Embed Size (px)
DESCRIPTION
Useful information for the patient with chronic renal failure.
Citation preview

1
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
[CHRONIC RENAL FAILURE]Useful information for the patient
2009
Gabriela Caballero

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
Chronic renal failure and its progression
Normal kidneys
Where they are
What they do
Common signs of kidney disease
Tests for kidney disease
Further information
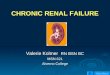
Where are the kidneys?
Most people have two kidneys, which sit at the back of the abdomen (behind the liver and intestines) in the small of the back on either side of the spine. Each is

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
11-14 cms (5-6 inches) long and is bean-shaped. It is very difficult to examine a normal kidney because they are far back when examined from the front, and behind a lot of muscles when examined from the back. From the kidneys, the collecting systems funnel the urine into tubes (ureters) go down to the bladder. The connection to the outside is along the urethra.
Arteries, veins, ureters and bladder. This image is one from the excellent animation described below.
A cross-section of the body taken along the red dotted line shown in the diagram above. (Imagine that the body has been cut across, and you are looking up from below.) The kidneys are to the back, and quite far in and difficult to feel from the surface.

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
Each kidney is joined to the largest artery in the body, the aorta, by a short renal artery. The kidneys have a huge blood supply - one fifth (20%) of normal blood flow leaving the heart.
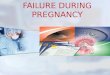
Inside each kidney, blood is channelled to 1 million tiny filters, each one called a glomerulus (the plural is glomeruli). Glomeruli are each joined onto small tubes (tubules) to make nephrons, and each day 150 litres (40 US gallons) of filtrate passes into the nephrons - 100 times the average daily amount of urine. As the fluid passes along these tubes, most of it is taken back into the blood stream (reabsorbed), leaving only those things that are to be sent out in the urine. Control mechanisms can vary
A single glomerulus and nephron - there are one million of these in each kidney.

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
the amount of water, salt, and other substances that are left in the urine when it
ANIMATION
Click here to see an animation of where the kidneys are, and a bit about how they work, from the Kidney Patient Guide (Wrexham Maelor Hospital, Wales). You need Flash Player on your PC (or Mac) to see it work (links to get this free are provided).
What do the kidneys do?
1. remove toxic waste products 2. remove excess water and salts
3. play a part in controlling your blood pressure

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
4. produce erythropoietin (epo for short) which stimulates red cell production from the bone marrow - you get anaemic without this
5. help to keep calcium and phosphate in balance for healthy bones
6. maintain the blood in a neutral (non-acid) state
Signs that the kidneys are not working properly
Urine tests may show blood or protein that should not normally be there. More information on haematuria (blood in the urine) and proteinuria (protein in the urine) is given on other pages.
Blood pressure may be high. Most people with high blood pressure do not have serious kidney disease, but high blood pressure can be a sign of kidney disease. It is more likely to be connected to kidney disease in people who are young, or have severe high blood pressure.
Trouble passing urine is rarely caused by kidney trouble - unless the kidneys are very severely damaged. It is more commonly caused by problems in the bladder, or in the nerves supplying the bladder, or by infection in the urine.
Pain around the kidneys is an uncommon symptom in kidney disease except with kidney stones, and

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
usually has alternative explanations. It is very common with kidney stones, and sometimes occurs with urine infections. Patients with large cysts in the kidney may get pain from them. Sometimes blockage of the artery to the kidney causes pain. Otherwise pain is unusual in kidney disease.
Other symptoms come from loss of kidney function. In the early stages of many kidney diseases, there are no symptoms at all. Kidney function needs to be quite badly damaged before any symptoms become noticeable. At first these are usually very vague and non-specific, and easily confused with many other conditions. A general slowing down and tiredness are common. Later symptoms may include loss of appetite, itch, poor sleep, and many others. Some of these are described on our pages on chronic renal failure and its progression.
Tests for kidney disease
Tests of kidney function
Imaging tests (X-rays etc.)
Biopsy
Tests of kidney function

