Embed Size (px)
Citation preview
at SciVerse ScienceDirect
Clinical Radiology 68 (2013) 568e573
Contents lists available
Clinical Radiology
journal homepage: www.cl in icalradiologyonl ine.net
Clinical applications of preoperative perforator planningusing CT angiography in the anterolateral thigh perforatorflap transplantationJ.F. Yang a, B.Y. Wang a, Z.H. Zhao a,*, P. Zhou b, F. Pang b, W.D. Sun b
aDepartment of Radiology, Shaoxing People’s Hospital (Zhejiang University Shaoxing Hospital), Shaoxing, Zhejiang, ChinabDepartment of Hand Surgery, Shaoxing People’s Hospital (Zhejiang University Shaoxing Hospital), Shaoxing, Zhejiang, China
article information
Article history:Received 22 September 2012Received in revised form15 November 2012Accepted 23 November 2012
* Guarantor and correspondent: Z.H. Zhao,Shaoxing People’s Hospital (Zhejiang UniversityZhongxing North Rd, Shaoxing, Zhejiang, China. Tfax: þ86 (0) 575 88228558.
E-mail address: [email protected] (Z.H. Zha
0009-9260/$ e see front matter � 2012 The Royal Cohttp://dx.doi.org/10.1016/j.crad.2012.11.011
AIM: To evaluate the reliability and utility of preoperative perforator planning usingcomputed tomography angiography (CTA) in anterolateral thigh perforator flap (ALTPF)transplantation.MATERIALS AND METHODS: Thirty-two consecutive patients who underwent extremity
reconstruction using the ALTPF were retrospectively reviewed from 2008 to 2012. Thesepatients were divided into two groups. In group I (n ¼ 16), suitable perforators were designedbased on four criteria using CTA. These were used for the operation and compared with theintraoperative findings. In group II (n ¼ 16), all patients underwent operation using conven-tional methods without preoperative perforator planning. The surgical results of all patientswere evaluated for flap complications, alteration of the donor site, donor site morbidity, andthe incidence of reoperation.RESULTS: In group I, there were no statistically significant differences between the param-
eters, including the calibre and location of the origin (perpendicular and horizontal distancefrom the origin of the perforator to both the superior lateral border of the patella and thelateral region of the thigh) of all planning perforators and the operative measurement results(p-values were 0.3, 0.422, and 0.129, respectively). The types were consistent with the oper-ative findings; the rate of the septocutaneous type was 31.25% (5/16), and the rate of themusculocutaneous type was 68.75% (11/16). The use of preoperative perforator planning ingroup I was associated with a significant reduction in flap complications (p ¼ 0.009) comparedwith group II. There was no difference between the two groups in alteration of the donor site,donor site morbidity, or the incidence of reoperation (p-values were 0.225, 0.225, and 0.33,respectively).CONCLUSION: Preoperative perforator planning using CTA in ALTPF transplantation is
a reliable and useful method resulting in safer operation with optimal outcome.� 2012 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Department of Radiology,Shaoxing Hospital), 568
el.: þ86 (0) 575 88228556;
o).
llege of Radiologists. Published by
Introduction
The anterolateral thigh perforator flap (ALTPF) hasbecome an increasingly popular reconstructive option fora range of soft-tissue defects because of its versatility. Themajor limitations of this flap are uncertainty in predictingthe anatomical location of the perforator and high
Elsevier Ltd. All rights reserved.

J.F. Yang et al. / Clinical Radiology 68 (2013) 568e573 569
variability in the perforator size and course.1 These limita-tions sometimes cause unsuccessful perforator explorationand limit the use of ALTPF transplantation. Imaging tech-niques that are used to detect the perforator of the ALTPF,include hand-held Doppler, colour duplex ultrasonography,digital subtraction angiography, computed tomographyangiography (CTA), and magnetic resonance angiography(MRA).2e4 The main disadvantage of hand-held Dopplerand colour duplex ultrasonography is that these twomethods do not reproduce a two (2D) or three-dimensional(3D) image of the complete vascular anatomy, which is veryimportant during flap design or flap evaluation.2 CTA andMRA are currently the best methods available to map thevasculature of flaps, but the depiction of smaller perforatorswith MRA is less accurate thanwith CTA. Digital subtractionangiography is slowly losing favour because it is a time-consuming and invasive technique.2 Some former studieshave mainly investigated the accuracy of CTA for showingthe perforator of the ALTPF,1,5e7 but the optimized preop-erative perforator planning in an actual clinical setting hasnot been reported. The aim of the study was to demonstratethe accuracy of CTA and evaluate the clinical value ofpreoperative perforator planning in ALTPF transplantation.
