Embed Size (px)
Citation preview

CLINICAL TRANSLATION OF ANIMAL MODELS OF TREATMENT RELAPSE
DUNCAN PRITCHARD1,2, MARGUERITE HOERGER
2, F. CHARLES MACE3, HEATHER PENNEY
1,AND BRIAN HARRIS
1
1ARAN HALL SCHOOL2BANGOR UNIVERSITY
3NOVA SOUTHEASTERN UNIVERSITY
Behavioral Momentum Theory (BMT) has inspired animal models of treatment relapse. We translated themodels of reinstatement and resurgence into clinical procedures to test whether relapse tests wouldreplicate behavior pattern found in basic research. Following multiple schedule baseline reinforcement ofa 16-year-old male’s problem behavior at equal rates by two therapists, treatment was introduced using avariable-interval, variable-time (VI VT) schedule arrangement with therapists delivering reinforcers atdifferent rates. Despite the differing rates of VI VT reinforcers, the treatment produced comparablereductions in problem behavior. Following successful treatment, the two therapists discontinued treatmentand resumed reinforcement of problem behavior at equal rates that constituted a reinstatement of baselineconditions. As predicted by BMT, reinstatement resulted in an immediate return of high rates of problembehavior but was 2.6 times higher for the therapist using the higher rate VI VT treatment. A secondtreatment phase was implemented followed by a test of resurgence in a single extended extinction sessionconducted separately for each therapist. The unequal VI VT treatment rates by therapists resulted in 2.1times greater responding in the resurgence test for the therapist who implemented the higher rate VI VTprocedure. These results are consistent with basic research studies and BMT.Key words: behavioral momentum, reinstatement, resurgence, treatment relapse
The fundamental finding from BehavioralMomentum Theory (BMT) research is thatbehavior is more persistent during disruptionin a context correlated with greater reinforce-ment (Nevin, 1992; Nevin & Grace, 2000; Nevin,Tota, Torquato & Shull, 1990). This generalfunctional relationship has attracted the atten-tion of translational researchers because of theimplications basic BMT research has for com-mon clinical treatments for behavior disorderssuch as differential reinforcement of alternativebehavior (DRA) and variable- and fixed-timereinforcer deliveries (VT, FT).
For example, Ahearn, Clark, Gardenier,Chung and Dube (2003) found that VT accessto toys reduced automatically reinforced ste-reotypic behavior relative to a no-interactionbaseline for three children with autistic disor-der. However, when stereotypic behavior wasdisrupted by providing children continuousaccess to an activity that competed with stereo-typed responses, stereotypy occurred more
often following the VT treatment comparedto sessions following the no-interaction base-line. BMT predicts this finding due to thehigher rate of reinforcement in the VTtreatment relative to baseline. Mace et al.(2010) reported similar findings for the effectsDRA can have on the resistance to extinction ofproblem behaviors that were reinforced bysocially mediated consequences (attention andfood). Thus, although treatments based onalternative reinforcement effectively reduceproblem behavior, they can paradoxicallyincrease its resistance to extinction (cf. Nevinet al., 1990).
Treatment relapse is a generic term used inseveral medical and mental health fields. Itrefers to the recurrence of a condition that hasbeen previously treated effectively. Podlesnikand Shahan (2009) examined three paradigmsof treatment relapse (reinstatement, resurgenceand renewal) with pigeons that are conceptual-ized within the framework of BMT. A commonbaseline procedure was used to test each of therelapse models. Pigeons were provided equal VI120-s response-dependent food in a two-compo-nent multiple schedule. Time-contingent foodwas added to one of the components on avariable time (VT) 20-s schedule. The tworelapse paradigms relevant to the currentresearch are reinstatement and resurgence.
