Embed Size (px)
Citation preview

Epilepsy & Behavior 34 (2014) 1–5
Contents lists available at ScienceDirect
Epilepsy & Behavior
j ourna l homepage: www.e lsev ie r .com/ locate /yebeh
Childhood-onset primary generalized epilepsy — Impacts on children'spreferences for participation in out-of-school activities
Batya Engel-Yeger a, Sharon Zlotnik b, Sarit Ravid c, Eli Shahar c,⁎a Department of Occupational Therapy, Faculty of Social Welfare and Health Sciences, University of Haifa, Haifa, Israelb Department of Occupational Therapy, Rambam Medical Center, Rappaport School of Medicine, Haifa, Israelc Child Neurology Unit & Epilepsy Service, Meyer Children Hospital, Rambam Medical Center, Haifa, Israel
⁎ Corresponding author at: Child neurology Unit & EpilCenter, Haifa, Israel Tel.: +972 4 8543059; fax: +972 4 8
E-mail address: [email protected] (E. Sh
http://dx.doi.org/10.1016/j.yebeh.2014.02.0211525-5050/© 2014 Elsevier Inc. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:Received 16 September 2013Revised 16 February 2014Accepted 19 February 2014Available online 22 March 2014
Keywords:ChildrenPrimary generalized epilepsyParticipationDaily activities
The purpose of this study was to compare preferences for participation in out-of-school activities betweenchildren with childhood-onset primary generalized epilepsy and their healthy peers. Overall, participants were56 children aged 6–11 years. The study group included 26 children with childhood-onset primary generalizedepilepsy. The controls were 30 healthy children. Parents of all participants completed a demographic andhealth status questionnaire. All children completed the Preference Assessment of Children (PAC) that profilesthe out-of-school activities the child wishes to participate in. Scores are calculated for five activity types, namely,recreational, active physical, social, skill-based, and self-improvement and for two domains of formal and infor-mal activities.Childrenwith generalized epilepsy showed a similar preference for participation in out-of-school activities as didtheir healthy peers. The study group showed a lower preference for participation in social activities but showed ahigher preference for participation in self-improvement activities. In both groups, younger children (aged6–8 years) showed a lower preference for participation in most PAC scales. Older children (aged 9–11 years)showed a higher preference for participation in social activities. Difference between genders was close to beingstatistically significant in the skill-based activities (F1,21= 3.84, p= .06),where girls showed a higher preferencecompared with boys.Intervention policies need to be undertaken in order to encourage children with epilepsy to participate in ac-tivities together with their healthy peers, aiming to enhance the well-being of children with primary general-ized epilepsy.
© 2014 Elsevier Inc. All rights reserved.
1. Introduction
Epilepsy is a common neurological disorder characterized by a ten-dency to develop recurrent seizures and is commonly defined by twoor more unprovoked seizures [1]. Epilepsy in children, including gener-alized epilepsy, is known to have several comorbidities, includingmotor[2], cognitive, and language deficiencies [3], and each of themmay havesubstantial social, physical, and psychological consequences on a child'sperformance and participation [4].
Participation, defined as an experience through which we acquireskills and competencies, connect with others, and find purpose andmeaning in life [5], is receiving greater attention in health practice andtheory. The conceptual model the World Health Organization Interna-tional Classification of Functioning Disability and Health (ICF) [4] em-phasizes that health is no longer narrowly equated with medicine, and
epsy Service, Rambam Meducal543405.ahar).
body dysfunctions are no longer seen as only determining disability[6]. One of the important factors of participation is activity preference[7], since participation can lead to the development of stronger interests[7,8]. These preferences are influenced by factors such as age, exposureto opportunities, proficiency, and enjoyment level [5,9]. Meaningfulparticipation is known to be essential for psychological and emotionalwell-being, skill development, life satisfaction, and competence [10].Participation enables children to explore their social, intellectual, emo-tional, communicative, and physical potential and is an importantpredictor of future life satisfaction [11].
Studies highlight that children with disabilities are at increased riskof limited participation in everyday activities [12,13] and tend to engagein less varied leisure activities. Their participation is manifested bya greater frequency of quiet recreation activities and fewer social ac-tivities [14,15]. Their social isolation and loneliness also impact theirpreference for activities [16–18].
