Embed Size (px)
Citation preview
This article was downloaded by: [Umeå University Library]On: 16 August 2014, At: 18:03Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Psychotherapy ResearchPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/tpsr20
Clients’ experiences of moments of sadness inpsychotherapy: A grounded theory analysisJennifer R. Henretty a , Heidi M. Levitt a & Susan S. Mathews ba Department of Psychology ,b Career and Psychological Counseling Center , University of Memphis , Memphis, TNPublished online: 18 Aug 2008.
To cite this article: Jennifer R. Henretty , Heidi M. Levitt & Susan S. Mathews (2008) Clients’ experiences ofmoments of sadness in psychotherapy: A grounded theory analysis, Psychotherapy Research, 18:3, 243-255, DOI:10.1080/10503300701765831
To link to this article: http://dx.doi.org/10.1080/10503300701765831
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Clients’ experiences of moments of sadness in psychotherapy: Agrounded theory analysis
JENNIFER R. HENRETTY1, HEIDI M. LEVITT1, & SUSAN S. MATHEWS2*
1Department of Psychology, and 2Career and Psychological Counseling Center, University of Memphis, Memphis, TN
(Received 2 April 2007; revised 19 October 2007; accepted 22 October 2007)
AbstractAlthough few studies have examined the experience of depression, no research has been conducted on the experience ofsadness in psychotherapy. In this study, clients were interviewed about their experience of sadness using an interpersonalprocess recall method, these interviews were subjected to grounded theory analysis, and a model of sadness experienced inpsychotherapy was derived. The resulting core category*in therapy, the experience of sadness is a struggle against the fearof becoming trapped within the painful, existential question ‘‘Who am I?’’*captures the essence of the experience of theclients’ sadness and describes the struggle, the causes of sadness, and ways therapists facilitated sadness exploration. Thefindings are discussed in reference to clinical application and future psychotherapy research.
Keywords: emotion in therapy; process research; qualitative research methods; experiential/existential/humanistic
psychotherapy; philosophical/theoretical issues in therapy research; sadness; psychotherapy
According to the American Psychological Associa-
tion’s Diagnostic and Statistical Manual of Mental
Disorders (fourth edition, text revision [DSM-IV-
TR]) nosology, psychotherapy clients presenting
with sadness may be suffering from many mental
health disorders, including major depressive disor-
der, dysthymic disorder, bipolar I and II disorders,
seasonal affective disorder, adjustment disorder, and
posttraumatic stress disorder. In this paradigm,
sadness is viewed as an elemental contributor to
depression. Alternatively, sadness can be viewed as a
healthy negative emotion, which is essential for
adaptive functioning and motivational in nature
(e.g., Horstmann, 2003; Huebner & Izard, 1988).
Researchers such as Nesse (1999) believe that as
the human species has evolved, the experience of
sadness has been, and still is, advantageous in a
number of ways. For example, sadness may prevent
immediate future losses by inciting action, sadness
may elicit help from kin, or the experience of sadness
may inspire a reassessment of major life strategies to
necessitate change. However, ‘‘because sadness oc-
curs in situations that are disadvantageous, and
because its characteristics so often seem useless or
harmful, the association bias readily leads to the false
assumption that sadness itself is the problem, instead
of part of the solution’’ (Nesse, p. 442).
Most therapeutic perspectives assume that emo-
tions, such as sadness, are important components of
mental health. Furthermore, for the process of
therapy to take its normal and desirable course, it
is widely believed that emotions should be expressed
(e.g., Greenberg, 1993; Hoehn-Saric, 1977; Plut-
chik, 2000). Nevertheless, therapists practicing un-
der different therapeutic orientations may view and
approach sadness quite differently. A therapist may
attempt directly to control and limit sadness (e.g., in
cognitive�behavioral therapy) or to evoke and ex-
plore the emotion (e.g., in emotion-focused ther-
apy). Furthermore, no therapeutic perspective has
derived a model specific to the experience of sadness
in psychotherapy (Malkinson, 2001), and there are
no previous investigations of the inner experience of
sadness within psychotherapy.
The investigators in this study were interested in
processes of sadness that cut across diagnoses,
disorders, and client concerns. On the front end,
this research did not distinguish among grief, loss,
and depression; nor did the question of what had
caused the sadness define the focus of the study.
*Susan S. Mathews is now at the Counseling and Testing Center, University of Kentucky, Lexington
Correspondence: Jennifer R. Henretty, Department of Psychology, 202 Psychology Building, University of Memphis, Memphis, TN 38152.
E-mail: [email protected]
Psychotherapy Research, May 2008; 18(3): 243�255
ISSN 1050-3307 print/ISSN 1468-4381 online # 2008 Society for Psychotherapy Research
DOI: 10.1080/10503300701765831
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

Using the interpersonal process recall method of
interviewing (Kagan, 1975), this study asked clients,
‘‘What is your experience of moments of sadness in
psychotherapy?’’ Grounded theory analysis (Glaser
& Strauss, 1967) then was used to explore that
subjective experience and to develop an empirically
grounded theory of sadness in therapy.
Method
Participants
Interviewees. Ten clients were interviewed for this
study (the rationale for this number of participants is
described in the Grounded Theory Analysis sec-
tion). The interviewees ranged in age from 20 to 63
years (M�32.9). Six of the interviewees were female
and four were male. Seven of the interviewees
identified themselves as Caucasian, one as African
American, one as biracial, and one as Jewish. The
interviewees expressed sadness about a variety of
topics, including death of a loved one, past addic-
tion, dissolution of relationships, and racial tension.
Nine of the 10 interviewed clients were seen by
female therapists. Five of the clients were seen by
therapists who were clinical or counseling doctoral
psychology interns practicing at an in-house uni-
versity training center serving the student popula-
tion. Two were seen by therapists who were clinical
doctoral psychology practicum students practicing at
an in-house university training center serving the
Memphis community. The remaining three were
seen by licensed psychologists in private practice in
the greater Memphis area. Four of the clients’
therapists identified their psychotherapeutic orienta-
tion as integrative, three as cognitive�behavioral, and
three as humanistic.
Researchers. Jennifer R. Henretty, a doctoral stu-
dent in clinical psychology at the University of
Memphis, conducted the interviews and the primary
analysis of the data. Heidi M. Levitt, an associate
professor at that university with expertise in qualita-
tive methods, met with the primary researcher
weekly to review the ongoing analysis and developing
theory. Susan S. Mathews, an adjunct professor at
the University of Memphis, made suggestions to the
final hierarchy and contributed to the project design.
Jennifer R. Henretty does not have an established
therapeutic orientation, and Heidi M. Levitt uses an
integrative approach to therapy based within a
humanistic constructivist approach. Susan S. Math-
ews holds interests in feminist therapy and hyp-
notherapy. At the onset of this study, the researchers
did not have expectations as to what the results
would reveal; however, they believed that many
people carry unresolved, often ignored sadness
within themselves until it becomes unavoidable,
and that therapy could teach clients to better under-
stand and cope with this emotion.
Procedure
Recruitment. Recruitment occurred in two steps.
The first entailed clients consenting to have one or
more of their therapy sessions audio recorded; the
second entailed clients’ consenting to be interviewed
about their recorded sessions. Recruitment took
place at two psychotherapy clinics and in two private
practices. Although all clients were recruited in two
steps, the process of recruitment varied slightly
depending on the location. In one of the clinics, all
sessions of interested clients were audio recorded as
part of a larger study. In the other settings, therapists
nominated clients based on the study’s eligibility
criteria, and those clients who were interested in
participating had one of their sessions audio re-
corded. Clients eligible for this study were adults
receiving individual psychotherapy who were not
exhibiting any psychotic symptoms or at high risk for
suicide. Furthermore, eligible clients could not be in
their first two sessions of therapy because these
sessions often entail intake procedures and, there-
fore, are not representative of the psychotherapeutic
process; nor could they be in their final two
termination sessions of therapy. The researchers
were interested in interviewing clients who had a
range of characteristics in order to obtain an
encompassing theory of sadness. They sought diver-
sity in clients’ age, race, gender, and reported cause
of sadness.
