamine agonistsDopamine agonists
Any drug that crosses the blood brain barrier and affects a neurotransmitter system may be associated with insomnia.
SSRI = Selective Serotonin Reuptake Inhibitor; SNRI = Serotonin and Norepinephrine Reuptake Inhibitor; Schweitzer, PPSM.
Treating insomnia with comorbidities
Comorbid psychiatric medical or psychiatric disorders may necessitate modifications to treatment, but do not necessarily indicate the patient should not be treated with CBT-IOptimize treatment of comorbid conditions (considering impact of medications on sleep)
“Comorbid” InsomniaIt doesn’t matter…
Comorbid Insomnia may:Worsen clinical outcomes and impact quality of life1
Predispose patients to recurrence of depression2
Persist despite treatment of the comorbid condition3
Insomnia treatment may actually improve outcomes for the comorbid condition (depression, pain)
Behavioral treatments are appropriate and effective for “comorbid insomnia”
1. Katz DA, McHorney CA. J Fam Pract. 2002;51:229-235.; 2. Chang PP, Ford DE, Mead LA, Cooper-Patrick L, Klag MJ. Am J Epidemiol. 1997;146:105-114.; 3. Ohayon MM, Roth T. Psychiatr Res. 2003;37:9-15.

1
Sleep Disorders Masquerading as Insomnia
Sonia Ancoli-Israel, PhD
Professor of PsychiatryDirector, Gillin Sleep and Chronomedicine Research Center
Director of Education, UCSD Sleep Medicine CenterDeputy Director, Stein Institute for Research on Aging
University of California San Diego
Diplomate, American Board of Sleep MedicineCertified, Behavioral Sleep Medicine
Obstructive Sleep Apnea
Pauses in breathing during sleep> 10 sec
Apnea = cessation of airflowHypopnea = decreased (>50% of baseline amplitude) airflow yp p ( p )+ 4% desaturation
Followed by loud snoring and gasping when breathing starts
Results in brief awakenings (arousals)
Excessive daytime sleepiness
Obstructive Sleep ApneaUpper airway collapse in the setting of ongoing (increased) pulmonary effort
Figure from Lyle et al (1999) American Family Physician 60:2279-2286
2
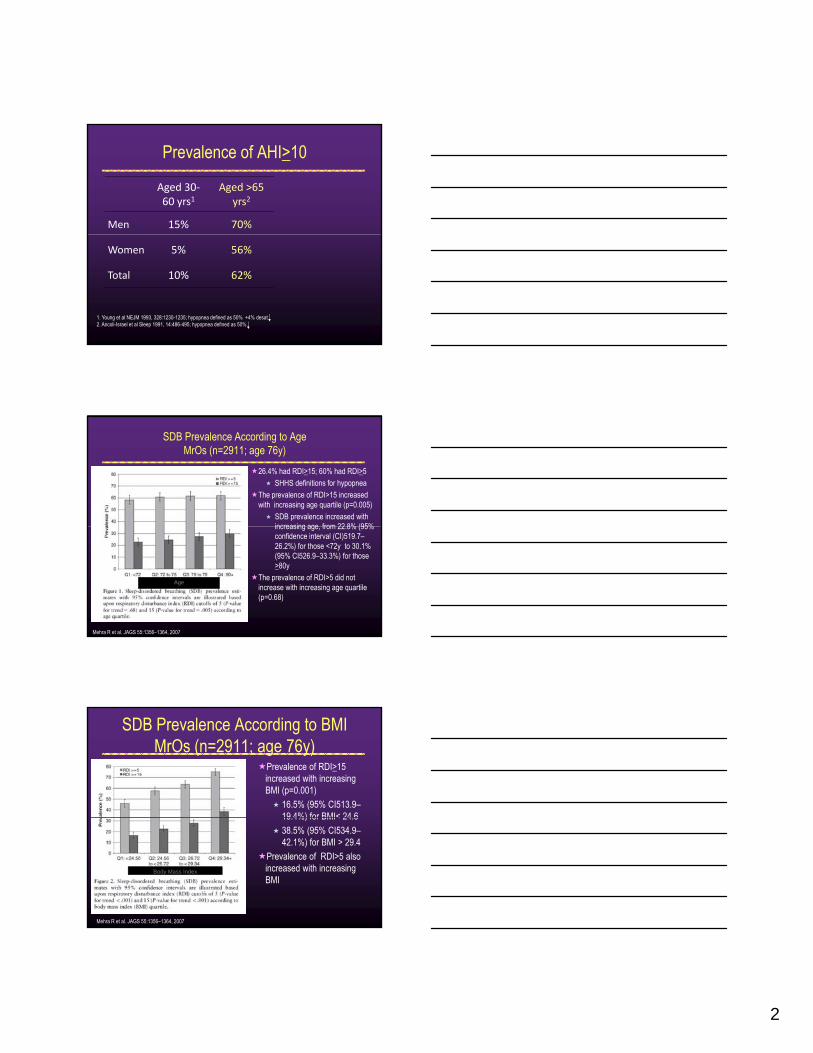
Prevalence of AHI>10
Aged 30‐60 yrs1
Aged >65 yrs2
Men 15% 70%
Women 5% 56%
Total 10% 62%
1. Young et al NEJM 1993, 328:1230-1235; hypopnea defined as 50% +4% desat2. Ancoli-Israel et al Sleep 1991, 14:486-495; hypopnea defined as 50%
SDB Prevalence According to AgeMrOs (n=2911; age 76y)
26.4% had RDI>15; 60% had RDI>5SHHS definitions for hypopnea
The prevalence of RDI>15 increased with increasing age quartile (p=0.005)
SDB prevalence increased with increasing age from 22 8% (95% increasing age, from 22.8% (95% confidence interval (CI)519.7–26.2%) for those <72y to 30.1% (95% CI526.9–33.3%) for those >80y
The prevalence of RDI>5 did not increase with increasing age quartile (p=0.68)
Age
Mehra R et al. JAGS 55:1356–1364, 2007
SDB Prevalence According to BMIMrOs (n=2911; age 76y)
Prevalence of RDI>15 increased with increasing BMI (p=0.001)
16.5% (95% CI513.9–19 4%) for BMI< 24 619.4%) for BMI< 24.638.5% (95% CI534.9–42.1%) for BMI > 29.4
Prevalence of RDI>5 also increased with increasing BMI
Body Mass Index
Mehra R et al. JAGS 55:1356–1364, 2007

3
Risk Factors for OSAAgeMale genderObesitySmokinggAlcohol before sleepFamily historyNasal obstruction
Clinical PresentationChronic loud snoringFrequent nocturnal awakeningsGasping arousals
Excessive daytime sleepiness
Wake with a dry mouth
Wake with a headache
Poor memory and Witnessed apneasFrequent nocturnal awakeningsFrequent nocturiaNon-restorative sleepProfuse sweating during sleep
Poor memory and concentration
Daytime fatigue
Changes in personality (impatient, easily irritated)
Ancoli-Israel (2007) Sleep Med Rev. 11(2):83-5; Ancoli-Israel et al (1991) Sleep 14(6):486–95
And sometimes insomnia
Consequences of Untreated OSASleep and Sleepiness
Sleep FragmentationExcessive Daytime SleepinessNocturia
Cardiovascular Effects
Impaired Cognitive FunctionPsychomotor vigilance AccuracySustained attentionConstructional abilitiesCardiovascular Effects
Increased blood pressureIncreased stroke risk
MortalityAHI ≥ 5 significantly associated with death (HR 1.97)
Depression?
Constructional abilitiesVisuospacial learningExecutive functionMotor performance
Impaired DrivingIncreased risk of MVAImpaired reaction timesDivided attention deficits
Reviewed in Norman and Loredo (2008) Clin Geriatr Med 24(1) 151-65

4
OSA EvaluationStarts in the waiting room
How sleepy is the patientObservationEpworth Sleepiness Scale
Full sleep historyp yBMI
41% of OSA attributable to a BMI ≥ 25 kg/m2
Neck circumferenceMen > 17 inchesWomen > 16 inches
Pharynx – Mallampati classification
Mallampati Classification
Diagnosis
Sleep history and clinical evaluationPolysomnography
Overnight laboratory sleep Overnight laboratory sleep studyUnattended home sleep study
Photos courtesy of Jose Loredo MD, MPH, FCCP

5
OSA: Severity index
Apnea-hypopnea Index (AHI)Number of apneas plus hypopneas per hour of sleep
Normal Less than 5/hrNormal Less than 5/hr
Mild 5 - 19/hr
Moderate 20 - 29/hr
Severe More than 30/hr
OSA: who needs treatment?
Abnormal sleep study (AHI > 5/hr), andExcessive daytime sleepinessHypertensionHeart failureHeart failureCoronary heart diseaseStrokePulmonary hypertension
OSA: Treatment optionsContinuous positive airway pressure (CPAP)Weight reductionSleeping in the lateral positionp g pJaw advancement devicesPharyngeal surgery

6
Restless Legs Syndrome
Restless Legs SyndromeFeelings of “creepy/crawling” sensations in legssensations in legsRelieved only with movementDiagnosis made on history
Restless Legs Syndrome Patients descriptions
BurningCreeping
WormyTingling
TuggingPullingInsects crawling inside legs
Pins and needlesPainfulPrickly
Prevalence of RLS by Age
ent w
ith R
LS
Age Group, Range in Years
Perc
e
Ohayon MM and Roth T. J Psychosom Res. 2002;53:547-554; Phillips B et al. Arch Intern Med. 2000;160:2137-2141; Berger K et al. Arch Intern Med. 2000;164:196-202; Rothdach AJ et al. Neurology. 2000;54:1064-1068; Lavigne GJ and Montplaisir JY. Sleep. 1994;17:739-743; Ulfberg J et al. Mov Disord. 2001;16:1159-1163.
Ohayon MM and Roth T. J Psychosom Res. 2002;53:547-554; Phillips B et al. Arch Intern Med. 2000;160:2137-2141; Berger K et al. Arch Intern Med. 2000;164:196-202; Rothdach AJ et al. Neurology. 2000;54:1064-1068; Lavigne GJ and Montplaisir JY. Sleep. 1994;17:739-743; Ulfberg J et al. Mov Disord. 2001;16:1159-1163.

7
Screening Questions1. Do you have, or have you sometimes experienced, recurrent, uncomfortable feelings or sensations in your legs while sitting or lying down?2. Do you have, or have you sometimes experienced, a recurrent need or urge to move your legs while sitting or lying down?need or urge to move your legs while sitting or lying down?3. Do these uncomfortable feelings or sensations in your legs, or the need or urge to move, disappear/improve when you are active or moving around?4. Are these uncomfortable feelings, or this urge to move, worse in the evening or at night compared with the morning?
Periodic Limb Movements in Sleep
Periodic Limb Movements in SleepLeg or legs jerk every 20-40 secondsClustered in repetitive episodesPLM index (PLMI) > 5 with arousalsDiagnosis of disorder
Made by PSGGenerally includes complaints of sleep or daytime consequences
RLS vs. PLMS
RLS symptom based on di i
PLMSEMG finding
diagnosisDiagnosed in office80% have PLMS
Diagnosed in sleep laboratory30% have RLS symptoms

8
Treatment for RLS/PLMSDopamine Agonists
ropinirole (Requip) 0.5-4 mg Can be safely titrated up to 4 mg po 2 hours before bedtime
pramipexole (Mirapex) 0.125-.5 mgUsually 0.5 to 0.75 mg po 2 hours before bedtime is enough to control RLS or PLMDcontrol RLS or PLMD
gabapentin enacarbil (Horizant) Extended-Release Tablets 600mgapproved for moderate-severe RLS600 mg once daily taken with food at about 5 PM; doubling dose does gets no additional benefit compared with the 600-mg dose, but caused an increase in adverse reactions
levodopa/carbidopa (Sinemet) 25/100 *
Hening et al. Sleep. 2004;27:560-583; Littner et al. Sleep. 2004;27:557-559.
* off-label
Wake up
Sleepy–Go to bed
Sleepy–Go to bed
Wake up
Standard phase
Delayed phase
Circadian Sleep Phases
Sleepy Go to bed
Wake up
18.00 21.00 24.00 3.00 6.00 9.00 12.00
Advanced phase
Time of Day
Modified from Ancoli-Israel, All I Want is a Good Night’s Sleep, Mosby 1996
Behavioral CRD ManagementOptimizing Alertness
Appropriatelytimed light
Barion A, Zee PC. Sleep Med. 2007;8(6):566-577; Sack RL, et al. Sleep. 2007;30(11):1460-1483; Sack RL, et al. Sleep. 2007;30(11):1484-1501; Takeyama H, et al. Ind Health. 2005;43(1):24-29.
Adequate sleep time Scheduled naps