Studies dealing with epilepsy in childhood indicate that in additionto the medical impacts of epilepsy, with respect to loss of control,drug effects [19], and comorbidity, epilepsy has a marked impact on a

2 B. Engel-Yeger et al. / Epilepsy & Behavior 34 (2014) 1–5
child's life [20]. Population-based studies emphasized that 70–76% ofchildren with epilepsy have some type of disability and higher rateof daily stressors affecting their daily lives and choices [21–23], andnoted that children with epilepsy aged 5–17 years participated infewer group and total sports activities as compared with their healthypeers. The authors stressed thenegative outcomes of that limited partic-ipation and highlighted the relation between reduced participation insports activities and children's obesity. Gordon et al. [24] added thateven if people with epilepsy show similar types of leisure activities asdo their healthypeers, thosewith epilepsy tend to choose to be involvedin specific kinds of activities. For example, in the physical activities, itwas noted that Canadian people aged 12–39 years who suffered fromepilepsy were more likely to use walking as a leisure physical activityand were less likely to be involved in ice hockey, weight training, andhome exercise compared with healthy controls.
At present, data concerning participation of children with epilepsyand specifically thosewith childhood-onset primary generalized epilep-sy are still scarce. Most studies refer to participation in a specific type ofactivity (social activity or sports activity) but lack the vast perspectiveon participation as expressed in other activity types. The purpose ofthe present study was to compare the activity preferences of childrenwith childhood-onset primary generalized epilepsy with those of typi-cally developing peers.
2. Methods
2.1. Participants
Fifty-six children, aged 6–11 years, participated in this study. Thestudy group included 26 children with childhood-onset primary gener-alized epilepsy (17 boys and 9 girls; mean age = 8.52 ± 1.59), whowere referred to the neurological service at Mayer's Children Hospital,Rambam Medical Center, Haifa, Israel. All were members of a two-parent family belonging to the middle class socioeconomic status. Thediagnosis of primary generalized epilepsy was based on the clinicalpresentation of generalized seizures along with generalized epilepti-form discharges recorded on the electroencephalography (EEG) fulfill-ing the criteria of the International League against Epilepsy [25]. Theseizures in all children receiving antiepileptic therapy, mainly valproicacid alone at lower effective doses, were controlled. Children's cognitivelevel was within normal limits. Additional chronic illnesses were notrecorded in the study group. The children studied in elementary schoolsin their community. Twenty-five children studied in the regular educa-tion system, and one child studied in a school for special education.However, the IQ level of all childrenwas in the normal range. Most par-ents were born in Israel (80% of the fathers and 85% of the mothers).
The control group included 30 healthy children (21 boys and 9 girls;mean age = 8.43 ± 1.63) with normal development, who werematched to the study group by age, gender, and living area. Thus, bothgroups shared similar facilities for out-of-school activities. The controlswere recruited by an advertisement that called for participating in astudy about children's patterns of participation in out-of-school activi-ties. Children with either established neurological disorders or learningdisabilities were excluded.
All participants were divided into two age groups: 6–8 yearsand 9–11 years. In the study group, the younger age group included12 children, and the older age group included 11 children (3 caseswere missing). In the control group, the younger age group included17 children, and the older age group included 13 children.
2.2. Instruments
2.2.1. Neurological assessment of children with epilepsyNeurological assessment includes a complete neurological examina-
tion; global developmental milestones including cognition, surface, andsleep-deprived EEG; and additional neuroimaging techniques including
computerized tomography (CT), magnetic resonance imaging (MRI),and positron emission tomography (PET) if required.
2.2.2. Demographic questionnaireDemographic questionnaire included data on a child's age, gender,
family sociodemographic level, health status, medications, treatments,and physiotherapies.
2.2.3. The Preference Assessment of Children (PAC) [8]The Preference Assessment of Children evaluates children's prefer-
ences for participation in out-of-school activities with no relation towhether the activities are actually performed. Each activity is drawnon a card. The card also includes a phrase (in words) describing the ac-tivity. Scores are obtained for five activity types derived through factoranalysis of participation preference data: recreational, active physical,social, skill-based, and self-improvement/educational scales. Two scoresare also provided for two separately evaluated domains — formal andinformal. The formal domain includes structured activities that involverules or goals and that have a formally designated coach, leader, orinstructor (e.g., taking art lessons, learning to dance, swimming, andgetting extra help for schoolwork from a tutor). The informal domainincludes activities that have little or no planning and often are initiatedby oneself (e.g., reading, hanging out, and attending a party).
