Embed Size (px)
Citation preview

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:
Emergency Department Asthma
CONTACTS: ERIC HOPPA, MD | KRISTIN WELCH, MD
LAST UPDATED: 10.21.19
©2019 Connecticut Children’s Medical Center. All rights reserved. 19-004
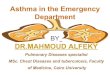
Inclusion Criteria: 1 yrs old, previous diagnosis of asthma or 2 previous episodes of wheezing, MPIS 5Exclusion Criteria: <1 yrs old, bronchiolitis or pneumonia as primary diagnosis, chronic cardiac or lung disease other than asthma
Initial Assessment (MPIS 5):Dexamethasone 0.6 mg/kg (max 16 mg) PO/IM
(Can substitute with prednisolone/prednisone/methylprednisolone 2 mg/kg at initial provider s discretion. Can omit if already on oral steroids.)
MPIS 5-6 MPIS 7
Albuterol 5 mg/Ipratropium 500 mcg
via nebulizer
Albuterol 4 puffs MDI/spacer (with teach) OR Albuterol 2.5 mg neb
Calculate MPIS
Discharge Criteria/Instructions: MDI/spacer teach F/u with PCP in 2-3 days Medications: Albuterol PRN
*Consider Prednisolone/Prednisone for patients thatmight benefit from longer steroids. Start 24 hours
after Dexamethasone dose.
MPIS 6 MPIS 7
Reassess in 15-30 minutes Calculate MPIS
MPIS 6 MPIS 7
Albuterol 4 puffsMDI/spacer(with teach)
if not already done
Long Albuterol treatment:• <20 kg: 10 mg over 1 hour
• >20 kg: 20 mg over 1 hour
• Reassess in 15-30 minutes• Calculate MPIS
MPIS 6 MPIS 13
Observe for 1 hour
Reassess Calculate MPIS
MPIS 6 MPIS 7
Discharge Criteria and Instructions:
MDI/spacer teach F/u with PCP in 2-3 days Medications: Albuterol q4hr
*Consider Prednisolone/Prednisone for patients that might benefit from longer steroids. Start
24 hours after Dexamethasone dose.
MPIS 11-12
Medications: Resume continuous
Albuterol at 20 mg/hr Consider additional
therapies per PICU consultation (e.g, methylprednisolone if not done, MgSO4, terbutaline)
Nursing: Place PIV (if not done)
Consults: Consult PICU attending
in ED: observe in ED for further improvement vs admission to PICU
Admission:- Admit to MS floor or PICU in discussion with IMT and
PICU attending- If to be admitted to MS floor,
ED provider to place order Initiate Albuterol wean . RT will rescore MPIS and speak
with provider to place appropriate
Albuterol order.
Medications: Resume continuous
Albuterol atprevious dose
ED provider to place order Initiate Albuterol wean
RT will rescore MPIS and speak with provider to place appropriate Albuterol order
Nursing: Place PIV
Admission: Admit to MS (PHM or Pulmonary if patient is known to them) See Inpatient Asthma Pathway
At time of transfer: Re-assess patient and calculate MPIS Inform attending and admitting team if MPIS is increasing Hold transfer if MPIS 13 and consider PICU consult
MPIS 7-8
Medications: Albuterol 5 mg neb
q2hr ED provider to place
order Initiate Albuterol wean
RT will rescore MPISand speak with provider to place appropriate Albuterol order
Nursing: Place PIV if
inadequate oral intake, or unable to take oral steroids
MPIS 9-10
Medications: Resume continuous
Albuterol atprevious dose
ED provider to place order Initiate Albuterol wean
RT will rescore MPIS and speak with provider to place appropriate Albuterol order
Nursing: Place PIV if
inadequate oral intake, or unable to take oral steroids

©2019 Connecticut Children’s Medical Center. All rights reserved. 19-004
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY: Inpatient Asthma
CONTACTS: CHRISTINA GIUDICE, APRN | ALEX HOGAN, MD | ANAND SEKARAN, MD
LAST UPDATED: 11.11.19
Admit to Medical/ Surgical Unit Oxygen: Titrate per order Oral Steroid:
o Prednisone or Prednisolone 1mg/kg/dose q12hr; <12 yr old: max 60 mg/day, 12 y/o: max 80 mg/day (Start 24 hr after dexamethasone. Total steroid course: 5 days)
o OR give additional dose of Dexamethasone 0.6 mg/kg (max 16mg) PO/IM prior to discharge
Determine initial MPIS If poor PO, place PIV and administer IVF with potassium Use asthma-specific H&P to document asthma severity and control
(Appendix A, Appendix B, Appendix C) Consider ordering medications for bedside delivery on admission
MPIS 11 MPIS 7-10
Initiate Phase 2: Albuterol MDI w/ spacer 8 puffs q2hr
(nebulizer can be used if patient sleeping or unable to perform proper MDI technique)
Initiate Albuterol Wean Protocol* Assess severity and treatment recommendations, start
Inhaled Corticosteroids (Appendix A, Appendix B, Appendix C, Appendix D)
Initiate Asthma Education and home treatment plan
Discontinue CR monitor Vital signs q4hr, MPIS q2hr Discontinue O2 when RA sat >92% Intermittent pulse ox once off O2
MPIS 13 x 1
Increase Albuterol to 20 mg/hr if on 10 mg/hr
Notify attending Obtain PICU consult Consider Mg sulfate
Inclusion Criteria: 1 yrs old, inadequate response to ED asthma treatment (see ED Asthma Pathway)Exclude Criteria: < 1yr old, primary diagnosis of bronchiolitis or pneumonia, active cardiac disease
Improvement? (Two consecutive scores in
appropriate range)
Improvement?