This research was conducted as partial fulfillment of thefirst author’s Ph.D. degree in psychology at BangorUniversity. Preparation of this article was supported inpart by NICHD 064576.Address correspondence to: Duncan Pritchard, Aran Hall
School, Rhydymain, Dolgellau, Gwynedd, LL40 2AR. Email:[email protected]: 10.1002/jeab.87
JOURNAL OF THE EXPERIMENTAL ANALYSIS OF BEHAVIOR 2014, 101, 442–449 NUMBER 3 (MAY)
442

In tests of the reinstatement paradigm,following extinction of baseline responding,food was presented response-independently infour sessions and response-dependently foranother four sessions, with session blocks beingseparated by a second phase of extinction. Foodwas presented independently of key pecks at 2and 8 s into the first presentation of eachcomponent in a session and later contingenton the first two responses in each component ofthe session; food was withheld for the remainderof the session. The reinstatement procedure wasan analog of the resumption of reinforcerdeliveries that had previously maintained prob-lem behavior. Although reinforcer rates duringthe response-independent and response-depen-dent tests were identical, the magnitude ofrelapse was greater in the component withadded VT reinforcers during baseline.For the resurgence model, extinction of the
target baseline key in both components wascombined with equal VI 30-s DRA for a secondkey and continued until responding on thetarget baseline key reduced below 10% ofbaseline. The resurgence test discontinuedreinforcement for all responses, but the re-sponse of interest was a resumption of respond-ing on the target baseline key in bothcomponents. Despite ongoing extinction ofthe target and alternative responses, baselinekey responding resumed in both componentsbut to a greater extent in the component withthe added VT reinforcers in baseline. Thisprocedure models treatment relapse followingdiscontinuation of an effective DRA treatment.The clinical value of these animal models of
treatment relapse depends on the extent towhich they predict clinically relevant humanbehavior exposed to treatment challengescommonly encountered in clinical settings.Only one clinical translational study has exam-ined the BMT reinstatement paradigm. DeL-eon, Willams, Gregory and Hagopian (2005)reported clinical data consistent with thereinstatement model of relapse. Problem be-havior was reinforced by attention on an FR1schedule during baseline. Following baselinereinforcement, all attention was withheld forproblem behavior until problem behavior waseliminated for four consecutive sessions. Atten-tion was reintroduced on a FT 60-s schedule forthree sessions and problem behavior immedi-ately returned as predicted by the reinstatementparadigm tested by Podlesnik and Shahan
(2009). However, DeLeon et al. did not arrangedifferent rates of reinforcement in a multipleschedule to demonstrate that reinstatementeffects were greater in the component correlat-ed with a higher rate of reinforcement.We are aware of only one clinical study that
approximates a test of one of the BMTparadigms of treatment relapse. MacDonald,Ahearn, Parry-Cruwys, and Bancroft (2013)conducted a clinical translation of the resur-gence paradigm of relapse described by Pod-lesnik and Shahan (2009) with some variationfrom the basic research. In the first phase of thestudy, problem behavior was alternately rein-forced on a CRF schedule and a variable-ratio(VR) 3 schedule in separate components of amixed schedule of reinforcement. Each rein-forcement component was followed by extinc-tion for all responses. The obtained rates ofreinforcement expressed as a ratio of intermit-tent to continuous reinforcement were 2.30,1.66, 1.41 and 1.8 for the four participants.Results showed that the transition from the CRFschedule to extinction resulted in substantiallyhigher rates of problem behavior than thetransition from VR 3 to extinction. Although theprocedure has no direct parallels with theanimal model of resurgence, MacDonald et al.(2013) did demonstrate that relatively higherrates of reinforcement for clinically significantproblem behavior can result in higher responserates during extinction.The present study aimed to translate the
animal models of reinstatement and resurgenceinto clinical procedures that closely approximatethose used in laboratory studies with nonhumans(e.g., Podlesnik & Shahan, 2009, 2010; Sweeney& Shahan, 2013). Both models were testedfollowing a multiple schedule arrangement of aVI VT treatment at different rates, therebyholding constant a 4-to-1 relative reinforcementratio in the schedule components. Reinstate-ment was tested by a return to contingentreinforcement of problem behavior and resur-gence was tested by extinction following success-ful treatment.
Method
Participant, Setting and MaterialsThe participant was a 16 year-old male with
severe intellectual disability and severe aggres-sive and disruptive behavior. All experimentalsessions were conducted in a 10m by 6m living
TRANSLATION OF TREATMENT RELAPSE MODELS 443

area that contained two sofas, two tables withbench seats and an enclosed television. Theparticipant had access to preferred items such aspicture books and toys throughout all sessions.One of two therapists and one or two datacollectors were present for all sessions. Theprimary data collector was blind to the experi-mental hypotheses.
