Embed Size (px)
Citation preview

Clinical Pharmacology Review NDA #: 205175 Submission Date: December 26, 2012 Brand Name: Ecoza Generic Name: Econazole nitrate, 1% Dosage Form: Foam Dosage Strength: 1% Reviewer: Chinmay Shukla, Ph.D. Team Leader: Doanh Tran, Ph.D. Division Director: Capt. E. Dennis Bashaw, Pharm. D. OCP Division: DCP-3 OND Division: Division of Dermatology and Dental Products Sponsor: Amderma Pharmaceuticals LLC. Relevant IND(s): 077,523 Submission Type: New-submission Indication: Topical treatment of interdigital tinea pedis Table of Contents
1. Executive Summary * * * * * * * * 1 1.1 Recommendation * * * * * * * * * 2 1.2 Post-Marketing Requirements/Commitments * * * * * 2 1.3 Summary of Important Clinical Pharmacology and Biopharmaceutics Findings* 2 2. Question Based Review * * * * * * * * 4 2.1 General Attributes of the Drug * * * * * * * 4 2.2 General Clinical Pharmacology * * * * * * * 6 2.3 Intrinsic Factors * * * * * * * * * 14 2.4 Extrinsic Factors * * * * * * * * * 16 2.5 General Biopharmaceutics * * * * * * * 17 2.6 Analytical Section * * * * * * * * 18 3. Detailed Labeling Recommendations * * * * * * 19 4. Individual Trial Review * * * * * * * * 22
1. Executive Summary
This NDA submission is for econazole nitrate Foam, 1% and the Sponsor has proposed
(b) (4)
an indication for the treatment of interdigital tinea pedis caused by Trichophyton rubrum(b) (4)
, Trichophyton mentagrophytes, Trichophyton tonsurans, Epidermophyton floccosum
The Sponsor has adopted 505(b)(2) regulatory pathway and has identified Econazole nitrate Cream, 1% (NDA 018751, Spectazole®) as a listed drug. Econazole nitrate Cream, 1% is approved as a once daily application for the topical treatment of tinea pedis, tinea cruris and tinea corporis caused by Trichophyton rubrum, Trichophyton mentagrophytes, Trichophyton tonsurans, Microsporum canis, Microsporum audouini, Microsporum gypseum and Epidermophyton floccosum, in the treatment of cutaneous candidiasis and in the treatment of tinea versicolor.
1
Reference ID: 3364532

The clinical program consists of four Phase 1 dermal safety trials, two Phase 2 trials which include an adult pharmacokinetic (PK) trial to support a bridge between the Foam and Cream formulations and a pediatric PK trial in subjects 12 to 17 years of age under maximal use conditions and two Phase 3 trials.
1.1 Recommendation
From a Clinical Pharmacology standpoint, this application is acceptable provided the labeling comments are adequately addressed by the Sponsor.
1.2 Post-Marketing Requirements
Conduct in-vitro assessments to evaluate the following: 1. Inhibition potential of econazole nitrate for enzymes CYP1A2, 2B6, 2C8, 2C9,
2C19, 2D6 and 3A4. 2. Induction potential of econazole nitrate for enzymes CYP1A2, 2B6 and 3A.
Further in-vivo assessment to address drug interaction potential may be needed based on the results of the in-vitro assessment.
1.3 Summary of Important Clinical Pharmacology and Biopharmaceutics Findings
To support this NDA the Sponsor has conducted PK assessment in the following trials: • D79-2902-07: Phase 2 safety and efficacy trial in adults with interdigital and/or
moccasin type tinea pedis • 0792951-109: Phase 2 pediatric PK trial (12-17 year old) in subjects with
interdigital tinea pedis • 0792951-303: Phase 3 safety and efficacy trial
PK results: In the adult trial (D79-2902-07), 19 subjects (male and female) with tinea pedis applied 2.4 g of econazole nitrate Foam 1% once daily to soles, toes, interdigital spaces and tops of both feet up to the ankles for 29 days. Blood samples were obtained on Day 29 at pre-dose and 1, 2, 4, 6, 8, and 12 hours after application. Results (mean ± SD) showed the time to reach peak plasma concentrations (Tmax) was 6.8 ± 5.1 h with maximum concentration (Cmax) of 417 ±218 pg/ml. The area under the concentration time curve for the first 12 hours post application on Day 29 (AUC0-12) was 3440 ± 1920 pg-h/ml.
In the pediatric trial, 18 subjects (male and female ages 12 - 17) with interdigital tinea pedis and positive fungal cultures were treated with a mean daily amount of 3.2 g of econazole nitrate 1% Foam once daily to soles, toes, interdigital spaces and tops of both feet up to the ankles for 4 weeks. Blood samples were obtained on Day 28 at pre-dose and 7 h and 11 h post-dose. The mean ± SD econazole plasma concentration was 397 ± 289, 534 ± 745 and 575 ± 638 pg/mL at pre-dose and 7 h and 11 h post-dose, respectively.
2
Reference ID: 3364532