9
RBD Case Example
A 60-year old surgeon began to punch and kick his wife and jump out of bed during nightmares of being attacked “by criminals, terrorists, and monsters who always tried to kill me.” Work-related stress was the presumed cause of his sleep disturbance but the violent behaviors intensified sleep disturbance, but the violent behaviors intensified despite retirement 3 years later. He sustained several head lacerations, and his wife once had a severe headache for 2 days after receiving an accidental blow to the ear. The proper diagnosis was established after 11 years. A prodrome of excessive limb and body jerking during sleep had been present for at least 33 years.
Principles and Practice of Sleep Medicine, 1994
Pharmacologic Treatment of RBD
Neurological examPharmacological Treatment
Clonazepam* – effective in ~90% of patients0.25-0.5mg at bedtimeTolerance generally does not developTolerance generally does not developDiscontinuation = immediate relapseMechanism of action unknown
Melatonin*One hour before bedtimestarting at 6mg; increasing to 12-15 mg
Behavioral treatment *off-label
Clonazepam: Frenette E.Med Clin North Am. 2010 May;94(3):593-614. Melatonin: Boeve BF, Silber MH, Ferman TJ. Sleep Med. 2003 Jul;4(4):281-4; Takeuchi N et al. Psychiatry Clin Neurosci. 2001 Jun;55(3):267-9
1
Assessing Insomnia
Sonia Ancoli-Israel, PhD
Professor of PsychiatryDirector, Gillin Sleep and Chronomedicine Research Center, p
Director of Education, UCSD Sleep Medicine CenterDeputy Director, Stein Institute for Research on Aging
University of California San Diego
Diplomate, American Board of Sleep MedicineCertified, Behavioral Sleep Medicine
Outline
Clinical InterviewPolysomnography (PSG)ActigraphySleep Diary / Questionnaires
Clinical interview (45-50 minutes)Sleep diaries
2 weeks pre-treatmentThroughout treatment (to assess response)
Our approach to assessment
Throughout treatment (to assess response)Sometimes questionnaires
Bedpartner/caregiverPre-post treatment questionnaires
Sometimes wrist actigraphyPoor historian, diaries unclearUnsatisfactory treatment response
Jennifer L. Martin, PhD

2
Clinical InterviewAsk questions about current sleep, sleep history, medical/psychiatric comorbidities, lifestyle factorsGather information on differentialGather information on differential diagnosisClinical expertise comes into play
Jennifer L. Martin, PhD
Sleep HistoryObtain complete sleep history, including specific sleep problems and sleep scheduleDetermine
Alcohol, caffeine and nicotine Alcohol, caffeine and nicotine consumptionUse of prescription and OTC medications and any illicit drugsPresence of concomitant medical or psychiatric conditionsRecent life stress
1. Consensus Conference. JAMA. 1984;251:2410-2414.2. Erman MK. In: Sleep Disorders: Diagnosis and Treatment. 1998:21-51.
Questions to Ask your PatientsTypical 24 hours
Do you have difficulty falling sleep/staying asleep?Does your lack of sleep effect your ability to function?Do you fall asleep at inappropriate times?If you could go to sleep and wake up at any time what If you could go to sleep and wake up at any time, what times would you choose?What time do you go to bed?/ to sleep?What time do you wake up?/ get out of bed?

3
Questions to Ask your PatientsSleep Disorders
Questions related to RLS/PLMSQuestions related to SDB
Snoring, gasping, observed apneasA k i ith d th i h d hAwakening with dry mouth; morning headache
Questions related to narcolepsyQuestions related to RBD
Polysomnography
Indicated for diagnosis ofObstructive sleep apneaNarcolepsyPLMSPLMSRBD
Not indicated for diagnosis ofInsomnia
Unless treatment non-response
Polysomnography: Recording Sleep
•EEG (brain activity)•EOG (eye movements)•EMG (muscle tone)
•Respiratory effort•Air flow•O2 saturation•EKG •Leg movements•Sound / Video

4
Sleep Variables
Total Sleep Period (TSP) =TST+WASO
Wrist Actigraphs
Mini Mitter Actiwatch
*Ambulatory Monitoring,Inc
AMI Octagonal Motionlogger Sleep Watch
Why Actigraphy?Ease of objective data collectionAcceptable to more patientsRecord over multiple days/nights
Can record for weeks/monthsCan record for weeks/monthsRelatively low-costStudy patients in “home” environmentAssess treatment outcomes
Ancoli-Israel et al, The role of actigraphy in the study of sleep and circadian rhythms. Sleep, 2003, 26(3)342-92

5
EM017
C1W0
C1W2
10/25/01
10/26/01
10/27/01
11/04/01
11/05/01
11/06/01
11/21/01
11/22/01
11/23/01
11/28/01
C1W1
Advantages
Easy to record for multiple nightsExample on left is 8 72 h i d
0000 2400 24001200 1200
C1W3
C4W0
C4W1
C4W2
C4W3
11/28/01
11/29/01
11/30/01
01/10/02
01/11/02
01/12/02
01/17/02
01/18/02
01/19/02
01/24/02
01/25/02
01/26/02
01/31/02
02/01/02
02/02/02
8 72-hours periods of recording during chemotherapy
Ancoli-Israel et al, The role of actigraphy in the study of sleep and circadian rhythms. Sleep, 2003, 26(3)342-92
Actigraphic Sleep/Wake Data Total sleep timeTotal wake timeNumber of awakeningsDuration of awakeningsSleep bouts/wake boutsNapping behavior
Ancoli-Israel et al, The role of actigraphy in the study of sleep and circadian rhythms. Sleep, 2003, 26(3)342-92
Use of actigraphy in the evaluation of sleep disorders: Recommendations
Actigraphy is indicated to assist in the evaluation of patients suspected of:
advanced sleep phase syndrome, delayed sleep phase syndrome and shift work disorder (Guidelines)syndrome and shift work disorder (Guidelines)Jet lag and non-24-hour sleep/wake rhythm, including that associated with blindness (Option)
Actigraphy is useful as an outcome measure in evaluating the response to treatment for circadian rhythm disorders (Guideline).
Morgenthaler et al. Practice parameters for the use of actigraphy in the assessment of sleep and sleep disorders: an update for 2007. SLEEP 2007;30(4):519-529

6
Use Actigraphy Plus…Sleep diaries/daily logsObservationsLight exposure
ALWAYS collect collateral information
Ancoli-Israel et al, The role of actigraphy in the study of sleep and circadian rhythms. Sleep, 2003, 26(3)342-92
Actigraphy Data: 72-year-old Man
shower shower“in bed”
Sleeping @ TV
nap
Actigraphy in insomnia patient and healthy control subject
Insomnia patient (68 yr. F) Control subject (78 yr. F)

7
Actigraphy in insomnia patient and healthy control subject
Control subject (78 yr. F)Insomnia patient (68 yr. F)
•Lower level of overall activity•Irregularity of sleep “window”•Inactive periods in day
•Higher level of overall activity•Regular sleep “window”•Few inactive periods in day
Bright White Light
Baseline
Cycle 4
Actigraphy Plots
Dim Red Light
Baseline
Cycle 4
MN noon MN Noon MN
TreatmentEffects
QuestionnairesGeneral sleep questionnaires (PSQI)Insomnia specific (ISI)Not diagnostic per se, but useful in pre/post assessment of treatment responseassessment of treatment responseSometimes used as measures of treatment response in research
Jennifer L. Martin, PhD

8
Sleep Questionnaires
Sleep DiaryPittsburgh Sleep Quality Index (PSQI)I i S it I d
Horne-Osberg Morningness/Eveningness ScaleBerlin QuestionnaireInsomnia Severity Index
(ISI)Epworth Sleepiness Scale
Berlin QuestionnaireSTOP
Consensus Sleep Diary
Filled out every morning for any given time periodSubjective estimates of sleep onset time, total sleep time, number and duration of awakenings, quality of sleep
Carney CE; Buysse DJ; Ancoli-Israel S; Edinger JD; Krystal AD; Lichstein KL; Morin CM. The consensus sleep diary: standardizing prospective sleep self-monitoring. SLEEP 2012;35(2):287-302.
sleep, Sleep efficiency can be computed
Percent of time spent asleep given the amount of time in bed
Consensus Sleep Diary
Carney CE; Buysse DJ; Ancoli-Israel S; Edinger JD; Krystal AD; Lichstein KL; Morin CM. The consensus sleep diary: standardizing prospective sleep self-monitoring. SLEEP 2012;35(2):287-302.

9
Pittsburgh Sleep Quality Index (PSQI)The PSQI measures reported sleep patterns and sleep problems
sleep qualitysleep latencysleep efficiencynapping behavior
19-item questionnaire 19 item questionnaire Demonstrated to have
high internal consistency (0.83),Test-retest reliability (0.85) diagnostic validity.
A global sleep quality score derived from the PSQI can be used to index overall quality of sleep over the prior one-week period. Global sleep quality scores are continuous (range 0-21) with high scores reflecting poor sleep quality.Scores >5 = poor sleep quality Buysse,D.J.,et al Sleep 14(4):331-338, 1991; Buysse,D.J., et al.
Psychiatry Res. 28(2):193-213, 1989.
Pittsburgh Sleep Quality Index (PSQI)Instructions: The following questions relate to your usual sleep habits during the past week only. Your answers should indicate the most accurate reply for the majority of days and nights in the past week. Please answer all questions.
1. During the past week, when have you usually going to bed at night?am/pm (usual bedtime)_______am/pm (usual bedtime)
2. During the past week, how long in minutes has it usually taken you to fall asleep each night? _____________ number of minutes3. During the past week, when have you usually gotten up in the morning? __________am/pm (usual wake time)4. During the past week, how many hours of actual sleep did you get at night? (this many be different than the number of hours you spend in bed.) _______ hours ______ minutes
Pittsburgh Sleep Quality Index (PSQI) (con’t)
5. During the past week, how often have you had trouble sleeping because you…a. cannot get to sleep within 30 minutes?b. wake up in the middle of the night or early morning?c. have to get up to use the bathroom?d. cannot breathe comfortably?e. cough or snore loudly?f. feel too cold?g. feel too hot?h. had bad dreams?i. have pain?j. other reasons? Describe: ___________________________
Answers are checked in a box: Not during the past week; Less than once a week; Once or twice a week; Three or more times a week

10
Pittsburgh Sleep Quality Index (PSQI) (con’t)
5 (con’t)How often during the past week have you had trouble sleeping because of this?6. During the past week, how would you rate your sleep quality overall?
very good; fairly good; fairly bad; very bad7. During the past week, how often have you taken medicine (prescribed or “over the counter”) to help you sleep?
not during the past week; less than once a week; once or twice a week; three or more not during the past week; less than once a week; once or twice a week; three or more times a week
8. During the past week, how often have you had trouble staying awake while driving, eating meals, or engaging in social activity?
not during the past week; less than once a week; once or twice a week; three or more times a week
9. During the past week, how much of a problem has it been for you to keep up enough enthusiasm to get things done?
no problem at all; only a very slight problem; somewhat of a problem; a very big problem
Insomnia Severity Index (ISI)Composed of seven items that evaluate:
(a) the severity of sleep-onset (initial), (b) sleep maintenance (middle), (c) early morning awakening (terminal) problems, (d) satisfaction with current sleep pattern, (e) interference with daily functioning (e) interference with daily functioning, (f) noticeability of impairment attributed to the sleep problem, (g) level of distress caused by the sleep problem.
Each of these items is rated on a five-point Likert scale (`0' . not at all, `4' . extremely) Time interval is `in the last 2 weeks'. Total scores range from 0 to 28, with high scores indicating greater insomnia severity.Valid and sensitive measure to detect changes in perceived sleep difficulties with treatment.
Bastien, CH; Vallieres, A; Morin, CM. Validation of the Insomnia Severity Index as an outcomemeasure for insomnia research. Sleep Medicine 2 (2001) 297-307
Insomnia Severity IndexInsomnia Severity IndexParticipant code:__________________ Date: _________________ 1. Please rate the current SEVERITY of your insomnia problem(s) ( 0 None; 1 Mild; 2 Moderate ; 3 Severe; 4 Very)
Difficulty falling asleep: 0 1 2 3 4Difficulty staying asleep: 0 1 2 3 4Problem waking up too early: 0 1 2 3 4
2. How SATISFIED/ dissatisfied are you with your current sleep pattern?Very Satisfied Very Dissatisfied
0 1 2 3 40 1 2 3 43. To what extent do you consider your sleep problem to INTERFERE with your daily functioning (e.g., daytime fatigue, ability t function at work/daily chores, concentration, memory, mood, etc.)
Not at all Interfering A Little Somewhat Much Very Much Interfering
0 1 2 3 44. How NOTICEABLE to other do you think your sleeping problem is in terms of impairing the quality of your life?
Not at all Noticeable Barely Somewhat Much Very Much Noticeable
0 1 2 3 45. How WORRIED/ Distressed are you about your current sleep problem?
Not at all A Little Somewhat Much Very Much 0 1 2 3 4
Bastion et al. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297-307.

