Embed Size (px)
Citation preview

Clinical Radiology (1994) 49, 56-58
Chest Radiography Guidelines for General A Practical Approach P. W. P. BEARCROFT, J. H. SMALL and C. D. R. FLOWER
Department of Radiology, Addenbrooke's Hospital, Cambridge
Practitioners:
An intensive programme of guideline development and dissemination is not always practical. We designed general practitioner guidelines for chest radiography and disseminated them to a group of 33 practices selected randomly from the practices that refer more than five patients for chest radiography annually. The subsequent 2500 requests were analysed and demographic data, the referring practice and the relevant history noted. We documented a reduction in the proportion of referrals that were contrary to the guidelines by 30.5% (from 8.2% to 5.7%, P = 0.016), a reduction in referral rate with an inadequate history by 29.7% (from 15.5% to 10.9%, P- - 0.0008) and an increase in the frequency that a presumptive diagnosis was stated by 14.5% (from 42.9~ to 49.1%, P = 0.0025). There was no overall reduction in referral rate in the study group and the reasons for this are discussed. We conclude that guidelines for chest radiography are effective in reducing inappropriate requests and can also improve the clinical information provided. Bcarcroft, P.W.P., Small, J.H. & Flower, C.D,R. (1994). Clinical Radiology 49, 56-58. Chest Radiography Guidelines for General Practitioners: A Practical Approach
Accepted for Publication 28 June 1993
Clinical guidelines for the use of radiological services are proliferating rapidly. However, their role in General Practice needs closer examination. Guidelines are most effective if they are designed by or in collaboration with those who are to use them, if reminders specific to the patient are issued at the time of consultation, and if they are disseminated through a dedicated education pro- gramme [1-5]. Such a process is time-consuming and expensive, and in the case of general practitioners (GPs), it may be impractical for the majority of General District or NHS Trust hospitals.
In practice, it is likely that radiologists will use the guidelines issued by the Royal College of Radiologists [6], which are intended for hospital practice and are based on national data, and amend them using their own experi- ence of local GP referral patterns. This experience may be based on a local survey or may be subjective. The guidelines will then be distributed to the referring GPs. There is little information available to quantify the effectiveness of such a policy with general practitioners. This study was designed to determine whether this approach is likely to result in a positive change in referral pattern,
M E T H O D S
Guidelines for referrals for chest radiography were developed after a previous study involving the prospec- tive analysis of 2017 consecutive chest radiograph refer- rals [7]. The presenting indications were compared with the subsequent radiological findings and those indica- tions with a particularly low yield were identified (Table 1). These guidelines, therefore, were specifically relevant to local practice and they highlighted those groups of
Correspondence to: Dr P. W. P. Bearcroft, Department of Radiology, Box 219, Addenbrooke's Hospital, Hills Road, Cambridge CB2 2QQ.
patients in whom, based on the previous study, significant abnormalities were uncommon. They were advisory only and included a general reminder that a good clinical history, together with a presumptive diagnosis, would allow a more helpful, accurate and patient-specific report.
GP practices were allocated using a random number table into either the study or control group. Guidelines were sent to all 122 GPs at the 33 practices in the study group during May 1991 together with relevant back- ground information, including a summary of a previous study performed at our department [7]. There was no communication with the 88 GPs in the control group. Neither group was aware that they were part of a study.
From June 1991 to July 1992, all 2500 GP requests for chest radiography were analysed prospectively. Demo- graphic and other relevant data were entered by a hospital audit officer. The majority of the examinations performed were then reported by one of two radiologists (PWPB and JS). They were graded into one of three groups: normal, significant abnormality and non-significant abnormality. The latter included age-related findings, chronic or congenital abnormalities and abnormalities unrelated to the presenting history which were felt to need no further investigation. The reporter was unaware from which group of GPs the request originated.
Table 1 - Summary of guidelines issued to general practitioners
The following groups of indications have been found to be associated with a low yield:
(1) Routine follow-up of patients with COAD. (2) Patients with hypertension as the only indication. (3) Those under 40 years old with non-specific ill health. (4) Those under 40 years old with non-specific chest pain. (5) A routine pre-employment screening examination. (6) Routine immigration examinations.
t
The general practitioners were reminded of the importance of giving a helpful clinical history including a presumptive diagnosis.
