Embed Size (px)
Citation preview
CHRONIC RENAL FAILURE
Mohammed Almeziny
BsPharm R,Ph. Msc PhD
Consultant clinical Pharmacist
Kidney Functions
Excretion of waste products Homeostasis
– regulation of electrolyte– blood volume.– blood pressure..
Acid-base balanceHormone secretion
– Erythropoietin.– Activation of vitamin D.
Chronic Kidney Disease (CKD)some definitions
CKD results when a disease process damages the structural or functional integrity of the kidney.
This is clinically detected using either physical exam (hypertension), laboratory (hematuria, proteinuria, microalbuminuria) or imaging studies (CT, MRI, or renal ultrasound).
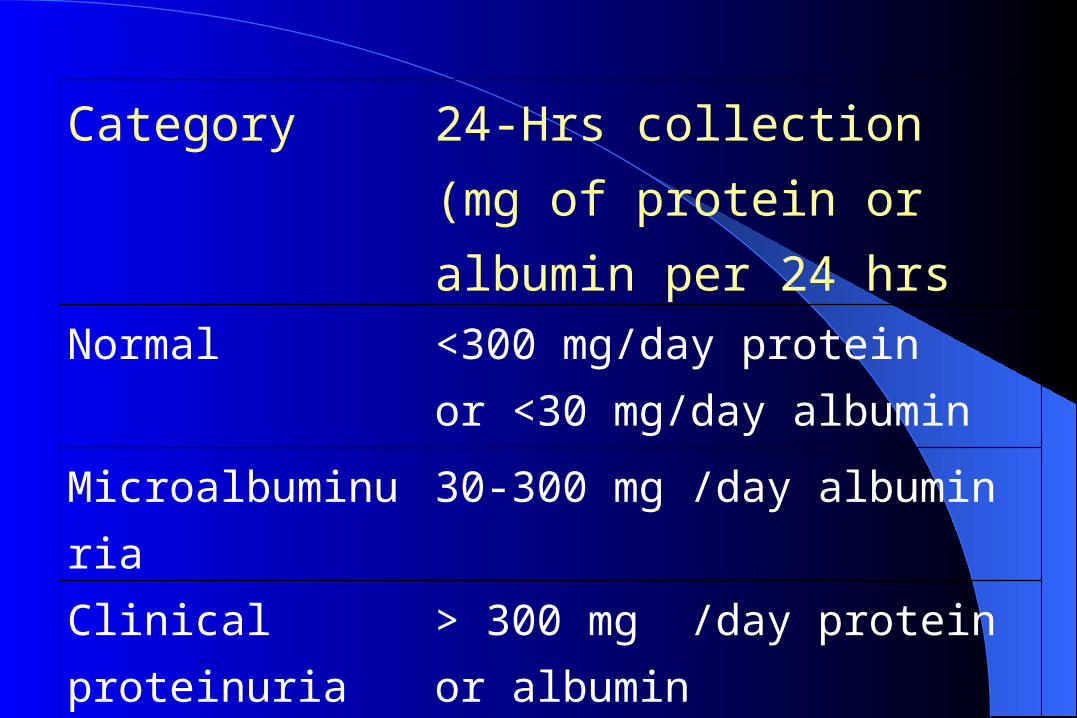
Category 24-Hrs collection (mg of protein or albumin per 24 hrs
Normal <300 mg/day proteinor <30 mg/day albumin
Microalbuminuria 30-300 mg /day albumin
Clinical proteinuria or albuminuria
> 300 mg /day protein or albumin
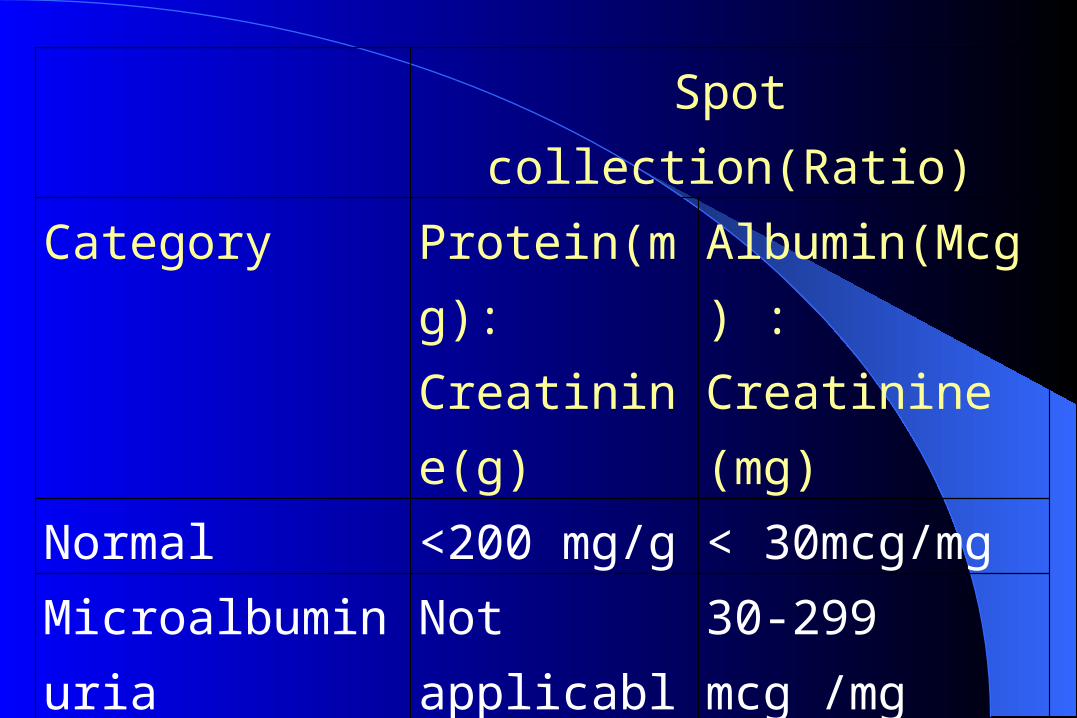
Spot collection(Ratio)Category Protein(mg):
Creatinine(g) Albumin(Mcg) : Creatinine (mg)
Normal <200 mg/g < 30mcg/mgMicroalbuminuria Not
applicable 30-299 mcg /mg
Clinical proteinuria or albuminuria
> 200 mg /g >300mcg/mg
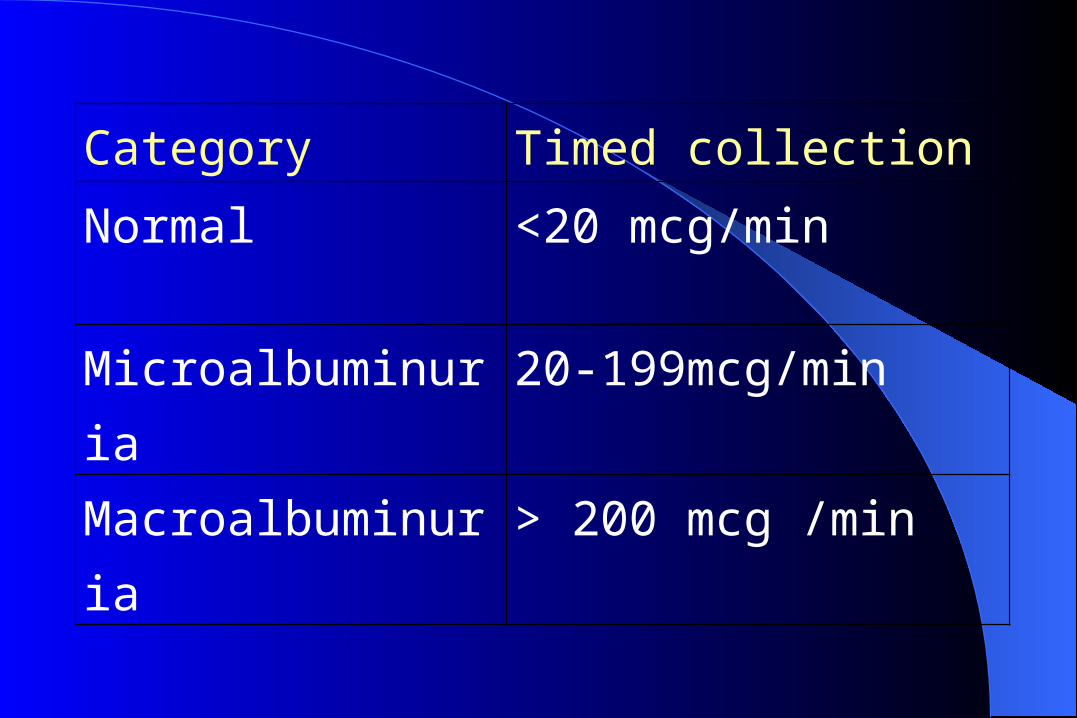