No
Initiate Phase 2 and follow pathway
Improvement? (MPIS 6 x2)
* ALBUTEROL WEAN PROTOCOL: RT s wean Albuterol
according to this MPIS-driven protocol
Wean when two consecutive scores are in appropriate range
RT s inform MD/APRN/PA of ALL changes in Albuterol dosing
Any escalation in care requires an exam by MD/ APRN/PA at bedside
MD/APRN/PA can authorize variance from protocol
Continue on pathway as MPIS dictates
Continue on pathway as MPIS dictates
No Yes
Yes
No Yes
Initiate Phase 1: Albuterol via continuous neb:
o <20kg: 10 mg/hro 20kg: 20 mg/hr
Initiate Albuterol Wean Protocol*o Option: If improving on 20 mg/hr, wean to
10 mg/hr prior to going to q2hr If not tolerating oral steroid:
o Methylprednisolone 1 mg/kg/dose IV q6hr (<12 yr old: max 60 mg/day; 12 max 80 mg/day)
Place PIV, if not already done CR monitor w/continuous pulse oximetry Vital signs q4hr, MPIS q2hr Initiate Asthma Education
Initiate Phase 3 Albuterol MDI w/ spacer 8 puffs q4hr
(nebulizer can be used if pt sleeping or unable to perform proper MDI technique)
Continue Inhaled Corticosteroids (Appendix A, Appendix B, Appendix C, Appendix D), and consider ordering medications for bedside delivery if not done
Discontinue O2 when RA sat >92% Intermittent pulse ox once off O2 Vital signs q4hr, MPIS q4hr Complete Asthma Education Supply nebulizer or spacer, if needed
Discharge Criteria:Off supplemental oxygen, MPIS 5 on q4hr albuterol, hydrated without need for IVFs,
asthma home management plan of care complete, asthma education complete and family given copy, appropriate follow up in place
Discharge Medications (to be outlined in Asthma Action Plan) Albuterol MDI with spacer: 4 puffs (or 2.5mg via neb) q4hr while awake Total oral steroid x3-5 days (prednisone/prednisolone vs 2nd dose of dexamethasone) Controller therapy (Appendix C, Appendix D), based on chronic severity (Appendix A,
Appendix B) Screen for Flu vaccine (Oct-March); administer if indicatedConsider transfer
to PICU
MPIS SCORING TOOLO2 Saturation
(RA)Accessory
Muscle Use I:E Ratio Wheezing Heart Rate Respiratory Rate
Score Score Score Score <3 yr old >3 yr old Score <6 yr old >6 yr old Score
>95% 0 None 0 2:1 0None: Good
aeration 0 <120 <100 0 <30 <20 0
93-95% 1 Mild 1 1:1 1End
expiratory 1 121-140 101-120 1 31-45 21-35 1
90-92% 2 Moderate 2 1:2 2Insp/Exp:
Good aeration 2 141-160 121-140 2 46-60 36-50 2
<90% 3 Severe 3 1:3 3
Insp/Exp: Decreased aeration 3 >160 >140 3 >60 >50 3
The following tests and treatments are NOT routinely indicated for the treatment of asthma: Ipratropium bromide should
not be administered after 24 hours of hospitalization
Chest x-rays (features typically associated with positive chest x-ray findings include fever, no family history of asthma, and localized lung exam findings)
Antibiotics (unless diagnosed with a bacterial infection)
NEXT PAGE

©2019 Connecticut Children’s Medical Center. All rights reserved. 19-004
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
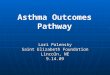
CLINICAL PATHWAY: Inpatient Asthma Appendix A: Simplified Controller Flowchart
Assessing Asthma Severity and Treatment Recommendations: Ages 5 and Up
Symptom Frequency 2 days/week > 2 days/week but NOT daily Daily Throughout the day
Night time awakenings 2x/month 3-4x/month >1x/week Every Night
Albuterol for symptom control 2 days/week >2 days/week Daily Several times per
dayInterfere with normal activity None Minor Limitation Some Limitation Extremely Limited
Exacerbations requiring systemic
steroids0-1/year 2/year with more frequent or intense events = greater severity
Intermittent Mild Persistent Moderate Persistent Severe Persistent
5-11 Years Old (STEP 1)Albuterol PRN
(STEP 2)2 Puffs Fluticasone
44 BID
(STEP 3)If start ing tx: 1 Puff Fluticasone 110 BID If stepping up tx: 1 Puff Fluticasone 110 BID + MontelukastOR 2 Puffs Fluticasone/Salmeterol 45/21 BID +/- Montelukast
(STEP 3 or 4)2 Puff Fluticasone/
Salmeterol 115/21 BID OR
Consult Pulmonary
12+ Years Old (STEP 1)Albuterol PRN
(STEP 2)2 Puffs Fluticasone
44 BID
(STEP 3)2 Puffs Fluticasone
44 BID + Montelukast OR 2
Puff Fluticasone 110 BID
(STEP 3 or 4) Fluticasone/
Salmeterol 115 mcg/21 mcg 2 Puff BID vs Fluticasone
110mcg 2 Puffs BID + Montelukast
Worst symptom documented above determines severity
Consult Pulmonology If: Patient Requires Step 5 Treatment, Or High Dose Inhaled Steroids (2+ Puffs 110 for 5-11yo, 2+ puffs 220 for >12 year old)
Montelukast
<6 years old 4mg daily; 6-14 years old: 5mg daily; >14 years old: 10mg daily
Fluticasone (Flovent)
Beclomethasone (Qvar)
44 mcg 40 mcg
110 mcg 80 mcg
Fluticasone/Salmeterol
(Advair)
Budesonide/Formoterol (Symbicort)
Mometasone/Formoterol
(Dulera)
45/21 mcg 80/4.5 mcg 100/5 mcg
115/21 mcg 160/4.5 mcg 200/5 mcg
1
2
3
4*Taking Controller Medications Appropriately:
Taking medications as prescribed >80% of the time (self report, pharmacy refills) Using correct technique (using a spacer correctly)
If insurance does not cover the recommended medication, see below for equivalent doses of inhaled steroids
If on meds, taking appropriately*?
If currently on medication & well
controlled, continue current treatment
NOIncrease Step by 1
UNLESS well controlled (all green answers above)
YES
Dosing Conversion
Chart
Consult (PRN)
Treatment Recommendation
(NHLBI STEP CORRELARY)
Classify Asthma Severity
Assess and DOCUMENT
Asthma Control for 2 Weeks Prior to Exacerbation
Determine severity if new
diagnosis of asthma
CONTACTS: CHRISTINA GIUDICE, APRN | ALEX HOGAN, MD | ANAND SEKARAN, MD
LAST UPDATED: 11.11.19
RETURN TOTHE BEGINNING

©2019 Connecticut Children’s Medical Center. All rights reserved. 19-004
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY: Inpatient Asthma Appendix B: NHLBI Asthma Classification
INIT
IAL
VIS
IT:
CL
AS
SIF
YIN
G A
ST
HM
A S
EV
ER
ITY
AN
D I
NIT
IAT
ING
TH
ER
AP
Y(i
n p
ati
en
ts w
ho
are
no
t cu
rre
ntl
y t
akin
g l
on
g-t
erm
co
ntr
ol
me
dic
ati
on
s)
Level o
f se
veri
ty (
Co
lum
ns
2–5
) is
dete
rmin
ed
by e
ven
ts lis
ted
in
Co
lum
n 1
fo
r b
oth
im
pair
men
t (f
req
uen
cy a
nd
in
ten
sity
of
sym
pto
ms
an
d f
un
cti
on
al lim
itati
on
s) a
nd
ris
k (
of
exacerb
ati
on
s).
Ass
ess
im
pair
men
t b
y p
ati
en
t’s
or
care
giv
er’
s re
call
of
even
ts d
uri
ng
th
e p
revio
us
2–4
weeks;
ass
ess
ris
k o
ver
the last
year. R
eco
mm
en
dati
on
s fo
r in
itia
tin
g t
hera
py
base
d o
n level o
f se
veri
ty a
re p
rese
nte
d in
th
e last
ro
w.
Co
mp
on
en
ts o
f S
eve
rity
Inte
rmit
ten
tP
ers
iste
nt
Mild
Mo
de
rate
Seve
re
Ag
es
0
–4 y
ears
Ag
es
5–1
1 ye
ars
Ag
es
≥12
ye
ars
Ag
es
0–4
ye
ars
Ag
es
5–1
1 ye
ars
Ag
es
≥1
2 y
ears
Ag
es
0–4
ye
ars
Ag
es
5–1
1 ye
ars
Ag
es
≥12
ye
ars
Ag
es
0–4
ye
ars
Ag
es
5–1
1 ye
ars
Ag
es
≥12
ye
ars
Impairment
Sym
pto
ms
≤2 d
ays/
week
>2 d
ays/
week b
ut
no
t d
aily
Daily
Th
rou
gh
ou
t th
e d
ay
Nig
htt
ime a
wake
nin
gs
0≤2
x/m
on
th1–
2x/m
on
th3
–4x/m
on
th3
–4x/m
on
th>
1x/w
eek b
ut
no
t n
igh
tly
>1x
/week
Oft
en
7x/w
eek
SA
BA
use
fo
r
sym
pto
m c
on
tro
l
(no
t to
pre
ven
t E
IB)
≤2 d
ays/
week
>2 d
ays/
week
but
no
t d
aily
>2 d
ays/
week b
ut
n
ot
daily
an
d n
ot
mo
re
than
on
ce o
n a
ny d
ay
Daily
Severa
l ti
mes
per
day
Inte
rfere
nce w
ith
n
orm
al acti
vit
yN
on
eM
ino
r lim
itati
on
So
me lim
itati
on
Extr
em
ely
lim
ited
Lu
ng
fu
ncti
on
FE
V1
(%
pre
dic
ted
)
FE
V1/
FV
C
No
t ap
plic
ab
le
No
rmal F
EV
1
betw
een
exacerb
ati
ons
>8
0%
>8
5%
No
rmal F
EV
1 b
etw
een
exacerb
ati
ons
>8
0%
No
rmal†
No
t ap
plic
ab
le>
80
%
>8
0%
>8
0%
No
rmal†
No
t ap
plic
ab
le6
0–8
0%
75
–80
%
60
–80
%
Red
uced
5%
†
No
t ap
plic
ab
le<
60
%
<75%
<6
0%
Red
uce
d >
5%
†
Risk
Ast
hm
a e
xacerb
ati
on
s re
qu
irin
g o
ral sy
stem
ic
co
rtic
ost
ero
ids‡
0–1
/year
≥2 e
xacerb
. in
6 m
onth
s,
or
wheezin
g
≥4x p
er
year
last
ing
>
1 d
ay
AN
D r
isk
facto
rs f
or
pers
iste
nt
ast
hm
a
≥2/y
ear
Co
nsi
der
seve
rity
an
d in
terv
al s
ince
last
ast
hm
a e
xace
rbati
on
. F
req
uen
cy a
nd
seve
rity
may
flu
ctu
ate
ove
r ti
me f
or
pati
en
ts in
any s
eve
rity
cate
go
ry.