The child sorts the cards into three piles according to howmuch he/she prefers to do the activity as follows: (1) really likes to do, (2) sortof likes to do, and (3) does not like to do. The preferences do not neces-sarily refer to activities that are actually performed.Mean scores are cal-culated for each activity type, for each domain, and for the PAC totalscore ranging from 1 to 3. Preliminary assessments of the PAC havedemonstrated sufficient internal consistency, test–retest reliability,and validity [8].
2.3. Procedure
The Ethical Committee of Rambam Medical Center approved theperformance of this study. When visiting Mayer's Children Hospital,Rambam Medical Center, Haifa, parents were asked to complete thedemographic/health status questionnaire. Meanwhile, the childrencompleted the PAC. In the control group, parents, who responded tothe advertisement calling to participate in this study, were asked tocomplete the demographic/health status questionnaire with the datacollector in a phone conversation. Another meeting with the childrenwho answered the inclusion criteria in their homes was performed.Each child completed the PAC in a quiet room in the presence of thedata collector.
2.4. Data analysis
Descriptive statistics were used to describe children's demographicdata and PAC scores. A multivariate analysis of variance (MANOVA)with the general linear model examined the significance of differencebetween the study groups, the age groups, and the genders in PACscale's scores. T-test examined the difference between groups in PACtotal score. Probabilities below .05 were considered significant.
3. Results
The comparison of both groups revealed that children with gener-alized epilepsy showed a lower preference for participation in socialactivities (F1,49 = 4.52, p = .04) and a higher preference for participa-tion in self-improvement activities (F1,49 = 4.99, p = .03) comparedwith the controls (Table 1).
Age group effect was found in the social activities (F1,49 = 10.34,p = .002). In both groups, younger children (aged 6–8 years) showeda lower preference for participation in most PAC activities. However,the difference between the age groups was significant only in the

Table 1Comparison of PAC scores between children with generalized epilepsy and healthy peers.
PAC scales Children withepilepsy(n = 26)
Controls(n = 30)
F1,49; T51
Mean SD Mean SD
Total activities 1.61 .31 1.61 .27 T = .54Formal domain 1.76 .32 1.81 .41 F = .93Informal domain 1.56 .33 1.54 .25 F = .07Recreational activities 1.54 .43 1.53 .32 F = .08Active physical activities 1.55 .47 1.51 .39 F = .28Social activities 1.56 .41 1.36 .23 F = 4.52⁎
Skill-based activities 1.75 .37 1.78 .47 F = .45Self-improvement activities 1.71 .32 1.91 .42 F = 4.99⁎
⁎ p ≤ 0.05.
3B. Engel-Yeger et al. / Epilepsy & Behavior 34 (2014) 1–5
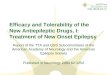
social activities— the older children (aged 9–11 years) showed a higherpreference for participation in social activities than did the younger chil-dren. This was found for the study group (F1,21 = 4.51, p = .04) (seeFig. 1) and for the controls (F1,28 = 5.97, p = .02) (see Fig. 2). Amongthe study group, difference between genders was on the verge ofbeing significant in the skill-based activities (F1,21 = 3.84, p = .06),where the girls showed a higher preference (mean = 1.55 ± .33)than did the boys (mean = 1.86 ± .36).
4. Discussion
The present study compared the activity preferences of childrenwith childhood-onset primary generalized epilepsy with those of typi-cally developing peers by using the PAC. The PAC provides a vast per-spective about participation in out-of-school activities. We chose toconduct this study based on the importance of participation to a child'sdevelopment and well-being and on the relatively limited literatureabout participation of children with epilepsy.
In general, childrenwith epilepsywere found to have similar prefer-ences for participation in out-of-school activities as did their healthypeers. This supports previous reports about participation of childrenwith physical disabilities [26,27]. Out-of-school activities includedmany leisure activities (such as doing crafts, reading, doing gymnastics,and hanging out) and activities performed in the community (such asparticipating in community organizations, going to the movies, andgoing to the public library). The PAC measures the child's preferenceseven if he/she does not actually participate in the activity. Thus, it maybe postulated that children with epilepsy wish to take part in activitiesand to feel an integrated part of the community as do their healthypeers.