Target Behaviors, Data Collection andInterobserver Agreement
Participant target behaviors were: (a) aggres-sion, defined as slapping, biting, kicking, head-butting, hitting the therapist with an object,spitting on the therapist, forceful pushing, andattempted eye gouging; and (b) disruption,defined as throwing objects and tearing paper.Staff attention took two forms. During thefunctional analysis baseline and reinstatementphases, staffmade disapproving comments (e.g.,‘stop that.’, ‘that hurts.’, ‘don’t tear things up.’)contingent on occurrences of aggression anddisruption. During treatment, therapists re-sponded to demands for attention or providedVT attention in the form of pleasant interactionwith the participant for approximately 10 s.
Two independent data collectors recordedcounts of aggression and disruption in continu-ous 10-s intervals. Staff attention was recordedusing a 10-s partial-interval procedure. Interob-server agreement was balanced across studyphases and calculated using the exact agreementmethod on a point-by-point or interval-by-inter-val method (Cooper, Heron & Heward, 2007)for an average of 59.3%of the sessions for Phases1a to 4 and during the entire session for Phase 5.Mean total agreement on occurrences andnonoccurrences across all phases was 89.0%(range, 73.6% to 100%).
ProcedureThe study was composed of five successive
phases. The conditions in each phase werearranged in a multiple schedule with mostcomponents presented in a strictly alternatingsequence, with exceptions noted below. Twodifferent therapists served as discriminativestimuli for the schedule components. Sessionswere conducted on consecutive days and allsessions except extinction in Phase 5 were10min in duration and separated by a 5minperiod without adult attention.
Phase 1—Functional analysis baseline. Previ-ous clinical work with this participant indicated
that his problem behavior was reinforced byattention (Mace et al., 2008). Separate attentionand control conditions were conducted bydifferent therapists (three sessions each forthe attention condition and three and twocontrol sessions conducted by Therapists 1 and2, respectively). Both therapists in the attentioncondition only interacted with the participantcontingent on problem behavior on a quasiran-dom VI 60-s schedule of reinforcement withouta limited hold. In the control condition, thetherapist provided near continuous interactionwith the participant and provided no instruc-tional demands. Mean obtained rates of atten-tion in the attention condition provided byTherapist 1 were 46.0/hr and 48.0/hr forTherapist 2. No attention was provided contin-gent on problem behavior by either therapist inthe control condition (see Table 1).
Phases 2 and 4—VI VT treatment provided atdifferent rates of reinforcement. Therapist 1and Therapist 2 provided attention at differentrates in a quasirandom VI VT schedule oftreatment. Each time reinforcers were sched-uled to be available, the therapist approachedthe participant and pointed to a photograph ofthe therapist and participant interacting alongwith a verbal prompt (‘would you like to talk?’—serving as an SD for communication). Commu-nication responses resulted in contingent atten-tion for 10 s (i.e., VI attention). If the participantfailed to respond to the prompt, the therapistprovided verbal and physical attention for asimilar duration (i.e., VT attention). Therapist 1provided attention on a VI VT 30-s schedule andTherapist 2 provided the same treatment on a VIVT 120-s schedule. No interaction occurredduring the interreinforcement intervals. Ob-tained rates of attention averaged 120/hr forTherapist 1 and 30/hr for Therapist 2 in bothtreatment phases. The VT component of thetreatment permitted scheduled and obtainedreinforcement rates to be equivalent. Treatmentsessions continued in phase 2 and phase 4 untilaverage rates of problem behavior for boththerapists were 8.5% and 17% of the initialfunctional analysis baseline, respectively.
Phase 3—Reinstatement of equal rates ofreinforcement. Following the initial treatmentphase, the VI VT intervention was discontinuedand both therapists resumed reinforcement ofaggression and disruption on equal VI 60-sschedules of reinforcement. In the attentioncondition, the mean rates of attention provided
444 DUNCAN PRITCHARD et al.

by Therapist 1 were 46.8/hr and 48.0/hr,respectively. In the control condition, no atten-tion was provided contingent on problembehavior by either therapist (see Table 1).Phase 5—Extinction test of resurgence. A
single 74-min session of extinction followed thesecond treatment phase for each therapist. Thetherapist stood within 1m of the participant atall times and did not look at or talk to theparticipant during the entire session. Therapist1 conducted the first extinction session andTherapist 2 conducted the second session fourhours later.