Rela
tive
an
nu
al r
isk o
f ex
ace
rbati
on
s m
ay b
e r
ela
ted
to
FE
V1.
Re
com
me
nd
ed
Ste
p f
or
In
itia
tin
g T
he
rap
y
(See “
Ste
pw
ise A
pp
roach
fo
r
Man
ag
ing
Ast
hm
a L
on
g T
erm
,”
pag
e 7
)
Th
e s
tep
wis
e a
pp
roach
is m
ean
t to
help
, no
t re
pla
ce, t
he c
linic
al
deci
sio
nm
akin
g n
eed
ed
to
meet
ind
ivid
ual p
ati
en
t n
eed
s.
Ste
p 1
Ste
p 2
Ste
p 3
Ste
p 3
m
ed
ium
-do
se
ICS
op
tio
nS
tep
3S
tep
3
Ste
p 3
m
ed
ium
-do
se
ICS
op
tio
n
or
Ste
p 4
Ste
p 4
or
5
Co
nsi
der
sho
rt c
ou
rse o
f o
ral s
yste
mic
co
rtic
ost
ero
ids.
In 2
–6 w
eeks,
dep
en
din
g o
n s
eve
rity
, ass
ess
leve
l of
ast
hm
a c
on
tro
l ach
ieve
d a
nd
ad
just
th
era
py a
s n
eed
ed
.
Fo
r ch
ildre
n 0
–4 y
ears
old
, if
no
cle
ar
ben
efi
t is
ob
serv
ed
in 4
–6 w
eeks,
co
nsi
der
ad
just
ing
th
era
py o
r alt
ern
ate
dia
gn
ose
s.
Ab
bre
via
tio
ns:
E
IB, e
xerc
ise-i
nd
uced
bro
nch
osp
am
; FE
V1,
forc
ed
exp
irato
ry v
olu
me in
1 s
eco
nd
; FV
C, f
orc
ed
vit
al c
ap
acit
y; I
CS
, in
hale
d c
ort
ico
stero
id; S
AB
A, s
ho
rt-a
cti
ng
beta
2-a
go
nis
t.
† N
orm
al F
EV
1/F
VC
by a
ge:
8–1
9 y
ears
, 85%
; 20
–39
years
, 80
%; 4
0–5
9 y
ears
, 75%
; 60
–80
years
, 70
%.
‡ D
ata
are
insu
fficie
nt
to li
nk f
req
uencie
s o
f exacerb
ati
ons
wit
h d
iffe
rent
levels
of
ast
hm
a s
everi
ty.
Genera
lly, m
ore
fre
quent
and
inte
nse
exacerb
ati
ons
(e.g
., re
quir
ing
urg
ent
care
, ho
spit
al o
r in
tensi
ve c
are
ad
mis
sio
n, a
nd
/or
ora
l co
rtic
ost
ero
ids)
in
dic
ate
gre
ate
r und
erl
yin
g d
isease
severi
ty.
Fo
r tr
eatm
ent
purp
ose
s, p
ati
ents
wit
h ≥
2 e
xacerb
ati
ons
may b
e c
onsi
dere
d t
o h
ave p
ers
iste
nt
ast
hm
a, e
ven in
the a
bse
nce o
f im
pair
ment
levels
co
nsi
stent
wit
h p
ers
iste
nt
ast
hm
a.
Genera
lly, m
ore
fre
quent
and
inte
nse
eve
nts
ind
icat
e g
reat
er
seve
rity
.
Genera
lly, m
ore
fre
quent
and
inte
nse
eve
nts
ind
icat
e g
reat
er
seve
rity
.
5Asthma Care Quick Reference
CONTACTS: CHRISTINA GIUDICE, APRN | ALEX HOGAN, MD | ANAND SEKARAN, MD
LAST UPDATED: 11.11.19
RETURN TOTHE BEGINNING

©2019 Connecticut Children’s Medical Center. All rights reserved. 19-004
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY: Inpatient Asthma Appendix B: NHLBI Asthma Classification
FO
LL
OW
-UP
VIS
ITS
: A
SS
ES
SIN
G A
ST
HM
A C
ON
TR
OL
AN
D A
DJ
US
TIN
G T
HE
RA
PY
Level o
f co
ntr
ol (
Co
lum
ns
2–4
) is
base
d o
n t
he m
ost
severe
co
mp
onent
of
imp
air
ment
(sym
pto
ms
and
functi
onal l
imit
ati
ons)
or
risk
(exacerb
ati
ons)
. A
ssess
imp
air
ment
by p
ati
ent’s
or
care
giv
er’
s
recall
of
events
list
ed
in C
olu
mn 1
duri
ng
the p
revio
us
2–4
weeks
and
by s
pir
om
etr
y a
nd
/or
peak fl
ow
measu
res.
S
ym
pto
m a
ssess
ment
for
long
er
peri
od
s sh
ould
refl
ect
a g
lob
al a
ssess
ment,
such a
s in
quir
ing
wheth
er
the p
ati
ent’s
ast
hm
a is
bett
er
or
wo
rse s
ince t
he la
st v
isit
. A
ssess
ris
k b
y r
ecall
of
exacerb
ati
ons
duri
ng
the p
revio
us
year
and
sin
ce t
he la
st v
isit
. R
eco
mm
end
ati
ons
for
ad
just
ing
thera
py b
ase
d o
n le
vel o
f co
ntr
ol a
re p
rese
nte
d in
the la
st r
ow
.
Co
mp
on
en
ts o
f C
on
tro
lW
ell C
on
tro
lle
dN
ot
We
ll C
on
tro
lle
dV
ery
Po
orl
y C
on
tro
lle
d
Ag
es
0–4
ye
ars
Ag
es
5–1
1 ye
ars
Ag
es
≥12
ye
ars
Ag
es
0–4
ye
ars
Ag
es
5–1
1 ye
ars
Ag
es
≥12
ye
ars
Ag
es
0–4
ye
ars
Ag
es
5–1
1 ye
ars
Ag
es
≥12
ye
ars
Impairment
Sym
pto
ms
≤2 d
ays/
week
≤2 d
ays/
week b
ut
no
t m
ore
than
o
nce o
n e
ach d
ay
≤2 d
ays/
week
>2 d
ays/
week
>2 d
ays/
week o
r m
ult
iple
tim
es
on
≤2
days/
week
>2 d
ays/
week
Th
rou
gh
ou
t th
e d
ay
Nig
htt
ime a
wake
nin
gs
≤1x/m
on
th≤2
x/m
on
th>
1x/m
on
th≥2
x/m
on
th1–
3x/w
eek
>1x
/week
≥2x/w
eek
≥4x/w
eek
Inte
rfere
nce w
ith
n
orm
al acti
vit
yN
on
eS
om
e lim
itati
on
Extr
em
ely
lim
ited
SA
BA
use
fo
r
sym
pto
m c
on
tro
l
(no
t to
pre
ven
t E
IB)
≤2 d
ays/
week
>2 d
ays/
week
Severa
l ti
mes
per
day
Lu
ng
fu
ncti
on
FE
V1
(% p
red
icte
d)
o
r p
eak fl
ow
(%
pers
onal
best
)
FE
V1/F
VC
No
t ap
plic
ab
le>
80
%
>8
0%
>8
0%
No
t ap
plic
ab
le
No
t ap
plic
ab
le6
0–8
0%
75
–80
%
60
–80
%
No
t ap
plic
ab
le
No
t ap
plic
ab
le<
60
%
<75
%
<6
0%
No
t ap
plic
ab
le
Valid
ate
d q
uest
ion
nair
es†
ATA
Q
AC
Q
AC
T
No
t ap
plic
ab
leN
ot
ap
plic
ab
le0
≤0.7
5‡
≥20
No
t ap
plic
ab
leN
ot
ap
plic
ab
le1–
2
≥1.5
16–1
9
No
t ap
plic
ab
leN
ot
ap
plic
ab
le3
–4
No
t ap
plic
ab
le
≤15
Risk
Ast
hm
a e
xacerb
ati
on
s re
qu
irin
g o
ral sy
stem
ic
co
rtic
ost
ero
ids§
0–1
/year
2–3
/year
≥2/y
ear
>3/y
ear
≥2/y
ear
Co
nsi
der
seve
rity
an
d in
terv
al s
ince
last
ast
hm
a e
xace
rbati
on
.