In adult subjects, the 90% confidence interval (CI) of the ratio of geometric means of AUC (0.73 to 1.87) and Cmax (0.74 to 1.46) of Foam vs. Cream were outside the no effect range of 0.8 to 1.25, suggesting that the Foam and the Cream are not bioequivalent. Based on ratio of geometric mean values, the Cmax of econazole appear to be similar (observed point estimate = 1.04), however, the exposure (AUC) of econazole following administration of the Foam formulation appears to be ~ 17% higher than the Cream (observed point estimate = 1.17).
In pediatric subjects (12-17 years) limited PK samples were obtained. The systemic econazole concentrations (geometric mean) appear to be approximately 2 fold higher at 7 h and 11 h post-dose following administration of the Foam formulation compared to the Cream.
Based on cross trial comparison, the geometric mean concentrations of econazole at 7 h and 11 h post-dose in pediatric subjects was ~ 1.7 and ~ 1.2 fold higher, respectively, than the 8 h and 12 h post-dose concentrations in adults, following administration of the Foam formulation.
In the Phase 3 trial (0792951-303), blood samples were analyzed for safety purpose only in subjects with ECG abnormalities. According to the Sponsor, single blood sample was obtained on Day 29 and Day 43 (or early termination) in 2 subjects with ECG abnormalities. Measurable econazole concentration was found only in 1 subject on Day 29 and this concentration was not higher than those observed in the PK trials.
Drug metabolism: According to the Sponsor, the pre-dose, 4 h and 12 h post-dose plasma samples on Day 29 from all subjects applying either econazole nitrate Foam or Cream from Trial D79-2902-07 (PK trial in adults) were examined for the presence of metabolites of econazole. This was an exploratory study for qualitative determination of the presence of metabolites. A sample from in-vitro hepatocyte incubation with econazole at 50 µM concentration was used as a control. Both a tandem mass spectrometer and a Quadrupole time-of-flight (Q-Tof) mass spectrometer with accurate mass capabilities were used to analyze the selected plasma samples. The Sponsor claims that the tandem mass spectrometer did show peaks at retention times similar to the econazole glucuronide metabolite in the plasma samples; however, the Q-Tof showed that these peaks were either noise or not related to econazole glucuronide metabolite that was identified in the in-vitro hepatocyte incubation study. Based on these results the presence of glucuronide metabolite of econazole is unlikely to be measurable at therapeutic doses.
Drug interactions: There have been cases of drug interactions between topical econazole nitrate and anticoagulant therapy with coumarins (warfarin and acenocoumarol) reported in the FDA Adverse Event Reporting System (FAERS) and medical literature. The Division of Dermatology and Dental Products (DDDP) requested Division of Pharmacovigilance (DPV) to evaluate the case reports in association with econazole use (see review dated 07/15/2013 by Dr. Jessica Weintraub in DARRTS under NDA 018751). DVP has recommended including language in all econazole labels regarding drug-drug interaction with warfarin, resulting in an increased anticoagulant effect of
3
Reference ID: 3364532

coumarins in association with topical econazole use. Clinical Pharmacology review on this issue can be found under NDA 018751 (see review by Dr. An-Chi Lu dated 08/28/2012 in DARRTS).
Formulation used: The adult PK trial (D79-2902-07) used the formulation manufactured in Sweden, while the pediatric PK trial (0792951-109) used the formulation manufactured in USA (commercial manufacturing site). The formulation was optimized during transfer and this included a change in the order of addition of the in-active ingredients. The overall composition of the formulation remained unchanged. The Sponsor has conducted in-vitro release test (IVRT) to bridge the formulation manufactured in Sweden and USA. According to Office of New Drugs Quality Assurance (ONDQA) reviewer Dr. Kelly Kitchens, the IVRT results are acceptable (for further details, see review in DARRTS by Dr. Kitchens).
QT prolongation: Based on the PK results of Trial D79-2902-07 (PK trial in adults), the Sponsor had applied for a waiver to conduct QT/QTc evaluations. Clinical Pharmacology concurred with Sponsor’s justification (see review in DARRTS dated 09/23/2009 under IND 077523 by Dr. Seongeun Cho).
Reviewer comments: Following administration of the Foam formulation, the systemic concentrations in pediatric was higher than adults, based on cross trial comparison. The highest mean (arithmetic mean) concentration in pediatrics was observed at the 11 hour post dose time point and it was 0.575 ng/mL. This concentration is ~1.5 nM (molecular weight of econazole = 381.68 g/mol), which is slightly above the sub-nanomolar threshold which is currently accepted by DDDP to waive TQT assessment for topical products. Considering the long history of econazole use and no QT related adverse events reported, the waiver for conducting TQT assessment is further justified.
Pediatric assessment: The Sponsor has conducted a pediatric PK trial (Trial 0792951109) under maximal use conditions in subjects 12 to 17 years of age with interdigital tinea pedis. For subjects 11 years of age and younger, the Sponsor has requested for a partial waiver of pediatric studies. At a meeting with the Pediatric Review Committee (PeRC) on 05/29/2013, PeRC agreed to the Sponsor’s partial waiver request.
Clinical Pharmacology Briefing: An optional intra-division level briefing was conducted on August 26, 2013 with the following in attendance: Hae-Young Ahn, E. Dennis Bashaw, Praveen Balimane, Jing Fang, Brian Chou, Gerald Tran, An-Chi Lu, Doanh Tran and Chinmay Shukla.
2. Question Based Review
2.1 General Attributes of the Drug
2.1.1 What are the highlights of the chemistry and physical-chemical properties of the drug substance and the formulation?
4
Reference ID: 3364532


Table 2:
Econazole nitrate 1% bulk Propellant (Butane, USP)
(b) (4)
(b) (4)
(b) (4)
2.1.2 What are the proposed mechanism of action and the therapeutic indications?
Mechanism of action: Econazole is an imidazole antifungal and drugs in this class act by inhibiting the biosynthesis of ergosterol which is a constituent of fungal cell membranes. Ergosterol serves as a bioregulator of membrane fluidity and is responsible for membrane integrity of in fungal cells.
Therapeutic indication: With this application, the Sponsor is seeking an indication of topical treatment of interdigital tinea pedis caused by Trichophyton rubrum, Tricophyton
(b) (4)mentagrophytes, Trichophyton tonsurans, Epidermophyton floccosum, (b) (4)
2.1.3 What is the proposed route of administration and dosage?
Proposed route of administration: Topical.
Proposed dosage: Once daily for 4 weeks.
2.2 General Clinical Pharmacology
2.2.1 What were the clinical trials conducted to support this NDA?
To support this application, the Sponsor has conducted four Phase 1 dermal safety trials, two Phase 2 trials which include an adult PK trial to support a bridge between the Foam and Cream and a pediatric PK trial under maximal use conditions and two Phase 3 trials. Table 3 shows a list of all clinical trials provided to support this application.
6
Reference ID: 3364532