Sk
Self-im
prov
emen
t acti
Form
al do
main
Info
rmal
dom
ain
Total
PAC scor
e
younger age group
older age group
Fig. 1. Comparison of PAC scores between age
Differences between groups were found in social activities — thestudy group showed a lower preference for participation in theseactivities compared with the controls. This result supports the studyof Jakovljević and Martinović [28], who reported reduced sociabilityamong children with multiple generalized seizure types aged11–18 years. Studies raise several reasons for the reduced social partic-ipation of children with epilepsy. First, seizures cause children to loseschool days [29]. Second, factors such as elevated anxiety (due to stressrelated to seizure clusters) also enhance their avoidance from socialevents. Third, drug side effects may contribute to stigma and socialsolitude. Clinicians should refer to these impacts and also pay attentionto age effects, since the reduced social participation of children withepilepsy may get worse with age and impair the child's physical andemotional quality of life [29].
Social participation is also crucial for integrating children withepilepsy in the community. Community participation and meaningfulrewarding activity are major goals in models of rehabilitation [30].Along these lines, Cushner-Weinstein et al. [31] found that a designedcamp for children with epilepsy improved their social interaction, re-sponsibility, and communication. Hence, understanding the activitypreference of children with epilepsy may assist in creating communityactivities that would fit their specific needs and enhance their inclusionwith their healthy peers.
In the present study, children with epilepsy showed a higher prefer-ence for participation in self-improvement activities. Self-improvementactivities include quiet activities, such as writing letters, reading, anddoing homework, which are usually performed at home and alone.The selection of quiet activities may be one way children manage ordeal with the side effects of medications [29]. Children may find moreconfidence and sense of control when participating in these activitiesin a relatively protective environment as their home. Nevertheless,self-improvement activities also include activities performed in thecommunity, such as going to the library, doing volunteer work, andshopping. It may be suggested that the higher preference for participa-tion in such activities also represents the children's desire to be involvedin the community and to enjoy the benefits of public places.
The results have demonstrated that among the children with epi-lepsy, the girls showed a higher preference for participation in skill-based activities than did the boys. This result supports the reports ofKing et al. [32] and Law et al. [13] on children with physical limita-tions. However, this interpretation should be further studied, sincethe difference between genders was not significant. Moreover, infor-mation about this issue among children with epilepsy is scarce andnot necessarily consistent with the present study results. For example,Jakovljević and Martinović [28], who evaluated children with epilepsyaged 11–18 years, found that girls demonstrated greater problemswith social competence than boys. Additional studies with larger
0
0.5
1
1.5
2
2.5
3
Recre
ation
al ac
tivitie
s
Active
phy
sical
activ
ities
Social
acti
vities
ill-ba
sed
activ
ities
vities
PAC scales
PA
C m
ean
sco
re
groups among the children with epilepsy.

0
0.5
1
1.5
2
2.5
3
Recre
ation
al ac
tivitie
s
Active
phy
sical
activ
ities
Social
acti
vities
Skill-b
ased
acti
vities
Self-im
prov
emen
t acti
vities
Form
al do
main
Info
rmal
dom
ain
Total
PAC scor
e
PAC scales
PA
C m
ean
sco
re
younger age group
older age group
Fig. 2. Comparison of PAC scores between age groups among the healthy peers.
4 B. Engel-Yeger et al. / Epilepsy & Behavior 34 (2014) 1–5
samples may shed light on gender role on participation patterns ofthis population.
In summary, although, in general, similarity exists in activity prefer-ences between with children with epilepsy and their healthy peers,the differences between groups may reflect the families'/children'scautious attitude toward social situations probably out of fear of sei-zures or fear of being revealed to have epilepsy: The parents' percep-tions are influenced by the overall atmosphere in the society andattitudes toward people with epilepsy. Moreover, participationin sports activities may be limited or even forbidden by the parentssince they have fear of situations associated with a potential increasedrisk of seizures or with stigmatization. Further studies are needed toassess the influence of a parent's perception of a child's preference forparticipation in activities.