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
Blood tests (more info about individual kidney blood tests)
Urea a simple test, but the result is affected by food and by dehydration
Creatinine a more reliable measure
More accurate tests to show GFRGFR means glomerular filtration rate, the most useful measure of kidney function. As the normal value is about 100, it gives an approximate 'score out of 100' for kidney function. However your normal GFR depends on your size and age.
Creatinine clearance
requires collection of all urine over 24h, with a blood test.
Isotope tracer tests
involve injecting a small amount of a substance and seeing how fast the kidneys remove it. This is usually more accurate than creatinine clearance.
Predicting GFR using just blood tests (eGFR, estimated GFR)Equations The Cockroft-Gault and MDRD

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
equations use use blood tests, age, and weight to work out approximately what the creatinine clearance or GFR are. They are not as good as measuring GFR directly, but they are very useful. Calculate yours (from the Renal Association website). Remember that this is not as accurate as measuring GFR, and in some people eGFR may be quite far from the real GFR. Explain reduced GFR.
Imaging tests (X-rays etc.)
A number of different kinds of test can be used to show the kidneys. These are some common examples.

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
Ultrasound is the most commonly used technique. It uses sound waves, not X-rays, and seems to be completely safe, even in pregnancy. The pictures look better during the examination than when 'stills' are shown. This image shows a normal kidney by ultrasound (top right), with a diagram below it to show the outline of the kidney.
CT - Computed tomography, the 'CAT scan', is widely used to show organs and structures. The one on the left shows just the left half of the body, with the kidney shown in pink on the diagram beside it (compare with the figure above).

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
MRI - Magnetic resonance imaging is another type of cross-sectional imaging like CT. It is sometimes useful for showing particular regions well, and it can sometimes be used to show blood vessels as an alternative to arteriography (see below). IVU (or IVP) - intravenous urography (or pyelography). In this test an injection of a substance that is eliminated through the kidneys is given. This shows up on X-rays, and it can be followed travelling from the kidney, down the ureters into the bladder. It is useful for showing the ureters and for

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
suspected kidney stones. This image shows the left kidney seen from the front, with dye in the collecting system leading into the top of the ureter.
Arteriography (angiography) This is a way of showing the blood supply to the kidneys. It usually requires injection of contrast material into the artery that you are trying to see. It is described on another page on angiography and angioplasty. Here is an example showing the blood supply to the left kidney. A thin tube has been passed into the main artery to the lower body (the aorta)

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
from the groin, and an injection of contrast material given. The renal artery on the left (the right side of the picture) is blocked, while that on the right is narrowed.
Kidney biopsy
A kidney biopsy involves taking a small sample of kidney through a needle to look at it under the microscope. More information about this test is given in our page on renal biopsy.
Renal failure means that the kidneys aren't working properly. If the renal failure is chronic, it is lasting and kidney function is unlikely to improve. However you can remain quite well until late on in chronic renal failure. It is therefore important to stop it from getting worse, if at all possible. 'Chronic renal failure' is often shortened to CRF. CKD, which stands for for 'Chronic kidney disease', means the same thing.
How do you know about chronic renal failure?

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
CKD (CRF) often gets worse - progression of CRFCan end-stage renal failure be prevented?What do kidneys do? Stages of kidney diseaseTreatment Is there anything else that I should do or not do?Further information
How do you know about chronic renal failure (CKD)?
As many people with chronic renal failure have no symptoms, it is often only diagnosed after blood tests. As your kidney function deteriorates, you might develop any of the following symptoms: poor appetite, nausea and vomiting, tiredness, fluid retention (swollen ankles or shortness of breath), itch, cramps, or restless legs. However there can be other explanations for most of these symptoms.
What about progression?
For some reason, once kidneys have been damaged, they may continue to get worse over months and years, even long after the disease that caused the damage has gone. This is more likely if you have high

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
blood pressure, and if there is much protein leaking into the urine. Renal failure that requires dialysis or a kidney transplant to keep you alive is known as end stage renal failure, or ESRF.
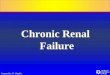
The graph shows a patient's kidney function over several years. His kidney function was severely damaged at first, but with treatment improved to about 30% of normal, so that he was quite well. Unfortunately
over the next 5 years his damaged kidneys slowly deteriorated, so that eventually he needed dialysis. This is a 'reciprocal creatinine' chart, which can help to show how things are going.
This is a blank reciprocal creatinine chart on which you can fill in your own results. Several blood test results over months or longer are needed to make the graph useful. The chart was made by Dr Richard Phelps.
Can end-stage renal failure be prevented?