Table 3: List of all clinical trials
Reference ID: 3364532
7

2.2.2 What are the design features of the clinical pharmacology and the clinical trials used to support dosing or claims?
Phase 2 - Design features of PK trial in adults (D79-2903-07): The primary objective of this trial was to substantiate a clinical bridge between econazole nitrate Foam, 1% and the listed drug econazole nitrate Cream, 1% based upon clinical outcome, safety, and plasma PK data. This was a multi-center, evaluator-blinded, randomized, vehicle controlled, parallel group comparison of econazole nitrate Foam, 1% with econazole nitrate Cream, 1% and the Foam vehicle. Approximately 135 subjects with tinea pedis who met the enrollment criteria with at least moderate scaling (interdigital and/or moccasin-type) and mild erythema (interdigital only) and a positive KOH finding were enrolled and randomized (1:1:1) to one of treatment arms.
The assigned study medication was applied once daily, preferably in the mornings for 4 weeks. Subjects were instructed to treat both feet by applying a thin uniform coat of the study medication over each foot in its entirety up to the inferior aspect of their ankles
8
Reference ID: 3364532

once a day (i.e., soles, toes, interdigital spaces and the top surfaces of both feet up to the ankles) independent of the area of disease involvement.
At the end of 4 weeks (Day 29), at selected PK sites, blood was drawn from all subjects at prior to the application of the last dose and at 1, 2, 4, 6, 8, and 12 hours post-dose to obtain plasma drug levels of econazole to determine the extent of systemic absorption following administration of the Cream and Foam formulations.
Phase 2 - Design features of maximal use PK trial in pediatrics (0792951-109): The primary objective of this trial was to compare the PK of econazole nitrate Foam, 1% with econazole nitrate Cream, 1% in subjects with interdigital tinea pedis aged 12 years to less than 18 years who were treated under maximal use conditions. This was a multi-center, randomized, double-blind, parallel-group trial.
Approximately 42 subjects who met the entry criteria were enrolled and randomized (1:1) to econazole nitrate, Foam 1% or the econazole nitrate, Cream 1% treatment group. The enrolled subjects had to have a clinical diagnosis of interdigital tinea pedis involving at least 2 web spaces in total extending no more than approximately 1 inch proximal to the web spaces or metatarsophalangeal joints; lesions were to have at least moderate scaling and mild erythema as defined as Grade 2 and Grade 1, respectively at Baseline.
The assigned investigational product was to be applied once daily in the morning for 4 weeks and subjects were instructed to apply a thin uniform coat of the investigational product to the soles, toes, interdigital spaces, and the tops of both feet (up to the ankles). The subjects were asked to avoid washing the treatment area for at least 4 hours after each application, continue treatment regardless of symptomatic improvement, and to record their dosing in a subject diary each day.
Subjects were also instructed to record the time at which they applied investigational product on the morning of Day 27 (approximately 24 hours prior to their final dose on Day 28) and to withhold application of their final dose pending blood draw for pre-lastdose PK assessment. Subjects were then to apply their final dose (Day 28) and provide blood samples at 7 hours (±1 hour) post-last-dose and at 4 hours (±1 hour) after the 7 hour blood draw. Baseline blood sample on (Day 1) were also obtained before the start of the treatment.
2.2.3 In which trials were PK assessed and what were the results?
To support this NDA the Sponsor has conducted PK assessment in the following trials as shown in Table 4:
9
Reference ID: 3364532

Table 4: List of trials with PK assessment Trial # Purpose Formulation
manufacturing site D79-2903-07 PK trial in adult subjects with tinea pedis to
establish a bridge between the Foam and Cream formulation
0792951-109 Maximal use PK trial in pediatric subjects aged 12 to < 18 years with interdigital tinea pedis
0792951-303 Phase 3 safety and efficacy trial – PK assessment conducted only in those subjects where ECG abnormalities were observed
(b) (4)
Summary of PK results of Trial D79-2903-07 (PK trial in adults): A summary of PK parameters for econazole nitrate following the administration of Cream and Foam formulation are shown in Table 5 below and the concentration versus time profile is shown in Figure 2.
Table 5: Summary of Mean ± SD PK parameters for Econazole following 29 days of once daily topical administration
Figure 2: Concentration (Mean ± SD) versus time profile on Day 29 for Econazole nitrate Foam, 1% and Cream 1%
10
Reference ID: 3364532