Red
ucti
on
in
lu
ng
g
row
th/P
rog
ress
ive lo
ss
of
lun
g f
un
cti
on
N
ot
ap
plic
ab
leE
valu
ati
on
req
uir
es
lon
g-t
erm
fo
llow
-up
care
.N
ot
ap
plic
ab
leE
valu
ati
on
req
uir
es
lon
g-t
erm
fo
llow
-up
care
.N
ot
ap
plic
ab
leE
valu
ati
on
req
uir
es
lon
g-t
erm
fo
llow
-up
care
.
Tre
atm
en
t-re
late
d
ad
vers
e e
ffects
Med
icati
on
sid
e e
ffect
s ca
n v
ary
in in
ten
sity
fro
m n
on
e t
o v
ery
tro
ub
leso
me a
nd
wo
rris
om
e.
Th
e le
vel o
f in
ten
sity
do
es
no
t co
rrela
te t
o s
peci
fic
leve
ls o
f co
ntr
ol b
ut
sho
uld
be c
on
sid
ere
d in
th
e o
vera
ll ass
ess
men
t o
f ri
sk.
Re
com
me
nd
ed
Acti
on
fo
r Tre
atm
en
t
(See “
Ste
pw
ise A
pp
roach
fo
r
Man
ag
ing
Ast
hm
a L
on
g T
erm
,”
pag
e 7
)
Th
e s
tep
wis
e a
pp
roach
is m
ean
t to
help
, no
t re
pla
ce, t
he c
linic
al
deci
sio
nm
akin
g n
eed
ed
to
meet
ind
ivid
ual p
ati
en
t n
eed
s.
Main
tain
cu
rren
t st
ep
.
Reg
ula
r fo
llow
-up
eve
ry 1
–6 m
on
ths.
Co
nsi
der
step
do
wn
if w
ell
con
tro
lled
fo
r at
least
3 m
on
ths.
Ste
p u
p 1
ste
pS
tep
up
at
least
1
step
Ste
p u
p 1
ste
pC
on
sid
er
sho
rt c
ou
rse o
f o
ral s
yste
mic
co
rtic
ost
ero
ids.
Ste
p u
p 1
–2 s
tep
s.
Reeva
luate
in 2
weeks
to a
chie
ve c
on
tro
l.
Reeva
luate
in 2
–6 w
eeks
to a
chie
ve c
on
tro
l.
Fo
r ch
ildre
n 0
–4 y
ears
, if
no
cle
ar
ben
efi
t o
bse
rved
in 4
–6
weeks
, co
nsi
der
adju
stin
g t
hera
py
or
alte
rnat
ive d
iag
no
ses.
Befo
re s
tep
up
in t
reatm
en
t:R
evie
w a
dh
ere
nce
to
med
icati
on
, in
hale
r te
chn
iqu
e, a
nd
envir
on
men
tal c
on
tro
l. If
alt
ern
ati
ve t
reatm
en
t w
as
use
d,
dis
con
tin
ue a
nd
use
pre
ferr
ed
tre
atm
en
t fo
r th
at
step
. F
or
sid
e e
ffect
s, c
on
sid
er
alt
ern
ati
ve t
reatm
en
t o
pti
on
s.
Ab
bre
via
tio
ns:
A
CQ
, Ast
hm
a C
on
tro
l Q
uest
ion
nair
e©; A
CT, A
sth
ma C
on
tro
l Te
stT
M; A
TA
Q, A
sth
ma T
hera
py A
ssess
men
t Q
uest
ion
nair
e©; E
IB, e
xerc
ise-i
nd
uced
bro
nch
osp
asm
; FV
C, f
orc
ed
vit
al cap
acit
y; F
EV
1, fo
rced
exp
irato
ry v
olu
me in
1 s
eco
nd
; S
AB
A, s
ho
rt-a
cti
ng
beta
2-a
go
nis
t.
† M
inim
al im
po
rtan
t d
iffe
ren
ce:
1.0
fo
r th
e A
TA
Q; 0
.5 f
or
the A
CQ
; no
t d
ete
rmin
ed
fo
r th
e A
CT.
‡ A
CQ
valu
es
of
0.7
6–1
.4 a
re in
dete
rmin
ate
reg
ard
ing
well-
co
ntr
olle
d a
sth
ma.
§ D
ata
are
in
suffi
cie
nt
to lin
k f
req
uen
cie
s o
f exacerb
ati
on
s w
ith
dif
fere
nt
levels
of
ast
hm
a c
on
tro
l. G
en
era
lly, m
ore
fre
qu
en
t an
d in
ten
se e
xacerb
ati
on
s (e
.g.,
req
uir
ing
urg
en
t care
, h
osp
ital o
r in
ten
sive c
are
ad
mis
sio
n, an
d/o
r o
ral co
rtic
ost
ero
ids)
in
dic
ate
po
ore
r ast
hm
a c
on
tro
l.
6 Asthma Care Quick Reference
CONTACTS: CHRISTINA GIUDICE, APRN | ALEX HOGAN, MD | ANAND SEKARAN, MD
LAST UPDATED: 11.11.19
RETURN TOTHE BEGINNING

©2019 Connecticut Children’s Medical Center. All rights reserved. 19-004
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY: Inpatient Asthma Appendix C: NHLBI Step-Up Therapy
STEPWISE APPROACH FOR MANAGING ASTHMA LONG TERMThe stepwise approach tailors the selection of medication to the level of asthma severity (see page 5) or asthma control (see page 6).
The stepwise approach is meant to help, not replace, the clinical decisionmaking needed to meet individual patient needs.
At each step: Patient education, environmental control, and management of comorbidities
0–4
ye
ars
of
ag
e
Intermittent Asthma
Persistent Asthma: Daily MedicationConsult with asthma specialist if step 3 care or higher is required. Consider consultation at step 2.
PreferredTreatment†
SABA as needed
low-dose ICS medium-dose ICS
medium-dose ICS+either LABA or montelukast
high-dose ICS+either LABA or montelukast
high-dose ICS+either LABA or montelukast+oral corticosteroids
AlternativeTreatment†,‡
cromolyn or montelukast
If clear benefit is not observed in 4–6 weeks, and medication technique and adherence are satisfactory, consider adjusting therapy or alternate diagnoses.
Quick-Relief Medication
�� SABA as needed for symptoms; intensity of treatment depends on severity of symptoms.�� With viral respiratory symptoms: SABA every 4–6 hours up to 24 hours (longer with physician consult). Consider short course of oral systemic corticosteroids if asthma exacerbation is severe or patient has history of severe exacerbations.�� Caution: Frequent use of SABA may indicate the need to step up treatment.
5–1
1 ye
ars
of
ag
e
Intermittent Asthma
Persistent Asthma: Daily MedicationConsult with asthma specialist if step 4 care or higher is required. Consider consultation at step 3.