11
Epworth Sleepiness Scale
Measures daytime sleepinessSpecifically measures the likelihood of dosing or falling asleep during 8 situations
Each situation rated from 0 (would never dose) to 3 Each situation rated from 0 (would never dose) to 3 (high chance of dosing) Total possible score 24Scores >10 = pathological daytime sleepiness
Johns MW (1991). "A new method for measuring daytime sleepiness: the Epworth sleepiness scale". Sleep 14 (6): 540–5
Epworth Sleepiness ScaleHow likely are you to doze off or fall asleep in the following situations, in contrast to feeling just tired? This refers to your usual way of life in recent times. Even if you have not done some of these things recently, try to work out how they would have affected you.
Sitting and reading Watching TV Sitting, inactive in a public place (e.g., a theater or a meeting) In a car for an hour without a break Lying down to rest in the afternoon when circumstances permit Sitting and talking to someone Sitting quietly after lunch without alcohol In a car, while stopped for a few minutes in traffic 0= would never doze
1= slight chance of dozing2= moderate chance of dozing3= high chance of dozing
Johns,M.W. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep 15:376-381, 1992.; Johns,M.W. Sleepiness in different situations measured by the Epworth sleepiness scale. Sleep 17:703-710, 1994.
11.70
14.70
17.50
15.00
20.00
Sco
re
Evaluation of Daytime Sleepiness
Papp et al, Academic Medicine, 2002; Mustafa et al, Sleep and Breathing, 2005
5.90
2.20
0.00
5.00
10.00
Normal Insomnia Sleep Apnea Residents Narcolepsy
Epw
orth
S

12
Berlin Questionnaire for Sleep Apnea CATEGORY 1
3 categories related to the risk of having sleep apnea.Patients can be classified into High Risk or Low Risk based on their responses to the individual items and their overall scores in the symptom categories.Categories and scoring:
Category 1: items 1 2 3 4 5
Add points. Category 1 is positive if the total score is 2 or more points
Category 2: items 6, 7, 8 (item 9 should be noted separately).
Item 6: if ‘a’ or ‘b’ is the response, assign 1 pointItem 7: if ‘a’ or ‘b’ is the response, assign 1 pointIt 8 if ‘ ’ i th i 1 Category 1: items 1, 2, 3, 4, 5.
Item 1: if ‘Yes’, assign 1 pointItem 2: if ‘c’ or ‘d’ is the response, assign 1 pointItem 3: if ‘a’ or ‘b’ is the response, assign 1 pointItem 4: if ‘a’ is the response, assign 1 pointItem 5: if ‘a’ or ‘b’ is the response, assign 2 points
Item 8: if ‘a’ is the response, assign 1 point
Add points. Category 2 is positive if the total score is 2 or more pointsCategory 3 is positive if the answer to item 10 is ‘Yes’ OR if the BMI of thepatient is greater than 30kg/m2.High Risk: if there are 2 or more Categories where the score is positiveLow Risk: if there is only 1 or no Categories where the score is positive
Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med. 1999 Oct 5;131(7):485-91
Berlin Questionnaire for Sleep Apnea CATEGORY 1
1. Do you snore?a. Yesb. No
c. Don’t knowIf you snore:2. Your snoring is:
a Slightly louder than breathing
4. Has your snoring ever bothered other people?
a. Yesb. Noc. Don’t Know
5. Has anyone noticed that you quitbreathing during your sleep?a. Slightly louder than breathing
b. As loud as talkingc. Louder than talkingd. Very loud – can be heard in adjacent rooms
3. How often do you snorea. Nearly every dayb. 3-4 times a weekc. 1-2 times a weekd. 1-2 times a monthe. Never or nearly never
g g y pa. Nearly every dayb. 3-4 times a weekc. 1-2 times a weekd. 1-2 times a monthe. Never or nearly never
Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med. 1999 Oct 5;131(7):485-91
Berlin Questionnaire for Sleep Apnea CATEGORY 2 and 3
6. How often do you feel tired or fatigued after your sleep?
a. Nearly every dayb. 3-4 times a weekc. 1-2 times a weekd. 1-2 times a monthe. Never or nearly never
7 During your waking time do you feel
8. Have you ever nodded off or fallen asleep while driving a vehicle?
a. Yesb. No
If yes:9. How often does this occur?
a. Nearly every dayb 3 4 ti k7. During your waking time, do you feel
tired, fatigued or not up to par?a. Nearly every dayb. 3-4 times a weekc. 1-2 times a weekd. 1-2 times a monthe. Never or nearly never
b. 3-4 times a weekc. 1-2 times a weekd. 1-2 times a monthe. Never or nearly never
CATEGORY 310. Do you have high blood pressure?
YesNoDon’t know
Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med. 1999 Oct 5;131(7):485-91

13
STOP Questionnaire for Obstructive Sleep Apnea
The STOP test consists of four questions plusHeight: _________ inches Weight: _________ lbs Age: _______ Male / Female Body Mass Index (BMI): _________ Collar size of shirt: S M L XL or _________ inches Neck Circumference: _________ cm
High risk of OSA: answering yes to two or more questions Low risk of OSA: answering yes to less than two questions
Chung, F., Yegneswaran, B., Liao, P., Chung, S., Vairavanathan, S., Islam, S., Khajehdehi, A., Shapiro C. (2008). STOP questionnaire. A tool to screen patients for obstructive sleep apnea. Anesthesiology, 108 (5), 812-21.
STOP Questionnaire for Obstructive Sleep Apnea
1. Snoring Do you snore loudly (louder than talking or loud enough to be heard through closed door)? Yes No 2. Tired Do you often feel tired, fatigued or sleepy y , g pyduring the day? Yes No 3. Observed Has anyone observed you stop breathing during your sleep? Yes No 4. Blood Pressure Do you have or are you being treated for high blood pressure? Yes No
Chung, F., Yegneswaran, B., Liao, P., Chung, S., Vairavanathan, S., Islam, S., Khajehdehi, A., Shapiro C. (2008). STOP questionnaire. A tool to screen patients for obstructive sleep apnea. Anesthesiology, 108 (5), 812-21.
Assessment TechniquesAdvantages and Disadvantages
Advantages Disadvantages
PSG -Most objective -$$$-Not a “complaint”
Wrist actigraphy -ObjectiveIn home environment
-$Less accurate for insomnia-In home environment -Less accurate for insomnia
patientsSleep diary -Minimize recall bias -Time consuming for patient
Questionnaires -Moderately objective -Recall bias-No differential diagnosis info.
Interview -Differential diagnosis-Clinician expertise
-Recall bias-Clinician bias
Jennifer L. Martin, PhD

14
When to refer to a Sleep Specialist?
When you have tried everything we are teaching you and your patient still has difficulty with sleep
When you suspect sleep apnea narcolepsy or REM When you suspect sleep apnea, narcolepsy or REM Behavior Disorder
Extra Slides
Describe your current sleep problems:_______________________When did this start?
Stressful events at that time?Any health changes at that time?
Insomnia Diagnostic Interview:History and Physical
Describe the course of your sleep problem: chronic or on/off?Did you sleep well prior to [above events]?Attempts to manage/deal with sleep problems:
Medications tried: (name, dose, frequency of use)Non-medication strategies tried:How well did they work?
Have you had an overnight sleep study?When?/Where?What were the results? Jennifer L. Martin, PhD

15
Do you work? If yes, what is your schedule? Night shifts?Does your work or daily activities impact your sleep scheduleAre there differences between weekends and weekdays?Is your sleep better/same/worse when away from home?
Sleep ScheduleB dti
Insomnia Diagnostic Interview:Current Sleep Schedule
BedtimeTime to fall asleep (sleep onset latency)Night awakenings (#, duration and cause)Morning wake time
Estimate the number of hours you sleep:On a "typical" nightOn a "good" nightHow much sleep is right for you?
What “predicts” a good/bad night of sleep?Jennifer L. Martin, PhD
Regular meal time? What time do you eat dinner?Do you eat a snack after dinner? What time? Do you drink
Coffee; how much:______________latest: ______________Tea (hot/iced); how much:________________ latest: ______S ft d i k h h l t t
Insomnia Diagnostic Interview:Sleep Related Habits (sleep hygiene)
Soft drinks; how much:_______________ latest:__________Eat chocolate; how much: ___________latest: ___________
Do you smoke? packs/day_____When did you start? How much alcohol do you drink? What time of day?Drugs_________________________� no � yes Exercise_________________________� no � yes
Type__________________________________________________how often____________________time of day_________________
Jennifer L. Martin, PhD
SLEEP ENVIRONMENTWhere do you sleep?
bed sofa/couch chair/recliner
th
Insomnia Diagnostic Interview:Sleep Environment (more Sleep Hygiene)
other____Do any of the following disrupt your sleep?
Uncomfortable bed?Temperature too hot or cold NoisesLight
Other sleep interruptions (e.g., children, bedpartner pets)
Jennifer L. Martin, PhD
16
Sleep ApneaSnoring - gasping choking - waking up with shortness of breathwitnessed apneas (someone saw you stop breathing in your sleep)nighttime sweating
i h d h
Insomnia Diagnostic Interview:Symptoms of Sleep Disorders
morning headaches dry mouth
Restless legs (creepy crawly): Is it worse in the evening and/or when trying to fall asleep?During the night do you kick your legs while asleep (usually witnessed)?
Non-REM parasomnias:Sleepwalking Sleeptalking Jennifer L. Martin, PhD
REM behavior disorders“acting out dreams”
Nightmareshow often?Wh did th t t?
Insomnia Diagnostic Interview:Symptoms of Sleep Disorders (con’t)
When did they start?_____
NarcolepsyIrresistible attacks of sleep that occur dailyFalling asleep and dreaming right awayDream-like hallucinations while falling asleep or waking upFeeling paralyzed just before falling asleep or right after waking upSudden weakness or loss of muscles tone during the day, often related to intense emotion or laughter (cataplexy)
Jennifer L. Martin, PhD
BEHAVIORS IN BED DURING THE NIGHTWhen you are awake at night,
How long do you stay awake in bed? ___________________________Do you think or worry?Do you:
eat in bed, what?
Insomnia Diagnostic Interview:Behaviors at night (in and out of bed)
, _______________________________________________work/other tasks in bed? _________________________________________watch TV in bed?_______________________________________________other activities in bed? ___________________________________________
When you awake at night do you GET OUT OF BED?Do you:
Watch TV ReadUse a computerDo housework Eat/drink (what___________________)
Jennifer L. Martin, PhD

17
Because of sleep problems do you experiencemood changes: - depressed - anxious - irritable -frustratedpoor concentration or memorysleepy or tiredfalling asleep during focused activityfalling asleep while driving THIS IS VERY IMPORTANT
Insomnia Diagnostic Interview:Impact of poor sleep on daytime functioning
g p gfalling asleep during sedentary activitylow energytrouble with work or schoolphysical symptomsworrying about sleep during the day
Does your functioning improve when you are sleeping better?
Jennifer L. Martin, PhD
Do you take "planned naps"; that is, fall asleep on purpose during the day or evening?
Time of day: _________________________________________Where nap:__________________________________________length of nap: ________________________________________h ft
Insomnia Diagnostic Interview:Daytime napping/dozing
how often: __________________________________________
Do you doze off or fall asleep without meaning to during the day or in the evening?
Time of day: _________________________________________Where nap:__________________________________________length of nap: ________________________________________how often: __________________________________________
Jennifer L. Martin, PhD
Some psychiatric problems can impact sleep. Have you been diagnosed with:
Insomnia Diagnostic Interview:Sleep-specific psychiatric history
Currently symptomatic? Currently being treated?DepressionBipolar Disorder
Do your sleep problems changes when your psychiatric symptoms change (e.g., sleep gets worse when depression gets worse?)
Psychosis or schizophreniaPTSDAlcohol or drug abuse Years sober:_____
Jennifer L. Martin, PhD

18
Some medical problems can impact sleep. Have you had/do you have:
Insomnia Diagnostic Interview:Sleep-specific medical history
Head injury When?Did you lose consciousness?
Memory problems or dementia When diagnosed?Stroke When?Hypertension Are you taking medications?Chronic pain Cause
Does it impact sleep?How many times to you get up and use the bathroom at night?
Diagnosed with BPH?Prostate cancer?
Other medical issues that impact sleep?
Jennifer L. Martin, PhD
Do you have a family history of sleep problems?InsomniaSleep apneaVery early or very late sleep schedulesOther
Insomnia Diagnostic Interview:Family history/genetic risk
Jennifer L. Martin, PhD

4/9/2012
1
Pharmacological TreatmentsSonia Ancoli-Israel, PhD
Professor of PsychiatryDirector, Gillin Sleep and Chronomedicine Research Center
Di t f Ed ti UCSD Sl M di i C tDirector of Education, UCSD Sleep Medicine CenterDeputy Director, Stein Institute for Research on Aging
University of California San Diego
Diplomate, American Board of Sleep MedicineCertified, Behavioral Sleep Medicine
Antihistamines (H1 Receptor Antagonists)
AdvantagesLow costOTC
Disadvantages
Adverse effects:Adverse effects:dry mouth, blurred vision, urinary retention, constipationi k f i d i t l Efficacy not consistent
Rapid development of tolerance to sedative effectsPotential for residual effectsNo well-defined effective dosePoorly defined half-life
Mendelson WB. In: Sleep Disorders: Diagnosis and Treatment. 1998:137-160.; Kupfer DJ, Reynolds CF III. N Engl J Med.1997;336:341-346.; Richardson, G. et al. 2002. J Clin Psychopharmacol. 22, 511-515.
risk of increased intraocular pressure in individuals with narrow angle glaucoma. residual daytime sedation, diminished cognitive function, delirium (particular concern in the elderly)
Diphenhydramine (25-50mg) Use in Hospitalized Elderly
Delirium symptomsInattentionDisorganized speechAl d i
Indication for sleep: 68%Altered consciousnessAbnormal psychomotor activityAltered sleep/wake cycle (inc awakenings and naps)Behavioral disturbance
Agostini et al, Arch Intern Med, 2001, 161:2091-97
Agostini et al, Arch Intern Med, 2001, 161:2091-97.