Category Timed collection
Normal <20 mcg/min
Microalbuminuria 20-199mcg/min
Macroalbuminuria > 200 mcg /min
CKD –SOME DEFINITIONS cont’d
Almost all patients with a GFR = 60 ml/min/1.73m2 have CKD.
However, since GFR declines normally with age (approximately 1ml/min/1.73 m2 /year after age 20), a GFR between 60 - 90 ml/min/1.73m2 in the elderly may not be indicative of the presence of CKD.
In order for patients to be classified as having CKD there must be some objective evidence on either physical exam, laboratory or imaging studies of kidney damage.
CKD- EtiologyAny primary or secondary renal parenchymal
disease that has a progressive course e.g glomerulonephritis,
Progressive tubulointerstitial nephritis, etcUnrecognized or untreated obstructive uropathyPolycystic kidney diseaseOften the cause is unknown
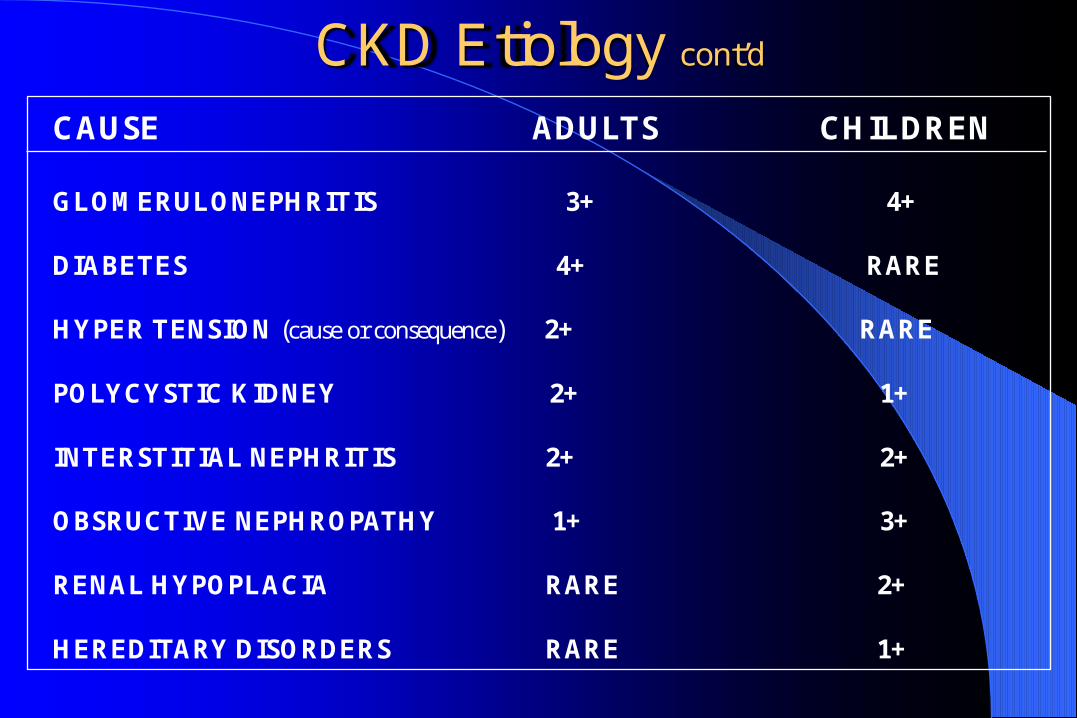
CKD Etiology cont’d
CAUSE ADULTS CHILDREN
GLOMERULONEPHRITIS 3+ 4+
DIABETES 4+ RARE
HYPER TENSION (cause or consequence) 2+ RARE
POLYCYSTIC KIDNEY 2+ 1+
INTERSTITIAL NEPHRITIS 2+ 2+
OBSRUCTIVE NEPHROPATHY 1+ 3+
RENAL HYPOPLACIA RARE 2+
HEREDITARY DISORDERS RARE 1+
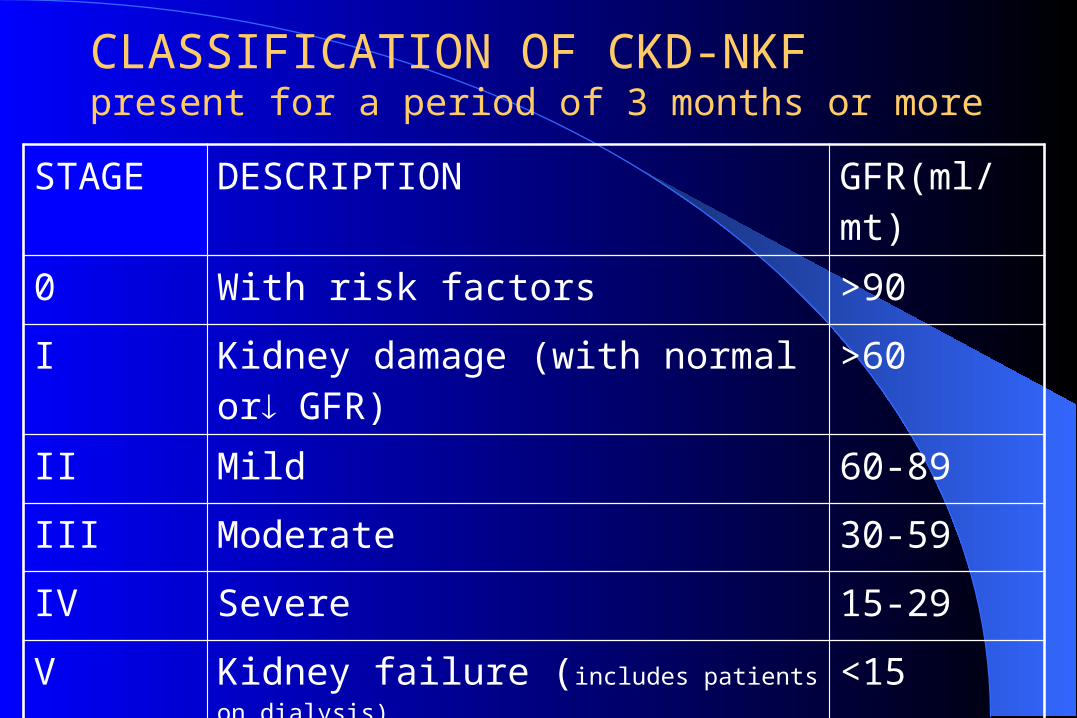
STAGE DESCRIPTION GFR(ml/mt)
0 With risk factors >90