Another important point is that considering the similar preferencesof children and the ICF model, it is important to refer to participation inits wider implications in the evaluation and intervention of childrenwith epilepsy [29]. Therapists should consider what the child wishesto participate in, even if it is not actually performed, and find theway to enhance the child's participation in his/her areas of interests.Such an approach may assure the optimal development of childrenwith epilepsy and elevate their quality of life [20]. In line with the cli-ent-centered approach, collecting information directly from the child,as was performed in the present study by using the PAC, may providea better understanding related to the child's point of view and self-experience. This may elevate the child's involvement in interventionand assist achieving intervention goals. Service providers for childrenwith epilepsy should consider factors that limit participation of thesechildren, such as lack of appropriate opportunities or suitable pro-grams, lack of physical assistance [33], and social problems withpeers. Intervention should focus on providing opportunities for thesechildren that would empower them, elevate their social interactions,reduce negative stereotypes, and enable them to become an integralpart of the community [21,34]. For achieving this, a collaboration be-tween physicians and other relevant health professions as occupationaltherapists, social workers, and psychologists is recommended. Inter-vention should also involve family members and education personnel[20].
Some limitations must be considered in the interpretations of thisstudy's results. First, the study consisted of a relatively small, conve-nience sample of children. In addition, other factors that might affectthe preferences of children, such as the severity of epilepsy, socioeco-nomic level, and parents' education, were not investigated. Larger stud-ies that would consider the impact of personal and familial factors onthe child's participation should be performed in order to enable the gen-eralizability of the results.
5. Conclusions
Medical professions should be aware that although children withepilepsy struggle with their complicated health condition and out-comes, they still wish to experience their childhood as do their healthyfriends and participate in similar activities. Multidisciplinaryintervention may enhance participation of children with epilepsy indaily life and, thus, encourage their development and elevate theirquality of life.
Conflict of interest
None of the authors has any conflict of interest to disclose.
References
[1] Engel J. Concepts of epilepsy. Epilepsia 1995;36(s1):23–9.[2] Hernandez MT, Sauerwein HC, Jambaque I, De Guise E, Lussier F, Lortie A, et al.
Deficits in executive functions and motor coordination in children with frontallobe epilepsy. Neuropsychologia 2002;40:384–400.
[3] Scabar A, Devescovi R, Blason L, Bravar L, Carrozzi M. Comorbidity of DCD and SLI:significance of epileptiform activity during sleep. Child Care Health Dev 2006;32:733–9.
[4] World Health Organization. International classification of functioning, disability andhealth. Geneva: World Health Organization; 2001.
[5] Law M. Participation in the occupations of everyday life. AJOT 2002;56(6):640–9.[6] Imrie B. Demystifying disability: a review of the international classification of func-
tioning, disability and health. Sociol Health Illn 2004;26(3):287–305.[7] Garton AF, Pratt C. Leisure activities of adolescent school students: predictors of
participation and interest. J Adolesc 1991;14:305–21.[8] King G, Law M, King S, Hurley P, Hanna S, Kertoy M, et al. Children's assessment of
participation and enjoyment (CAPE) and preferences for activities of children(PAC). San Antonio, TX: Harcourt Assessment, Inc.; 2004.
[9] Larson RW, Verma S. How children and adolescents spend time across the world:work, play, and developmental opportunities. Psychol Bull 1999;125:701–36.
[10] Lovell TA, Datillo J, Jekubovich NJ. Effects of leisure education on women aging withdisabilities. Act Adapt Aging 1996;21(2):37–58.
[11] Law M, Finkelman S, Hurley P, Rosenbaum P, King S, King G, et al. Participation ofchildren with physical disabilities: relationships with diagnosis, physical function,and demographic variables. Scand J Occup Ther 2004;11(4):156–62.
[12] Engel-Yeger B, Jarus T, Anabi D, Law M. Differences in patterns of participation be-tween youth with cerebral palsy and typical developing peers. AJOT 2009;63(1):96–104.
[13] Law M, King G, King S, Keroy M, Hurley P, Rosenbaum P, et al. Patterns of participa-tion in recreational and leisure activities among children with complex physicaldisabilities. Dev Med Child Neurol 2006;48:337–42.
