Embed Size (px)
Citation preview

Vol. 36, No. 4-Fall Issue 237
CLASSROOM TEACHERS’ PERCEIVED ROLE IN DENTAL HEALTH EDUCATION
E. Marcia Boyer, BS, MS, M Phil.”
Introduction
Several papers have been written discussing who could best teach dental health edu- cation in the public school setting. 3 Some favor the dentist and the dental hygienist because they are the most knowledgeable and would be regarded as authori- ties. X J ~ , ’ W Others favor the classroom teacher because she has continual contact with the children and is trained in pedagogy.
Currently, the emphasis is on the classroom teacher as the individual of choice to instruct children about dental health in the school. In addition to the reasons given, the lack of dental personnel employed in school settings and the suggested dental manpower shortage support the choice of the classroom teacher.
A few studies have indicated that the classroom teacher may not have sufficient dental knowledge to teach dental health. Zody2 found that classroom teachers’ scores on a dental health knowledge test corresponded to their students’ scores. Mullins and SprouseIs con- ducted a study to determine teachers’knowledge . . . “of the conventional dental wisdom and of the newer dental plaque control concepts.” They concluded that school teachers are not knowledgeable about dental health or prevention.
Since school dental health education is often the responsibility of the elementary Loupe’O studied teachers’ agreement with the implied and explicit roles s delegated to teachers in the oral health education curriculum guides
from the Minnesota Department of Health. They concluded that teachers were in agree- ment with roles related to instructional content, but disagreed with responsibility for administering and coordinating children’s dental health care.
The purpose of this investigation was to utilize measures similar to those used by King and Loupe’O to determine teachers’ attitudes toward their role in dental health instruc- tion. More specifically, the objectives of this study were to determine 1) teachers’ self-per- ceived adequacy to teach selected dental health topics, 2) teachers’ attitudes toward teachers’ responsibility for dental health, and 3) if teachers’ perceived adequacy and atti- tudes varied with the number of exposures to senior dental hygiene students teaching dental health in their classrooms.
lR,li,gO
Methods
Lt‘ritten questionnaires were mailed in May 1975 to 173 public school teachers whose pupils had “received” dental health programs given by senior dental hygiene students from the Dental Hygiene Department of the University of Iowa in the 1974-75 school year. The teachers had no active roles in dental health lessons and oral hygiene skills practice. The dental health programs, which were conducted over a four to six week period, were designed by dental hygiene students and varied from classroom to classroom. Some 128 teachers in the Iowa City schools and one rural school had “participated” in the programs in previous years (subsequently referred to as “More-than-one-year participation”). The remaining 45 teachers were from five rural schools and had not participated before 1974 (“One-year participation”). All except seven of the teachers taught at the elementary level. In addition, the attitudinal portion of the questionnaire was sent to 21 teachers who had never participated in the programs (“No previous participation”) and did not know they would be participating. The school nurse who distributed the questionnaires to these 21 teachers stated that a dental health program was being considered for the coming year.
“College of Dentistry, Department of Dental Hygiene, University of Iowa, Iowa City, Iowa 52242
238 Journal of Public Health Dentistry
Questionnaires were received from 164 teachers or a response of 84 percent. Ques- tionnaires were received from 121 of the 128 teachers who had more than one year of par- ticipation (79 percent response rate); 42 questionnaires were received from the 45 teachers who had one year of participation (93 percent response rate); and 21 questionnaires were received from the 21 teachers who had no previous participation (100 percent response rate).
