Embed Size (px)
DESCRIPTION
Clinical Pharmacology
Citation preview

Pediatrics in Review Vol. 19 No. 12 December 1998 423
ARTICLE
DefinitionPharmacology in its broader senserefers to the history, chemicophysi-cal properties, source, biochemicaland physiological effects, disposi-tion, mechanisms of action, andtherapeutic and nontherapeutic usesof drugs. This definition obviouslyis beyond the interest of most clini-cians. The demand for a clinicallyoriented discipline has led to thedevelopment of clinical pharma-cology, which focuses on the effectsof drugs in humans.
The subdiscipline of pediatricclinical pharmacology presents difficult challenges. Rapid and significant age-related physiologicchanges, especially during the first year of life, dictate a dynamicyet cautious therapeutic approach. Furthermore, despite a significantincrease in the knowledge of drugdisposition in infants and children
over the past few years, pharma-cokinetic/pharmacodynamic inter-actions remain poorly understood.Finally, many obstacles preventrational and timely accumulation of important data about drug han-dling and response in children. Only recently have pediatric clini-cal pharmacology studies beenexpected by the United States Foodand Drug Administration (FDA) asan integral part of regulatory reviewfor all agents used in children.Hopefully this will lead toward evidence-based pharmacotherapy in the pediatric population.
EpidemiologyAccording to one report, an averageof 0.9 medication per patient-contactis prescribed in pediatric practicecompared with 1.1 drugs perpatient-contact for all the disci-plines together. By their first 5 yearsof life, 95% of children have beenprescribed medications, with anaverage of 8.5 courses of prescrip-tions and 5.5 different medications.Within this 5-year period, the great-est number of prescriptions is given
to children between 7 and 12 monthsof age. These data, together with thelimited clinical drug trials that havebeen conduced in infants and chil-dren, suggest the need for a moreevidence-based approach similar tothe pharmacotherapy employed inother age groups.
Pharmacokinetic Principlesin Neonates and Infants andTheir Clinical RelevanceNeonates and infants represent anunstable pharmacokinetic condition.Special attention must be paid topharmacokinetic variables as rapidand significant age-related changesin drug absorption, distribution, and clearance occur in the first few months of life.
DRUG ABSORPTION
Drug absorption in infants and children follows the same generalprinciples as in adults, but becauserelatively more sites of drug admin-istration are used in neonates, spe-cial considerations must be paid tothe different determinants affectingdrug absorption from each site.
Absorption from the Gastrointestinal(GI) Tract
Diminished intestinal motility anddelayed gastric emptying in neo-nates and infants result in a longerperiod of time for a drug to reachsimilar plasma concentrations ininfants as in older children after oral administration. Oral absorptionof acetaminophen, phenobarbital,and phenytoin, reflected in part bybioavailability, has been shown tobe lower in infants than in olderchildren and adults (Table 1).
Different flora colonize the sterilefetal intestine, depending on whetherthe newborn is breastfed or formula-fed. The change in bacterial floraduring the newborn period affectsthe hydrolysis of drug conjugatesthat are excreted in bile. Absorption
Clinical Pharmacology and Therapeutic Drug Monitoring in Neonates and ChildrenRonen Loebstein, MD* and Gideon Koren, MD*
IMPORTANT POINTS
1. Neonates and children exhibit unstable pharmacokinetics, and knowl-edge of age-related changes in drug absorption, distribution, andclearance is essential to optimize drug efficacy and avoid toxicity.
2. Measurement of drug concentrations at times of the expected peak ortrough is crucial for accurate interpretation and subsequent dosing;lack of knowledge of the time of drug delivery to the patient orrandom sampling will result in useless therapeutic drug monitoring.
3. Administration of drugs that inhibit hepatic drug metabolism (such ascimetidine, erythromycin, ciprofloxacin, or omeprazole) concomitantlywith drugs metabolized by the liver that have a narrow therapeuticrange may lead to increased plasma concentrations and, therefore,toxicity.
4. Explaining the nature of the illness and providing precise instructionsabout treatment, including the names and purposes of the drug(s) prescribed and specific instructions about dosage, have been demonstrated to improve compliance.