Results
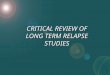
Figure 1 shows the participant’s rates ofaggression and disruption during the functionalanalysis baseline, VI VT treatments in the initialand replication phases, and reinstatement ofbaseline reinforcement of problem behavior asimplemented by the two therapists. Meanresponses per min by phase and therapist arepresented in Table 1. The functional analysisbaseline showed clear differentiation betweenproblem behavior in the attention condition(Phase 1a) and the control condition (Phase1b)for both therapists, thus confirming that prob-lem behavior was maintained by therapistattention. The VI VT intervention producedsimilar reductions in problem behavior acrosstherapists in both treatment phases (M¼ 2.7/min for Therapist 1 and 1.9/min for Therapist 2—reduced from 8.3/min in the functionalanalysis baseline) despite the fourfold differ-ence in treatment reinforcement rates thatfavored Therapist 1. However, reinstatementof comparable rates of baseline reinforcementresulted in the return of problem behavior thataveraged 2.6 times higher with Therapist 1 whoimplemented the higher rate VI VT treatment.Mean reinstatement data expressed as propor-tion of baseline was 2.5 for Therapist 1 and 0.95for Therapist 2.Figure 2 shows the cumulative number of
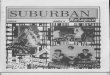
aggressions and disruptions during the singleextended extinction session for both therapistsand represents a test of the resurgence paradigmof relapse. Problem behavior first occurred14.8min into extinction for Therapist 1 and therewere four occurrences at minute 19.2. High-rateproblem behavior began at minute 36.5; however,there were only eight occurrences of problembehavior prior to this point. Responding remained
Tab
le1
Meanrespon
seratesan
dob
tained
reinforcer
ratesco
ntin
genton
prob
lem
behaviorin
allp
hases
except
Phase1a
forTherap
ist1an
dTherap
ist2.
Phase1a
Phase1b
Phase2
Phase3
Phase4
Phase5
Equ
alBLSR
þBLCon
trol
Uneq
ualVI
VTSR
þEqu
alSR
þReinstatem
ent
Uneq
ualVI
VTSR
þEXTResurge
nce
Respo
nses/
min
SRþ/
hr
Respo
nses/
min
SRþ/
hr
Respo
nses/
min
SRþ/
hr
Respo
nses/
min
SRþ/
hr
Respo
nses/
min
SRþ/
hr
Respo
nses/min
SRþ/
hr
Therap
ist1
8.30
460.03
03.18
120
20.72
46.8
1.98
120
1.95
0Therap
ist2
8.30
480.05
01.52
307.94
482.63
300.89
0
TRANSLATION OF TREATMENT RELAPSE MODELS 445

fairly steadyuntilminute 54.7, lasting18.2min, andthen slowed markedly to minute 74.0 when therehad been 5.0min without problem behavior. ForTherapist 2, the first problem behavior occurred
comparatively early into extinction at minute 2.0and twomore responses occurred at minute 3.2. Asharp but short burst of responding (63 responsesin 0.8min)began atminute 37.7 after 25 responses
Fig. 1. Aggression and disruption per min for all sessions in the functional analysis and reinstatement phases and two VIVT treatment phases conducted by Therapist 1 and Therapist 2.
Fig. 2. Cumulative number of aggressions and disruptions per min during a single extinction session for Therapist 1 andTherapist 2.
446 DUNCAN PRITCHARD et al.

hadoccurred. Atminute 38.5, responding stoppedabruptly with only 3 responses occurring theremainder of the resurgence test.Overall responserate during extinction was 1.9/min for Therapist 1compared to 0.9/min for Therapist 2.