Materials and methods
Patients
The local institutional review board approved this study,and the patients’ informed consent was obtained. BetweenJanuary 2008 and April 2012, 32 patients with soft-tissuedefects caused by trauma or diabetic foot in the limbsunderwent ALTPF transplantation. These patients weredivided into groups I and II depending onwhether they hador had not undergone preoperative perforator planning. Ingroup I, 16 patients (11 male, five female; mean age43.7 � 13.5 years, range 16e69 years) underwent preoper-ative perforator planning using CTA. In group II (n ¼ 16), allpatients (12 male, four female; mean age 43.5 � 11.2 years,range 24e57 years) underwent traditional ALTPF trans-plantation (following the schema of searching for septocu-taneous perforators, followed by musculocutaneousperforators, anteromedial thigh perforators, perforators ofthe tensor fascia lata flap and the contralateral leg if noperforators were identified).1
CT technique
Images were obtained using a 64 detector-row helical CTsystem (Philips 64, Philips Medical Systems, Cleveland, OH,America). The patients were oriented in the supine feet-firstposition and scanned during resting respiration. The scanrange was from the pubic symphysis to the superior marginof the tibia. The CT parameters for all images reviewed wereas follows: 120 KVp; 150mA; 1mm section thickness; 0.797beam pitch; 35 mm/s table feed; 512 � 512 matrix;32 cm � 32 cm scan field of vision (FOV). Intravenouscontrast-enhanced imaging was undertaken with theadministration of 1.8 ml/kg of a non-ionic contrast agent
(iopromide, 370 mg iodine/ml; Ultravist 370, Schering,Berlin, Germany) via a power injector (Missouri TMXD2001,Ulrich Medical, Ulm, Germany) at the rate of 4 ml/s. Auto-matic bolus tracking was performed within the region ofinterest (ROI), which was placed on the common femoralartery at the level of the pubic symphysis, so that the CTvalue of this ROI accurately reflected the concentration ofcontrast agent in the lateral circumflex femoral artery nearthe perforator to display the perforator clearly. The CTsystem was triggered to scan when the 100 HU of thethreshold was detected.
The volumetric data acquired were used to reconstructimages with a section thickness of 0.65 mm and reformat-ted by maximum intensity projection (MIP), multiplanarreconstruction (MPR), and 3D volume-rendered (VR)images using commercially available software (ExtendedBrilliance workspace for Philips 64).
Perforator analysis and planning
Each image set was examined and reconstructed by thesame operator, which kept the technical approach consis-tent at each time point of the procedure. All the measure-ments were performed three times, and themean valuewasused. The measurement and evaluation of the calibre,length, and type (septocutaneous, musculocutaneous) ofperforator were performed on VR, MIP, MPR, and axialsource images by two radiologists in a consensus reading. Ifa consensus could not be reached, an expert radiologist(Z.H.Z., with 18 years of CT experience) determined the finalresult. Because the course of the perforator was usuallycurved or irregular, it was difficult to accurately measurethe length of the perforator. The straight length wasmeasured on VR and MIP to assess the length of theperforator and this parameter was not compared with theoperative findings. It was the preference of the surgeonsthat a minimum perforator diameter of 1 mm be consideredas the basis of a flap to avoid transplantation failure.1
Therefore, 1 mm was considered to be the minimum forperforator evaluation purposes to be enrolled in the anal-ysis. To select suitable perforators for operation, four itemswere analysed in turn: (1) perforator size in diameter, (2)longer length of pedicle, (3) septocutaneous perforator, (4)the perforator contralateral to the side of the lesion(Fig 1aec). After selecting a suitable perforator, its originwas located based on the perpendicular and horizontaldistance from the origin of the perforator to both thesuperior lateral border of the patella and the lateral regionof the thigh (Fig 1d).