I Kidney damage (with normal or GFR) >60
II Mild 60-89
III Moderate 30-59
IV Severe 15-29
V Kidney failure (includes patients on dialysis) <15
CLASSIFICATION OF CKD-NKFpresent for a period of 3 months or more
CKD - symptomsStage 1 or 2 CKD disease usually do not have any
symptoms or metabolic derangements.Anorexia, nausea, vomiting, weight lossMuscle cramps, especially at nightPruritis Fatigue, weakness, coldness Amenorrhea, decreased libidoThese symptoms are collectively referred to as theuremic syndrome.
CKD – signs
Pallor (from the anemia)Hypertension (usually, but not always !)Hypertensive target organ damage (eg retinopathy,
left ventricular hypertrophy)Peripheral type sensory neuropathy
CKD - Diagnosis
May be suspected on basis of clinical presentationMore often, diagnosed by blood tests
– Elevated serum creatinine– Elevated serum urea
May be discovered incidentally during workup for– anemia, amenorrhea or anorexia
CKD– Diagnosis (cont’d)
Serum creatinine is a marker of glomerular filtration rate– GFR ~ Creatinine Clearance, or– GFR ~ Urine creatinine excretion per 24 h
Plasma Creatinine– If the SrCr is doubled, CrCl is roughly halved
– if the SrCr is tripled, CrCl is reduced to roughly one third; etc.