All interested clients were told that the study’s
concentration was the psychotherapy process. Sad-
ness was not mentioned as a focus so as not to
change the course of the therapy under examination.
Clients were informed that full participation would
entail the audio recording of at least one of their
therapy sessions as well as an interview about their
experience of therapy. This interview, they were told,
would take place within 72 hrs of their recorded
session, would last from 1 to 2 hrs, and would
provide $20 compensation. Clients also were noti-
fied that they could consent to have their session
recorded (Step 1 of recruitment) and then decide
after their recorded session whether or not they
wanted to consent to participate in an interview
(Step 2 of recruitment).
Additionally, it was explained to clients that their
therapists would not have access to any of the
information shared within the interviews but that
their therapists would know that they were partici-
244 Henretty, Levitt, and Mathews
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

pating in the study, because the therapists recorded
the sessions and had to give permission to be
recorded themselves. Therapists were given scripts
to facilitate discussion of the study between therapist
and client. These scripts emphasized to clients that
therapists would feel fine whether clients decided to
participate or not, and that the therapy would not be
influenced regardless of the decision.
Interpersonal Process Recall Interviews. Born from
Kagan et al.’s investigations into empathy, interper-
sonal process recall (IPR) was a technique designed
to ‘‘stimulate recall of the underlying dynamics
involved in an interpersonal interaction’’ (Kagan &
Schauble, 1969, p. 313). The technique originally
involved a participant and an interviewer watching a
video-recorded interaction, with either party free to
pause the recording to discuss the participant’s
recalled thoughts and feelings, interpret statements,
and elaborate on meanings. ‘‘Apparently the [parti-
cipant] feels removed enough from the [recording] of
himself . . . that he is able to think of the ‘person’ . . .as a being well known to him, yet not quite he’’
(Kagan, Krathwohl, & Miller, 1963, p. 239). This
removed examination of oneself makes this method
suitable to explore the subjective, sometimes fleet-
ing, experience of clients’ sadness during psy-
chotherapy; therefore, the current study uses a
variation of Kagan et al.’s IPR technique.
For this study, interested clients who met the
eligibility requirements were contacted after their
audio-recorded session to set up an individual meet-
ing to discuss and possibly conduct an IPR interview.
IPR interviews commenced after clients were told
that the interview’s focus would be on their experi-
ence of sadness in therapy and after they consented
to be interviewed. During the IPR interviews, each
client and the primary researcher listened to the
audio recording of the client’s session. All clients
were asked to pause the recording when they
recognized that they had begun experiencing sadness
in the session. The interviewer inquired about
sections of the recording, however, if they had been
overlooked by a client and yet appeared to demon-
strate client sadness.
The interviews were semistructured. The inter-
view questions (see Appendix) were designed to be
nonbiasing and to elaborate on the central question
of the interview: ‘‘What is your experience of
moments of sadness in psychotherapy?’’ Specific
questions explored the genesis of the individual
moments of sadness, how the experience of sadness
might have changed within the interaction, and
clients’ reaction to different interventions by their
therapists. It was difficult to tabulate the number of
sadness experiences discussed in each interview
because some clients reported experiencing a sad-
ness throughout their session and others described
sadness experiences as interconnected and hard to
separate.
On average interviews were 1.5 hrs (range�1�2hrs). At the end of each interview, clients were asked
about their experience of the IPR interview to
validate the credibility of the interview process and
gain more understanding about the information
gathered therein. In addition, to encourage clients
to continue processing their sadness experiences,
they were asked to consider whether there was
anything from the interview that they wished to
discuss with their therapist in their next session.
Grounded Theory Analysis. Grounded theory ana-
lysis (see Glaser & Strauss, 1967, for a detailed
description) allows a researcher to study a subjective
experience and, through a method of inductive
categorization, generate a model of the phenom-
enon. It is an approach to research that is designed to
stimulate rather than verify theory. This study used a
version of this method that has been advocated by
Rennie, Phillips, and Quartaro (1986).
After each IPR interview on a client’s experience
of sadness had been transcribed, it was analyzed and
divided into chunks of text that differentially ex-
pressed a main idea, or meaning, related to sadness.
These meaning units (Giorgi, 1970) were compared
and organized into emerging themes, or descriptive
categories. In turn, the initial descriptive categories
were grouped based on their commonalities into
more abstract, higher order categories. These higher
order categories then were compared and even
higher order categories emerged. The organizing
and sorting of meaning units into higher and higher
order categories continued, producing a data hier-
archy, until the core category was formed at the
hierarchy’s apex.
The researchers, whose epistemology is based
within a methodological hermeneutic approach (see
Rennie, 2000, for a detailed description), view
grounded theory initially as a process of ‘‘abduc-
tion,’’ in which researchers, immersed in the data at
hand, develop provisional theories about the com-
monalities between units of data. Then a process of
induction is used to assess whether that under-
standing best represents the commonalities in evi-
dence. These developing theories continually are
refined and reassessed as units are added into
categories and as categories are organized into higher
order categories.