4/9/2012
2
Antihistamines (H1 Receptor Antagonists)
Antihistamines (H1 receptor antagonists, such as diphenhydramine) are the most commonly used OTC treatments for chronic insomnia used OTC treatments for chronic insomnia,
there is no systematic evidence for efficacy
significant concerns about risks of these medications.
NIH State of the Science Conference Statement Manifestations and Management of Chronic Insomnia in Adults. Sleep 28(9): 1049-1057, 2005
Sedating AntidepressantsAdvantages
Potentially advantageous for patients experiencing chronic insomnia secondary to depression
DisadvantagesDisadvantages
Efficacy not consistent
Poor side effect profile, including cardiovascular effects and residual effects
No well-defined effective doseNational Center on Sleep Disorders Research. Sleep. 1999;22(suppl 2):S402-S408.; National Sleep Foundation. Treating Insomnia in the Primary Care Setting [monograph].2000; Jancin B. Clin Psych News. April, 2000:28.
Approved for use as an antidepressant6.4-hour t1/2 in adults, 11.6-hour t1/2 in elderly people
Popularity may be related to perceived safety, generic availability, unscheduled status and lack of restrictions on
Trazodone
y,prescription durationInsomnia trials are usually small (<30 patients), short (≤3 weeks), conducted in patients with comorbid depression or SSRI-induced insomnia, and rely on subjective measurements
Mendelson WB (2005), J Clin Psychiatry 66(4):469-476
4/9/2012
3
Anti-depressants - TrazodoneBased on recent surveys, the antidepressant trazodone is now the most commonly prescribed medication for the treatment of insomnia in the United States. In short-term use, trazodone is sedating and improves several sleep parameters. These initial effects may not last beyond 2 weeks. However, there are no studies of long-term use of trazodone for treatment of insomnia.
NIH State of the Science Conference Statement Manifestations and Management of Chronic Insomnia in Adults. Sleep 28(9): 1049-1057, 2005
Anti-depressants
Data on other antidepressants (e.g., amitriptyline and mirtazepine) in individuals with chronic insomnia are lacking. All antidepressants have potentially significant adverse All antidepressants have potentially significant adverse effects, raising concerns about the risk–benefit ratio.
NIH State of the Science Conference Statement Manifestations and Management of Chronic Insomnia in Adults. Sleep 28(9): 1049-1057, 2005
Other Sedating Medications
A number of other sedating medications have been used in the treatment of insomnia.
barbiturates (e.g., phenobarbital) antipsychotics (e g quetiapine and olanzepine) antipsychotics (e.g., quetiapine and olanzepine).
Studies demonstrating the usefulness of these medications for either short- or long-term management of insomnia are lacking. Furthermore, all of these agents have significant risks, and thus their use in the treatment of chronic insomnia cannot be recommended.
NIH State of the Science Conference Statement Manifestations and Management of Chronic Insomnia in Adults. Sleep 28(9): 1049-1057, 2005

4/9/2012
4
Major Conclusions from the NIH State-of-the-Science Insomnia Conference 2005
Antihistamines (H1 receptor antagonists)no systematic evidence for efficacy significant concerns about risks
All antidepressants have potentially significant adverse All antidepressants have potentially significant adverse effects, raising concerns about the risk–benefit ratio. Barbiturates and antipsychotics have significant risks, and thus their use in the treatment of chronic insomnia cannot be recommended.
NIH State of the Science Conference Statement Manifestations and Management of Chronic Insomnia in Adults. Sleep 28(9): 1049-1057, 2005
Pharmacological TreatmentThere are currently >14 medications approved by the FDA for treatment of insomnia.
benzodiazepines e.g., estazolam, flurazepam, quazepam, temazepam, and triazolam triazolam
nonbenzodiazepine (BzRAs)e.g., eszopiclone, zaleplon, zolpidem, zolpidem MR, other variations of zolpidem (sublingual; sublingual low dose, oral spray)
Melatonin receptor agonistramelteon
Low dose doxepin
Pharmacokinetics of Approved Agents for InsomniaGeneric Agent (Trade name) Older Benzodiazepines
Recommended Dose (mg) Half-life Range
(h)
Flurazepam HCL 15 or 30 47-100*Quazepam (Doral) 7.5 or 15 39-73*
Estazolam (ProSom) 0.5, 1 or 2 10-24
Temazepam (Restoril) 7.5, 15 or 30 3.5-18.4
*Includes active metabolite(s)
Consensus Conference. JAMA. 1984;251:2410-2414.; Physicians’ Desk Reference. 1991, 1999 and 2004. FDA Web site. Eszopiclone. www.fda.gov/cder/foi/label/2004/021476lbl.pdf. Accessed 1/25/05.
Triazolam (Halcion) 0.125 or 0.25 1.5-5.5
Newer Nonbenzodiazepines
Eszopiclone (Lunesta) 1, 2, or 3 6.0Zolpidem (Ambien) 5 or 10 1.4-4.5Zolpidem MR (Ambien CR) 6.25 or 12.5 2.8-2.9Zaleplon (Sonata) 5, 10 or 20 1.0Melatonin Receptor AgonistsRamelteon (Rozerem) 8 2-5HistamineDoxepin (Silenor) 3,6

4/9/2012
5
Newest forms of ZolpidemAll approved for short term use
Zolpimist Oral sprayEach metered actuation delivers 5 mg of zolpidem tartrate in 100 μL. Because it works rapidly (within 15 min), needs to be taken immediately at bedtime
Edluar bli l t bl t di l d t ith t tsublingual tablet - dissolves undertongue without water
5 mg and 10 mg strength Intermezzo
Approved for middle of the night usesublingual tablet - dissolves undertongue without water1.75 mg and 3.5 mg
BzRAs - Conclusions from the NIH State-of-the-Science Insomnia Conference 2005Results from clinical trials indicate that these agents are efficacious in the short-term management of insomnia The frequency and severity of these adverse effects are much lower in the newer benzodiazepine receptor agonists
most likely because these agents have shorter half livesmost likely because these agents have shorter half-lives.Although the available literature suggests that, in the short term, tolerance and abuse of the benzodiazepine receptor agonists are not major problems in the general population with chronic insomnia, long-term use needs further study.
NIH State of the Science Conference Statement Manifestations and Management of Chronic Insomnia in Adults. Sleep 28(9): 1049-1057, 2005
Choosing A Pharmacologic Therapy
Do you have difficulty initiating or maintaining sleep (or both)?How many hours can you devote to sleep or inactivity, after taking the
medication?
Agent Initiates Sleep
Maintains Sleep
Sleep with limited opportunity
Required Inactivity
Eszopiclone (Lunesta) √ √ 8+ hoursEszopiclone (Lunesta) √ √ 8+ hoursZaleplon (Sonata) √ √ 4 hoursZolpidem (Ambien) √ 7-8 hoursZolpidem MR (Ambien CR) √ √ 7-8 hoursZolpidem sublingual (Edluar) √ 7-8 hoursZolpidem oral spray (Zolpimist) √ 7-8 hoursZolpidem sublinqual (Intermezzo) √ √ 4 hoursRamelteon (Rozerem) √ -Doxepin (Silenor) √ -

4/9/2012
6
Pharmacology SummaryOver the counter (OTC) sleep agents lack safety and efficacy data supporting their use in chronic insomnia - risks outweigh the benefits.1
Few data support use of sedating antidepressants in insomnia not associated with depression. Side-effect profile worse than indicated agents1
Short intermediate and long-acting benzodiazepines are efficacious Short, intermediate and long acting benzodiazepines are efficacious, but safety and adverse event profile worse than newer agents.1
Short-acting nonbenzodiazepine hypnotics are effective in initiating sleep and/or maintaining sleep and have superior safety/AE profile to older agents. 1
Melatonin agonists have new mechanism of action, and appear to be effective.
1. NIH State of the Science Conference Statement Manifestations and Management of Chronic Insomnia in Adults. Sleep 28(9): 1049-1057, 2005
Head-to-Head comparisons and combined treatments
ore
24 –
22 –
20 –
18
CBT
temazepam
Combined*
Placebo
Cognitive Behavioral Therapy vs Pharmacotherapy for Insomnia in Older Adults
#
Tota
l Sco
Assessment
Pretreatment Post-treatment
3-month follow-up
12-month follow-up
24-month follow-up
18 –
16 –
14 –
12 –
10 –
acebo
*CBT+temazepam
Morin CM, Colecchi C, Stone J, Sood R, Brink D. JAMA. 1999;281:991-999.
#
#
#
#
##
#
# Significantly better than placebo at time point

4/9/2012
7
CBT and Pharmacological Therapy (PCT) for insomniaSleep onset latency (diary)
7080
in)
PCT (zolpidem; n=15) CBT (n=15)PCT + CBT (n=18) Placebo (n=15)
203040506070
pre-tx mid-tx post-tx 1-mo 3-mo 6-mo 12-mo
Slee
p la
tenc
y (m
Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Arch Intern Med. 2004;164:1888-1896.
CBT and Pharmacological Therapy vs. Combined Therapy
CBT aloneGreatest improvements in sleep-onset latency & sleep efficiencyMost “normal” sleepers post-treatmentTherapeutic gains maintained for 1 year
Combination therapy Similar to CBT alone
Zolpidem Initial improvements in sleep Return to near-baseline sleep at the end of treatment
Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Arch Intern Med. 2004;164:1888-1896.
CBT and Pharmacological Therapy for insomniaPolysomnography data
120
140
160
180
me
(min
)
20
40
60
80
100
pre-tx post-tx 6-mo
Tota
l wak
e tim
CBT (n=18 zopiclone (n=16) placebo (n=12)
Siversten et al. 2006. JAMA.
4/9/2012
8
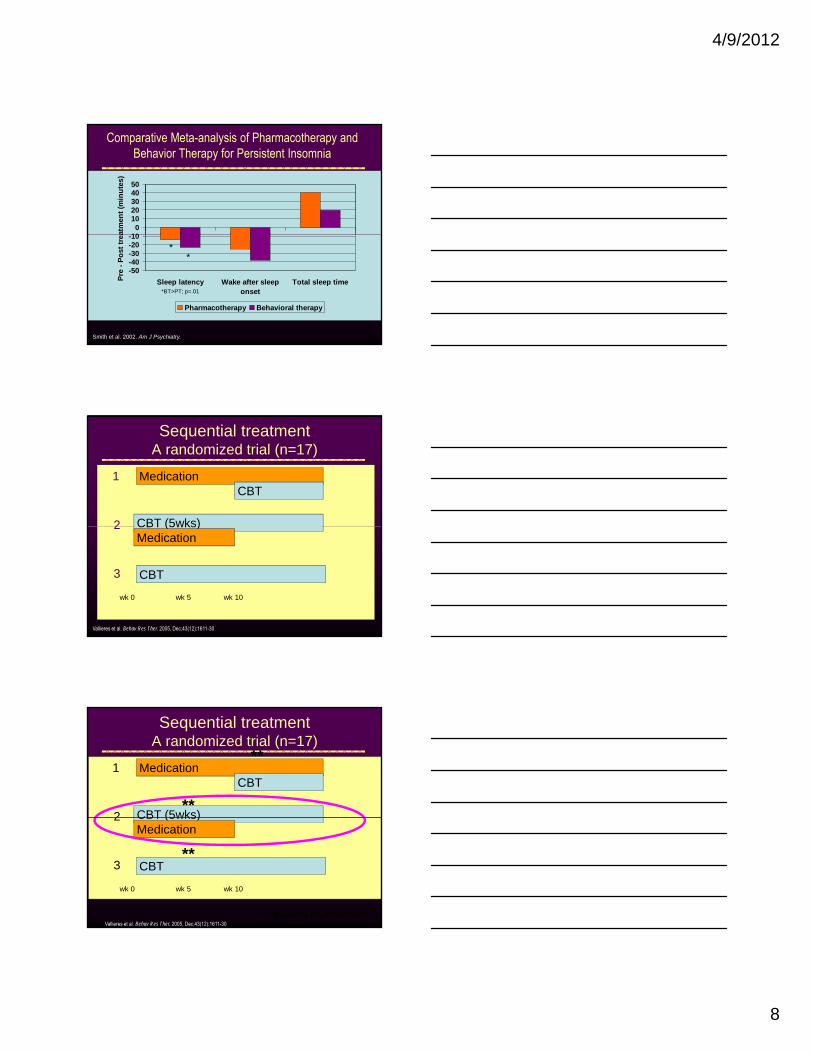
Comparative Meta-analysis of Pharmacotherapy and Behavior Therapy for Persistent Insomnia
100
1020304050
atm
ent (
min
utes
)
-50-40-30-20-10
Sleep latency Wake after sleeponset
Total sleep timePre
- Pos
t tre
a
Pharmacotherapy Behavioral therapy
**
*BT>PT; p=.01
Smith et al. 2002. Am J Psychiatry.
Sequential treatmentA randomized trial (n=17)
1
2
MedicationCBT
CBT (5wks)2
3
CBT (5wks)
CBT
Medication
wk 0 wk 5 wk 10
Vallieres et al. Behav Res Ther. 2005, Dec;43(12):1611-30
Sequential treatmentA randomized trial (n=17)
1
2
MedicationCBT
CBT (5wks)
**
**2
3
CBT (5wks)
CBT
Medication
wk 0 wk 5 wk 10
Vallieres et al. Behav Res Ther. 2005, Dec;43(12):1611-30**greatest improvement
**