Discussion
This study is the first clinical translation of thereinstatement paradigm of treatment relapsebased on BMT research that conducted relapsetests following treatments with different rates ofreinforcement. Following a multiple schedulebaseline reinforcement of problem behavior atequal rates by two therapists, treatment wasintroduced using a VI VT schedule arrangementwith therapists delivering reinforcers at differ-ent rates at a 4-to-1 ratio. Despite the differingrates of VI VT reinforcers, the treatmentproduced comparable reductions in problembehavior. Following successful treatment, thetwo therapists discontinued treatment andresumed reinforcement of problem behaviorat equal rates that constituted a reinstatement ofbaseline conditions (see Podlesnik & Shahan,2009; response-dependent reinstatement). Aspredicted by BMT, reinstatement resulted in animmediate return of high rates of problembehavior that were 2.6 times higher for thetherapist using the higher rate VI VT treatment.A second treatment phase was implementedfollowed by a test of resurgence in a singleextended extinction session conducted sepa-rately for each therapist. The unequal VI VTtreatment rates implemented by therapistsresulted in 2.1 times greater responding in theresurgence test for the therapist who imple-mented the higher rate VI VT procedure (cf.,MacDonald et al., 2013).We note that this study should be considered
preliminary because the demonstrations weremade with only one subject. Had multiplesubjects been studied, the order of the resur-gence extinction tests across therapists couldhave been counterbalanced. This leaves openthe possibility that the lower frequency ofresponding during extinction for Therapist 2may have been partially affected by Therapist 1conducting extinction four hours earlier. How-ever, the participant’s first response duringextinction with Therapist 2 occurred approxi-mately 12.8min before it did with Therapist 1,and the response rate being 2.1 times higher forTherapist 1 than Therapist 2 is similar to the first
extinction session in Podlesnik and Shahan(2009, Fig. 4, p. 361).A key feature of BMT relapse experiments is
that they employ a two-component multipleschedule with different reinforcer rates in thecomponents. This phase provides the basis forbetween-component comparisons during ex-tinction and the subsequent reintroduction ofreinforcers. Our clinical translation differedfrom the procedures used by Podlesnik andShahan (2009). In the animal model, the two-component baseline that served as the basis forcomparisons during relapse tests was analogousto baseline reinforcement of problem behavior.By contrast, our relapse tests followed a two-component treatment designed to produceclinically significant reductions in problembehavior from a no-treatment baseline.A second difference between the animal and
translational procedures was the amount ofreinforcement provided during reinstatement.In the animal model of reinstatement, theresponse-independent and response-depen-dent variations both provided only two rein-forcers in the first presentation of eachcomponent in a session. Pyszczynski and Shahan(2011) used a similar response-independentprocedure in a relapse model of ethanolseeking. From a clinical translation viewpoint,these animal models can be seen as temporaryreinstatement of reinforcers and represent ashort-term lapse in treatment integrity (i.e.,failing to withhold reinforcement of problembehavior). The present clinical translationreturned to VI 60-s reinforcement throughoutall reinstatement sessions, clinically represent-ing a complete lapse of treatment integrity.A third difference between the laboratory and
clinical procedures is the number and durationof the extinction sessions. In their resurgenceexperiment, Podlesnik and Shahan (2009)discontinued reinforcement of the target andalternative keys in both components for twoconsecutive five-session blocks. Our clinical testof resurgence was done in a single extendedextinction session for both therapists. Conduct-ing several extinction sessions with a participantwith clinically severe behavior disorder can becontraindicated if the behavior is capable ofproducing serious injury. Therefore, we optedfor a single session of extinction for boththerapists to minimize as much as possible anyinjury to the therapists. However, despite theprocedural differences between the laboratory
TRANSLATION OF TREATMENT RELAPSE MODELS 447

models and clinical translations, the clinicalfindings reported here are consistent with thenonhuman data and are predicted by BMT.
Although the present study is preliminary, if theclinical findings are replicated, it suggests thatDRAand/or VT/FT treatments may have the undesir-able side effect of strengthening the persistence ofproblem behavior and increasing the likelihood oftreatment relapse when treatment integrity iscompromised. Our study is also consistent withrecent basic research with rats. Sweeney andShahan (2013) compared the effectiveness andresistance to extinction of high-rate and low-rateDRA that differed by tenfold. Both the targetresponse (lever press) and alternative response(nose poke) were more resistant to extinction inthe high-rate DRA component. The finding thatthe magnitude of relapse may be greater usinghigher-rate reinforcers contradicts practice that iswidely prescribed in the applied behavior analysisliterature (Carr et al., 2000; Chowdhury & Benson,2011; Cooper, Heron & Heward, 2007; Petscher,Rey & Bailey, 2009).