5. Although most drugs are excreted into human milk by passive diffusion, the amount ingested by the infant rarely is sufficient toattain therapeutic concentrations or cause adverse effects.
*Division of Clinical Pharmacology andToxicology, Department of Pediatrics andPopulation Health Sciences, Research Institute, The Hospital for Sick Children,University of Toronto, Toronto, Ontario,Canada.

424 Pediatrics in Review Vol. 19 No. 12 December 1998
of vitamin K and other lipid-solublevitamins also is influenced by thedevelopment of intestinal flora.
Disease conditions such as diar-rhea, giardiasis, cystic fibrosis, andceliac disease might interfere withdrug absorption from the GI tract.
Rectal Administration of Drugs
Rectal drug administration may beuseful in conditions such as nauseaand vomiting and status epilepticus,for induction of anesthesia, and foradministration of drugs that have alarge first-pass effect (blood suppliesto the anus and lower rectum draindirectly into the inferior vena cava).Solutions of diazepam have beendemonstrated to be well absorbedfrom the rectum compared with suppositories, for which absorption is erratic and incomplete. In light of its poor absorption from intra-muscular injection sites, rectaladministration of diazepam solutionsoffers effective anticonvulsive andsedative therapy, especially becausediazepam bioavailability has beenshown to be higher after rectal thanoral administration.
In addition to benzodiazepines,barbiturates have been administeredrectally to children with great suc-cess. Rectal diazepam has been used effectively in the treatment of febrile seizures. Similarly, rec-tally administered midazolam andatropine for other indications wereclinically more effective than intra-muscular administration.
Absorption from IntramuscularInjection Sites
Local and drug-related factors arethe most important determinantsaffecting drug absorption after intramuscular injection. Blood supply and flow to and from theinjected muscle are the most im-portant local factors. Clinical con-ditions such as low cardiac output,respiratory distress syndrome, andother circulatory disturbances may compromise blood supply tothe muscles severely, leading todecreased absorption from the injection site. The degree of muscu-lar activity affects primarily the rateof drug absorption from intramuscu-lar sites. Immobile infants demon-strate slower absorption rates fromintramuscular injection sites; exer-cise may enhance drug absorption,as has been demonstrated for insulinand exercise-induced hypoglycemia.
Phenytoin provides a classicexample of drug-related factorsaffecting absorption from intramus-cular injection sites. This drug’s pKis 9.2, and the acid form is insolublein water. Because the muscle envi-ronment is more acidic than blood,the sodium salt of phenytoin is con-verted into the acid form, which precipitates at the site of injection.This results in slow and erraticabsorption of phenytoin from intramuscular sites.
More rapid absorption followingintramuscular administration hasbeen demonstrated for benzathinepenicillin and clindamycin in thepediatric age group compared with adults.
DRUG DISTRIBUTION AND PROTEIN BINDING
Drug distribution and protein bind-ing in neonates and children are dictated by changes in body compo-sition that occur with development.The total body water compartment is larger among preterm neonates(85% of total body weight) com-pared with term neonates (70% to75%) and adults (50% to 60%).Similarly, the extracellular watercompartment is 40% of body weightin the neonate compared with 20%in the adult. These data are clini-cally relevant because many drugs,especially water-soluble ones (eg,aminoglycosides), are distributed
throughout the extracellular watercompartment. Therefore, the volumeof the extracellular water compart-ment determines drug concentrationat the receptor site. Conversely, totalbody fat in preterm infants is 1% oftotal body weight compared with15% in term neonates. This affectslipid-soluble drugs such as digoxin,which may accumulate in smalleramounts in immature infants.
Another determinant of drug distribution is protein binding. Generally, neonates, especiallypreterm neonates, are at risk ofaltered drug-protein interaction.Decreased plasma concentrations of total protein and albumin in newborns and infants lead todecreased drug-protein binding. In vitro studies comparing free drug concentrations in cord bloodand adult plasma have demonstratedsignificantly higher cord/adult freedrug ratios for salicylates, sulfon-amides, morphine, phenobarbital,and phenytoin. Because the freedrug exerts the pharmacologic drugeffect, the increased free drug con-centrations in neonates may result ingreater drug effect or even toxicitydespite normal total (bound plusunbound) drug concentrations.