The questionnaires were three pages in length and the second page contained ques- tions on perceived adequacy and attitudes toward teaching dental health. The first and third pages were designed to evaluate the specific dental health programs presented by senior dental hygiene students.2
Results
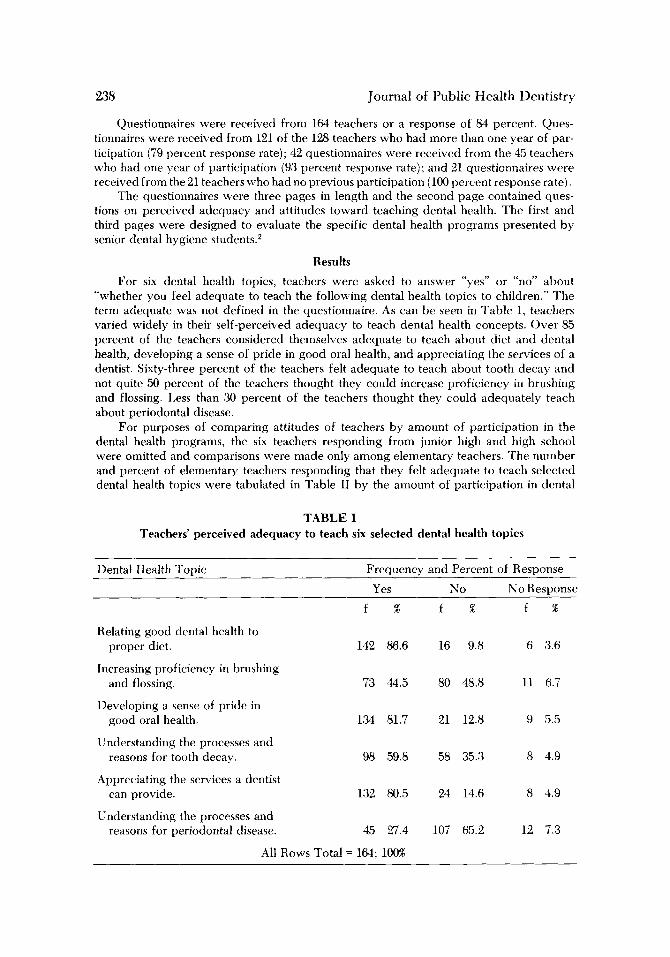
For six dental health topics, teachers were asked to answer “yes” or “no” about “whether you feel adequate to teach the following dental health topics to children.” The term adequate was not defined in the questionnaire. As can be seen in Table 1, teachers varied widely in their self-perceived adequacy to teach dental health concepts. Over 85 percent of the teachers considered themselves adequate to teach about diet and dental health, developing a sense of pride in good oral health, and appreciating the services of a dentist. Sixty-three percent of the teachers felt adequate to teach about tooth decay and not quite 50 percent of the teachers thought they could increase proficiency in brushing and flossing. Less than 30 percent of the teachers thought they could adequately teach about periodontal disease.
For purposes of comparing attitudes of teachers by amount of participation in the dental health programs, the six teachers responding from junior high and high school were omitted and comparisons were made only among elementary teachers. The number and percent of elementary teachers responding that they felt adequate to teach selected dental health topics were tabulated in Table I1 by the amount of participation in dental
TABLE I Teachers’ perceived adequacy to teach six selected dental health topics
Dental Health Tovic Freauencv and Percent of Resvonse
Yes N O No Response
Relating good dental health to proper diet.
f % f % f %
142 86.6 16 9.8 6 3.6
Increasing proficiency in brushing and flossing. 73 44.5 80 48.8 11 6.7
Developing a sense of pride in good oral health. 134 81.7 21 12.8 9 5.5
Understanding the processes and reasons for tooth decay. 98 59.8 58 35.3 8 4.9
Appreciating the services a dentist can provide. 132 80.5 24 14.6 8 4.9
Understanding the processes and reasons for periodontal disease. 45 27.4 107 65.2 12 7.3
All Rows Total = 164; 100%

Vol. 36, No. 4-Fall Issue 239
health programs. A chi-square test was performed for each dental health topic to deter- mine if statistically significant differences existed by amount of participation. If a signifi- cant difference was found, the source of significant difference was isolated by the chi- square method described by Fleiss?