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
Sometimes it can - and even if it cannot be prevented, it can often be delayed by many years. This involves careful attention to the things mentioned under 'treatment' below. However attention to two things may be especially important:
Blood pressure
Blood pressure control, particularly using ACE inhibitors and related drugs
DietThis is more controversial and the risks and benefits need careful analysis.
See what treatment is required below for more information about these.
Stages of kidney disease
In the last few years a useful classification of renal failure has been developed. It needs you to know your GFR - glomerular filtration rate. This can be measured, or predicted from your age, weight, blood tests etc. The KDOQI stages of kidney disease are:
Stage GFR Description Treatment stage1 90+ Normal kidney
function but urine or other abnormalities point to kidney disease
Observation, control of blood pressure

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
2 60-89
Mildly reduced kidney function, urine or other abnormalities point to kidney disease
Blood pressure control, monitoring, find out why.
3 30-59
Moderately reduced kidney function
More of the above, and probably diagnosis, if not already made.
4 15-29
Severely reduced kidney function
Planning for endstage renal failure - more info
5 14 or less
Very severe, or endstage kidney failure (sometimes call established renal failure)
See treatment choices for endstage renal failure.
Stage 2 kidney disease is a tricky area, because normal GFR falls with age, and therefore many normal older people may fall into this category. Equations used to predict GFR (rather than real measurements) may also give falsely low results in people with near-normal function.
At stages 1-3 kidney disease you don't usually feel unwell - this usually just begins at stage 4. Despite this, at stages 1-3 you:

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
Are at risk of going on to get more severe kidney disease
Are at increased risk of getting heart disease or other illnesses affecting arteries.
It is known that you can reduce both of these risks by careful monitoring and treatment. This page includes information about this and is particularly relevant to stages 2-4.
The different diseases that can cause renal failure may also influence what are the best treatments for you.
What do kidneys do?
1. remove toxic waste products 2. remove excess water and salts
3. play a part in controlling your blood pressure
4. produce erythropoietin ( epo for short) which stimulates red cell production from the bone marrow - you get anaemic without this
5. help to keep calcium and phosphate in balance for healthy bones
6. maintain the blood in a neutral (non-acid) state

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
What treatment is required?
Some kidney diseases require specific treatment that will help that particular problem. Here we are describing general treatment that may be required for anyone with failing kidneys, whatever the cause.
Fluid and salt problems
You may have to follow a fluid restriction or have to take 'water tablets' (diuretics, for example Frusemide), and to restrict salt intake. This is to prevent fluid overload which can cause troublesome symptoms such as swollen ankles or shortness of breath. Your doctor may give you a 'target' or 'ideal' weight (also called dry weight). Occasionally people have the opposite problem, and need to take extra fluid and salt.
Blood pressure
Most people will have to take medication to control blood pressure. Excellent blood pressure control has been shown to slow down the progression of chronic renal failure, in addition to the benefits to the heart and blood vessels elsewhere in the body. Different

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
medicines suit different people, but often an ACE inhibitor (or a similar drug) will be recommended, as these are particularly good for kidney diseases. Your doctors will advise you about this (and see separate information on high blood pressure in kidney disease).
Anaemia
The anaemia that goes with renal failure is mainly due to a deficiency of a hormone called erythropoietin (Epo). Epo is produced by the kidney to stimulate red blood cell production from the bone marrow. A deficiency of Epo leads to anaemia.
Often the anaemia of renal failure can be helped by taking iron. Some people remain short of iron even when taking iron tablets. If so, you might need a course of intravenous iron injections. This is usually done at the hospital as an out patient.
With more severe anaemia you may be prescribed Epo, which has to be given as injections, usually once or twice a week. You can learn to give this to yourself quite easily.
Bones
Renal bone disease can be a serious problem for people who have had chronic renal failure for a long time. It can cause aches, pains and sometimes