CKD - Diagnosis (cont’d)
Serum creatinine is also proportional to body muscle mass:
Since creatinine is a muscle byproduct, you must “eyeball” the patient’s muscle mass when
interpreting SrCr
– eg. Young well-muscled man– Elderly wasted woman– Ideal body weight
CKD – Diagnosis (cont’d)
Associated laboratory findings - hematologic: Clinical results:– normocytic normochromic anemia– predisposition to infection– easy bleeding
CKD – Diagnosis (cont’d)
Associated laboratory findings - Ca++ & P:Hypocalcemia
– decreased renal 1-hydroxylation of 25-OH D3 to 1,25(OH)2 D3– Hyperphosphatemia– retention of dietary P, GFR
CKD - Diagnosis (cont’d)
Associated laboratory findings - Ca++ & P: Secondary hyperparathyroidism– PTH secretion stimulated by– Hypocalcemia– Hyperphosphatemia– Decreased 1,25 (OH)2 D3 concentration
CKD- Diagnosis (cont’d)
Associated laboratory findings - Ca++ & P:Results:
– PTH is postulated to be one of the “uremic toxins” – besides bone problems, excess levels of PTH
associated with– Anemia– Pruritis– Myocardial fibrosis
CKD Diagnosis (cont’d) If a patient presents with an elevated SrCr, you must
distinguish if it reflects ARF or CRF
Acute renal failure Potentially reversible
Blood values are changingpt. is unstable
Chronic renal failure- Not reversible- Blood values stable- pt. is stable
Duration of symptoms Absence of acute illness in face of very high urea and
creatinine Small kidneys on imaging Bone disease Neurological Complications Skin / nail / eye changes
FACTORS SUGGESTING CHRONICITY
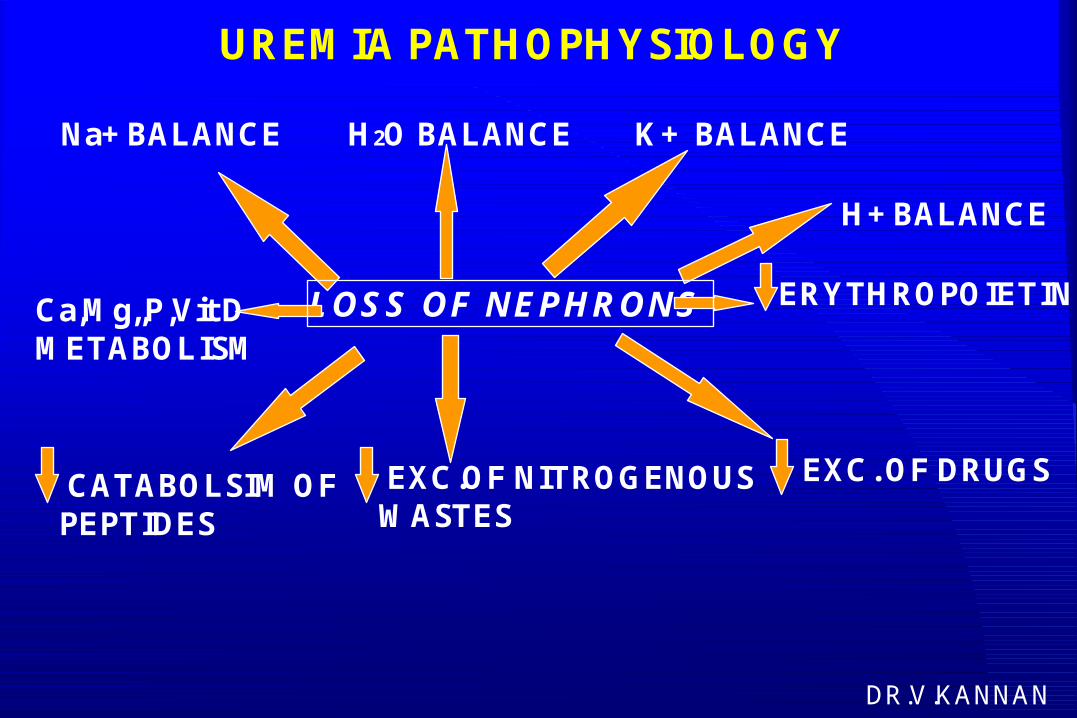
UREMIA PATHOPHYSIOLOGY
LOSS OF NEPHRONS
Na+ BALANCE H2O BALANCE K+ BALANCE
H+ BALANCE
EXC. OF DRUGSEXC.OF NITROGENOUSWASTES
Ca,Mg,,P,Vit DMETABOLISM
CATABOLSIM OFPEPTIDES
ERYTHROPOIETIN
DR.V.KANNAN
· DIAGNOSIS: AETIOLOGY; EST.CHRONICITY· ASSESMENT OF SEVERITY· ASSESMENT OF NUTRITIONAL STATUS· CONSERVATIVE MANAGEMENT· PREDIALYSIS / TRANSPLANTATION EVALUATION· DIALYSIS ACCESS / HBV VACCINATION· DIALYSIS / TRANSPLANTATION
APPROACH TO THE PATIENT WITH CKD
Systemic Lupus Erythematosis (SLE)Obstructive NephropathyIschemic NephropathyPyelonephritisGlomerulonephritisHypertensive Nephrosclerosis
TREATABLE CAUSES OF CKD
AVOID AGGRAVATING RF
CONSERVATIVE Mx OF CKD
SLOW PROGRESSION OF RF TREAT. UREMIC SYMP.