There were significant differences by amount of participation for teachers’ perceived abilities to relate good dental health to proper diet, understand the processes and reasons for tooth decay, and understand the processes and reasons for periodontal disease. More teachers who had participated in the dental health programs for one year or more felt adequate to teach about dental decay (p = .026) and about diet and dental health ( p = ,016) than teachers who had not participated previously. A different pattern developed for teaching about periodontal disease. More teachers who had participated for more than one year felt adequate than teachers who either had participated for only one year or had not participated previously ( p = ,023). It should be noted again that few teachers in all cate- gories felt adequate to teach about periodontal disease. No significant differences were found b y amount of participation for the items: increasing proficiency in brushing and flossing, developing a sense of pride in good oral health, and appreciating the services a dentist can provide.
A five-point scale was utilized to determine degree of agreement with seven items related to what the classroom teacher’s responsibility for dental health should be. A score of one indicated strongly agree and a score of five indicated strongly disagree. The items and ratings for all teachers are summarized in Table 111. Teachers appear to he in agree- ment that it should be their responsibility to have pride in personal oral hygiene and be a model for children, refer children with dental problems to the nurse, and motivate chil- dren to have good dental health. Teachers strongly disagree that it should be the teacher’s responsibility to follow-up the child’s dental health progress by visits with the parents. Teachers also do not consider it the teacher’s responsibility to distribute and record dental health cards or demonstrate proper toothbrushing technics to the class. Teachers were divided in regard to administering emergency care in case of a dental accident.
To determine if teachers’ degree of agreement varied with participation in the Univer- sity of Iowa school dental health programs, median ratings were determined for each item and a median test p e r f ~ r m e d . ~ Four items had identical medians for the three groups. For the two items, “responsibility for distributing dental health cards” (p = .25) and “motivating children to establish good oral hygiene” (p = .50), the differences could easily have occurred by chance. There was a difference at the .10 significance level for teachers’ agreement with the item on responsibility for parental visits to follow-up children’s dental health progress. The teachers with more than one year’s exposure to the dental health programs and those with no exposure strongly disagreed with the item, while the teachers with one year’s exposure disagreed.