Increased concentrations of freefatty acids and unconjugated biliru-bin in the newborn also affect drugprotein binding. Both free fatty acids and unconjugated bilirubinhave high affinity for albumin,which can result in competition and even displacement of drugsfrom albumin binding sites.
Differences in the distribution of different agents into the centralnervous system are clinically im-portant in antimicrobial therapy formeningitis. The relatively tighterjunctions in the brain endothelialcapillaries and the close approxima-tion of the glial connective tissue to the capillary endothelium limitthe distribution of drugs to brain tissue. This is especially relevant forwater-soluble antibiotics (eg, amino-glycosides), which are less likely tocross the blood-brain barrier.
CLEARANCE
Hepatic Drug Metabolism
Although the major organ of drugmetabolism is the liver, many otherorgans, including the lungs, GI tract,
PHARMACOLOGYDrug Monitoring
TABLE 1.Oral Drug Absorption
(Bioavailability) of SelectedDrugs in Neonates Compared
with Older Children
ORAL DRUG ABSORPTION
Acetaminophen Decreased
Ampicillin Increased
Diazepam No change
Digoxin No change
Pencillin G Increased
Phenobarbital Decreased
Phenytoin Decreased
Sulfonamides No change

Pediatrics in Review Vol. 19 No. 12 December 1998 425
or blood, are capable of metaboliz-ing drugs. Drug metabolism canresult in either generation of weakeror inactive metabolites or transfor-mation of a parent compound orprodrug into the active compound(theophylline to caffeine, codeine tomorphine) or an even more activemetabolite. Drug metabolism is categorized in two major steps:phase I reactions in which a mole-cule is biotransformed into a morewater-soluble metabolite and phaseII reactions in which a drug or itsmetabolite is conjugated with en-dogenous molecules.
Generally, phase I reactions (oxidation, reduction, methylation)reach maximal maturity by 6 monthsof age. Age-related changes in drugmetabolism have been demonstratedfor theophylline. In neonates, only10% of theophylline is methylatedto caffeine, with 50% of the drugexcreted unchanged in the urine.With maturation of the hydroxyl-ation and acetylation of hepaticenzymes, the rate of theophyllineclearance increases, resulting in the short half-life demonstrated in infants and children (3 to 5 h)compared with adults (8 h).
Hepatic phase II reactions (gluco-ronidation, sulfation, acetylation) aresubstantially lower (50% to 70% ofadult values) in early neonatal life.Glucuronide formation reaches itsfull maturity (adult values) betweenthe third and fourth years of life.The decreased ability of neonates to metabolize drugs results in pro-longed elimination half-lives. Drugdoses and dosing schedules that donot take into account these changespredispose neonates to adverse drug reactions and even to toxicityfrom overdose.
Drug Excretion (Table 2)
Renal function demonstrates an age-dependent increase in functionalcapacity. The glomerular filtrationrate (GFR) in neonates is 30% to40% of the adult value. By the endof the first week of life, both theGFR and renal plasma flow haveincreased by 50%. By the end of thethird week, GFR is usually 50% to60% of the adult value and by 12months, it reaches the adult value.
The clinical relevance of thesechanges is apparent with renally
eliminated agents such as amino-glycosides, penicillins, and digoxin.For example, the dosage of genta-micin for a neonate younger than 7 days of age is 5 mg/kg per daydivided into two doses at 12-hourintervals. This dosage changes to 7.5 mg/kg per day divided into threedoses at 8-hour intervals in childrenolder than 7 days. Similarly, renalclearance of digoxin has beendemonstrated to increase from 33 mL/min/1.73 m2 in neonates to 98 and 144 mL/min/1.73 m2 at 3 months and 1.5 years, respectively.
Because certain disease statesmay alter the normal maturationprocess of renal function, doseadjustments that usually are madeaccording to the predicted rate ofrenal function maturation during the first weeks of life may not beappropriate.