This procedure is understood by the researchers to
represent an interplay between subjective and objec-
tive processes: The abductions are a subjective
impression of commonalities and the process of
Moments of sadness 245
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4
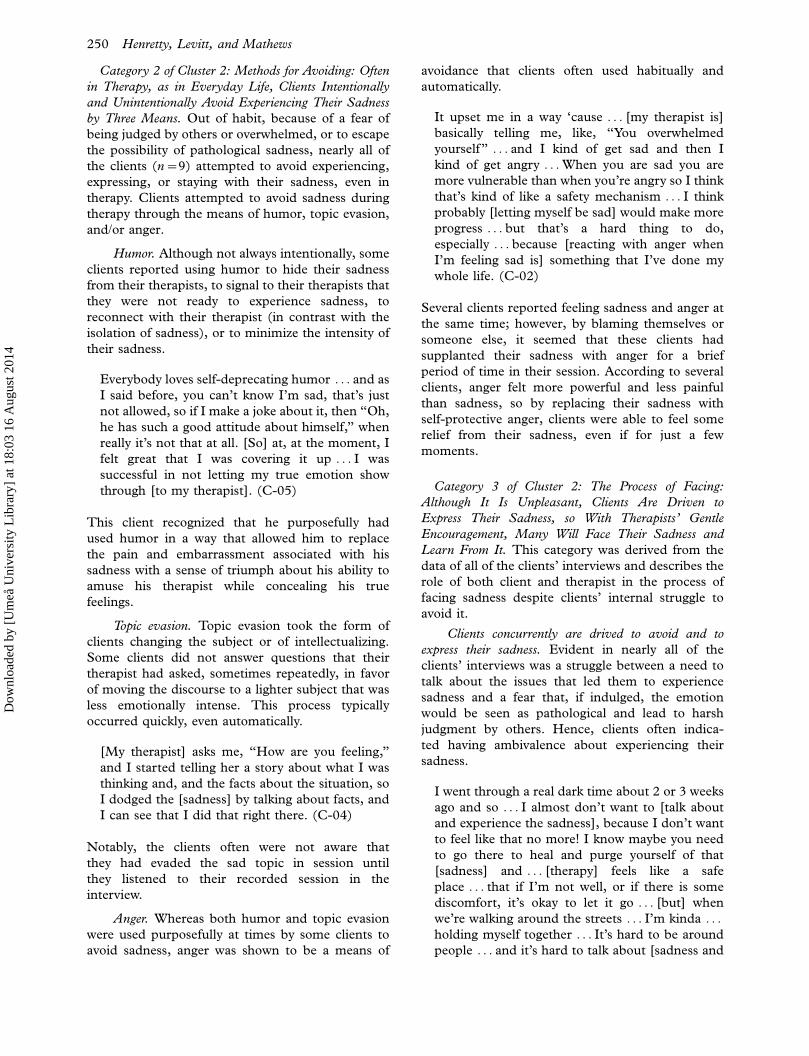
yrogetac eroC N retsulC N yrogetaC N yrogetacbuS N
8 ?I ma ohW :msicitirc-fles htiw detaicossa ssendaS
8 em tuoba ssendaS ni I ma ohW :msicitirc-rehto htiw detaicossa ssendaS
?srehto ot noitaler2
dna ssenilenol morf ssendaS tuohtiw I ma ohW :ssol
?tsol evah I tahw tuohtiw I ma ohW ?srehto6
ehT :?I ma ohW
noitseuq laitnetsixe
ni ssendas gniylrednu
yparehtohcysp
01
8 )srehto ro/dna( em rof ssendaS era ohW :ssendas citsiurtlA laitnetsixe regral dnA ?ew
gninaem s'efil tuoba snoitseuq4
6 etauteprep-fles nac ssendaS a sa :gniwollaw tuoba snrecnoC fo raef peed a fo tluser
ot detnaw stneilc ynam ,ssendas rieht ni kcuts gnimoceb
yllaminim ylno ssendas ecneirepxe
9
7 gnol oot rof tlef nehw evitcudorpnu eb nac ssendaS
5 romuH
7 noisave cipoT
ht ni netfO :gnidiova rof sdohteM ,efil yadyreve ni sa ,ypare
tninu dna yllanoitnetni stneilc gnicneirepxe diova yllanoitne
snaem eerht yb ssendas rieht
9
5 regnA
sserpxe ot dna diova ot nevird era yltnerrucnoc stneilC
ssendas rieht01
eht ,ypareht nI
fo ecneirepxe
elggurts a si ssendas
fo raef eht tsniaga
deppart gnimoceb
,lufniap eht nihtiw
noitseuq laitnetsixe
”?I ma ohW“
01
htiw elggurts ehT
ot :ypareht ni ssendas
ro ,diova ,wollaw
?ecaf
01
nevird era stneilc ,tnasaelpnu hguohtlA :gnicaf fo ssecorp ehT
os ,ssendas rieht sserpxe ot eltneg ’stsipareht htiw ,
ecaf lliw ynam ,tnemegaruocne ti morf nrael dna ssendas rieht
01 yb ssendas fo noitarolpxe egaruocne stsiparehT
igdelwonkca ,gnidael gnitcelfer dna ,gn01
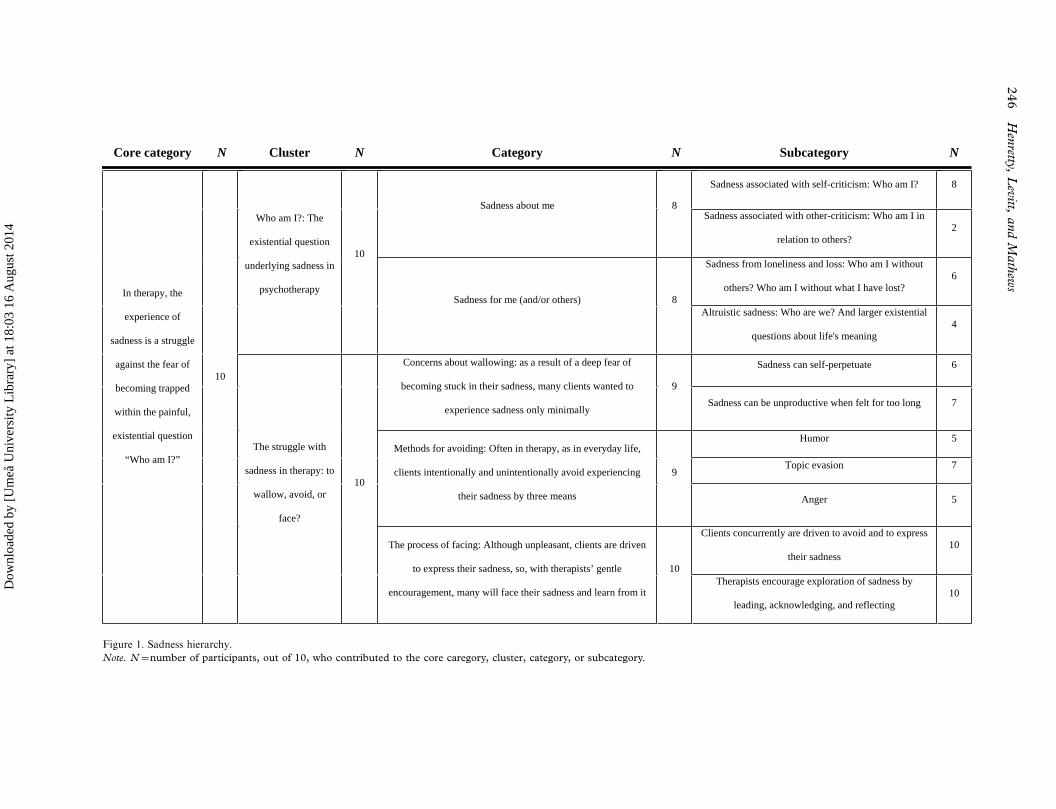
Figure 1. Sadness hierarchy.
Note. N�number of participants, out of 10, who contributed to the core caregory, cluster, category, or subcategory.
246
Hen
retty,L
evitt,
and
Math
ews
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

induction is an empirical analysis of the data.
However, objective analysis itself is thought to be a
form of perspective taking housed within subjectivity
(hence, different people may adopt somewhat dif-
ferent perspectives when trying to be objective; see
Nelson, 1990, for a detailed discussion of sub-
jectivity�objectivity and empiricism); therefore,
grounded theory analysis often is considered an
interpretive process. As such, it is important for
investigators to foster self-awareness during the
analysis.
To do so, in this study the primary researcher kept
a log, or memos, of her beliefs, perceptions, and
theories pertaining to sadness during the interview
and analysis phases of the study. This process
allowed the researcher to keep track of and cultivate
her developing understandings and to note decisions
made about the coding and method. Also, it allowed
her to examine her hesitations in interpretation and
explicitly recognize her assumptions, thereby redu-
cing the effect of biases on the analysis.
During the analysis phase, IPR interviews con-
tinued to be conducted and incorporated into the
developing hierarchy until saturation (Glaser &
Strauss, 1967) was reached (i.e., the point at which
transcripts, when broken into meaning units and
added to the hierarchy, resulted in no additional
higher order categories). In this study, saturation
occurred at the seventh transcript, meaning that the
last three transcripts, although they were included in
the hierarchy, did not contribute novel higher order
categories. The NUD*IST 4 (Non-Numerical Un-
structured Data Indexing Searching and Theorizing;
1997) software program was used to facilitate the
organization of the data into a hierarchical structure.
Results
The data derived from the interview transcripts
consisted of 417 meaning units. Because some
meaning units were assigned to more than one first
order category, the final 10-level hierarchy included
786 total meaning units. The following terms are
used to describe the top levels in the analysis, those
that are theoretically most meaningful: The core
category is the highest layer in the hierarchy and
subsumes two clusters. The first cluster contains two
categories (high-level categories) and the second
cluster contains three categories; these five cate-
gories in total are composed of 11 subcategories
(Figure 1). This section is organized so that the
core category is described first. Each cluster then is
discussed, including a description of the categories
each cluster subsumes and the subcategories each
category subsumes.