Collection of intraoperative data and operation results
In group I, the perforator parameters, including calibre,and the location of the origin were measured, and the typeof perforator was identified during the operation. Theoperation results of all patients, including flap complica-tions, alteration of the donor site, donor site morbidity, andreoperation were recorded.

Figure 1 A 40-year-old man underwent CTA of the thighs. (a) VR image of the left thigh showed that perforator 1 (arrowhead) was larger thanperforator 2 (arrow), but the length of the pedicle was shorter than for perforator 2. (b) The calibre of the left perforator 2 was 1.9 mm (arrow),(c) and the type of perforator 2 was identified as septocutaneous on both the axial view and the oblique coronal MPR (arrow). (d) Finally, theorigin of the left perforator 2 was located.
J.F. Yang et al. / Clinical Radiology 68 (2013) 568e573570
Statistical analysis
SPSS statistical software (version 17.0; SPSS) was used forall data analysis. The data on selected perforators in group Iwere analysed using the paired t-test, and the values werereported as the mean � standard deviation. The operationresults of the two groups were analysed using chi-squareanalysis. p < 0.05 was considered statistically significant.
Results
The accuracy of perforator planning using CTA
There were 16 perforators used for transplantation byplanning, with eight perforators in each thigh. The calibre
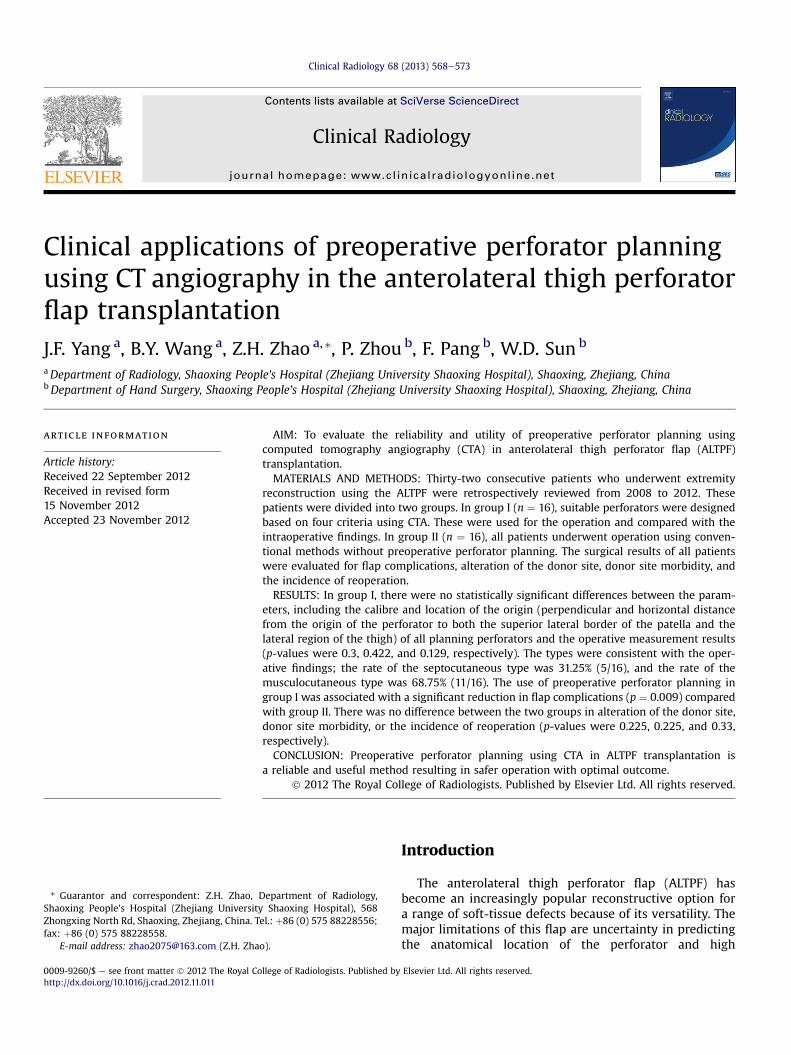
and location of the origin of all planning perforators werenot statistically significant different compared with theoperative measurement results (Table 1; Fig 2a). The typeswere consistent with the operative findings; the rate of theseptocutaneous type was 31.25% (5/16), and the rate of themusculocutaneous type was 68.75% (11/16; Fig 2b).