4/9/2012
9
Sequential treatmentA randomized trial (n=17)
Each treatment sequence produced significant sleep improvements, but at different points in time. For the first sequence, most of the sleep improvement was obtained after the introduction of CBTF th th d CBT l i t
**
**For the other sequence and CBT alone, improvement appeared during the first weeks. These results suggest that sleep improvement seems affected by the way treatments are combined. A sequence beginning with a combined treatment followed by CBT alone seems to produce the best outcome.
Vallieres et al. Behav Res Ther. 2005, Dec;43(12):1611-30**greatest improvement
**
Treating insomnia requires a comprehensive clinical approach…
Managing insomnia requires a multifactorial approachTreatments should be individualized, considering:
A comprehensive clinical approach
considering:Functional consequences of insomniaTreatable underlying conditionsRisk/benefit ratio of treatmentPatient preferences
Winkelman JW. A Primary Care Approach to Insomnia Management.Available at: www.medscape.com/viewprogram/3807_pnt. Accessed: January 8, 2006.

4/9/2012
10
A comprehensive clinical approachFirst-line therapies should be
Non-pharmacological interventions, especially multicomponent CBTsNewer hypnotics
Nonpharmacological interventionsNonpharmacological interventionsDemonstrated efficacy and effectivenessDifficult to access
Pharmacological interventions“Safer than they used to be”Highly effective for short-term useMay be appropriate for long-term use in some patients

Getting started
Jennifer L. Martin, PhD CBSMAdjunct Assistant Professor
David Geffen School of MedicineUniversity of California, Los Angeles
Career Research Scientist and PsychologistVA Greater Los Angeles Health Care System
Certified, Behavioral Sleep Medicine
Getting Started
Is CBT-I recommended and is it effective?
Who should NOT get CBT-I?
Teaching CBT-I to your patient sleep educationIntroducing the treatment approach
Jennifer L. Martin, PhD
Clinical Guidelines for Chronic Insomnia
Psychological and behavioral interventions are effective and recommended in the treatment of chronic primary and co-morbid insomnia.These treatments are effective for adults of all agesThese treatments should be utilized as an initial intervention when appropriate and conditions permit.
Schutte-Rodin, et al. Clinical guideline for the evaluation and mangagment of chronic insomnia in the adult. JCSD 2008; 4(5):487-504

AASM1 APA2
Sleep Hygiene No rec. Not EST
Cognitive therapy No rec. Not EST
EMG Biofeedback Guideline EST (modest)
Paradoxical intention Guideline EST (strong)
Sleep restriction Guideline EST (strong)
Stimulus Control Standard EST (strong)
Relaxation therapies Standard EST (strong)
CBT-I (with or without relaxation therapy)
Standard EST (strong)
AASM=American Academy of Sleep MedicineAPA=American Psychological Association; EST=empirically supported therapy (level of research support)
1. Morgenthaler et al, Sleep. 29 (11), 2006. 2. http://psychology.sunysb.edu/eklonsky-/division12/treatments/insomnia_cognitive.html. accessed 4/17/09.
Practice Parameters for Behavioral Treatment of Insomnia(AASM 2006)
For the treatment of chronic insomnia:Stimulus control therapy is effective and recommendedRelaxation training is effective and recommendedSleep restriction is effective and recommended CBT, with or without relaxation, is effective and recommendedMulticomponent therapy (with or w/o cognitive therapy) is effective
and recommendedParadoxical intention is effective and recommendedBiofeedback is effective and recommended
Insufficient evidence for sleep hygiene education as a single therapy
Morgenthaler et al. Sleep, 2006; 29(11)1415-1419
Mean Effect Sizes for Psychological / Behavioral Treatment of Insomnia
Effe
ct s
ize Large
Medium
Small
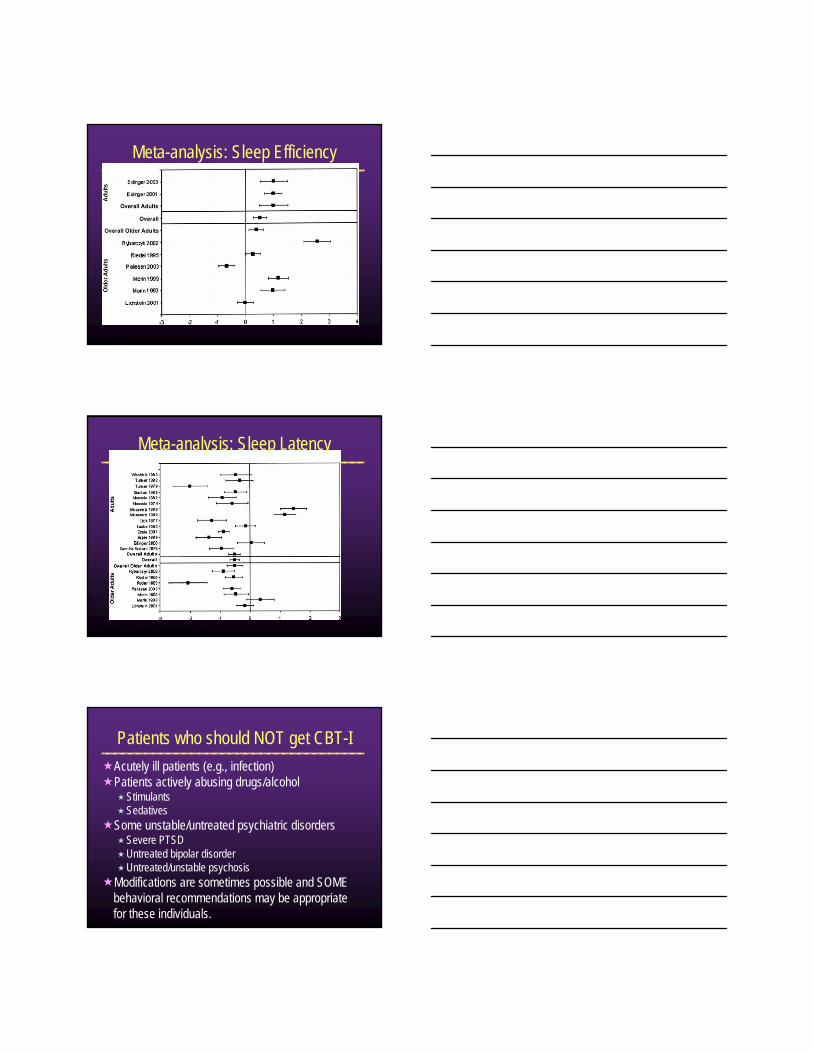
Meta-analysis: Sleep Efficiency
Irwin et al. Health Psychology, 2006.
Irwin et al. Health Psychology, 2006.
Meta-analysis: Sleep Latency
Acutely ill patients (e.g., infection)Patients actively abusing drugs/alcohol
StimulantsSedatives
Some unstable/untreated psychiatric disordersSevere PTSDUntreated bipolar disorderUntreated/unstable psychosis
Modifications are sometimes possible and SOME behavioral recommendations may be appropriate for these individuals.
Patients who should NOT get CBT-I
Jennifer L. Martin, PhD

Patients with insomnia problems For more than 1 monthThat impacts functioning or causes worry/distress
Patients who are interested in an approach other than medications
Patients may be using sleeping pills and still get CBT-IPatients with comorbid conditions that may be exacerbated by poor sleep (which is almost everything, it turns out)
Patients who should get CBT-I
Jennifer L. Martin, PhD
Sample CBT-I treatment plan (weekly or bi-weekly sessions)
Clinical evaluation
Assign sleep diary
Session 1 Sleep education, stimulus control, sleep restriction
Session 2 Titrate TIB, sleep hygiene education
Session 3 Titrate TIB, relaxation training (optional)Session 4 Titrate TIB, cognitive therapy
Session 5 Titrate TIB, relapse prevention, long-term habits
Follow-up Optional: follow-up after 2-3 months, problem solving, referrals for additional treatment
Jennifer L. Martin, PhD
Sleep diary
As with many behavioral treatments, patient “buy-in” is requiredSome recommendations are counter-intuitive.
Patient will be asked to do the OPPOSITE of what he has been doing so far to cope with his insomnia
Education lays the groundwork for relapse prevention after treatment endsThis part is “more sales than psychology,” and personal style comes in to play
Sleep Education: Laying the goundwork
Jennifer L. Martin, PhD

DO NOT assume that your patient has accurate information about sleep! The internet is full of erroneous claims and misinformation…DO NOT skip sleep education to save time – you will regret it later
Simplify or elaborate on a case-by-case basis
Sleep Education: Laying the groundwork
2-process model of sleep regulationHomeostatic processCircadian process
A model for how insomnia develops3 P’s model (or expansion of that model)
Introducing CBT-IRecommendations are based on how sleep works and how insomnia develops
Sleep Education
Jennifer L. Martin, PhD
Homeostasis – “Sleep Drive”

Circadian Rhythms – “Biological Clock”
Sleep-Wake CycleCircadian and Homeostatic Regulation of Sleep
Wake
Sleep
Wake Propensity
9 am 3 pm 9 pm 3 am 9 amAsleepAwake
Melatonin
Sleep Drive
Circadian Alerting
Signal
Adapted from Kilduff TS, Kushida CA. Circadian regulation of sleep. In: Chokroverty S, ed. Sleep Disorders Medicine: Basic Science, Technical Considerations, and Clinical Aspects. 2nd ed. Boston, Mass: Butterworth-Heineman; 1999. [Evidence Level C]. Kennaway DJ, Voultsios A. J Clin Endocrinol Metab. 1998;83:1013-1015. [Evidence Level C]
2-process model of sleep regulationHomeostatic processCircadian process
A model for how insomnia develops3 P’s model (or expansion of that model)
Introducing CBT-IRecommendations are based on how sleep works and how insomnia develops
Sleep Education
Jennifer L. Martin, PhD

A Model of Insomnia
Threshold
Spielman, Glovinsky. The varied nature of insomnia. In: Hauri P, ed. Case studies in insomnia. New York: Plenum Press; 1991:1‐15.
The 3 P’s spelled out…Predisposing Precipitating Perpetuating
“Risk factors” “Big events” Why you STILL can’t sleep…
•Genetics•Early learning•Chronic conditions•Depressive disorders
•Marriage (or divorce)•Job loss (or new job)•Birth (or death)•Illness•Relocation•Depressive episode
•Going to bed early•Getting up late•Taking naps•Canceling things because of insomnia•Worrying about your sleep problems!
Cognitive-Behavioral Therapy
A Model of Insomnia
Threshold
Spielman, Glovinsky. The varied nature of insomnia. In: Hauri P, ed. Case studies in insomnia. New York: Plenum Press; 1991:1‐15.
Cognitive-Behavioral Therapy

2-process model of sleep regulationHomeostatic processCircadian process
A model for how insomnia develops3 P’s model (or expansion of that model)
Introducing CBT-IRecommendations are based on how sleep works and how insomnia develops
Sleep Education
Jennifer L. Martin, PhD
Start to introduce the concepts of sleep restriction / stimulus control
In the “best case”, the patient will start telling you what she needs to do…
“So…maybe I’m just spending too long in bed…”“Worrying about this insomnia thing is just making it worse, then…”
You can ask, “Does what I just described make sense to you?”
Start to introduce the concepts of sleep restriction / stimulus control
Remember what you learned from your evaluation and tailor the next part to the individual patient
For example…Patient takes a nap on weekends to make up for lost sleepOn weeknights, he goes to bed very early to “try to get enough sleep to get through the next day.”