The 90% CI between the ratio of geometric means of the AUC and Cmax of econazole following administration of the Foam versus Cream formulation for all subjects in the PK population is shown in Table 6.
Table 6: 90% CI between the ratio of geometric means of AUC and Cmax following the administration of econazole nitrate Foam (Test) vs. Cream (Reference) for all subjects in the PK population
Reviewer comments: The 90% CI of the geometric means of AUC and Cmax of Foam vs. Cream were outside the no effect range of 0.8 to 1.25 suggesting that the Foam and the Cream are not bioequivalent. Based on the point estimate value, the exposure (AUC) of econazole nitrate following administration of the Foam formulation appears to be ~ 17% higher than the Cream.
Summary of PK results of Trial 0792951-109 (Maximal use PK trial in pediatrics): Limited PK samples were obtained in this trial and hence no PK parameters were estimated. Table 7 shows a summary of mean econazole concentrations assessed following administration of the Foam and Cream formulations and Table 8 shows geometric mean concentrations.
Table 7: Summary of Mean ± SD concentrations (pg/mL) of Econazole following Foam or Cream administrations
11
Reference ID: 3364532
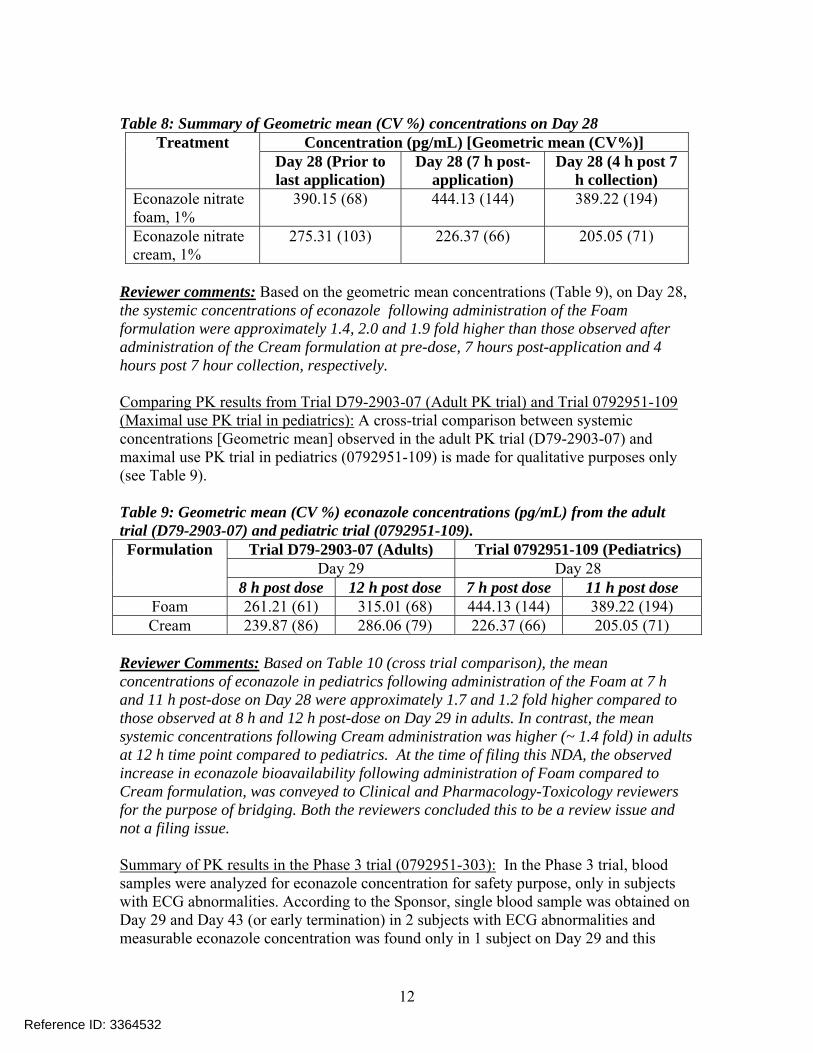
Table 8: Summary of Geometric mean (CV %) concentrations on Day 28 Treatment Concentration (pg/mL) [Geometric mean (CV%)]
Day 28 (Prior to last application)
Day 28 (7 h post-application)
Day 28 (4 h post 7 h collection)
Econazole nitrate foam, 1%
390.15 (68) 444.13 (144) 389.22 (194)
Econazole nitrate cream, 1%
275.31 (103) 226.37 (66) 205.05 (71)
Reviewer comments: Based on the geometric mean concentrations (Table 9), on Day 28, the systemic concentrations of econazole following administration of the Foam formulation were approximately 1.4, 2.0 and 1.9 fold higher than those observed after administration of the Cream formulation at pre-dose, 7 hours post-application and 4 hours post 7 hour collection, respectively.
Comparing PK results from Trial D79-2903-07 (Adult PK trial) and Trial 0792951-109 (Maximal use PK trial in pediatrics): A cross-trial comparison between systemic concentrations [Geometric mean] observed in the adult PK trial (D79-2903-07) and maximal use PK trial in pediatrics (0792951-109) is made for qualitative purposes only (see Table 9).
Table 9: Geometric mean (CV %) econazole concentrations (pg/mL) from the adult trial (D79-2903-07) and pediatric trial (0792951-109). Formulation Trial D79-2903-07 (Adults) Trial 0792951-109 (Pediatrics)
Day 29 Day 28 8 h post dose 12 h post dose 7 h post dose 11 h post dose
Foam 261.21 (61) 315.01 (68) 444.13 (144) 389.22 (194) Cream 239.87 (86) 286.06 (79) 226.37 (66) 205.05 (71)
Reviewer Comments: Based on Table 10 (cross trial comparison), the mean concentrations of econazole in pediatrics following administration of the Foam at 7 h and 11 h post-dose on Day 28 were approximately 1.7 and 1.2 fold higher compared to those observed at 8 h and 12 h post-dose on Day 29 in adults. In contrast, the mean systemic concentrations following Cream administration was higher (~ 1.4 fold) in adults at 12 h time point compared to pediatrics. At the time of filing this NDA, the observed increase in econazole bioavailability following administration of Foam compared to Cream formulation, was conveyed to Clinical and Pharmacology-Toxicology reviewers for the purpose of bridging. Both the reviewers concluded this to be a review issue and not a filing issue.
Summary of PK results in the Phase 3 trial (0792951-303): In the Phase 3 trial, blood samples were analyzed for econazole concentration for safety purpose, only in subjects with ECG abnormalities. According to the Sponsor, single blood sample was obtained on Day 29 and Day 43 (or early termination) in 2 subjects with ECG abnormalities and measurable econazole concentration was found only in 1 subject on Day 29 and this
12
Reference ID: 3364532

concentration was not higher than those observed in the PK trials. Specifically Subject 14-005 had Baseline, Day 29 and Day 43 blood concentrations below the level of quantification (BLQ) while Subject 03-016 had Baseline and early termination (Day 36) concentrations BLQ, but on Day 29, the systemic concentration of econazole was 216 pg/mL.
2.2.4 What information is known about drug metabolism?
According to the Sponsor, the pre-dose, 4 h and 12 h post-dose plasma samples on Day 29 from all subjects applying either econazole nitrate Foam or Cream from Trial D792902-07 (PK trial in adults) were examined for the presence of metabolites of econazole. This was an exploratory study for qualitative determination of the presence of metabolites. A sample from in-vitro hepatocyte incubation with econazole at 50 µM concentration was used as a control. Both a tandem mass spectrometer and a Quadrupole time-of-flight (Q-Tof) mass spectrometer with accurate mass capabilities were used to analyze the selected plasma samples. The Sponsor claims that the tandem mass spectrometer did show peaks at retention times similar to the econazole glucuronide metabolite in the plasma samples; however, the Q-Tof showed that these peaks were either noise or not related to econazole glucuronide metabolite that was identified in the in-vitro hepatocyte incubation study. Based on these results the presence of glucuronide metabolite of econazole is unlikely to be measurable at therapeutic doses.
2.2.6 What is the safety profile of econazole?
The clinical safety of econazole nitrate Foam 1% was evaluated over the course of eight clinical trials (four Phase 1 trials, two Phase 2 trials, and two Phase 3 trials). According to the Sponsor, in the Phase 1 trials, econazole nitrate Foam 1% was safe, with no dermal irritation, dermal sensitization, phototoxicity, or photosensitization observed, and a very low rate of adverse events (AEs) of mild to moderate severity, reported. The Sponsor has further reported that the two Phase 2 PK trials showed comparable safety outcomes between the Foam and the reference product Cream and no AEs or systemic toxicity were observed. In the Phase 3 trial 079-2951-303, which included an econazole nitrate Cream 1% comparator group, the Sponsor has claimed that the number of subjects reporting at least one AE was similar between all treatment groups. In the two Phase 3 trials, the Sponsor has reported the AEs to be generally mild and the most common ones were local irritation, headache and nasopharyngitis. Severe AEs have been reported in 6 subjects in the combined safety population and these include hypertension, pain associated with kidney stone, pain associated with hernia surgery, localized infection and musculoskeletal pain. All these were deemed not related to the treatment by the Sponsor. There were no deaths reported in any of the clinical trials.
Reviewer comments: For additional information on safety, please see review by medical officer Dr. Amy Woitach in DARRTS.
2.2.7 Has the potential for QT prolongation adequately addressed?
13
Reference ID: 3364532