Drug InteractionsClinically significant drug interac-tions can be defined as clinicallymeasurable modifications in eithermagnitude or duration of action ofone drug caused by prior or con-comitant administration of anothersubstance. Some drug interactionscan be desirable, such as seen withthe treatment of hypertension byusing multiple drugs with differentmechanisms of action. Other interac-tions can be adverse. It is estimatedthat serious, life-threatening adversedrug reactions occur in 3% of hospi-talized patients, with 7% of these
caused by drug interactions. Mecha-nisms of drug interactions can beclassified as pharmacokinetic andpharmacodynamic.
INTERACTIONS AFFECTINGORAL BIOAVAILABILITY
Drug interactions in the GI tract can decrease the oral bioavailabilityof the index drug. For example,tetracyclines can chelate calcium,magnesium, or iron, leading todecreased absorption of the cation-tetracycline complex. Drugs thatdamage the intestinal absorptive surface, such as oral neomycin orantineoplastic agents, may lead todecreased absorption of otherwisewell-absorbed drugs.
Gastric emptying can be phar-macologically enhanced (metoclo-pramide, domperidone) or delayed(morphine, anticholinergics, ant-acids), which affects the rate rather than the extent of absorption.This may be clinically relevantwhen a rapid onset of drug effect is desired (eg, pain relief, sedation,sepsis). Finally, for drugs that have an extensive first-pass effect(ie, those that are extracted ormetabolized during transit across the intestinal epithelium or duringthe first pass through the liver), suchas beta-blockers, calcium channelblockers, tricyclic antidepressants,and morphine, the primary factoraffecting clearance is hepatic bloodflow. Therefore, coadministration of drugs that decrease hepatic bloodflow such as cimetidine would beexpected to raise the steady-state
PHARMACOLOGYDrug Monitoring
TABLE 2. Changes in Elimination Half-life (hours) During Development
NEWBORN INFANTDRUG (0 TO 28 d) (1 TO 24 mo) CHILD ADULT
Acetaminophen 4.9 4.5 3.6
Amikacin 5.0 to 6.5 1.6 2.3
Amoxicillin 3.7 0.9 to 1.9 0.6 to 1.5
Cefuroxime 5.5 3.5 1.2 1.5
Diazepam 30 10 25 30
Digoxin 18 to 33 37 30 to 50
Gentamicin 4.0 2.6 1.2 2 to 3
Theophylline 30 6.9 3.4 8.1
Vancomycin 4.1 to 9.1 2.2 to 2.4 5 to 6

426 Pediatrics in Review Vol. 19 No. 12 December 1998
concentration of the previously men-tioned agents.
PROTEIN BINDING DRUG INTERACTIONS
Protein is bound primarily to albu-min and alpha2-glycoprotein. Theserum concentration of a measureddrug usually refers to the total drugconcentration in the plasma (freeplus protein bound), although onlythe free drug exerts the pharmaco-logic effect. Drugs that are highlybound to proteins are subject to displacement by other drugs thathave high affinity for the same protein binding sites. This mayresult in a transient increase in thefree concentrations of the indexdrug, followed by redistribution and increased clearance, creating
a new equilibrium of both drugs.This phenomenon will result in clinically significant effects in cases in which the index drug has a small volume of distribution, anarrow therapeutic window, andrapid onset of action in relation to its plasma concentration.
DRUG INTERACTIONS AFFECT-ING BIOTRANSFORMATION
Many of the prescribed drugs in thepediatric population may inhibit orenhance the metabolism of otherdrugs. The significance of this inter-action is dictated by the magnitudeof the decrease or increase in clear-ance of the index drug. Generally,modifications in the magnitude ofhepatic drug metabolism caused bydrug-drug interactions are difficultto predict because most drugs aremetabolized by several differentpathways, and the quantitative fraction of each pathway is hard to evaluate.
Most inhibitors of hepatic drugmetabolism bind to an essential partof the enzyme system, resulting in a functionally impaired or inactiveenzyme that cannot oxidize, reduce,or hydrolyze medications. The mostuseful agents that have inhibitory
effects on hepatic drug metabolismprescribed for the pediatric agegroup are cimetidine, erythromycin,ciprofloxacin, and omeprazole.Coadministration of these agentswith a medication that has a narrowtherapeutic range, such as theophyl-line, may result in increased plasmaconcentration and even toxicity ofthe theophylline.