Core Category: In Therapy, the Experience of
Sadness Is a Struggle Against the Fear of
Becoming Trapped Within the Painful,
Existential Question ‘‘Who Am I?’’
The core category was generated to capture the
essence of the experience of the clients’ sadness in
therapy. Sadness, when experienced in therapy, was
an existential event for the clients, usually a self-
critical one. Sadness arose for the clients when the
topic of discussion had existential implications
regarding who the client is, who the client strives
to become, and how the client relates in the world.
When clients were able to experience sadness and
identify the cause of their self-criticism, they became
better able to evaluate their judgments and to
motivate themselves to change or, instead, to learn
to accept themselves as they are.
There was a fundamental struggle central to the
experience of sadness that existed because the
clients (intentionally and unintentionally) were
driven concurrently to avoid and face their sadness
in therapy. Nearly all of the clients avoided sadness
to some extent because it was emotionally and
physically painful and exhausting, it rendered them
vulnerable to others’ judgment, and they reported
being accustomed to hiding their sadness from
others in everyday life. In addition, nearly all of
the clients were afraid that their sadness was, or
would become, consuming and unhealthy if in-
dulged. However, many of the clients felt a strong
need to express their sadness and tell their story.
Plus, some of the clients viewed their sadness as a
powerful tool for motivation and self-knowledge.
Therefore, many of the clients chose to struggle
against their fears and confront their sadness in
session. The core category was derived from the
commonalities that were identified within the
following two clusters.
Cluster 1: Who Am I? The Existential Question
Underlying Sadness in Psychotherapy. The first cluster
focused on the origin of sadness for clients and was
generated from meaning units from all 10 of the
participants. The data for this cluster indicated that
the sadness experienced in sessions had existential
implications or meanings. For clients to have felt
sadness during therapy, they had to have had
experiences that undermined their conceptualiza-
tions of being: the meaning or order they ascribed
to life, their values, and/or their understandings of
who they are. There were two categories in this
cluster.
Category 1 of Cluster 1: Sadness About Me. The
findings suggested that most of the sadness experi-
Moments of sadness 247
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

ences that clients (n�8) reported reflected a
sadness about themselves, a gnawing self-critical
sadness indicative of the existential question, ‘‘Who
am I?’’ This self-criticism was reported to have a
haunting quality in that it often loomed in the
clients’ thoughts but less often became the focus of
thought itself. As a result, clients rarely thought
they could influence or reassess these judgments.
For example, one client (C-10) reflected on his
experience in session:
I just sort of talked myself into [my sadness];
about how I can’t really escape and I’m just stuck
being alive and being who I am, and that’s
honestly something that I am not really cool with
and that makes me sad.
This existential sadness was associated with
self-critical perceptions of oneself incited by self
or by others, as described in the following sub-
categories.
Sadness associated with self-criticism: ‘‘Who am I?’’
This sadness took the form of direct self-criticism
and often pertained to feelings such as ‘‘I am not
who I want to be’’ or ‘‘I am not myself.’’ In these
moments, sadness evolved from a sense of futility in
reaction to harsh self-evaluation. For instance, a
client conveyed,
I felt . . . sadness because . . . I feel . . . hopeless
about things . . . like, ‘‘Oh I can’t ever have this
conversation, and I can never be vulnerable like
this in real life’’ and . . . that makes me feel sad
because I . . . believe that, even though . . . my
rational mind isn’t really sure . . . the negative
thoughts around it make me feel . . . .deeply hope-
less about my personality, which is a lot sadder.
(C-01)
This client was expressing sadness over her belief
that she will never be able to show her vulnerability
because it is beyond the realm of how she exists in
the world. Whereas her critical thoughts came from
who she is now, this type of self-critical sadness also
was related to who the client used to be:
When you’re . . . active in AA, you’re supposed to
be alright; you’re supposed to be okay now,
cause you don’t do those things anymore, you
know what I mean. But . . . I guess the sadness
is . . . not really disgust, that’s not really the right
word, but just ‘‘Damn, you know, why’d you do
all that?’’ and I know that I’m an alcoholic . . .but still, how can that be so much, how can that
make all your decisions for you? So, it’s just, it’s
sad. (C-09)
Clients’ sadness of this sort often was expressed in
relation to feelings of guilt and self-loathing because
who they were was not aligned with their notion of
who they should have been.
Sadness associated with other-criticism: ‘‘Who am I in
relation to others?’’ This form of sadness appeared to
be based on self-criticism rooted in others’ assess-
ments. Although clients sometimes saw the criticism
as having become an introject, they often attributed
it to others even while they used it to condemn
themselves:
The . . . fact of . . . not being accepted by different
classes [bothers me]. Ah, I don’t know, it just, it
makes me feel . . . like I’m different, kind of an
outcast. And, and if I feel that way, or if I feel
like I’m being judged, if I feel like I’m being
attacked, then that, it does, it saddens me,
because a lot of times it’s things that I have no
control over. (C-03)
This subcategory also illustrates that just because the
sadness is self-critical does not preclude the possibi-
lity that the client may be living in a societal context
(e.g., classism, racism, sexism) that fosters the self-
criticism.
Category 2 of Cluster 1: Sadness For Me (and/or
Others). Also experienced by clients (n�8) was an
existential sadness that was not self-critical but
instead stemmed from loneliness, loss, or others’
hardship.
Sadness from loneliness and loss: ‘‘Who am I without
others?’’ ‘‘Who am I without what I have lost?’’ This
sadness for oneself tended to pertain to poignant
experiences of existential loneliness or loss (of some-
thing, such as a job or ideal, or of someone, as in
death or a relational breakup). For example, one
client said,
[My sadness is] just torrential, it’s like I might be
going to drown . . . it’s so overwhelming. It’s so
lonely and . . . bittersweet to have this incredible
relationship and it’s gone . . . I was so blessed to
have had him in my life*that part is fabulous . . .but the bad part is that he’s gone . . . I don’t
know . . . how I’m . . . going to be able to go on.
(C-06)
Her sadness resulting from loss, much like that of the
other clients who described this type of sadness, led
to profound questions about future identities, as she
had to envision new ways of living in the world and
making meaning in spite of loneliness and significant
loss.
248 Henretty, Levitt, and Mathews
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

Altruistic sadness: ‘‘Who are we?’’ and larger existen-
tial questions about life’s meaning. When clients had
sadness about others’ hardship (altruistic sadness),
the experience made them question their values in
relating to others, their meanings about relation-
ships, or the way they had made sense of the world.
As one participant described,
It’s such a huge thing . . . that sadness for my
mother and what she faced all those years
ago . . . Sadness at seeing her when she was, I
remember when she was telling me, lying in the
hospital room bed, about it. (C-08).
This sense of sadness over learning of her mother’s
past abuse forced the client to question her
fundamental beliefs about the world being safe
and just.
Across the categories and subcategories in this
cluster, clients’ sadness was described as rooted
within the existential question of ‘‘Who am I?’’ The
sadness made the clients question who they are in
relation to others, who they are in relation to whom
they would like to be, or who they are in relation to
their world and its meaning.
Cluster 2: The Struggle With Sadness in Therapy: To
Wallow, Avoid, or Face? The second cluster focused
on the process of experiencing in-session sadness for
clients and was generated from data from all of the
participating clients. Whereas nearly all the clients
reported that experiencing some sadness was helpful
to the process of therapy, many of the clients
expressed an aversion to the experience of sadness.