Results of the operations
No patient in group I required alteration of the donor siteduring operation, and donor site morbidity did not occurafter transplantation. Two patients had flap complications(12.5%): the flap was swollen and became distended due toa venous return obstruction in one patient, and his trans-planted flap survived after transplantation of a greatsaphenous vein. The wound infection of another patient
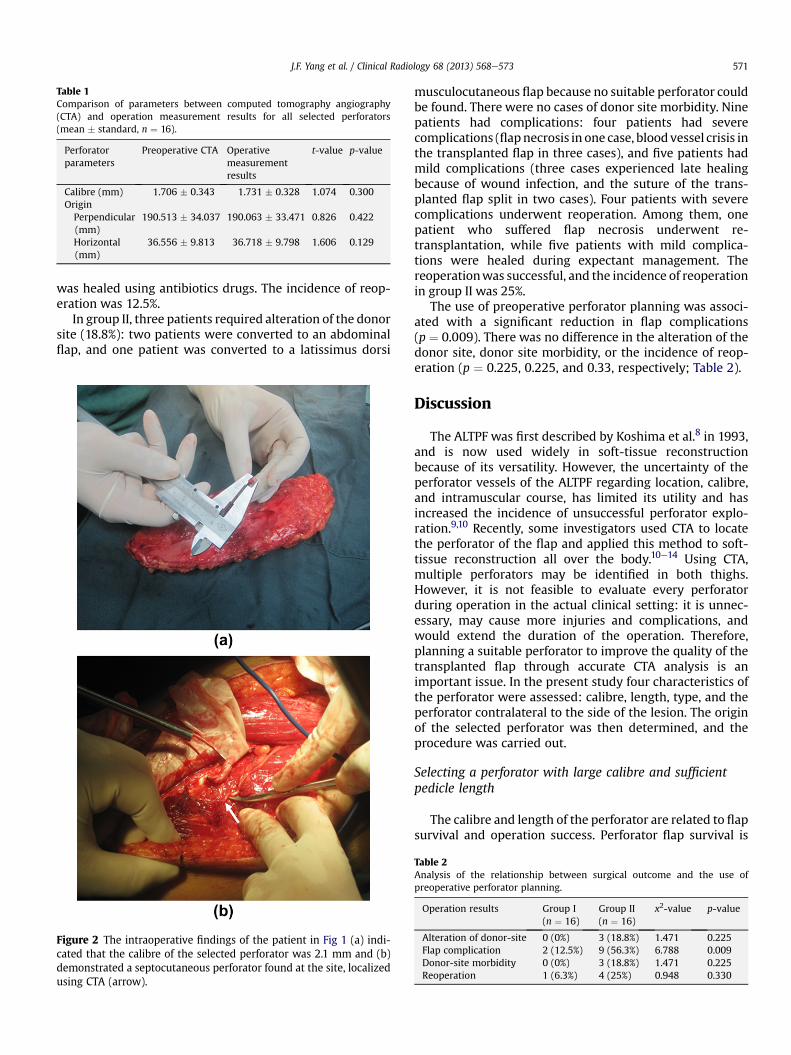
Table 1Comparison of parameters between computed tomography angiography(CTA) and operation measurement results for all selected perforators(mean � standard, n ¼ 16).
Perforatorparameters
Preoperative CTA Operativemeasurementresults
t-value p-value
Calibre (mm) 1.706 � 0.343 1.731 � 0.328 1.074 0.300OriginPerpendicular(mm)
190.513 � 34.037 190.063 � 33.471 0.826 0.422
Horizontal(mm)
36.556 � 9.813 36.718 � 9.798 1.606 0.129
J.F. Yang et al. / Clinical Radiology 68 (2013) 568e573 571
was healed using antibiotics drugs. The incidence of reop-eration was 12.5%.