Basic and clinical researchers have begunexamining solutions to this undesirable sideeffect of DRA and/or VT/FT behavioral treat-ments. Mace et al. (2010) showed, first with ratsand then with children with intellectual devel-opmental disabilities, that increased resistanceto extinction could be reduced or eliminated byfirst training the alternative response in aseparate context from the context correlatedwith reinforcement of a target response orproblem behavior. Once the alternative re-sponse is established, discriminative stimuli forthe alternative response can be introduced tothe treatment setting and effectively treatproblem behavior without increasing the mag-nitude of relapse. Podlesnik, Bai & Elliffe (2012)replicated this general finding with pigeons.Wacker et al. (2011) suggested a second relapseremedy. They provided extended functionalcommunication training (FCT) to treat child-ren’s destructive behavior over an average of9 months. FCT is a differential reinforcement ofalternative behavior (DRA) procedure duringwhich an individual is taught a communicativebehavior that replaces the problem behavior.Typically, the problem behavior is placed onextinction (Carr & Durand, 1985). At fourpoints in time during the course of the child-ren’s treatment, discontinuation of DRA com-bined with extinction provided tests ofresurgence. The average magnitude of relapse
reduced over successive resurgence tests. Thedata patterns over the long-term treatmentconformed closely to a formula developed byShahan and Sweeney (2011) that assumes thatDRA simultaneously disrupts problem behaviorand strengthens the persistence of alternativebehavior.
The present study suggests a third potentialsolution to the problem of treatment relapse. VIVT treatment produced comparable reductionsin problem behavior when delivered at bothhigh and low rates. Basic researchers may findthis finding counterintuitive. For example, inthe Sweeney and Shahan (2013) study, high-rateDRA produced more rapid reductions in thetarget response and rapid acquisition and rate ofthe alternative response compared to the low-rate DRA condition. However, our oppositeclinical findings may be attributable to thecomposition of contemporary behavioral treat-ments. It is common for behavioral treatmentsto make the alternative response less effortfuland to reinforce the alternative response with areinforcer of higher quality than the reinforcermaintaining problem behavior (Mace &Roberts, 1993). The present VI VT treatmentrequired the participant to point to a photo-graph to receive attention in the form of smiles,praise, back pats and tickles compared todisapproving comments provided in the func-tional analysis baseline. If replicated, thisfinding that low-rate treatment was as effectiveas high-rate treatment will have beneficialimplications for clinicians who aim to achievegood treatment integrity in natural settings forlong periods of time. Low-rate reinforcement-based treatments have been found to yieldbetter treatment integrity than their high-ratecounterparts (Chowdhury & Benson, 2011).
Finally, Sweeney and Shahan (2013) demon-strated a fourth potential remedy for treatmentrelapse. In addition to a high-rate and low-rateDRA condition, their experiment included aschedule-thinning condition. The high-rate andthinning conditions began the first session withVI 10-s reinforcement of nose poking. Thefading group of rats had their schedules thinneddaily by 10 s until it reached the value of the low-rate DRA group (i.e., VI 100-s). During theresurgence extinction test, relapse was signifi-cantly lower in the thinning group compared tothe high-rate DRA group, and was not statisti-cally different from the low-rate DRA group.This is important because it modeled a practical
448 DUNCAN PRITCHARD et al.

and widely used schedule-thinning procedurethat significantly reduced the magnitude oftreatment relapse relative to the high-rate DRAcondition.The present study and those cited in this
paper illustrate a theory-driven approach toconceptualize clinical phenomena and establishthe basic processes involved in the seriousclinical problem of treatment relapse. In manycases, basic and clinical researchers are collabo-rating formally and informally on their workfollowing a bi-directional translation researchmodel (Mace, 1994; Mace & Critchfield, 2010).The pace of development of the BMT model oftreatment relapse appears to be benefiting fromthis approach to research.
References
Ahearn,W.H., Clark, K.M., Gardenier, N. C., Chung, B. I., &Dube, W. V. (2003). Persistence of stereotypic behavior:Examining the effects of external reinforcers. Journal ofApplied Behavior Analysis, 36, 439–448.
Carr, J. E., Coriaty, S.,Wilder, D. A., Gaunt, B. T., Dozier, C. L.,& Britton, L. N.,… Reed, C. L. (2000). A review of ‘non-contingent’ reinforcement as treatment for the aberrantbehavior of individuals with developmental disabilities.Research in Developmental Disabilities, 21, 377–391.
Carr, E. G., & Durand, V. M. (1985). Reducing behaviorproblems through functional communication training.Journal of Applied Behavior Analysis, 18, 111–126.
Chowdhury, M., & Benson, B. A. (2011). Use of differentialreinforcement to reduce behavior problems in adultswith intellectual disabilities: A methodological review.Research in Developmental Disabilities, 32, 383–394.