This paradox created an internal struggle for the
clients during therapy that they constantly had to
negotiate. They appeared to be oriented to the
conflict in three ways.
Category 1 of Cluster 2: Concerns About Wallowing:
Because of a Deep Fear of Becoming Stuck in Their
Sadness, Many Clients Wanted to Experience Sadness
Only Minimally. Nearly all of the clients (n�9)
talked about their fear of, or aversion to, becoming
trapped or staying with their sadness for too long.
Several of the clients mentioned that in the past they
had ‘‘wallowed’’ in sadness and that they did not
want to have that experience again. Although the
clients did not explicitly describe this state of being
stuck in sadness as pathological, many used words
indicative of this conceptualization. For example,
clients described sadness as ‘‘not feeling well,’’ ‘‘an
addiction,’’ being ‘‘in bad shape,’’ being ‘‘crazy,’’ and
going ‘‘nuts.’’ As one client commented,
You don’t want to be that sad all the time
[because] . . . you’re kind of being looked down
upon; or you’ll be considered a freak or . . . an
outcast . . . .[and] that you’re out of lock step with
the rest of the world. Isn’t that bizarre? It’s like you
have a disease and it might be catching? . . . And ‘‘I
don’t want to give it to you.’’ Or ‘‘I’m afraid I
might catch it . . . ’’ They’re more afraid that they
might catch it from you. (C-06)
This concern led clients to push away the experience
of sadness when it arose, even in therapy. They
worried that allowing themselves to fully engage their
sadness could lead to depression and, subsequently,
harsh judgment by others.
Sadness can self-perpetuate. Some clients dis-
cussed the experience of being sad about sadness.
Because sadness was thought to be a dangerous
emotion, knowing that they were sad seemed to
make them feel even sadder for themselves.
When I’m talking about discouragement and
about trying to change aspects of my life and . . .failed attempts, I’m experiencing sadness because
I’m not only . . . remembering those attempts but I
kind of also emotionally relive them . . . So right
there, I’m . . . feeling sad . . . realizing I [emotion-
ally relive past sadness] and how it hinders me . . .I’m recognizing that I do that and that makes me
sad. (C-05)
This client worried that he would become trapped in
a cyclical process of ever increasing sadness with
little chance for escape.
Sadness can be unproductive when felt for too long.
Among those clients who believed the experience of
sadness to be advantageous to the process of therapy,
many clients expressed a belief that sadness was
good only in moderation. Although these clients
often examined their sadness in therapy, they con-
tinued to hold reservations about the hazards of the
emotion.
I know [sadness is] there, I just don’t want [it] to
stay there; I just don’t want it to be part of my
makeup . . . I kind of fight it . . . and I know that’s
not probably healthy, but I fight it; I don’t want to
feel it . . . I think at times it is [helpful to feel
sadness] . . . but I also think that . . . in times
I’ve . . . stayed stuck on the sadness . . . too long
to where it’s counterproductive. (C-04)
It seemed that these clients feared that if they were
not careful, their sadness could become pathological
and consuming; consequently, exploration pro-
ceeded with caution.
Moments of sadness 249
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4
Category 2 of Cluster 2: Methods for Avoiding: Often
in Therapy, as in Everyday Life, Clients Intentionally
and Unintentionally Avoid Experiencing Their Sadness
by Three Means. Out of habit, because of a fear of
being judged by others or overwhelmed, or to escape
the possibility of pathological sadness, nearly all of
the clients (n�9) attempted to avoid experiencing,
expressing, or staying with their sadness, even in
therapy. Clients attempted to avoid sadness during
therapy through the means of humor, topic evasion,
and/or anger.
Humor. Although not always intentionally, some
clients reported using humor to hide their sadness
from their therapists, to signal to their therapists that
they were not ready to experience sadness, to
reconnect with their therapist (in contrast with the
isolation of sadness), or to minimize the intensity of
their sadness.
Everybody loves self-deprecating humor . . . and as
I said before, you can’t know I’m sad, that’s just
not allowed, so if I make a joke about it, then ‘‘Oh,
he has such a good attitude about himself,’’ when
really it’s not that at all. [So] at, at the moment, I
felt great that I was covering it up . . . I was
successful in not letting my true emotion show
through [to my therapist]. (C-05)
This client recognized that he purposefully had
used humor in a way that allowed him to replace
the pain and embarrassment associated with his
sadness with a sense of triumph about his ability to
amuse his therapist while concealing his true
feelings.
Topic evasion. Topic evasion took the form of
clients changing the subject or of intellectualizing.
Some clients did not answer questions that their
therapist had asked, sometimes repeatedly, in favor
of moving the discourse to a lighter subject that was
less emotionally intense. This process typically
occurred quickly, even automatically.
[My therapist] asks me, ‘‘How are you feeling,’’
and I started telling her a story about what I was
thinking and, and the facts about the situation, so
I dodged the [sadness] by talking about facts, and
I can see that I did that right there. (C-04)
Notably, the clients often were not aware that
they had evaded the sad topic in session until
they listened to their recorded session in the
interview.
Anger. Whereas both humor and topic evasion
were used purposefully at times by some clients to
avoid sadness, anger was shown to be a means of
avoidance that clients often used habitually and
automatically.
It upset me in a way ‘cause . . . [my therapist is]
basically telling me, like, ‘‘You overwhelmed
yourself ’’ . . . and I kind of get sad and then I
kind of get angry . . . When you are sad you are
more vulnerable than when you’re angry so I think
that’s kind of like a safety mechanism . . . I think
probably [letting myself be sad] would make more
progress . . . but that’s a hard thing to do,
especially . . . because [reacting with anger when
I’m feeling sad is] something that I’ve done my
whole life. (C-02)
Several clients reported feeling sadness and anger at
the same time; however, by blaming themselves or
someone else, it seemed that these clients had
supplanted their sadness with anger for a brief
period of time in their session. According to several
clients, anger felt more powerful and less painful
than sadness, so by replacing their sadness with
self-protective anger, clients were able to feel some
relief from their sadness, even if for just a few
moments.
Category 3 of Cluster 2: The Process of Facing:
Although It Is Unpleasant, Clients Are Driven to
Express Their Sadness, so With Therapists’ Gentle
Encouragement, Many Will Face Their Sadness and
Learn From It. This category was derived from the
data of all of the clients’ interviews and describes the
role of both client and therapist in the process of
facing sadness despite clients’ internal struggle to
avoid it.
Clients concurrently are drived to avoid and to
express their sadness. Evident in nearly all of the
clients’ interviews was a struggle between a need to
talk about the issues that led them to experience
sadness and a fear that, if indulged, the emotion
would be seen as pathological and lead to harsh
judgment by others. Hence, clients often indica-
ted having ambivalence about experiencing their
sadness.
I went through a real dark time about 2 or 3 weeks
ago and so . . . I almost don’t want to [talk about
and experience the sadness], because I don’t want
to feel like that no more! I know maybe you need
to go there to heal and purge yourself of that
[sadness] and . . . [therapy] feels like a safe
place . . . that if I’m not well, or if there is some
discomfort, it’s okay to let it go . . . [but] when
we’re walking around the streets . . . I’m kinda . . .holding myself together . . . It’s hard to be around
people . . . and it’s hard to talk about [sadness and
250 Henretty, Levitt, and Mathews
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

what makes me sad] and it’s not safe to talk about
that stuff in most circles. (C-04)
Furthermore, most of the clients described sadness
as powerfully negative, even disintegrating:
I’m coming unglued; I’m coming unglued. I can
hear [the sadness] in my voice. I’m losing it . . . It’s
crushing me. It’s so sad. It’s hurting me so bad . . .It is totally, totally overwhelming . . . [My sadness
is] terrible because it’s just so all encompassing
and it drags you down and it’s scary and you
wonder, ‘‘Well, how long is it going to be with
me?’’ (C-06)
Despite the pain in these experiences, nearly all of
the clients indicated that expressing their sadness at
times felt good, motivated them to act, or helped
them understand why they felt sad, all of which they
believed would help them to feel less sad in the
future.