· Avoid volume depletion / excess· Careful drug usage· Avoid electrolyte imbalance· Avoid pregnancies in high risk cases· Avoid urinary instrumentation & contrast studies
MEASURES TO AVOID AGGRAVATING RF
· Cardiac Failure· Drugs: NSAIDS, ACEI, AG, Contrasts, etc· Volume depletion· HTN - uncontrolled / over treatment· Obstruction· Infection- renal / extra renal· Catabolism: Infection, GI bleed, surgery, etc· Electrolyte Disturbances
REVERSIBLE FACTORS AGGRAVATING CKD
Control HTN / cardiac risk factorsDietary protein restrictionScreen & treat UTIControl hyperphosphatemia / hyperuricemiaTreat hyperlipidemiaACE inhibitorsTreatment of primary causeGlycemic control in diabetes
Measures to Slow Progression of Rf
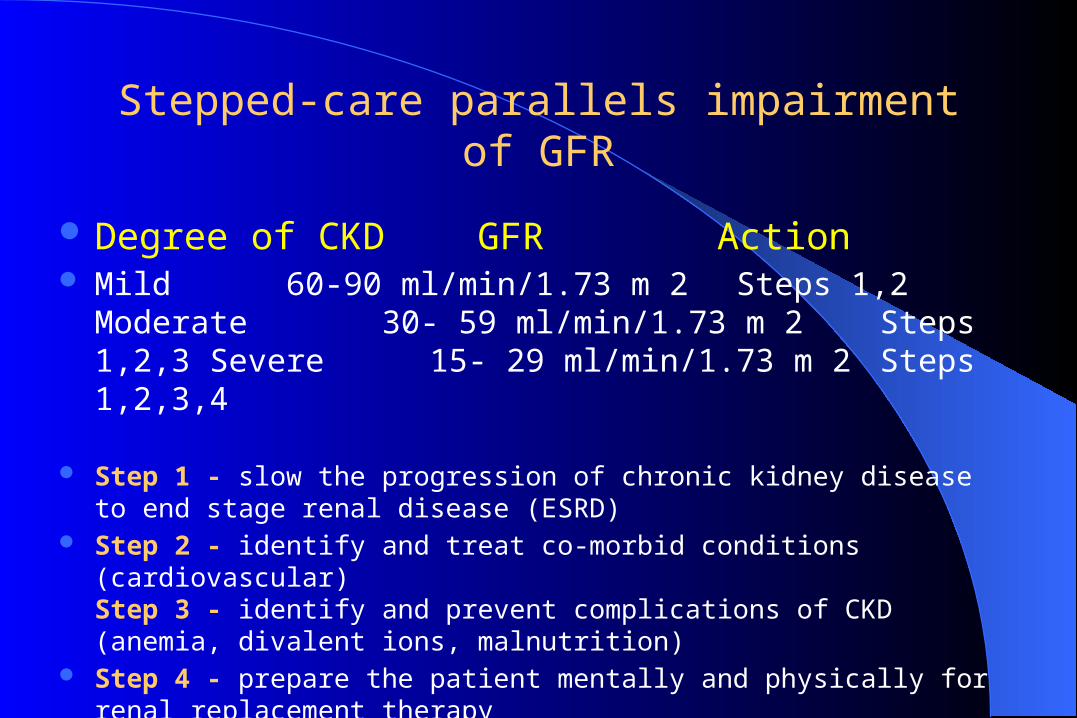
Degree of CKD GFR Action Mild 60-90 ml/min/1.73 m 2 Steps 1,2
Moderate 30- 59 ml/min/1.73 m 2 Steps 1,2,3 Severe 15- 29 ml/min/1.73 m 2 Steps 1,2,3,4
Step 1 - slow the progression of chronic kidney disease to end stage renal disease (ESRD)
Step 2 - identify and treat co-morbid conditions (cardiovascular)Step 3 - identify and prevent complications of CKD (anemia, divalent ions, malnutrition)
Step 4 - prepare the patient mentally and physically for renal replacement therapy