PreferredTreatment†
SABA as needed low-dose ICS low-dose ICS+either LABA, LTRA, or theophylline(b)
OR
medium-dose ICS
medium-dose ICS+LABA
high-dose ICS+LABA
high-dose ICS+LABA+oral corticosteroids
AlternativeTreatment†,‡
cromolyn, LTRA, or theophylline§
medium-dose ICS+either LTRA or theophylline§
high-dose ICS+either LTRA or theophylline§
high-dose ICS +either LTRA or theophylline§
+oral corticosteroids
Consider subcutaneous allergen immunotherapy for patients who have persistent, allergic asthma.
Quick-Relief Medication
�� SABA as needed for symptoms. The intensity of treatment depends on severity of symptoms: up to 3 treatments every 20 minutes as needed. Short course of oral systemic corticosteroids may be needed.�� Caution: Increasing use of SABA or use >2 days/week for symptom relief (not to prevent EIB ) generally indicates inadequate control and the need to step up treatment.
≥12
ye
ars
of
ag
e
Intermittent Asthma
Persistent Asthma: Daily MedicationConsult with asthma specialist if step 4 care or higher is required. Consider consultation at step 3.
PreferredTreatment†
SABA as needed low-dose ICS low-dose ICS+LABA
OR
medium-dose ICS
medium-dose ICS+ LABA
high-dose ICS+LABA
AND
consider omalizumab for patients who have allergies††
high-dose ICS+LABA+oral corticosteroid§§
AND
consider omalizumab for patients who have allergies††
AlternativeTreatment†,‡
cromolyn, LTRA,or theophylline§
low-dose ICS+either LTRA,theophylline,§ or zileuton‡‡
medium-dose ICS+either LTRA, theophylline,§ or zileuton‡‡
Consider subcutaneous allergen immunotherapy for patients who have persistent, allergic asthma.
Quick-Relief Medication
�� SABA as needed for symptoms. The intensity of treatment depends on severity of symptoms: up to 3 treatments every 20 minutes as needed. Short course of oral systemic corticosteroids may be needed.�� Caution: Use of SABA >2 days/week for symptom relief (not to prevent EIB ) generally indicates inadequate control and the need to step up treatment.
Abbreviations: EIB, exercise-induced bronchospasm; ICS, inhaled corticosteroid; LABA, inhaled long-acting beta2-agonist; LTRA, leukotriene receptor antagonist; SABA, inhaled
short-acting beta2-agonist.
† Treatment options are listed in alphabetical order, if more than one. ‡ If alternative treatment is used and response is inadequate, discontinue and use preferred treatment before stepping up.§ Theophylline is a less desirable alternative because of the need to monitor serum concentration levels.
Based on evidence for dust mites, animal dander, and pollen; evidence is weak or lacking for molds and cockroaches. Evidence is strongest for immunotherapy with single allergens. The role of allergy in asthma is greater in children than in adults.
†† Clinicians who administer immunotherapy or omalizumab should be prepared to treat anaphylaxis that may occur.‡‡ Zileuton is less desirable because of limited studies as adjunctive therapy and the need to monitor liver function.§§ Before oral corticosteroids are introduced, a trial of high-dose ICS + LABA + either LTRA, theophylline, or zileuton, may be considered, although this approach has not been studied
in clinical trials.
ASSESS CONTROL:
STEP UP IF NEEDED (first, check medication adherence, inhaler technique, environmental control, and comorbidities)
STEP DOWN IF POSSIBLE (and asthma is well controlled for at least 3 months)
STEP 1STEP 6STEP 5STEP 4STEP 3STEP 2
FO
LL
OW
-UP
VIS
ITS
: A
SS
ES
SIN
G A
ST
HM
A C
ON
TR
OL
AN
D A
DJ
US
TIN
G T
HE
RA
PY
Level o
f co
ntr
ol (
Co
lum
ns
2–4
) is
base
d o
n t
he m
ost
severe
co
mp
onent
of
imp
air
ment
(sym
pto
ms
and
functi
onal l
imit
ati
ons)
or
risk
(exacerb
ati
ons)
. A
ssess
imp
air
ment
by p
ati
ent’s
or
care
giv
er’
s
recall
of
events
list
ed
in C
olu
mn 1
duri
ng
the p
revio
us
2–4
weeks
and
by s
pir
om
etr
y a
nd
/or
peak fl
ow
measu
res.
S
ym
pto
m a
ssess
ment
for
long
er
peri
od
s sh
ould
refl
ect
a g
lob
al a
ssess
ment,
such a
s in
quir
ing
wheth
er
the p
ati
ent’s
ast
hm
a is
bett
er
or
wo
rse s
ince t
he la
st v
isit
. A
ssess
ris
k b
y r
ecall
of
exacerb
ati
ons
duri
ng
the p
revio
us
year
and
sin
ce t
he la
st v
isit
. R
eco
mm
end
ati
ons
for
ad
just
ing
thera
py b
ase
d o
n le
vel o
f co
ntr
ol a
re p
rese
nte
d in
the la
st r
ow
.
Co
mp
on
en
ts o
f C
on
tro
lW
ell C
on
tro
lle
dN
ot
We
ll C
on
tro
lle
dV
ery
Po
orl
y C
on
tro
lle
d
Ag
es
0–4
ye
ars
Ag
es
5–1
1 ye
ars
Ag
es
≥12
ye
ars
Ag
es
0–4
ye
ars
Ag
es
5–1
1 ye
ars
Ag
es
≥12
ye
ars
Ag
es
0–4
ye
ars
Ag
es
5–1
1 ye
ars
Ag
es
≥12
ye
ars
Impairment
Sym
pto
ms
≤2 d
ays/
week
≤2 d
ays/
week b
ut
no
t m
ore
than
o
nce o
n e
ach d
ay
≤2 d
ays/
week
>2 d
ays/
week
>2 d
ays/
week o
r m
ult
iple
tim
es
on
≤2
days/
week
>2 d
ays/
week
Th
rou
gh
ou
t th
e d
ay
Nig
htt
ime a
wake
nin
gs
≤1x/m
on
th≤2
x/m
on
th>
1x/m
on
th≥2
x/m
on
th1–
3x/w
eek
>1x
/week
≥2x/w
eek
≥4x/w
eek
Inte
rfere
nce w
ith
n
orm
al acti
vit
yN
on
eS
om
e lim
itati
on
Extr
em
ely
lim
ited
SA
BA
use
fo
r
sym
pto
m c
on
tro
l
(no
t to
pre
ven
t E
IB)
≤2 d
ays/
week
>2 d
ays/
week
Severa
l ti
mes
per
day
Lu
ng
fu
ncti
on
FE
V1
(% p
red
icte
d)
o
r p
eak fl
ow
(%
pers
onal
best
)
FE
V1/F
VC
No
t ap
plic
ab
le>
80
%
>8
0%
>8
0%
No
t ap
plic
ab
le
No
t ap
plic
ab
le6
0–8
0%
75
–80
%
60
–80
%
No
t ap
plic
ab
le
No
t ap
plic
ab
le<
60
%
<75
%
<6
0%
No
t ap
plic
ab
le
Valid
ate
d q
uest
ion
nair
es†
ATA
Q
AC
Q
AC
T
No
t ap
plic
ab
leN
ot
ap
plic
ab
le0
≤0.7
5‡
≥20
No
t ap
plic
ab
leN
ot
ap
plic
ab
le1–
2
≥1.5
16–1
9
No
t ap
plic
ab
leN
ot
ap
plic
ab
le3
–4
No
t ap
plic
ab
le
≤15
Risk
Ast
hm
a e
xacerb
ati
on
s re
qu
irin
g o
ral sy
stem
ic
co
rtic
ost
ero
ids§
0–1
/year
2–3
/year
≥2/y
ear
>3/y
ear
≥2/y
ear
Co
nsi
der
seve
rity
an
d in
terv
al s
ince
last
ast
hm
a e
xace
rbati
on
.