Enzyme induction, on the otherhand, can enhance the clearance ofindex drugs, which can lead todecreased or even loss of efficacy.Rifampin, a well-known inducer of hepatic metabolism, has beenimplicated as a potential cause ofgraft rejection via increased clear-ance of cyclosporine and predni-sone. It also has been claimed to be the cause of oral contraceptives
failing because of their increasedmetabolism. Phenytoin, anotherinducer of hepatic biotransforma-tion, has been shown to induce withdrawal symptoms in patientsreceiving methadone chronically.The ability of phenobarbital to induce the oxidizing enzyme sys-tem found in hepatic endoplasmicreticulum may enhance the hepaticmetabolism of any drug that under-goes metabolism by this system.
Phenobarbital-induced effects onthe metabolism of drugs from a vari-ety of classes have been reported,including analgesics (acetamino-phen), antibacterials (chlorampheni-col, doxycycline, metronidazole),anticoagulants (warfarin), beta-blockers (propranolol), cortico-steroids, and opioid analgesics.
If an induction interaction isestablished, the dose of the indexdrug should be increased. If theinducing drug is discontinued, theindex drug dose should be decreasedto avoid toxicity.
DRUG INTERACTIONS DUE TOALTERED RENAL FUNCTION
Drugs excreted entirely by glomer-ular filtration are unlikely to beaffected by other drugs. However,
clearance of drugs that are activelytransformed into the tubular lumencan be inhibited significantly byother drugs. Methotrexate toxicitymay be induced by inhibition of its tubular secretion by salicylates.Renal clearance of lithium is re-duced significantly in the presenceof thiazides, and a low effective circulating volume combined withincreased sodium reabsorptionincreases lithium reabsorption.
Drug interactions may have ad-vantages. For example, probenecidenhances the tubular secretion ofpenicillin.
The pediatrician should try todecrease the possible risk of druginteractions by being cognizant ofthe potential in high-risk clinical settings. Drugs that have low toxic/therapeutic ratios and a steep dose-response relationship represent amajor risk. Clinically relevant exam-ples of such drugs include warfarin,digoxin, lithium, theophylline, andaminoglycosides. Patients at risk for drug interactions include thosereceiving polypharmacy (the risk ofdrug interaction increases with thenumber of drugs used), critically illpatients, and drug abusers.
Drug Use During LactationThe relevance of drug use duringlactation is highlighted by the pat-tern of breastfeeding over the pastseveral decades. In the UnitedStates, the proportion of womenbreastfeeding their babies was estimated at 60% in the late 1980scompared with 30% in the 1950s.
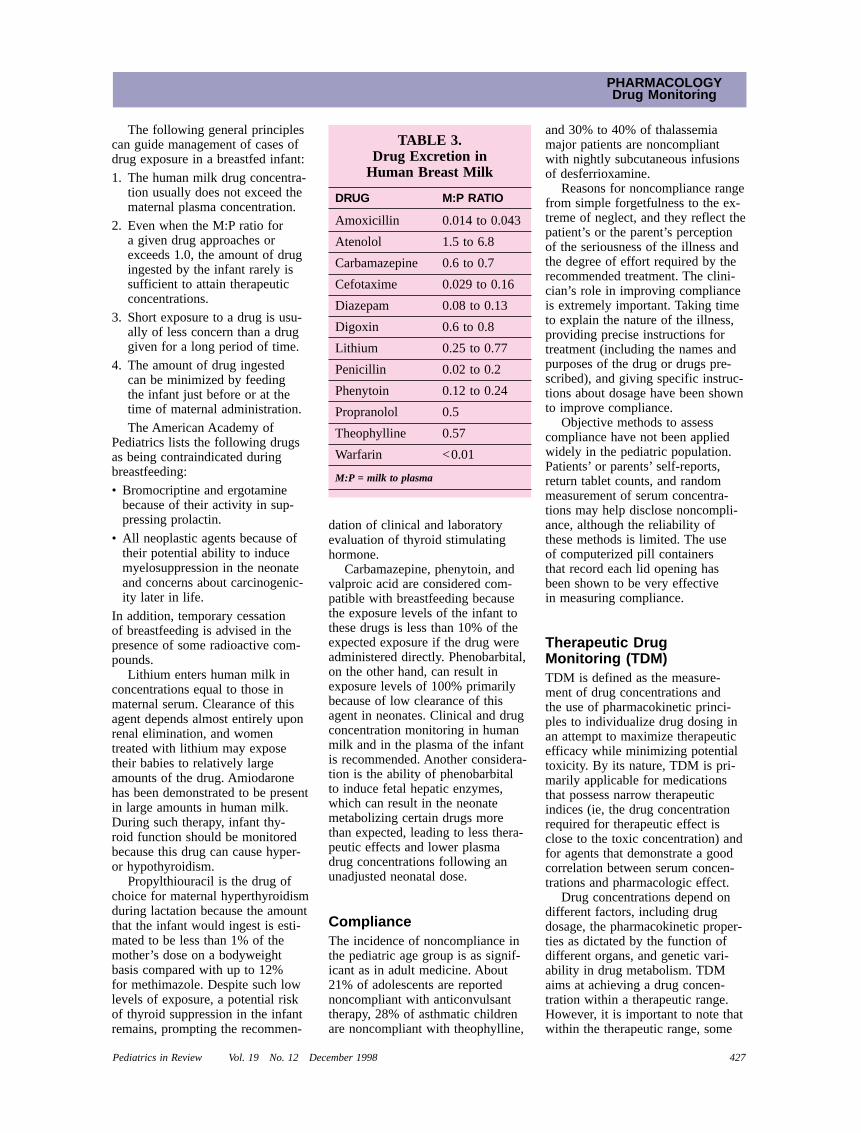