Based on the PK results of Trial D79-2902-07 (PK trial in adults), the Sponsor had applied for a waiver to conduct QT/QTc evaluations. Clinical Pharmacology concurred with Sponsor’s justification (see review in DARRTS dated 09/23/2009 under IND 077523 by Dr. Seongeun Cho).
Reviewer comments: Following administration of the Foam formulation, the systemic concentrations in pediatric was higher than adults, based on cross trial comparison. The highest mean (arithmetic mean) concentration in pediatrics was observed at the 11 hour post dose time point and it was 0.575 ng/mL. This concentration is ~1.5 nM (molecular weight of econazole = 381.68 g/mol), which is slightly above the sub-nanomolar threshold which is currently accepted by DDDP to waive TQT assessment for topical products. Considering the long history of econazole use and no QT related adverse events reported, the waiver for conducting TQT assessment is further justified.
2.3 Intrinsic Factors
2.3.1 What intrinsic factors (age, gender, race, weight, height, disease, genetic polymorphism, pregnancy, and organ dysfunction) influence exposure (PK usually) and/or response, and what is the impact of any differences in exposure on efficacy or safety responses?
2.3.1.1 Effect of gender
The effect of gender on PK of econazole nitrate was not explored.
2.3.1.2 Effect of disease
In the adult PK trial (D79-2902-07), the Sponsor evaluated the effect of disease state on PK of econazole nitrate (see Table 10 and 11) by comparing the AUC and Cmax obtained from subjects with healed skin and not-healed skin.
Table 10: PK parameters in healed and not-healed skin PK Parameters Healed Skin Not-healed skin
(Geometric mean) Foam (n=2) Cream (n=6) Foam (n=11) Cream (n=9) AUC (pg*h/mL) 3184.5 1663.5 2830.6 2510.6 Cmax (pg/mL) 361.6 317.4 384.6 314.8
Table 11: Effect of disease state on PK of econazole nitrate Ratio (Not-healed/Healed) AUC (pg*h/mL) Cmax (pg/mL)
Foam 0.88 1.06 Cream 1.51 0.99
Reviewer comments: The exposure (AUC) of econazole in the Cream arm appears to be slightly higher in subjects with not-healed skin compared to healed skin. While in the Foam arm; it appears that disease resolution had minimal effect on PK. Any definitive conclusions cannot be made because of limited number of subjects.
14
Reference ID: 3364532

The Sponsor has also provided statistical analysis by calculating the 90% CI of the ratio of geometric mean of AUC and Cmax following administration of the Foam and Cream formulation in subjects with healed and not healed skin (also included is data in subjects whose disease state is unknown) (see Table 12).
Table 12: 90% CI between the ratio of geometric means of AUC and Cmax following the administration of econazole nitrate Foam (Test) vs. Cream (Reference) based on subgroup analysis by disease condition
15
Reference ID: 3364532

Reviewer comments: From the data in the healed vs. not-healed skin, the systemic levels of econazole following administration of the Foam formulation appears to be higher than Cream. The same observation cannot be made in subjects with “unknown” disease state, which shows opposite effect. However, it should be noted that these observations are based on limited data, especially in the Foam arm which had only 2 subjects with healed skin.
2.3.1.3 Pediatric subjects
The Sponsor has conducted a pediatric PK trial (Trial 0792951-109) under maximal use conditions in subjects 12 to 17 years of age with interdigital tinea pedis. For subjects 11 years of age and younger, the Sponsor has requested for a partial waiver of pediatric studies. At a meeting with the Pediatric Review Committee (PeRC) on 05/29/2013, PeRC agreed to the Sponsor’s partial waiver request.
2.3.1.4 Renal impairment
The Sponsor has not evaluated PK in subjects with renal impairment.
2.3.1.5 Hepatic impairment
The Sponsor has not evaluated PK in subjects with hepatic impairment.
2.3.1.6 What pregnancy and lactation use information is there in the application?
The Sponsor has not evaluated PK in pregnant and /or lactating females.
2.4 Extrinsic Factors
2.4.1 What extrinsic factors (drugs, herbal products, diet, smoking, and alcohol use) influence dose-exposure and/or response and what is the impact of any differences in exposure or response?
The influence of extrinsic factors on dose-exposure and/or response was not explored.
2.4.2 Drug interactions
There have been cases of drug interactions between topical econazole nitrate and anticoagulant therapy with coumarins (warfarin and acenocoumarol) reported in the FDA Adverse Event Reporting System (FAERS) and medical literature. The Division of Dermatology and Dental Products (DDDP) requested Division of Pharmacovigilance (DPV) to evaluate the case reports in association with econazole use (see review dated 07/15/2013 by Dr. Jessica Weintraub in DARRTS under NDA 018751). DVP has recommended including language in all econazole labels regarding drug-drug interaction with warfarin, resulting in an increased anticoagulant effect of coumarins in association
16
Reference ID: 3364532


2.6 Analytical Section
2.6.1 How are the active moieties identified, and measured in the plasma and urine in the clinical pharmacology and biopharmaceutics studies?
Econazole concentrations were identified using high performance liquid chromatography (HPLC) with tandem quadrupole mass spectrometric (MS/MS) detection.
2.6.2 Which metabolites have been selected for analysis and why?
In the adult PK trial (D79-2902-07), the Sponsor had attempted to assess the presence of metabolites in selected PK samples. The Sponsor claims that since none of the metabolites were identified they were not selected for analysis. Further, this is a 505(b)(2) application and relative bioavailability of parent is usually adequate and assessment of metabolites is usually not needed.
2.6.3 For all moieties measured, is free, bound, or total measured?
Total concentrations for econazole were measured.
2.6.4 What is the range of the standard curve? How does it relate to the requirements for clinical studies?
Range: 100 pg/mL to 50,000 pg/mL.
This range was adequate as none of the plasma concentrations for econazole in the clinical trials exceeded the upper limit of 50,000 pg/mL.
Reviewer comments: Bioanalytical work for all the clinical trials was performed by (b) (4)
2.6.5 What are the accuracy and precision at LLOQ?
Within-run accuracy % 3.37 Between-run accuracy % 5.21 Within-run precision % 4.00 Between-run precision % 8.00
2.6.6 What is the sample stability under the conditions used in the study (long-term, freeze-thaw, sample-handling, sample transport, autosampler, etc.)?
Freeze/Thaw cycle stability Stable for 3 cycles at -70 ºC Room temperature stability 25 hours Refrigeration stability 76 hours at 5 ºC Long term stability 188 days at -70 ºC
18
Reference ID: 3364532