CHEST RADIOGRAPHY GUIDELINES
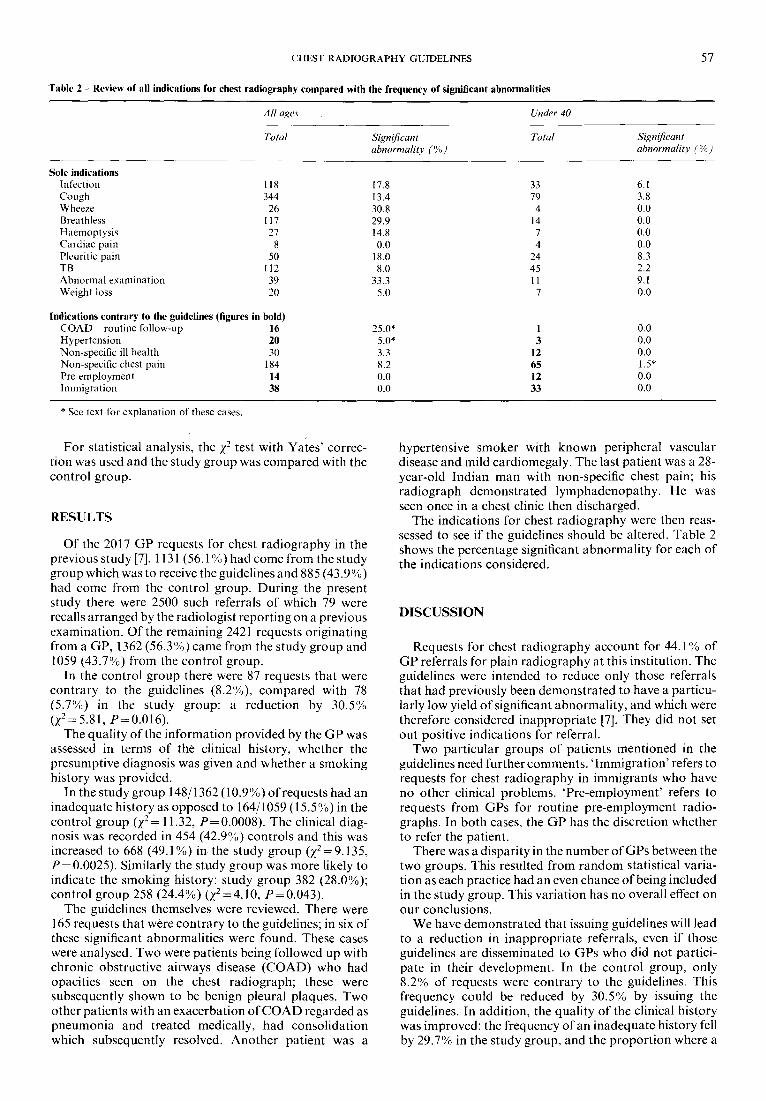
Table 2 - Review of all indications for chest radiography compared with the frequency of significant abnormalities
57
All ages Under 40
Total Significant Total abnormality (%)
Significant abnormality (%)
Sole indications Infection 118 17.8 33 6.1 Cough 344 13.4 79 3.8 Wheeze 26 30.8 4 0.0 Breathless 117 29.9 14 0.0 Haemoptysis 27 14.8 7 0.0 Cardiac pain 8 0.0 4 0.0 Pleuritic pain 50 18.0 24 8.3 TB 112 8.0 45 2.2 Abnormal examination 39 33.3 11 9.1 Weight loss 20 5.0 7 0.0
Indications contrary to the guidelines (figures in bold) COAD routine follow-up 16 25.0* 1 0.0 Hypertension 20 5.0" 3 0.0 Non-specific ill health 30 3.3 12 0.0 Non-specific chest pain 184 8.2 65 1.5" Pre-employment 14 0.0 12 0.0 Immigration 38 0.0 33 0.0
* See text for explanation of these cases.
For statistical analysis, the Z 2 test with Yates' correc- tion was used and the study group was compared with the control group.
RESULTS
Of the 2017 GP requests for chest radiography in the previous study [7], 1131 (56.1%) had come from the study group which was to receive the guidelines and 885 (43.9%) had come from the control group. During the present study there were 2500 such referrals of which 79 were recalls arranged by the radiologist reporting on a previous examination. Of the remaining 2421 requests originating from a GP, 1362 (56.3%0) came from the study group and 1059 (43.7%) from the control group.
In the control group there were 87 requests that were contrary to the guidelines (8.2%), compared with 78 (5.7%) in the study group: a reduction by 30.5% (Z2= 5.81, P=0.016).
The quality of the information provided by the GP was assessed in terms of the clinical history, whether the presumptive diagnosis was given and whether a smoking history was provided.
In the study group 148/1362 (10.9%) of requests had an inadequate history as opposed to 164/1059 (15.5 %) in the control group (Z 2 = 11.32, P = 0.0008). The clinical diag- nosis was recorded in 454 (42.9%) controls and this was increased to 668 (49.1%~ in the study group (Z2= 9.135, P = 0.0025). Similarly the study group was more likely to indicate the smoking history: study group 382 (28.0%); control group 258 (24.4%) (Z2= 4.10, P = 0.043).
The guidelines themselves were reviewed. There were 165 requests that were contrary to the guidelines; in six of these significant abnormalities were found. These cases were analysed. Two were patients being followed up with chronic obstructive airways disease (COAD) who had opacities seen on the chest radiograph; these were subsequently shown to be benign pleural plaques. Two other patients with an exacerbation of COAD regarded as pneumonia and treated medically, had consolidation which subsequently resolved. Another patient was a
hypertensive smoker with known peripheral vascular disease and mild cardiomegaly. The last patient was a 28- year-old Indian man with non-specific chest pain; his radiograph demonstrated lymphadenopathy. He was seen once in a chest clinic then discharged.