Stepped-care parallels impairment of GFR
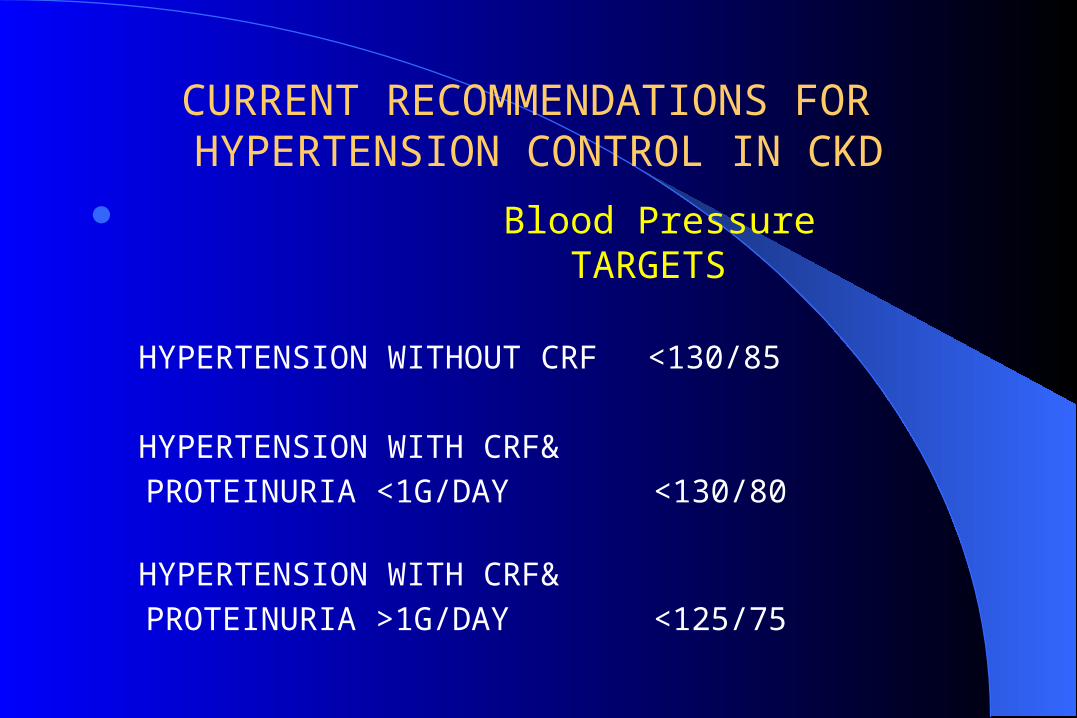
Blood Pressure
TARGETS
HYPERTENSION WITHOUT CRF <130/85
HYPERTENSION WITH CRF&
PROTEINURIA <1G/DAY <130/80
HYPERTENSION WITH CRF&
PROTEINURIA >1G/DAY <125/75
CURRENT RECOMMENDATIONS FOR HYPERTENSION CONTROL IN CKD
ACEI/ARB RECOMMENDATIONS FOR USE IN CKD
ACE INHIBITOR AS FIRST LINE THEPRAPY IN TYPE-1 & TYPE-2 DM PATIENTS WITH
MICRO/ MACROALBUMINURIA EVEN WITHOUT HTN/RF
ALL PATIENTS WITH HTN AND/OR PROTEINURIA
angiotensin receptor blockers (ARBs),
Complications ANEMIA: the kidneys secrete 90% of the
endogenous hormone erythropoietinCARDIOVASCULAR DISEASEDISORDERS OF CALCIUM AND
PHOSPHORUS HOMEOSTASIS: occur in stages 3 to 5 CKD, hyperparathyroidism
MALNUTRITION:It is recommend to evaluate for signs of malnutrition when the GFR < 60 mL/min
TREATMENT OF UREMIC SYMPTOMS
GI SYMPTOMS:• Protein Restriction• Correct Acidosis• Small Frequent meals• Antiemetics • H2 Antagonists• AL.OH Gel
ITCHING:• Protein Restriction• Phosphate Restriction• Antihistaminics• Emollients• UV Radiation• Cholestyramine• Boluso of Xylocaine• Erythropoietin
NEUROMUSCULAR:• Protein Restriction• Vitamins• Exercise• Muscle Relaxants• Tranquilizers• Quinine• Anti-depressants• Correction of Anemia