(b) (4)
APPPEARS THIS WAY ON ORIGINAL
21
Reference ID: 3364532

4. INDIVIDUAL TRIAL REVIEW
Trial number D79-2902-07: Adult PK bridging trial
Title: A Multi-Center Randomized, Evaluator-Blinded, Vehicle Controlled, Parallel Group Comparison Study of the Safety and Efficacy of Econazole Nitrate Foam 1%, Econazole Nitrate 1% Cream and Foam Vehicle in Subjects with Tinea Pedis
Trial objectives: Primary: To provide support in establishing a clinical bridge between Econazole Nitrate Foam 1% and the reference product based upon clinical outcome, safety, and PK data.
Secondary: To determine and compare the safety, including local tolerability, and efficacy of Econazole Nitrate Foam 1%, with Econazole Nitrate Cream 1%, and Foam vehicle in subjects with tinea pedis.
Trial drugs: • Econazole Nitrate Foam 1% (Lot #M7036) administered once a day (QD)
(Formulation manufacturing site - Sweden) • Econazole Nitrate Cream 1% (Fougera) (Lot #Z80) administered once a day (QD) • Foam Vehicle (Lot #M7035) administered once a day (QD)
Primary efficacy endpoint: Complete cure indicated by negative KOH and negative fungal culture and no evidence of clinical disease at Day 43.
Secondary efficacy endpoints: • Effective Treatment: negative KOH, negative fungal culture, no or mild (a score
of 0 or 1) erythema and/or scaling with all other signs or symptoms being absent (score = 0) at Day 43 (Week6).
• Mycological cure: negative KOH and negative culture at Day 43 (Week 6). • Clinical Improvement defined as responses of good, very good, or excellent as
determined from Investigator and Subject Assessments at Day 29 (Week 4) and Day 43 (Week 6).
• Changes from baseline in individual and cumulative signs and symptoms of disease (erythema, scaling/hyperkeratosis, cracking/fissuring, maceration, vesiculation and pruritus) for each type of tinea pedis at each visit on a zero (none) to three (severe) point scale.
Safety endpoints: • Plasma levels of Econazole Nitrate at the end of treatment. • Tolerability of treatment, local and systemic adverse events at each visit. • Laboratory data: hematology, serum chemistry, and urinalyses at Baseline and
Day 29.
Trial design: Subjects with tinea pedis with at least moderate scaling (Interdigital and/or Moccasin-type) and mild erythema (Interdigital only) and a positive KOH finding at the
22
Reference ID: 3364532

Screening/Baseline visit and those who met the enrollment criteria were enrolled and randomized (1:1:1) to each of treatment arm.
198 subjects were screened and 135 were enrolled/randomized in the trial as follows: • 43 subjects were randomized to Econazole Nitrate (EN) Foam, 1% • 45subjects were randomized to Econazole Nitrate Cream, 1% • 47 subjects were randomized to Foam Vehicle
The assigned study medication was applied once daily, preferably in the mornings for 4 weeks. Subjects were instructed to treat both feet by applying a thin uniform coat of the study medication over each foot in its entirety up to the inferior aspect of their ankles once a day (i.e., soles, toes, interdigital spaces and the top surfaces of both feet up to the ankles) independent of the area of disease involvement. Given the physical differences in the two “active” dosage forms (Foam and Cream), particular care was taken to assure the clinical evaluator was “blinded” with respect to the medication type dispensed to the subjects.
At Days 8 and 15, safety evaluation and clinical grading was performed and dermatophyte cultures taken at the Baseline visit were reviewed to ensure that subjects were eligible to continue in the trial. Subjects with negative Baseline dermatophyte cultures, exclusive of subjects participating in the PK aspect of the trial, were discontinued.
At the end-of-treatment (Day 29), safety evaluation, clinical grading and repeat KOH test and mycological culture were performed. All subjects were asked to withhold the last morning application of the study medication until after skin scrapings (specimens for KOH and cultures) had been collected. At this visit, all subjects had blood drawn to obtain end-of-treatment labs.
At the end of 4 weeks (Day 29), at selected PK sites, blood was drawn from all subjects at prior to the application of the last dose and at 1, 2, 4, 6, 8, and 12 hours post-dose to obtain plasma drug levels of Econazole nitrate to determine the extent of systemic absorption following administration of the Cream and Foam formulations.
At the end of study (Day 43), subjects with positive Baseline fungal cultures returned for the final visit for clinical evaluations and repeat KOH testing and mycological cultures were performed. At each visit, adverse reactions including local skin reactions, concurrent procedures, and changes in concomitant medications during the study were recorded.
Overall there were 63 subjects that were screen failures because of negative KOH evaluations. Figure 3 shows a schematic representation of the disposition of subjects in this trial.
23
Reference ID: 3364532

Figure 3: Disposition of Subjects
Definitions of the populations: Intent-to-Treat Population (ITT): All subjects enrolled in the trial that were randomized, and dispensed the study medication were considered in the ITT population. ITT also includes subjects who discontinued prematurely from the trial following administration of study medication (e.g., subjects who were found to lack a positive Baseline fungal culture) were included in the ITT population. No efficacy analyses were conducted on the ITT population.
Modified Intent-to-Treat Population (MITT): All subjects enrolled in the trial who were randomized and dispensed the study medication, and who had a positive Baseline fungal culture were included in the MITT population, a subset of the ITT population.
24
Reference ID: 3364532


Demographics: MITT population demographics are shown in Table 14 below and in Table 15, population by treatment group and subject sub-group is shown.
Table 14: Demographics of the MITT population
Table 15: MITT population by treatment and subject sub-groups
Subject disposition: A summary of subject disposition for all enrolled subjects is shown in Table 16.
26
Reference ID: 3364532

Table 16: Summary of subject disposition for all enrolled subjects
Baseline characteristics: Description of disease sub-type and mycology at baseline in MITT population is shown in Table 17.
Table 17: Baseline characteristics of MITT population
PK results: Table 18 shows the mean PK parameters of econazole following 29 Days of once-daily topical application of Foam, Cream or Foam Vehicle and the mean concentration versus time profile is shown in Figure 4
27
Reference ID: 3364532