Homeostasis – “Sleep Drive”
Nap
Homeostasis – “Sleep Drive”Going to bed early
Circadian Rhythms – “Biological Clock”
Going to bed early

Sleep restriction
The BEST way to synchronize these two forces is to get out of bed at the same time every dayget out of bed at the same time every day
Get into bed when…Sleep drive is highThe circadian alerting signal is low (i.e., your clock is telling you it’s time to sleep)i.e., you are SLEEPY!
Then wait for sleep to unfold…
Stimulus control
Trying to sleep makes sleep impossibleDON’T think about a white bear!
The more you try, the harder it is
Stimulus Control• If you have been spending a lot of time awake in bed
TRYING to sleep…• You probably associate your bed with exactly that…• Changing that association will take practice…

Reviewing the patient’s sleep diary
Calculate the averages:Time in bed = bedtime to get-up timeTotal time awake = time to fall asleep + time awake at night + early morning awakeningsTotal sleep time = time in bed – total time awakeSleep Efficiency = Total sleep time / Time in bed
The sleep diary
Similar to checking blood pressure…Identify high blood pressure…Start medication, make lifestyle changes…Re-check blood pressure…Adjust if needed…Until blood pressure is normal

Send the patient home with a new sleep diary“More art than science.”Complete the diary IN THE MORNING about the night before.DO NOT complete the sleep diary in the middle of the night.
Sleep Diary

4/9/2012
1
Cognitive-Behavioral Treatment of Chronic Insomnia:
Sleep Restriction and Stimulus ControlSonia Ancoli-Israel, PhD
Professor of PsychiatryProfessor of PsychiatryDirector, Gillin Sleep and Chronomedicine Research Center
Director of Education, UCSD Sleep Medicine CenterDeputy Director, Stein Institute for Research on Aging
University of California San Diego
Diplomate, American Board of Sleep MedicineCertified, Behavioral Sleep Medicine
Fill Out Sleep Diaries
Consensus Sleep Diary
Carney CE; Buysse DJ; Ancoli-Israel S; Edinger JD; Krystal AD; Lichstein KL; Morin CM. The consensus sleep diary: standardizing prospective sleep self-monitoring. SLEEP 2012;35(2):287-302.

4/9/2012
2
Sleep RestrictionImprove sleep continuity by limiting time spent in bed to match time asleep
Total sleep time determined from sleep diaries
Useful for both sleep onset and sleep maintenance problems
Spielman AJ, Saskin P, Thorpy MJ. Sleep. 1987;10:45-56.Morin CM. J Clin Psychiatry. 2004;65(suppl 16):33-40.
IT’S ALL ABOUT SLEEP EFFICIENCYNormal sleep efficiency is 90-95% in adult populationsAverage sleep efficiency seen in sleep clinics: 70% No one ever sleeps 100% of the time
Time in Bed (Sleep Restriction)
No one ever sleeps 100% of the timeGoal is 85%+
Jennifer L. Martin, PhD
Calculate sleep efficiency (from sleep diary):Time asleep / Time in bedTime asleep = time in bed – (time to fall asleep + time awake at night)
Titrate Time in Bed (Sleep Restriction)
awake at night)
Jennifer L. Martin, PhD

4/9/2012
3
Sleep-Restriction Therapy RulesCut bedtime to actual amount patient reports sleeping (plus 15 minutes), but not <4 hours/night
Prohibit sleep outside of these hours
Have patient report daily the amount of sleep obtained
Compute sleep efficiency (SE); based on moving average of 5 nights
when SE is >85%, increase bedtime by 15 minutes
With the elderly, SE cutoff is 80%. Allow a 30-minute napSpielman, Saskin & Thorpy, Sleep. 1987;10:45-56; Morin CM. J Clin Psychiatry. 2004;65(suppl 16):33-40..Spielman, Saskin & Thorpy, Sleep. 1987;10:45-56; Morin CM. J Clin Psychiatry. 2004;65(suppl 16):33-40..
Sleep Restriction
Anchor sleep schedule to wake timeKeep rigid bed and rise times
Review strategies for staying awakeSleep will probably be less before it is moreGoal is to consolidate sleep
Sleep deprivation will actually help
IT’S ALL ABOUT SLEEP EFFICIENCYSleep efficiency <85%, TIB by 15 minutes
Titrate Time in Bed (Sleep Restriction)
Sleep efficiency >90%, TIB by 15 minutesOtherwise, keep TIB the same for another week
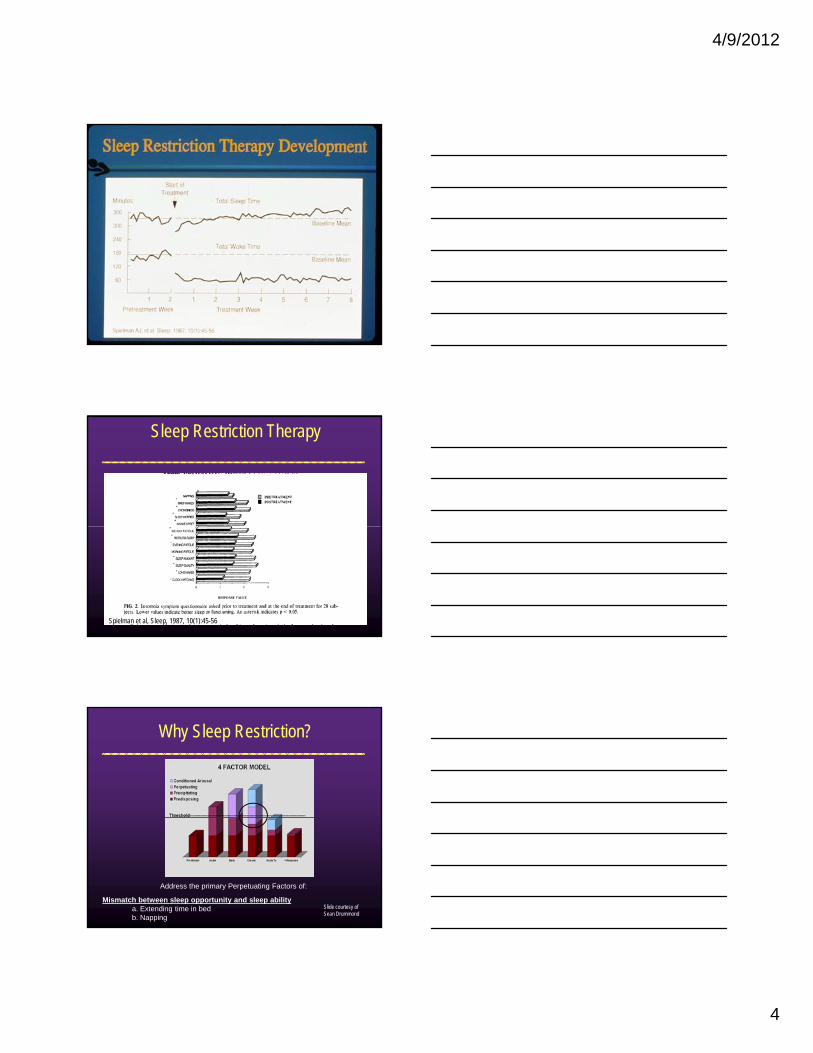
4/9/2012
4
Sleep Restriction Therapy
Spielman et al, Sleep, 1987, 10(1):45-56
Why Sleep Restriction?
Address the primary Perpetuating Factors of:
Mismatch between sleep opportunity and sleep abilitya. Extending time in bedb. Napping
Slide courtesy of Sean Drummond

4/9/2012
5
Sleep Restriction: Mr. M
Initial sleep diary (mean over 2 weeks)Bedtime: 9:30 PMMorning rise time: 7:00 AMTotal time in bed: 9.5 hoursT t l l ti 6 5 hTotal sleep time: 6.5 hoursSleep efficiency: 68%
Initial “restricted” scheduleDesired morning rise time: 6:30 AMBedtime: 12:00 AMNo daytime napping or sleeping outside of this time period
Jennifer L. Martin, PhD
Sleep Restriction: Mr. M (cont’d)
When sleep efficiency is >85% (or 80% in older persons), increase sleep period by 15 minutesInitial “restricted” schedule (Week 1)
“In bed”: 12:00 AM to 6:30 AM
Total sleep time : 6 hoursSleep efficiency: 92%
Modified schedule (Week 2)“In bed”: 11:45 AM to 6:30 AM
Extend by 15 minutes every 4 to 7 days until sleep efficiency is at desired level or sleep is satisfactory
Jennifer L. Martin, PhD
Sleep restriction: Mr. M12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11
Initial TIB: 9.5 hours
Final TIB: 7.5 hours
Jennifer L. Martin, PhD

4/9/2012
6
Sleep Restriction: Mr. M
{{
Jennifer L. Martin, PhD
Sleep Restriction: Mr. M
Jennifer L. Martin, PhD
Stimulus ControlConsidered one of the most effective behavioral treatmentsBased on the behavioral principle of classical conditioningclassical conditioning
Insomnia leads to stress, anxiety, wakefulnessThis takes place in bedin bedThe bedbed becomes associated with stress anxiety The bedbed becomes associated with stress, anxiety, wakefulness
Chesson AL, Anderson WM, Littner M, et al. AASM standards of practice committee. Sleep. 1999;22:1-6.
=Worry…Wakefulness…Waiting…

4/9/2012
7
Stimulus Control (cont’d)
Treatment involves changing the association:
≠Worry…Wakefulness…Waiting…
If you’re not asleep, get out of bedOver one or more nights, sleep drive increases, and sleep onset occurs more quickly. Over multiple trials, the bed is again associated with rapid sleep onset.
Chesson Jr, AL, Anderson WM, Littner M, et al. AASM standards of practice committee. Sleep. 1999;22:1-6.
= A “cue” for falling A “cue” for falling asleep fast…asleep fast…
Stimulus Control: Typical Instructions
Fixed morning rise time, 7 days a week, regardless of how much sleep during the nightThe bed is only for sleep (and sex)Sleep only in bed (no couch napping)Go to bed only when sleepyLeave the bedroom if awake for > about 20 minutes
no clock watchingReturn to bed only when sleepyDo not nap during the day
Chesson Jr, AL, Anderson WM, Littner M, et al. AASM standards of practice committee. Sleep. 1999;22:1-6.
READ IN BED
WATCH TV IN BED
EAT IN BED
GOOD STIMULUS CONTROL STIMULUS DYSCONTROL
ODDS 1 IN 2 ODDS 1 IN 8
Stimulus Control
BEDROOM BEDTIME
SEX BEDROOM BEDTIME
SLEEP
SEX
SLEEP
WATCH TV IN BED
WORK IN BED
WORRY IN BED
CLEAN BDRM Slide courtesy of Sean Drummod

4/9/2012
8
Assume you will be up all nightThis helps reduce anxiety about not sleeping
Partake in quiet and sedentary activitiesDo not cook a full meal for the next day!
Stimulus Control:What to do when you get up?
yDo not do something where you lose track of time
Go back to bed when you cannot stay up any longerDon’t get too comfortable
You only want to sleep in bedDo not give yourself too much light
Why Stimulus Control?
Address the primary Perpetuating Factor of:
Poor Stimulus Control
Slide courtesy of Sean Drummond

4/9/2012
9
Send the patient home with a sleep diary“More art than science.”Complete the diary IN THE MORNING about the i ht b f
Sleep Diary
night before.DO NOT complete the sleep diary in the middle of the night.