Discussion
These findings that teachers considered themselves adequate to teach about diet, pride in oral health, and appreciation of the services of a dentist, but that they considered themselves less adequate to teach about dental decay are consistent with King and Lonpe’s findings.’O In contrast to the findings here that less than 50 percent of the teachers thought they could increase proficiency in brushing and flossing, 70 percent of the teachers in King and Loripe’s study thought they could. King and Loupe did not include periodontal disease in their questionnaire.
There were some differences of perceived ability to teach dental health topics by amount of participation in the dental health programs. There was a tendency for more teachers who had participated in the programs to indicate adequacy to teach dental health. The one exception was that most teachers, regardless of amount of participation,
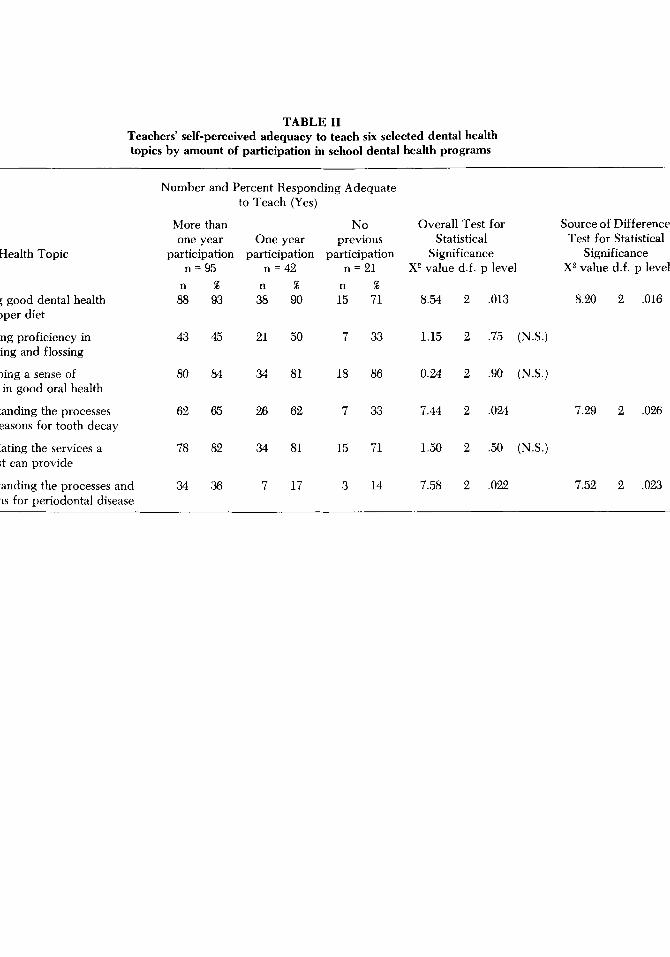
TABLE I1 Teachers' self-perceived adequacy to teach six selected dental health topics by amount of participation in school dental health programs
Dental Health Topic
Relating good dental health to proper diet
Increasing proficiency in brushing and flossing
Developing a sense of pride in good oral health
Understanding the processes and reasons for tooth decay
Appreciating the services a dentist can provide
Understanding the processes and reasons for periodontal disease
Number and Percent Responding Adequate to Teach (Yes)
More than No Overall Test for one year One year previous Statistical
participation participation participation Significance n = 95 n = 42 n = 21 X2 value d.f. p level
n 88
43
80
62
78
34
% n 93 38
45 21
84 34
65 26
82 34
36 7
% n 90 15
50 7
81 18
62 7
81 15
17 3
% 71 8.54
33 1.15
86 0.24
33 7.44
71 1.50
14 7.58
2 .013
2 .75 (N.S.)
2 .90 (N.S.)
2 .024
2 .50 (N.S.)
2 .022
Source of Difference Test for Statistical
Significance X2 value d.f. p level
8.20 2 ,016
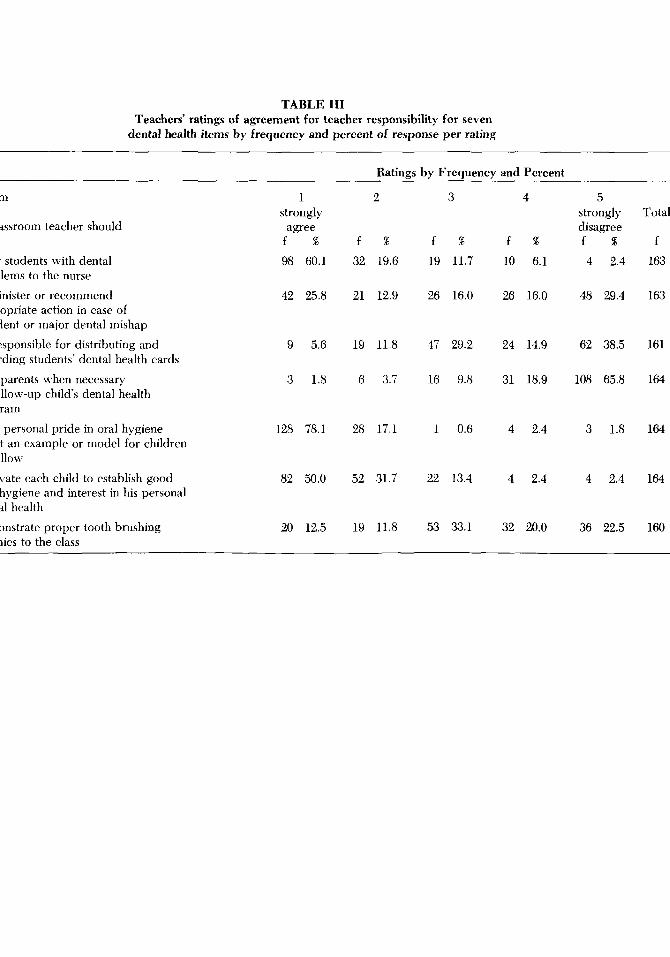
TABLE I11 Teachers’ ratings of agreement for teacher responsibility for seven
dental health items by frequency and percent of response per rating
z ?
I Ratings by Frequency and Percent 4
Item
The classroom teacher should
1.