The indications for chest radiography were then reas- sessed to see if the guidelines should be altered. Table 2 shows the percentage significant abnormality for each of the indications considered,
D I S C U S S I O N
Requests for chest radiography account for 44.1% of GP referrals for plain radiography at this institution. The guidelines were intended to reduce only those referrals that had previously been demonstrated to have a particu- larly low yield of significant abnormality, and which were therefore considered inappropriate [7], They did not set out positive indications for referral.
Two particular groups of patients mentioned in the guidelines need further comments. ' Immigrat ion ' refers to requests for chest radiography in immigrants who have no other clinical problems. 'Pre-employment ' refers to requests from GPs for routine pre-employment radio- graphs. In both cases, the GP has the discretion whether to refer the patient.
There was a disparity in the number of GPs between the two groups. This resulted from random statistical varia- tion as each practice had an even chance of being included in the study group. This variation has no overall effect on our conclusions.
We have demonstrated that issuing guidelines will lead to a reduction in inappropriate referrals, even if those guidelines are disseminated to GPs who did not partici- pate in their development. In the control group, only 8.2% of requests were contrary to the guidelines. This frequency could be reduced by 30.5% by issuing the guidelines. In addition, the quality of the clinical history was improved: the frequency of an inadequate history fell by 29.7% in the study group, and the proportion where a

58 CLINICAL RADIOLOGY
smoking history and a presumptive diagnosis were men- tioned increased by 14.8'7o and 14.5% respectively.
We found that issuing guidelines resulted in no overall reduction in the referral rate in the study group. There are two contributing factors to this. Firstly, the guidelines only related to a small subset of all the clinical indications for referral 8.2% in the control group. The remaining 91.8% of referrals can therefore be considered appro- priate and it was not our aim to reduce these referrals as significant pathology could be missed. A further reduc- tion in inappropriate referrals would therefore have little effect on the overall referral rate. Second, GPs on the periphery of our catchment area have a choice of hospitals to which to refer and issuing guidelines may have encouraged referral to our department. This would swell the numbers of referrals in the study group, by an amount that is unquantifiable, but would not affect the control group. In addition, there may have been cross- fertilization between study and control groups as GPs meet professionally and socially. Such an effect would be conservative, leading to a reduction in the overall differ- ence.
We confirmed that, if our guidelines had been adhered to, no significant pathology would have been missed during the study. In addition, reanalysis of the referrals produced the same six groups of patients showing that the results of the previous study are reproducible [7].
A comparable study issued guidelines for several targeted examinations to all referring GPs [8]. There was a reduction by 28% in requests for those examinations that had been targeted. That study used non-targeted examin- ations as controls. They did not discuss changes in the clinical information provided.
The data needed for this analysis had to be collected specifically for the purpose. It would not be possible to use the data that are already collected routinely as a basis for a pilot study nor for subsequent clinical audit; this has obvious financial implications [9-11].
C O N C L U S I O N
Issuing guidelines to GPs is an effective technique to reduce inappropriate requests for chest radiography even when the overall standard of referral is high. Conversely, appropriate referrals are not affected. The quality of the clinical information can also be improved. We conclude that developing and disseminating guidelines in this way is a practical approach that is both effective and accept- able to our GP colleagues.
REFERENCES
1 Russell I, Grimshaw J. The effectiveness of referral guidelines: a review of the methods and findings of published evaluations. In: Roland M & Coulter A, eds. Hospital Referrals. Oxford: Oxford University Press, 1992:124 138.
2 Mugford M, Banfield P, O'Hanlow M. Effects of feedback of information on clinical practice: a review. British Medical Journal 1991;303:398-402.
3 Nelson AR. Orphan data and the unclosed loop: a dilemma in PSRO and medical audit. New England Journal of Medicine 1976; 295(11):617-619.
4 Royal College of Radiologists Working Party. Influence of the Royal College of Radiologists guidelines on hospital practice: a multicentre study. British Medical Journal 1992;304:740 743.
5 Fowkes FGR, Evans KT, Hartley G. Multicentre trial of 4 strategies to reduce use of a radiological test. Lancet 1986;i:367 370.
6 Royal College of Radiologists. Making the best use of a department of radiology. Guidefines for doctors. London: Royal College of Radiologists, I989.
7 Keogan M J, Padhani AR, Flower CDR. Chest radiography for general practitioners: scope for change? Clinical Radiology 1992; 46:51-54.
8 Vos Meiring P, Wells IP. The effect of radiological guidelines for General Practitioners in Plymouth. Clinical Radiology 1990;42:327 329.
9 Yudkin PL, Redman CWG. Obstetric audit using routinely col- lected computerised data. British Medical Journal 1990:301 : 1371 1373.
10 Crombie IK, Davies HTO. Computers in audit: servants or sirens? British Medical Journal 1991;303:403 404.
11 Lyons C. Gumpert R. Medical audit data: counting is not enough. British Medical Journal 1990;300:1563 1566.





