In group II, three patients required alteration of the donorsite (18.8%): two patients were converted to an abdominalflap, and one patient was converted to a latissimus dorsi
Figure 2 The intraoperative findings of the patient in Fig 1 (a) indi-cated that the calibre of the selected perforator was 2.1 mm and (b)demonstrated a septocutaneous perforator found at the site, localizedusing CTA (arrow).
musculocutaneous flap because no suitable perforator couldbe found. There were no cases of donor site morbidity. Ninepatients had complications: four patients had severecomplications (flapnecrosis in one case, bloodvessel crisis inthe transplanted flap in three cases), and five patients hadmild complications (three cases experienced late healingbecause of wound infection, and the suture of the trans-planted flap split in two cases). Four patients with severecomplications underwent reoperation. Among them, onepatient who suffered flap necrosis underwent re-transplantation, while five patients with mild complica-tions were healed during expectant management. Thereoperationwas successful, and the incidence of reoperationin group II was 25%.
The use of preoperative perforator planning was associ-ated with a significant reduction in flap complications(p ¼ 0.009). There was no difference in the alteration of thedonor site, donor site morbidity, or the incidence of reop-eration (p ¼ 0.225, 0.225, and 0.33, respectively; Table 2).
Discussion
The ALTPF was first described by Koshima et al.8 in 1993,and is now used widely in soft-tissue reconstructionbecause of its versatility. However, the uncertainty of theperforator vessels of the ALTPF regarding location, calibre,and intramuscular course, has limited its utility and hasincreased the incidence of unsuccessful perforator explo-ration.9,10 Recently, some investigators used CTA to locatethe perforator of the flap and applied this method to soft-tissue reconstruction all over the body.10e14 Using CTA,multiple perforators may be identified in both thighs.However, it is not feasible to evaluate every perforatorduring operation in the actual clinical setting: it is unnec-essary, may cause more injuries and complications, andwould extend the duration of the operation. Therefore,planning a suitable perforator to improve the quality of thetransplanted flap through accurate CTA analysis is animportant issue. In the present study four characteristics ofthe perforator were assessed: calibre, length, type, and theperforator contralateral to the side of the lesion. The originof the selected perforator was then determined, and theprocedure was carried out.
Selecting a perforator with large calibre and sufficientpedicle length
The calibre and length of the perforator are related to flapsurvival and operation success. Perforator flap survival is
Table 2Analysis of the relationship between surgical outcome and the use ofpreoperative perforator planning.
Operation results Group I(n ¼ 16)
Group II(n ¼ 16)
x2-value p-value
Alteration of donor-site 0 (0%) 3 (18.8%) 1.471 0.225Flap complication 2 (12.5%) 9 (56.3%) 6.788 0.009Donor-site morbidity 0 (0%) 3 (18.8%) 1.471 0.225Reoperation 1 (6.3%) 4 (25%) 0.948 0.330

J.F. Yang et al. / Clinical Radiology 68 (2013) 568e573572
based on a plentiful blood supply, and the surgeons preferaminimumperforatordiameterof 1mmfor consideration asthe basis of a flap.1 Therefore, searching for a large-calibreperforator is the first step of preoperative perforator plan-ning for ALTPF transplantation. Theoretically, the larger thecalibre of the perforator, the higher the survival rate of theflap; however, transplantation failurewill occur if the lengthof the perforator is too short to connect to the artery of therecipient site.14 Therefore, evaluating the length of theperforator is also significant for ensuring a successful oper-ation. By using preoperative perforator planning in thepresent study,flap complicationswere significantly reduced.Inparticular, noflapnecrosis occurred in theplanning group.Minor flap complications, such as flap infection, were alsodecreased because of the plentiful blood supply. The inci-dence of reoperation is related to severe complications, butthere was no significant difference between groups I and II,perhaps due to insufficient cases. The reason for altering thedonor site was usually a lack of appropriate calibre orinsufficient length of the perforator found during the oper-ation. According to Chen et al.,6 the percentage of cases inwhich no optimal perforator was found was 5.4e16%. Nopatient in the perforator planning group required alterationof donor site during the operation. However, there was nosignificant difference between the two groups. This lack ofsignificance may also be related to the insufficient numbercases in the present study. It is unquestioned that dependingon the accuracy of the CTA, preoperative perforator planningdiminishes the likelihood of altering the donor site duringtransplantation. In the present study, 14 perforators wereselectedusing these twocriteria. Forperforatorswith similaror sufficient calibre and length, the perforator was selectedbased on its type.