Red
ucti
on
in
lu
ng
g
row
th/P
rog
ress
ive lo
ss
of
lun
g f
un
cti
on
N
ot
ap
plic
ab
leE
valu
ati
on
req
uir
es
lon
g-t
erm
fo
llow
-up
care
.N
ot
ap
plic
ab
leE
valu
ati
on
req
uir
es
lon
g-t
erm
fo
llow
-up
care
.N
ot
ap
plic
ab
leE
valu
ati
on
req
uir
es
lon
g-t
erm
fo
llow
-up
care
.
Tre
atm
en
t-re
late
d
ad
vers
e e
ffects
Med
icati
on
sid
e e
ffect
s ca
n v
ary
in in
ten
sity
fro
m n
on
e t
o v
ery
tro
ub
leso
me a
nd
wo
rris
om
e.
Th
e le
vel o
f in
ten
sity
do
es
no
t co
rrela
te t
o s
peci
fic
leve
ls o
f co
ntr
ol b
ut
sho
uld
be c
on
sid
ere
d in
th
e o
vera
ll ass
ess
men
t o
f ri
sk.
Re
com
me
nd
ed
Acti
on
fo
r Tre
atm
en
t
(See “
Ste
pw
ise A
pp
roach
fo
r
Man
ag
ing
Ast
hm
a L
on
g T
erm
,”
pag
e 7
)
Th
e s
tep
wis
e a
pp
roach
is m
ean
t to
help
, no
t re
pla
ce, t
he c
linic
al
deci
sio
nm
akin
g n
eed
ed
to
meet
ind
ivid
ual p
ati
en
t n
eed
s.
Main
tain
cu
rren
t st
ep
.
Reg
ula
r fo
llow
-up
eve
ry 1
–6 m
on
ths.
Co
nsi
der
step
do
wn
if w
ell
con
tro
lled
fo
r at
least
3 m
on
ths.
Ste
p u
p 1
ste
pS
tep
up
at
least
1
step
Ste
p u
p 1
ste
pC
on
sid
er
sho
rt c
ou
rse o
f o
ral s
yste
mic
co
rtic
ost
ero
ids.
Ste
p u
p 1
–2 s
tep
s.
Reeva
luate
in 2
weeks
to a
chie
ve c
on
tro
l.
Reeva
luate
in 2
–6 w
eeks
to a
chie
ve c
on
tro
l.
Fo
r ch
ildre
n 0
–4 y
ears
, if
no
cle
ar
ben
efi
t o
bse
rved
in 4
–6
weeks
, co
nsi
der
adju
stin
g t
hera
py
or
alte
rnat
ive d
iag
no
ses.
Befo
re s
tep
up
in t
reatm
en
t:R
evie
w a
dh
ere
nce
to
med
icati
on
, in
hale
r te
chn
iqu
e, a
nd
envir
on
men
tal c
on
tro
l. If
alt
ern
ati
ve t
reatm
en
t w
as
use
d,
dis
con
tin
ue a
nd
use
pre
ferr
ed
tre
atm
en
t fo
r th
at
step
. F
or
sid
e e
ffect
s, c
on
sid
er
alt
ern
ati
ve t
reatm
en
t o
pti
on
s.
Ab
bre
via
tio
ns:
A
CQ
, Ast
hm
a C
on
tro
l Q
uest
ion
nair
e©; A
CT, A
sth
ma C
on
tro
l Te
stT
M; A
TA
Q, A
sth
ma T
hera
py A
ssess
men
t Q
uest
ion
nair
e©; E
IB, e
xerc
ise-i
nd
uced
bro
nch
osp
asm
; FV
C, f
orc
ed
vit
al cap
acit
y; F
EV
1, fo
rced
exp
irato
ry v
olu
me in
1 s
eco
nd
; S
AB
A, s
ho
rt-a
cti
ng
beta
2-a
go
nis
t.
† M
inim
al im
po
rtan
t d
iffe
ren
ce:
1.0
fo
r th
e A
TA
Q; 0
.5 f
or
the A
CQ
; no
t d
ete
rmin
ed
fo
r th
e A
CT.
‡ A
CQ
valu
es
of
0.7
6–1
.4 a
re in
dete
rmin
ate
reg
ard
ing
well-
co
ntr
olle
d a
sth
ma.
§ D
ata
are
in
suffi
cie
nt
to lin
k f
req
uen
cie
s o
f exacerb
ati
on
s w
ith
dif
fere
nt
levels
of
ast
hm
a c
on
tro
l. G
en
era
lly, m
ore
fre
qu
en
t an
d in
ten
se e
xacerb
ati
on
s (e
.g.,
req
uir
ing
urg
en
t care
, h
osp
ital o
r in
ten
sive c
are
ad
mis
sio
n, an
d/o
r o
ral co
rtic
ost
ero
ids)
in
dic
ate
po
ore
r ast
hm
a c
on
tro
l.
7Asthma Care Quick Reference
CONTACTS: CHRISTINA GIUDICE, APRN | ALEX HOGAN, MD | ANAND SEKARAN, MD
LAST UPDATED: 11.11.19
RETURN TOTHE BEGINNING

©2019 Connecticut Children’s Medical Center. All rights reserved. 19-004
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY: Inpatient Asthma Appendix D: Comparative Daily Dosages
ES
TIM
AT
ED
CO
MP
AR
AT
IVE
DA
ILY
DO
SA
GE
S:
IN
HA
LE
D C
OR
TIC
OS
TE
RO
IDS
FO
R L
ON
G-T
ER
M A
ST
HM
A C
ON
TR
OL
0–4
ye
ars
of
ag
e5
–11
ye
ars
of
ag
e≥1
2 y
ears
of
ag
e
Daily D
ose
Lo
wM
ed
ium
Hig
hLo
wM
ed
ium
Hig
hLo
wM
ed
ium
Hig
h
ME
DIC
AT
ION
Be
clo
me
thaso
ne
MD
I†
40
mcg
/pu
ff
80
mcg
/pu
ff
N/A
N/A
N/A
80
–16
0 m
cg
1–2 p
uff
s
2x/d
ay
1 p
uff
2x/d
ay
>16
0–3
20
mcg
3–4
pu
ffs
2x/d
ay
2 p
uff
s 2x/d
ay
>3
20
mcg
≥3 p
uff
s 2x/d
ay
80
–24
0 m
cg
1–3
pu
ffs
2x/d
ay
1 p
uff
am
, 2 p
uff
s p
m
>24
0–4
80
mcg
4–6
pu
ffs
2x/d
ay
2–3
pu
ffs
2x/d
ay
>4
80
mcg
≥4 p
uff
s
2x/d
ay
Bu
de
son
ide
DP
I†
90
mcg
/in
hala
tio
n
180
mcg
/ in
hala
tio
n
N/A
N/A
N/A
180
–36
0 m
cg
1–2 in
hs†
2x/d
ay
>3
60
–720
mcg
3–4
inhs†
2x/d
ay
2 in
hs†
2x/d
ay
>720
mcg
≥3 in
hs†
2x/d
ay
180
–54
0 m
cg
1–3
in
hs†
2x/d
ay
1 in
h†
am
, 2 in
hs†
pm
>54
0–1
,08
0 m
cg
2–3
inhs†
2x/d
ay
>1,0
80
mcg
≥4 in
hs†
2x/d
ay
Bu
de
son
ide
Ne
bu
les
0.2
5 m
g
0.5
mg
1.0
mg
0.2
5–0
.5 m
g
1–2 n
eb
s†/d
ay
1 n
eb
† /d
ay
>0
.5–1
.0 m
g
2 n
eb
s†/d
ay
1 n
eb
† /d
ay
>1.0
mg
3 n
eb
s†/d
ay
2 n
eb
s†/d
ay
0.5
mg
1 n
eb
† 2x/d
ay
1 n
eb
† /d
ay
1.0
mg
1 n
eb
† 2x/d
ay
1 n
eb
† /d
ay
2.0
mg
1 n
eb
† 2x/d
ay
N/A
N/A
N/A
Cic
leso
nid
e M
DI†
80
mcg
/pu
ff
160
mcg
/pu
ff
N/A
N/A
N/A
80
–16
0 m
cg
1–2 p
uff
s/d
ay
1 p
uff
/day
>16
0–3
20
mcg
1 p
uff
am
, 2
pu
ffs
pm
– 2 p
uff
s 2x/d
ay
1 p
uff
2x/d
ay
>3
20
mcg
≥3 p
uff
s 2x/d
ay
≥2 p
uff
s 2x/d
ay
160
–320
mcg
1–2 p
uff
s 2x/d
ay
>3
20
–64
0 m
cg
3–4
puff
s 2x/
day
2 p
uff
s 2x/d
ay
>6
40
mcg
≥3 p
uff
s 2x/d
ay
Flu
nis
olid
e M
DI†
80
mcg
/pu
ff
N/A
N/A
N/A
160
mcg
1 p
uff
2x/d
ay
320
–48
0 m
cg
2–3
puff
s 2x/
day
≥48
0 m
cg
≥4 p
uff
s 2x/d
ay
320
mcg
2 p
uff
s 2x/d
ay
>3
20
–64
0 m
cg
3–4
puff
s 2x/
day
>6
40
mcg
≥5 p
uff
s 2x/d
ay
It
is p
refe
rab
le t
o u
se a
hig
her
mcg
/puff
or
mcg
/inhala
tio
n f
orm
ula
tio
n t
o a
chie
ve a
s lo
w a
num
ber
of
puff
s o
r in
hala
tio
ns
as
po
ssib
le.