Most drugs are excreted intohuman milk by passive diffusion,making the drug concentration inmilk directly proportional to theconcentration in maternal plasma.Because human milk is slightlymore acidic than plasma, drugs thattypically pass into milk are weakbases, lipid-soluble, and poorlybound to proteins. The milk:plasma(M:P) ratio, which compares drugconcentrations in milk with that in maternal plasma, serves as anindex of the extent of drug excre-tion in the milk (Table 3). However, to determine infant exposure todrugs in human milk, the infant’sclearance of the drug also must be considered.
PHARMACOLOGYDrug Monitoring
The most useful drugs that have inhibitory effects on hepatic drug metabolism prescribed for the pediatric age groupare cimetidine, erythromycin, ciprofloxacin, and omeprazole.
Pediatrics in Review Vol. 19 No. 12 December 1998 427
The following general principlescan guide management of cases ofdrug exposure in a breastfed infant:
1. The human milk drug concentra-tion usually does not exceed thematernal plasma concentration.
2. Even when the M:P ratio for a given drug approaches orexceeds 1.0, the amount of drugingested by the infant rarely issufficient to attain therapeuticconcentrations.
3. Short exposure to a drug is usu-ally of less concern than a druggiven for a long period of time.
4. The amount of drug ingested can be minimized by feeding the infant just before or at thetime of maternal administration.
The American Academy of Pediatrics lists the following drugsas being contraindicated duringbreastfeeding:
• Bromocriptine and ergotaminebecause of their activity in sup-pressing prolactin.
• All neoplastic agents because oftheir potential ability to inducemyelosuppression in the neonateand concerns about carcinogenic-ity later in life.
In addition, temporary cessation of breastfeeding is advised in thepresence of some radioactive com-pounds.
Lithium enters human milk inconcentrations equal to those inmaternal serum. Clearance of thisagent depends almost entirely uponrenal elimination, and womentreated with lithium may exposetheir babies to relatively largeamounts of the drug. Amiodaronehas been demonstrated to be presentin large amounts in human milk.During such therapy, infant thy-roid function should be monitoredbecause this drug can cause hyper-or hypothyroidism.
Propylthiouracil is the drug ofchoice for maternal hyperthyroidismduring lactation because the amountthat the infant would ingest is esti-mated to be less than 1% of themother’s dose on a bodyweight basis compared with up to 12% for methimazole. Despite such lowlevels of exposure, a potential riskof thyroid suppression in the infantremains, prompting the recommen-
dation of clinical and laboratoryevaluation of thyroid stimulatinghormone.