Components of CBT-I:Sleep Hygiene Education and Relaxation Skills Training
Jennifer L. Martin, PhD CBSMAdjunct Assistant Professor
David Geffen School of MedicineUniversity of California, Los Angeles
Career Research Scientist and PsychologistVA Greater Los Angeles Health Care System
Certified, Behavioral Sleep Medicine
Sleep Hygiene is…
Education about behaviors, environmental conditions, and other factors that may interfere with sleep
Important to query as part of a sleep history to rule out specific behavioral or environmental causes of poor sleep and to identify issues to target during comprehensive treatment
Stepanski EJ, Wyatt JK. Sleep Medicine Reviews. 2003;7:215‐225.Hauri P. The sleep disorders. 2nd ed. Kalamazoo, Michigan: Upjohn Pharmaceuticals, 1977.
A hand-outEvidence-based careAn effective stand-alone treatment for insomnia
What sleep hygiene is NOT…
Jennifer L. Martin, PhD

Poor sleep hygiene
Too much time in bed or an irregular sleep scheduleExcessive nappingCaffeine, alcohol, nicotine that interferes with sleepExercise or mental stimulation near bedtimePoor sleep environment
Cut Down on Your Time in Bed Staying in bed longer than your body needs to sleep contributes to insomniaCutting down on time in bed (even by 30 minutes) can improve sleep qualityIn one study 90% of insomnia patients needed to curtail their time in bedMost patients cannot do this without specific guidance of CBT-I
Establish and keep a regular sleep schedule
A regular sleep schedule (get-up time especially) improves sleep quality
Structure daytime activities enough to support regular sleep habits
Exercise about 6 hours before bedtimeInsomnia patients have flatter temperature rhythms.Intense exercise increases body temperature, followed by a compensatory decrease which promotes sleep.Late afternoon/early evening exercise may be most helpful for sleep.
DO NOT exercise close to bed time to try to “wear yourself out”
When you wake up during the night...
What is the first thing you do?
What time do you wake up at night?

Avoid a Bedroom Clock
Set an alarm, then hide all time pieces (including your smart phone)
Do not “monitor the passage of time” until morning
You will sleep best away from any time pressures
Experiment with dark curtains, a steady noise or a change in room temperature. The ideal sleep environment is that which is most comfortable for the patient
Alcohol helps many people fall asleep, BUT it causes them to wake up more often during the night.
Alcohol should not be used to promote sleep

Nicotine and Sleep
Nicotine has a paradoxical effect It is both a relaxant and stimulant
Nicotine has a paradoxical effect – it is a stimulant and a relaxant
Smoking alleviates nicotine withdrawalSmoking is also stimulating
“Quitting” is best, but often not realistic Focus on eliminating nicotine near bedtime and at
night
Avoid (or limit) caffeine near bedtime
Caffeine Content (mg) in Coffee
Note: The listed caffeine content is average for a standard brewed cup of coffee; certain brewing methods may increase or decrease the average caffeine content per cup. Courtesy of NSF
Brewed, drip method 8 oz 85 mgCaffe Latte 6 oz 90 mgCaffe Mocha 6 oz 90 mgCappucino 6 oz 90 mgCappucino, decaf 8 oz 4 mgCoffee 8 oz 110 mgCoffee, decaf 8 oz 5 mgEspresso 1 oz 90 mgEspresso, decaf 1 oz 10 mgInstant coffee 8 oz 75 mg

Caffeine Content (mg) in 8 oz of Soda
Note: The listed caffeine content is average for a standard brewed cup of coffee; certain brewing methods may increase or decrease the average caffeine content per cup.
Courtesy of NSF
7-UP 0 Jolt 48
Caffeine free Coca Cola 15 Mello Yello 34
Caffeine free Diet Coke 15 Minute Maid Orange Soda 0
Coca Cola 23 Mountain Dew 37Diet 7-UP 23 Mr. Pibb 40Diet Coke 31 Mug Root Beer 0Diet Dr. Pepper 28 Pepsi 25Diet Mountain Dew 37 Pepsi ONE 37
Diet Pepsi 24 RC Cola 36Diet RC 36 Shasta Cola 45Diet Sprite 0 Sprite 0Dr. Pepper 28 Sunkist Orange Soda 28
Caffeine Content (mg) in 8 oz Tea
Courtesy of NSF
Arizona Black Iced Tea 16 mgArizona Green Iced Tea 7.5 mgBrewed, Imported Brands 60 mgBrewed, Major US Brands 40 mgIced 25 mgInstant 28 mgLipton Brisk Iced Tea 6 mgSnapple Iced Tea, all varieties 21 mg
Caffeine Content (mg) in Ice Cream
Courtesy of NSF
Cappuccino Chocolate Chunk 8 oz 8 mgCappuccino Mocha Fudge 8 oz 8 mgCoffee 8 oz 40-60mgCoffee Fudge, Low Fat 8 oz 30 mgCoffee Frozen Yogurt, Fat Free 8 oz 40 mgFrappuccino Bar (one bar) 2.5 oz 15 mgNo Fat Coffee Fudge Frozen Yogurt 8 oz 85 mg

Caffeine Content (mg) in 1 Tablet OTC
Note: The listed caffeine content is average for a standard brewed cup of coffee; certain brewing methods may increase or decrease the average caffeine content per cup.
Courtesy of NSF
Anacin 13 Mello Yello 100
Cafergot 100 Minute Maid Orange Soda 15
Caffedrine 100 No Doz max; Vivarin 200Coryban D 30 No Doz reg strength 100Darvon Compound 32 Percodan 32Dexatrim 200 Permathene Water Off 10Dristan 30 Pre Mens Forte 100
Excedrin max strength 65 Prolamine 50Fiorinal 40 Triaminicin 140Midol 32 Vanquish 30
Caffeine Content (mg)
Courtesy of NSF
Coffee 8 oz 110 Snapple Iced Tea
8 oz 21
Coffee, decaf 8 oz 5 Brewed Tea 8 oz 40-60
Cappuccino 6 oz 90 Mountain Dew 8 oz 37Cappuccino, decaf
8 oz 4 Coca Cola 8 oz 23
Espresso 1 oz 90 Shasta Cola 8 oz 45Espresso, decaf 1 oz 10 Excedrin max 1 tab 65Instant coffee 8 oz 75 Midol 1 tab 65
Coffee ice cream 8 oz 40-60 Midol 1 tab 32
Eat a Light Snack
A glass of milk, cheese and crackers or any other light snack may help insomnia patients stay asleep

Limit liquids near bedtime
Teaching Sleep Hygiene• In rare cases, a clear sleep hygiene issue arises
– “I’ll die before I give up my coffee. It’s all I drink!”• Patients with chronic insomnia often have poor sleep
hygiene– Correcting these problems is typically insufficient
• Effective sleep hygiene intervention:– Identify 1-2 issues that are particularly salient– Ask patient to maintain change for >2 weeks– Keep a diary to track progress– Follow-up to assess effectiveness
Jennifer L. Martin, PhD
Relaxation tools…

Relaxation…
Ask your patients what they do that is relaxing
If the answer is NOTHING, help them find something or teach them a new skill (exercises later)
If they have a strategy that they already use (yoga, listening to music…) Discuss incorporating that into a pre-bedtime routine
Relaxation Therapies• Progressive Muscle Relaxation (PMR)
– Most widely investigated treatment method for insomnia– Teaching the patient to recognize and release muscular
tension using a standardized training procedure and protocol• Biofeedback
– Using physiological measures to teach patients to relax – Once patient learns to relax, procedure is used at sleep onset
and/or during nighttime awakenings• Both PMR and biofeedback have been shown to help
insomnia in some individuals; however, techniques can be difficult for patients to learn and progress is slow
Morin CM, Hauri PJ, Espie CA, et al. Sleep. 1999;22:1-23.
Relaxation Therapies (cont’d)
Relaxation response must be “overlearned”Patients should practice relaxation skills daily for2 to 3 weeks before attempting them at bedtime
Recent studies show benefits of Tai Chi1 and Yoga2
on insomniaThese interventions may act through relaxation mechanisms (biological and psychological) and/or by increasing daytime physical activity
1. Li F, Fisher KJ, Harmer P, et al. J Am Geriatr Soc. 2004;52:892-900.2. Khalsa SB. Appl Psychophysiol Biofeedback. 2004;29:269-278.

Relaxation therapiesDemonstration: Autogenic Training
A relaxation technique similar to meditation. Through a series of self-statements about heaviness and warmth in different parts of the body, a positive effect is induced on the autonomic nervous system. A meta-analytic review in 2002 found positive effects of autogenic training across a range of diagnoses.
Stetter & Kupper , 2002
Relaxation therapiesDemonstration: Grounding
A mindful exercise focused on the bodyHelps the body connect to the Earth’s energyCan be very brief (1 minute) or longerExamples…
Walk barefoot. Attend to the contact of your foot to the ground.Hold a special object. Concentrate on how it feelsAdopt a seated grounded posture. Feet evenly on floor. Focus on Earth’s energy moving into your body.

Components of CBT-I:Cognitive therapy, Long-term sleep habits
Jennifer L. Martin, PhD CBSMAdjunct Assistant Professor
David Geffen School of MedicineUniversity of California, Los Angeles
Career Research Scientist and PsychologistVA Greater Los Angeles Health Care System
Certified, Behavioral Sleep Medicine
Cognitive Therapy for Insomnia
“So far, we have focused on what people DO that can make insomnia worse.”
Too much time in bedDoing things other than sleeping in bed
“Now we are going to talk about another piece of the puzzle, that is, what we THINK about that impacts our sleep.”
Attitudes and beliefs about sleepThoughts, worries, concerns at night
Cognitive therapy
Jennifer L. Martin, PhD

Session 3 4
Feelings
Thoughts
Behaviors
Cognitive Therapy
Challenge dysfunctional beliefs about sleep“I must sleep 8 hours”
Correct unrealistic expectations “I should never wake up at night”
Reconsider insomnia consequences “I can’t function without 8 hours of sleep”
Morin CM, Hauri PJ, Espie CA, et al. Sleep. 1999;22:1‐23.Morin CM. J Clin Psychiatry. 2004;65(suppl 16):33‐40.Morin CM. Insomnia: psychological assessment and management. NewYork: Guilford Press, 1993.
EXERCISE #1: WHY THOUGHTS MATTER

It was a dark and stormy night…
Session 3 7
Thinking About Sleep
Whether we are aware of it or not, we all think about why we can’t sleep (the causes of insomnia) and what will happen if we don’t sleep (the consequences of insomnia).
Both can keep us up at night.
Our thoughts can also affect our feelings and our behaviors.
Session 3 8
What keeps you up at night?
Ruminating about the past?Planning for the future?Problem-solving?Thinking about your health?Thinking about sleeping?Thinking about sounds you’re hearing around you?Thinking about thinking???
Session 3 9

The connection between thoughts and sleep
What we think about can affect sleep, whether we’re aware of it or not.
General thoughts and worries (non-sleep related)Unhelpful thoughts, beliefs, or attitudes about sleep
Unhelpful thoughts about sleep can cause frustration or anxiety. This can make it harder to fall asleep and harder to stay asleep, too.
Unhelpful thoughts can actually cause insomnia!
10Session 3
EXERCISE #2: THIS INSOMNIA WILL KILL ME…
Step 1: How long have you had insomnia:
Number of years ___________________________Nights with insomnia per week ________________Total nights w/ insomnia_____________________
(years X 52 weeks)
2,340 nights of insomnia2,340 nights of insomnia
Exercise: Catastrophizing about insomnia consequences
Jennifer L. Martin, PhD
10 years
4.5 x/week2,340 nights of insomnia

Discuss meaning of this number…Note (from your evaluation) what patient has said about potential consequences of insomniaRevisit those fearsHave they happened before? If so, how often?
Exercise: Catastrophizing about insomnia consequences
Jennifer L. Martin, PhD
I can’t go to work tomorrowI’ll screw something upI’ll lose my jobI’ll lose my houseMy family will be homeless
MY FAMILY WILL BE HOMELESS BECAUSE I CAN’T SLEEP!
Exercise: Catastrophizing about insomnia consequences
Jennifer L. Martin, PhD
This is really bad for my healthMy doctor told me sleep is really importantI read that if I don’t get at least 7 hours, I could dieI already had a heart attack. All this stress is going to give me another one
I AM GOING TO DIE BECAUSE I CAN’T SLEEP!
Exercise: Catastrophizing about insomnia consequences
Jennifer L. Martin, PhD

Identify a more helpful thoughtDoes it seem helpful to lie in bed and tell yourself your family will be homeless if you don’t get to sleep RIGHT NOW!!!???
Generate an alternative that is both true and helpful
Exercise: Catastrophizing about insomnia consequences
Jennifer L. Martin, PhD
A more helpful thought“I might not feel my best at work tomorrow, but I can get through the day. I’ve done it a thousand times before.”
Write it downSay it over and over againOut loud
Exercise: Catastrophizing about insomnia consequences
Jennifer L. Martin, PhD
EXERCISE #3: THINKING AND WORRYING IN BED

Insomnia patients often worry about things at nightFor some patients, this is the only quiet time they have to think about thingsFor some patients, the worries are magnified during sleepless nights…
We say, “Schedule some time with your thoughts.”
Exercise:Worry time (similar to CBT for GAD)
Jennifer L. Martin, PhD
Thinking TimePick a time and place that you do not associate with other activities. Make an appointment!
Use this time to address the thoughts that keep you up at night.
Put your day to rest – jot down what’s on your mind. Simply be more aware of your thoughts.Plan your next day or make a To Do list.Think of solutions to a problem or worry – What actions can you take now? Who or where can you turn to for help?
Be active in your thinking!20Session 3
Session 3 21
Thoughts NotebookMonday, January 20, 20118:00pm, Kitchen Table
I am not sure if I will have enough medication to last me through my entire trip when I go see my family next month.
Steps I can take:-Count how many pills I have left and figure out how many pills I will need while I am away-Call the pharmacy if I won’t have enough.-Ask the pharmacist to call my doctor if necessary.
•Write down the time and place for your Thinking Time.
•Record your thought or worry.
•Write down steps and ideas about how you will address your thought or worry.