Selecting the septocutaneous perforator
The septocutaneous and musculocutaneous perforatorsmostly arise from the descending or the ascending andtransverse branches of the lateral circumflex femoral artery.In 10e20% of cases, the descending branch distributes sep-tocutaneous perforators, which can followa course betweenthe rectus femoris and the vastus lateralis muscle and crossthe fascia lata to supply the skin of the lateral thigh. Mus-culocutaneous perforators, which cross the vastus lateralismuscle and the deep fascia to supply the skin, were found in80e90% of cases.5,15 If the planning perforator is septocuta-neous, flap dissection is likely to be easier, and the injurycaused during operation and donor site morbiditydecreased. Thus, surgeons should select the septocutaneousperforator where possible. In the present study, the septo-cutaneous rate was 31.25%, and the musculocutaneous ratewas 68.75% in the preoperative planning group owing toconscious selection for septocutaneous perforators. Thismethod was used in two patients because the septocuta-neous perforator had sufficient calibre and length. Therewasno patient with donor sitemorbidity in group I, compared tothree cases in group II. Although there was no significantdifference between the two groups, selecting the septocu-taneous perforator still has a certain value.10
Selecting the perforator contralateral to the side of thelesion
In the past, surgeons would choose the donor thighcontralateral to the lesion because it was convenient toaddress the donor site and the recipient site. However,when there was no perforator to use or if the perforatorfound during exploration of the donor thigh was notoptimal for the flap design, it was necessary to changestrategy and explore the other thigh or convert to anotherflap for the reconstruction. The operative time and surgicaldifficulties increased when the chosen thigh was subop-timal.10 With the application of preoperative CTA, surgeonscan choose the thigh with a suitable perforator. However,selecting the contralateral flap of the lesion is moreconvenient for the operation, and the duration of theoperation is reduced if a large-calibre septocutaneousperforator can be used. Regrettably, there was no chance touse this criterion in the present study.
Locating the origin of the selected perforator
If the surgeon pinpoints the origin of a suitable perfo-rator after planning the perforator, the operation will bemore efficient and it will alleviate unnecessary donor sitemorbidity and shorten the operation time. In traditionalALTPF transplantation, the surgeon simply explored theperforator, located in the inferolateral quadrant of a circlewith a radius of 3 cm, with the midpoint between theanterior superior iliac spine and the superolateral corner ofthe patella.16 CTA using CT-guided stereotactic navigationalsystems to precisely localize individual perforators has beenshown to guide flap design and dissection effectively.17
These systems require special software to calculate andmeasure the location of the perforator. However, in thepresent study, the transverse line was drawn on the supe-rior border of the patella, and then the perpendicular andhorizontal distance from the origin of the perforator to boththe superior lateral border of the patella and the lateralregion of the thigh was measured. This method was moreconvenient and produced accurate information regardingthe location of the perforator. In addition, the depth fromthe thigh surface to the origin was measured, but this valuecould not be marked on the thigh before operation, so thisparameter was not adopted.
In conclusion, CTA provides accurate perforator parame-ters. Using CTA during preoperative perforator planning toselect the optimal perforator will not only ensure the flapobtains sufficient blood supply to survive, butwill alsomakethe operationmore expedient, avoid unnecessary donor sitescars, and minimize flap complications, the incidence ofreoperation, and donor site morbidity. Although the perfo-ratorof theALTPF is not theonly factor, it is a crucial factor fortransplanted flap survival and success of the operation.Through the present research, preoperative perforatorplanning using CTA in ALTPF transplantationwas found to bereliable and useful, resulting in safer operations.
The present study had limitations. The first limitationwas the small size of the study groups, which meant that

J.F. Yang et al. / Clinical Radiology 68 (2013) 568e573 573
statistically significant differences in alteration of the donorsite or in donor site morbidity between two groups couldnot be established. Second, the duration of surgery was notavailable to evaluate the advantage of preoperative perfo-rator planning in ALTPF transplantation; the duration ofoperation was not available for some patients who under-went traditional transplantation. There was no way tocompare this value with the preoperative planning group.However, the duration of operation undoubtedly decreasedthrough preoperative planning to select the suitableperforator and pinpoint it. The third limitation is radiationexposure to x-rays, which could not be avoided during CTAexaminations. An x-ray dose that is as low as possible is veryimportant for each patient’s health. Thus, the priority forfuture research will be to investigate the minimum radia-tion dose that produces satisfactory image quality.