2.
3.
4.
5.
6.
- i.
refer students with dental problems to the nurse
administer or recommend appropriate action in case of accident or major dental mishap
be responsible for distributing and recording students’ dental health cards
visit parents when necessary to follow-up child’s dental health program
have personal pride in oral hygiene to set an example or model for children to follow
motivate each child to establish good oral hygiene and interest in his personal dental health
demonstrate proper tooth brushing technics to the class
1 strongly
agree f %
98 60.1
42 25.8
9 5.6
3 1.8
128 78.1
82 50.0
20 12.5
2
f %
32 19.6
21 12.9
19 11.8
6 3.7
28 17.1
52 31.7
19 11.8
3
f % 19 11.7
26 16.0
47 29.2
16 9.8
1 0.6
22 13.4
53 33.1
4
f %
10 6.1
26 16.0
24 14.9
31 18.9
4 2.4
4 2.4
32 20.0
5 strongly disagree f % 4 2.4
48 29.4
62 38.5
108 65.8
3 1.8
4 2.4
36 22.5
9 Total
f 163
U v)
2 CD
163
161
164
164
164
160

242 Journal of Public Health Dentistry
felt adequate to teach about developing a sense of pride in good oral health. Statistically significant differences by amount of participation for the topics of proper diet and the process of caries seem to indicate that participation in the programs makes teachers feel more adequate to teach these topics. On the other hand, the difference in perceived ability to teach about periodontal disease comes after more than one year of participation. This finding would indicate that other variables are influencing teachers’ perceived adequacy to teach dental health.
It is quite possible that since the Iowa City schools have participated longer, more information has been presented on periodontal disease whereas, in rural schools with programs just beginning, greater concentration may have been placed on the decay process, proper diet, and personal oral hygiene skills. Differences may also be related to experiences in private dental offices or dental health practices in the home.” Teachers’ interest and participation in the dental health programs could also result in differing re- sponses. A lack of formal teacher preparation to teach dental health was probably similar for all teachers. This study did not control other factors but a follow-up study is p!anned to see if changes do occur for the three groups with participation in the program this year.
For the most part, teachers were consistent in what they considered should be their responsibility in regard to dental health: passive activities which involved being a good model or referring students to the school nurse. Dental health activities which re- quired that the teacher be actively responsible, such as distributing and recording dental health cards, were usually not considered responsibilities of the teachers. One difference found in this study and the one by King and Loupe was the teachers in this study did not consider it their responsibility to demonstrate proper toothbrushing technics to the class whereas the teachers studied by King and Loupe did (median 1.84).l0
There were essentially no differences in attitudes of the teachers about their respon- sibilities in the areas of dental health by amount of participation in the program. In addi- tion, the consistency of these attitudinal responses with those of King and Loupe suggests that teachers view similarly their responsibilities for children’s dental health activities.
Although King and Loupe’s study indicated that teachers did think it their responsi- bility to demonstrate proper toothbrushing, two of their findings reinforce that teachers do not desire the responsibility for school dental health education. Their study showed that (1) the majority of teachers preferred one unit on dental health instruction, such as during National Children’s Dental Health Week, and (2) only nine percent thought dental health should be taught weekly.1° The finding in the present study that teachers do not think they should have active responsibility for dental health activities suggests that school dental health educational approaches which place primary responsibility upon the class- room teacher may not succeed. Teachers’ attitudes should be considered when planning school dental health education.
Summary
This investigation utilized mail questionnaires to determine public school teachers’ perceived adequacy to teach six dental health topics and responsibility for dental health in the classroom. The majority of public school teachers surveyed in Iowa City and sur- rounding communities felt adequate to teach dental health topics with two major excep- tions: increasing proficiency in brushing and flossing, and understanding the processes and reasons for periodontal disease. More importantly, this study indicates that iany teachers do not consider dental health activities to be responsibilities of the public s,nool teacher.