Thoughts Outside Your Thinking Time
If thoughts come up outside of your thinking time (including while you are in bed), jot them down in your notebook and come back to them during your scheduled thinking time.
Attending to your thoughts or worries during the middle of the night won’t help you to solve your problems – let your mind sleep!
Session 3 22
SLEEPING WELL OVER THE LONG RUN…
Up to this point, sleep schedule has been rigid and regular In the long-term, bed times and wake up times can be a little more flexible
The exception is people with delayed sleep phase syndrome who will need to maintain a regular sleep schedule indefinitely.
Long-term habits
Jennifer L. Martin, PhD

Bedtime: Bedtime can range from 15 minutes before to 15 minutes after your current bedtime.
Wake up time: Wake up time can range from 15 minutes before to 15 minutes after.
Do this for 1 month…
Long-term habits
Jennifer L. Martin, PhD
If, after 1 month, you are still sleeping well, try taking a day off!
Stick with your sleep schedule for 6 out of 7 days. On the 7th day, do whatever you want! Go to bed later, sleep later – it's up to you.
Do this for 1 month…
Long-term habits
Jennifer L. Martin, PhD
"The catch“Schedule your “off” days.It can be easy to sleep “off schedule” more than once a week and drift back into old habits. This can lead down a dangerous road, and can lead to the return of sleep problems.
Long-term habits
Jennifer L. Martin, PhD

Sleep scheduleStimulus control activitiesDealing with worry/anxietySleep hygiene strategies
Ask the patient, then add to the list yourself
ALMOST ALL PATIENTS BENEFIT MOST FROM SLEEP RESTRICTION AND STIMULUS CONTROL
What has been most helpful
You will have another bad night of sleep. This is a NORMAL reaction to stressful events.
Expect it and be prepared with a planRelapse to “chronic insomnia” (i.e., >1 month) is rare after CBT-I – about 5-15%Use what you have learned to prevent a few bad nights from becoming a chronic problemKeep some sleep diaries around and do the following…
Dealing with insomnia relapse
Jennifer L. Martin, PhD
One night of poor sleep:Get out of bed if you’re not asleep within 30 minutes. Go back to bed only when you're sleepy. Get up at your regular wake up time.
Step 1: Dealing with insomnia recurrence
Jennifer L. Martin, PhD

Two consecutive nights of poor sleep:Stay up one hour later than your bedtime. Keep your wake up time the same. Do it even if you were planning to sleep in that day. Once you are sleeping well (sleep efficiency >85%), go to bed 30 minutes earlier every 2 days until you’re back where you started. This should take about a week.
Step 2: Dealing with insomnia recurrence
Jennifer L. Martin, PhD
If you have few bad nights:Don’t be discouraged! Start keeping a sleep diary, and follow the plan for an additional week.These experiences will increase your confidence
Step 3: Dealing with insomnia recurrence
Jennifer L. Martin, PhD
If you can’t get back on track on your own after one monthCome in for a “booster” session
Step 4: Dealing with insomnia recurrence
Jennifer L. Martin, PhD

SLEEP EVALUATION Page 1 of 6
Jennifer L. Martin, PhD, CBSM
Name:____________________________ Date:__________________ HISTORY OF SLEEP COMPLAINT Describe your current sleep problems:____________________________________________________ __________________________________________________________________________________ Onset of problems: When did this start? Any stressful events at that time? Any health changes at that time? Describe the course of your sleep problem: chronic or on/off? Did you sleep well prior to [above events]? Attempts to manage/deal with sleep problems: Medications tried: (name, dose, frequency of use) How well did they work? Non-medication strategies tried: How well did they work? Have you had a sleep study? What were the results? CURRENT SLEEP SCHEDULE What is a typical day like for you? What is your routine?______________________________________ __________________________________________________________________________________ � no � yes Do you work? What hours? _________________________________ � no � yes Did you ever do overnight shift work? Does your work schedule or daily activities impact sleep schedule________________________ � no � yes Current shift work____________________________________________ � no � yes Differences between weekends and weekdays_________________________ _________________________________________________________________ Sleep quality/patterns when away from home � better__________________ � same ____________________� worse____________________

SLEEP EVALUATION Page 2 of 6
Jennifer L. Martin, PhD, CBSM
Bedtime:__________________________________________________________ Time to fall asleep (sleep onset latency)_________________________________ Night awakenings (# and duration):_____________________________________ Awakened by: _____________________________________________________ � don’t know__________________________________________ Do you wake up too early in the morning?_______________________________ Morning wake time:_________________________________________________ Estimate the number of hours you sleep:
On a "typical" night___________ On a "good" night____________
How much sleep is right for you?_______________ What “predicts” a good night of sleep?________________ What “predicts” a bad night of sleep?_________________ DAYTIME NAPPING Do you take "planned naps"; that is, fall asleep on purpose during the day or evening? � no � yes time of day: _________________________________________ where nap:__________________________________________ length of nap: ________________________________________ how often: __________________________________________ Do you sometimes doze off or fall asleep without meaning to during the day or in the evening? � no � yes time of day: _________________________________________ where nap:__________________________________________ how long asleep: _____________________________________ how often: __________________________________________ SLEEP-RELATED HABITS (sleep hygiene) Do you have: � no � yes Regular meals: Dinner time_______________________________________ � no � yes Snack after dinner: time __________________________________________ � no � yes Coffee; how much:______________latest: ___________________________ � no � yes Tea; how much:________________ latest: ___________________________ � no � yes Soda; how much:_______________ latest: ___________________________ � no � yes Chocolate; how much: ___________latest: ___________________________ � no � yes Smokes; packs/day______________started smoking____________________ � no � yes Alcohol; how much:_____________ what time of day __________________ � no � yes Marijuana______________________________________________________ � no � yes Drugs_________________________________________________________ � no � yes Exercise; Type__________________________________________________ how often____________________time of day_________________

SLEEP EVALUATION Page 3 of 6
Jennifer L. Martin, PhD, CBSM
Sleep environment Do any of the following disrupt your sleep? � no � yes Uncomfortable bed?______________________________________________ � no � yes Temperature � too hot � too cold _______________________________ � no � yes Noise, source______________________how often_____________________ � no � yes Light, source______________________how often_____________________ � no � yes bedpartner ________How does bedpartner disrupt sleep? __________________ � no � yes Children or other care recipients? Describe______________________________ Age of children/care recipients_________________________________________ Type of care required_________________________________________________ � no � yes Other sleep interruptions__________________________________________ SYMPTOMS OF SLEEP DISORDERS � no � yes Snoring � no � yes gasping � no � yes choking � no � yes waking up with shortness of breath � no � yes witnessed apneas (someone saw you stop breathing) � no � yes nighttime sweating � no � yes morning headaches � no � yes Restless legs (creepy crawly): In the evening When trying to fall asleep During the night Kicking legs while asleep (usually witnessed) � no � yes Sleepwalking � no � yes sleeptalking � no � yes “acting out dreams” � no � yes Nightmares If yes, how often?_________________When did they start?_____________ � no � yes Irresistible attacks of sleep that occur daily � no � yes Falling asleep and dreaming right away � no � yes Dream-like hallucinations while falling asleep or waking up? � no � yes Feeling paralyzed just before falling asleep or right after waking up? � no � yes Sudden weakness or loss of muscles tone during the day, often related to intense
emotion or laughter Other:______________________________________________________________________

SLEEP EVALUATION Page 4 of 6
Jennifer L. Martin, PhD, CBSM
BEHAVIORAL / CONDITIONING CONSIDERATIONS Where do you sleep � bed � sofa/couch � chair/recliner � other_________________________ When you are awake at night, How long do you stay awake in bed? ______________________________________ Do you think or worry in bed? � no � yes About what?_______________________________________ Do you: � no � yes eat in bed, what? _______________________________________________ � no � yes work/other tasks in bed? _________________________________________ � no � yes watch TV in bed?_______________________________________________ � no � yes other activities in bed? ___________________________________________ When you awake at night do you GET OUT OF BED? � no � yes If yes, what do you do? � no � yes watch TV � no � yes read � no � yes work � no � yes eat (what___________________) � no � yes do other activities? What? ____________________ IMPACT ON DAYTIME FUNCTIONING Because of sleep problems do you experience � no � yes mood changes: � depressed � anxious � irritable � frustrated � no � yes poor concentration or memory _____________________________________ � no � yes sleepy or tired __________________________________________________ � no � yes falling asleep during focused activity________________________________ � no � yes falling asleep while driving________________________________________ � no � yes falling asleep during sedentary activity_______________________________ � no � yes low energy_____________________________________________________ � no � yes trouble with work or school________________________________________ � no � yes physical symptoms ______________________________________________ � no � yes worrying about sleep during the day ________________________________ Does your functioning improve when you are sleeping better? � no � yes functioning improves with better sleep_______________________________

SLEEP EVALUATION Page 5 of 6
Jennifer L. Martin, PhD, CBSM
PSYCHIATRIC HISTORY Some psychiatric problems can impact sleep. Have you been diagnosed with: � no � yes depression � no � yes currently symptomatic � no � yes bipolar disorder � no � yes currently symptomatic � no � yes anxiety � no � yes currently symptomatic � no � yes psychosis � no � yes currently symptomatic � no � yes PTSD � no � yes currently symptomatic � no � yes alcohol/substance use � no � yes currently using ________sober � no � yes other:_________________________________________________________ Do your sleep problems changes when your psychiatric symptoms change (e.g., sleep gets worse when depression gets worse?) � no � yes sleep changes with psychiatric symptoms_____________________________ Are you currently being treated for any psychiatric conditions? medications (Rx and OTC):_____________________________________________________ other treatments (psychotherapy, other):___________________________________________ How is your mood today?___________________________ Over the past few weeks?____________________________ � no � yes Suicidal ideation? _________________________________________________ ____________________________________________________________ MEDICAL HISTORY Some medical problems can impact sleep. � no � yes Are you currently receiving care for any chronic health problems?_____________ ____________________________________________________________________ � no � yes Are you taking any medications?________________________________________ ____________________________________________________________________ Do your sleep problems changes when your medical symptoms change (e.g., sleep gets worse when depression gets worse?) � no � yes sleep changes with psychiatric symptoms_____________________________ Have you had/do you have: � no � yes head injury, when_____________________________LOC______________ � no � yes memory problems, dementia_______________________________________ � no � yes stroke_________________________________________________________ � no � yes hypertension____________________________________________________ � no � yes pain, cause_____________________disrupts sleep?____________________ � no � yes other__________________________________________________________ How many times use bathroom at night? ___________________________________________ � no � yes BPH? Prostate cancer? Other?
SLEEP EVALUATION Page 6 of 6
Jennifer L. Martin, PhD, CBSM
FAMILY HISTORY OF SLEEP PROBLEMS � no � yes describe_______________________________________________________ DIAGNOSTIC IMPRESSION(S) Axis I: _________________________________________________
__________________________________________________ Axis II: _________________________________________________ Axis III: _________________________________________________ Axis IV: _________________________________________________ Axis V: __________________________________________________ TREATMENT PLAN (Discussed with and agreed upon by patient):
� sleep diary � CBT-I appropriate Considerations for providing CBT-I ____________________________________________________________________ ____________________________________________________________________ ____________________________________________________________________ ____________________________________________________________________ � referrals/consultations _________________________________
Next appointment: ____________________________________________









![Cognitive Behavioral Therapy for Insomnia - Turner White ... · PDF fileand are also observed cognitive behavioral therapy for insomnia (CBT-I) [6] ... the adaptation of cognitive](https://img.dokumen.tips/doc/110x75/5a7892127f8b9a7b698cf1ad/cognitive-behavioral-therapy-for-insomnia-turner-white-are-also-observed-cognitive.jpg)



