† A
bb
revia
tio
ns:
D
PI,
dry
po
wd
er
inhale
r (r
eq
uir
es
deep
, fast
inhala
tio
n);
inh, i
nhala
tio
n; M
DI,
mete
red
do
se in
hale
r (r
ele
ase
s a p
uff
of
med
icati
on);
neb
, neb
ule
.
8 Asthma Care Quick Reference
CONTACTS: CHRISTINA GIUDICE, APRN | ALEX HOGAN, MD | ANAND SEKARAN, MD
LAST UPDATED: 11.11.19
RETURN TOTHE BEGINNING

©2019 Connecticut Children’s Medical Center. All rights reserved. 19-004
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY: Inpatient Asthma Appendix D: Comparative Daily Dosages
0–4
ye
ars
of
ag
e5
–11
ye
ars
of
ag
e≥1
2 y
ears
of
ag
e
Daily D
ose
Lo
wM
ed
ium
Hig
hLo
wM
ed
ium
Hig
hLo
wM
ed
ium
Hig
h
ME
DIC
AT
ION
Flu
ticaso
ne
MD
I†
44
mcg
/pu
ff
110
mcg
/pu
ff
220
mcg
/pu
ff
Flu
ticaso
ne
DP
I†
50
mcg
/in
hala
tio
n
100
mcg
/in
hala
tio
n
25
0 m
cg
/in
hala
tio
n
176
mcg
2 p
uff
s 2x/d
ay
N/A
>17
6–3
52 m
cg
3–4
pu
ffs
2x/d
ay
1 p
uff
2x/d
ay
N/A
>352 m
cg
≥2 p
uff
s
2x/d
ay
N/A
88
–176
mcg
1–2 p
uff
s
2x/d
ay
100
–20
0 m
cg
1–2 in
hs†
2x/d
ay
1 in
h†
2x/d
ay
>17
6–3
52 m
cg
3–4
pu
ffs
2x/d
ay
1 p
uff
2x/d
ay
>20
0–4
00
mcg
3–4
inhs†
2x/d
ay
2 in
hs†
2x/d
ay
>352 m
cg
≥2 p
uff
s 2x/d
ay
>4
00
mcg
>2 in
hs†
2x/d
ay
1 in
h†
2x/d
ay
88
–26
4 m
cg
1–3
pu
ffs
2x/d
ay
100
–30
0 m
cg
1–3 in
hs†
2x/d
ay
>26
4–4
40
mcg
2 p
uff
s 2x/d
ay
1 p
uff
s 2x/d
ay
>30
0–5
00
mcg
2 in
hs†
2x/d
ay
1 in
h†
2x/d
ay
>4
40
mcg
3 p
uff
s 2x/d
ay
≥2 p
uff
s 2x/d
ay
>5
00
mcg
≥3 in
hs†
2x/d
ay
≥2 in
hs†
2x/d
ay
Mo
me
taso
ne
DP
I†
110
mcg
/in
hala
tio
n
220
mcg
/in
hala
tio
n
N/A
N/A
N/A
110
mcg
1 in
h† /
day
220
–44
0 m
cg
1–2 in
hs†
2x/d
ay
1–2 in
hs†
/day
>4
40
mcg
≥3 in
hs†
2x/d
ay
≥3 in
hs†
div
ided
in
2 d
ose
s
110
–220
mcg
1–2 in
hs†
pm
1 in
h†
pm
>220
–44
0 m
cg
3–4
inhs†
pm
or
2 in
hs†
2x/d
ay
1 in
h†
2x/d
ay o
r 2 in
hs†
pm
>4
40
mcg
≥3 in
hs†
2x/d
ay
≥3 in
hs†
div
ided
in
2 d
ose
s
It
is p
refe
rab
le t
o u
se a
hig
her
mcg
/puff
or
mcg
/inhala
tio
n f
orm
ula
tio
n t
o a
chie
ve a
s lo
w a
num
ber
of
puff
s o
r in
hala
tio
ns
as
po
ssib
le.
† A
bb
revia
tio
ns:
D
PI,
dry
po
wd
er
inhale
r (r
eq
uir
es
deep
, fast
inhala
tio
n);
inh, i
nhala
tio
n; M
DI,
mete
red
do
se in
hale
r (r
ele
ase
s a p
uff
of
med
icati
on);
neb
, neb
ule
.
Th
era
pe
uti
c I
ssu
es
Pe
rtain
ing
to
In
hale
d C
ort
ico
ste
roid
s (I
CS
s) f
or
Lo
ng
-Te
rm A
sth
ma C
on
tro
l
��T
he
mo
st im
po
rtan
t d
ete
rmin
an
t o
f ap
pro
pri
ate
do
sin
g is
the
clin
icia
n’s
ju
dg
me
nt
of
the
pati
en
t’s
resp
on
se t
o t
he
rap
y. T
he c
linic
ian
mu
st m
on
ito
r th
e p
ati
en
t’s
resp
on
se o
n s
evera
l clin
ical p
ara
mete
rs (
e.g
., sy
mp
tom
s; a
cti
vit
y level;
measu
res
of
lun
g f
un
cti
on
) an
d a
dju
st t
he d
ose
acco
rdin
gly
. O
nce a
sth
ma c
on
tro
l is
ach
ieved
an
d s
ust
ain
ed
at
least
3 m
on
ths,
th
e d
ose
sh
ou
ld b
e c
are
fully
tit
rate
d d
ow
n t
o t
he
min
imu
m d
ose
necess
ary
to
main
tain
co
ntr
ol.
��S
om
e d
ose
s m
ay b
e o
uts
ide p
ackag
e la
belin
g, e
specia
lly in
the h
igh-d
ose
rang
e.
Bud
eso
nid
e n
eb
uliz
er
susp
ensi
on is
the o
nly
inhale
d c
ort
ico
stero
id (
ICS
) w
ith
FD
A-a
pp
roved
lab
elin
g f
or
child
ren <
4 y
ears
of
ag
e.
��M
ete
red
-do
se in
hale
r (M
DI)
do
sag
es
are
exp
ress
ed
as
the a
ctu
ato
r d
ose
(am
ount
leavin
g t
he a
ctu
ato
r and
deliv
ere
d t
o t
he p
ati
ent)
, whic
h is
the la
belin
g r
eq
uir
ed
in t
he
Unit
ed
Sta
tes.