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
fractures. The aim is to prevent it, as treatment is much harder later. In renal failure typically the calcium level in the blood becomes low and the phosphate level high. This imbalance neeeds treating, or the body overproduces parathyroid hormone in an attempt to control it, and this causes thinning of the bones. You may have to take a combination of the following:
Alfacalcidol or calcitriol: these are active forms of Vitamin D, which is often short in renal failure, as the kidneys fail to process it.
Phosphate binders (eg Phosex, Calcichew, Calcium 500, Renagel) help to prevent too much absorption of phosphate from the gut and thus keep the level in the blood lower. Your diet may also help with this.
Diet
You will be asked to follow a special diet in which there may be controlled amounts of protein, salt, phosphate, and potassium. You may not need to restrict all of these, and recommendations are likely to change with time. It is also important to avoid under-feeding. This is why the dietitian is an important member of the renal team.

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
Diet in Renal Failure and CKD
'Kidney Diet Home'
There isn't a 'Renal Diet'
There is no single renal diet, best advice will vary according to you, and your tests. On these pages we can only give some general ideas and advice.
Detailed advice for patients with severe kidney disease (less than 30% function, stages 4 and 5 CKD) is best from a renal dietitian.
What's in food?
Protein

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
About protein
A typical daily intake in the UK is 60-80g, about 1g/kg of ideal body weight. If you are eating enough calories you can manage with 45-60g
(0.75g/kg). The richest sources of protein are Animal protein - meat, fish, cheese, eggs, milk, and Vegetable protein - nuts, pulses (beans, lentils etc), tofu, quorn.
Excessive intake of protein must be avoided in CKD, and sometimes a low protein diet has been advised for patients with renal failure. We don't usually do this.
In CKD protein intake should be normal - not high, not too low.
On haemodialysis a slightly higher protein intake is recommended. On PD a higher protein intake is recommended due to a small loss of protein from the drained fluid (dialysate).
How much protein does food contain?

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
Milk 500ml (a pint is 568ml)
17g
Yoghurt (1 pot) 7g
40g portion of cheese
10g
Tin of beans (small, 135g)
7g
Cooked meat 100g26-28g
Egg (1 medium) 8g
Sodium (salt)
About sodium (salt)
A typical daily intake in the UK is 150 - 200mmol (9-12g of

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
salt, or 3-5g of sodium). We need less than half of this.Only around 10% of sodium is found in fresh food, the rest is added as salt or sodium bicarbonate in cooking and food processing, and as table salt sprinkled on the food after cooking.
Common salt is sodium chloride. Modern diets contain too much salt, and sick kidneys cannot cope. High salt intake leads to high blood pressure and to fluid retention and overload. Many blood pressure tablets only work properly if combined with a reduced salt intake.
In most patients with kidney disease or on dialysis we recommend keeping salt down to 'no added salt' levels of less than 100mmol/day (6g of salt, which is just over 2g of sodium - and still a lot more than we need). This allows small amounts of salt to be used in cooking, but means limiting very salty foods, and not adding salt to food after it has been cooked. Less salt may be better still!
Salt substitutes such as 'Lo-Salt' are not suitable for patients with renal failure, because they contain large amounts of potassium.
Many pre-cooked meals and a lot of canned or preserved food have a high salt content.
Sodium can also be found in some medicines. Effervescent or soluble painkillers are a particular

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
problem - don't use them if you need to control your salt intake.
Potassium
About potassium
A typical daily intake in the UK is 50-150mmolPotassium is found particularly in leafy vegetables and most fruit and fruit juice, and in potatoes, especially if they are
fried or baked.
Potassium levels can be high in severe renal failure and on dialysis, but potassium intake should not be restricted routinely - only if tests show high potassium levels. This is because potassium-containing foods include many healthy foods.Very high potassium levels (e.g. 6.5 or higher) can be dangerous as they can lead to a cardiac arrest. As well as diet, some drugs can cause high potassium in