BIBLIOGRAPHY 1. Albertini, T., Boffa, J., and Kaplis, N. A. A dental health education program in the open classroom:
report of a pilot study. J. Sch. Health, 43:566-71, 1973.
Vol. 36, No. 4-Fall Issue 243
2. Boyer, E. Marcia. Teacher satisfaction with University of Iowa dental education programs. Iowa
3. Carlyon, W. H. Creative, innovative, vital and dynamic health education programs that fail.
4. Clark, C. A,, Fintz, J. B., and Elwell, K. R. Eliminating dental plaque in the sixth grade. J. Pub.
5. Clewett, J. A. A consideration of dental health education. Health Educ. J., 34:115-8, 1975. 3. Cohen, Lois K., and Lucye, H. A position on school dental health education. J. Sch. Health,
7. Fleiss, J. L. Statistical methods for rates and proportions. New York, Wiley, 1973 (p. 92-7). 8. Johns, C. K., and Muhler, J. C. Can dental health education reduce permanent tooth loss? Am.
9. Harshbarger, T. R. Introductory statistics; a decision map. New York, Macmillan, 1971 (pp. 327-
10. King, M. J., and Loupe, M. J. Teachers’ perceptions of responsibility in oral health education.
11. Kriesberg, Louis, and Treiman, Beatrice. Socioeconomic status and the utilization of dentists’
12. Maddick, I. H. Assessment of a dental health program. J. Sch. Health, 40:273-4, 1970. 13. Martens, L. V., et al. Developing brushing performance in second graders through behavior
modification. Health Serv. Rep. 88:818-23, 1973. 14. Masters, P. H. Classroom teacher, effective classroom education. Am. Soc. Prev. Dent. J.,
2:38-41, 1972. 15. Mullins, Raynor, and Sprouse, W. Dental health knowledge of elementary school teachers in
Bowling Green. Kentucky, 1972. Am. SOC. Prev. Dent. J., 360-5. 1973. 16. Myers, Sharon E., and Downs, R. A. Comparative findings in school systems with differing ap-
proaches to dental health education. J. Sch. Health, 38:604-10, 1968. 17. Rayner, J . F., and Cohen, Lois K. School dental health education, pp. 275-307. (In Richards, N. D.
andCohen, L. K., eds. Social sciences and dentistry; a critical bibliography. London, Federation Dentaire Internationale, 1971.)
18. Stein, G., Cribbs, R., and Lannon, G. Experiences in establishing a “Toothkeeper” preventive dentistry program for elementary school students. Am. Soc. Prev. Dent. J., 4:46-8, 1974.
19. Williford, J. W., et al. Report of a study demonstrating improved oral health through education. J. Dent. Child, 34:183-9, 1967.
20. Young, Marjorie A. C. Dental health education: an overview of selected concepts and princi- ples relevant to programme planning. Internat. J. Health Educ., 13:2-26, 1970.
21. Zody, S. A study comparing a dental health education program among first, third, and sixth grade children. Indiana Dent. A. J., 4993-8, 1970.
Dent. J., 62:40-41, 1976.
Mich. Dent. A. J., 57:92-7, 1975.
Health Dent., 33:70-4, 1973.
40361-5, 1970.
Dent. A. J., 7135-8, 1965.
9).
Abstr. J. Dent. Res. 53:166, 1974.
services. Am. Col. Dent. J., 27:147-65, 1960.
Monkey Hear; Monkey Do
Frodo no longer is a lively seeker of mere fun in his early environment. He has become the dean of research workers at the Kresge Hearing Research Institute of The Univer- sity of Michigan. On the job, he displays a smile which exposes his long canine teeth whenever he collects his pay on banana-flavored pellets. He is a descendant of genus macaque, ringtail monk‘eys. Trained for a new experiment in hearing, he sits in his office chair and turns on a flashing red signal when he hears a sound through his headset and then collects the pellet. His job permits an Old-world monkey to enjoy the life of Riley and not miss his early home in a rain forest.
-Richard Hiatt in University of Michigan’s Research News (KAE)





