Carbamazepine, phenytoin, andvalproic acid are considered com-patible with breastfeeding becausethe exposure levels of the infant tothese drugs is less than 10% of theexpected exposure if the drug wereadministered directly. Phenobarbital,on the other hand, can result inexposure levels of 100% primarilybecause of low clearance of thisagent in neonates. Clinical and drugconcentration monitoring in humanmilk and in the plasma of the infantis recommended. Another considera-tion is the ability of phenobarbital to induce fetal hepatic enzymes,which can result in the neonatemetabolizing certain drugs morethan expected, leading to less thera-peutic effects and lower plasma drug concentrations following anunadjusted neonatal dose.
ComplianceThe incidence of noncompliance inthe pediatric age group is as signif-icant as in adult medicine. About21% of adolescents are reportednoncompliant with anticonvulsanttherapy, 28% of asthmatic childrenare noncompliant with theophylline,
and 30% to 40% of thalassemiamajor patients are noncompliantwith nightly subcutaneous infusionsof desferrioxamine.
Reasons for noncompliance rangefrom simple forgetfulness to the ex-treme of neglect, and they reflect thepatient’s or the parent’s perceptionof the seriousness of the illness andthe degree of effort required by therecommended treatment. The clini-cian’s role in improving complianceis extremely important. Taking timeto explain the nature of the illness,providing precise instructions fortreatment (including the names andpurposes of the drug or drugs pre-scribed), and giving specific instruc-tions about dosage have been shownto improve compliance.
Objective methods to assess compliance have not been appliedwidely in the pediatric population.Patients’ or parents’ self-reports,return tablet counts, and randommeasurement of serum concentra-tions may help disclose noncompli-ance, although the reliability ofthese methods is limited. The use of computerized pill containers that record each lid opening hasbeen shown to be very effective in measuring compliance.
Therapeutic Drug Monitoring (TDM)TDM is defined as the measure-ment of drug concentrations and the use of pharmacokinetic princi-ples to individualize drug dosing inan attempt to maximize therapeuticefficacy while minimizing potentialtoxicity. By its nature, TDM is pri-marily applicable for medicationsthat possess narrow therapeuticindices (ie, the drug concentrationrequired for therapeutic effect isclose to the toxic concentration) andfor agents that demonstrate a goodcorrelation between serum concen-trations and pharmacologic effect.
Drug concentrations depend ondifferent factors, including drugdosage, the pharmacokinetic proper-ties as dictated by the function ofdifferent organs, and genetic vari-ability in drug metabolism. TDMaims at achieving a drug concen-tration within a therapeutic range.However, it is important to note thatwithin the therapeutic range, some
PHARMACOLOGYDrug Monitoring
TABLE 3.Drug Excretion in
Human Breast Milk
DRUG M:P RATIO
Amoxicillin 0.014 to 0.043
Atenolol 1.5 to 6.8
Carbamazepine 0.6 to 0.7
Cefotaxime 0.029 to 0.16
Diazepam 0.08 to 0.13
Digoxin 0.6 to 0.8
Lithium 0.25 to 0.77
Penicillin 0.02 to 0.2
Phenytoin 0.12 to 0.24
Propranolol 0.5
Theophylline 0.57
Warfarin <0.01
M:P = milk to plasma

428 Pediatrics in Review Vol. 19 No. 12 December 1998
patients will not respond completelyand others will experience toxicitydue to pharmacokinetic and phar-macodynamic differences amongindividuals.
Appropriate timing of drug con-centration measurement is crucialfor accurate TDM. Trough levels,measured prior to drug administra-tion, provide accurate interpretationof drug concentrations. Peak levelsare less accurate because they aresubject to significant variability due to differences in absorption anddistribution rates. Measurement ofpeak levels usually is reserved formedications that have short half-lives in which peak levels are asso-ciated with efficacy or toxicity. Random sampling of drug concen-trations is not appropriate becausethe accuracy is diminished markedly.