T
his
is d
iffe
rent
fro
m t
he d
osa
ge e
xp
ress
ed
as
the v
alv
e d
ose
(am
ount
of
dru
g le
avin
g t
he v
alv
e, n
ot
all
of
whic
h is
availa
ble
to
the p
ati
ent)
, whic
h is
use
d in
many E
uro
pean c
ountr
ies
and
in s
om
e s
cie
nti
fic li
tera
ture
. D
ry p
ow
der
inhale
r (D
PI)
do
ses
are
exp
ress
ed
as
the a
mo
unt
of
dru
g in
the in
hale
r fo
llow
ing
acti
vati
on.
��F
or
child
ren <
4 y
ears
of
ag
e:
The s
afe
ty a
nd
effi
cacy o
f IC
Ss
in c
hild
ren <
1 year
of
ag
e h
as
no
t b
een e
stab
lished
. C
hild
ren <
4 y
ears
of
ag
e g
enera
lly r
eq
uir
e d
eliv
ery
of
ICS
(b
ud
eso
nid
e a
nd
fluti
caso
ne M
DI)
thro
ug
h a
face m
ask
that
fits
snug
ly o
ver
no
se
and
mo
uth
to
avo
id n
eb
uliz
ing
in t
he e
yes.
F
ace s
ho
uld
be w
ash
ed
aft
er
treatm
ent
to p
revent
local c
ort
ico
stero
id s
ide e
ffects
. F
or
bud
eso
nid
e, t
he d
ose
may b
e g
iven
1–3 t
imes
daily
. B
ud
eso
nid
e s
usp
ensi
on is
co
mp
ati
ble
wit
h a
lbute
rol,
ipra
tro
piu
m,
and
levalb
ute
rol n
eb
uliz
er
solu
tio
ns
in t
he s
am
e n
eb
uliz
er.
Use
only
jet
neb
uliz
ers
, as
ult
raso
nic
neb
uliz
ers
are
ineff
ecti
ve f
or
susp
ensi
ons.
F
or
fluti
caso
ne M
DI,
the d
ose
sho
uld
be d
ivid
ed
2 t
imes
daily
; the lo
w d
ose
fo
r child
ren <
4 y
ears
of
ag
e is
hig
her
than f
or
child
ren 5
–11
years
of
ag
e b
ecause
of
low
er
do
se d
eliv
ere
d w
ith f
ace m
ask
and
data
on e
fficacy in
yo
ung
child
ren.
ES
TIM
AT
ED
CO
MP
AR
AT
IVE
DA
ILY
DO
SA
GE
S:
IN
HA
LE
D C
OR
TIC
OS
TE
RO
IDS
FO
R L
ON
G-T
ER
M A
ST
HM
A C
ON
TR
OL
(co
nti
nu
ed
)
9Asthma Care Quick Reference
CONTACTS: CHRISTINA GIUDICE, APRN | ALEX HOGAN, MD | ANAND SEKARAN, MD
LAST UPDATED: 11.11.19
RETURN TOTHE BEGINNING

©2019 Connecticut Children’s Medical Center. All rights reserved. 19-004
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY: Inpatient Asthma Appendix D: Comparative Daily Dosages
USUAL DOSAGES FOR OTHER LONG-TERM CONTROL MEDICATIONS*
Medication 0–4 years of age 5–11 years of age ≥12 years of age
Combined Medication (inhaled corticosteroid + long-acting beta2-agonist)
Fluticasone/Salmeterol — DPI† 100 mcg/50 mcg, 250 mcg/50 mcg, or 500 mcg/50 mcg
MDI† 45 mcg/21 mcg, 115 mcg/21 mcg, or 230 mcg/21 mcg
Budesonide/Formoterol — MDI† 80 mcg/4.5 mcg or 160 mcg/4.5 mcg
Mometasone/Formoterol — MDI† 100 mcg/5 mcg
N/A†
N/A†
N/A†
1 inhalation 2x/day; dose depends on level of severity or control
2 puffs 2x/day; dose depends on level of severity or control
N/A†
1 inhalation 2x/day; dose depends on level of severity or control
2 puffs 2x/day; dose depends on level of severity or control
2 inhalations 2x/day; dose depends on severity of asthma
Leukotriene Modifiers
Leukotriene Receptor Antagonists (LTRAs)Montelukast — 4 mg or 5 mg chewable tablet,4 mg granule packets, 10 mg tablet
Zafirlukast — 10 mg or 20 mg tablet
Take at least 1 hour before or 2 hours after a meal. Monitor liver function.
5-Lipoxygenase InhibitorZileuton — 600 mg tablet
Monitor liver function.
4 mg every night at bedtime (1–5 years of age)
N/A†
N/A†
5 mg every night at bedtime (6–14 years of age)
10 mg 2x/day (7–11 years of age)
N/A†
10 mg every night at bedtime
40 mg daily (20 mg tablet 2x/day)
2,400 mg daily (give 1 tablet 4x/day)
Immunomodulators
Omalizumab (Anti IgE†) — Subcutaneous injection, 150 mg/1.2 mL following reconstitution with 1.4 mL sterile water for injection
Monitor patients after injections; be prepared to treat anaphylaxis that may occur.
N/A† N/A† 150–375 mg subcutaneous every 2–4 weeks, depending on body weight and pretreatment serum IgE level
Cromolyn
Cromolyn — Nebulizer: 20 mg/ampule 1 ampule 4x/day, N/A† <2 years of age
1 ampule 4x/day 1 ampule 4x/day
Methylxanthines
Theophylline — Liquids, sustained-release tablets, and capsules
Monitor serum concentration levels.
Starting dose 10 mg/kg/day; usual maximum:�� <1 year of age: 0.2 (age in weeks) + 5 = mg/kg/day�� ≥1 year of age: 16 mg/kg/day
Starting dose 10 mg/kg/day; usual maximum: 16 mg/kg/day
Starting dose 10 mg/kg/day up to 300 mg maximum; usual maximum: 800 mg/day
Inhaled Long-Acting Beta2-Agonists (LABAs) – used in conjunction with ICS† for long-term control; LABA is NOT to be used as monotherapy
Salmeterol — DPI† 50 mcg/blister
Formoterol —DPI† 12 mcg/single-use capsule
N/A†
N/A†
1 blister every 12 hours
1 capsule every 12 hours
1 blister every 12 hours
1 capsule every 12 hours
Oral Systemic Corticosteroids
Methylprednisolone — 2, 4, 8, 16, 32 mg tablets
Prednisolone — 5 mg tablets; 5 mg/5 cc, 15 mg/5 cc
Prednisone — 1, 2.5, 5, 10, 20, 50 mg tablets; 5 mg/cc, 5 mg/5 cc
�� 0.25–2 mg/kg daily in single dose in a.m. or every other day as needed for control�� Short course “burst”: 1–2 mg/kg/day, max 60 mg/d for 3–10 days
�� 0.25–2 mg/kg daily in single dose in a.m. or every other day as needed for control�� Short course “burst”: 1–2 mg/kg/day, max 60 mg/d for 3–10 days
�� 7.5–60 mg daily in single dose in a.m. or every other day as needed for control�� Short course “burst”: to achieve control, 40–60 mg/day as single or 2 divided doses for 3–10 days
* Dosages are provided for those products that have been approved by the U.S. Food and Drug Administration or have sufficient clinical trial safety and efficacy data in the appropriate age ranges to support their use.
† Abbreviations: DPI, dry powder inhaler; IgE, immunoglobulin E; MDI, metered-dose inhaler; N/A, not available (not approved, no data available, or safety and efficacy not established for this age group).
The most important determinant of appropriate dosing is the clinician’s judgment of the patient’s response to therapy. The clinician must monitor the patient’s response on several clinical parameters (e.g., symptoms; activity level; measures of lung function) and adjust the dose accordingly. Once asthma control is achieved and sustained at least 3 months, the dose should be carefully titrated down to the minimum dose necessary to maintain control.
10 Asthma Care Quick Reference
RETURN TOTHE BEGINNING
CONTACTS: CHRISTINA GIUDICE, APRN | ALEX HOGAN, MD | ANAND SEKARAN, MD
LAST UPDATED: 11.11.19