Table 18: Summary of Mean ± SD PK parameters for econazole following 29 days of once daily topical administration
Figure 4: Concentration (Mean ± SD) versus time profile on Day 29 for econazole nitrate Foam, 1% and Cream 1%
The 90% confidence interval (CI) between the ratio of geometric means of the AUC and Cmax of econazole nitrate following administration of the Foam versus Cream formulation for all subjects in the PK population is shown in Table 19. Further, the 90% CI between the ratio of geometric means of the AUC and Cmax of econazole nitrate following administration of the Foam versus Cream formulation based on subgroup analysis by disease type is shown in Table 20.
28
Reference ID: 3364532

Table 19: 90% CI between the ratio of geometric means of AUC and Cmax following the administration of econazole nitrate Foam (Test) vs. Cream (Reference) for all subjects in the PK population
Reviewer comments: The 90% CI of the geometric means of AUC and Cmax of Foam vs. Cream are outside the no effect range of 0.8 to 1.25 suggesting that the Foam and the Cream are not bioequivalent. Based on the point estimate value, the exposure (AUC) of econazole nitrate following administration of the Foam formulation appears to be ~ 17% higher than the Cream.
Table 20: 90% CI between the ratio of geometric means of AUC and Cmax following the administration of econazole nitrate Foam (Test) vs. Cream (Reference) based on subgroup analysis by disease type
29
Reference ID: 3364532

Reviewer comments: The 90% CI of the geometric means of Cmax and AUC of Foam vs. Cream are outside the no effect range of 0.8 to 1.25 suggesting that the Foam and the Cream are not bioequivalent in all the sub-analysis categories. Furthermore, the systemic exposure (AUC) of econazole was slightly higher following Foam administration compared to the Cream. However, due to limited number of subjects, any strong conclusions cannot be made.
Effect of disease: The Sponsor evaluated the effect of disease state on PK of econazole (see Table 21 and 22) by comparing the AUC and Cmax obtained from subjects with healed skin and not-healed skin.
Table 21: PK parameters in healed and not-healed skin PK Parameters Healed Skin Not-healed skin
(Geometric mean) Foam (n=2) Cream (n=6) Foam (n=11) Cream (n=9) AUC (pg*h/mL) 3184.5 1663.5 2830.6 2510.6 Cmax (pg/mL) 361.6 317.4 384.6 314.8
Table 22: Effect of disease state on PK of econazole nitrate Ratio (Not-healed/Healed) AUC (pg*h/mL) Cmax (pg/mL)
Foam 0.88 1.06 Cream 1.51 0.99
Reviewer comments: The exposure (AUC) of econazole in the Cream arm appears to be slightly higher in subjects with not-healed skin compared to healed skin. While in the Foam arm; it appears that disease resolution had minimal effect on PK. Any definitive conclusions cannot be made because of limited number of subjects.
The Sponsor has also provided statistical analysis by calculating the 90% CI of the ratio of geometric mean of AUC and Cmax following administration of the Foam and Cream formulation in subjects with healed and not healed skin (also included is data in subjects whose disease state is unknown) (see Table 23).
30
Reference ID: 3364532

Table 23: 90% CI between the ratio of geometric means of AUC and Cmax following the administration of econazole nitrate Foam (Test) vs. Cream (Reference) based on subgroup analysis by disease condition
Reviewer comments: From the data in the healed vs. not-healed skin, the systemic levels of econazole following administration of the Foam formulation appears to be higher than Cream. The same observation cannot be made in subjects with “unknown” disease state, which shows opposite effect. This observation is backed by limited data especially in the Foam arm which had only 2 subjects with healed skin.
31
Reference ID: 3364532
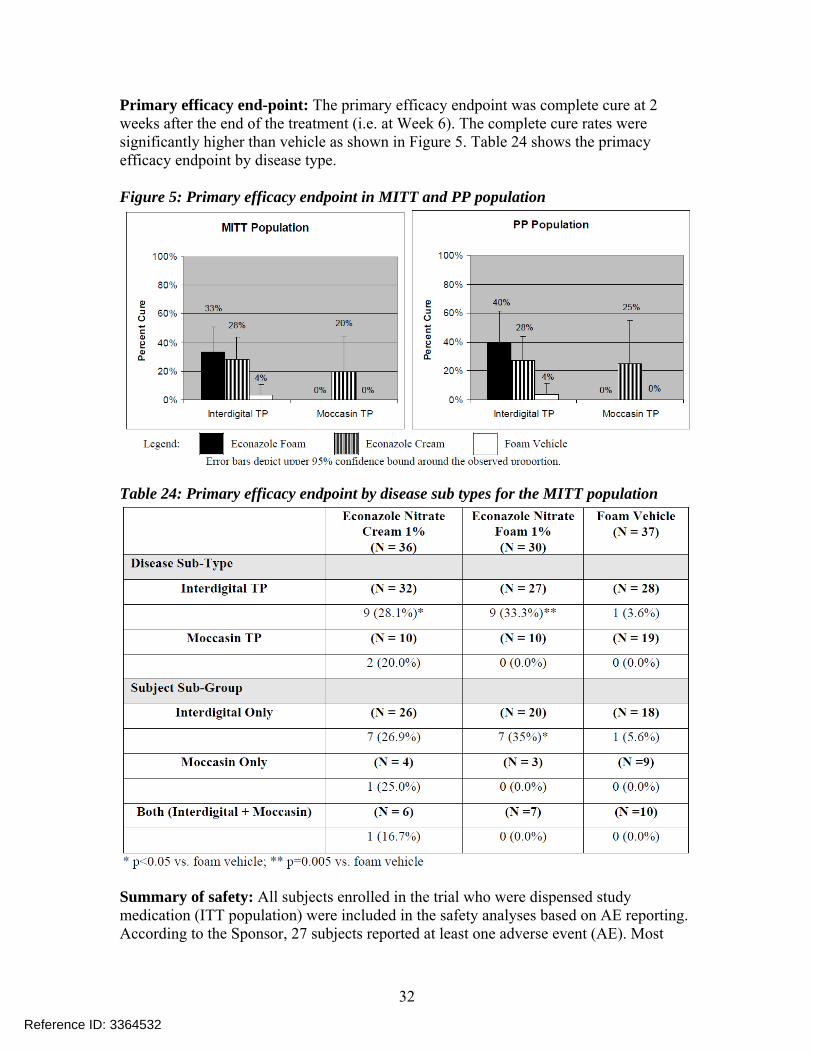
Primary efficacy end-point: The primary efficacy endpoint was complete cure at 2 weeks after the end of the treatment (i.e. at Week 6). The complete cure rates were significantly higher than vehicle as shown in Figure 5. Table 24 shows the primacy efficacy endpoint by disease type.
Figure 5: Primary efficacy endpoint in MITT and PP population
Table 24: Primary efficacy endpoint by disease sub types for the MITT population
Summary of safety: All subjects enrolled in the trial who were dispensed study medication (ITT population) were included in the safety analyses based on AE reporting. According to the Sponsor, 27 subjects reported at least one adverse event (AE). Most
32
Reference ID: 3364532