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
patients with CKD, and there are some other causes. More detail is available from the links below.
Fluid (liquids)
About fluid
Most people drink 1-2 litres a day and don't need to reduce fluid intake until kidney disease is very severe. But if you are a dialysis patient who doesn't produce urine, you have
to cut down the amount you drink - that's obvious.
All drinks contain mostly water. Fluids refer to all drinks taken per day. If you are not on dialysis, you should not restrict fluids unless you have a particular problem with fluid overload, you should just drink when you are thirsty. For most patients there is no special benefit from drinking extra water.
If you have a problem with fluid retention, it is very important to limit salt intake. It is impossible to control your fluid intake if you are taking too much salt - you just get too thirsty.

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
On haemodialysis the fluid allowance for each patient often needs to be quite strictly controlled.
Phosphate
About phosphate
Phosphate is found in association with protein, especially in milk and cheese. Only a few other foods contain a lot of phosphate like wholegrain cereals,
baking powder, shellfish. Other sources are convenience foods which have phosphates added by food manufacturers.
Too much phosphate in the blood (hyperphosphataemia) usually becomes a significant problem in the later stages of renal failure (stages 4 and 5 CKD, usually less than 20% kidney function). The problem continues for most dialysis patients, as dialysis does not remove enough phosphate unless it is

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
very frequent or intensive. A combination of diet and medicines are usually needed.
Calcium and phosphate are a major problem for kidney patients, causing serious bone disease across the years if they cannot be controlled. High calcium and phosphate also makes you itch very badly, and is probably damaging to arteries too. People with very poor phosphate control don't do so well on dialysis.
Diet alone is rarely enough to control phosphate in severe renal failure, and medicines called phosphate binders are also used. These are taken with food, and work by keeping the phosphate in your food in the gut, preventing it being absorbed into the blood when the food is digested. It is important that these are taken at the right time just before food (or with it) as they won't work otherwise.
In both CKD and dialysis patients, the aim is to keep phosphate levels below 1.8mmol/l. Download short information from the box above about phosphate in food and phosphate binders.
Energy
High energy foods
Too few calories lead to the breakdown of muscle

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
to provide energy. If you lose muscle you become weak and debilitated. Once this has happened it takes months to recover strength. Appetite is decreased in many patients with kidney disease, and in some it is necessary to provide supplements.
Malnutrition can be a serious problem in severe kidney disease and in some dialysis patients. It tends to be a particular problem in people who have had other illnesses, or a complicated time as they have developed kidney failure. Help from expert dietitians is very valuable if this occurs.
Acidaemia
In renal failure the kidneys are unable to excrete the normal acid waste products of the body. People in renal failure often have too much acid in the blood (acidaemia) and have to take bicarbonate tablets to neutralise this.
Prevention of heart disease, stroke and vascular diseasePeople with kidney disease are at greatly increased risk of heart disease, stroke and problems with the circulation. It is particularly important that you should not smoke as this increases the risk of heart disease even further. You should also attempt to maintain a healthy diet and take regular exercise. Cholesterol and other lipids are often high in kidney disease, this may require special medication.
Once you have advanced renal failure (stages 3-4), at each visit you make to clinic the following things will be in the minds of the staff who see you:

2
[CHRONIC RENAL FAILURE] 5 de febrero de 2009
Fluid balanceBlood pressure controlDiet and nutritionAnaemiaPrevention of bone diseaseThe levels of other things in the bloodPrevention of heart disease, stroke and vascular disease
Is there anything else that I should do or not do?
Don't smoke Avoid anti-inflammatory drugs (including some
that can be bought without a prescription, such as ibuprofen) unless they are approved by a doctor who knows about your kidney problem. They can sometimes worsen kidney function in people with damaged kidneys.
Eat a healthy diet, and follow the recommended special diet if you have one.
Take regular exercise
Be sure to have your blood pressure checked regularly and to take treatment that is prescribed for it