Acknowledgement
The authors thank Dr Jianfeng Ping and Dr Xujun Hu forsorting operation data; Wenping Dong, Weiyong Qian, BingChen, and Xuzhong Ying for arranging CTA examination fortransplantation patients.
References
1. Rozen WM, Ashton MW, Pan WR, et al. Anatomical variations in theharvest of anterolateral thigh flap perforators: a cadaveric and clinicalstudy. Microsurgery 2009;29:16e23.
2. Smit JM, Klein S, Werker PM. An overview of methods for vascularmapping in the planning of free flaps. J Plast Reconstr Aesthet Surg2010;63:e674e82.
3. Ulatowski q. Colour Doppler assessment of the perforators of antero-lateral thigh flap and its usefulness in preoperative planning. Pol PrzeglChir 2012;84:119e25.
4. Cheng HT, Lin FY, Chang SC. Evaluation of diagnostic accuracy usingpreoperative handheld Doppler in identifying the cutaneous perforatorsin the anterolateral thigh flap: a systematic review. Plast Reconstr Surg2012;129:769ee70e.
5. Zhang YZ, Li YB, Jiang YH, et al. Three-dimensional reconstructivemethods in the visualization of anterolateral thigh flap. Surg Radiol Anat2008;30:77e81.
6. Chiu WK, Lin WC, Chen SY, et al. Computed tomography angiographyimaging for the chimeric anterolateral thigh flap in reconstruction of fullthickness buccal defect. ANZ J Surg 2011;81:142e7.
7. Garvey PB, Selber JC, Madewell JE, et al. A prospective study of preop-erative computed tomographic angiography for head and neck recon-struction with anterolateral thigh flaps. Plast Reconstr Surg 2011;127:1505e14.
8. Koshima I, Fukuda H, Yamamoto H, et al. Free anterolateral thigh flapsfor reconstruction of head and neck defects. Plast Reconstr Surg1993;92:421e8. discussion 429e30.
9. Chen Z, Zhang C, Lao J, et al. An anterolateral thigh flap based on thesuperior cutaneous perforator artery: an anatomic study and casereports. Microsurgery 2007;27:160e5.
10. Chen SY, Lin WC, Deng SC, et al. Assessment of the perforators ofanterolateral thigh flaps using 64-section multidetector computedtomographic angiography in head and neck cancer reconstruction. Eur JSurg Oncol 2010;36:1004e11.
11. Rosson GD, Shridharani SM, Magarakis M, et al. Three-dimensionalcomputed tomographic angiography to predict weight and volume ofdeep inferior epigastric artery perforator flap for breast reconstruction.Microsurgery 2011;31:510e6.
12. Katz RD, Manahan MA, Rad AN, et al. Classification schema for anatomicvariations of the inferior epigastric vasculature evaluated by abdominalCT angiograms for breast reconstruction. Microsurgery 2010;30:593e602.
13. Ghattaura A, Henton J, Jallali N, et al. One hundred cases of abdominal-based free flaps in breast reconstruction. The impact of preoperativecomputed tomographic angiography. J Plast Reconstr Aesthet Surg2010;63:1597e601.
14. Liu SC, Chiu WK, Chen SY, et al. Comparison of surgical result of ante-rolateral thigh flap in reconstruction of through-and-through cheekdefect with/without CT angiography guidance. J Craniomaxillofac Surg2011;39:633e8.
15. Ribuffo D, Atzeni M, Saba L, et al. Angio computed tomography preop-erative evaluation for anterolateral thigh flap harvesting. Ann Plast Surg2009;62:368e71.
16. Wei FC, Jain V, Celik N, et al. Have we found an ideal soft-tissue flap? Anexperience with 672 anterolateral thigh flaps. Plast Reconstr Surg2002;109:2219e26. discussion 2227e30.
17. Rozen WM, Ashton MW, Stella DL, et al. Developments in perforatorimaging for the anterolateral thigh flap: CT angiography and CT-guidedstereotaxy. Microsurgery 2008;28:227e32.





