subjects experienced AEs that were mild or moderate in severity and as per the Sponsor, the AEs were considered not related to study medication. Only two AEs were reported as severe: one in the Cream group that was not related and one in the Foam Vehicle group. AE rates were similar across the two active treatment groups with the fewest AEs being reported in the foam vehicle group. There were no deaths or SAEs that led to treatment interruption.
Reviewer comments: For further information see review by the medical office Dr. Amy Woitach in DARRTS.
Trial number 0792951-109: Pediatric PK trial
Title: A Multi-Center, Randomized Comparative Study of the Pharmacokinetics of Econazole Nitrate 1% Foam and Econazole Nitrate 1% Cream in Subjects with Interdigital Tinea Pedis Aged 12 Years to Less Than 18 Years
Trial objective: The primary objective of the study was to compare the PK of econazole nitrate Foam 1% with econazole nitrate Cream 1% in subjects with interdigital tinea pedis aged 12 years to less than 18 years who were treated under maximal use conditions.
Trial design: Approximately 42 subjects who met the entry criteria were enrolled and randomized (1:1) to econazole nitrate, Foam 1% or the econazole nitrate, Cream 1% treatment group. The enrolled subjects had to have a clinical diagnosis of interdigital tinea pedis involving at least 2 web spaces in total extending no more than approximately 1 inch proximal to the web spaces or metatarsophalangeal joints; lesions were to have at least moderate scaling and mild erythema as defined as Grade 2 and Grade 1, respectively at Baseline.
The assigned investigational product was to be applied once daily in the morning for 4 weeks and subjects were instructed to apply a thin uniform coat of the investigational product to the soles, toes, interdigital spaces, and the tops of both feet (up to the ankles). The subjects were asked to avoid washing the treatment area for at least 4 hours after each application, continue treatment regardless of symptomatic improvement, and to record their dosing in a subject diary each day.
Subjects were also instructed to record the time at which they applied investigational product on the morning of Day 27 (approximately 24 hours prior to their final dose on Day 28) and to withhold application of their final dose pending blood draw for pre-lastdose PK assessment. Subjects were then to apply their final dose (Day 28) and provide blood samples at 7 hours (±1 hour) post-last-dose and at 4 hours (±1 hour) after the 7 hour blood draw. Baseline blood sample on (Day 1) were also obtained before the start of the treatment.
At each visit, including the Screening/Baseline visit, any adverse events (AEs) including local skin reactions, concurrent procedures, and changes in concomitant medications
33
Reference ID: 3364532


Subject enrollment: A total of 50 subjects were randomized (25 each in the Econazole nitrate Foam, 1% and Econazole nitrate Cream, 1% groups, respectively). All randomized subjects were included in the MITT Population. Seventeen subjects were excluded from the PK analysis (PKIN) population. Specifically 7 subjects in the Foam arm, and 9 in the Cream arm that were excluded due to a negative baseline fungal culture and 1subject in the Cream arm was excluded due to incomplete PK blood collections [Subject (08-006) moved out of the country and did not complete Day 28/Visit 3]. Summary is shown in Table 26 and 27.
Table 26: Summary of subject enrollment:
Table 27: Summary of disqualified subjects from PKIN population:
Demographics: Subject demographics are shown in Table 28.
35
Reference ID: 3364532

Table 28: Summary of subject demographics
Amount of formulation used (PKIN Subjects): The mean amount of Foam used was 3.2 g/day and the mean amount of Cream used was 3.9 g/day (see Table 29).
Table 29: Summary of the amount of formulation used
36
Reference ID: 3364532

Analysis of Efficacy: Investigator assessment of response to treatment at Day 28 (end of treatment) is summarized in Table 30. According to the Sponsor, in the Foam and the Cream groups the majority of investigator assessments of responses to treatment were recorded as excellent or very good.
Table 30: Summary of investigator response to treatment
PK results: Since limited PK samples were obtained in this trial, no PK parameters were estimated. Table 31 shows a summary of mean econazole concentrations assessed following administration of the Foam and Cream formulations and Table 32 shows geometric mean concentrations.
Table 31: Summary of Mean ± SD concentrations (pg/mL) of Econazole following Foam or Cream administrations
37
Reference ID: 3364532

Table 32: Summary of Geometric mean (CV %) concentrations on Day 28 Treatment Concentration (pg/mL) [Geometric mean (CV %)]
Day 28 (Prior last application)
Day 28 (7 h post-application)
Day 28 (4 h post 7 h collection)
Econazole nitrate foam, 1%
390.15 (68) 444.13 (144) 389.22 (194)
Econazole nitrate cream, 1%
275.31 (103) 226.37 (66) 205.05 (71)
Reviewer comments: Based on the geometric mean concentrations (Table 9), on Day 28, the systemic concentrations of econazole following administration of the Foam formulation were approximately 1.4, 2.0 and 1.9 fold higher than those observed after administration of the Cream formulation at pre-dose, 7 hours post-application and 4 hours post 7 hour collection, respectively.
Summary of safety: No AEs, SAEs, or deaths were reported and no subject discontinued treatment.
Reviewer comments: For further information see review by the medical office Dr. Amy Woitach in DARRTS.
38
Reference ID: 3364532

---------------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------------
----------------------------------------------------
This is a representation of an electronic record that was signed electronically and this page is the manifestation of the electronic signature.
/s/
CHINMAY SHUKLA 08/28/2013
DOANH C TRAN 08/28/2013
EDWARD D BASHAW 08/29/2013 Concur with proposed PMR
Reference ID: 3364532





