THEOPHYLLINE
Theophylline serum concentrationsof 10 to 20 mcg/mL have beenshown to induce clinical broncho-dilation in asthmatic children; con-centrations of 5 to 10 mcg/mL areeffective for diaphragmatic stimula-tion. Plasma concentrations higherthan 20 mcg/mL are associated withan increasing incidence of toxicity.
AMINOGLYCOSIDES
Aminoglycoside-induced ototoxicityand nephrotoxicity are closelyrelated to peak serum concentra-tions. Prolonged peak levels of gen-tamicin of 12 to 14 mcg/mL and/ortrough levels above 2 mcg/mL havebeen shown to increase the risk of both toxicities significantly.
CHLORAMPHENICOL
Chloramphenicol serum concentra-tions of 25 mcg/mL or higher havebeen demonstrated to increase therisk for reversible bone marrow suppression. However, this toxicityshould be distinguished from therare idiosyncratic form of chloram-phenicol-induced bone marrow sup-pression, which has no correlationwith serum concentrations.
VANCOMYCIN
Vancomycin-induced nephrotoxicityand ototoxicity are dose-related.Although the relationship between athreshold serum concentration andboth toxicities is difficult to deter-mine, trough concentrations greaterthan 30 mg/L and 80 to 100 mg/Lare associated with an increased riskfor nephrotoxicity and ototoxicity,respectively.
SummaryFrom a pharmacotherapy perspec-tive, the process of development and growth represents an unstableand dynamic condition. Age-relatedchanges in drug absorption, distri-bution, and metabolism amongneonates, infants, and prepubescentchildren create a unique situationthat may increase drug toxicity ofsome agents and protect from toxic-ity of other agents. Understandingthe age-related changes in drug disposition that are relevant for therapeutic response and toxicity is essential for optimizing pharma-cotherapy at different stages ofchildhood.
SUGGESTED READINGAmerican Academy of Pediatrics. Committee
on Drugs. Transfer of drugs and otherchemicals into human milk. Pediatrics.1994;93:137–150
Brodie MJ, Feely J. Adverse drug interaction.Br Med J. 1988;296:845–849
Kearns GL, Reed MD. Clinical pharmacoki-netics in infants and children: a reap-praisal. Clin Pharmacokinet. 1989;17S1:26–67
MacLeod SM, Radde IC. Textbook of Pedi-atric Clinical Pharmacology. Littleton,Mass: PSG Publishing; 1993
Maxwell GM. Principles in Pediatric Phar-macology. New York, NY: Oxford Univer-sity Press; 1984
Naranjo CA, Busto U, Sellers EM. A methodfor estimating the probability of adversedrug reactions. Clin Pharm Ther. 1981;30:239–245
Stewart CF, Hampton EM. Effect of matura-tion on drug disposition in pediatricpatients. Clin Pharm. 1987;6:548–564
PHARMACOLOGYDrug Monitoring
PIR QUIZ17. Which of the following drugs is
contraindicated for use by the breastfeeding mother?A. Carbamazepine.B. Ergotamine.C. Propylthiouracil.D. Phenytoin.E. Valproic acid.
18. Which of the following is notan inhibitor of hepatic drug metabolism?A. Cimetidine.B. Ciprofloxacin.C. Erythromycin.D. Omeprazole.E. Theophylline.
19. Because of decreased drug proteinbinding in newborns and infants compared with adults, increased free drug concentrations in neonatesmay result in greater drug effect or even toxicity despite normal total drug concentrations. This phenomenon is true of each of the following drugs except:A. Digoxin.B. Morphine.C. Phenobarbital.D. Phenytoin.E. Salicylates.
20. The oral bioavailability of tricyclicantidepressants is enhanced by:A. Drug damage to the intestinal
absorptive surface.B. Drug interactions in the
gastrointestinal tract.C. Drugs that decrease hepatic
blood flow.D. Pharmacologic delay of gastric
emptying.E. Pharmacologic enhancement of
gastric emptying.
21. The bioavailability of which of the following drugs is increased in neonates compared with older children?A. Ampicillin.B. Diazepam.C. Digoxin.D. Phenobarbital.E. Phenytoin.





