Cooper, J. O., Heron, T. E., & Heward, W. L. (2007). Appliedbehavior analysis, (2nd Edition). SaddleRiver, NJ: PearsonEducation.
DeLeon, I. G., Williams, D. C., Gregory, M. K., & Hagopian,L. P. (2005). Unexamined potential effects of thenoncontingent delivery of reinforcers. European Journalof Behavior Analysis, 5, 57–69.
MacDonald, J. M., Ahearn, W. H., Parry-Cruwys, D., &Bancroft, S. (2013). Persistence during extinction:Examining the effects of continuous and intermittentreinforcement on problem behavior. Journal of AppliedBehavior Analysis, 46, 333–338.
Mace, F. C. (1994). Basic research needed for stimulating thedevelopment of behavioral technologies. Journal of theExperimental Analysis of Behavior, 61, 529–550.
Mace, F. C., & Critchfield, T. S. (2010). Translationalresearch in behavior analysis: Historical traditions andimperative for the future. Journal of the ExperimentalAnalysis of Behavior, 93, 293–312.
Mace, F. C., McComas, J. J., Mauro, B. C., Progar, P. R.,Taylor, B., Ervin, R., & Zangrillo, A. N. (2010).Differential reinforcement of alternative behavior
increases resistance to extinction: Clinical demonstra-tion, animal modeling, and clinical test of one solution.Journal of the Experimental Analysis of Behavior, 93, 349–367.
Mace, F. C., & Roberts, M. L. (1993). Factors affectingselection of behavioral interventions. In J. Reichle, &D. P. Wacker (Eds.), Communicative alternatives tochallenging behavior: Integrating functional assessment andintervention strategies (pp. 113–133). Baltimore, MD: PaulH. Brookes Publishing.
Mace, F. C., Zangrillo, A. N., Prager, K., Carolan, E., Hoerger,M., Thomas, K., & Pritchard, D. (2008). A methodologyfor maintaining low levels of attention-maintainedproblem behaviors following variable-time schedulethinning. European Journal of Behavior Analysis, 9, 149–156.
Nevin, J. A. (1992). An integrative model for the study ofbehavioral momentum. Journal of the ExperimentalAnalysis of Behavior, 57, 301–316.
Nevin, J. A., & Grace, R. C. (2000). Behavioral momentumand the Law of Effect. Behavioral and Brain Sciences, 23,73–130.
Nevin, J. A., Tota, M. E., Torquato, R. D., & Shull, R. L.(1990). Alternative reinforcement increases resistanceto change: Pavlovian or operant contingencies? Journalof the Experimental Analysis of Behavior, 53, 359–379.
Petscher, E. S., Rey, C., & Bailey, J. S. (2009). A review ofempirical support for differential reinforcement ofalternative behavior. Research in Development Disabilities,30, 409–425.
Podlesnik, C. A., Bai, J. Y. H., & Elliffe, D. (2012). Resistanceto extinction and relapse in combined stimuluscontexts. Journal of the Experimental Analysis of Behavior,98, 169–189.
Podlesnik, C. A., & Shahan, T. A. (2009). Behavioralmomentum and relapse of extinguished operantresponding. Learning and Behavior, 37, 357–364.
Podlesnik, C. A., & Shahan, T. A. (2010). Extinction, relapseand behavioral momentum. Behavioral Processes, 84, 400–411.
Pyszczynski, A. D., & Shahan, T. A. (2011). Behavioralmomentum and relapse of ethanol seeking: non-drugreinforcement in a context increases relative reinstate-ment. Behavioural Pharmacology, 22, 81–86.
Shahan, T. A., & Sweeney, M. M. (2011). A model ofresurgence based on behavioral momentum theory.Journal of the Experimental Analysis of Behavior, 95, 91–108.
Sweeney, M., & Shahan, T. (2013). Effects of high, low, andthinning rates of alternative reinforcement on responseelimination and resurgence. Journal of the ExperimentalAnalysis of Behavior, 1, 1–15.
Wacker, D. P., Harding, J. W., Berg, W. K., Lee, J. F., Schieltz,K. M., Padilla, Y. C. … Shahan, T. A., (2011). Anevaluation of persistence of treatment effects duringlong-term treatment of destructive behavior. Journal ofthe Experimental Analysis of Behavior, 96, 261–282.
Received: July 11, 2013Final Acceptance: February 6, 2014
TRANSLATION OF TREATMENT RELAPSE MODELS 449