If you examine why you’re sad, I think it helps you
understand certain, certain things like um, I mean
there’s certain things about me that I get really
upset about . . . I wouldn’t have been able to
recognize that maybe 2 years ago but because
I’ve talked about it with [my therapist], I can see
that a little bit, I can see it clearly, you know, and
so . . . I didn’t get as upset as I used to. (C-07)
Therefore, almost all of the clients were willing to
face their sadness, at least for brief periods of time.
While experiencing sadness, nearly all of the
clients would move into the intense emotion, then
retreat, and subsequently move back in. It seemed
that by briefly distancing themselves from the sad-
ness when its duration or intensity became too great,
the clients were more able and willing to return to
their sadness and continue the exploration. There-
fore, this retreating response served as a brief but
beneficial respite, allowing the clients to consolidate
their thoughts, reconnect with the therapist, or
manage the intensity of their emotions.
Therapists encourage exploration of sadness by
leading, acknowledging, and reflecting. Clients re-
ported that their therapists facilitated this explora-
tion by leading the conversation to focus on the
sadness at a pace that felt comfortable to the client,
by being nonjudgmental, and by simply being ‘‘a
professional.’’ This gentle encouragement instilled
clients with a sense of trust in their therapists and in
the process of therapy.
I beat around the bush . . . I don’t know if [my
therapist] knows that about me or what, but . . . if
she would have asked me from the beginning,
‘‘How does [giving up custody of your son] relate
to you [abandoning] your dogs?,’’ I would have
come up with something so quick . . . who knows
what I would have done. But the way that she’s
making me beat around the bush . . . and . . . giving
me time to . . . get my head around it . . . I’m able
to talk about it . . . ‘cause . . . if it’s sudden I put up
the defenses . . . immediately. (C-09)
Also, some of the clients indicated that they made
gains in understanding and alleviating their sadness
when their therapists reflected their feelings and
their sad narratives back to them.
Whenever [my therapist] asks me questions like
that, when she kind of recaps it, it makes me feel a
lot better . . . What I think she’s trying to do is
trying to challenge me to think of something
different . . . or put things in a different perspec-
tive. It just makes me feel a lot better because then
I can kind of tie stuff in as far as like what she and I
are talking about and see how it’s relating to me as
far as why I’m [in therapy]. (C-03)
Listening to their therapists redescribe their experi-
ence of sadness provided some clients the distance
and perspective needed to make connections and
develop self-compassion.
Additionally, it seemed that it was important for
some clients to learn how to hold the experience of
sadness at hand long enough both to feel the
emotion and to explore what the sadness meant for
them. This lesson could be a difficult but transfor-
mational one because it afforded clients new ways of
dealing with and learning from their sadness instead
of fearing and avoiding the experience.
[My therapist is] saying here, ‘‘What will it be like
to give yourself permission to [be sad]?’’ It really
was [a new idea to me]. It blew me away . . . She’s
just helping me try to . . . say [to myself], ‘‘You
know, this is where you are and it’s okay.’’ And
‘‘It’s okay to grieve because you’ve had so much on
your plate and you haven’t been able to [be sad]
but now you can; now you must.’’ It’s good . . . It’s
a real relief . . . I need to cut myself some slack . . .It’s validating . . . It’s okay to have [sadness] . . . it’s
normal. (C-10)
Once they saw their sadness as valid and normal,
some of the clients allowed themselves to fully
experience their sadness, and, as a result, they
developed new understandings about their experi-
ence.
Moments of sadness 251
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

In summary, the results of this research suggested
that (a) at root, the majority of the clients’ sadness
was linked to self-criticism that impacted the mean-
ing the clients made of themselves, their lives, and
their world; and (b) that the process of exploring and
expressing sadness was daunting for the clients, who
were afraid that their sadness would overpower and
control them. Furthermore, this conceptual model
provided an understanding of the intrapsychic con-
flict that the clients navigated while accessing (or
choosing not to access) their sadness in therapy and
identified ways that their therapists facilitated sad-
ness exploration.
Discussion
Sadness as Terribly Good
Most of the participants believed that experiencing,
expressing, and exploring sadness was helpful in
therapy, yet many of these same clients were fearful
of the emotion. They feared the vulnerability to
others’ judgment, the possibility of being over-
whelmed, the emotional pain and physical discom-
fort, and so forth, all of which led them to avoid their
sadness. Understanding this dichotomy may be
important for clinicians in two main respects.
First, by recognizing that many clients are inter-
ested in exploring their sadness in session, therapists,
especially novice therapists who may feel uncomfor-
table guiding clients to painful experiences, can feel
confident facilitating an exploration of sadness.
Clients reported that helpful facilitation included
the therapist directly acknowledging sadness when it
arose; encouraging and even giving explicit permis-
sion, if necessary, for clients to express their sadness;
and validating or normalizing the sadness (see
Category 3 of Cluster 2). Additionally, for novice
therapists uncomfortable with sadness, an awareness
of the existential questions underlying sadness can
provide a framework within which to explore the
meanings of sadness (see Cluster 1). With these
questions in mind, sadness may become a tool useful
for shedding light on clients’ hidden assumptions,
purposes, and meanings and for helping to identify
needs.
Second, it also is important to consider how
clients manage the internal struggle that sadness
may present. While experiencing and expressing
sadness, clients may move in and out of the intense
emotion to better manage it. When therapists
notice their clients avoiding sadness, these findings
suggest that the exploration of sadness may be
facilitated if therapists allow their clients to step
back from the sadness for brief periods of time. By
momentarily moving away from the sadness when
its duration or intensity becomes too great, some
clients may feel relief and a sense of reconnection
with their therapist (see Category 2 of Cluster 2).
Humor especially, as well as the therapists’ appro-
priate reaction to it (e.g., smiling and chuckling),
may be a powerful means for sad clients to
reconnect with their therapists. However, therapists
will want to help clients return to the exploration of
sadness, because the clients in this study felt that
exploration was useful when it occurred at a
tolerable pace (see Category 3 of Cluster 2).
Many therapeutic orientations propose that the
expression or processing of negative emotions such
as sadness is essential to the work of therapy. For
instance, Greenberg et al. hypothesized that depres-
sion results, in part, from incomplete processing of
emotional experience (Greenberg, Elliott, & Foer-
ster, 1990; Greenberg & Paivio, 1997), and there is
a large body of research on the negative psycholo-
gical and health consequences of avoiding and
suppressing emotions (e.g., Butler et al., 2003;
Gross & Levenson, 1997; John & Gross, 2004;
Richards & Gross, 1999). This model of sadness
does not conflict with this information, but adds to
it by specifying that the act of distancing oneself
from sadness actually may be productive if it is
temporary and acts to solidify the alliance (see
Categories 2 and 3 of Cluster 2). Furthermore,
these findings propose that sadness experiences
might be studied better in a differentiated manner,
tracking sadness that is experienced as useful in
session as opposed to sadness that is overwhelming
and nonproductive.
Sadness and Existential Exploration
Emotions are theorized to be a tool for directing
one’s attention to unmet needs in several therapies
(e.g., Elliott, Watson, Goldman, & Greenberg,
2004; Silberschatz & Sampson, 1991). The model
of sadness proposed in this study, however, adds to
this literature by specifying that these needs are, at
their core, of an existential nature and related to
self-acceptance. This interpretation is grounded in
the findings that the participating clients’ sadness
in therapy was shown repeatedly to be rooted in
self-criticism, self-questioning, and identity ex-
ploration.