[14] King G, Law M, King S, Rosenbaum P, Kertoy MK, Young NL. A conceptual modelof the factors affecting the recreation and leisure participation of children withdisabilities. Phys Occup Ther Pediatr 2003;23(1):63–90.
[15] Meijer SA, Sinnema G, Bijstra JO, Mellenbergh GJ, Wolters WHG. Social func-tioning in children with a chronic illness. J Child Psychol Psychiatry 2002;41:309–17.
[16] Engel-Yeger B, Ziv-On D. The relationship between sensory processing difficultiesand leisure activity preference of children with different types of ADHD. Res DevDisabil 2011;32(3):1154–62.

5B. Engel-Yeger et al. / Epilepsy & Behavior 34 (2014) 1–5
[17] Jarus T, Lourie-Gelberg Y, Engel-Yeger B, Bart O. Participation patternsof school-aged children with and without DCD. Res Dev Disabil2011;32:1323–31.
[18] King GA, Specht JA, Schultz I, Warr-Leeper G, Redekop W, Risebrough N. Social skillstraining for withdrawn unpopular children with physical disabilities: a preliminaryevaluation. Rehabil Psychol 1997;42(1):47–60.
[19] Bordonne C, Delalande O, Heran F. Disability and epilepsy. J Radiol 2010;91(12):1398–405.
[20] Ville D. Daily life of an epileptic child. Rev Prat 2012;62(10):1410–4.[21] Sillanpää M, Cross HJ. The psychosocial impact of epilepsy in childhood. Epilepsy
Behav 2009;15(2):S5–S10.[22] van Campen JS, Jansen FE, Steinbusch LC, Joëls M, Braun KP. Stress sensitivity
of childhood epilepsy is related to experienced negative life events. Epilepsia2012;53(9):1554–62.
[23] Wong J, Wirrell E. Physical activity in children/teens with epilepsy compared withthat in their siblings without epilepsy. Epilepsia 2006;47(3):631–9.
[24] Gordon KE, Dooley JM, Brna PM. Epilepsy and activity — a population-based study.Epilepsia 2010;51(11):2254–9.
[25] ILAE. http://www.ilae.org/Visitors/About_ILAE/Index.cfm. (last accessed: 20 August2013).
[26] Engel-Yeger B, Engel A, Kessel A. Differences in leisure activities between childrenwith allergic rhinitis and healthy peers. Int J Pediatr Otorhinolaryngol2010;74(12):1415–8.
[27] Engel-Yeger B, Shani-Adir A, Kessel A. Participation in leisure activities and sensorymodulation deficiencies of children with atopic dermatitis. Acta Paediatr 2011;100:e152–7.
[28] Jakovljević V, Martinović Ž. Social competence of children and adolescents withepilepsy. Seizure 2006;15(7):528–32.
[29] Mathiak K, Łuba M, Mathiak K, Karzel K, Wolańczyk T, Szczepanik E, et al. Qualityof life in childhood epilepsy with lateralized epileptogenic foci. BMC Neurol2010;10(1):69.
[30] King G, LawM, King S, Hurley P, Rosenbaum P, Hanna S, et al. Children's assessmentof participation and enjoyment (CAPE) and preferences for activities of children(PAC). San Antonio, Tx: Harcourt Assessment; 2004.
[31] Cushner-Weinstein S, Berl M, Salpekar JA, Johnson JL, Pearl PL, Conry JA, et al.The benefits of a camp designed for children with epilepsy: evaluating adaptivebehaviors over 3 years. Epilepsy Behav 2007;10(1):170–8.
[32] King G, Law M, King S, Hurley P, Hanna S, Kertoy M, et al. Measuring children'sparticipation in recreation and leisure activities: construct validation of the CAPEand PAC. Child Care Health Dev 2006;33(1):28–39.
[33] Schleien S, Green F, Heyne L. Integrated community recreation. In: Snell M, editor.Instruction of students with severe disabilities. 4th ed. New York: MacMillan;1993. p. 526–55.
[34] Law M, Haight M, Milroy B, Willms D, Stewart D, Rosenbaum P. Environmentalfactors affecting the occupations of children with physical disabilities. J Occup Sci1999;6(3):102–10.