SKELETAL:• Decrease & Bind Phosp• Treat acidosis• Calcium Supplements• Clacitriol / 1 Alpha• Treat severe hyperuricemia
ANEMIA• Iron, Folate & B12• Erythropoietin• Transfusion
• Uremic symptoms, e.g. nausea, weight loss• Recent change in philosophy to “early start”, where
patient is started on dialysis before getting sick• Attempt to start dialysis when creatinine clearance is <15 ml /
min• Diabetics are started on dialysis sooner (cr cl < 20
ml/min) because they don’t tolerate uremia well
INDICATIONS FOR DIALYSIS
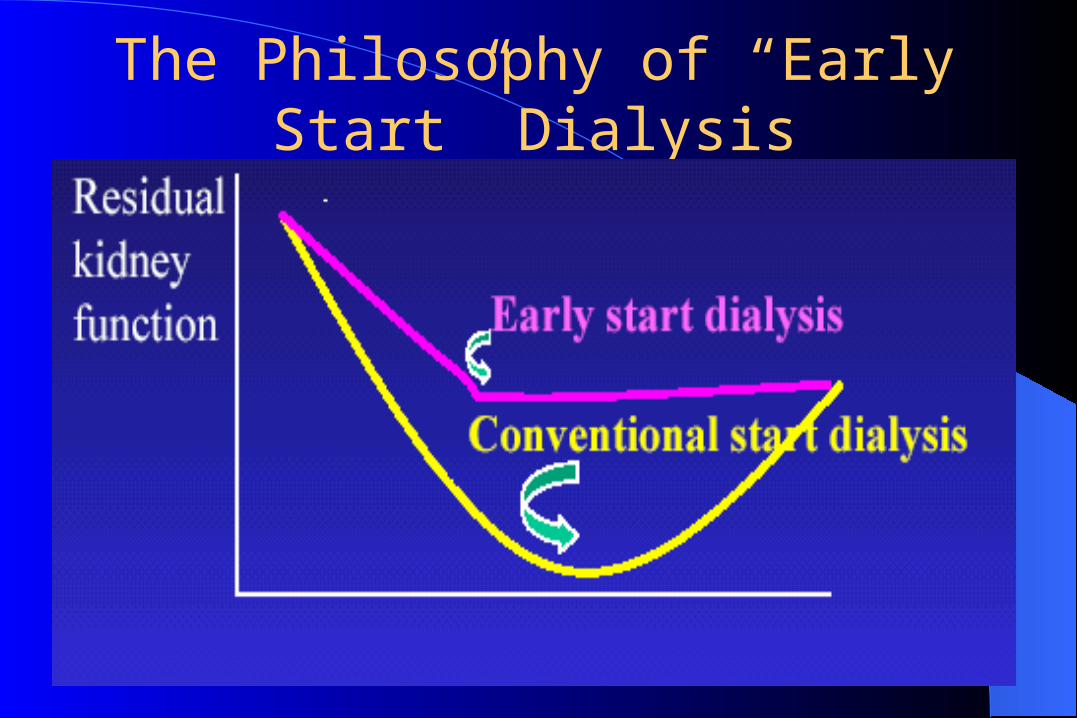
The Philosophy of “Early Start” Dialysis
Goals of Dialysis
1. Solute/toxin removal (blood purification)2. Removal of salt and water (ultrafiltration)
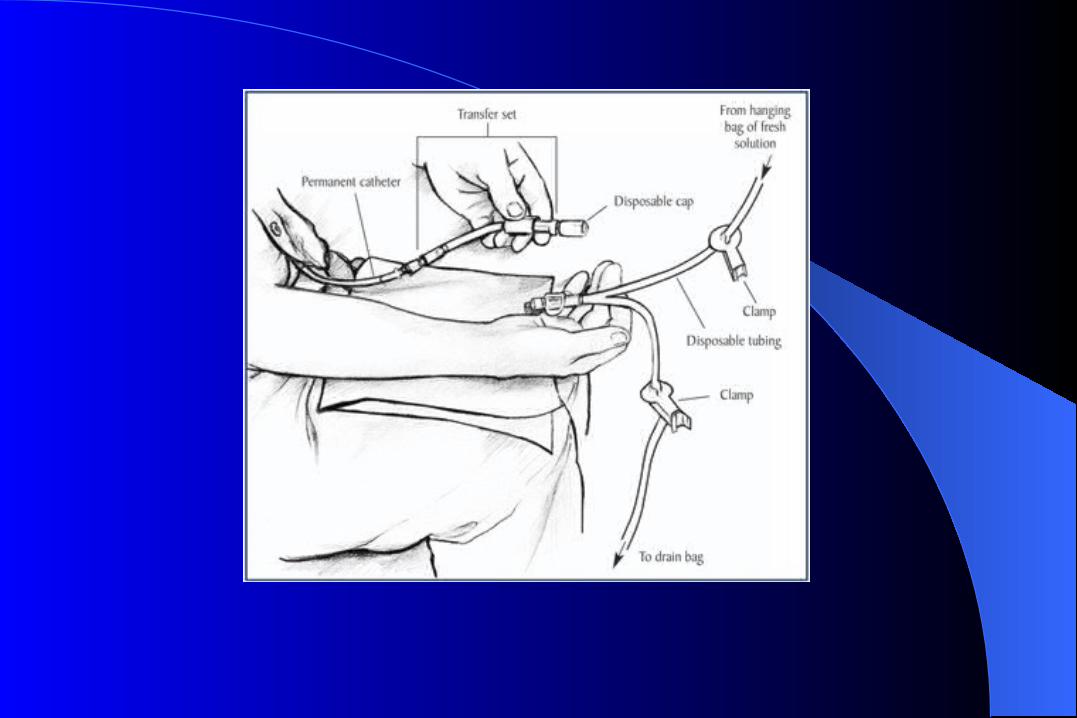
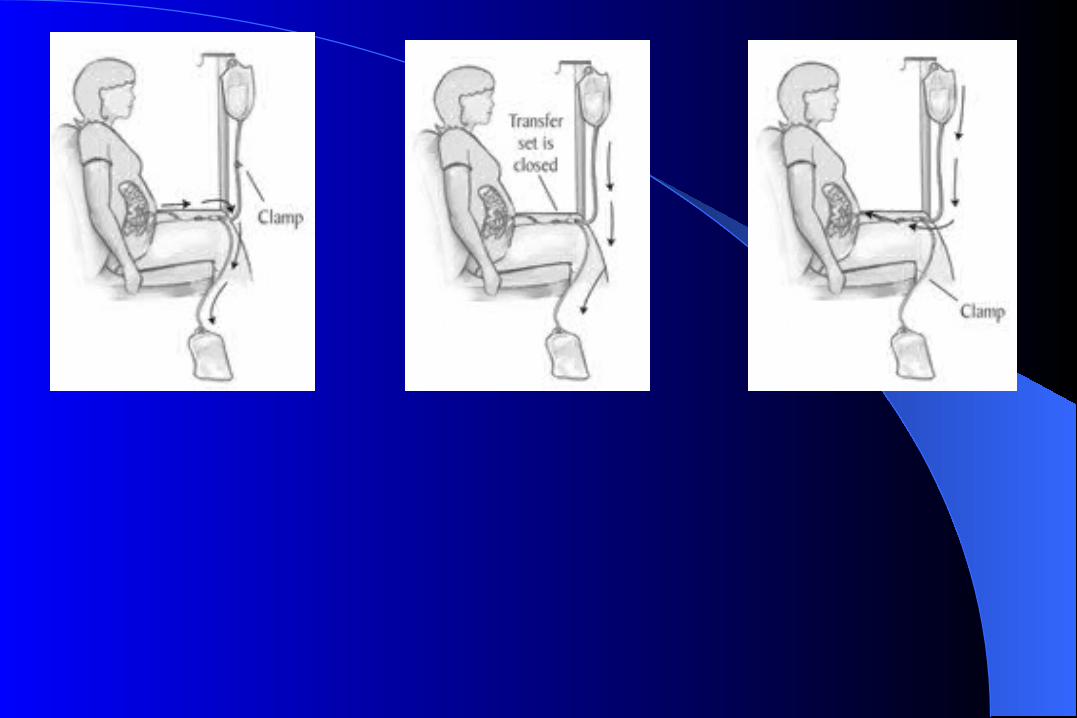
Peritoneal DialysisCatheter is inserted surgically or laparoscopically
into peritoneal cavityDialysis fluid high in glucose concentration is
instilled through catheter and allowed to dwell in the cavity
Uremic toxins diffuse from ECF into the peritoneal fluid
Ultrafiltration by osmosis (glucose in fluid)
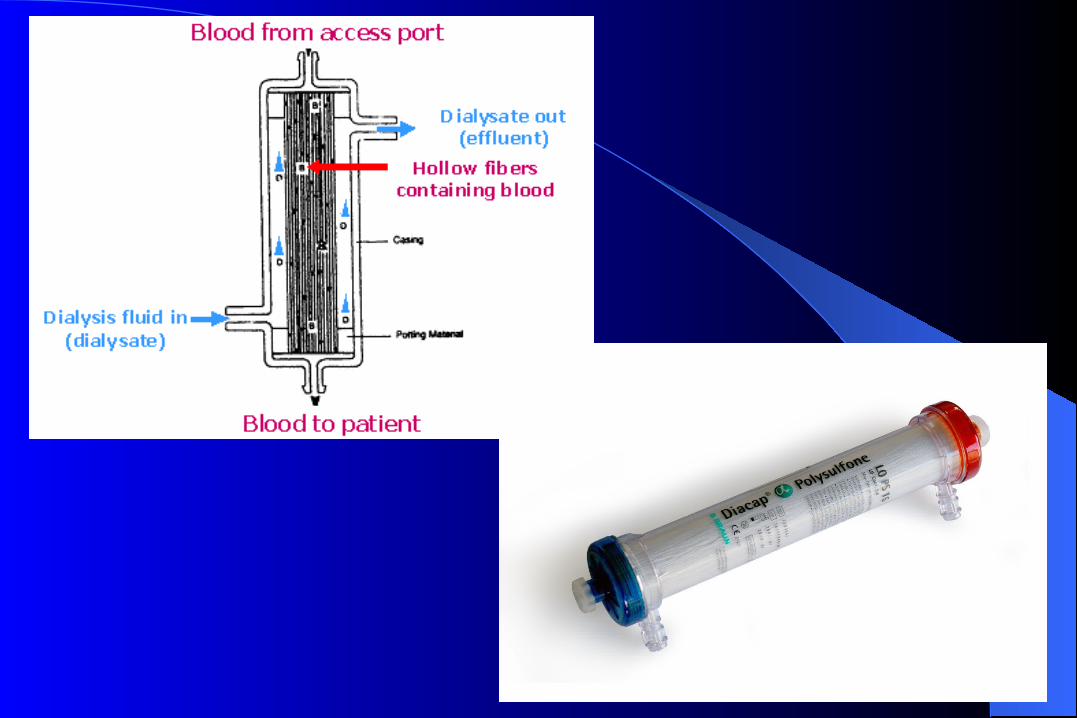
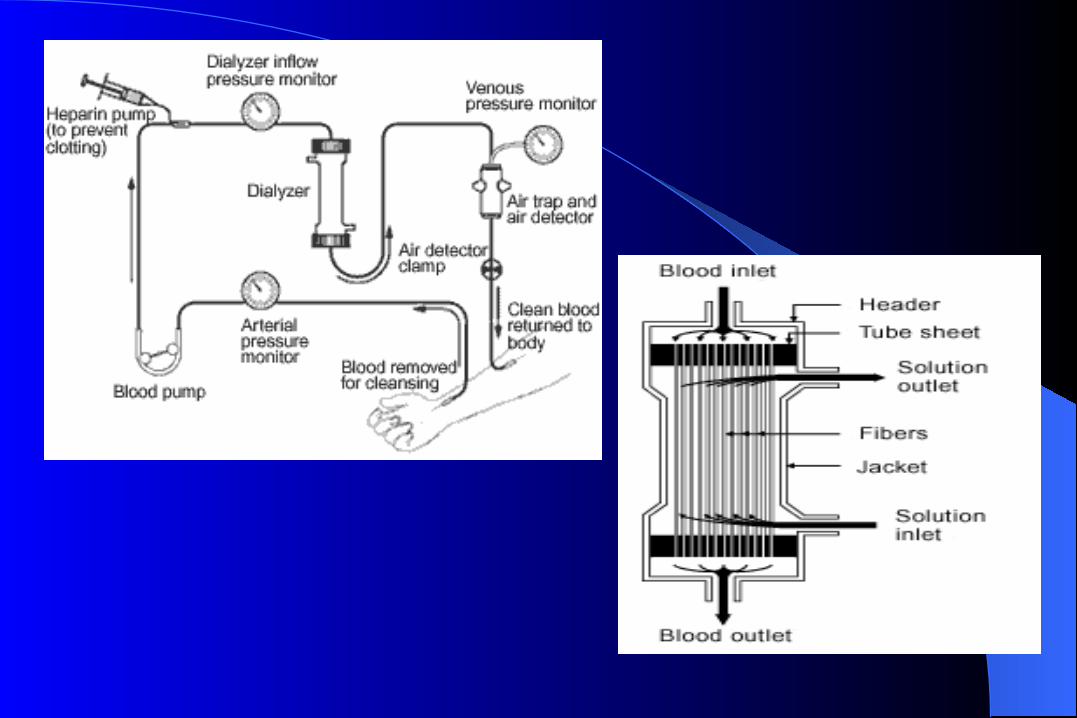
HemodialysisBlood is removed from the body and travels to the
hemodialysis machine where it is run across a semipermeable membrane with a physiologic solution on the other side of the membrane
Uremic toxins cross into dialysate by diffusion and convection
Ultrafiltration by a hydraulic pressure placed across the dialysis membrane
Hemodialysis (cont’d)Intermittent hemodialysis
– Typically patients undergo dialysis for 3 to 4 hours daily or on alternate days depending on their catabolic state
Continuous hemodialysis– Continuous renal-replacement therapy, patients undergo
dialysis Continuously usually, it is recommended because of hemodynamic instability.
Hemodialysis (cont’d)Usually done as an intermittent procedure, eg for 4
hours 3 X a weekRequires a vascular access to allow for repeated needle
insertion and high blood flow rates– construction of an arteriovenous fistula in the fore arm– insertion of a prosthetic vascular graft in the arm, or– indwelling catheter into a major vein
Renal Transplantation
A successful kidney transplant is the only way to fully, or almost fully, correct uremia
Types of Renal Transplantation
– Cadaveric (4 to 5 years waiting time)– Living related– Living unrelated

dialysis





