Existential psychotherapists view a client’s dis-
tress, such as sadness, as originating from conflicts
brought about by how it is for the client to exist in
the world (Spinelli, 2002). This way of being is
based on the client’s implicit assumptions, beliefs,
feelings, attitudes, and values toward self, others,
and the world in general (Laing, 1960; Laing &
Esterson, 1964; Spinelli, 1997, 2002; Yalom, 1989).
252 Henretty, Levitt, and Mathews
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

In existential psychotherapy, sadness is not patholo-
gized, nor is the amelioration of sadness the primary
task for an existential therapist. Rather, therapist and
client attempt to expose and consider the emotion as
an expression or implication of the client’s wider way
of functioning so that this way of being may be
assessed and given the opportunity to evolve (Saha-
kian, 1976).
Being genuinely sad means that one responsibly
confronts the significations of one’s [sadness]; one
lets go of and ultimately says goodbye to the self
that one has heretofore been; one risks letting go
of the no-longer-possible familiar world with its
familiar horizons. This grieving of one’s loss is a
transformation of one’s world/self/others/[identity-
sustaining] projects; it renews one and enables one
to discover and set up new [meanings]. (Linn,
1985)
In the current study, sadness appeared to be
connected to needs often associated with combating
self-criticism and related both directly and indirectly
to self-acceptance (see Category 1 of Cluster 1). The
need to feel valuable to others, the need to forgive
oneself, and the need to express oneself to others are
a few examples of the needs that arose. Using this
understanding of sadness may assist therapists in
initiating profound existential dialogues and in
guiding clients to identify needs, which could help
them begin to take new actions toward change.
According to Yalom, ‘‘It is only when therapy
enlists deep emotions that it becomes a powerful
force for change’’ (1989, p. 35). Therapeutic dis-
cussions about sadness also can help clinicians shift
the topic of therapy to a big-picture perspective;
from the concrete question, ‘‘What has made me
sad?’’ to the complex questions, ‘‘How has who I am
led me to be sad?’’ and ‘‘How has who I wish to be
led me to be sad?’’
This study may encourage psychotherapy re-
searchers to seek differentiation in the content of
sadness experiences, such that they can track ex-
istential concerns underlying sadness. Specifically,
researchers may wish to distinguish times during
which sadness is motivated by self-critical evaluation
(sadness about me) as opposed to sadness that is
motivated by loss (sadness for me) to examine
whether differences exist between the processes
associated with each type of sadness.
Sadness in Sickness or in Health
As successive editions of the DSM have been
published, the different disorders that sadness
characterizes ‘‘have become more differentiated
and have broadened horizontally into qualitatively
new forms of disorders and vertically into milder
variants of recognized conditions’’ (Haslam, 2005,
p. 36). Thus, it has been argued that the DSM-IV-
TR may wrongly pathologize many normal psycho-
logical variations of emotion (Kutchins & Kirk,
1997), such as sadness, and inflate the estimated
prevalence of disorders, such as depression, in the
community (Horwitz, 2002). According to Wake-
field, Schmitz, First, and Horwitz, (2007), up to
25% of people who have been diagnosed with major
depressive disorder, using the DSM diagnostic
criteria, in fact may be reacting with normal sadness
to stressful life events. However, under the DSM
paradigm, which remains the overarching paradigm
of psychodiagnostics, sadness is viewed as a symp-
tom of pathology. The results of this study suggest
that clients not only are aware of, but share,
this understanding of sadness (see Category 1 of
Cluster 2).
Possibly the most important implication of this
research is that clients avoided sadness out of fear
that their sadness is, or may become, pathological. In
this study, this fear was so powerful that it at times
overshadowed the clients’ belief that exploring sad-
ness in therapy is important and useful (see Cluster
2). It seems that we cannot overlook the possibility
that the field of psychology has played a role in the
pathologizing of sadness in clinical practice and
everyday life. The plethora of research on depression
and the paucity of research on sadness may be
further evidence of our bias toward conceptualizing
sadness in pathological terms.
The results of this study indicated that the clients
were experiencing conflict in session about whether
it was safe to explore their sadness, and that this
conflict arose in part because they were afraid that
others might judge them as pathological. Despite
this fear, the clients repeatedly commented that
exploring their sadness had been helpful and healthy
in therapy. Consequently, therapists and psychother-
apy researchers may wish to consider how the
pathologizing of sadness by our culture and our
profession may be negatively affecting our clients. A
fair interpretation may be that, by challenging our
culture’s assumptions about sadness, our field might
be able to take steps toward normalizing sadness,
which in turn could facilitate the process of explor-
ing sadness for clients and perhaps people in general.
Therefore, it may be of benefit for researchers to
study the beliefs that clients hold about emotional
experience before entering psychotherapy and to
examine how these beliefs and attitudes might
influence psychotherapy outcome.
Moments of sadness 253
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

Strengths and Limitations of Findings
In this study, the credibility of the findings was
enhanced by a number of credibility checks. Every
interview ended with questions designed to verify the
comprehensiveness of the data collection and the
researchers worked together to achieve consensus in
their interpretation of the findings. Finally, satura-
tion of the conceptual categories was achieved,
which suggests that the analysis was comprehensive
and that continued data collection was likely to be
redundant.
The participating clients of this study demon-
strated diversity on a variety of characteristics
relevant to sadness in psychotherapy. In addition to
diversity on characteristics like gender and age,
significant to the purpose of the study are the facts
that the clients represented a wide range of causes of
sadness and that their therapists represented a wide
range of theoretical perspectives on psychotherapy.
There was a lack of diversity, however, in that all
clients were seen in individual, outpatient psy-
chotherapy. Therefore, caution should be applied
in using this model to understand how sadness
functions within group or couples therapy contexts
and with clients treated as inpatients. Furthermore,
because most of the participating clients were college
students, the results may not be characteristic of the
general population.
This study focused only on the experience of
sadness as discussed and experienced in therapy;
therefore, the resulting conceptual model may not be
as relevant for extra-therapy experiences of sadness.
Although the results revealed that sadness experi-
enced in session was of an existential nature, it may
be that for sad topics to be important enough to be
discussed in therapy they had to have shaken clients’
conceptualizations of themselves or of their world,
but that outside of therapy sadness does not always
fit into this existential paradigm. For a more
complete understanding, future research could ex-
amine sadness experienced within different contexts.
Additionally, this study did not examine how sadness
moments are evidenced within therapy sessions;
future research might explore how the internal
experiences described herein correspond with the
external representation of sadness.
Implications
Future inquiries could continue to build on the small
body of literature on sadness in psychotherapy by
examining the experiences of sadness in a narrower
scope to see whether differences exist in the experi-
ence for clients. Possible topics include sadness as
related to loneliness, altruistic sadness after a natural
disaster, or sadness in the context of a diagnosis such
as major depressive disorder or posttraumatic stress
disorder. Evidence shows that cultural variation
exists in the way people cope with sadness (Vander-
voort, 2001); future studies could examine and
compare clients’ experiences of sadness in other
cultures with those found herein, particularly in
relation to the pathologizing of sadness. Indeed, if
our culture was unafraid of experiencing, exploring,
and subsequently understanding sadness, we might
be better able to garner lessons from our sadness
about ourselves and our needs for the future.
Acknowledgements
We thank Lorna Horishny, Dr. Jane Clement, and
Dr. Carl Gilleylen at the Career and Psychological
Counseling Center and Dr. James Whelan at the
Psychological Services Center, University of Mem-
phis, for facilitating this research. We also thank Dr.
Robert Neimeyer for his helpful suggestions.
References
American Psychiatric Association. (2000). Diagnostic and statistical
manual of mental disorders (4th ed., text rev.). Washington, DC:
Author.
Butler, E. A., Egloff, B., Wlhelm, F. H., Smith, N. C., Erickson,
E. A., & Gross, J. J. (2003). The social consequences of
expressive suppression. Emotion, 3(1), 48�67.
Elliott, R., Watson, J. C., Goldman, R. N., & Greenberg, L. S.
(2004). Learning emotion-focused therapy: The process-experiential
approach to change. Washington, DC: American Psychological
Association.
Giorgi, A. (1970). Psychology as a human science: A phenomen-
ological based approach. New York: Harper & Row.
Glaser, B. J., & Strauss, A. (1967). The discovery of grounded theory:
Strategies for qualitative research. Chicago: Aldine.
Greenberg, L. S. (1993). Emotion and change processes in
psychotherapy. In M. Lewis & J. M. Haviland (Eds), Handbook
of emotions (pp. 499�508). New York: Guilford Press.
Greenberg, L. S., Elliott, R., & Foerster, F. (1990). Experiential
process in the psychotherapeutic treatment of depression. In D.
McCann & N. Endler (Eds), Depression: New directions in theory,
research, and practice (pp. 157�185). Toronto, Ontario, Canada:
Wall & Emerson.
Greenberg, L. S., & Paivio, S. C. (1997). Working with emotions in
psychotherapy. New York: Guilford Press.
Gross, J. J., & Levenson, R. W. (1997). Hiding feelings: The acute
effects of inhibiting negative and positive emotion. Journal of
Abnormal Psychology, 106, 95�103.
Haslam, N. (2005). Dimensions of folk psychiatry. Review of
General Psychology, 9(1), 35�47.
Hoehn-Saric, R. (1977). Emotions and psychotherapies. American
Journal of Psychotherapy, 31(1), 83�96.
Horstmann, G. (2003). What do facial expressions convey:
Feeling states, behavioral intentions, or action requests? Emo-
tion, 3, 150�166.
Horwitz, A. V. (2002). Creating mental illness. Chicago: University
of Chicago Press.
Huebner, R. R., & Izard, C. E. (1988). Mothers’ responses to
infants’ facial expressions of sadness, anger, and physical
distress. Motivation and Emotion, 12, 185�196.
254 Henretty, Levitt, and Mathews
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4

John, O. P., & Gross, J. J. (2004). Healthy and unhealthy emotion
regulation: Personality processes, individual differences, and
life span development. Journal of Personality, 72(6), 1301�1334.
Kagan, N. (1975). Interpersonal process recall: A method of influen-
cing human interaction. Houston, TX: University of Houston.
Kagan, N., Krathwohl, D. R., & Miller, R. (1963). Stimulated
recall in therapy using video tape: A case study. Journal of
Counseling Psychology, 10(3), 237�243.
Kagan, N., & Schauble, P. G. (1969). Affect simulation in
interpersonal process recall. Journal of Counseling Psychology,
16(4), 309�313.
Kutchins, H., & Kirk, S. A. (1997). Making us crazy: DSM: The
psychiatric bible and the creation of mental disorders. New York:
Free Press.
Laing, R. D. (1960). The divided self. London: Tavistock.
Laing, R. D., & Esterson, A. (1964). Sanity, madness, and the
family. Harmondsworth, England: Penguin.
Linn, S. E. (1985). Being depressed: An existential-phenomenological
investigation. (Doctoral dissertation, Duquesne University).
Dissertation Abstracts International, 46(6-B), 2070.
Malkinson, R. (2001). Cognitive-behavioral therapy of grief: A
review and application. Research on Social Work Practice, 11(6),
671�698.
Nelson, L. H. (1990). Who knows: From Quine to a feminist
empiricism. Philadelphia: Temple University Press.
Nesse, R. M. (1999). The evolution of hope and despair. Social
Research, 66(2), 429�469.
NUD*IST 4 [Computer software]. (1997). Doncaster, Victoria,
Australia: QSR International Pty Ltd.
Plutchik, R. (2000). Therapist tactics for uncovering emotions. In
R. Plutchik (Ed.), Emotions in the practice of psychotherapy:
Clinical implications of affect theories (pp. 127�138). Washington,
DC: American Psychological Association.
Rennie, D. L. (2000). Grounded theory methodology as metho-
dical hermeneutics: Reconciling realism and relativism. Theory
& Psychology, 10(4), 481�501.
Rennie, D. L., Phillips, J. R., & Quartaro, G. K. (1986).
Grounded theory: A promising approach to conceptualization
in psychology. Canadian Psychology, 29(2), 139�150.
Richards, J. M., & Gross, J. J. (1999). Composure at any cost? The
cognitive consequences of emotion suppression. Personality and
Social Psychology Bulletin, 25, 1033�1044.
Sahakian, W. S. (1976). Philosophical psychotherapy: An existen-
tial approach. Journal of Individual Psychology, 32(1), 62�69.
Silberschatz, G., & Sampson, H. (1991). Affects in psychopathol-
ogy and psychotherapy. In J. D. Safran & L. S. Greenberg
(Eds), Emotion, psychotherapy, and change (pp. 113�129). New
York: Guilford Press.
Spinelli, E. (1997). Tales of un-knowing: Eight stories of existential
therapy. New York: New York University Press.
Spinelli, E. (2002). The therapeutic relationship as viewed by
existential psychotherapy: Re-embracing the world. Journal of
Contemporary Psychotherapy, 32(1), 111�118.
Vandervoort, D. J. (2001). Cross-cultural differences in coping
with sadness. Current Psychology, 20(2), 147�154.
Wakefield, J. C., Schmitz, M. F., First, M. B., & Horwitz, A. V.
(2007). Extending the bereavement exclusion for major depres-
sion to other losses: Evidence from the National Comorbidity
Survey. Archives of General Psychiatry, 64(4), 433�440.
Yalom, I. (1989). Love’s executioner and other tales of psychotherapy.
New York: Basic Books.
APPENDIX
SADNESS INTERVIEW QUESTIONS
‘‘What is your experience of moments of
sadness in psychotherapy?’’
1. What about this moment triggered a feeling of sadness for you?
2. What was happening for you at this time in session? What were
you thinking?
3. What was that feeling like for you (emotionally/physically)?
. What did it feel like inside you to have that feeling?
. What words best describe it?
. Were there any other feelings that were going along with
the feeling of sadness, that came just before or were
underneath the feeling of sadness?
4. Did what the therapist was doing impact or change your
feelings?
. If so, how?
. Was there anything that you thought your therapist did
that was helpful or unhelpful?
. If unhelpful, is there anything that could have been done
differently?
5. Did that feeling of sadness change or in any way lessen or
increase?
. If so, when?
. If the feeling ended, what happened that made it end or
change?
. Would you have wanted to stay in that feeling longer?
Would it have been helpful?
. What came in place of that feeling, if anything?
6. Is there anything else that is happening at that moment that
seems important or relevant to the feeling of sadness and your
process of therapy?
7. Does it feel like what is important about that moment has been
fully described?
End-of-Interview Questions
1. Do you feel that there is anything else I should know to better
understand your experience of sadness?
2. Were there any questions that weren’t asked in this interview
that seem important to you?
3. Do you have any feedback for me on how I could make this
interview an easier or better experience?
4. After having been through this interview, do you have any
theories about how sadness changes in therapy?
5. Is there anything that you think would be helpful for you to
continue to talk to your therapist about in your next session?
Moments of sadness 255
Dow
nloa
ded
by [
Um
eå U
nive
rsity
Lib
rary
] at
18:
03 1
6 A
ugus
t 201
4